branhamella catarrhalis respiratory infections fileabstracf: bronhomei/q catan-holis is an aerobic...
TRANSCRIPT

Eur Resplr J 1992, 5, 67H79
Branhamella catarrhalis respiratory Infections
B. Barreiro*, L. Esteban*, E. Prats*, E. Verdaguer**, J. Dorca*, F. Manresa*
Branhamella catarrhalis respiratory infections. B. Barreiro, L. Esteban, E. Prats, E. Verdaguer, J . Dorca, F. Manresa.
Depts of • Pneumology and • • Microbiology, Hospital de Bellvitge, University of Barcelona, Barcelona, Spain. ABSTRACf: Bronhomei/Q catan-holis Is an aerobic Gram-negative diplococcus. It
has been traditionally regarded as an oropharyngeal commensal and untU recently was only identified as a pathogen In cases of bronchopulmonary Infections. The aim of this study was to analyse the characteristics of the respiratory Infections caused by B. catarrhalis and to know the antibiotic susceptibility of this microorganism.
Correspondence: B. Barreiro Servei de Pneumologia Hospital de Bellvitge Cl Feixa Llarga s/n 08907 L'Hospitalet del Llobregat Barcelona We retrospectively studied 32 lower respiratory tract Infections, caused by B.
catan-halis (20 cases of bronchial Infection and 12 cases of pneumonia), diagnosed between 1988-1989 in our hospital.
Spain
Keywords: Antibiotic resistance Branhamel/a catarrlralis bronchial infection
All patients bad an underlying disease; ch.ronic obstructive pulmonary disease (COPD) and chronic heart disease being the most frequent. The aetiological diagnostic procedures were: sputum culture in 28 cases (15 In pure culture and 13 mixed), protected specimen brush (PSB) In three cases and transthoracic needle aspiration (TNA) In one case. Twenty B. catarrhalis Isolates were penicillin and ampic.lllin·resistant, 11 In the pneumorua group and 9 In the bronchial Infection group. All Isolates were sensitive to amoxyclllin·clavulanlc acid and second generation cephalosporin. ln our group four patients died.
pneumonia
Received: June 28 1991 Accepted after revision February 11 1992
We conclude that B. catan-halis Is a not Infrequent cause of respiratory lnfec· tion, particularly In COPD patients, and that the high incidence of antibiotic resistance to penidlUn and ampicillin should be taken Into account before consld· erlng an empirical antibiotic treatment. Eur Respir J., 1992, 5, 675-679.
B. catarrhalis is a Gram·negative coccus, commonly found in the upper respiratory tract. Although it has long been considered a nonpathogenic commensal, some sporadic cases of sinusitis, laryngitis, otitis media, sepsis, endocarditis and pneumonia have been reported in children and adults [1-4).
Nowadays, however, B. catarrha/is is third after Haemophilus influenzae and Streptococcus pneumoniae [1, 5] as the causative organism in lower respiratory tract infections, and various degrees of antibiotic resistance for B. catarrhalis have been reported [6-9).
We have retrospectively analysed the lower respira· tory tract infections caused by B. catarrhalis seen in our hospital.
Materials and methods
We have reviewed all of the B. catarrha/is isolates obtained from the respiratory samples (sputum, transthoracic needle aspiration (TNA) and bronchoscopic protected specimen brush (PSB)), blood and pleural fluid of those patients admitted into the hospital with respiratory infection and from all those who had nosocomial pneumonia, during a period of two years, from January 1988 until December 1989.
