bone markers can give answers in 3 months how long do your ... · how long do your osteoporosis ....
TRANSCRIPT

Bone markers can give answers in 3 monthsHow long do your osteoporosis patients have to wait?

+1.0
-1.0
-2.0-2.5-3.0
-4.0
0.0 Normal Bone Density
Low Bone Mass
Presence of Osteoporosis
Determining the severity of a patient’s bone loss
Osteoporosis is a disease characterized by low bone mass and structural deterioration of bone tissue, leading to bone fragility and an increased risk of fractures of the hip, spine, and wrist.1
Flexible and intelligent solutions A bone mineral density (BMD) test is the standard process used to determine a patient’s bone health. The most commonly used BMD assay is a Dual Energy X-ray Absorptiometry (DXA) test.2
A patient’s DXA result is then compared to the ideal or peak BMD of a healthy 30-year old adult to yield that patient’s T-score. A T-score of 0 means that patient is equal to the norm. The more standard deviations below 0, the lower that patient’s BMD score and the higher their risk of bone fracture.2
Osteoporosis
The severity of a low T-score is depicted on this basic scale, where a T-score of -2.5 or lower indicates osteoporosis2
Normal healthy bone Diseased osteoporotic bone
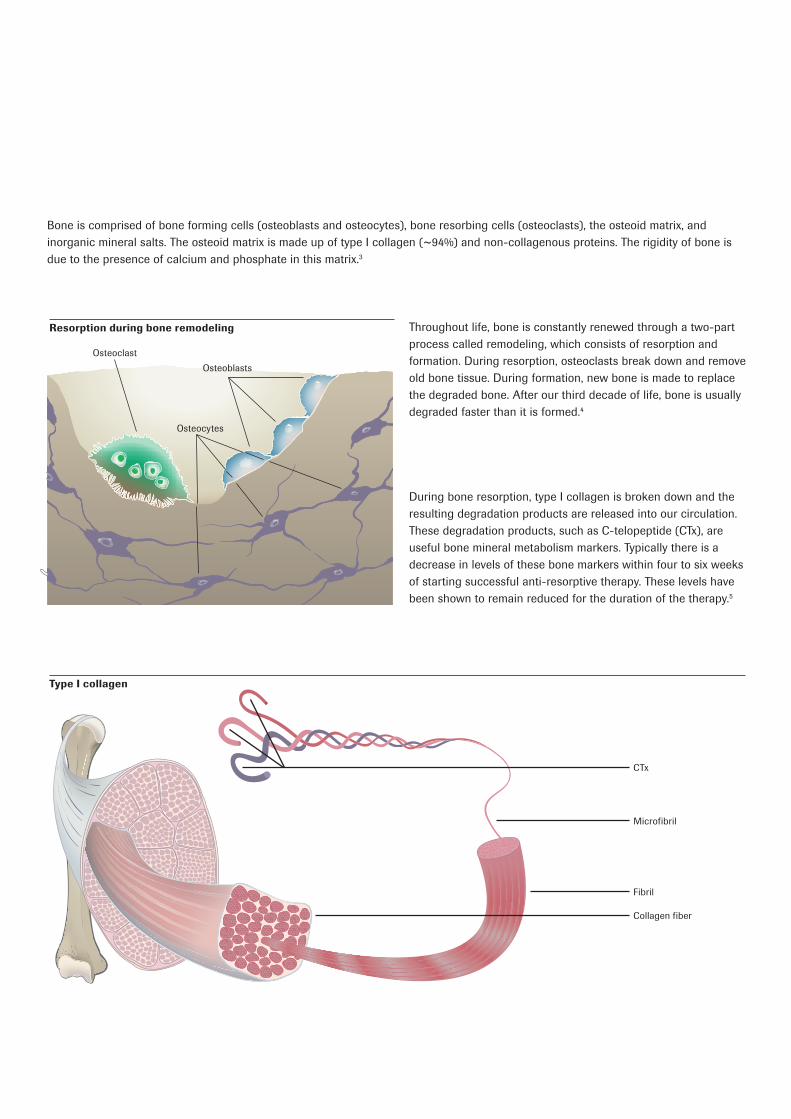
Bone is comprised of bone forming cells (osteoblasts and osteocytes), bone resorbing cells (osteoclasts), the osteoid matrix, and inorganic mineral salts. The osteoid matrix is made up of type I collagen (~94%) and non-collagenous proteins. The rigidity of bone is due to the presence of calcium and phosphate in this matrix.3
