bmj openrozeena garner mbbs mrcp (rheum) 2, rakesh kumari mbbs md mrcp (rheum) 2, peter lanyon dm...
TRANSCRIPT
For peer review only
Prevalence, risk factors and associations of Primary
Raynaud’s Phenomenon: Systematic review and meta-
analysis of observational studies
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006389
Article Type: Research
Date Submitted by the Author: 15-Aug-2014
Complete List of Authors: Garner, Rozeena; Queens Medical Centre, Rheumatology Kumari, Rakesh; Queens Medical Centre, Rheumatology Lanyon, Peter; Nottingham University Hospital, Rheumatology; Queens
Medical Centre, Rheumatology Doherty, Michael ; University of Nottingham, Academic Rheumatology Zhang, Weiya; University of Nottingham, Academic Rheumatology; Nottingham University, Academic Rheumatology
<b>Primary Subject Heading</b>:
Epidemiology
Secondary Subject Heading: Rheumatology
Keywords: RHEUMATOLOGY, EPIDEMIOLOGY, STATISTICS & RESEARCH METHODS
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on M
arch 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006389 on 16 March 2015. D
ownloaded from
For peer review only
1
Prevalence, risk factors and associations of Primary Raynaud’s Phenomenon: Systematic
review and meta-analysis of observational studies
Rozeena Garner MBBS MRCP (Rheum) 2, Rakesh Kumari MBBS MD MRCP (Rheum)
2, Peter
Lanyon DM FRCP MRCGP DRCOG2, Michael Doherty MA MD FRCP
1, 2, Weiya Zhang BMed
MEpi PhD1
1Academic Rheumatology, University of Nottingham, UK;
2Department of Rheumatology,
Queens Medical Centre, UK
Correspondence to:
Dr Weiya Zhang
Academic Rheumatology
Clinical Sciences Building
Nottingham City Hospital
Nottingham NG5 1PB
UK
Telephone: +44 (0)115 823 1756
Fax: +44 (0)115 823 1757
Page 1 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
2
Email: [email protected]
Keywords: Primary Raynaud’s phenomenon, prevalence, incidence, risk factors, systematic
review
Word Count: Abstract: 243, main text: 2685
Page 2 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
3
Abstract
Objective: To systematically review the literature with regard to the prevalence, incidence,
risk factors and associations of primary Raynaud’s phenomenon (PRP).
Method: A systematic review of the literature of observational studies for PRP was
undertaken using five electronic databases. Any studies reporting prevalence, incidence and
risk factors of PRP were collected. Relative risk or odds ratio (OR) and 95% confidence
interval (CI) were extracted or calculated to present the association between risk factors
and PRP. Random effects model was used to pool the results.
Results: 33 articles assessing a total of 33, 733 participants were included in this analysis (2
cohort, 17 cross-sectional and 14 case-control studies). The mean prevalence of PRP was
4.85% (95% CI 2.08%, 8.71%) in the general population. The annual mean incidence of PRP
was 0.25% (95% CI 0.17, 0.33). Risk factors and associations for PRP included female gender
(OR 1.65, 95% CI 1.42, 1.91), family history (OR 16.6, 95% CI 7.44, 36.8), smoking (OR 1.27,
95% CI 1.06, 1.53), manual occupation (OR 2.66 95% CI 1.73, 4.08), migraine (OR 4.02, 95%
CI 2.62, 6.17), cardiovascular disease (OR 1.69, 95% CI 1.22, 2.34) and marital status (OR
0.60, 95% CI 0.43, 0.83). The definition of PRP varied considerably between studies.
Conclusion: This is the first systematic review of the prevalence, incidence, risk factors and
associations of PRP. Further study using uniform strict criteria for the condition is required
to confirm these findings, particularly the possible association with cardiovascular disease.
Page 3 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
4
Strengths and limitations of this study
• This is the first meta-analysis of the literature for the global epidemiology of primary
Raynaud’s phenomenon (PRP).
• The prevalence and incidence of PRP in different countries were estimated. Female
gender, positive family history, smoking and migraines were found to be the major risk
factors for PRP.
• The lack of original data restricted an adequate estimation of the age-effect on PRP.
• Different definitions of PRP handicapped a comparison between countries
INTRODUCTION
In the 19th century, Maurice Raynaud first described Raynaud’s phenomenon (RP) as an
episodic, symmetrical, vasospastic disorder resulting in classic triphasic colour change,
trophic changes limited to the skin and uncomfortable sensory symptoms of the extremities
in the absence of arterial occlusion.[1] Further criteria have been suggested to distinguish
Primary Raynaud’s phenomenon (PRP) from secondary Raynaud’s phenomenon which
include detail regarding symptom duration, negative autoimmune serology, normal serum
inflammatory markers and capillaroscopy, and the clinical absence of any underlying
disease.[1-4] Use of colour charts to aid diagnosis has also been used.[4, 5] Despite this,
there is no unifying definition that is used worldwide for PRP.
There have been a number of studies performed in various countries reporting the
prevalence of PRP. The reported prevalence ranges from less than 1% up to 20%
depending on definitions and population selected.[6] In contrast, few studies have
examined the incidence of PRP and the true burden of PRP in the general population
remains unclear. PRP is thought to be more common in women, particularly when it
develops at a young age.[7] There are also reports of a hereditary component and links
with other vasospastic conditions such as migraine.[8-11] It is uncertain whether other co-
Page 4 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
5
morbidities or risk factors particularly related to vascular diseases such as ischaemic heart
disease and/or smoking have an association with PRP.
The primary objective of this study was to perform a systematic review of observational
studies to summarise the literature with regard to the prevalence, incidence and risk
factors/associations of PRP. The secondary objective was to examine the current definitions
used to define PRP worldwide.
METHODS
1: Literature search – data sources and search strategy
A systematic literature search was undertaken in June 2011 using five databases: Medline,
Embase, Cinahl, Amed and Pubmed. The search terms for “Raynauds” or “Raynauds
disease” were combined with the terms “epidemiology” , “prevalence”, “risk” or “incidence”
to generate the citations (see Appendix 1). “Cross sectional”, “case-control” or “cohort”
studies and “systematic review” were also applied for types of studies.
Abstracts were reviewed and the full papers were sought where abstracts were felt to be
relevant. Any duplicate articles were excluded (Figure 1). Where there was difficulty in
article retrieval, the authors were contacted via email. The literature search and abstract
review was completed by RG and validated by WZ.
Page 5 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
6
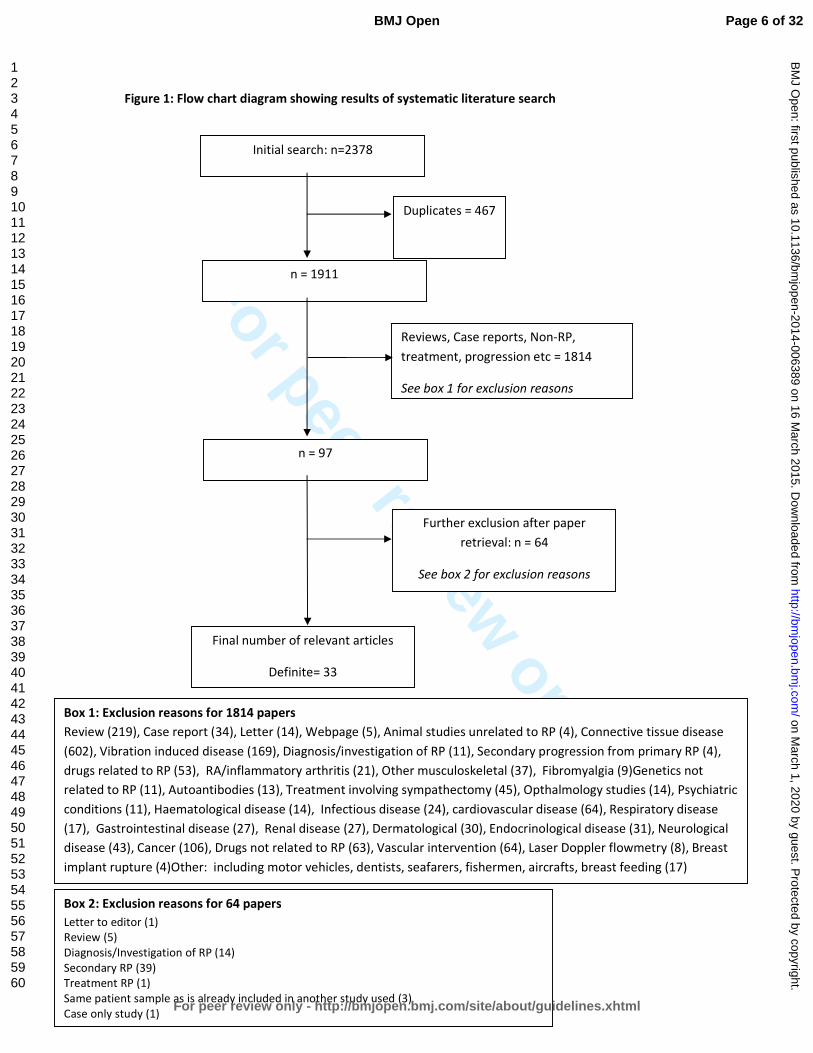
Figure 1: Flow chart diagram showing results of systematic literature search
Initial search: n=2378
n = 1911
n = 97
Final number of relevant articles
Definite= 33
Further exclusion after paper
retrieval: n = 64
See box 2 for exclusion reasons
Duplicates = 467
Reviews, Case reports, Non-RP,
treatment, progression etc = 1814
See box 1 for exclusion reasons
Box 1: Exclusion reasons for 1814 papers
Review (219), Case report (34), Letter (14), Webpage (5), Animal studies unrelated to RP (4), Connective tissue disease
(602), Vibration induced disease (169), Diagnosis/investigation of RP (11), Secondary progression from primary RP (4),
drugs related to RP (53), RA/inflammatory arthritis (21), Other musculoskeletal (37), Fibromyalgia (9)Genetics not
related to RP (11), Autoantibodies (13), Treatment involving sympathectomy (45), Opthalmology studies (14), Psychiatric
conditions (11), Haematological disease (14), Infectious disease (24), cardiovascular disease (64), Respiratory disease
(17), Gastrointestinal disease (27), Renal disease (27), Dermatological (30), Endocrinological disease (31), Neurological
disease (43), Cancer (106), Drugs not related to RP (63), Vascular intervention (64), Laser Doppler flowmetry (8), Breast
implant rupture (4)Other: including motor vehicles, dentists, seafarers, fishermen, aircrafts, breast feeding (17)
Box 2: Exclusion reasons for 64 papers
Letter to editor (1)
Review (5)
Diagnosis/Investigation of RP (14)
Secondary RP (39)
Treatment RP (1)
Same patient sample as is already included in another study used (3)
Case only study (1)
Page 6 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
7
2: Inclusion and Exclusion Criteria
Inclusion criteria: studies reporting the prevalence and/or incidence of PRP; studies
reporting potential risk factors associated with PRP; studies reporting human data on PRP in
people of any age; studies in any language (4 articles required translation – 1 Japanese, 1
Turkish, 1 French, 1 Italian).
Exclusion criteria (Figure 1): studies assessing treatment of PRP; studies involving
participants with Raynauds secondary to other diseases; studies assessing Raynauds in a
specific occupation e.g., people using vibration tools; unpublished material, case reports,
editorials, letters or reviews.