We used the criteria described by MuRRAY and WAsHINGTON [10) for microscopic examination of sputum cytology. If specimens demonstrated a preponderance of polymorphonuclear leucocytes and less than 25 squamous epithelial cells per high-power field (HPF), we cultured on general purpose media (blood agar, chocolate agar and on differential medium McConkey agar). Isolates from protected catheter brush were cultured quantitatively in aerobic and anaerobic media: cut-off point to separate colonization and infection was 103 colony forming units (CFU)·ml·1
[11, 12]. B. catarrhalis was identified as intracellular or extracellular Gram-negative diplococci with a positive oxidase-catalase reaction [13, 14]. The samples were tested for antibiotics using a disk diffusion test, BAUER
et al. [15], and the penicillin-resistant samples were tested for the production of beta-lactamase using a chromogenic cephalosporin test (Nitrocefin disk~) [16]. The isolates were separated into mixed and pure, but all of them were considered for the study.
The diagnosis of pneumonia was accepted when clinical symptoms of respiratory tract infection (cough, purulent phlegm, chest pain and fever) were present in association with a pulmonary infiltration. When no radiological abnormalities accompanied the clinical symptoms, the case was considered a bronchial
676 B. BARREIRO ET AL.
infection. We collected the following information from each of the patients: age, sex, underlying disease, clinical symptoms, origin of collected samples, bacteriological results with beta-lactamase production, chest X-ray findings and clinical outcome.
Results
During this two year period, B. catarrhalis was isolated from respiratory secretions of 32 patients: 12 had pneumonia and 20 bronchial infection. Table 1 shows the general characteristics of the patients with pneumonia and bronchial infection caused by B. catarrhalis.
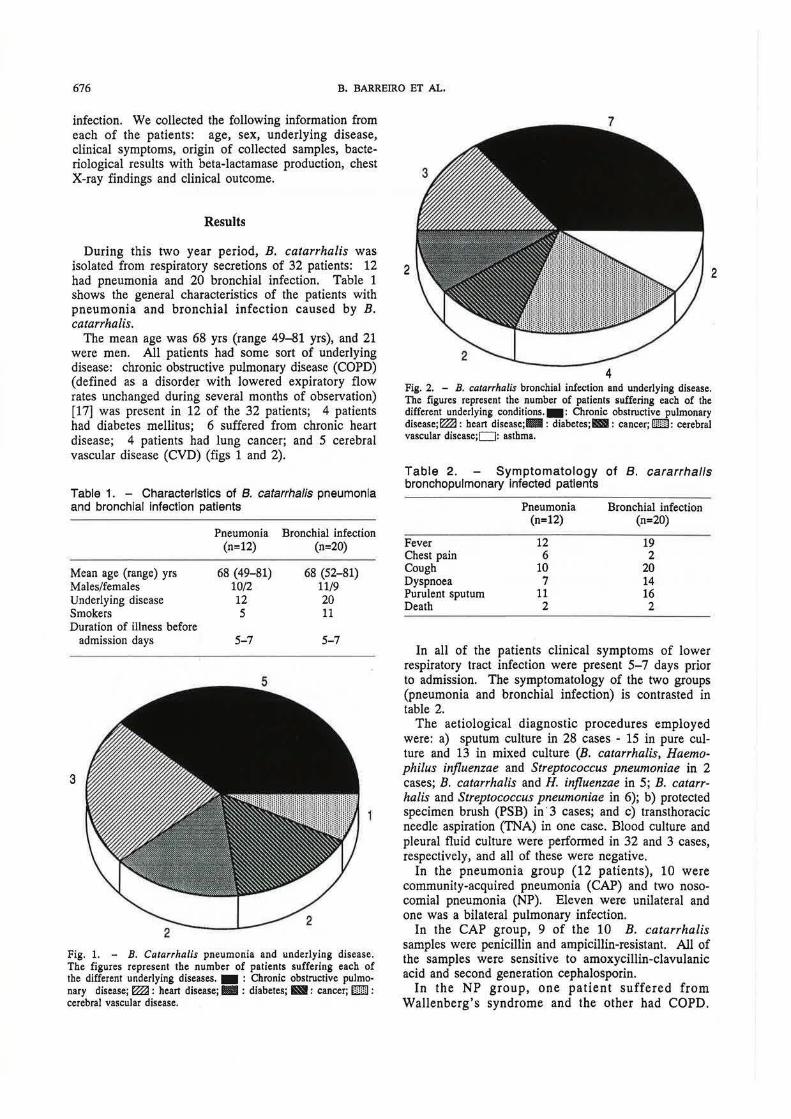
The mean age was 68 yrs (range 49-81 yrs), and 21 were men. ALl patients had some sort of underlying disease: chronic obstructive pulmonary disease (COPD) (defined as a disorde.r with lowered expiratory flow rates unchanged during several months of observation) [17] was present in 12 of the 32 patients; 4 patients had diabetes mellitus; 6 suffered from chronic heart disease; 4 patients had lung cancer; and 5 cerebral vascular disease (CVD) (figs 1 and 2).