Throughout life, bone is constantly renewed through a two-part process called remodeling, which consists of resorption and formation. During resorption, osteoclasts break down and remove old bone tissue. During formation, new bone is made to replace the degraded bone. After our third decade of life, bone is usually degraded faster than it is formed.4
During bone resorption, type I collagen is broken down and the resulting degradation products are released into our circulation. These degradation products, such as C-telopeptide (CTx), are useful bone mineral metabolism markers. Typically there is a decrease in levels of these bone markers within four to six weeks of starting successful anti-resorptive therapy. These levels have been shown to remain reduced for the duration of the therapy.5
Resorption during bone remodeling
Type I collagen
Osteoblasts
Microfibril
CTx
Collagen fiber
Fibril
Osteocytes
Osteoclast
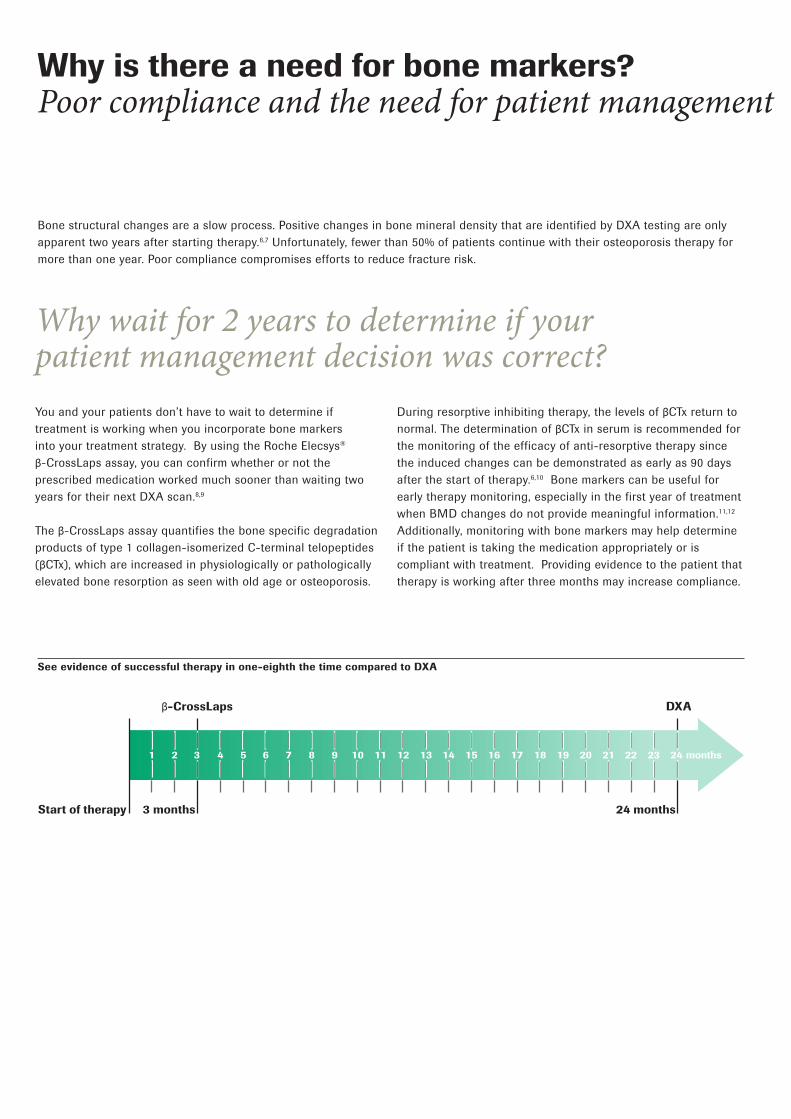
1 2 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 months3
Start of therapy 3 months
β-CrossLaps DXA
24 months
Why is there a need for bone markers?Poor compliance and the need for patient management
Bone structural changes are a slow process. Positive changes in bone mineral density that are identified by DXA testing are only apparent two years after starting therapy.6,7 Unfortunately, fewer than 50% of patients continue with their osteoporosis therapy for more than one year. Poor compliance compromises efforts to reduce fracture risk.