3. Data extraction and quality assessment
Study characteristics including age range, gender ratio and total number of participants in
the study were documented. The study design, country, setting (i.e. hospital or community
based) were also assessed and noted. If more than one article used the same study
population, the article where the data was felt to be presented most clearly was used in the
study. The definition of PRP and instruments used to confirm the condition were also
documented. The number of cases of PRP out of the number of people studied in a certain
time in the general population was documented as unadjusted crude prevalence. Incidence
figures were documented if the number of new cases of PRP in the population at risk
studied over a given period of time was stated.
Page 7 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
8
Risk factors and associations in the form of relative risk (RR) or Odds ratio (OR) were
extracted or calculated for the following:
o Constitutional: age, gender
o Environmental: employment, education, marital status, sex hormone
medications
o Genetic: family history in 1st
degree relatives
o Associations: smoking, alcohol, cardiovascular disease, migraine
An independent reviewer (RK) assessed a random selection of articles to ensure quality of
data extraction. The checklist for the Meta-analysis of Observational Studies in
Epidemiology (MOOSE) was followed to report the findings.[12]
4. Statistical analysis
Individual data for prevalence and incidence were derived from the original report either
directly or indirectly from the information provided in each study. Individual data for RR or
OR for risk factors or associations with PRP were extracted from the original report or
calculated using the available data given in the study. The fixed effects model was used to
combine the data if they were homogenous, otherwise the random effects model was used
if the data were heterogeneous.[13] Heterogeneity was examined using Forrest plots,
Cochran Q tests and I2
statistic as a measure for inconsistency due to chance.[14, 15]
Publication bias was assessed using funnel plots and Eggers test.[16] All analyses were
undertaken using StatsDirect© Version 2.7.9.
Page 8 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
9
RESULTS
1: Study characteristics
2378 citations were found in the initial literature search. 467 duplicates were removed and
1871 citations were excluded as they did not meet the inclusion criteria (Figure 1). The final
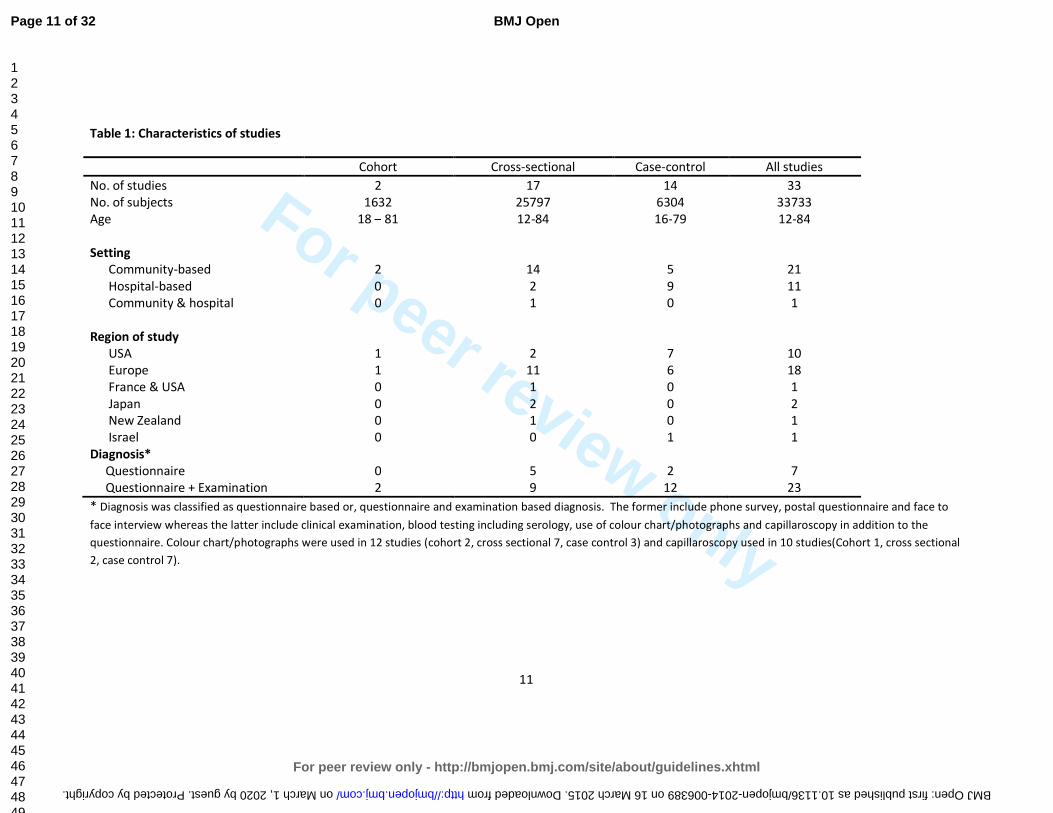
number of studies available for analysis was 33 (33, 733 subjects). There were 2 cohort
studies[17, 18] (1, 632 subjects), 17 cross-sectional studies[6, 19-34] (25, 797 subjects) and
14 case-control studies[7-11, 35-43] (6, 304 subjects) (Table 1). Data for incidence and
prevalence were taken from cohort and cross-sectional studies respectively. Data for risk
factors were taken from all studies as long as the results were reported.
Age ranges across different study designs were as follows: case-control (16-79 years), cohort
(18-81 years), cross sectional (12-84 years). 67% of the studies involved participants
recruited in a community based setting. The majority of studies were conducted in Europe
(18)[6, 9, 17, 20, 22, 24, 25, 27, 28, 30, 31, 33-35, 37, 39-41] or the USA (10)[7-8, 10-11, 18-
19, 21, 36, 38, 42], however other countries of origin included Japan (2)[23, 26], New
Zealand (1)[32] and Israel (1)[43]. One comparison study included participants from USA and
France.[29]
Participants were surveyed by means of phone, face-to-face interview, and/or postal
questionnaire. 26 studies included a physical examination which also included blood testing
(including serology), nail fold capillaroscopy and use of colour chart/photographs (Table 1)
10 studies used specific criteria to define PRP (3 studies Allen & Brown[8, 19, 30], 3 Leroy &
Medsger[9, 34, 35], 4 UK Scleroderma Study Group[6, 20, 31-32]). The remaining studies
Page 9 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
10
used a combination of cold sensitivity, varying degrees of colour change and sensory
symptoms via questionnaire or interview to define PRP. Colour charts or photographs to
indicate colour change were used in 12 studies[6-7, 9-10, 17-18, 23, 26-27, 29, 31, 33] and
nailfold capillaroscopy was performed as part of the examination in 10 studies.[8-9, 17, 29,
34, 35, 37, 39-41] In 15 studies, blood testing including serology and/or inflammatory
markers were performed.[6, 8-9, 11, 22, 28, 31, 34-35, 37-42]
Page 10 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
11
Table 1: Characteristics of studies
Cohort Cross-sectional Case-control All studies
No. of studies 2 17 14 33
No. of subjects 1632 25797 6304 33733
Age 18 – 81 12-84 16-79 12-84
Setting
Community-based 2 14 5 21
Hospital-based 0 2 9 11
Community & hospital 0 1 0 1
Region of study
USA 1 2 7 10
Europe 1 11 6 18
France & USA 0 1 0 1
Japan 0 2 0 2
New Zealand 0 1 0 1
Israel 0 0 1 1
Diagnosis*
Questionnaire 0 5 2 7
Questionnaire + Examination 2 9 12 23
* Diagnosis was classified as questionnaire based or, questionnaire and examination based diagnosis. The former include phone survey, postal questionnaire and face to
face interview whereas the latter include clinical examination, blood testing including serology, use of colour chart/photographs and capillaroscopy in addition to the
questionnaire. Colour chart/photographs were used in 12 studies (cohort 2, cross sectional 7, case control 3) and capillaroscopy used in 10 studies(Cohort 1, cross sectional
2, case control 7).
Page 11 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
12
2: Prevalence of PRP
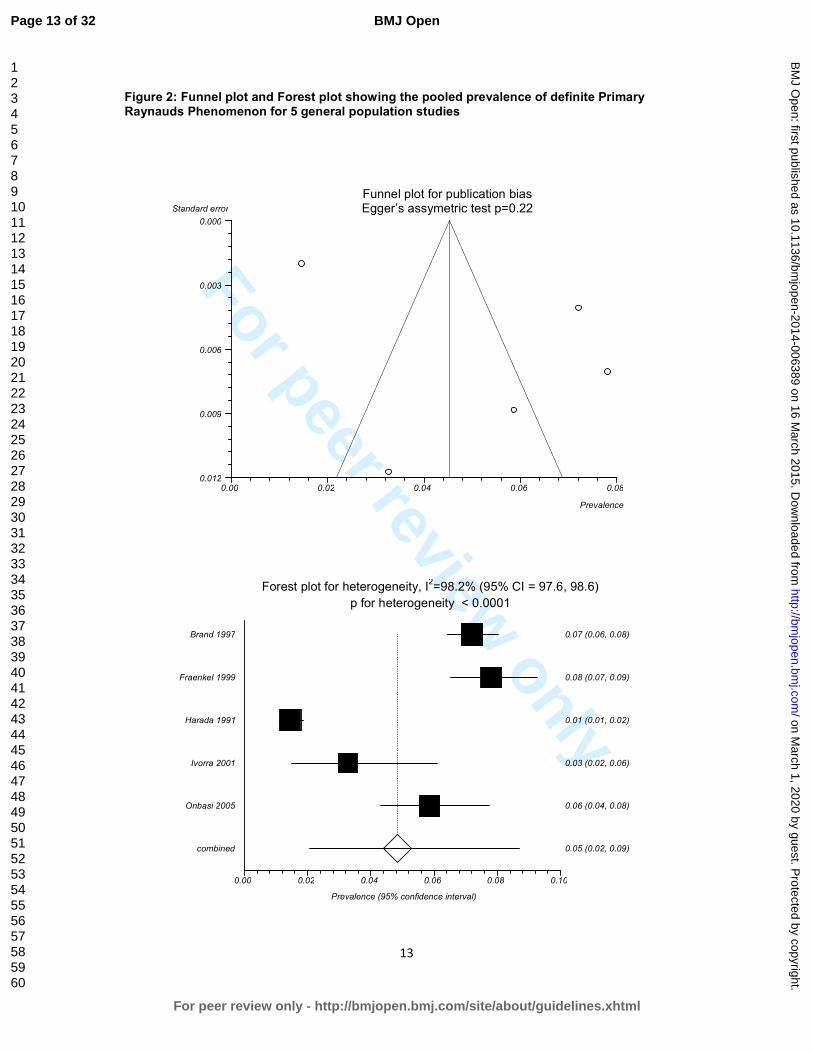
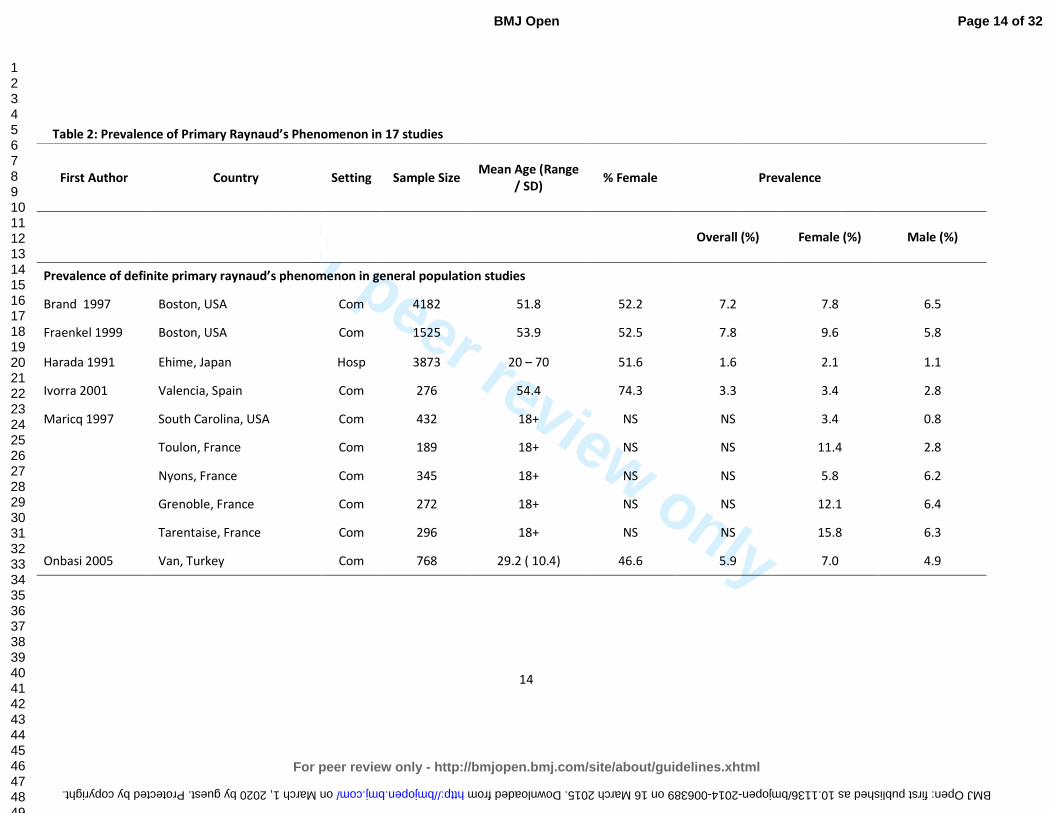
The overall prevalence for definite PRP varied from 1.6 – 7.2% in 6 cross sectional studies in
the general population (women: 2.1-15.8% and men 0.8-6.5%).[19, 21, 23, 25, 29, 31] The
pooled prevalence was 4.85% (95% CI 2.08%, 8.71%) (Figure 2), with 5.74% (95% CI 2.74,
9.75) in women and 4.12% (95% CI 1.60, 7.74) in men.
