brain injury in stillbirths confidential · iugr, abnormal brain liver ratio, stressed adrenals,...
TRANSCRIPT
ConfidentialBrain Injury in Stillbirths• Becher et al 471 SB
– 35% had brain injury• Suggests Stillbirth often has previous
acute events• More common in IUGR in preterms• Associated with smaller placenta
» BJOG 2006 113;310-7

Confidential
Intrapartum Stillbirth - brain stem showing older changes

ConfidentialPlacental changes• Ischaemic
– Small, abnormal shape (? Due to localised uterine effects)
– Infarcts and ischaemic changes– Unreconstructed blood vessels/Atherosis– Thrombotic
• Villitis– Some Viral most probably immune
• Chromosomal mosaicism

ConfidentialIschaemic
Normal

ConfidentialMaternal Vascular Invasion

Confidential
Preeclampsia

Confidential

Confidential
Term 2 kg. Placenta 359 g Fetal distress

Confidential

Confidential

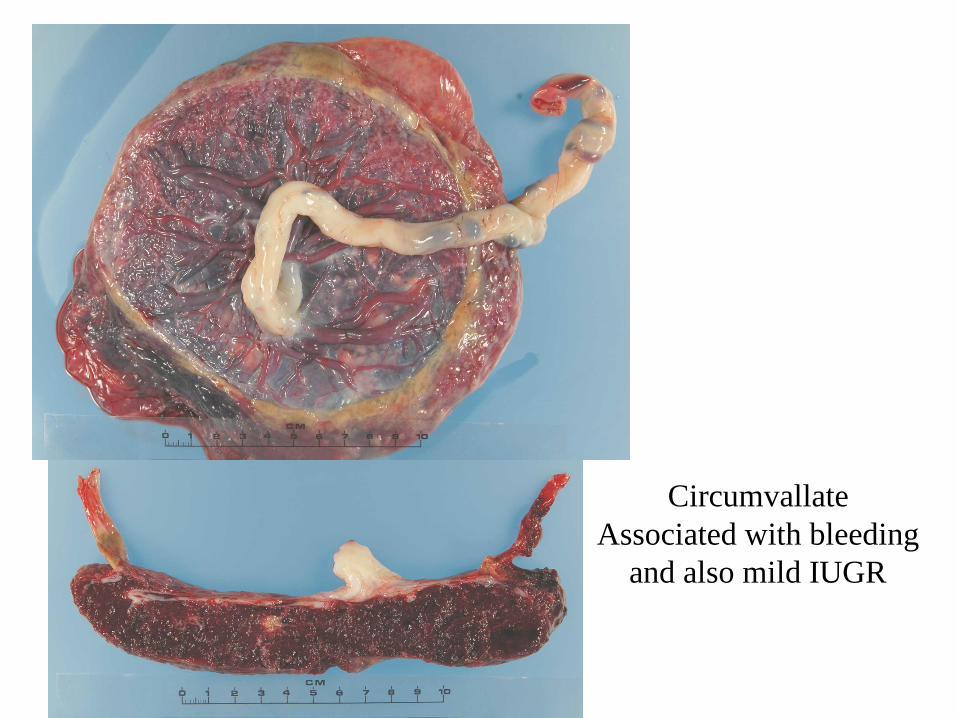
ConfidentialUmbilical cord and membranes
• Often thin in IUGR• Abnormal insertion• Circumvallate/circummarginate
membranes

ConfidentialVelamentous Cord insertion
Confidential
CircumvallateAssociated with bleeding
and also mild IUGR

ConfidentialIUGR vs non IUGR
• Often similar placental changes i.e. ischaemic seen in non-IUGR (including “unexplained Stillbirth”)
• Continuum of disease

ConfidentialModel(s)• The majority of stillbirths have some clues.• Many have evidence of chronic condition -
IUGR, abnormal brain liver ratio, stressed adrenals, costochondral junction, placental changes
• Many have evidence of previous brain changes
• Terminal episode appears to occur suddenly
• Therefore Stillbirth appears to have an acute and often a chronic cause

ConfidentialUnexplained
PIH/PE
IUGR
CongenitalAnomaly
Infection
The pigeon holes are not clearThe autopsy helps define the groups

ConfidentialPlacental Supply
Time
Relative demand
Sleeping/active, maternal pyrexia
Uterine contractions, IVC?
Term
Fetal demand
Absolute demand

ConfidentialThe tip of the DoHAD (Barker) Iceberg
• Stillbirths probably reflect the tip of fetal disease– Share features with
• Neonatal encephalopathy, Cerebral palsy, SIDS
– Abnormal fetal nutrition and metabolic syndrome

ConfidentialThe IUGR stillbirth and DOHAD
• The stillbirth and particularly the IUGR gives an insight into how the adult diseases may be developing in utero.
• Reduced number of glomeruli in kidney• Changes in IGF in rat liver with fetal IUGR
model• Pancreas ? No change in ß cells, ? Insulin
resistance

ConfidentialCESDI 8th Report -Adverse Findings
Failure to recognise high risk woman at booking 30Growth
Inadequate monitoring 33Failure to recognise or act on IUGR 35
Fetal MovementFailure to act on reduced fetal movements 21Mother reporting after delivery or not explained
48Management of pregnancy e.g high risk/diabetes
177Communications documentation 95Lifestyle, smoking poor antenal attendance
39Post delivery
Post mortem quality issues 66Screening 11
No. Comments
720 comment on 420 women

ConfidentialConclusion
• The autopsy (& particlularly the placenta) remains pivotal to obtaining information about each loss
• Helps identify and then classify IUGR• It provides important research possibilities• Quality of autopsy issues• It forms only part of the multidisciplinary
review of each case.

Confidential

ConfidentialAcknowledgements
• Jan Dickinson and Belinda Jennings & the PNLS team.
• Mary-Anne Measey & Catherine Harrison• Vicky Flenady & PSANZ Team• Cathy Buccilli-Douglas, Vivien Gee• The many parents who have allowed us to
examine their babies and given us the privilege to help them.

Confidential

ConfidentialCord anomalies• Cord Length
» >80 cm in 3.7%, 100 cm in 0.5%
• Knots (?10x) 1% of normal births• Nuchal loops (15% of normal deliveries)• Twists ?? <1 per 9cm• Velamentous and marginal cord SB 3-4 x more
common• Thin cord (often IUGR more prone to knots,
compression)• Meconium effects• Histological changes often not seen but?…….
» http://sidsalliance.org/conf2005/library/Cord%20Accident%20Ha