Why wait for 2 years to determine if your patient management decision was correct?You and your patients don’t have to wait to determine if treatment is working when you incorporate bone markers into your treatment strategy. By using the Roche Elecsys® β-CrossLaps assay, you can confirm whether or not the prescribed medication worked much sooner than waiting two years for their next DXA scan.8,9
The β-CrossLaps assay quantifies the bone specific degradation products of type 1 collagen-isomerized C-terminal telopeptides (βCTx), which are increased in physiologically or pathologically elevated bone resorption as seen with old age or osteoporosis.
During resorptive inhibiting therapy, the levels of βCTx return to normal. The determination of βCTx in serum is recommended for the monitoring of the efficacy of anti-resorptive therapy since the induced changes can be demonstrated as early as 90 days after the start of therapy.6,10 Bone markers can be useful for early therapy monitoring, especially in the first year of treatment when BMD changes do not provide meaningful information.11,12 Additionally, monitoring with bone markers may help determine if the patient is taking the medication appropriately or is compliant with treatment. Providing evidence to the patient that therapy is working after three months may increase compliance.
See evidence of successful therapy in one-eighth the time compared to DXA
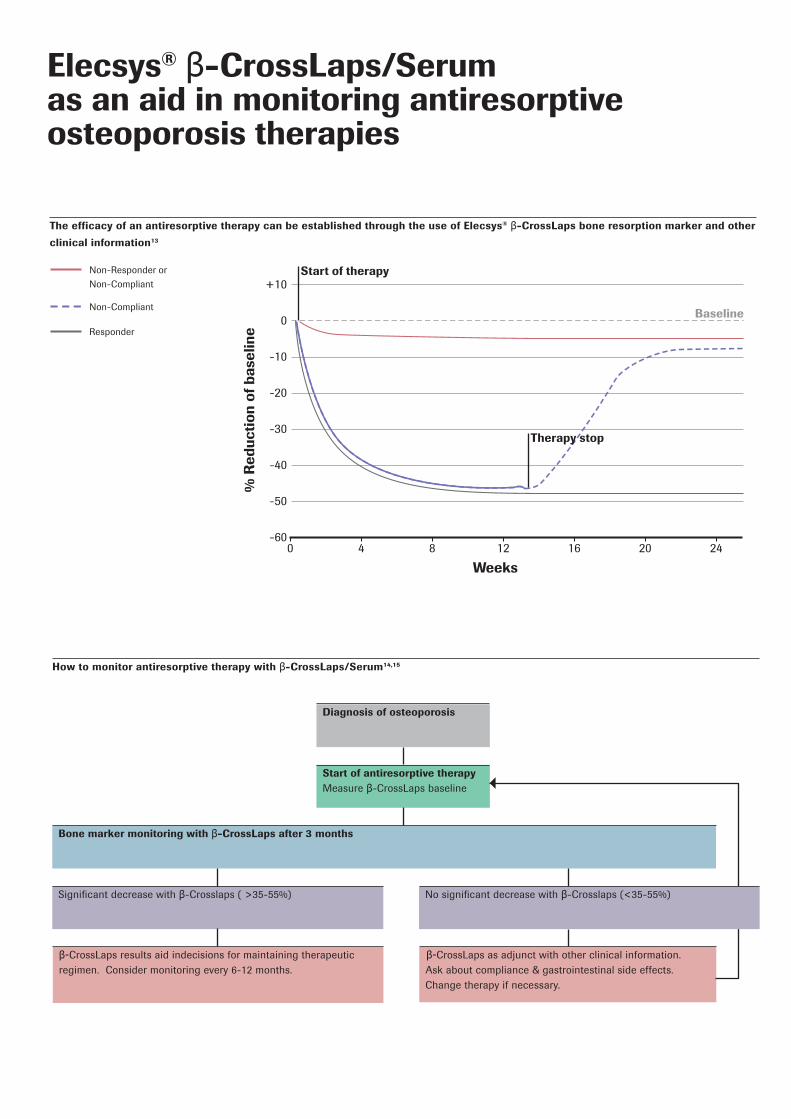
Diagnosis of osteoporosis
Start of antiresorptive therapy Measure β-CrossLaps baseline
Significant decrease with β-Crosslaps ( >35-55%)
β-CrossLaps results aid indecisions for maintaining therapeutic regimen. Consider monitoring every 6-12 months.