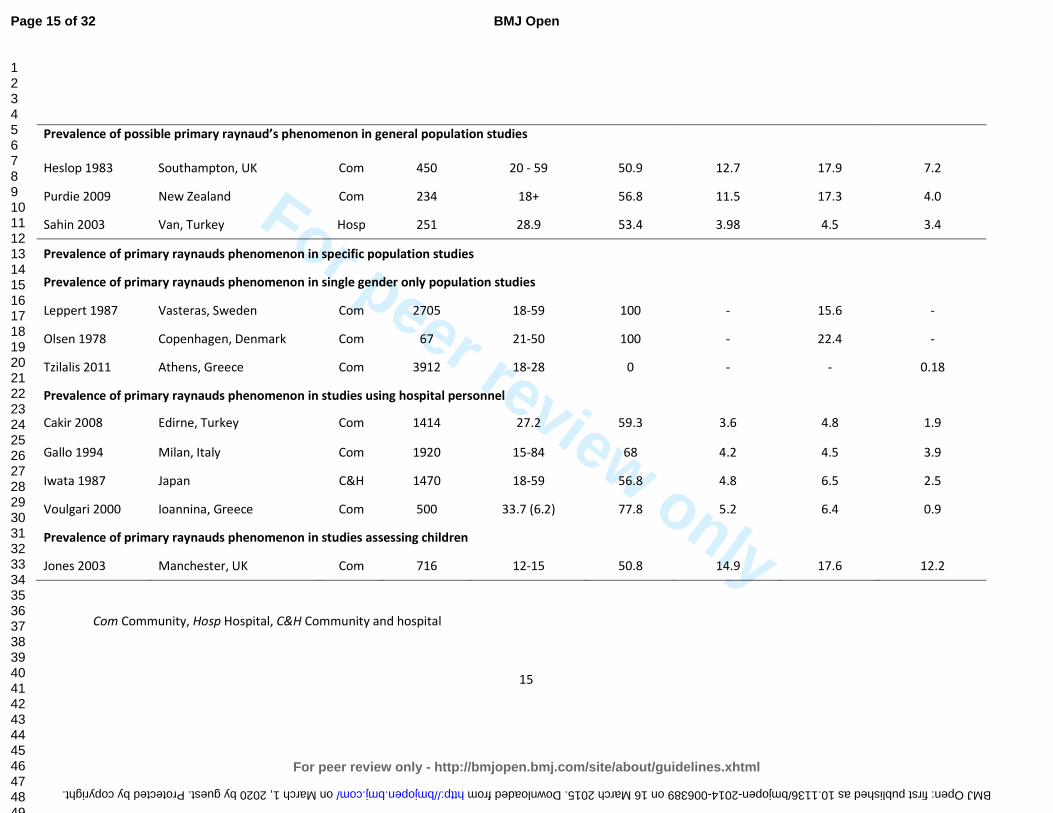
The overall prevalence for possible PRP ranges from 3.98% to 12.7% (women: 4.5-17.9% and
men: 3.4-7.2%) in three cross sectional studies.[24, 32-33] The prevalence in specific
populations varies depending on the studies (Table 2)
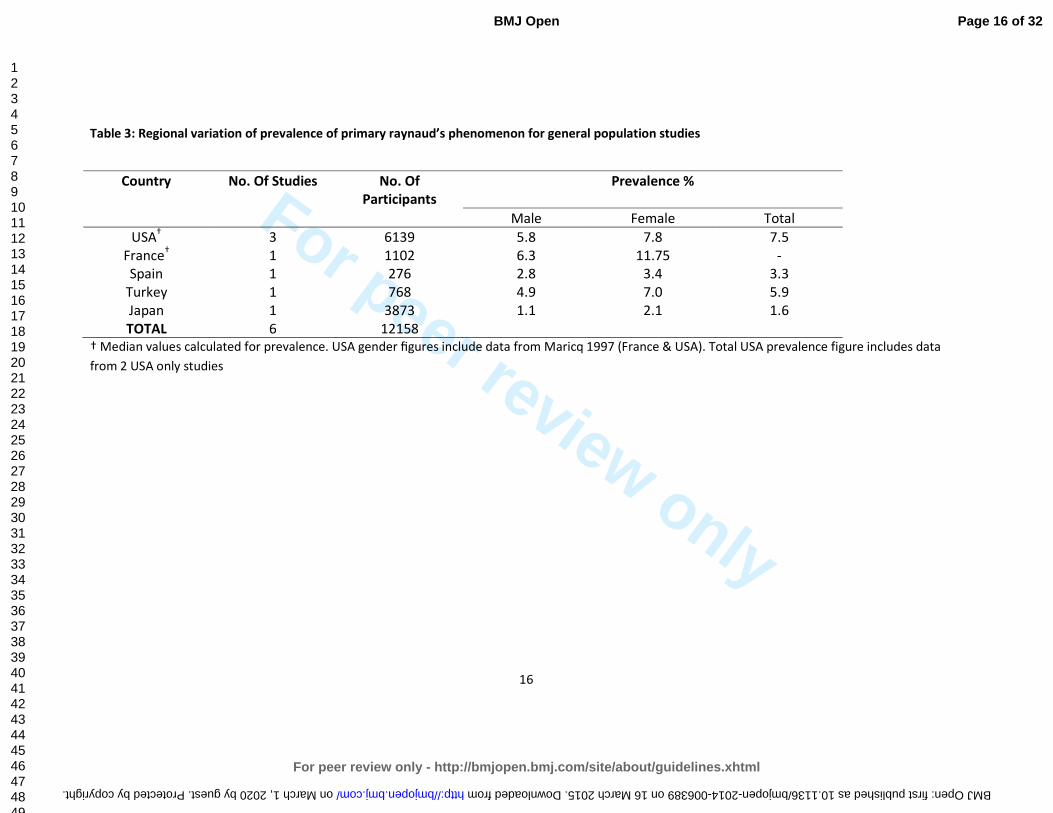
In 6 studies assessing the general population we found the lowest prevalence of PRP in
Japan with an overall prevalence of 1.6 (2.1% in women, 1.1% in men).[23] Highest overall
prevalence figures were found in the USA with a median prevalence of 7.5% (7.8% in
women, 5.8% in men,).[19, 21] A study from France also showed high prevalence figures of
11.75% in women and 6.5% in men (median values).[29] (Table 3)
Five studies reported prevalence of PRP by age.[6, 26-28, 32] Leppert (1987) reported that
prevalence in 4 age bands 18-29, 30-39, 40-49 and 50-59 were 11%, 16%, 14% and 16%
respectively. The other four other studies (Iwata (1987), Voulgari (2000) Purdie (2009) and
Jones (2003) also failed to find any increase or decrease in PRP with age.
