board meeting wednesday 10 december 2014 2.30pm a+ … · board meeting wednesday 10 december 2014...
TRANSCRIPT
Board Meeting
Wednesday 10 December 2014
2.30pm
A+ Trust RoomClinical Education Centre
Level 5Auckland City Hospital
Grafton
Communities, Quality Healthcare
Published 2/12/14
1

Auckland District Health BoardMeeting of the Board 10/12/14
AgendaMeeting of the Board
10 December 2014
Venue: A+ Trust Room, Clinical Education Centre, Level 5, Auckland City Hospital, Grafton
Time: 2.30pm
ADHB Board Members PresentDr Lester Levy (Chair)Jo AgnewPeter AitkenDoug ArmstrongJudith BassettDr Chris ChambersDr Lee Mathias (Deputy Chair)Robyn NortheyMorris PitaGwen Tepania-PalmerIan Ward
ADHB Management PresentAilsa Claire Chief Executive OfficerSimon Bowen Director of Health Outcomes – Auckland and
Waitemata District Health BoardsMargaret Dotchin Chief Nursing OfficerFionnagh Dougan Director Provider ServicesDr Debbie Holdsworth Director Funding – Auckland and Waitemata District
Health BoardsDr Andrew Old Chief Strategy, Participation and InnovationRosalie Percival Chief Financial OfficerLinda Wakeling Chief of Intelligence and InformaticsSue Waters Chief Health Professions OfficerDr Margaret Wilsher Chief Medical Officer
ADHB Senior StaffLita Foliaki Pacific Planning & Funding ManagerNaida Glavish General Manager Maori Health & Chief Advisor TikangaBruce Levi Acting Pacific General Manager for Hospital Services,
Waitemata and AucklandAuxilia Nyangoni Deputy Chief Financial OfficerMarlene Skelton Corporate Business ManagerGilbert Wong Director Communications
(Other staff members who attend for a particular item are named at the start of the minute for that item)
Apologies Members:
Apologies Staff: Margaret Dotchin, Fionnagh Dougan (early departure), Auxilia Nyangoni
Register of InterestsDoes any member have an interest they have not previously disclosed?Does any member have an interest that may give rise to a conflict of interest with a matter on the agenda?
Karakia
AgendaPlease note that agenda item times are estimates only
2.30pm 1 ATTENDANCE AND APOLOGIES
2 CONFLICTS OF INTEREST
2:35pm 3 CONFIRMATION OF MINUTES 29 OCTOBER 2014
4 ACTION POINTS 29 OCTOBER 2014 - NIL
2:40pm 5 PRESENTATION
2
Auckland District Health BoardMeeting of the Board 10/12/14
5.1 Services and Food Workers’ Union presenting their submission in relation to the future state of Food Services at Auckland DHB
2:55pm 6 CHAIRMAN’S REPORT – VERBAL
3:00pm 7 CHIEF EXECUTIVE’S REPORT
3:10pm 8 LIFT THE HEALTH OF PEOPLE IN AUCKLAND CITY – CPHAC RECOMMENDATIONS
8.1 The Auckland Plan – Working with Auckland Council to Create the World’sMost Liveable City
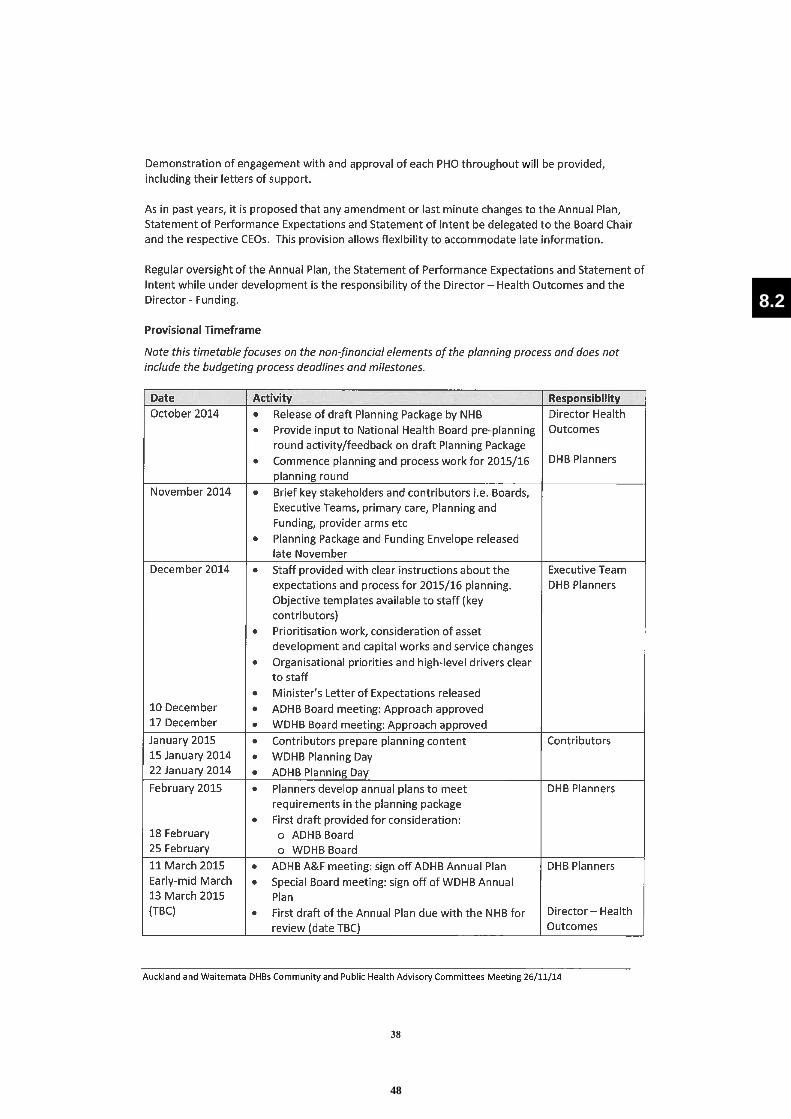
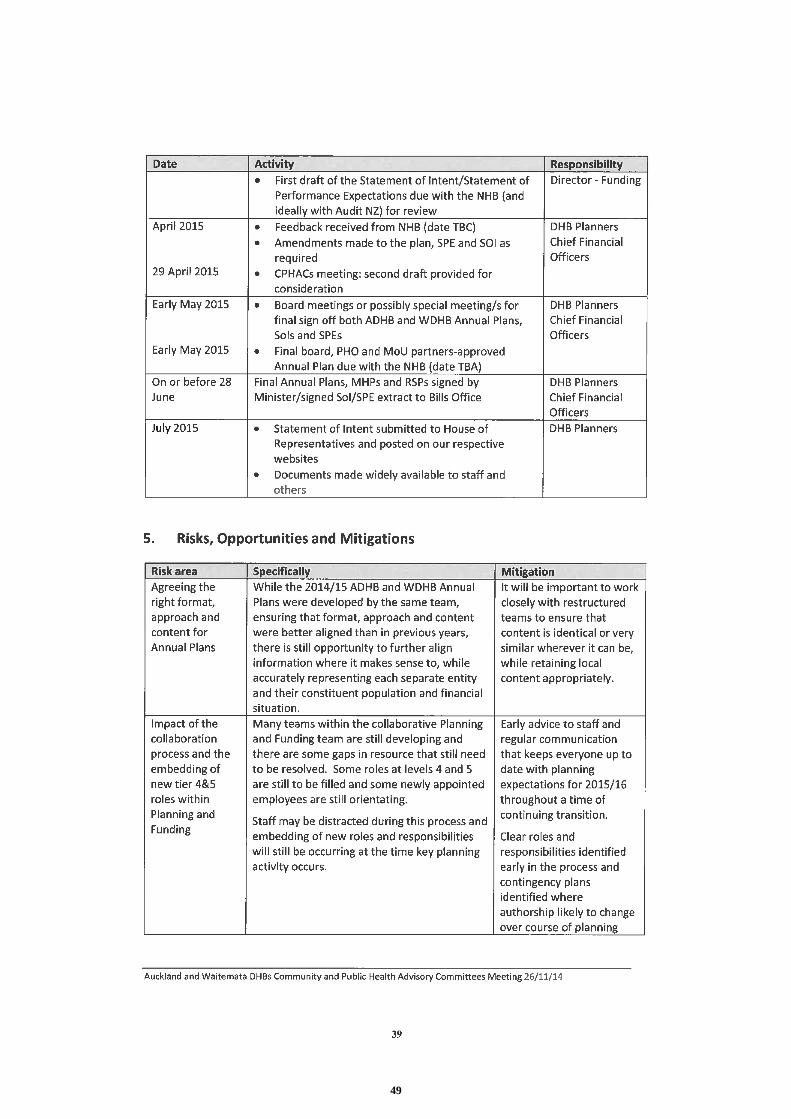
8.2 2015/2016 Annual Plan Approach
3:20pm 9 LIVE WITHIN OUR MEANS - NIL
3:25pm 10 GENERAL BUSINESS10.1 Te Toka Tumai – a Strategy for Auckland DHB to 201810.2 Establishment of Executive Committee of the Board
3:40pm 11 RESOLUTION TO EXCLUDE THE PUBLIC
Next Meeting Wednesday 18 February 2015 at 2.30pm A+ Trust Room, Clinical Education Centre, Level 5, Auckland City Hospital, Grafton
Hei Oranga Tika Mo Te Iti Me Te Rahi
Healthy Communities, Quality Healthcare
3
Auckland District Health BoardMeeting of the Board 17 September 2014
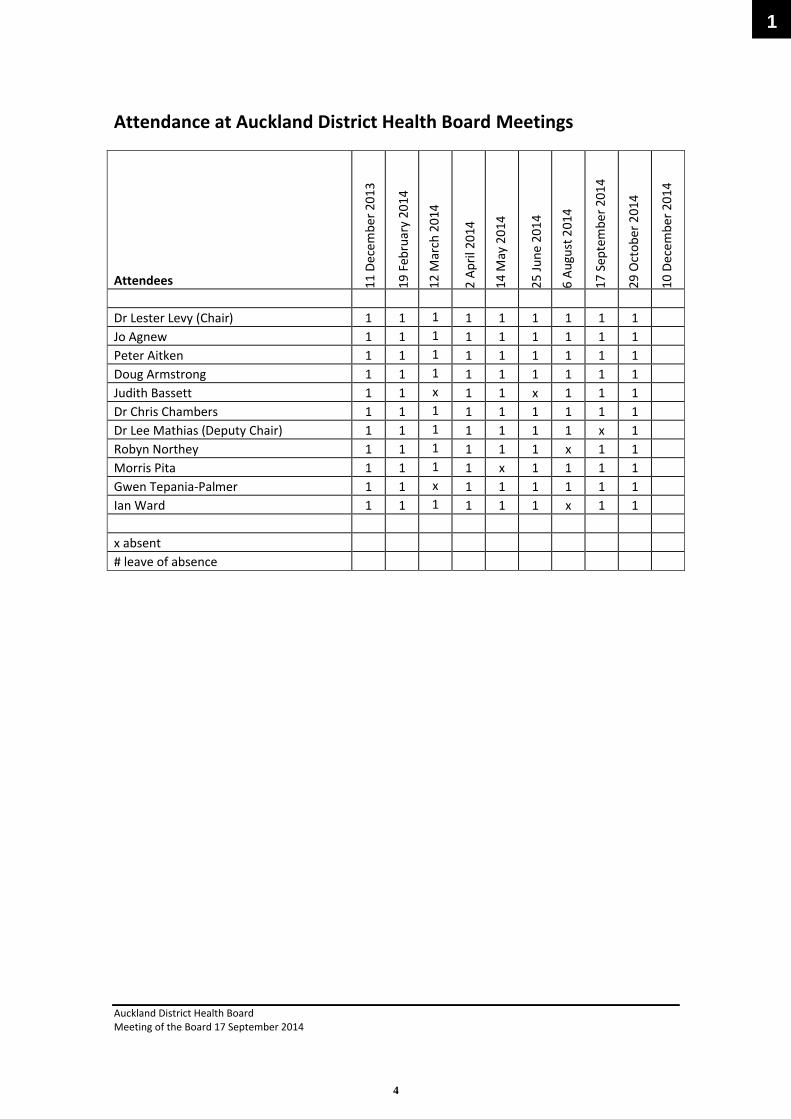
Attendance at Auckland District Health Board Meetings
Attendees 11 D
ecem
ber 2
013
19 F
ebru
ary
2014
12 M
arch
201
4
2 Ap
ril 2
014
14 M
ay 2
014
25 Ju
ne 2
014
6 Au
gust
201
4
17 S
epte
mbe
r 201
4
29 O
ctob
er 2
014
10 D
ecem
ber 2
014
Dr Lester Levy (Chair) 1 1 1 1 1 1 1 1 1Jo Agnew 1 1 1 1 1 1 1 1 1Peter Aitken 1 1 1 1 1 1 1 1 1Doug Armstrong 1 1 1 1 1 1 1 1 1Judith Bassett 1 1 x 1 1 x 1 1 1Dr Chris Chambers 1 1 1 1 1 1 1 1 1Dr Lee Mathias (Deputy Chair) 1 1 1 1 1 1 1 x 1Robyn Northey 1 1 1 1 1 1 x 1 1Morris Pita 1 1 1 1 x 1 1 1 1Gwen Tepania-Palmer 1 1 x 1 1 1 1 1 1Ian Ward 1 1 1 1 1 1 x 1 1
x absent# leave of absence
1
4