β-CrossLaps as adjunct with other clinical information. Ask about compliance & gastrointestinal side effects. Change therapy if necessary.
Bone marker monitoring with β-CrossLaps after 3 months
+10
-20
-30
-10
0
-50
-40
-60
% R
educ
tion
of b
asel
ine
0
Weeks84 16 2012 24
Start of therapyNon-Responder or
Non-Compliant
Non-Compliant
Responder
Therapy stop
Baseline
No significant decrease with β-Crosslaps (<35-55%)
How to monitor antiresorptive therapy with β-CrossLaps/Serum14,15
The efficacy of an antiresorptive therapy can be established through the use of Elecsys® β-CrossLaps bone resorption marker and other
clinical information13
Elecsys® β-CrossLaps/Serum as an aid in monitoring antiresorptive osteoporosis therapies
David Hevert, MDDavid B. Hevert is a board-certified Internist and is the founder of Glades Medical Group in Boca Raton, Florida. The Glades Medical Group services approximately 10,000 patients, many of whom have osteoporosis or osteopenia. For the past twenty-five years, Dr. Hevert has been medical director of a CLIA-certified lab.16
Presently, Dr. Hevert serves as Medical Director to the Louis & Anne Green Memory and Wellness Center at Florida Atlantic University (FAU) in addition to being the Medical Director for Manor Care Rehabilitation Center in Boca Raton. He is also a clinical professor for the Schmidt Medical School at FAU and University of Miami Miller School of Medicine.17
Bone healthBefore the use of bone markers, clinicians used basic x-ray films and imaging systems such as MRI and CT scans to determine bone health of a patient. Dual energy X-ray absorptiometry, or DXA, (previously DEXA) was designed to measure bone mineral density. A DXA scanner produces a high energy and low energy X-ray beam, which both pass through a patient’s bone. The amount that passes through is measured and the difference between the two beams determines bone density.2
β-CrossLaps / Serum CTx Roche’s β-CrossLaps is an immunoassay used to determine the amount of degradation products, namely CTx, of type I collagen as an aid in assessing bone resorption. The test may be used as an aid in monitoring anti-resorptive therapies in postmenopausal women and people diagnosed with osteopenia.10
David Hevert, MD
“Our practice has found CTx to be the best marker through our trials and research. It is easily done, cost-effective, requires no radiation, and can measure changes accurately.”