Page 12 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
13
Figure 2: Funnel plot and Forest plot showing the pooled prevalence of definite Primary Raynauds Phenomenon for 5 general population studies
Funnel plot for publication bias Egger’s assymetric test p=0.22
0.00 0.02 0.04 0.06 0.080.012
0.009
0.006
0.003
0.000
Prevalence
Standard error
Forest plot for heterogeneity, I2=98.2% (95% CI = 97.6, 98.6)
p for heterogeneity < 0.0001
0.00 0.02 0.04 0.06 0.08 0.10
combined 0.05 (0.02, 0.09)
Onbasi 2005 0.06 (0.04, 0.08)
Ivorra 2001 0.03 (0.02, 0.06)
Harada 1991 0.01 (0.01, 0.02)
Fraenkel 1999 0.08 (0.07, 0.09)
Brand 1997 0.07 (0.06, 0.08)
Prevalence (95% confidence interval)
Page 13 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
14
Table 2: Prevalence of Primary Raynaud’s Phenomenon in 17 studies
First Author Country Setting Sample Size
Mean Age (Range
/ SD)
% Female
Prevalence
Overall (%)
Female (%) Male (%)
Prevalence of definite primary raynaud’s phenomenon in general population studies
Brand 1997 Boston, USA Com 4182 51.8 52.2 7.2 7.8 6.5
Fraenkel 1999 Boston, USA Com 1525 53.9 52.5 7.8 9.6 5.8
Harada 1991 Ehime, Japan Hosp 3873 20 – 70 51.6 1.6 2.1 1.1
Ivorra 2001 Valencia, Spain Com 276 54.4 74.3 3.3 3.4 2.8
Maricq 1997 South Carolina, USA Com 432 18+ NS NS 3.4 0.8
Toulon, France Com 189 18+ NS NS 11.4 2.8
Nyons, France Com 345 18+ NS NS 5.8 6.2
Grenoble, France Com 272 18+ NS NS 12.1 6.4
Tarentaise, France Com 296 18+ NS NS 15.8 6.3
Onbasi 2005 Van, Turkey Com 768 29.2 ( 10.4) 46.6 5.9 7.0 4.9
Page 14 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
15
Prevalence of possible primary raynaud’s phenomenon in general population studies
Heslop 1983 Southampton, UK Com 450 20 - 59 50.9 12.7 17.9 7.2
Purdie 2009 New Zealand Com 234 18+ 56.8 11.5 17.3 4.0
Sahin 2003 Van, Turkey Hosp 251 28.9 53.4 3.98 4.5 3.4
Prevalence of primary raynauds phenomenon in specific population studies
Prevalence of primary raynauds phenomenon in single gender only population studies
Leppert 1987 Vasteras, Sweden Com 2705 18-59 100 - 15.6 -
Olsen 1978 Copenhagen, Denmark Com 67 21-50 100 - 22.4 -
Tzilalis 2011 Athens, Greece Com 3912 18-28 0 - - 0.18
Prevalence of primary raynauds phenomenon in studies using hospital personnel
Cakir 2008 Edirne, Turkey Com 1414 27.2 59.3 3.6 4.8 1.9
Gallo 1994 Milan, Italy Com 1920 15-84 68 4.2 4.5 3.9
Iwata 1987 Japan C&H 1470 18-59 56.8 4.8 6.5 2.5
Voulgari 2000 Ioannina, Greece Com 500 33.7 (6.2) 77.8 5.2 6.4 0.9
Prevalence of primary raynauds phenomenon in studies assessing children
Jones 2003 Manchester, UK Com 716 12-15 50.8 14.9 17.6 12.2
Com Community, Hosp Hospital, C&H Community and hospital
Page 15 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
16
Table 3: Regional variation of prevalence of primary raynaud’s phenomenon for general population studies
Country No. Of Studies No. Of
Participants
Prevalence %
Male Female Total
USA† 3 6139 5.8 7.8 7.5
France† 1 1102 6.3 11.75 -
Spain 1 276 2.8 3.4 3.3
Turkey 1 768 4.9 7.0 5.9
Japan 1 3873 1.1 2.1 1.6
TOTAL 6 12158
† Median values calculated for prevalence. USA gender figures include data from Maricq 1997 (France & USA). Total USA prevalence figure includes data
from 2 USA only studies
Page 16 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
17
3: Incidence of Primary Raynauds Phenomenon
Only two studies reported incidence rates.[17-18] Carpentier et al reported an annual
incidence rate of 0.25% (95% CI 0.17, 0.33), with 0.24% in women and 0.26% in men and
Suter et al reported a 7-year incidence of 1.87% (2.2% in women and, 1.5% in men). Neither
study provided 95%CIs.
4: Risk factors and associations
In 18 studies (23, 197 participants), there was a positive association between female gender
and PRP (OR 1.65, 95% CI 1.42, 1.91).[6-7, 9, 18-27, 31-33, 35, 42] Family history, assessed in
2 studies looking at 1st degree relatives, also had a positive significant association with PRP
(OR 16.6, 95%CI 7.44, 36.8).[8-9] No significant association was found with education
beyond primary school age.[6, 35] (Table 4). Manual occupation (not including vibration
tool use) had an OR of 2.66 (95% CI 1.73, 4.08) in 1 study of 3873 participants.[23] In 4
studies, marriage had an OR of 0.60 (95% CI 0.43, 0.83).[6-7, 21, 35] Smoking was found to
have an association in 9 studies giving a pooled OR of 1.27 (95% CI 1.06, 1.53).[7, 9-11, 18,
20-21, 30, 42] Alcohol use,[21, 42] participants with positive Helicobacter Pylori
investigations[37, 39] and those with conditions such as diabetes,[21] hypertension[11, 21]
and hypercholesterolaemia[21] did not have a significant association with PRP.
Migraine had a positive significant association with a pooled OR of 4.02 (95% CI 2.62, 6.17)
in 6 studies.[6, 9-11, 20, 43] One study of 3442 participants reported a positive association
of cardiovascular disease with PRP with an OR of 1.69 (95% CI 1.22, 2.34).[42]
Cardiovascular disease in this study included a history of ischaemic heart disease,
Page 17 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
18
intermittent claudication, congestive cardiac failure and cerebrovascular disease. A single
study using 81 participants did not show a positive significant association of coronary heart
disease with PRP.[38]
A positive association was found in participants taking oestrogen replacement therapy alone
in two studies with an OR of 2.34 (95% CI 1.42, 3.84).[21, 36] However no significant
association was found in combined oestrogen and progesterone replacement therapy[36] in
postmenopausal women or in oral contraceptive pill[10-11] use in two other studies. A
study by Smyth et al looking at allele frequencies of known polymorphisms of candidate
vasoactive mediator genes (eNOS, BKRG, ET01 and ETA receptor genes) did not show any
association.[9] Shemirani et al looked at clotting factors in participants with PRP and found a
significant association with methyltetrahydrofolate reductase C677T mutations (OR 0.4, 95%
CI 0.2, 0.9) but no difference in other thrombosis-associated alleles (FVLeiden, prothrombin
G20210A).[40]
Page 18 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
19
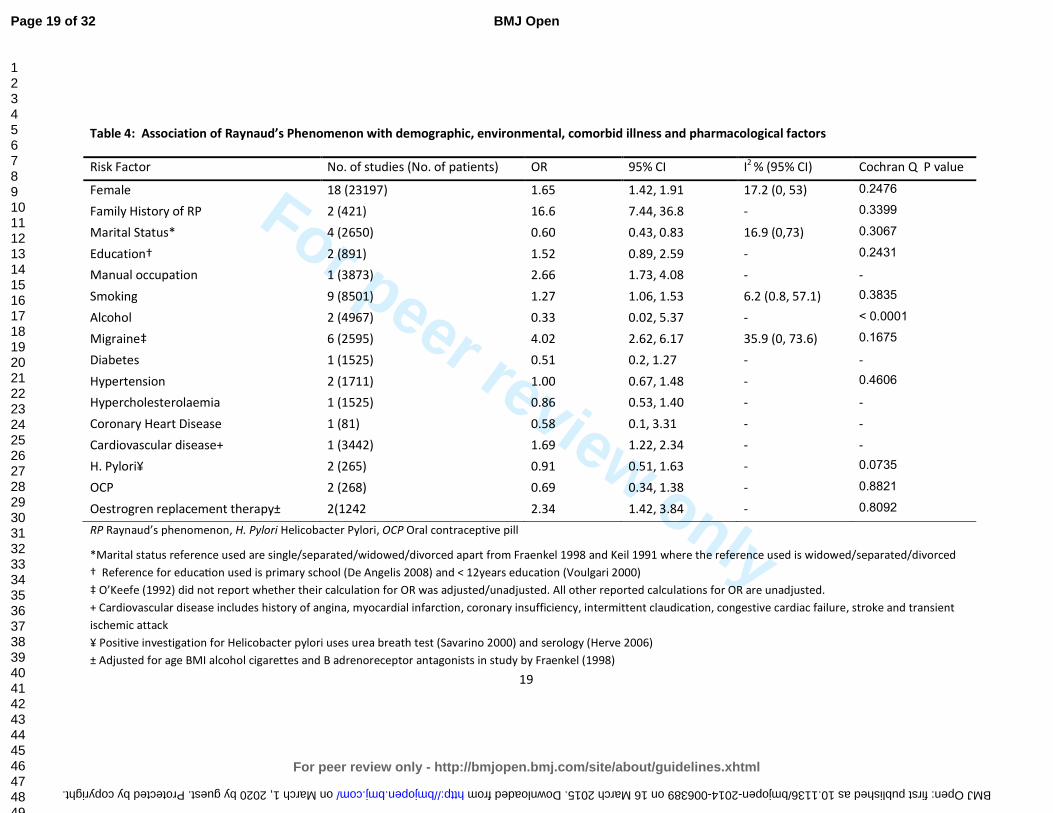
Table 4: Association of Raynaud’s Phenomenon with demographic, environmental, comorbid illness and pharmacological factors
Risk Factor No. of studies (No. of patients) OR 95% CI I2
% (95% CI)
Cochran Q P value
Female 18 (23197) 1.65 1.42, 1.91 17.2 (0, 53) 0.2476
Family History of RP 2 (421) 16.6 7.44, 36.8 - 0.3399
Marital Status* 4 (2650) 0.60 0.43, 0.83 16.9 (0,73) 0.3067
Education† 2 (891) 1.52 0.89, 2.59 - 0.2431
Manual occupation 1 (3873) 2.66 1.73, 4.08 - -
Smoking 9 (8501) 1.27 1.06, 1.53 6.2 (0.8, 57.1) 0.3835
Alcohol 2 (4967) 0.33 0.02, 5.37 - < 0.0001
Migraine‡ 6 (2595) 4.02 2.62, 6.17 35.9 (0, 73.6) 0.1675
Diabetes 1 (1525) 0.51 0.2, 1.27 - -
Hypertension 2 (1711) 1.00 0.67, 1.48 - 0.4606
Hypercholesterolaemia 1 (1525) 0.86 0.53, 1.40 - -
Coronary Heart Disease 1 (81) 0.58 0.1, 3.31 - -
Cardiovascular disease+ 1 (3442) 1.69 1.22, 2.34 - -
H. Pylori¥ 2 (265) 0.91 0.51, 1.63 - 0.0735
OCP 2 (268) 0.69 0.34, 1.38 - 0.8821
Oestrogren replacement therapy± 2(1242 2.34 1.42, 3.84 - 0.8092
RP Raynaud’s phenomenon, H. Pylori Helicobacter Pylori, OCP Oral contraceptive pill
*Marital status reference used are single/separated/widowed/divorced apart from Fraenkel 1998 and Keil 1991 where the reference used is widowed/separated/divorced
† Reference for educaXon used is primary school (De Angelis 2008) and < 12years education (Voulgari 2000)
‡ O’Keefe (1992) did not report whether their calculation for OR was adjusted/unadjusted. All other reported calculations for OR are unadjusted.
+ Cardiovascular disease includes history of angina, myocardial infarction, coronary insufficiency, intermittent claudication, congestive cardiac failure, stroke and transient
ischemic attack
¥ Positive investigation for Helicobacter pylori uses urea breath test (Savarino 2000) and serology (Herve 2006)
± Adjusted for age BMI alcohol cigarettes and B adrenoreceptor antagonists in study by Fraenkel (1998)
Page 19 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
20
DISCUSSION
This is the first meta-analysis of the literature for the prevalence, incidence, risk factors and
associations of PRP. Overall the pooled mean prevalence of PRP in the general population
was 4.85% (95% CI 2.08%, 8.71%) (Figure 2) and the mean incidence was 0.25% (95% CI
0.17, 0.33) per annum.[17] Major risk factors/associations of PRP include female gender,
family history of PRP, migraine, smoking, cardiovascular disease, manual occupation,
oestrogren replacement therapy and possibly marital status. (Table 4).
Variations in prevalence were observed between countries (Table 3) though this could
reflect use of different diagnostic criteria rather than real differences in prevalence. Almost
all studies demonstrate a higher prevalence of PRP in women. This may be due to a
relationship with female hormones as two studies found an association between PRP and
use of oestrogen replacement therapy alone,[21, 36] although no association was found
between combined oestrogen and progesterone replacement or the oral contraceptive
pill.[10-11, 36] In contrast, prevalence of PRP does not increase with age in all published
studies with a wide age range of participants from 12 years up to 84 years. This accords
with the clinical observation that PRP usually starts in teenage years and that later
development, which is far less common, is characteristic of secondary RP. While the former
may be driven predominantly by genetic risk factors, later onset “primary” Raynaud’s may
be predominantly influenced by environmental exposures such as vascular microtrauma
from manual usage and vibrating tools. In terms of other environmental factors we did find
a weak negative association between marital status and PRP with an OR of 0.60 (95%CI 0.43,
Page 20 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
21
0.83) in those that are married vs. single/separated/widowed/divorced.[6-7, 21, 35]
However, there is no plausible biological explanation for this and the reported data may not
be free from confounding bias.