Auckland District Health BoardBoard Meeting 10 December 2014
Conflicts of Interest Quick Reference GuideUnder the NZ Public Health and Disability Act Board members must disclose all interests, and the full nature of the interest, as soon as practicable after the relevant facts come to his or her knowledge.
An “interest” can include, but is not limited to:
∑ Being a party to, or deriving a financial benefit from, a transaction∑ Having a financial interest in another party to a transaction∑ Being a director, member, official, partner or trustee of another party to a transaction or a
person who will or may derive a financial benefit from it∑ Being the parent, child, spouse or partner of another person or party who will or may derive a
financial benefit from the transaction∑ Being otherwise directly or indirectly interested in the transaction
If the interest is so remote or insignificant that it cannot reasonably be regarded as likely to influence the Board member in carrying out duties under the Act then he or she may not be “interested in the transaction”. The Board should generally make this decision, not the individual concerned.
Gifts and offers of hospitality or sponsorship could be perceived as influencing your activities as a Board member and are unlikely to be appropriate in any circumstances.
∑ When a disclosure is made the Board member concerned must not take part in any deliberation or decision of the Board relating to the transaction, or be included in any quorum or decision, or sign any documents related to the transaction.
∑ The disclosure must be recorded in the minutes of the next meeting and entered into the interests register.
∑ The member can take part in deliberations (but not any decision) of the Board in relation to the transaction if the majority of other members of the Board permit the member to do so.
∑ If this occurs, the minutes of the meeting must record the permission given and the majority’s reasons for doing so, along with what the member said during any deliberation of the Board relating to the transaction concerned.
IMPORTANT
If in doubt – declare.
Ensure the full nature of the interest is disclosed, not just the existence of the interest.
This sheet provides summary information only - refer to clause 36, schedule 3 of the New Zealand Public Health and Disability Act 2000 and the Crown Entities Act 2004 for further information (available at www.legisaltion.govt.nz) and “Managing Conflicts of Interest – Guidance for Public Entities” (www.oag.govt.nz ).
2
5
Auckland District Health BoardBoard Meeting 10 December 2014
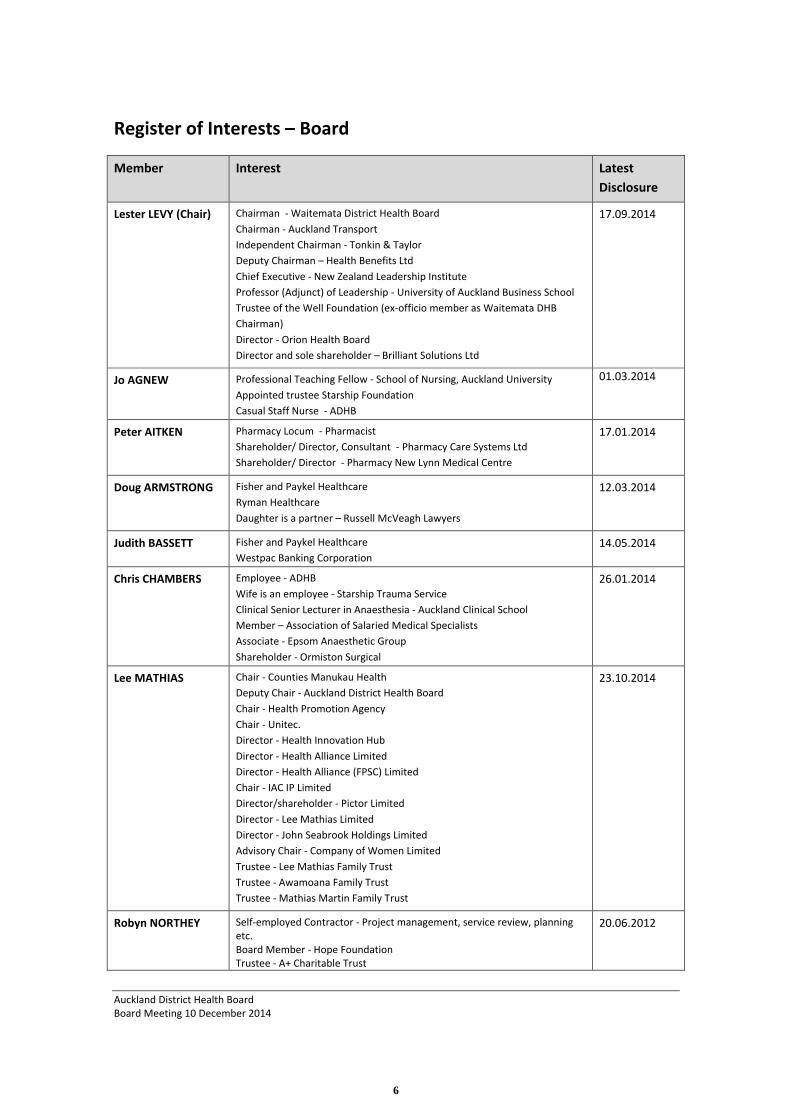
Register of Interests – Board
Member Interest Latest Disclosure
Lester LEVY (Chair) Chairman - Waitemata District Health BoardChairman - Auckland TransportIndependent Chairman - Tonkin & TaylorDeputy Chairman – Health Benefits LtdChief Executive - New Zealand Leadership InstituteProfessor (Adjunct) of Leadership - University of Auckland Business SchoolTrustee of the Well Foundation (ex-officio member as Waitemata DHB Chairman)Director - Orion Health BoardDirector and sole shareholder – Brilliant Solutions Ltd
17.09.2014
Jo AGNEW Professional Teaching Fellow - School of Nursing, Auckland UniversityAppointed trustee Starship FoundationCasual Staff Nurse - ADHB
01.03.2014
Peter AITKEN Pharmacy Locum - PharmacistShareholder/ Director, Consultant - Pharmacy Care Systems LtdShareholder/ Director - Pharmacy New Lynn Medical Centre
17.01.2014
Doug ARMSTRONG Fisher and Paykel HealthcareRyman HealthcareDaughter is a partner – Russell McVeagh Lawyers
12.03.2014
Judith BASSETT Fisher and Paykel HealthcareWestpac Banking Corporation
14.05.2014
Chris CHAMBERS Employee - ADHBWife is an employee - Starship Trauma ServiceClinical Senior Lecturer in Anaesthesia - Auckland Clinical SchoolMember – Association of Salaried Medical SpecialistsAssociate - Epsom Anaesthetic GroupShareholder - Ormiston Surgical
26.01.2014
Lee MATHIAS Chair - Counties Manukau Health Deputy Chair - Auckland District Health BoardChair - Health Promotion AgencyChair - Unitec.Director - Health Innovation Hub Director - Health Alliance LimitedDirector - Health Alliance (FPSC) LimitedChair - IAC IP LimitedDirector/shareholder - Pictor LimitedDirector - Lee Mathias LimitedDirector - John Seabrook Holdings LimitedAdvisory Chair - Company of Women LimitedTrustee - Lee Mathias Family TrustTrustee - Awamoana Family TrustTrustee - Mathias Martin Family Trust
23.10.2014
Robyn NORTHEY Self-employed Contractor - Project management, service review, planning etc.Board Member - Hope Foundation Trustee - A+ Charitable Trust
20.06.2012
6
Auckland District Health BoardBoard Meeting 10 December 2014
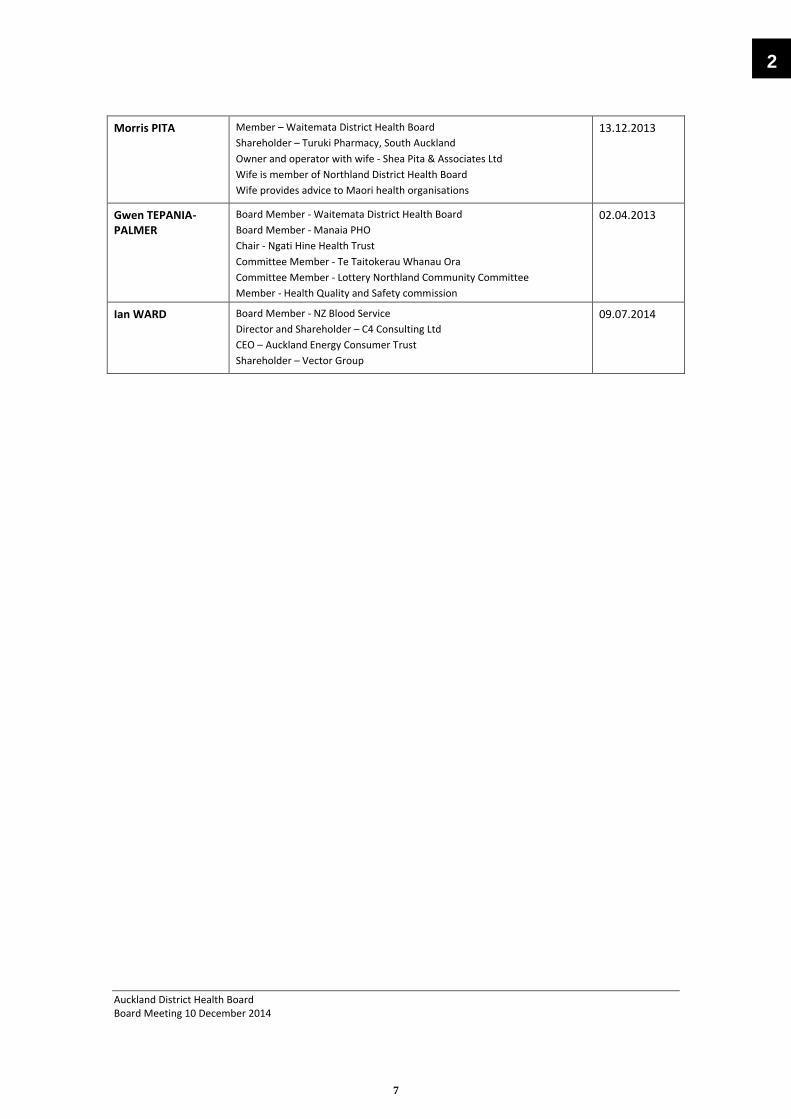
Morris PITA Member – Waitemata District Health BoardShareholder – Turuki Pharmacy, South AucklandOwner and operator with wife - Shea Pita & Associates LtdWife is member of Northland District Health BoardWife provides advice to Maori health organisations
13.12.2013
Gwen TEPANIA-PALMER
Board Member - Waitemata District Health BoardBoard Member - Manaia PHOChair - Ngati Hine Health TrustCommittee Member - Te Taitokerau Whanau OraCommittee Member - Lottery Northland Community CommitteeMember - Health Quality and Safety commission
02.04.2013
Ian WARD Board Member - NZ Blood ServiceDirector and Shareholder – C4 Consulting LtdCEO – Auckland Energy Consumer TrustShareholder – Vector Group
09.07.2014
2
7