David Hevert, MD
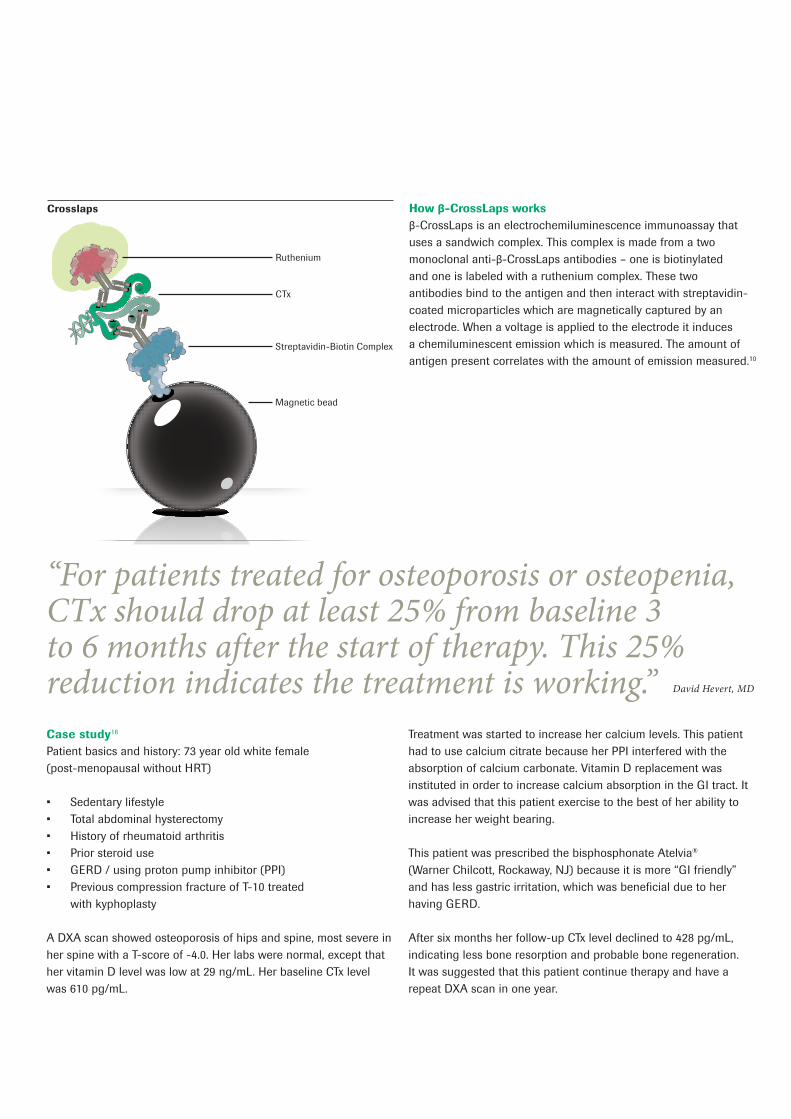
Magnetic bead
Streptavidin-Biotin Complex
CTx
Ruthenium
Crosslaps
“For patients treated for osteoporosis or osteopenia, CTx should drop at least 25% from baseline 3 to 6 months after the start of therapy. This 25% reduction indicates the treatment is working.”
How β-CrossLaps worksβ-CrossLaps is an electrochemiluminescence immunoassay that uses a sandwich complex. This complex is made from a two monoclonal anti-β-CrossLaps antibodies – one is biotinylated and one is labeled with a ruthenium complex. These two antibodies bind to the antigen and then interact with streptavidin-coated microparticles which are magnetically captured by an electrode. When a voltage is applied to the electrode it induces a chemiluminescent emission which is measured. The amount of antigen present correlates with the amount of emission measured.10
Case study16
Patient basics and history: 73 year old white female (post-menopausal without HRT)
• Sedentary lifestyle• Total abdominal hysterectomy• History of rheumatoid arthritis • Prior steroid use• GERD / using proton pump inhibitor (PPI)• Previous compression fracture of T-10 treated
with kyphoplasty
A DXA scan showed osteoporosis of hips and spine, most severe in her spine with a T-score of -4.0. Her labs were normal, except that her vitamin D level was low at 29 ng/mL. Her baseline CTx level was 610 pg/mL.
Treatment was started to increase her calcium levels. This patient had to use calcium citrate because her PPI interfered with the absorption of calcium carbonate. Vitamin D replacement was instituted in order to increase calcium absorption in the GI tract. It was advised that this patient exercise to the best of her ability to increase her weight bearing.