The association of cardiovascular disease and autoimmune disease is well documented and
thought to be due to accelerated atherosclerosis as a result of chronic inflammation,
treatment such as glucocorticoids as well as the traditional risk factors for cardiovascular
disease.[44-50] A link between cardiovascular disease and PRP has been shown in only one
study[42] and a reason for this association is not known. It is unlikely to be due to an
inflammatory process or related to medication and with PRP having predominance for the
female population and onset at a young age it not clear if traditional cardiovascular risk
factors play a part. However, smoking was found to have positive association with PRP in
our study (OR 1.27, 95% CI 1.06, 1.53). It is well known that smoking is one of three
(smoking, hypertension and hyperlipidaemia) main risk factors for cardiovascular and
cerebrovascular disease.[51-57] Smoking may be the same risk factor for PRP and CVD.
Whether smoking causes PRP first then CVD is an interesting question which deserves
further research. More interestingly, we found a very strong association between migraine
and PRP (OR 4.02, 95%CI 2.62, 6.17). It has been previously shown that migraine is due to a
cascade of vascular and neural events.[44-45] However, a review by Rosamund suggested
migraine was not shown to be linked with coronary heart disease but possibly shares a
common underlying pathophysiology with Raynaud’s phenomenon and other vasospastic
disorders such as variant angina.[58-59] It is thought there may be other factors that may
affect the underlying mechanism for these vasospastic conditions as episodes occur at
different times with differing precipitants.[60-61] Further study may help clarify whether
Page 21 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
22
PRP is a benign vasospastic disorder or whether there is underlying pathology affecting the
vascular wall associated with traditional risk factors seen in cardiovascular disease.
There are number of caveats to this study. Firstly, it was striking that there was no uniform
definition for diagnosis of PRP. Only 39% of studies looking at prevalence had a precise
definition for PRP, thereby reducing the number of studies we used to assess pooled
prevalence. We feel that an amalgamation of the generally more commonly used definitions
would ensure that the diagnosis is clear by assessing symptoms, using colour chart or
photographs for confirmation of colour change and carefully exclude underlying conditions
including checking for digital infarcts/ulceration, nailfold capillaroscopy and assessing
autoimmune screen and inflammatory markers. Secondly, as our objective was to
specifically examine the epidemiology of PRP a large proportion of studies were excluded
because they focused on secondary Raynaud’s phenomenon, especially related to
connective tissue diseases and vibration white finger. In addition we also excluded studies
that looked at investigation or treatment of PRP. This left only a small number of studies to
assess. From the studies included, there was a great deal of variation in the population of
participants used. 9 out of the 17 studies used investigated participants in the general
population whereas the remainder examined specific populations such as single gender,
children or hospital/medical personnel. Furthermore, there was considerable variation in
the risk factors addressed in each study and this may have affected the significance and
association, or lack of association between the risk factors and PRP. We tried to extract as
many risk factors from each study as possible to use in our analysis. In the future, a larger
multinational population study may help us to get a better understanding of the disease.
This would be particularly useful if standardised criteria were used to include participants in
Page 22 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
23
the studies, using strict definition for PRP (as mentioned previously) and data was collected
in a similar fashion assessing a wide variety of possible risk factors (particularly related to
cardiovascular disease and vasospastic disoders) for more accurate data analysis.
CONCLUSION
This first systematic review summarises the burden of PRP in the general population using
published literature. It is not a rare condition (prevalence 4.85% and annual incidence
0.25%). It starts at a young age, is more common in women and associates with a family
history and with smoking. In addition, people with PRP are 4 times more likely to have
migraine than those without this condition.
ACKNOWLEDGEMENT: Our sincere thank you to Joanna Ramowski and Helen Richardson for
article retrieval and support. Also special thank you to Anu Suokas, Karin Tatsumoa,
Professor Tiraje Truncer, Ana Valdes and Maggie Wheeler for language translation.
AUTHOR CONTRIBUTIONS
Study conception and design: Dr Zhang, Professor Doherty, Dr Lanyon, Dr Garner
Acquision of data: Dr Garner, Dr Kumari, Dr Zhang
Statistical Analysis: Dr Garner, Dr Zhang
Analysis and interpretation of data: Dr Garner, Dr Zhang, Professor Doherty, Dr Lanyon
Page 23 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
24
Manuscript preparation and final approval of manuscript: Dr Garner, Dr Zhang, Professor
Doherty, Dr Lanyon
Funding No funding
Competing interests None
Ethical approval and patient consent Not required
Data sharing statement No unpublished data were used in this study. No additional data
available.
Page 24 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
25
REFERENCES
1 Allen E, Brown G. Raynaud disease: A critical review of minimal requisites for diagnosis. Am J Med
Sci 1932;183(2):187-200.
2 LeRoy E, Medsger T. Raynaud’s phenomenon: a proposal for classification. Clin Exp Rheumatol
1992;10:485-488.
3 Bowling J, Dowd P. Raynaud’s disease. Lancet 2003;361:2078-80.
4. Brennan P, Silman A, Black C, et al. Validity and reliability of three methods used in the diagnosis
of Raynaud's phenomenon. The UK Scleroderma Study Group. Br J Rheumatol 1993;32(5):357-61.
5 Maricq H, Weinrich M. Diagnosis of Raynaud’s phenomenon assisted by colour charts. J Rheumatol
1988;15(3):454-459.
6 Voulgari P, Alamanos Y, Papazisi D, et al. Prevalence of Raynaud's phenomenon in a healthy Greek
population. Ann Rheum Dis 2000;59(3):206-210.
7 Keil J, Maricq H, Weinrich M, et al. Demographic, social and clinical correlates of Raynaud
phenomenon. Int J Epidemiol 1991;20(1):221-224.
8 Freedman R, Mayes M. Familial aggregation of primary Raynaud's disease. Arthritis and
Rheumatism 1996;39(7):1189-1191.
9 Smyth AE, Hughes AE, Bruce IN, Bell AL. A case-control study of candidate vasoactive mediator
genes in primary Raynaud's phenomenon. Rheumatology (Oxford) 1999;38(11):1094-1098.
10 O'Keeffe S, Tsapatsaris N, Beetham W. Association between Raynaud's phenomenon and
migraine in a random population of hospital employees. J Rheumatol 1993;20(7):1187-1188.
11 O'Keeffe S, Tsapatsaris N, Beetham W. Increased prevalence of migraine and chest pain in
patients with primary Raynaud disease. Ann Intern Med 1992;116(12 Pt 1):985-989.
12 Stroup D, Berlin J, Morton S, et al. Meta-analysis of Observational Studies in Epidemiology
(Moose) group. JAMA 2000;283:2008-2012.
13 Whitehead A, Whitehead J. A general parametric approach to the meta-analysis of randomised
clinical trials. Stat Med 1991;10:1665-77.
14 Gavaghan D, Moore R, McQuay H. An evaluation of homogeneity tests in meta-analyses in pain
using simulations of individual patient data. Pain 2000;85:415-24.
15 Higgins J, Thomspon S, Deeks J, et al. Measuring inconsistency in meta-anlyses. BMJ
2003;327:557-60.
16 Egger M, Davey Smith G, Schneider M, et al. Bias in meta-anlysis detected by a simple, graphical
test. BMJ 1997;315:629-34.
17 Carpentier P, Satger B, Poensin D, et al. Incidence and natural history of Raynaud phenomenon: a
long-term follow-up (14 years) of a random sample from the general population. J Vasc Surg 2006;
44(5):1023-1028.
18 Suter L, Murabito J, Felson D, et al. The incidence and natural history of Raynaud's phenomenon
in the community. Arthritis Rheum 2005; 52(4):1259-1263.
19 Brand F, Larson M, Kannel W, et al. The occurrence of Raynaud's phenomenon in a general
population: the Framingham Study. Vasc Med 1997;2(4):296-301.
20 Cakir N, Pamuk O, Donmez S, et al. Prevalence of Raynaud's phenomenon in healthy Turkish
medical students and hospital personnel. Rheumatol Int 2008; 29(2):185-188.
21 Fraenkel L, Zhang Y, Chaisson C F et al. Different factors influencing the expression of raynaud's
phenomenon in men and women. Arthritis Rheum 1999;42(2):306-310.
22 Gallo E, Bianchi E, Motta A, et al. [The incidence of Raynaud's phenomenon in 1920 residents in
Milan]. [Italian] Incidenza del fenomeno di Raynaud in 1920 residenti in Milano. Minerva
Cardioangiol 1994;42(1-2):65-71.
Page 25 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
26
23 Harada N, Ueda A, Takegata S. Prevalence of Raynaud's phenomenon in Japanese males and
females. J Clin Epidemiol 1991;44(7):649-655.
24 Heslop J, Coggon D, Acheson E. The prevalence of intermittent digital ischaemia (Raynaud's
phenomenon) in a general practice. J R Coll Gen Pract 1983;33(247):85-89.
25 Ivorra J, Perales J, Carballido C, et al. Prevalence of Raynaud's phenomenon in general practice in
the East of Spain. Clin Rheumatol 2001;20(2):88-90.
26 Iwata H, Makimo S, Miyashita K. [Prevalence of Raynaud's phenomenon in individuals not using
vibrating tools]. Sangyo Igaku - Japanese Journal of Industrial Health 1987;29(6):500-503.
27 Jones G, Herrick A, Woodham S, et al. Occurrence of Raynaud's Phenomenon in Children Ages 12-
15 Years: Prevalence and Association with Other Common Symptoms. Arthritis Rheum
2003;48(12):3518-352.
28 Leppert J, Aberg H, Ringqvist I, et al. Raynaud's phenomenon in a female population: prevalence
and association with other conditions. Angiology 1987;38(12):871-877.
29 Maricq H, Carpentier P, Weinrich M, et al. Geographic variation in the prevalence of Raynaud's
phenomenon: A 5 region comparison. J Rheumatol 1997;24(5):879-889.
30 Olsen N, Nielsen S. Prevalence of primary Raynaud phenomena in young females. Scand J Clin Lab
Invest 1978;38(8):761-764.
31 Onbasi K, Sahin I, Onbasi O, et al. Raynaud's phenomenon in a healthy Turkish population. Clin
Rheumatol 2005;24(4):365-369.
32 Purdie G, Harrison A, Purdie D. Prevalence of Raynaud's phenomenon in the adult New Zealand
population. N Z Med J 2009;122(1306):55-62.
33 Sahin I, Onbasi K, Onbasi O, et al. Raynaud's Phenomenon in Healthy Population Who Admitted to
the Hospital in Van Region, Turkey [Turkish] Van Yoresinde Hastaneye Basvuran Saglikli
Populasyonda Raynaud Fenomeni. Ondokuz Mayis Universitesi Tip Dergisi 2003;20(2):73-77.
34 Tzilalis V, Panagiotopoulos N, Papatheodorou G, et al. Prevalence of Raynaud's phenomenon in
young Greek males. Clin Rheumatol 2011;30(1):57-59.