Auckland District Health BoardMeeting of the Board 29/10/14 Page 1 of 9
MinutesMeeting of the Board
29 October 2014
Minutes of the Auckland District Health Board meeting held on Wednesday, 29 October 2014 in the A+ Trust Room, Clinical Education Centre, Level 5, Auckland City Hospital, Grafton commencing at 2:30pm
Auckland DHB Board Members PresentDr Lester Levy (Chair)Jo AgnewPeter AitkenDoug ArmstrongJudith BassettDr Chris ChambersDr Lee Mathias (Deputy Chair)Robyn NortheyMorris PitaGwen Tepania-PalmerIan Ward
Auckland DHB Management PresentAilsa Claire Chief Executive OfficerSimon Bowen Director of Health Outcomes – Auckland and
Waitemata District Health BoardsMargaret Dotchin Chief Nursing OfficerFionnagh Dougan Director Provider ServicesDr Debbie Holdsworth Director Funding – Auckland and Waitemata District
Health BoardsDr Andrew Old Chief Strategy, Participation and InnovationRosalie Percival Chief Financial OfficerVivienne Rawlings Chief Human Resources OfficerLinda Wakeling Chief of Intelligence and InformaticsSue Waters Chief Health Professions OfficerDr Margaret Wilsher Chief Medical Officer
Auckland DHB Senior Staff PresentJoanne Brown Funding & Development Manager - HospitalsJulie Helean Assistant Director StrategyAuxilia Nyangoni Deputy Chief Financial OfficerMarlene Skelton Corporate Business Manager
(Other staff members who attend for a particular item are named at the start of the minute for that item)
1 ATTENDANCE AND APOLOGIES
That the apology of Gilbert Wong, Director Communications be received.
2 CONFLICTS OF INTEREST
There were no declarations of conflicts of interest for any items on the open agenda.
Lee Mathias drew attention to the fact that her registered interests had been updated between meetings with the revised interests appearing in this agenda.
3 CONFIRMATION OF MINUTES 17 SEPTEMBER 2014 (Pages 8-14)
Resolution: Moved Peter Aitken/Seconded Judith Bassett
That the minutes of the Auckland District Health Board meeting held on 17 September 2014 be confirmed as a true and correct record.
Carried
3
8
Auckland District Health BoardMeeting of the Board 29/10/14 Page 2 of 9
4 ACTION POINTS 17 SEPTEMBER 2014 (Pages 8-14)
There was no comment with regard to action points from the meeting of 17 September 2014.
5 CHAIRMAN’S REPORT
Lester Levy advised that Board Chairs had met with the new Minister of Health, Dr Jonathan Coleman. He briefly relayed some key observations from that meeting:
∑ Some changes around the margins of targets had been indicated but nothing of significance. The path prescribed is still very much following that set by Tony Ryall.
∑ The new cancer target will attract more attention.
∑ There will be an increased focus on inter agency collaboration, children and the elderly. To support this increased focus Dr Jonathan Coleman had also been given the portfolio of Sport and Recreation. This coupled with the Health portfolio provides an avenue for tackling chronic disease and obesity.
∑ Lester Levy felt that it had been clearly signalled that if a Board was performing and delivering to the key targets it would be given the space to do more things. However, those that were underperforming would face more intense monitoring.
6 CHIEF EXECUTIVE’S REPORT (Pages 15-23)
The Chief Executive asked that her report be taken as read, highlighting that:
∑ There had been an increase in requests for information, interviews and access from news media and production organisations. The breadth in topics of interest had also expanded. Lester Levy commented that the Board had approved a charging policy for requests where time to gather the required data exceeded a set level and that perhaps management needed to apply that policy.
∑ On 16 September the specialist Mother and Baby Unit was officially opened at the Child and Family Unit of Starship Children’s Hospital.
∑ Applications have now closed for the Health Excellence Awards and the Annual Awards Event takes place on Wednesday 3 December 2014.
∑ Invitations have been sent out to staff who quality for Long Service Awards. This year two events will be held to recognise those with more than 30 years of consecutive employment, on 17 November.
∑ Auckland DHB staff are participating in the regional Feetbeat Challenge with 29 teams made up of more than 190 staff walking 30-minutes-a-day.
∑ Performance relating to meeting the national health targets in relation to the
9
Auckland District Health BoardMeeting of the Board 29/10/14 Page 3 of 9
emergency departments had slipped due to winter pressures.
∑ The power outage has exposed vulnerable relationships around emergency care within the community. It was evident that backup arrangements for generated power did not come to fruition for many residential facilities and there was confusion around the role of the PHO in such incidents. However the incident had been extremely well managed.
∑ Smoking prevalence for Māori pregnant mothers at time of booking to birth is significantly higher than other ethnicities in both Waitemata and Auckland District Health Boards. The Māori Health Gain Team is in the process of identifying strategies and activities to support Māori pregnant mothers to become and stay smoke-free.
∑ A Confirmation Ceremony (Ava Ceremony) for Bruce Levi the General ManagerPacific Health was held on 15 September 2014. It was a milestone event in the journey of District Health Board Pacific Health.
Matters covered in discussion of the report and in response to questions included:
∑ Lee Mathias noted that bed days saved were now being filled by growth indicating a new trend in higher patient numbers presenting and a higher level of acuity. The Board needed to keep this in mind when considering savings made as it was easy to lose sight of the gains made along the way. Without those gains the position could be much more severe.
That the report be received.
7 LIFT THE HEALTH OF PEOPLE IN AUCKLAND CITY - COMMUNITY ANB PUBLIC HEALTHADVISORY COMMITTEE RECOMMENDATIONS
There were no recommendations to consider.
8 LIVE WITHIN OUR MEANS
8.1 Eastern Bays Hospice Update (Pages 24-26)
Debbie Holdsworth, Director Funding advised that Palliative Care Services were discussed at the Community and Public Health Advisory Committee on 30 April 2014. As Eastern Bays Hospice is not funded by the District Health Board, the item did not include any information on this hospice. As a result the following action arose from that meeting; “Palliative Care –information relating to Eastern Bays Hospice to be obtained and reported to Auckland DHB”.
This paper provides information on the services offered by Eastern Bays Hospice, a charity that provides services for any metro Auckland person able to access their service.
Eastern Bay Hospice provides a range of non-specialist services to people with palliative care needs. People access these services as they need them. Care is planned in relation to individual need. The hospice has a good working relationship with the specialist palliative
3
10
Auckland District Health BoardMeeting of the Board 29/10/14 Page 4 of 9
care service to ensure people get the care they need at the time that it is needed.
Eastern Bays Hospice fund their service through charity shops and fundraising. This is consistent with how the other hospices in metro Auckland fund non-specialist services.
Subsequent to this action, the Community and Public Health Advisory Committee haverequested a broader review of hospice funding with a focus on their sustainability. This will be brought to both Auckland and Waitemata District Health Boards in due course.
That the report be received
8.2 Values for Auckland DHB: Progress Update (Pages 27-32)
Dr Andrew Old Chief Strategy, Participation and Innovation and Julie Helean, Assistant Director Strategy spoke to the report advising that:
∑ The Values Project is well underway with work on track to produce a set of organisational values by December 2014.
∑ The main data gathering exercise was successfully completed in July and August with workshops being run during the “At Our Best Week”.
∑ The “At Our Best Week” engagement generated over 400 pages of free-text responses describing the positive and negative experiences associated with Auckland DHB. This has been collated into word pictures by facilitator, Tim Keogh, some of which are attached as pictorial examples of the staff findings.
Matters covered in discussion of the report and in response to questions included:
∑ Lester Levy noting that the desire to be “appreciated” is endemic of all organisations.
∑ Ian Ward asking if there had been any surprises for management when collating the feedback and being advised that while good information had existed in regard to what was valued by Maori and Pacific patients this did not extend to the Asian population. The Asian patient experience to services is very different as they valuedifferent things.
∑ Ailsa Claire advised that management was looking at how best to engage with the Asian community but that strategies that worked for the Maori and Pacific communities would not necessarily be ones that appealed to or were valued by the Asian community. Andrew Old advised that this was just the beginning of a very long piece of work and that the next steps were to refine what the values and behaviours would look like and then how to make these real for the organisation.
∑ Morris Pita noted that there were some very good examples of organisational values statements in existence and how these were arrived at should be investigated. Hesuggested that Fisher and Pykel had a values statement that was particularly well
11
Auckland District Health BoardMeeting of the Board 29/10/14 Page 5 of 9
constructed and worthy of note.
That the Board note the Values Project is progressing with options for a set of values being drafted.
9 GENERAL BUSINESS
There was none.
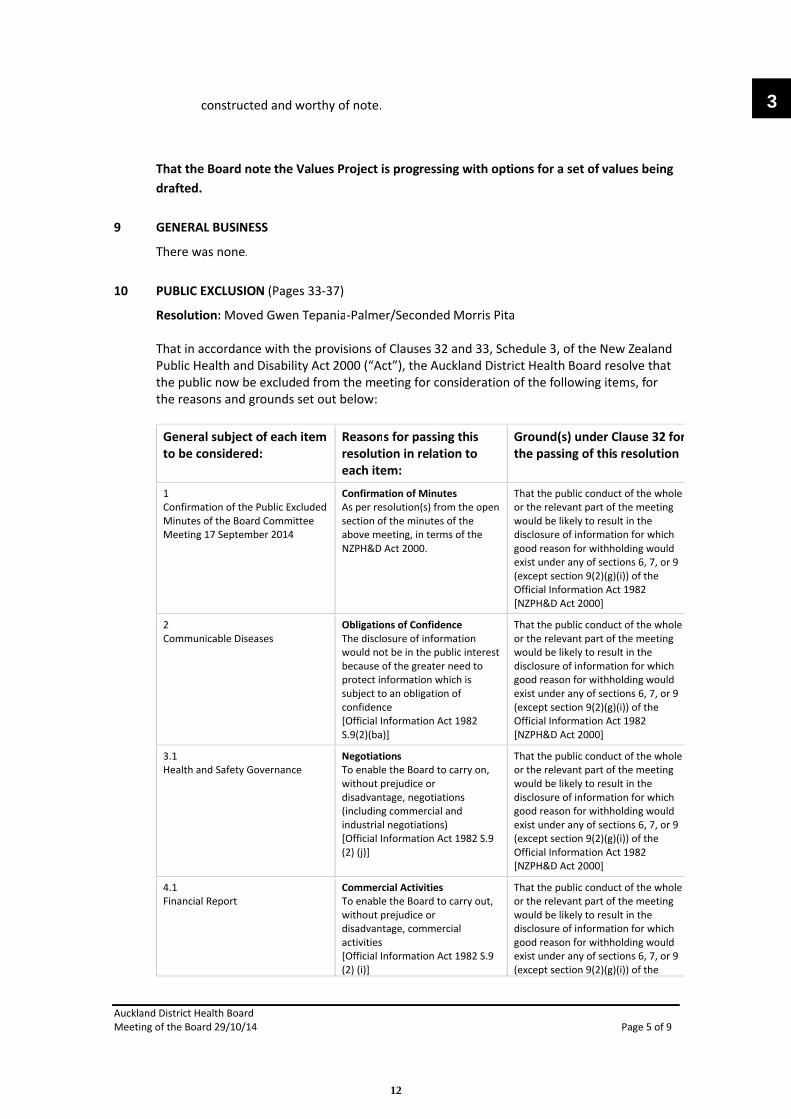
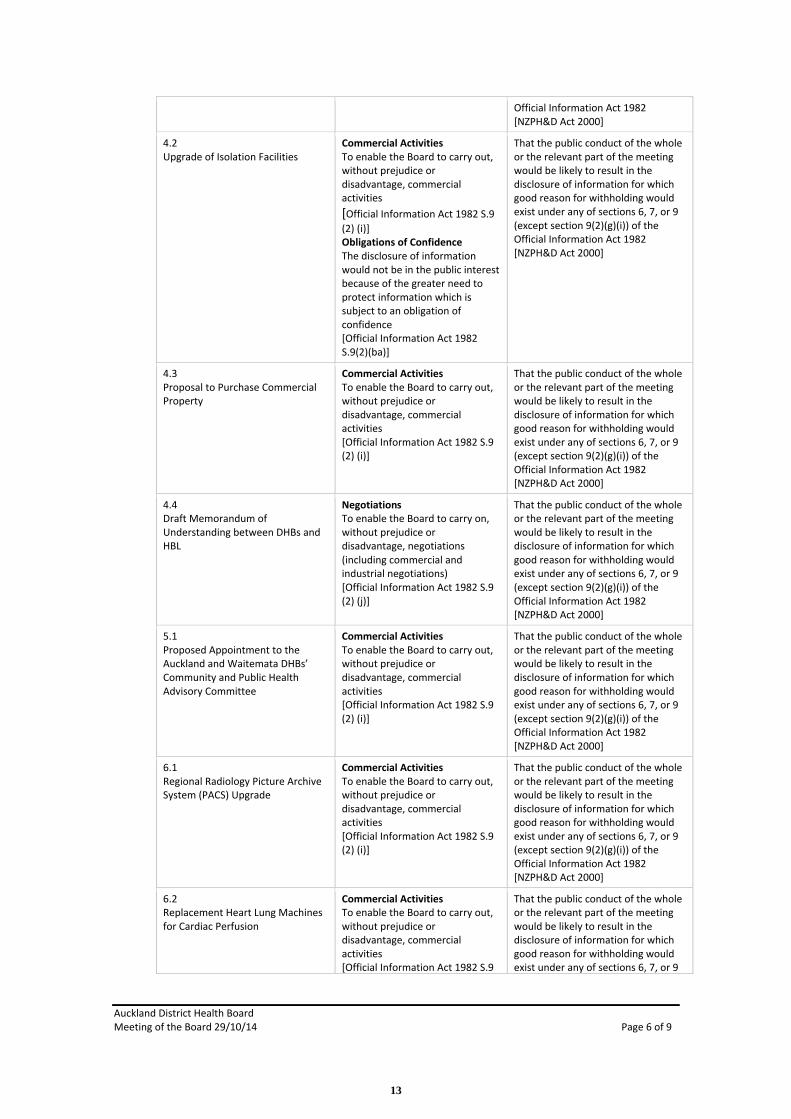
10 PUBLIC EXCLUSION (Pages 33-37)
Resolution: Moved Gwen Tepania-Palmer/Seconded Morris Pita
That in accordance with the provisions of Clauses 32 and 33, Schedule 3, of the New Zealand Public Health and Disability Act 2000 (“Act”), the Auckland District Health Board resolve that the public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below:
General subject of each itemto be considered:
Reasons for passing this resolution in relation to each item:
Ground(s) under Clause 32 for the passing of this resolution
1Confirmation of the Public Excluded Minutes of the Board Committee Meeting 17 September 2014
Confirmation of MinutesAs per resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
2Communicable Diseases
Obligations of ConfidenceThe disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 S.9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
3.1Health and Safety Governance
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4.1Financial Report
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the
3
12
Auckland District Health BoardMeeting of the Board 29/10/14 Page 6 of 9
Official Information Act 1982 [NZPH&D Act 2000]
4.2Upgrade of Isolation Facilities
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]Obligations of ConfidenceThe disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 S.9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4.3Proposal to Purchase Commercial Property
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4.4Draft Memorandum of Understanding between DHBs and HBL
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
5.1Proposed Appointment to the Auckland and Waitemata DHBs’ Community and Public Health Advisory Committee
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.1Regional Radiology Picture Archive System (PACS) Upgrade
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.2Replacement Heart Lung Machines for Cardiac Perfusion
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9
13
Auckland District Health BoardMeeting of the Board 29/10/14 Page 7 of 9
(2) (i)] (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
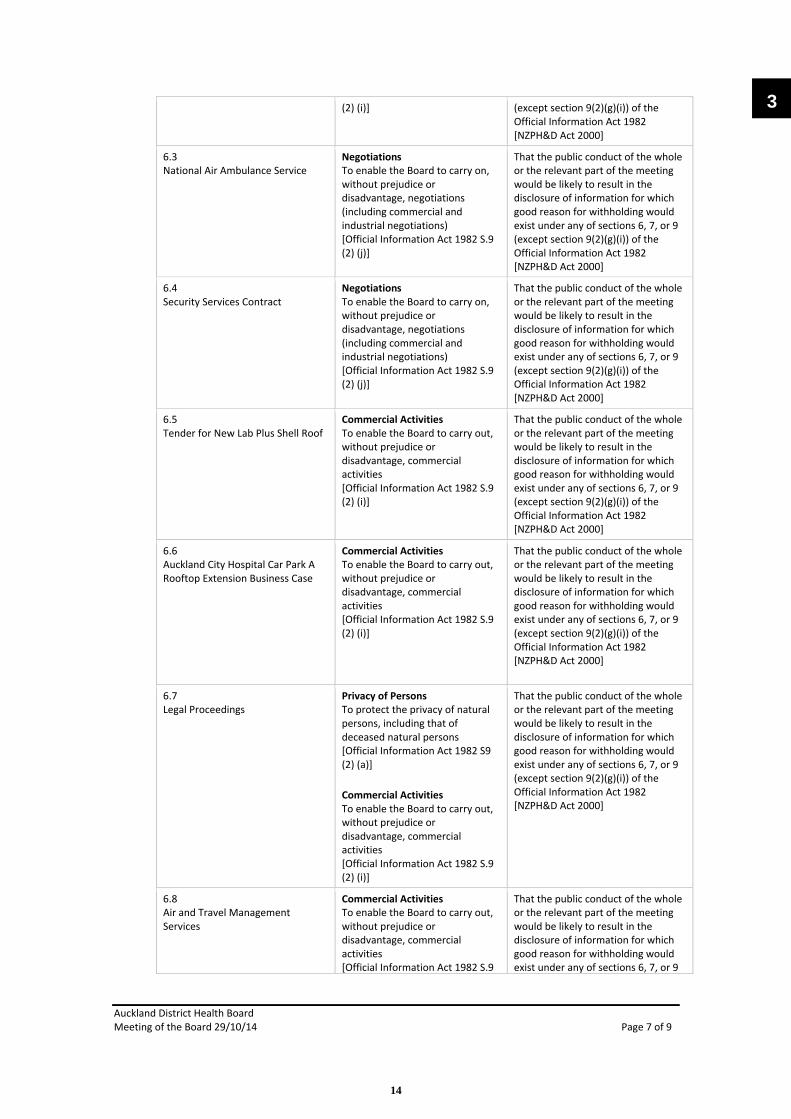
6.3National Air Ambulance Service
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.4Security Services Contract
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.5Tender for New Lab Plus Shell Roof
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.6Auckland City Hospital Car Park A Rooftop Extension Business Case
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.7Legal Proceedings
Privacy of PersonsTo protect the privacy of natural persons, including that of deceased natural persons[Official Information Act 1982 S9 (2) (a)]
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.8Air and Travel Management Services
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9
3
14
Auckland District Health BoardMeeting of the Board 29/10/14 Page 8 of 9
(2) (i)] (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
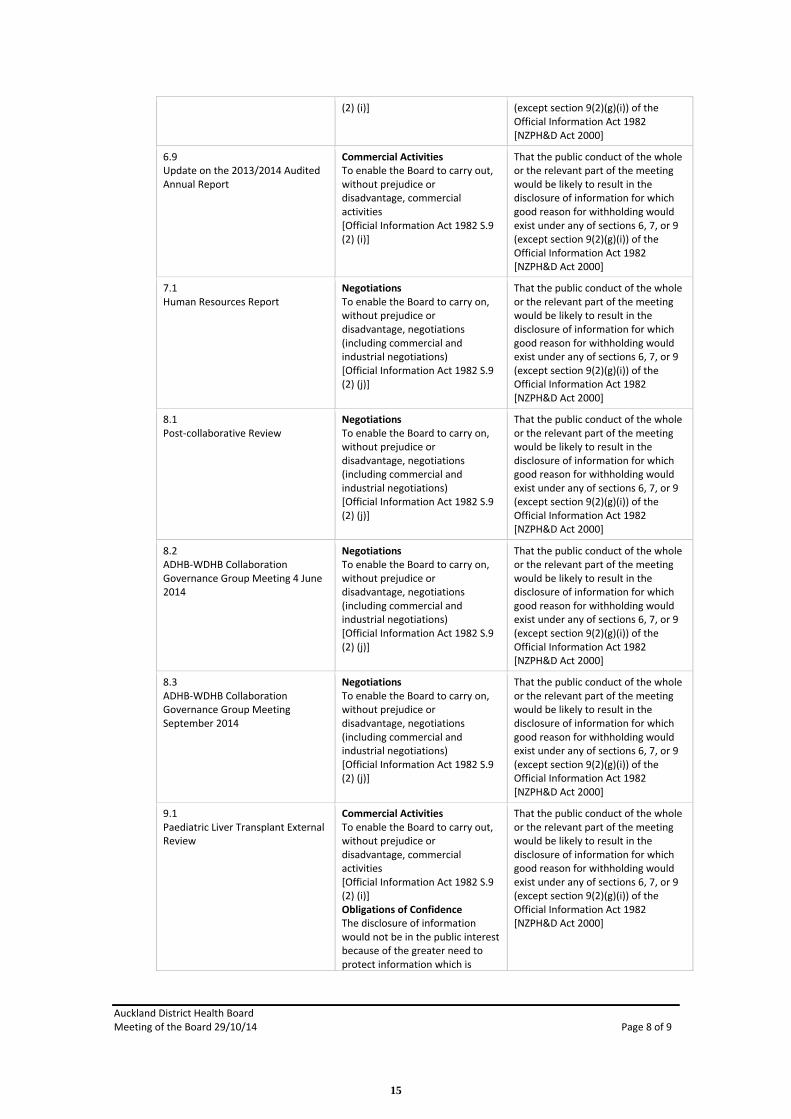
6.9Update on the 2013/2014 Audited Annual Report
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
7.1Human Resources Report
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
8.1Post-collaborative Review
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
8.2ADHB-WDHB Collaboration Governance Group Meeting 4 June 2014
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
8.3ADHB-WDHB Collaboration Governance Group Meeting September 2014
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
9.1Paediatric Liver Transplant External Review
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]Obligations of ConfidenceThe disclosure of information would not be in the public interest because of the greater need to protect information which is
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
15