Table 1. - Characteristics of B. catarrhalls pneumonia and bronchial Infection patients
Mean age (range) yrs Males/females Underlying disease Smokers Duration of illness before
admission days
3
Pneumonia (n=12)
68 (49-81) 10/2 12 5
5-7
Bronchial infection (n=20)
68 (52-81) 11/9 20 11
5-7
Fig. 1. - B. Catarrhalis pneumonia and underlying disease. The figures represent the number of patients suffering each of the different underlying diseases. - : Chronic obstructive pulmonary disease; ~ : heart disease;- : diabetes; Ill: cancer; m : cerebral vascular disease.
4 Fig. 2. - B. catarrhalis bronchial infection and underlying disease. The figures represent the number of patients suffering each of the different underlying conditions.-: Chronic obstructive pulmonary disease;~: heart disease;-: diabetes;BI: cancer; W: cerebral vascular disease;O : astbma.
Table 2. Symptomatology of B. cararrhalis bronchopulmonary Infected patients
Fever Chest pain Cough Dyspnoea Purulent sputum Death
Pneumonia (n=12)
12 6
10 7
11 2
Bronchial infection (n=20)
19 2
20 14 16 2
In all of the patients clinical symptoms of lower respiratory tract infection were present 5-7 days prior to admission. The symptomatology of the two groups (pneumonia and bronchial infection) is contrasted in table 2.
The aetiological diagnostic procedures employed were: a) sputum culture in 28 cases - 15 in pure culture and 13 in mixed culture (B. catarrhalis, Haemophi/us influenzae and Streptococcus pneumoniae in 2 cases; B. catarrhalis and H. influenzae in 5; B. catarrhalis and Streptococcus pneumoniae in 6); b) protected specimen brush (PSB) in· 3 cases; and c) transthoracic needle aspiration (TNA) in one case. Blood culture and pleural fluid culture were performed in 32 and 3 cases, respectively, and all of these were negative.
In the pneumonia group (12 patients), 10 were community-acquired pneumonia (CAP) and two nosocomial pneumonia (NP). Eleven were unilateral and one was a bilateral pulmonary infection.
In the CAP group, 9 of the 10 B. catarrhalis samples were penicillin and ampicillin-resistant. All of the samples were sensitive to amoxycillin-clavulanic acid and second generation cephalosporin.
In the NP group, one patient suffered from Wallenberg's syndrome and the other had COPD.

BRANHAMELLA CATARRHALIS RESPIRATORY INFECTIONS 677
25
20
~
~ 15 0 :n
..0 E
10 ::::J z
5
0 Pen Amp TMP-SMZ Tetr A-cla Cef(2)
Antibiotic resistance
Fig. 3. - Antibiotic resistance of B. catarrhalis. The figures at the top of the columns represent the number of B. catarrhalis samples resistant to the antibiotics. Pen: penicillin; Amp: ampicillin; TMP-SMZ: trimethoprim-sulphamethoxazole; Tetr: tetracycline; A-cla: amoxycillinclavulanic acid; Cef(2): second generation cephalosporin.
The first patient was treated with amoxycillin and cefonicid and died from his underlying disease within the first four days of treatment. The patient with COPD was treated with cefotaxime and recovered from the pneumonia. All samples in this group were penicillin and ampicillin-resistant, but sensitive to amoxycillin-clavulanic acid and second generation cephalosporin.