35 De Angelis R, Salaffi F, Grassi W. Health-related quality of life in primary Raynaud phenomenon. J
Clin Rheumatol 2008;14(4):206-210.
36 Fraenkel L, Zhang Y, Chaisson C, et al. The association of estrogen replacement therapy and the
Raynaud phenomenon in postmenopausal women. Ann Intern Med 1998;129(3):208-212.
37 Herve F, Cailleux N, Benhamou Y, et al. [Helicobacter pylori prevalence in Raynaud's disease].
[French] Prevalence des infections a Helicobacter pylori au cours de la maladie de Raynaud. Revue
de Medecine Interne 2006;27(10):736-741.
38 Koh K, Kim S, Lee K, et al. Does prevalence of migraine and Raynaud's phenomenon also increase
in Korean patients with proven variant angina? Int J Cardiol 1995; 51(1):37-46.
39 Savarino V, Sulli A, Zentilin P, et al. No evidence of an association between Helicobacter pylori
infection and Raynaud phenomenon. Scand J Gastroenterol 2000;35(12):1251-1254.
40 Shemirani A, Szomjak E, Balogh E, et al. Polymorphism of clotting factors in Hungarian patients
with Raynaud's. Blood Coagul Fibrinolysis 2011;22(1):56-59.
41 Susol E, MacGregor A, Barrett J, et al. A two-stage, genome-wide screen for susceptibility loci in
primary Raynaud's phenomenon. Arthritis Rheum 2000;43(7):1641-1646.
42 Suter L, Murabito J, Felson D, et al. Smoking, Alcohol Consumption, and Raynaud's Phenomenon
in Middle Age. Am J Med 2007;120(3):264-271.
43 Zahavi I, Chagnac A, Hering R, et al. Prevalence of Raynaud's phenomenon in patients with
migraine. Arch Intern Med 1984;144(4):742-744.
44 Shoenfeld Y, Gerli R, Doria A, et al. Accelerated atherosclerosis in autoimmune rheumatic
diseases. Circulation. 2005;112: 3337–3347.
45 Tyrrell P, Beyene J, Feldman B, et al. Rheumatic Disease and Carotid Intima-Media Thickness: A
Systematic Review and Meta-Analysis. Arterioscler Thromb Vasc Biol 2010;30:1014-1026.
Page 26 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
27
46 Schoenfeld S, Kasturi S, Costenbader K. The epidemiology of atherosclerotic cardiovascular
disease among patients with SLE: a systematic review. Semin Arthritis Rheum 2013:43(1):77-95 doi:
10.1016/j.semarthrit.2012.12.002. [published Online First 17 February 2013].
47 Peters M, Symmons D, McCarey D, et al. EULAR evidence-based recommendations for
cardiovascular risk management in patients with rheumatoid arthritis and other forms of
inflammatory arthritis. Ann Rheum Dis 2010;69: 325-331 doi: 10.1136/ard.2009.113696. [Published Online
First 22 September 2009].
48 Gabriel S, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and
comorbidity of the rheumatic diseases. Arthritis Res Ther 2009;11(3):229 doi: 10.1186/ar2669.
[published Online First 19 May 2009].
49 Lévy L, Fautrel B, Barnetche T, et al. Incidence and risk of fatal myocardial infarction and stroke
events in rheumatoid arthritis patients. A systematic review of the literature. Clin Exp Rheumatol
2008;26:673-9.
50 Avina-Zubieta J, Choi H, Sadatsafavi M, et al. Risk of cardiovascular mortality in patients with
rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum 2008;59:1690-7.
51 Burns D. Epidemiology of smoking-induced cardiovascular disease. Prog Cardiovasc
Dis. 2003;46(1):11-29.
52 De Backer G. Risk factors and prevention of cardiovascular disease: A review. Dialogues in
Cardiovascular Medicine 2008;13(2):83-99.
53 O’Donnell M, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic
stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010:376(9735):112-
123.
54 JBS3 Board. Joint British Societies’ consensus recommendations for the prevention of
cardiovascular disease (JBS3) Heart 2014;100(Suppl 2)::ii1–ii67.
55 British Cardiac Society, British Hyperlipidaemia Association, British Hypertension Society,
endorsed by the British Diabetic Association. Joint British recommendations on prevention of
coronary heart disease in clinical practice. Heart 1998;80(Suppl 2):S1–29.
56 Joint British Societies. JBS 2: Joint British Societies’ guidelines on prevention of
cardiovascular disease in clinical practice. Heart 2005;91(Suppl 5):v1–52.
57 Goff D, Lloyd-Jones D, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of
cardiovascular risk: a report of the American College of Cardiology/American Heart Association task
force on practice guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2935-59.
58 Gasparini C, Sutherland H, Griffiths L. Studies on the pathophysiology and genetic basis of
migraine. Curr Genomics 2013; 14:300-315.
59 Lipton R, Bigal M. Migraine: Epidemiology, impact and risk factors for progression. Headache
2005;45[Suppl 1]:S3-S13.
60 Rosamond W. Are migraine and coronary heart disease associated? An epidemiologic review.
Headache 2004; 44[Suppl 1]:S5-S12.
61 Miller D, Waters D, Warnica W, et al. Is variant angina the coronary manifestation of generalised
vasospastic disorder? N Engl J Med 1981;304:763-766.
Page 27 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
Supplementary file
Appendix 1: Medline/Embase/Cinahl/AMED search strategy
Any field
No limitations
1: Randomised control trial (exploded)
2: Double blind (exploded)
3: Single blind (exploded)
4: Placebo (exp)
5: Comparative study (exp)
6: 1 OR 2 OR 3 OR 4 OR 5
7: meta-analysis or systematic review
8: metanalysis exp
9: quantitative review
10: quantitative overview
11: statistical pool
12: 7 or 8 or 9 or 10 or 11
13: Cohort studies exp
14: cohort stud
15: exp prospective studies
16: prospective stud
17: relative risk
18: incidence exp
19: 13 or 14 or 15 or 16 or 17 or 18
20: exp case- control studies
21: case control stud
22: exp retrospective studies
23: retrospective stud
24: exp odds ratio
25: odds ratio
26: 20 or 21 or 22 or 23 or 24 or 25
27: exp cross sectional
28: cross sectional
29: exp risk
30: prevalence exp
31: 27 or 28 or 29 or 30
32: Raynaud Disease
33: Raynaud
34: 32 or 33
35: Epidemiology
36: 19 or 26 or 31 or 35
37: 34 and 36 (incidence or risk or prevalence or epidemiology) and raynauds
38: 32 and 35 (raynauds and epidemiology)
39: 30 and 32 ( prevalence and raynaud disease)
40: 18 and 32 (incidence and raynaud disease)
41: 12 and 33 (systematic review and raynauds disease)
42: 6 and 32 (RCT and Raynauds disease)
Page 28 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
PubMed search strategy
#43 Search (#6) AND #33 RCT and Raynauds disease
#42 Search (#12) AND #33 systematic review and raynauds disease
#41 Search (#18) AND #33 incidence and raynaud disease
#40 Search (#30) AND #33 prevalence and raynaud disease
#39 Search (#33) AND #36 raynauds and epidemiology
#38 Search (#35) AND #37 (incidence or risk or prevalence or epidemiology) and raynauds #37 Search (((#19) OR #26) OR #31) OR #36 #36 Search Epidemiology #35 Search (#33) OR #34 #34 Search Raynaud #33 Search Raynauds Disease #31 Search (((#27) OR #28) OR #29) OR #30 #30 Search prevalence #29 Search risk #28 Search "cross sectional"[All Fields] #27 Search cross sectional #26 Search (((((#20) OR #21) OR #22) OR #23) OR #24) OR #25 #25 Search "odds ratio"[All Fields] #24 Search odds ratio #23 Search "retrospective studies"[All Fields] #22 Search retrospective studies #21 Search "case control"[All Fields] #20 Search case control #19 Search (((((#13) OR #14) OR #15) OR #16) OR #17) OR #18 #18 Search incidence #17 Search relative risk #16 Search "prospective studies"[All Fields] #15 Search prospective studies #14 Search "cohort studies"[All Fields] #13 Search cohort studies #12 Search ((((#7) OR #8) OR #9) OR #10) OR #11 #11 Search statistical pool #10 Search quantitative overview #9 Search quantitative review #8 Search systematic review #7 Search meta-analysis #6 Search ((((#1) OR #2) OR #3) OR #4) OR #5 #5 Search comparative study #4 Search placebo #3 Search single blind #2 Search double blind #1 Search randomised control trials
Page 29 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
Section/topic # Checklist item Reported on page #
TITLE
Title 1 Identify the report as a systematic review, meta-analysis, or both. 1
ABSTRACT
Structured summary 2 Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number.
3
INTRODUCTION
Rationale 3 Describe the rationale for the review in the context of what is already known. 4
Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS).
4,5
METHODS
Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number.
Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years
considered, language, publication status) used as criteria for eligibility, giving rationale. 6-7
Information sources 7 Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched.
5
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated.
5, Supplementary material – appendix 1
Study selection 9 State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis).
5-7
Data collection process 10 Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators.
7-8
Data items 11 List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made.
Risk of bias in individual studies
12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis.
7-8
Summary measures 13 State the principal summary measures (e.g., risk ratio, difference in means). 7-8
Page 30 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of
consistency (e.g., I2) for each meta-analysis.
8
Page 1 of 2
Section/topic # Checklist item Reported on page #
Risk of bias across studies 15 Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies).
8
Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified.
RESULTS
Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram.
6, 9
Study characteristics 18 For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations.
9-11
Risk of bias within studies 19 Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12).
Results of individual studies 20 For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot.
12-19
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency. 13
Risk of bias across studies 22 Present results of any assessment of risk of bias across studies (see Item 15). 13
Additional analysis 23 Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). 12-19
DISCUSSION
Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers).
20-23
Limitations 25 Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias).
20-23
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research. 20-23
FUNDING
Funding 27 Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review.
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
Page 31 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
For more information, visit: www.prisma-statement.org.