Auckland District Health BoardMeeting of the Board 29/10/14 Page 9 of 9
subject to an obligation of confidence [Official Information Act 1982 S.9(2)(ba)]
9.2Community Laboratory Services Transition Update
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
9.3Regional Wicked Project (formerly Northern Region PAS Project) Status Update
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
Carried
The meeting closed at 4.45pm.
Next MeetingThe next ordinary scheduled meeting will be held:2:00pm, Wednesday, 10 December 2014A+ Trust Room, Clinical Education Centre, Level 5, Auckland City Hospital, Grafton
Signed as a true and correct record of the Auckland District Health Board meeting held on Wednesday, 29 October 2014.
_____________________________________________ Chair ___________________________ Date
3
16

Auckland District Health BoardMeeting of the Board 10/12/2014Page 1
Chief Executive’s Report
Recommendation
That the report is received.
Prepared by: Ailsa Claire (Chief Executive)
Glossary
AWHI = Auckland-wide healthy Housing InitiativeCVD = Cardiovascular DiseasePBP = Pacific Best PracticePHO = Primary Health Organisation SSC = Surgical Safety ChecklistTamariki Maori = Maori childrenTautai Fakataha = Pacific Health Team
1. Introduction
This report covers the period from 11 October to 25 November. It includes an update on the management of the wider health system and is a summary of progress against the Board’s priorities to confirm that matters are being appropriately addressed.
2.1 Public information released for the media
Auckland DHB made public statements or facilitated media coverage about:
∑ Auckland DHB’s Department of Forensic Pathology∑ Maternity services being once again accredited as Baby Friendly∑ The ‘Falls Concept Ward’∑ The finalists in the five categories of its Health Excellence Awards 2014∑ Auckland-region DHBs consulting staff on a food services proposal∑ Reducing harm from high-risk medicines∑ AUT students making a difference for kids in Starship Hospital
We received 89 requests for information, interviews or for access from news media and production organisations in the period from 10 October to 25 November. Media enquiries included interest in:
∑ Advance Care Planning∑ Filming paediatric endocrinologist Professor Alistair Gunn for the Royal Society∑ Demand for bariatric beds∑ Wards designated for Ebola treatment∑ The DHB’s Forensic Pathology service∑ HPV and its epidemiology∑ Legionella∑ The food services business case in the light of news about HBL
7
17
Auckland District Health BoardMeeting of the Board 10/12/2014Page 2
Apart from those noted, the remaining enquiries over the period were routine requests about the status of patients hospitalised following crimes or accidents or who were of interest because of their public profile.
Of the 12 Official Information Act requests reviewed in this period, seven were from media organisations.
2.2 Social Media ActivityOur social media audiences at the end of the period were:
∑ Facebook – 2497∑ Twitter – 1275∑ LinkedIn – 2688
The most popular items of content last month were:∑ White Ribbon Day∑ Health Excellence Award winners∑ High-fives – patient stories∑ International Anaesthesia Day
2.3 Events, internal communications and people
Events
Health Excellence AwardsThe finalists for the Health Excellence Awards were announced in October. The winners will be celebrated at the Annual Awards Event which takes place on Wednesday 3 December 2014 at the Auckland War Memorial Museum. This year we increased the number of applications from primary and community care providers by including a category of Community Health and Wellbeing.
Ka Pai WhanauThe traditional clinical staff engagement model of Celebration Week has been broadened to encompass more evenly spread events over December that include both and staff and stakeholder engagement throughout the month. This is dubbed Ka Pai Whānau to convey the core element of thank you to staff for their efforts in the calendar year.
Help Our Kids fundraisingThe Starship Foundation fundraising partnership with the New Zealand Herald has concluded. It delivered $207,000 for the upgrade of Starship’s operating theatres and surgical facilities.
Long serviceTwo Long Service ceremonies Awards were held on 17 November to recognise staff who achieved 30 and 40 years’ service. About 150 staff attended with their family, friends and colleagues. The feedback from attendees was very positive and further long service events will be held in the New Year.
Quality Grand RoundsTwo Quality Grand Rounds took place. The themes were:
o Unlocking the Joy - Learnings from the 2014 Asia Pacific Healthcare Forum. o Rapid Improvement Events – ‘five days from problem identification to implemented
solution’.
18
Auckland District Health BoardMeeting of the Board 10/12/2014Page 3
Health Outcomes Grand Round – is it worth the struggle?Professor Doug Selman, Director of the National Addiction Centre spoke at the second in a series of Health Outcomes Grand Rounds. Professor Selman talked about the health and social cost of alcohol misuse and alcohol reform legislation.
Bike-to-work BreakfastAuckland Transport and Auckland DHB hosted a bike-to-work breakfast to celebrate the opening of the new storage facilities for bicycles. Cyclists were able to take advantage of a free bike-check anda light breakfast. The new bicycle facilities provide 50 secure, covered, spaces for bikes.
White Ribbon DayA social media campaign took place in the run-up to White Ribbon Day on 25 November. Staff from around the organisation had their photos taken holding up messages supporting an end to domestic violence. On 25 November White Ribbons were handed out at Auckland City Hospital and Greenlane Clinical Centre.
Organ Awareness Day - 11 OctoberOrgan Donation New Zealand ran an information booth at Auckland City Hospital in the week leading up to this awareness day. CMO Margaret Wilsher featured in a 10 October effort to help highlight the campaign and the display via social media. DHB internal and external communications have shared links to their campaign information.
International Anaesthesia Day – 16 OctoberOur DHB anaesthetists ran a display on level 5 at Auckland City Hospital to promote the profession and connect to the national campaign with the same aim.
Internal communications∑ Blog posts were published by the CE on our Long Service initiative, the Health Excellence
Awards, alcohol reform, parking and food services. In addition, Chief Financial Officer Rosalie Percival, as acting CE, posted on security.
∑ One team talk blog was posted by Director of Communications, Gilbert Wong.∑ 21 news updates were published on the DHB intranet.∑ Eight eNova (weekly electronic newsletters) were published.∑ Staff were invited to have their say on the Food Services proposal.∑ An edition of Nova magazine was published.
People
Local HeroesThirty eight people were nominated as ‘Local Heroes’ during October and November. Local hero awards were presented to Sue Patience and Kieran Barling. Their nominators told us:
“Sue, a staff nurse in the Haemodialysis Unit was nominated by a patient, who told us, “There are so many wonderful things that I can describe about Sue. She is so amazing, so caring, loving and giving of herself. She is very accurate and there are no shortcuts when doing her job. When I first started at the Home Haemodialysis Unit, Sue taught me the machine, helped me with the troubleshooting and I nearly always got her on the 24hr helpline we have. I love her; she has made my life worth living.”
“Kieran, a staff nurse was nominated by a patient who told us, “Kieran was a wonderful nurse to my Dad, while he was a patient in Remuera Ward in August and September. Dad really liked Kieran and we all greatly appreciated the high standard of nursing that he provided. He was always patient,
7
19
Auckland District Health BoardMeeting of the Board 10/12/2014Page 4
kind and an outstanding listener. Always attentive and aware of Dad's needs, he made the time that Dad was in his care, much better.”
Dr Jared NoelTributes were paid to Dr Jared Noel, a doctor at Auckland City Hospital who passed away in October.
Leigh AndersonLeigh Anderson of the Auckland DHB Performance Improvement team has been presented with the 2014 Perioperative Nurses College NZNO Christina (Tina) Ackland Award for Outstanding Services to the Perioperative Community.
Professor Ed GaneThe Auckland City Hospital hepatologist and liver transplant specialist Professor Edward Gane received the Health Research Council of New Zealand’s Liley Medal at a Research Honours Dinner on 26 November for demonstrating a safer, more effective treatment for people with hepatitis C virus.The medal recognises Professor Gane’s outstanding contribution to the health and medical sciences in the field of clinical hepatology. Professor Gane was the lead author on two very highly cited papers in the New England Journal of Medicine, which showed that people could be cured of the hepatitis C virus in 12 weeks using an antiviral treatment called sofosbuvir.
Professor Alistair GunnStarship Children’s Hospital paediatric endocrinologist and Auckland University Faculty of Medical and Health Sciences Professor Alistair Gunn was also honoured on the same date as Professor Gane.The Royal Society of New Zealand presented Alistair with the MacDiarmid Medal for outstanding scientific research which demonstrates potential for human benefit. The committee making the award said Professor Gunn had made a “major contribution to perinatal physiology and neuroscience.” Professor Gunn was made a Fellow of the Royal Society in 2009.
Kim BrackleyAuckland DHB Principal Pharmacist, Education & Training, Kim Brackley, is the new president of the New Zealand Hospital Pharmacists Association. This professional advocacy organisation represents 80 per cent of the country’s hospital pharmacists and works to promote hospital pharmacy and encourage collaboration within the sector.
Christine EtheringtonChristine Etherington has been appointed on a one year contract as the Director of Strategic Human Resources for Auckland District Health Board. Christine has most recently served as the General Manager, Human Resources for the Ministry of Social Development. During her time there she and her team’s work was recognised with a number of awards, including the Institute of Public Administration of New Zealand Award for improving performance for Transitions - a leadership development programme.
3. Collaboration – Auckland and Waitemata DHBs
Tertiary Services ReviewA review of tertiary services, led by the joint funder is now underway. A systematic methodology has been agreed in addition to a prioritised list of services, starting with paediatric services.
20
Auckland District Health BoardMeeting of the Board 10/12/2014Page 5
The expected outputs are speciality-specific service specifications which will provide both clinical services and funders with:
∑ clarity of referral∑ eligibility criteria∑ admission and discharge processes∑ volumes and scope of services to be provided.
It will also include analysis for the agreed list of services that considers:
∑ clinical need and nationwide access∑ cost and contribution∑ workforce and clinical sustainability
The Funder is currently working with Information Management’s Business Intelligence team to complete the financial analysis. Meetings have been set up with the respective services where this information will be presented and inform the subsequent process.
The provisional timeline for the completion of this work is August 2015. Additional resource has been contracted to undertake this work and the timeline will be reviewed early in the New Year to see if this can be brought forward.
4. Strategy, Participation and Improvement
Strategy and ValuesThe end is in sight with our organisation’s Strategy and Values development work. Particular challenges have been accurately reflecting both the commissioner and the provider parts of the organisation in the strategy, and finding the right words to connect with the themes we heard through the values work. A final draft is included in the Board papers.
This month sees the formal launch of our Design for Health & Wellbeing Lab (DHWLab) collaboration with Auckland University of Technology. This year has been about establishing and testing the relationship and processes and the results already are impressive. As part of our Ka Pai Whānau celebration month we have the DHWLab setup as an exhibition and I encourage Board members to make the time to visit and see first-hand the good work that is being done. The DHWLab is in the Clinical Education Centre at Auckland City Hospital, Level five.
DHB WebsiteAuckland DHB has gone to market to seek proposals for a refreshed Auckland DHB website that is patient and visitor focussed. The DHB has signed an agreement with the Department of Internal Affairs and Silverstripe to use the public sector common web platform. This enables efficiencies of scale and sharing of experience and knowledge with a range of public sector organisations.
The refreshed website will incorporate a dynamic, intelligent knowledge base. The application is in use already by Auckland Council, the University of Auckland and the Ministry of Social Development. The dynamic knowledge base will enable visitors to the website to pose questions and receive responses. Through regular analytics, it will allow the DHB to know if it is providing the information its patients and visitors need and want. The dynamic knowledge base will also be able to be accessed on the Auckland DHB Facebook platform to further enhance engagement.
7
21