In the group of bronchial infection caused by B. catarrhalis, 9 of the 20 B. catarrhalis samples were penicillin and ampicillin resistant. All of the B. catarrhalis obtained from the respiratory samples in this group were amoxycillin-clavulanic acid and second generation cephalosporin sensitive organisms.
The bacteriological results of our study were as follows: 1) 20 of the B. catarrhalis recovered from the respiratory samples were penicillin and ampicillinresistant organisms; 2) 16 were trimethoprimsulphamethoxazole resistant microorganisms; and 3) all strains were amoxycillin-clavulanic acid and second generation cephalosporin sensitive (fig. 3).
Discussion
Most reports establish the aetiological diagnosis of a respiratory tract infection caused by B. catarrhalis on the results of the sputum culture. Several authors support the view that when the B. catarrhalis is obtained in pure (or with great predominance) culture of the sputum, the use of other bacteriological procedures is not necessary for the aetiological diagnosis [1, 5, 18, 19). In the literature we can find arguments in favour of the causative role of B. catarrhalis in a respiratory infection such as: a) B. catarrhalis has been observed in histological preparations of patients who had died of pneumonia [18]; b) previous studies have
demonstrated that the finding of B. catarrhalis in large numbers in expectorated sputum specimens correlate well with recovery of the organism by transtracheal aspiration (5]; c) in many cases the pathogenic role of B. catarrhalis in respiratory infections has been demonstrated by the isolation of the microorganism in a respiratory sample (pure or predominant culture), a favourable clinical outcome and the disappearance of the microorganism from the sputum with the appropriate antibiotic [9, 20).
As reported in most series, a high percentage of these patients had an underlying disease, and the frequent presence of other pathogens in the upper respiratory samples could complicate the interpretation of bacteriological results [18, 21]. In fact, all of the polymicrobial samples in our study showed the most common organisms usually found in the upper respiratory tract of COPD patients.
The diagnostic value of the transtracheal needle aspiration is about 80% in bacterial pneumonia and anaerobic pulmonary infections [22, 23]; but the specificity is reported to be low in some circumstances: 22% of patients with lung cancer and 40% of patients with chronic bronchitis show false positive results due to contamination of the bronchial tree (24, 25). For these reasons other invasive procedures could be useful in the diagnosis of B. catarrhalis pneumonia. In our study, four patients were diagnosed by means of non-conventional bacteriological procedures (three by PSB and one by TNA).
Table 3 shows a comparative analysis of the clinical and microbiological features of B. catarrhalis bronchopulmonary infections. During a period of two years 12 cases of pneumonia due to B. catarrhalis have been diagnosed. As has been observed in other studies, B. catarrhalis infection commonly affects patients with underlying disease, particularly COPD (2, 9, 20, 26-28).

678 8. BARREIRO ET AL.
Table 3. - Comparison with other reports on the clinical and microbiological features of B. catarrhalis pulmonary infection
NINANB et al. [1) SLEVJN et al. [5] WRJOIIT et al. [9) Barreiro et al.
Year 1978 1984 1990 1991 Patients n 11 101 42 32
Underlying COPD COPD COPD COPD disease Emphysema Asthma Cancer Asthma
Heart disease
Antibiotic Amp Amp Cef(3) Cef(3) treatment Ery Tetr Ery
Cef(2) A-cla A-cla Tetr TMP-SMZ Amp
Cef(2)
Beta-lactamase producing 10 30 67 62 B. catarrhalis %
Mortality n (%) 1(10) 5(5) 9(21) 4(12)
Amp: ampicillin; Ery: erythromycin; Cef(2): second generation cephalosporin; Cef(3): third generation cephalosporin; A-cla: amoxycillin-clavulanic acid; TMP-SMZ: trimethoprim-sulphamethoxazole; Tetr: tetracycline; COPD: chronic obstructive pulmonary disease.