Page 2 of 2
Page 32 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
Prevalence, risk factors and associations of Primary
Raynaud’s Phenomenon: Systematic review and meta-
analysis of observational studies
Journal: BMJ Open
Manuscript ID: bmjopen-2014-006389.R1
Article Type: Research
Date Submitted by the Author: 11-Dec-2014
Complete List of Authors: Garner, Rozeena; Queens Medical Centre, Rheumatology Kumari, Rakesh; Queens Medical Centre, Rheumatology Lanyon, Peter; Nottingham University Hospital, Rheumatology; Queens
Medical Centre, Rheumatology Doherty, Michael ; University of Nottingham, Academic Rheumatology Zhang, Weiya; University of Nottingham, Academic Rheumatology; Nottingham University, Academic Rheumatology
<b>Primary Subject Heading</b>:
Epidemiology
Secondary Subject Heading: Rheumatology
Keywords: RHEUMATOLOGY, EPIDEMIOLOGY, STATISTICS & RESEARCH METHODS
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on M
arch 1, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2014-006389 on 16 March 2015. D
ownloaded from
For peer review only
1
Prevalence, risk factors and associations of Primary Raynaud’s Phenomenon: Systematic 1
review and meta-analysis of observational studies 2
3
Rozeena Garner MBBS MRCP (Rheum) 2, Rakesh Kumari MBBS MD MRCP (Rheum)
2, Peter 4
Lanyon DM FRCP MRCGP DRCOG2, Michael Doherty MA MD FRCP
1, 2, Weiya Zhang BMed 5
MEpi PhD1 6
1Academic Rheumatology, University of Nottingham, UK;
2Department of Rheumatology, 7
Queens Medical Centre, UK 8
9
10
Correspondence to: 11
Dr Weiya Zhang 12
Academic Rheumatology 13
Clinical Sciences Building 14
Nottingham City Hospital 15
Nottingham NG5 1PB 16
UK 17
Telephone: +44 (0)115 823 1756 18
Fax: +44 (0)115 823 1757 19
Page 1 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
2
Email: [email protected] 1
2
Keywords: Primary Raynaud’s phenomenon, prevalence, incidence, risk factors, systematic 3
review 4
Word Count: Abstract: 244, main text: 3133 5
6
Page 2 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
3
Abstract 1
Objective: To systematically review the literature with regard to the prevalence, incidence, 2
risk factors and associations of primary Raynaud’s phenomenon (PRP). 3
Method: A systematic review of the literature of observational studies for PRP was 4
undertaken using five electronic databases. Any studies reporting prevalence, incidence and 5
risk factors of PRP were collected. Relative risk or odds ratio (OR) and 95% confidence 6
interval (CI) were extracted or calculated to present the association between risk factors 7
and PRP. Random effects model was used to pool the results. 8
Results: 33 articles assessing a total of 33, 733 participants were included in this analysis (2 9
cohort, 17 cross-sectional and 14 case-control studies). The pooled prevalence of PRP was 10
4.85% (95% CI 2.08%, 8.71%) in the general population. The pooled annual incidence of PRP 11
was 0.25% (95% CI 0.19, 0.32). Risk factors and associations for PRP included female gender 12
(OR 1.65, 95% CI 1.42, 1.91), family history (OR 16.6, 95% CI 7.44, 36.8), smoking (OR 1.27, 13
95% CI 1.06, 1.53), manual occupation (OR 2.66 95% CI 1.73, 4.08), migraine (OR 4.02, 95% 14
CI 2.62, 6.17), cardiovascular disease (OR 1.69, 95% CI 1.22, 2.34) and marital status 15
(married) (OR 0.60, 95% CI 0.43, 0.83). The definition of PRP varied considerably between 16
studies. 17
Conclusion: This is the first systematic review of the prevalence, incidence, risk factors and 18
associations of PRP. Further study using uniform strict criteria for the condition is required 19
to confirm these findings, particularly the possible association with cardiovascular disease. 20
21
Page 3 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
4
1
Strengths and limitations of this study 2
• This is the first meta-analysis of the literature for the global epidemiology of primary 3
Raynaud’s phenomenon (PRP). 4
• The prevalence and incidence of PRP in different countries were estimated. Female 5
gender, positive family history, smoking and migraines were found to be the major risk 6
factors for PRP. 7
• The lack of original data restricted an adequate estimation of the age-effect on PRP. 8
• Different definitions of PRP handicapped a comparison between countries 9
10
INTRODUCTION 11
In the 19th century, Maurice Raynaud first described Raynaud’s phenomenon (RP) as an 12
episodic, symmetrical, vasospastic disorder resulting in classic triphasic colour change, 13
trophic changes limited to the skin and uncomfortable sensory symptoms of the extremities 14
in the absence of arterial occlusion.[1] Further criteria have been suggested to distinguish 15
Primary RP (PRP) from secondary RP which include detail regarding symptom duration, 16
negative autoimmune serology, normal serum inflammatory markers and capillaroscopy, 17
and the clinical absence of any underlying disease.[1-4] Use of colour charts to aid 18
diagnosis has also been used.[4, 5] Despite this, there is no unifying definition that is used 19
worldwide for PRP. 20
21
There have been a number of studies performed in various countries reporting the 22
prevalence of RP. The reported prevalence ranges from less than 1% (in men) and up to 23
20% (in women) depending on definitions and population selected.[6] In contrast, few 24
studies have examined the incidence of PRP and the true burden of PRP in the general 25
population remains unclear. PRP is thought to be more common in women, particularly 26
when it develops at a young age.[7] There are also reports of a hereditary component and 27
Page 4 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
5
links with other vasospastic conditions such as migraine.[8-11] It is uncertain whether other 1
co-morbidities or risk factors particularly related to vascular diseases such as ischaemic 2
heart disease and/or smoking have an association with PRP. 3
4
The primary objective of this study was to perform a systematic review of observational 5
studies to summarise the literature with regard to the prevalence, incidence and risk 6
factors/associations of PRP. The secondary objective was to examine the current definitions 7
used to define PRP worldwide. 8
METHODS 9
1: Literature search – data sources and search strategy 10
A comprehensive systematic literature search was undertaken in June 2011 and re-run in 11
October 2014 using five databases: Medline, Embase, Cinahl, Amed and Pubmed. The 12
search terms for “Raynauds” or “Raynauds disease” were combined with the terms 13
“epidemiology” , “prevalence”, “risk” or “incidence” to generate the citations (see Appendix 14
1 for full details of search strategy). “Cross sectional”, “case-control” or “cohort” studies and 15
“systematic review” were also applied for types of studies. 16
Abstracts were reviewed and the full papers were sought where abstracts were felt to be 17
relevant. Any duplicate articles were excluded (Figure 1). Where there was difficulty in 18
article retrieval, the authors were contacted via email. The literature search and abstract 19
review was completed by RG and validated by WZ. Reference lists of the review articles 20
were also examined for relevant studies. 21
22
Page 5 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
6
2: Inclusion and Exclusion Criteria 1
Inclusion criteria: studies reporting the prevalence and/or incidence of PRP; studies 2
reporting potential risk factors associated with PRP; studies reporting human data on PRP in 3
people of any age; studies in any language (4 articles required translation – 1 Japanese, 1 4
Turkish, 1 French, 1 Italian). 5
Exclusion criteria (Figure 1): studies assessing treatment of PRP; studies involving 6
participants with RP secondary to other diseases; studies assessing RP in a specific 7
occupation e.g., people using vibration tools; unpublished material, case reports, editorials, 8
letters or reviews. 9
3. Data extraction and quality assessment 10
Study characteristics including age range, gender ratio and total number of participants in 11
the study were documented. The study design, country, setting (i.e. hospital or community 12
based) were also assessed and noted. If more than one article used the same study 13
population, the article where the data was felt to be presented most clearly was used in the 14
study. The definition of PRP and instruments used to confirm the condition were also 15
documented. The number of cases of PRP out of the number of people studied in a certain 16
time in the general population was documented as unadjusted crude prevalence. Incidence 17
figures were documented if the number of new cases of PRP in the population at risk 18
studied over a given period of time was stated. 19
Individual odds ratio (OR), relative risk (RR) or hazard ratio (HR) and their 95%confidence 20
interval (CI) were extracted or calculated for the following: 21
Page 6 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
7
o Constitutional: age, gender 1
o Environmental: employment, education, marital status, sex hormone 2
medications 3
o Genetic: family history in 1st
degree relatives 4
o Associations: smoking, alcohol, cardiovascular disease, migraine 5
6
All studies were reviewed by RG to assess study quality and for data extraction and were 7
validated by WZ. An independent reviewer (RK) assessed a random selection of articles to 8
ensure quality of data extraction. Study quality was assessed according to study design 9
(cohort, cross-sectional and case control), setting (community or hospital), sample size, case 10
definition, exposure definition, confounding factors and adjustment. Quality scoring for 11
studies was not performed as it is not possible or fair to assign equal weight to different 12
quality aspects related to the study. However, current consensus standards of reporting 13
meta-analysis of observational studies in epidemiology (MOOSE) [12] were followed, and 14
subgroup/sensitivity analysis was undertaken to examine the changes of the estimate 15
according to different quality aspects 16
4. Statistical analysis 17
Individual data for prevalence and incidence were derived from the original report either 18
directly or indirectly from the information provided in each study. The pooled proportion 19
was calculated as the back-transform of the weighted mean of the transformed proportion, 20
using inverse arcsine variance weights for the fixed effects model and DerSimonian-Laird 21
(1986) weights for the random effects model. [13, 14] Cumulative incidence and 95%CI were 22
Page 7 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
8
transformed into incidence rate data (i.e., incidence per 100 person-years) and pooled 1
incidence rate was estimated. Individual data for OR, RR and HR were pooled to present 2
the overall relative risk of all observational studies, as well as separately for each specific 3
risk measure or study design as appropriate. Random-effects mode was used to pool the 4
data.[15] Heterogeneity was examined using Forest plots, Cochran Q tests and I2
statistic as 5
a measure for inconsistency due to chance.[16, 17] Publication bias was assessed using 6
funnel plots and Eggers test or the Harbord test if the number of studies included in the 7
meta-analysis was too small (≤4).[18] All analyses were undertaken using StatsDirect© 8
Version 2.7.9. 9
10
RESULTS 11
1: Study characteristics 12
2378 citations were found in the initial literature search. 467 duplicates were removed and 13
1871 citations were excluded as they did not meet the inclusion criteria (Figure 1). The final 14
number of studies available for analysis was 33 (33, 733 subjects). There were 2 cohort 15
studies[19, 20] (1, 632 subjects), 17 cross-sectional studies[6, 21-36] (25, 797 subjects) and 16
14 case-control studies[7-11, 37-45] (6, 304 subjects) (Table 1). Data for incidence and 17
prevalence were taken from cohort and cross-sectional studies respectively. Data for risk 18
factors were taken from all studies as long as the results were reported. 19
Age ranges across different study designs were as follows: case-control (16-79 years), cohort 20
(18-81 years), cross sectional (12-84 years). 67% of the studies involved participants 21
recruited in a community based setting. The majority of studies were conducted in Europe 22
Page 8 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
9
(18)[6, 9, 19, 22, 24, 26, 27, 29, 30, 32, 33, 35-37, 39, 41-43] or the USA (10)[7-8, 10-11, 20-1
21, 23, 38, 40, 44], however other countries of origin included Japan (2)[25, 28], New 2
Zealand (1)[34] and Israel (1)[45]. One comparison study included participants from USA and 3
France.[31] 4
Participants were surveyed by means of phone, face-to-face interview, and/or postal 5
questionnaire. 26 studies included a physical examination which also included blood testing 6
(including serology), nail fold capillaroscopy and use of colour chart/photographs (Table 1) 7
10 studies used specific criteria to define PRP (3 studies [8, 21, 32] Allen & Brown[1], 3[9, 8
36, 37]Leroy & Medsger[2], 4[6, 22, 33-34] UK Scleroderma Study Group[4]). The remaining 9
studies used a combination of cold sensitivity, varying degrees of colour change and sensory 10
symptoms via questionnaire or interview to define PRP. Colour charts or photographs to 11
indicate colour change were used in 12 studies[6-7, 9-10, 19-20, 25, 28-29, 31, 33, 35] and 12
nailfold capillaroscopy was performed as part of the examination in 10 studies.[8-9, 19, 31, 13
36, 37, 39, 41-43] In 15 studies, blood testing including serology and/or inflammatory 14
markers were performed.[6, 8-9, 11, 24, 30, 33, 36-37, 39-44] 15
Studies with clear definition of PRP or clear exclusion criteria for secondary RP were 16
categorised as “definite PRP” in this study. Studies with less clear definition of PRP were 17
categorised as “possible PRP”. Studies with clear definition of secondary RP were excluded.18
Page 9 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
10
2: Prevalence of PRP 1
The overall prevalence for definite PRP varied from 1.6 – 7.2% in 6 cross sectional studies in 2
the general population (women: 2.1-15.8% and men 0.8-6.5%).[21, 23, 25, 27, 29, 33] The 3
pooled prevalence was 4.85% (95% CI 2.08%, 8.71%) (Figure 2), with 5.74% (95% CI 2.74, 4
9.75) in women and 4.12% (95% CI 1.60, 7.74) in men. We used the Harbord test to detect 5
publication bias (1.59 92.5% CI -21.6,24.8, P=0.87) 6
The overall prevalence for possible PRP ranges from 3.98% to 12.7% (women: 4.5-17.9% and 7
men: 3.4-7.2%) in three cross sectional studies.[26, 34-35] The prevalence in specific 8
populations varies depending on the studies (Table 2) 9
In 6 studies assessing the general population we found the lowest prevalence of PRP in 10
Japan with an overall prevalence of 1.6 (2.1% in women, 1.1% in men).[25] Highest overall 11
prevalence figures were found in the USA with a median prevalence of 7.5% (7.8% in 12
women, 5.8% in men,).[21, 23] A study from France also showed high prevalence figures of 13
11.75% in women and 6.3% in men (median values).[31] (Table 3) 14
Five studies reported prevalence of PRP by age.[6, 28-30, 34]. Three did not find any age-related 15
prevalence (Leppert1987, Iwata 1987 and Voulgari 2000). Purdie (2009) reported a higher 16
prevalence of PRP in younger compared to older age groups, whereas Fraenkel (1999) reported 17
higher prevalence in older age groups in men (adjusted OR=2.3, 95%CI 1.0 to 5.2 highest vs. lowest 18
tertile) but not in women (adjusted OR=0.9, 95%CI 0.4 to 1.6). Jones (2003) also showed a slight 19
increase in prevalence by age in yearly increments between ages 12-15 years. 20
21
22
Page 10 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
11
3: Incidence of Primary Raynauds Phenomenon
Only two studies reported incidence rates.[19-20] Carpentier et al reported an annual
incidence rate of 0.25% (95% CI 0.17, 0.33), with 0.24% in women and 0.26% in men and
Suter et al reported a 7-year incidence of 1.87% (2.2% in women and, 1.5% in men), which
was converted to an annual incidence rate of 0.26% (95%CI 0.17, 0.39). The pooled annual
incidence rate of these two studies was therefore 0.25% (95%CI 0.19, 0.32).