Auckland District Health BoardMeeting of the Board 10/12/2014Page 6
Video WallWith Intelligence and Informatics, the DHB will also be trialling a video wall in the DHW Lab space for later use in the main reception area. Communications is working with the provider on developing a networked content management system and establishing sources of health-related video content.
4. Performance of the Wider Health System
4.1 National Health Targets Performance Summary
Status Comment
Acute patient flow (ED 6 hr) Oct 93%, Target 95%
Improved access to elective surgery 99% to plan for the year
Shorter waits for radiation therapy & chemotherapy
Oct 100%, Target 100%, Year to Date 100%
Better help for smokers to quit Oct 97%, Target 95%
Cardiac bypass surgery Oct 71 patients, Target < 104
More heart & diabetes checks Sep Qtr 90%, Target 90%
Increased immunisation 8 months Sep Qtr 95%, Target 95%
Key: Proceeding to plan Issues being addressed
Target unlikely to be met
More Heart and Diabetes Checks Health Target Q1 2014/15
Target: 90 per cent of the eligible adult population will have had their cardiovascular disease (CVD) risk assessed in the last five years by July 2015.
The More Heart and Diabetes Checks results are monitored against the Primary Health Organisation (PHO) Integrated Performance Incentive Framework and are reported in the Ministry of Health DHB performance tables.
At the end of October 2014, 90 per cent of the population was estimated to have been CVD-risk assessed. The result was based on the weekly reports provided by the PHOs. The Maori CVD risk assessment rate has remained relatively static at 87.0 per cent for Q1 of 2014-15, while the Pacific population’s CVD risk assessment rate remained constant at 90 per cent.
There has been an increase in demand for assessments which has been met by:
∑ practice support to run outreach clinics∑ providing funding for phlebotomy and extra nurse resource∑ purchasing a Point of Care testing machine to collect blood results ∑ tools to identify patients who have not had a risk assessment∑ weekly target meetings at the PHO and practice level∑ virtual assessments through Patient Management Systems and Dr Info queries∑ text-to-remind and home visits to complete assessments.
22
Auckland District Health BoardMeeting of the Board 10/12/2014Page 7
The Planning, Funding and Outcomes team continues to meet with the PHOs on a monthly basis to discuss coverage and activities undertaken to maintain the 90 per cent target. Recent meetings have focused on increasing coverage for Maori and Pacific people.
The Ministry of Health have confirmed the bonus funding available to the PHOs who achieved the 2013-14 target of 90 per cent. This funding will be available to all four PHOs in the Auckland DHB area from 30 November 2014.
Better Help for Smokers to Quit – Primary Care Health Target Q1 2014/15
Target: 90 per cent of enrolled patients who smoke and are seen by a health practitioner in primary care are offered advice and help to quit by July 2015.
The Better Help for Smokers to Quit results are also monitored against the PHO Integrated Performance Incentive Framework and are reported in the Ministry of Health’s DHB performance tables. While the Quarter One result was 96 per cent, the estimated result up to the end of Octoberwas 90 per cent. The PHOs are doing well in building sustainability into their systems and maintaining their performance but the performance has dropped as the number of people needing advice jumps at the beginning of each quarter. We expect to see the performance climb again as the quarter progresses.
A series of workshops with stakeholders have been held to review and revise existing strategies and to develop new strategies reduce the number of smokers.
4.2 Clinical Governance Commentary
GP Open DayThe first GP open day was held on Monday 10th August with over 60 GPs visiting the adult emergency department and APU. The GPs were able to meet informally with various members of the Senior Leadership Team and, following presentations on acute winter load and elective surgical throughput, had an opportunity to discuss matters of concern. There was a high degree of engagement and much positive feedback about the opportunity to come into the hospital and meet directly with executives and senior clinical leaders. On the basis of that feedback, we are planning to hold further open days with thematic content e.g. children’s health, older peoples’ health and cardiac.
Minister’s VisitThe Minister of Health, the Hon Dr Jonathan Coleman visited Auckland City Hospital in October and met with senior clinical leaders. He also toured the radiation oncology service, stopping at the National Anaesthesia Day display on level 5, and on into the Starship Children’s hospital operating rooms. He indicated his interest in clinical leadership, children's health (including vulnerable children), obesity and mental health. This was a positive meeting and one that was well received by all participants.
Research WeekPlanning is underway for the annual research week - to be held this year 24-28 November. In recognition of the Auckland Academic Health Alliance, the Young Investigator Award presentations were held at the Faculty of Medicine and Health Sciences 4 December, when an announcement about a significant joint research fund was made.
7
23
Auckland District Health BoardMeeting of the Board 10/12/2014Page 8
Dr Richard SullivanAfter a comprehensive recruitment and selection process Dr Richard Sullivan has been appointed Deputy CMO and will assume some portfolio responsibilities and provide on-going cover and support to the CMO.
Dr Sullivan is also the Director for Cancer and Blood; the Director of the Northern Cancer Network, the Joint Clinical Lead for National Medical Oncology Models of Care; Chair of Adolescence and Young Adult (AYA) Network governance group and a member Cancer Control New Zealand.
Quality and Safety MarkersQuality and Safety Markers for the July - September quarter were submitted to the Health Quality and Safety Commission in the week of 14 November. In Falls Risk Assessment we had 92 per centcompliance and in Falls Care Plans a 95 per cent compliance. Both of these are above the 90 per centtarget and similar to the previous quarter. The hand hygiene audit found compliance with 76 per cent of ‘moments’, which was the same as the previous quarter and above the >70 per cent national target. The Surgical Safety Checklist (SSC) audit found documentation of use of all three components of the checklist in 85 per cent (95% confidence interval 80–92%) of operating room procedures. This remains below the target of > 90 per cent, but the weakest element (documentation of “Sign out”) has improved from the 72 per cent reported in the previous quarter. We will shortly switch to being a pilot site for a new SSC measure using direct observation of both compliance and engagement, a much more real-life and relevant assessment. Central line associated bacteraemia (CLAB) remains a well-performing area with only one case in the quarter and a rate of 0.36 per 1000 catheter days.
4.3 Financial Performance
For October 2014, we recorded a year-to-date net deficit of $(0.8)m, which is on budget. Year-to-date income and expenditure is on budget. However, there are favorable line variances in clinical supply and funder provider payment lines offset by unfavorable variances in outsourced personnel and infrastructure cost lines. Our savings program is on track to achieve an overall target of $49.6m with YTD savings to September of $11.6m versus a budget of $11.5m, supporting our year-end breakeven target.
4.4 Primary Care and Community Services
The Alliance Leadership Team (ALT) continues to meet regularly and has:∑ met with Te Pou Matakana, the Māori Whanau Ora commissioning agency, to discuss
opportunities for collaboration∑ agreed to the continual development and funding of clinical pathways. They have also asked
for an evaluation of this programme in terms of both uptake and effectiveness∑ approved the intervention logic model for diabetes.
Consultation on a rural alliance has concluded with agreement that the scope will include:1. Provision of a ‘rural lens’ on DHB service development. This means that the DHB will
engage with the Rural Alliance Leadership Team on proposed service delivery change to obtain a rural perspective on:
a. potential positive and negative impacts on rural communitiesb. possible mechanisms to mitigate any negative impactsc. and to identify opportunities for improved service delivery to rural communities.
24
Auckland District Health BoardMeeting of the Board 10/12/2014Page 9
2. Overseeing a programme of work to provide advice to the DHBs on opportunities to improve health care services in rural communities. This includes opportunities to improve general practice capability and capacity to provide an expanded range of services to better meet the health needs of their local populations with an aim of reducing unnecessary travel for patients to DHB facilities.
3. Oversee and provide direction in an advisory capacity for the review of Waiheke Island health services, including endorsement of advice to the Auckland Waitemata Alliance and/or to the board of Auckland District Health Board.
4. Oversee and provide direction in an advisory capacity regarding any rural health workforce development and planning activity.
5. Oversee and provide direction in an advisory capacity for any agreed work programmes with a focus on health care for rural communities.
The Rural Alliance will start meeting in 2015.
After-HoursWe have begun development of the quality framework for the after-hours services and this will be ready in time for inclusion in the procurement process to be started early in 2015.
4.5 Māori Health
Ethnicity Data Audit ToolImplementation of the Ethnicity Data Audit Tool (EDAT) Project is progressing well. The training package for West Coast DHB has been delivered with negotiations underway for delivery of training for Bay of Plenty and Counties Manukau District Health Boards. The target is to have 95 per cent of general practitioner practices implement EDAT by June 2015. Currently 25 per cent of practices have implemented EDAT.
Māori Health PlanThe process for developing the 2015/16 Māori Health Plan is underway. The development of activities to achieve national targets will include robust engagement with Memorandum of Understanding partners, Māori Providers, PHOs and internal parties. The plan will also look to support improvements in Māori health gain for up to three locally identified priority areas.
YouthImproving the health of tamariki Māori is a local priority in the 2014/15 Māori Health Plan. Analysis of indicators about access to sexual health, oral health and primary healthcare services has been conducted and revealed significant inequalities for tamariki Māori. Focus groups with tamariki Māori will be conducted to identify enablers to accessing health services. Given the diverse needs of thisgroup we will seek input from tamariki Māori who are:
∑ attending school∑ not attending school or training and not employed∑ not attending school and are employed.
We will also include rural and urban perspectives. This information will be used to identify strategies and activities to improve access and tamariki Māori heath gain.
7
25
Auckland District Health BoardMeeting of the Board 10/12/2014Page 10
4.6 Pacific health report
Tautai Fakataha Pacific Navigation team
Pacific Best Practice sessions Auckland DHBWe delivered Pacific Best Practice sessions in a Cardiovascular Directorate study day on 28 Oct. A proposal for Pacific Best Practice/Pacific Cultural Competency Training is being developed by the Regional Pacific Projects Team
Regional Pacific Health Science AcademiesThese are set to start in the 2015 academic year, with student recruitment and selection completed in Onehunga High and Waitakere College. Contracts will be signed off once proposed budgets finalised. Mangere College will leave the from Health Science Academy programme as their model of did not fit with the Regional Pacific Health Science Academies programme.
Regional Tertiary Mentoring ProgrammeWork continues in setting up infrastructure for the Mentor Me programme and an event was held 16 Oct at the AUT City Campus which was attended by more than 40 students and 8 mentors. They metHilda Fa’asalele, Chief Advisor and undergraduate medical student, Saleimoa Bill Sami.
Tautai Fakataha - Pacific support services
Social Support and Cultural AssessmentsSocial Support and Cultural Assessments make up the largest s ingle categories of referral to the service.
OutreachOutreach by the team included short presentations to Family Violence and Children Young Person Services training held every month. The team continues to follow up on Did Not Attend families in Cancer and Blood Services and in the Cardiac Rehabilitation Service.
The Auckland-wide healthy Housing Initiative is receiving Tautai Fakataha support and in turning taking referrals. Project lead Nicky Cranshaw provides AWHI training sessions every two-threemonths for new staff and others who would like refresher training.
ReferralsTautai Fakataha are receiving referrals from the Bariatric and Hepatobiliary Clinic regarding patients not attending and are supporting patients by organising transport and advocating on their behalf. This is both during clinic appointments and supporting in their keeping up with follow-up appointments. We note that the need for language support remains high, especially for Niue and Tuvalu patients
Matua (elder) Advisory Council at Auckland DHBDevelopment of a Pacific elders advisory body at Auckland DHB is underway, utilising the mental health matua advisory council at Waitemata DHB. This will strengthen the pacific cultural leadership in the DHB and will be made up of senior, matua and Pacific leaders from their organisations. This will be launched next year.
26
OPEN
Auckland District Health BoardMeeting of the Board 6 August 2014
The Auckland Plan – Working with Auckland Council to Create the World’s Most Liveable City
Recommendation
Resolution
That the Board:
(a) Formally endorse the Auckland Plan.
(b) Provide support and encouragement to working very closely with the Auckland Council on issues going forward and developing relationships at all levels of the organisations from governance to the operational level.
Carried
Prepared by: Paul Garbett (Board Secretary, Waitemata DHB)
Glossary
1. BackgroundThis was discussed by the Community and Public Health Advisory Committee at their meeting on 26 November 2014, open item at page 7 and is recommended to the Board.
8.1
27

28
8.1
29

30
8.1
31
32
8.1
33
34
8.1
35
36
8.1
37
38
8.1
39
40

8.1
41
42
8.1
43

OPEN
Auckland District Health BoardMeeting of the Board 6 August 2014
2015/2016 Annual Plan Approach
Recommendation
Resolution
That the Board:
(a) Approve the approach to annual planning for 2015/16, including the longer term direction and timetable.
(b) Note the national planning guidance, including updates and changes.
Carried
Prepared by: Paul Garbett (Board Secretary, Waitemata DHB)
Glossary
1. BackgroundThis was discussed by the Community and Public Health Advisory Committee at their meeting on 26 November 2014, open item 3.1, page 35 and is recommended to the Board.
8.2
44
45
8.2
46
47
8.2
48
49

8.2
50

OPEN
Auckland District Health BoardBoard Meeting – 10 December 2014Page 1
Te Toka Tumai - a Strategy for Auckland DHB to 2018
Recommendation
That the Board:
Approve the final draft Strategy for Auckland DHB for stakeholder consultation
Prepared by: Julie Helean, Assistant Director StrategyApproved/Endorsed by: Dr Andrew Old, Chief of Strategy, Participation and Improvement
Ailsa Claire, Chief Executive
Attachments: The final draft of the Strategy for Auckland DHB
1. Executive SummaryThis paper updates the Board on the overall Strategy for Auckland DHB. Some of the early work done on the strategy has been revised. In early versions, a settings-based approach dominated and within this, the need for the DHB to be more active in work outside the hospital. This work was based on the self-directed model of care and adaptations of this. It proposed that the DHB expand activities that enable people to take greater responsibility for health and wellbeing. The expectation being that, a) ‘empowering’ people, and, b) developing more services in the community, would help to reduce demand on the hospital.
Feedback to date has suggested a need to not lose emphasis on the clinical expertise of the hospital and related services. This needs to be a point of focus and not simply assumed. We have also revised some of the language. It’s important that the message conveys our belief that we are all experts about our own bodies and our health. The big shift we need for the future is the sense of health workers, a) recognising the sovereignty of the individual, and, b) working in ways that partner with patients, concentrating on what matters most for each patient.
This version of the strategy has been modified on the basis of feedback from the senior team and others. The current version now concentrates more deliberately on the dual role that the DHB has as Commissioner/Funder and Provider. We have also brought the provider issues to the foreground and made them more explicit. Managing provider services in a sustainable way while expanding our clinical, teaching and research expertise is one of our greatest challenges for the future.
While the strategy remains high level, it provides sufficient direction for both the Funder and Provider. The detail for each priority action and within each workstream will sit in in other plans. The Strategy will remain a live document and will iterate to ensure it meets the on-going needs of the organisation.
The next steps are to take this version to our community partners for their feedback and support.We are also working with the Chief Adviser Tikanga to make sure that the Māori language is used correctly and that we have appropriate use of Tikanga.
10.1
51