In our study four patients died, a figure similar to the studies of NINANE et al. [1] and SLEVIN et al. [5] but lower than that obtained by WRIOHT et al. [9], probably because this last study included patients with cancer.
The respiratory infections are commonly treated with beta-lactam antibiotics [7]. The antibiotics administered in other reports were frequently beta-lactam antibiotics, erythromycin, tetracycline and trimethoprimsulphamethoxazole. These antibiotic treatments are similar to those used in our study, except for the last two antibiotics.
In our material, a large number of microorganisms are resistant to commonly used antibiotics: 20 were penicillin and ampicillin-resistant. This antibiotic resistance frequently leads to therapeutic failure. The indirect pathogenicity of B. catarrhalis has been definitely demonstrated by BROOK [29] in his overview on the failure of penicillin to eradicate a Group A betahaemolytic streptococcal infection in the presence of beta-lactamase producing bacteria, including B. catarrhalis.
When treating these diseases it is essential to know the minimal inhibitory concentration (MIC) of the different antibiotics. From table 3 it is evident that the increasing rate of beta-lactamase production by B. catarrhalis over the last 20 yrs is probably due to the routine use of commonly used antibiotics for respiratory infections.
According to our results, and those of others series, the therapeutic alternatives to the resistant microorganisms may be: amoxycillin-clavulanic acid [30], erythromycin, second or third generation cephalosporins and ciprofloxacin [31]. The selection of the appropriate antibiotic will reduce the morbidity and mortality of the patients with B. catarrhalis respiratory infections even
though in most cases the underlying disease is the most important prognostic factor [5, 8, 9].
We believe that: 1) B. catarrhalis respiratory tract infections are not uncommon in the community; and 2) in our geographical area the level of antibiotic resistance has important therapeutic implications.
References
1. Ninane G, Joly J, Kraytman M. - Bronchopulmonary infection due to Branhamel/a catarrhalis: 11 cases assessed by transtracheal puncture. Br Med J, 1978; 1: 276-278. 2. Doer GV, Miller MJ, Winn RE. - Branhamella (Neisseria) catarrhalis systemic disease in humans. Arch Intern Med, 1981; 141: 169(}...1692. 3. Right PW, Wallance RJ Jr. - Pneumonia due to Moraxella (Branhamella) catarrhalis. Semin Respir Infec, 1989; 4(1): 40-46. 4. Guthrie R, Bakenjaster K, Nelson R, Woskobnik R. -Branhamella catarrhalis sepsis: a case report and review of the literature. J Infect Dis, 1988; 158(4): 907. 5. Slevin NJ, Aitken J, Thornley P. - Clinical and microbiological features of Branhamella catarrhalis bronchopulmonary infection. Lancet, 1984; i: 782-783. 6. Calder MA, Croughan MJ, McLeod DT, Ahmed F. -The incidence and antibiotic susceptibility of Branhamella catarrhalis in respiratory infections. Drugs, 1986; 31 (Suppl. 3): 11-16. 7. Kallings I. - Sensivity of Branhamella catarrhalis to oral antibiotics. Drugs, 1986; 31 (Suppl. 3): 17-22. 8. McLeod DT, Calder MJ, Croughan MJ, Ahmed F. -Bronchopulmonary infection due to Branhamella catarrhalis. Clinical features and therapeutic response. Drugs, 1986; 31 (Suppl. 3): 109-112. 9. Wright PW, Wallace RJ, Shepherd R. - A descriptive study of 42 cases of Branhamella catarrhalis pneumonia. Am J Med, 1990; 88 (Suppl. SA): 2S-8S.