This patient was prescribed the bisphosphonate Atelvia® (Warner Chilcott, Rockaway, NJ) because it is more “GI friendly” and has less gastric irritation, which was beneficial due to her having GERD.
After six months her follow-up CTx level declined to 428 pg/mL, indicating less bone resorption and probable bone regeneration. It was suggested that this patient continue therapy and have a repeat DXA scan in one year.
COBAS and LIFE NEEDS ANSWERS are trademarks of Roche.
Elecsys® ß-CrossLaps assay are trademarks of Roche.Atelvia is a registered trademark of Warner Chilcott Company, LLC.
©2015 Roche
Roche Diagnostics International Ltd461-61822-0915USAwww.cobas.com
References NIH Osteoporosis and Related Bone Diseases National Resource Center web site. www.niams.nih.gov/
Health_Info/Bone/Osteoporosis/osteoporosis_ff.asp. Accessed September 30, 2015.
NIH Osteoporosis and Related Bone Diseases National Resource Center web site. www.niams.nih.gov/
Health_Info/Bone/Bone_Health/bone_mass_measure.asp. Accessed September 30, 2015.
International Osteoporosis Foundation web site. www.iofbonehealth.org/introduction-bone-biology-
all-about-our-bones. Accessed September 30, 2015.
NIH Osteoporosis and Related Bone Diseases National Resource Center web site. www.niams.nih.gov/
Health_Info/Bone/Bone_Health/. Accessed September 30, 2015.
Seibel MJ. Biochemical markers of bone turnover part I: Biochemistry and variability. Clin
Biochem Rev. 2005 26(4), 97-122.
North American Menopause Society. Management of osteoporosis in postmenopausal women. 2006 position statement of The North American Menopause Society. Menopause. 2006 13(3), 340-367.
Bonnick SL, Shulman L. Monitoring osteoporosis therapy: bone mineral density, bone turnover markers, or both? Am J Med. 2006 119(4 Suppl 1), S25-31.
Reginster JY. Adami S, Lakatos P, et al. Efficacy and tolerability of once-monthly oral ibandronate in postmenopausal osteoporosis: 2 year results from the MOBILE study. Ann
Rheum Dis. 2006 65(5), 654-661.
Black DM, Delmas PD, Eastell R et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med. 2007 356(18), 1809-1822.
ß-CrossLaps/serum [package insert]. Indianapolis, IN: Roche Diagnostics Corporation; 2013.
Vasikaran SD. Utility of biochemical markers of bone turnover and bone mineral density in management of osteoporosis. Crit Rev Clin Lab Sci. 2008 45(2), 221-258.
Garnero P. Biomarkers for osteoporosis management: utility in diagnosis, fracture risk prediction and therapy monitoring. Mol Diagn Ther. 2008 12(3), 157-70.
Tanko LB, Mouritzen U, Lehmann HJ, et al. Oral ibandronate: changes in markers of bone turnover during adequately dosed continuous and weekly therapy and during different suboptimally dosed treatment regimens. Bone. 2003 32(6), 687-693.
Brown JP, Albert C, Nassar BA, Adachi JD, Cole D, Davison KS, et al. Bone turnover markers in the management of postmenopausal osteoporosis. Clin Biochem. 2009 42(10-11), 929-942.
Delmas PD, Eastell R, Garnero P, Seibel MJ, Stepan J. The use of biochemical markers of bone turnover in osteoporosis: Committee of Scientific Advisors of the International Osteoporosis Foundation. Osteoporos Int. 2000 11(Suppl 6), S2-12.
Hevert DB. Glades Medical Group Experience. Roche Diagnostics Bone Turnover Marker Advisory Board Meeting. Orlando, FL. November 14, 2014.
Glades Medical Group web site. www.gladesmedical.com. Accessed September 30, 2015.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
xxxx
xxxx
xxx a
0000
- x.
x X
X