OPEN
Auckland District Health BoardBoard Meeting – 10 December 2014Page 2
2. The Provider StrategyA planning session was held with the Provider Group in early November. From this planning day,several themes were selected to drive future activity. These themes aligned well with the draft workstreams in the Strategy and the Strategy now encompasses the majority of issues that are currentlyfacing the Provider and the organisation as a whole. We are keen that every staff member has ‘a clear line of sight’ from the work they are doing, to the high level direction of the organisation.
A Provider Strategy is being developed concurrently. This will tease out more of the complexity of providing services to a local population as well as services on contract to other DHBs. The issues around cost pressures and solutions will sit in the Provider Plan. It is critical to ensure a logical connection between this work, our annual plan and our various provider and directorate plans.
3. Annual Plan for 2015/16The first year actions to advance the Strategy will go into the Annual Plan for 2015-16. In order to inform the Annual Plan, our Strategy work needs to be completed by February 2015 and we are well on track to achieve this. We are working closely with the Planner for Auckland DHB to make sure that the various plans under development are done together and are designed with good and logical links between them.
4. Values workA considerable amount of effort has gone into developing a new set of values for Auckland DHB. Although this has taken longer than was imagined, the Strategy is considerably improved by being grounded in a set of values that set the organisational culture and behaviour.
The Values Project will arrive at a set of organisational values by the end of December 2014. The results of Values Week have been analysed and various options for values developed and tested. We have been greatly assisted in this process by Tim Keogh of April Strategy. Many options and iterations of values have been tested with a variety of staff groups and especially with our executive.
The preferred option under final discussion at the moment is:
The words in bullet points are taken directly from language used by patients and staff through the process.
52