BRANHAMEUA CATARRHALIS RESPIRATORY INFECTIONS 679
10. Murray PR, Washington JA. - Microscopic and bacteriologic analysis of expectorated sputum. Mayo C/in Proc, 1975; 50: 339-344. 11. Wimberley N, Bass JB, Boid BW, Kirkpatrick MB, Serio RA, Pollock HM. - Use of bronchosropic protected catheter brush for the diagnosis of pulmonary infections. Chest, 1982; 81: 556-562. 12. Chastre J, Vian F, Brun P. - Prospective evaluation of the protected specimen brush for the diagnosis of pulmonary infections in ventilated patients. Am Rev Respir Dis, 1984; 130: 924-929. 13. Doern GV, Morse S. - Branhamella (Neisseria) catarrhalis: criteria for laboratory identification. J Clin Microbial, 1980; 11(2): 193-195. 14. Aitken J, Thornley P. - Isolation of Branhamella catarrhalis from sputum and tracheal aspirate. J Clin Microbial, 1983; 18(5): 1262-1263. 15. Bauer A, Kirby W, Sherris WM, Turk M. - Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol, 1966; 45: 493. 16. Montgomery K, Raymundo J, Drew WL. - Chromogenic cephalosporin spot test to detect beta-lactamase in clinically significant bacteria. J Clin Microbial, 1979; 9: 205. 17. ATS. - Standards for the diagnosis and care of patients with chronic obstructive lung disease (COPD) and asthma. Am Rev Respir Dis, 1986; 2: 225-228. 18. Thornley P, Aitken J, Drennan Ch. - Branhamella catarrhalis infection of the lower respiratory tract: reliable diagnosis by sputum examination. Br Med J, 1982; 285: 1537-1538. 19. Riou JY, Guibourdenche M. - Branhamel/a catarrhalis. New methods of bacterial diagnosis. Drugs, 1986; 31 (Suppl. 3): 1-6. 20. Nicotra B, Rivers M, Lumen I, Wallace R. Branhamella catarrhalis as a lower respiratory tract pathogen
in patients with chronic lung disease. Arch Intern Med, 1986; 146: 890-893. 21. Pollard AJ, Wallace RJ, Wilson RW, Nash D, Luman JI. - Incidence of Branhame/la catarrhalis in the sputa of patients with chronic lung disease. Drugs, 1986; 31 (Suppl. 3): 103-108. 22. lrvin R, Pratter M. - Transtracheal aspiration procedure: a protocol. Chest, 1981; 79: 245-247. 23. Ries K, Levison M, Kaye D. - Transtracheal aspiration in pulmonary infection. Arch Intern Med, 1974; 133: 453-458. 24. Bjerkestrand G, Digranes A, Schreiner A. - Bacteriological findings in transtracheal aspirates from patients with chronic bronchitis and bronchiectasis. Scand J Respir Dis, 1975; 56: 201-207. 25. Fosieck B, Parker RH, Cohen MH, Kane RC. Fiberoptic bronchoscopy and culture from the lower respiratory tract. Chest, 1977; 72: 5-9. 26. Srinivasan G, Raff MJ, Templeton W, Givens S, Graves C, Melo J. - Branhame/la catarrhalis pneumonia. Am Rev Respir Dis, 1981; 123: 553-555. 27. Capewell S, McLeod DT, Calder M, Coughan MJ, Ahmed F, Seaton A. - Pneumonia due to Branhame/la catarrhalis. Thorax, 1988; 43: 929-930. 28. Juen KY, Seto WH, Ong SJ. - The significance of Branhamella catarrhalis in bronchopulmonary infections. A case control study. J Infect, 1989; 19: 251-256. 29. Brook I. - Direct and indirect pathogenicity of Branhamella catarrhalis. Drugs, 1986; 31 (Suppl. 3): 97-102. 30. Thornley P, Aitken JM, Nichol G, Slevin N . Amoxycillin-clavulanic acid combination in bronchopulmonary infection due to beta-lactamase producing Branhamella catarrhalis. Drugs, 1986; 31 (Suppl. 3): 113-114. 31. Feleke G, Khan F. - Branhamella infections. An increasingly common respiratory illness. Postgrad Med, 1989; 85: 379-386.