OPEN
Auckland District Health BoardBoard Meeting – 10 December 2014Page 3
Each value will have a corresponding translation in Māori. We are working with our Chief Adviser Tikanga and her team to make sure that we represent our relationship with Māori correctly, and that we have the appropriate use of te reo alongside the English words.
Throughout the process, there was a Maya Angelou quote that resonated well with people and it will sit as part of the material that supports the values.
I've learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel.
Maya Angelou
This quote has been translated into Māori by Matua Pita Pou.
We are currently testing these final preferred values with some groups of staff and with our executive. Once we have completed this final feedback phase, we will return to the Board. This version of the Strategy includes the preferred set of values that are being consulted on. Once agreed, the final values will have a high profile across the Strategy and related material, and the organisation.
In 2015 the values will be rolled out across the organisation as part of a coordinated organisation development plan.
5. Next StepsIn December we will complete the final wave of feedback on the proposed values. They will be incorporated into the Strategy and the work to roll them out will be led by the new Director of Strategic Human Resources who joins us in the New Year.
The Strategy will be circulated to our community partners, and in particular to Te Runanga o Ngati Whatua and our Primary Health Organisations, for their feedback and support.
The Strategy will inform the Provider Strategy process which is underway and the Annual Plan for 2015/16.
We will keep the Board updated on progress as the detailed work to progress the Strategy is developed.
10.1
53
1
Te Toka Tumai The Strategy for Auckland District Health Board to 2018
Healthy communities -- World-class healthcare -- Achieved Together Hei O ranga T ika Mo Te I t i Me Te Rah i
Our values underpin everything we do.
Tēnā koe
- I see you and welcome you as a person
Respect
- Respect, nurture and care for each other
Work together
- A team with colleagues, patients and families
Aim high
- Aspire to excellence & the safest care
Health is personal. It begins where we live, learn, work and play. Each one of us has different experiences and aspirations for our health and wellbeing, for our whānau, and our community. People thrive when they are able to act with autonomy. We will enable people to determine and achieve the health outcomes that matter to them. We will support them with world leading health, healthcare and disability services that are cohesive, equitable and sustainable.
As a District Health Board we are charged with improving, promoting and protecting the health of our local population, and, to the extent possible, to do this in a way that responds to the things that matter for each person who comes in contact with us. This strategy concentrates on five areas where a self-determining approach requires real changes in how we do things.
Our updated assessment of health need has identified the areas causing the greatest ill health and disability for our population. These areas need our attention. We will be tough on the problems that are claiming so many lives. Many of the long-terms consequences and deaths associated with heart disease, cancer and diabetes are avoidable. We need to work on policies and relationships right across our district so that healthy eating and physical activity are easy choices for people to make. We will do this in meaningful partnership with our patients, whānau, iwi and communities.
As Auckland DHB we are unique. As a tertiary and national centre, we provide specialist services that are not available elsewhere. Over half our activity is for patients outside our district. We are also a major academic facility, carrying a large and essential training and research role for the country. These are strengths and points of distinction. These multiple roles also put pressure on resources and on our ability to serve our own population. It’s a delicate balance.
The way we work needs to be sustainable over the long term. That means being well prepared to meet growing demands. We need to think critically about the design and delivery of our services and be bold in our innovations. We can only do this with the involvement of our Treaty partners, patients, whānau and communities.
Ailsa Claire Dr Lester Levy Chief Executive Chair
Te Toka Tumai is the Māori term for Auckland DHB. It refers to the rock that stands firm in the sea of the Waitemata harbour of Tamaki Makaurau (Auckland).
The rock reminds us that the health system needs to be a solid whole, where all the activities across the continuum of health are joined.
Te Toka Tumai is our proud and stable foundation when the going is tough. Our lives may depend on it.
54
2
Our greatest challenges
Getting tough on the right problems
Heart disease and stroke are two of the largest causes of avoidable death in our district. This is an area with the largest opportunity for improvement. 70% of cardiovascular disease may be linked to risk factors that we can modify through lifestyle. Screening programmes for cardiovascular disease link people with early signs of problems to treatment. The number of people with diabetes has more than doubled since 2003 and this affects about 6% of our population. People with diabetes need help to manage risk factors, such as blood pressure and blood sugar levels, and encouragement to have eye tests. Māori and Pacific people carry a heavier burden than other ethnicities for heart disease and for diabetes.
Cancer makes up 28% of all deaths, with the most significant being breast (in women), lung and colorectal cancers, and prostate cancers in men. Although screening for breast cancer is free, a third of eligible women do not participate. For lung cancer, the continuing reduction in smoking rates is a high priority.
One in eight of our residents suffers from some form of mental illness with 3.5 % of our population using mental health services. Māori are particularly affected by mental health problems, being twice as likely as Europeans to use services. Pacific people report anxiety and distress twice as often as Europeans, but do not access mental health services. We need to work with localities and with communities of interest to build the kind of supports and services that we know act as buffers for people living with stress, disadvantage and discrimination.
Healthier lifestyles to prevent deaths and long term conditions
Approximately a quarter of deaths for our population are potentially avoidable. Of these, half could have been avoided through adopting a healthier lifestyle; a quarter could be prevented by getting problems (like hypertension) managed before they lead to illness; and a quarter could be avoided through getting illnesses treated early on. Eleven percent of adults in our district are regular smokers, with higher rates among Māori and Pacific people.
One in five adults are obese, and over half are overweight. Our rate of hazardous alcohol consumption is higher than the national rate across all ethnicities except for Asian. About half our population meet the recommended level for daily exercise, and more than 40% do not meet daily fruit and vegetable guidelines. Health services play a key role in supporting our population to stop smoking, eat more healthily and to exercise more.
Building a sense of shared responsibility for wellbeing
Helping our population to achieve health, independence and wellbeing requires an investment in prevention and early intervention work. This largely happens in local communities, working with partner organisations, iwi and communities. It is hard to balance the need for prevention work along the immediate and growing demand for health services. It is especially hard to resource action that tackles the social determinants of poor health e.g. poverty, isolation, violence and discrimination. Prevention requires a shared responsibility for making Auckland healthy. It means working with other public agencies and services on improved housing, education, employment, and the physical environment, as well as access to health services.
Putting real meaning and effort behind health equity
The gap in life expectancy is increasing with Māori and Pacific people living (on average) six to eight years less than the European/Other population. Māori and Pacific people are two to three times more likely to be hospitalised than European. More Māori and Pacific people will die from a number of chronic diseases. Nearly 20% of our population live in areas that are highly deprived, and high deprivation is associated with poorer health outcomes.
10.1
55
3
We have failed to make significant impacts for disadvantaged groups. Our health needs assessment data shows that significant inequities between groups exist. Some people miss out on the health services they need, while others report a negative experience when they do come for help. We need to be bold in making the health system free from discrimination. We need dedicated programmes and services to redress inequity, particularly for Māori where we have clearly defined responsibilities under the Treaty. Pacific people and those living in poverty also need focused work, along with our significant and growing Asian population.
Focus on both young and old
Inequities persist in infant and child death rates and hospitalisation. The infant mortality rate for Māori and Pacific is nearly twice that of European/Others, with the most common causes of death: perinatal conditions, congenital conditions, and sudden infant death. For children aged 1-14, the most common causes of death are cancer, congenital anomalies, accidents and suicide. Children are admitted to hospital most commonly for injuries, gastroenteritis, asthma and infections. The incidence of rheumatic fever is one lower than the national average, however significant inequities are present for Māori and Pacific populations.
The percentage of children enrolled with a PHO by the age of three months is much lower than the national average. Immunisation by 8 months of age is low for Māori. The most common causes of mortality for young people aged 15-24 years are intentional and unintentional injury, cardiovascular diseases and cancer. The most common acute admissions for young people aged 15-24 years are for injury, abdominal or pelvic pain and skin infections.
Older people have greater needs for health services and hospital care, and occupy about 45% of our medical and surgical beds. With the projected increase in the population aged 65 and over, there is a real need to ensure that people retain good health into older age.
Developing our people - a culture that lives our values
Our organisation covers over 10,000 diverse staff. These staff are responsible for planning services, funding services and for direct service provision, support services and research. Regardless of the size and complexity of our organisation, it’s vital that we make changes, and at a pace to meet demand, while at the same time being mindful of our important national teaching and training responsibility. Staff need a clear direction for the future, clear expectations and accountabilities, and a work programme aligned with vision and values. It’s important to have a strong sense of identity and foundation. Having a clear purpose and shared ways of working helps us measure and track results.
Doing more work in the community, specifically with primary care
We have to focus on what is most important to people to support their health and wellbeing, and to do this in a way that is financially sustainable over time. Currently we are predominantly a hospital focussed health system. There is significant opportunity to expand our primary and community services to rebalance the system and provide services that are more responsive to people’s needs. We know there are services we currently deliver in our hospitals that could be delivered in the community and we will work in partnership across the system to redesign our models of care around the patient.
The cost of tertiary and quaternary services needs to be fully covered
The funding we get from government needs to covers health and disability services across the system – from work in the community through to specialist services in the hospital. On top of our Funding Envelope, our DHB gets paid for the work we do for patients referred from other DHBs. The amount we are paid for some of our high cost specialist work does not cover the full cost of the treatment. Although these prices are set nationally, the pricing model has left us having to offset national work from funds that are earmarked for our own population. As a hospital of last resort, Auckland takes patients from all over NZ and the Pacific and carries the greatest burden for the costs associated with specialist interventions.
56
4
Our approach to 2018
People come first We recognise that the best health systems in the world are oriented around people. The people we serve - our patients, their families and communities, and our own workforce. Externally, we will work to ensure that everything we do, from the design of our buildings to the care we provide is designed with patients and families first and foremost. Internally we will work with our staff with the aim of becoming the employer of choice within Auckland.
Values to drive a change in culture
Our values-based approach will distinguish the work we do. Fundamentally the focus is on people; they come first. This recognises that people and communities are the experts when it comes to their health. When people need help from professionals, we’ll make it personal, attending to what matters for each person. This is respectful, just and human. We will make our values known and understood. The values will be visible across our actions: Tēnā koe, Respect, Work together, Aim high.
Good governance and accountability
As a good employer, we will invest in our people to build a strong, values-based organisation with robust governance and accountability.
Clinical and research excellence, and training
As NZ’s foremost specialist hospital, we strive for excellence in health practice. People trust the services we provide knowing they are getting the best in specialist care and research. We are driven to continually search for new ways of working and for interventions that put Auckland DHB at the forefront of health and healthcare. As NZs largest teaching hospital, we dedicate time and resource to developing health professionals for the future.
Self-determination to guide our models of care
People are healthier when they have autonomy and can set the direction for their health and healthcare. Health professionals can enable patients and communities to achieve the goals they determine for themselves. We will move away from ‘fixing people’ or ‘doing things to people’. We affirm the mana of the person and their right to determine what’s best for them. This approach recognises the expertise of the patient. Patients trust that we will attend to the things that matter to them. Family and whānau will be partners in the care of the patient.
Working with localities on the issues that matter to them
We will invest in our communities to ensure they are participating across the system. Communities know what’s needed and they can help determine, design and, in some cases, deliver health services locally. We will work with specific localities to help them determine the services they need and the best way of delivering this.
Recognising the strength in diversity and cross boundary work
Auckland is unique in the diversity of cultures. Our health work reflects this, as well as including a great diversity of skills and disciplines. Strengths-based work helps us see the value in our differences. This ecological approach says that there’s a place for everyone in the system. Work in teams and integrating services across borders makes the best of resources and streamlines care for the patient.
We’re tough on problems, not on people, and we focus on the right things
We need to get more vocal about the health problems that matter. Many hospital admissions are avoidable, some through a change in lifestyle and some through earlier engagement with primary care. Rather than blaming the individual, we need to use our expertise in health to work with other policy makers. We can take a lead on making it easier for people to be active, to eat healthy food and to engage confidently with services when these are needed. We know where we need to focus our efforts and we will work across the system to achieve the necessary change.
10.1
57
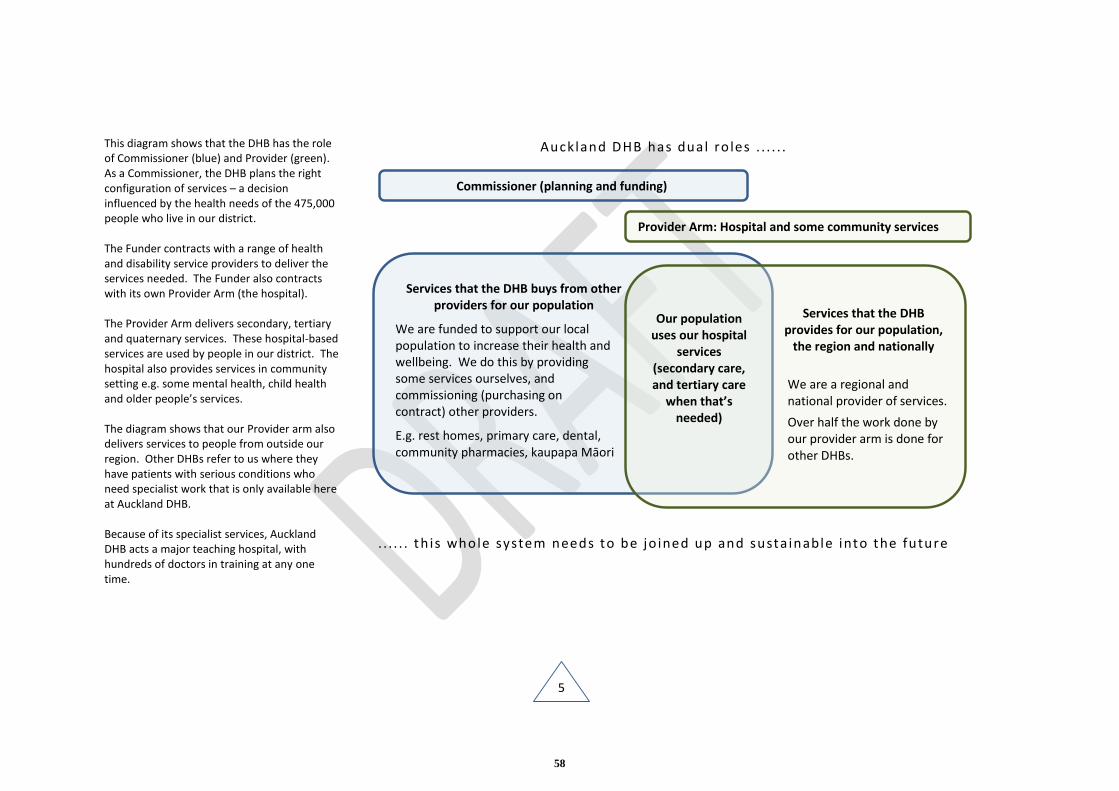
5
This diagram shows that the DHB has the role of Commissioner (blue) and Provider (green). As a Commissioner, the DHB plans the right configuration of services – a decision influenced by the health needs of the 475,000 people who live in our district. The Funder contracts with a range of health and disability service providers to deliver the services needed. The Funder also contracts with its own Provider Arm (the hospital). The Provider Arm delivers secondary, tertiary and quaternary services. These hospital-based services are used by people in our district. The hospital also provides services in community setting e.g. some mental health, child health and older people’s services. The diagram shows that our Provider arm also delivers services to people from outside our region. Other DHBs refer to us where they have patients with serious conditions who need specialist work that is only available here at Auckland DHB. Because of its specialist services, Auckland DHB acts a major teaching hospital, with hundreds of doctors in training at any one time.
Auckland DHB has dual ro les . . . . . .
. . . . . . th is whole system needs to be jo ined up and susta inable into the future
Services that the DHB buys from other providers for our population
We are funded to support our local population to increase their health and wellbeing. We do this by providing some services ourselves, and commissioning (purchasing on contract) other providers.
E.g. rest homes, primary care, dental, community pharmacies, kaupapa Māori
Services that the DHB provides for our population,
the region and nationally
We are a regional and national provider of services.
Over half the work done by our provider arm is done for other DHBs.
Our population uses our hospital
services (secondary care, and tertiary care
when that’s needed)
Commissioner (planning and funding)
Provider Arm: Hospital and some community services
58
6
Our five priority areas
1. Patients and whānau at the centre
Where we are today – the case for change The view from 2018
Our values (tena koe, respect, work together, aim high) remind us to engage mindfully with patients and communities. This means stopping, listening and hearing what matters to each person. We need to make the time to do this and to have the system support us.
Patients want to control the care they need. Families and whānau want to be partners in care. This requires health services tailored to suit each patient’s needs. Greater use of technology will be one key way in which patients can direct their own care in the future. We must accelerate the ways and means by which patients can access and manage their own health records.
Our care pathways are not clearly defined or accessible, and there are many examples of variability and inefficiency with little use of outcome data.
Whānau Ora promises wrap-around help for the patient and whanau. Care will be coordinated and situated where it’s needed. We can do more to have family and whānau engaged as partners in care. We need to ensure cultural concordance and respect.
People living in Auckland DHB need to know how to keep healthy and where to go for help. Patients want health and disability services linked across the system. We will have more services where people work, live and play.
We have parts of a patient centred system, and we have made a good start, but there is much more we can do.
Patients have the information they need to make decisions, and the system is oriented such that they are able to determine their own care consistently across every interaction.
Our measures of success have shifted from things we define, to achievement of the outcomes defined within patients’ own care plans. Patient experience outcomes are a key part of the accountability framework.
Patients and whānau are intimately involved in service planning and in governance
We are making use of communication technology so we can communicate with patients and families in ways that they choose. Patient portals are in place
First impressions of our services, whether it’s receipt of a letter or arriving at our front door, are exemplary. Co-design with patients has led to easy wayfinding to and through our facilities. The pathways of care are clear, informed by evidence and designed around patients. Where required, there will be people in the system to help patients navigate.
Family and carers will be a core part of the care team. Patient and family driven care plans, e.g. end of life care plans will be the norm.
Insight, via surveys and other means, drives our improvements.
Co-design approaches are embedded for every directorate and locality co-design is visible through consumer and family forums. Comprehensive wellness programmes are in place.
We will be renowned for our patient-centred approaches, whether it’s through our personal interactions and championing of self-determination of care, our easy access to patient and family education and information, or our health promoting physical facilities.
10.1
59
7
2. Values and equity underpin everything we do
Where we are today – the case for change The view from 2018
We collect a lot of data on our performance and health outcomes but are not good at using that information to understand our performance and make positive change. We need to make much better use of the data we collect. Most of our current data exists at a high level making directorate level action difficult.
In order to reduce health inequities, we need to make sure that our funding follows the need, and we have dedicated programmes and services.
We need to work with Te Runanga o Ngāti Whātua to accelerate the plan for Māori health. Systems need to be configured around Māori health gain and our MoU arrangement with our Treaty partner.
The organisation and all our processes need to be culturally safe. We know that staff welcome diversity across culture, professional group, treatment methodologies and disciplines. This is a point of some distinction for Auckland DHB. However along with diversity comes the need for training and supports so that staff feel confident working across cultures and disciplines.
Part of the equity agenda will do more to recognise the role that women continue to play as caregivers and as the mainstay of our workforce.
We have a solid foundation to build a values-based culture but there is much work to do to embed it across all parts of the organisation.
We will be using the information we already have to understand our current performance and prioritise our work, based on what we know.
We will work with our people to agree what needs to be done to reduce inequalities and will set goals and performance targets by directorate to reduce inequity in outcomes, including specific measures and timelines.
Our health resources follow the need. The health and disability system is more fair and just, and it actively reduces inequity. Working directly with high need communities and community leaders we are making the needed improvements to our systems and practices.
We have become the employer of choice in Auckland because we have a strong, values-based culture that people believe in and model. People are proud to work for Auckland DHB.
Everybody will know our values and understand what they mean to them and their work. People will see the organisation really living the values, from the Board and senior management right throughout the organisation.
There will be transparency in the work we do and in our performance.
60
8
3. Guarantee safety and high quality work
Where we are today – the case for change The view from 2018
Auckland DHB has a very specialised and skilled staff that, on the whole, provide excellent clinical services. But we can do better.
We don’t make best use of clinical outcome data and when we do it’s not always consistent or timely. We don’t routinely use our data to inform our improvement activity and our safety culture tends to be reactive rather than proactive. We tend to have low visibility of the improvements we make.
We have access to international benchmarking but don’t always use this to best effect. We know we have differences in outcomes for different groups and we need to focus on both identifying and reducing inequalities where they exist.
Much like other areas, we don’t operate as a cohesive unit across the DHB. We could accelerate our learning and improvement by more open and deliberate sharing and collaboration between services.
Cultural safety needs to be a given. Training across the DHB will make sure everyone is skilled to make a positive difference.
We know we have to make the transitions between services much better and with the patient having much more control in this process. This way of working makes sure that we design services that best fit patient needs.
Well defined outcome measures for all services which are used to improve and inform. The measures are important to patients and to staff
Safety and clinical outcome data is directing our future actions in a planned and consistent way with a focus on outcome informed improvement
We make good use of international and local collaborations for benchmarking. The benchmark comparisons are consistent and valid for us and drive us to constantly improve.
We have fostered a culture of transparency where outcomes are shared with all: patients, staff and stakeholders alike.
People trust our services, knowing we provide the best in specialist care and research. Auckland DHB is synonymous with clinical and research excellence. A strength is our continual search for new and better ways of working. A thirst for inquiry and innovation helps us to stay abreast of growing expectations around treatment.
Our practice is reflective which means keeping an eye on continuous improvement. Staff are mindful of their practice and learn from peers and colleagues. Patient experience ratings improve for prioritised groups and we see a reduction in hospital adverse events such as falls and infections.
We are leading quality and safety work, setting a standard well beyond the expected. The patient feedback cycle has been accelerated so we learn how to improve our performance at every step. We are quick to respond to patient feedback and to complaints.
More coordinated and integrated care has led to reduced clinic non-attendance (DNA) and re-admission rates. More people are managing their long term conditions in the community, with enhanced community and primary care assistance when required.
10.1
61
9
4. Get the best outcomes from our resources
Where we are today – the case for change The view from 2018
A great many of the resource issues facing us are sector wide issues. We have to do more work with every dollar we get from government and this pressure will only increase over time.
It’s important that we fully understand the scope of work we do as a tertiary and national hospital of last resort. This work needs to be costed accurately and funded appropriately. Work that is not covered under our existing payment arrangements is done to the detriment of our own population. There is real urgency in addressing this.
We need to work with our regional partners to establish the right mix and configuration of specialist work for our region and to support working nationally on specialist services and price.
Some currently hospital-based work could be managed within primary care. There needs to be genuine collaboration across primary and secondary care to develop new models of care that reduce reliance on hospital services. Many of our hospital admissions and re-admissions point to us missing problems at an early stage. We want these problems managed earlier by the person’s GP.
All DHB staff need an understanding of basic improvement science to help us get the best value from our resources.
We know from overseas hospitals that our volunteer base could be expanded to occupy a more defined and legitimate place in the health and disability sector. We need to develop our volunteer workforce and open the doors to them.
Sustainability requires us to think well beyond health. As one of the country’s largest employers we need to show leadership in the use of the country’s resources and the waste we create.
By 2018, we will see much more work being done in the community, with primary care being the hub that manages the care that people need.
Hospital services will be used more selectively i.e. when these are really needed.
Close and collaborative working relationships with our local, regional and national funders mean that our hospital services will be running within the funding allocated.
There will be real clarity about the tertiary and national services that other DHBs want us to provide for their patients with clear and agreed service specifications for each.
Everyone in the system will have information so they can make the best decisions, including patients and families, as well as staff.
Through our community partnerships and support we will see improved health literacy with a reduction in the gaps between health outcomes for high need groups compared to others.
Whānau Ora and wrap around care tailored to the patient will be well established and contributing to reduced admission rates and better health outcomes.
All our staff are trained in basic improvement methods and we have a visible culture of improvement where people are always looking to do things better.
We will have a highly developed and expanded volunteer programme that is a model for other health organisations to learn from.
62
10
5. Enabling people, systems and structures
Where we are today – the case for change The view from 2018
We hold considerable accountability as a DHB, however our vision and purpose are not clearly articulated and understood.
Our new structure is streamlining responsibility in our provider arm. There is one line of accountability that holds Directors responsible for quality health service delivery within their service area but there is an urgent need to support those leaders to develop their skills, their teams and the organisation as a whole.
We have many great people and departments but we do not function as a whole. Our internal communication needs to improve with information shared more openly and widely.
In 2014 we engaged widely around a new set of values for Auckland DHB. In the coming years these need to be embedded through the development and roll-out of an organisational development plan. Our values need to be visible in action and applied across everything we do.
Our current IT infrastructure is fragmented, unstable and system-centric. We have a once in a generation opportunity through the regional ‘Wicked’ programme to transform this key enabler and we must take it.
As a health organisation we need to play our part and role model action on climate change.
We know we are not the best employer we could be. We frequently fall short of standards we set ourselves and this needs to change. We are conscious that the systems we create can act as barriers to innovation, to equity and may impede the kind of fundamental human connections that are so vital to the health system.
All of our 10,000 staff, and the population we serve, are clear about why we are here and the difference we are trying to make.
Our system is understood and decision making is clear with accountability both known and enacted across the continuum of care. Our leaders are supported by strong clinical governance and accountability frameworks across this decision making that includes our primary and community care partners. In particular we will honour our responsibilities to manawhenua.
We will be acknowledged as an organisation where there is clear line of sight from the “Board to the floor” with every employee knowing how they are contributing. There will be clear lines of communication, responsibility and accountability.
Our values have set a path for a change in culture, and we have made a long-term commitment to training and development for all staff and for our leaders.
We will see an increased number of Māori and Pacific across the Auckland DHB health workforce, and our volunteer base significantly expanded across the system with clearly defined roles.
Our staff will be trained and demonstrating cultural competence, and will be working with patients in ways that motivate and enable them to determine their care.
We will have shifted some services and redeveloped others so they are closer to settings that work for the most vulnerable people.
We have the right mix of specialist services for the region and these are funded sustainably. We continue to generate world-leading clinical research.
Auckland DHB is acknowledged as a leader in the public sector for energy use and waste minimisation.
10.1
63
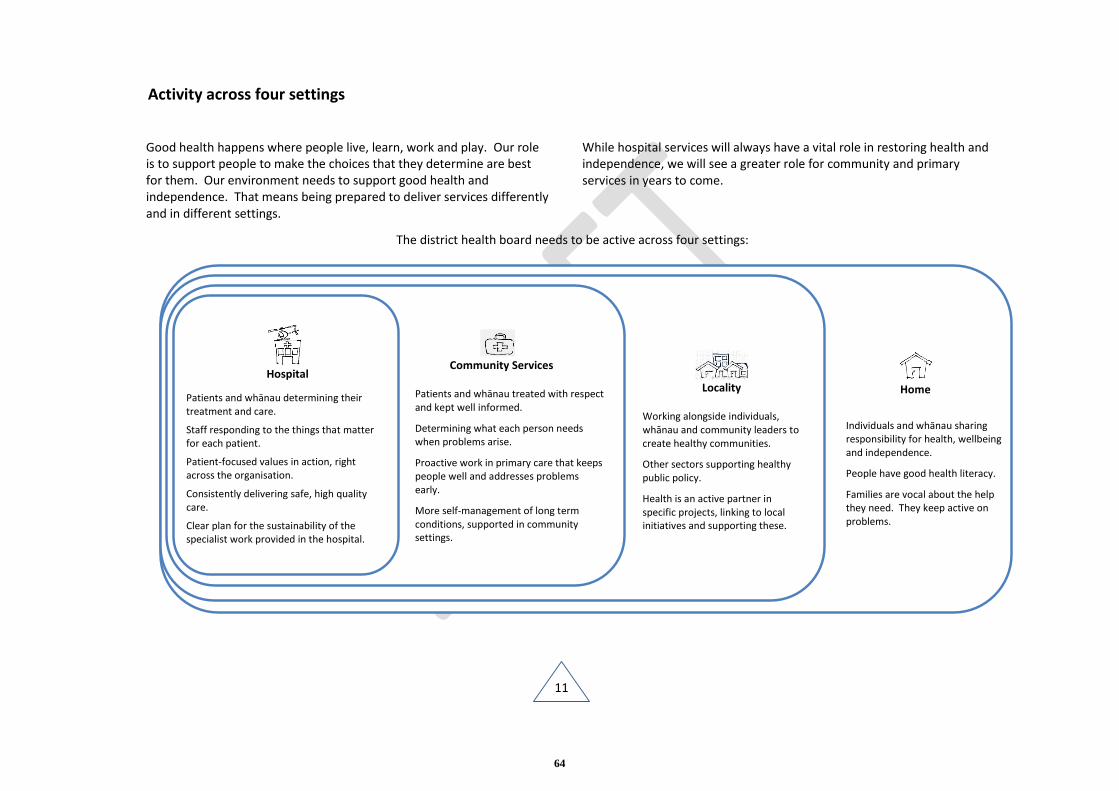
11
Activity across four settings
Good health happens where people live, learn, work and play. Our role is to support people to make the choices that they determine are best for them. Our environment needs to support good health and independence. That means being prepared to deliver services differently and in different settings.
While hospital services will always have a vital role in restoring health and independence, we will see a greater role for community and primary services in years to come.
The district health board needs to be active across four settings:
Home
Individuals and whānau sharing responsibility for health, wellbeing and independence.
People have good health literacy.
Families are vocal about the help they need. They keep active on problems.
Locality
Working alongside individuals, whānau and community leaders to create healthy communities.
Other sectors supporting healthy public policy.
Health is an active partner in specific projects, linking to local initiatives and supporting these.
Community Services
Patients and whānau treated with respect and kept well informed.
Determining what each person needs when problems arise.
Proactive work in primary care that keeps people well and addresses problems early.
More self-management of long term conditions, supported in community settings.
Hospital
Patients and whānau determining their treatment and care.
Staff responding to the things that matter for each patient.
Patient-focused values in action, right across the organisation.
Consistently delivering safe, high quality care.
Clear plan for the sustainability of the specialist work provided in the hospital.
Patients and whānau determining their treatment
and care.
Staff focused on responding to the things that matter for
each patient.
Patient-focused values in action, right across the
organisation.
Consistently deliver safe, high quality care.
Clear plan for the sustainability of the specialist
64
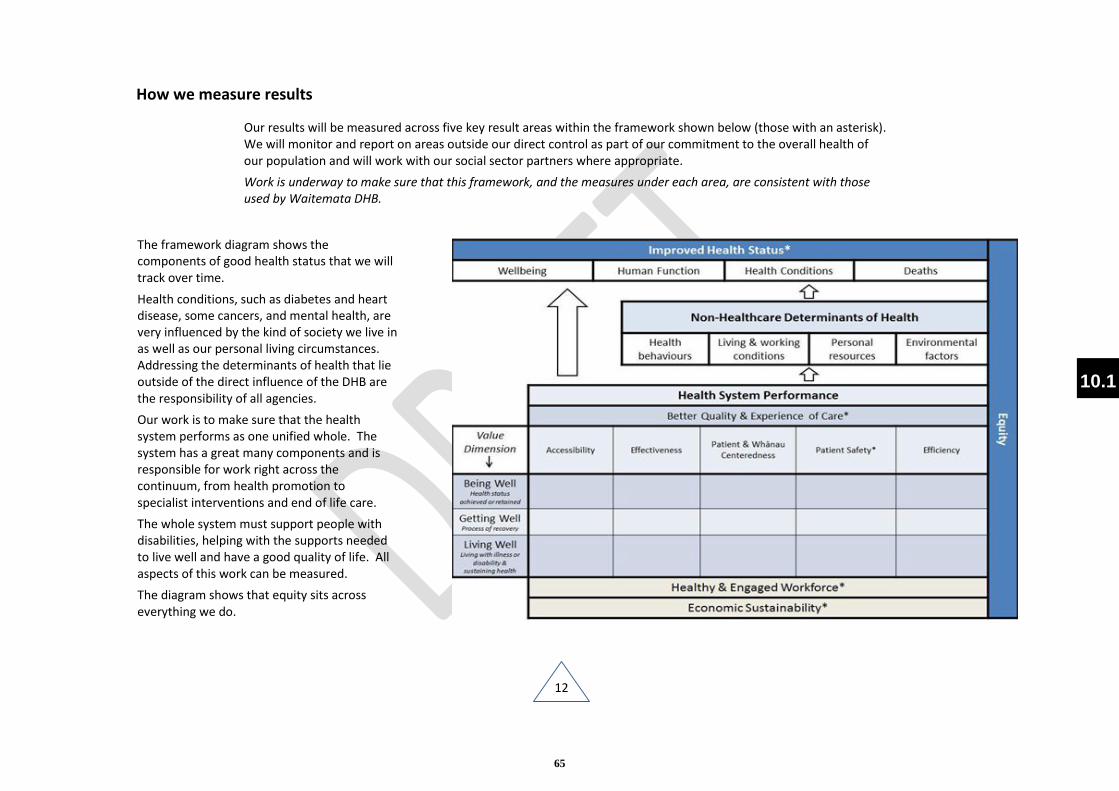
12
How we measure results
Our results will be measured across five key result areas within the framework shown below (those with an asterisk). We will monitor and report on areas outside our direct control as part of our commitment to the overall health of our population and will work with our social sector partners where appropriate.
Work is underway to make sure that this framework, and the measures under each area, are consistent with those used by Waitemata DHB.
The framework diagram shows the components of good health status that we will track over time.
Health conditions, such as diabetes and heart disease, some cancers, and mental health, are very influenced by the kind of society we live in as well as our personal living circumstances. Addressing the determinants of health that lie outside of the direct influence of the DHB are the responsibility of all agencies.
Our work is to make sure that the health system performs as one unified whole. The system has a great many components and is responsible for work right across the continuum, from health promotion to specialist interventions and end of life care.
The whole system must support people with disabilities, helping with the supports needed to live well and have a good quality of life. All aspects of this work can be measured.
The diagram shows that equity sits across everything we do.
10.1
65
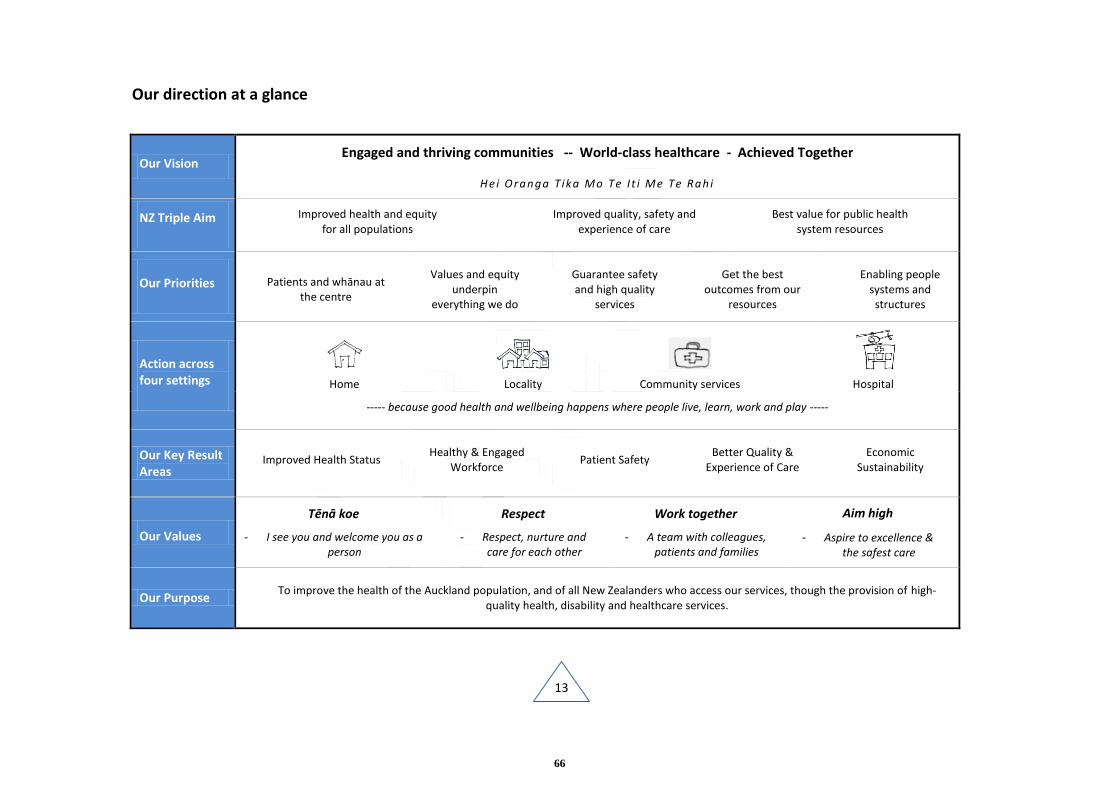
13
Our direction at a glance
Our Vision Engaged and thriving communities -- World-class healthcare - Achieved Together
Hei O ranga T ika Mo Te I t i Me Te Rah i
NZ Triple Aim Improved health and equity for all populations
Improved quality, safety and experience of care
Best value for public health system resources
Our Priorities Patients and whānau at the centre
Values and equity underpin
everything we do
Guarantee safety and high quality
services
Get the best outcomes from our
resources
Enabling people systems and structures
Action across four settings
Home
Locality
Community services
Hospital
----- because good health and wellbeing happens where people live, learn, work and play -----
Our Key Result Areas
Improved Health Status Healthy & Engaged
Workforce Patient Safety
Better Quality & Experience of Care
Economic Sustainability
Our Values
Tēnā koe
- I see you and welcome you as a person
Respect
- Respect, nurture and care for each other
Work together
- A team with colleagues, patients and families
Aim high
- Aspire to excellence & the safest care
Our Purpose To improve the health of the Auckland population, and of all New Zealanders who access our services, though the provision of high-
quality health, disability and healthcare services.
66
OPEN
Auckland District Health BoardMeeting of the Board 10/12/2014
Establishment of Executive Committee of the Board
Recommendation
1. That the Board approve the establishment of an Executive Committee (under schedule 3 clause 38 of the New Zealand Public Health and Disability Act 2000) to consider any matters that require the urgent attention of the Board during the Christmas/ New Year Board recess.
2. That membership of the Committee is to comprise the Board Chair, the Deputy Board Chair (Lee Mathias), Ian Ward, Jo Agnew and Gwen Tepania-Palmer, with a quorum of three members (the Chair needs to be one of the three members).
3. That the Executive Committee be given delegated authority to make decisions on the Board’s behalf relating to the urgent approval of business cases, leases and the awarding of contracts for facilities development, services and supplies and information services and on any other urgent recommendations from a Committee or the Chief Executive (same arrangements as last year).
4. That all decisions made by the Executive Committee be reported back to the Board at its meeting on 18 February 2015.
5. That the Executive Committee be dissolved as at 18 February 2015.
Prepared by: Dr Lester Levy (Board Chairman) and Marlene Skelton (Corporate Business Manager)
Glossary
NZPH&D Act - New Zealand Public Health and Disability Act 2000
1. Purpose
To seek the Board’s approval to establish a committee to conduct pressing Board business during the Christmas/New Year recess.
2. Background
The final normal scheduled meeting of the Board for the year is on 10 December 2014. The next meeting is on 18 February 2015. There might be some items of business requiring approval at Board level that need to be processed during this period.
Under the NZPH&D Act (Schedule 3 Clause 38) there is provision for the Board to establish one or more committees for a particular purpose or purposes.
3. Proposal
As in recent years, it is proposed that the Executive Committee should have a relatively small membership so that it can be convened at short notice, should this be necessary. The proposed membership is the Board Chair and Deputy Chair (Lee Mathias), Ian Ward, Jo Agnew and Gwen Tepania-Palmer, with a quorum of three (the Chair needs to be one of the three members).
It is expected that, by their nature, any items referred to this Committee are likely to need to be taken in public excluded session. The date and agenda items of any meeting(s) would, assoon as confirmed, be advised to all Board members and meeting(s) publicly notified if they involve any open meeting agenda reports.
10.2
67

Auckland District Health Board Page 1 of 3Meeting of the Board 10/12/14
Resolution to exclude the public from a meeting
Recommendation:That in accordance with the provisions of Clauses 32 and 33, Schedule 3, of the New Zealand Public Health and Disability Act 2000 (“Act”):
The public now be excluded from the meeting for consideration of the following items, for the reasons and grounds set out below:
General subject of each item to be considered:
Reasons for passing this resolution in relation to each item:
Ground(s) under Clause 32 for the passing of this resolution
1Confirmation of the Public Excluded Minutes of the Board Committee Meeting 29 October 2014
Confirmation of MinutesAs per resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act 2000.
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
2Confirmation of the Confidential Addendum Minute Meeting of the Board held on 29 October 2014
Confirmation of MinutesAs per resolution(s) from the open section of the minutes of the above meeting, in terms of the NZPH&D Act 2000
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
3Health and Safety Report
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
Obligations of ConfidenceThe disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 S.9(2)(ba)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
4.1Financial Report
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
11
68
Auckland District Health Board Page 2 of 3Meeting of the Board 10/12/14
6.1Fluroscopy Replacement Machines
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.2Cytology Service Fit-Out
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.3Perioperative Service Fleet Instruments
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.4Auckland DHB Authorised Banking Signatories
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.5Food Services Business Case
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
That the public conduct of the whole or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
6.6Upgrade of Access Control and CCTV Systems at Auckland DHB/dispensation
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
7.1Human Resources Report
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982
69
Auckland District Health Board Page 3 of 3Meeting of the Board 10/12/14
[NZPH&D Act 2000]
8.1Women’s Health Auckland DHB/Waitemata DHB Collaboration Options for Change
NegotiationsTo enable the Board to carry on, without prejudice or disadvantage, negotiations (including commercial and industrial negotiations)[Official Information Act 1982 S.9 (2) (j)]
Obligations of ConfidenceThe disclosure of information would not be in the public interest because of the greater need to protect information which is subject to an obligation of confidence [Official Information Act 1982 S.9(2)(ba)]
or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
9.1DHB Board Community Lab
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
9.2Regional Wicked Project Status Update
Commercial ActivitiesTo enable the Board to carry out, without prejudice or disadvantage, commercial activities[Official Information Act 1982 S.9 (2) (i)]
or the relevant part of the meeting would be likely to result in the disclosure of information for which good reason for withholding would exist under any of sections 6, 7, or 9 (except section 9(2)(g)(i)) of the Official Information Act 1982 [NZPH&D Act 2000]
11
70