4: Risk factors and associations
In 18 studies (23, 197 participants), there was a positive association between female gender
and PRP (OR 1.65, 95% CI 1.42, 1.91).[6-7, 9, 20-29, 33-35, 37, 44] Family history, assessed in
2 studies looking at 1st degree relatives, also had a positive significant association with PRP
(OR 16.6, 95%CI 7.44, 36.8).[8-9] No significant association was found with education
beyond primary school age.[6, 37] (Table 4). Manual occupation (not including vibration
tool use) had an OR of 2.66 (95% CI 1.73, 4.08) in 1 study of 3873 participants.[25] In 4
studies, being married was associated with a lower risk of PRP with OR of 0.60 (95% CI 0.43,
0.83) compared with being single/divorced/widowed.[6-7, 23, 37] Smoking was found to
have an association in 9 studies giving a pooled OR of 1.27 (95% CI 1.06, 1.53).[7, 9-11, 20,
22-23, 32, 44] Alcohol use,[23, 44] participants with positive Helicobacter Pylori
investigations[39, 41] and those with conditions such as diabetes,[23] hypertension[11, 23]
and hypercholesterolaemia[23] did not have a significant association with PRP.
Migraine had a positive significant association with a pooled OR of 4.02 (95% CI 2.62, 6.17)
in 6 studies.[6, 9-11, 22, 45] One study of 3442 participants reported a positive association
Page 11 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
12
of cardiovascular disease with PRP with an OR of 1.69 (95% CI 1.22, 2.34).[44]
Cardiovascular disease in this study included a history of ischaemic heart disease,
intermittent claudication, congestive cardiac failure and cerebrovascular disease. A single
study using 81 participants did not show a positive significant association of coronary heart
disease with PRP.[40]
A positive association was found in participants taking oestrogen replacement therapy alone
in two studies with an OR of 2.34 (95% CI 1.42, 3.84).[23, 38] However no significant
association was found in combined oestrogen and progesterone replacement therapy[38] in
postmenopausal women or in oral contraceptive pill[10-11] use in two other studies. A
study by Smyth et al looking at allele frequencies of known polymorphisms of candidate
vasoactive mediator genes (eNOS, BKRG, ET01 and ETA receptor genes) did not show any
association.[9] Shemirani et al looked at clotting factors in participants with PRP and found a
significant association with methyltetrahydrofolate reductase C677T mutations (OR 0.4, 95%
CI 0.2, 0.9) but no difference in other thrombosis-associated alleles (FVLeiden, prothrombin
G20210A).[42]
DISCUSSION
This is the first meta-analysis of the literature for the prevalence, incidence, risk factors and
associations of PRP. Overall the pooled mean prevalence of PRP in the general population
was 4.85% (95% CI 2.08%, 8.71%) (Figure 2) and the mean incidence was 0.25% (95% CI
0.17, 0.33) per annum.[19] Major risk factors/associations of PRP include female gender,
family history of PRP, migraine, smoking, cardiovascular disease, manual occupation,
oestrogren replacement therapy and possibly marital status. (Table 4).
Page 12 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
13
Variations in prevalence were observed between countries (Table 3) though this could
reflect use of different diagnostic criteria rather than real differences in prevalence. The
heterogeneity of prevalence figures may also reflect the differences in the way the studies
were conducted, the selection of participants (e.g., age and gender), and the disease
definition. All studies (except for Maricq 1997) demonstrate a higher prevalence of PRP in
women. This may be due to a relationship with female hormones as two studies found an
association between PRP and use of oestrogen replacement therapy alone,[23, 38] although
no association was found between combined oestrogen and progesterone replacement or
the oral contraceptive pill.[10-11, 38] In contrast, prevalence of PRP does not increase with
age in five published studies with a wide age range of participants from 12 years up to 84
years.[6, 28-30, 34] This accords with the clinical observation that PRP usually starts in
teenage years and that later development, which is far less common, is characteristic of
secondary RP. While the former may be driven predominantly by genetic risk factors, later
onset “primary” Raynaud’s may be predominantly influenced by environmental exposures
such as vascular microtrauma from manual usage and vibrating tools. In terms of other
environmental factors we did find a weak negative association between marital status and
PRP with an OR of 0.60 (95%CI 0.43, 0.83) in those that are married vs.
single/separated/widowed/divorced.[6-7, 23, 37] However, there is no plausible biological
explanation for this and the reported data may not be free from confounding bias.
The association of cardiovascular disease and autoimmune disease is well documented and
thought to be due to accelerated atherosclerosis as a result of chronic inflammation,
treatment such as glucocorticoids as well as the traditional risk factors for cardiovascular
disease.[46-52] A link between cardiovascular disease and PRP has been shown in only one
Page 13 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
14
study[44] and a reason for this association is not known. It is unlikely to be due to an
inflammatory process or related to medication and with PRP having predominance for the
female population and onset at a young age it not clear if traditional cardiovascular risk
factors play a part. However, smoking was found to have positive association with PRP in
our study (OR 1.27, 95% CI 1.06, 1.53). It is well known that smoking is one of three
(smoking, hypertension and hyperlipidaemia) main risk factors for cardiovascular and
cerebrovascular disease.[53-59] Smoking may be the same risk factor for PRP and CVD.
Whether smoking causes PRP first then CVD is an interesting question which deserves
further research. More interestingly, we found a very strong association between migraine
and PRP (OR 4.02, 95%CI 2.62, 6.17). It has been previously shown that migraine is due to a
cascade of vascular and neural events.[46-47] However, a review by Rosamund suggested
migraine was not shown to be linked with coronary heart disease but possibly shares a
common underlying pathophysiology with Raynaud’s phenomenon and other vasospastic
disorders such as variant angina.[60-61] It is thought there may be other factors that may
affect the underlying mechanism for these vasospastic conditions as episodes occur at
different times with differing precipitants.[62-63] Further study may help clarify whether
PRP is a benign vasospastic disorder or whether there is underlying pathology affecting the
vascular wall associated with traditional risk factors seen in cardiovascular disease.
There are number of caveats to this study. Firstly, it was striking that there was no uniform
definition for diagnosis of PRP. Only 39% of studies looking at prevalence had a precise
definition for PRP, thereby reducing the number of studies we used to assess pooled
prevalence. It is possible that the variation in definition of PRP together with the way
participants were recruited and assessed may have led to under- or over-estimation of the
Page 14 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
15
true prevalence of PRP in the general population. We feel that an amalgamation of the
generally more commonly used definitions would ensure that the diagnosis is clear by
assessing symptoms, using colour chart or photographs for confirmation of colour change
and carefully exclude underlying conditions including checking for digital infarcts/ulceration,
nailfold capillaroscopy and assessing autoimmune screen and inflammatory markers.
Secondly, as our objective was to specifically examine the epidemiology of PRP a large
proportion of studies were excluded because they focused on secondary Raynaud’s
phenomenon, especially related to connective tissue diseases and vibration white finger. In
addition we also excluded studies that looked at investigation or treatment of PRP. This left
only a small number of studies to assess. From the studies included, there was a great deal
of variation in the population of participants used. 9 out of the 17 studies used investigated
participants in the general population whereas the remainder examined specific populations
such as single gender, children or hospital/medical personnel. Furthermore, there was
considerable variation in the risk factors addressed in each study and this may have affected
the significance and association, or lack of association between the risk factors and PRP. We
tried to extract as many risk factors from each study as possible to use in our analysis. In the
future, a larger multinational population study may help us to get a better understanding of
the disease. This would be particularly useful if standardised criteria were used to include
participants in the studies, using strict definition for PRP (as mentioned previously) and data
was collected in a similar fashion assessing a wide variety of possible risk factors
(particularly related to cardiovascular disease and vasospastic disoders) for more accurate
data analysis.
Page 15 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
16
CONCLUSION
This first systematic review summarises the burden of PRP in the general population using
published literature. It is not a rare condition (prevalence 4.85% and annual incidence
0.25%). It starts at a young age, is more common in women and associates with a family
history and with smoking. In addition, people with PRP are 4 times more likely to have
migraine than those without this condition.
ACKNOWLEDGEMENT: Our sincere thank you to Joanna Ramowski and Helen Richardson for
article retrieval and support. Also special thank you to Anu Suokas, Karin Tatsumoa,
Professor Tiraje Truncer, Ana Valdes and Maggie Wheeler for language translation.
AUTHOR CONTRIBUTIONS
Study conception and design: Dr Zhang, Professor Doherty, Dr Lanyon, Dr Garner
Acquision of data: Dr Garner, Dr Kumari, Dr Zhang
Statistical Analysis: Dr Garner, Dr Zhang
Analysis and interpretation of data: Dr Garner, Dr Zhang, Professor Doherty, Dr Lanyon
Manuscript preparation and final approval of manuscript: Dr Garner, Dr Zhang, Professor
Doherty, Dr Lanyon
Funding No funding
Competing interests None
Ethical approval and patient consent Not required
Data sharing statement No unpublished data were used in this study. No additional data
available.
Page 16 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
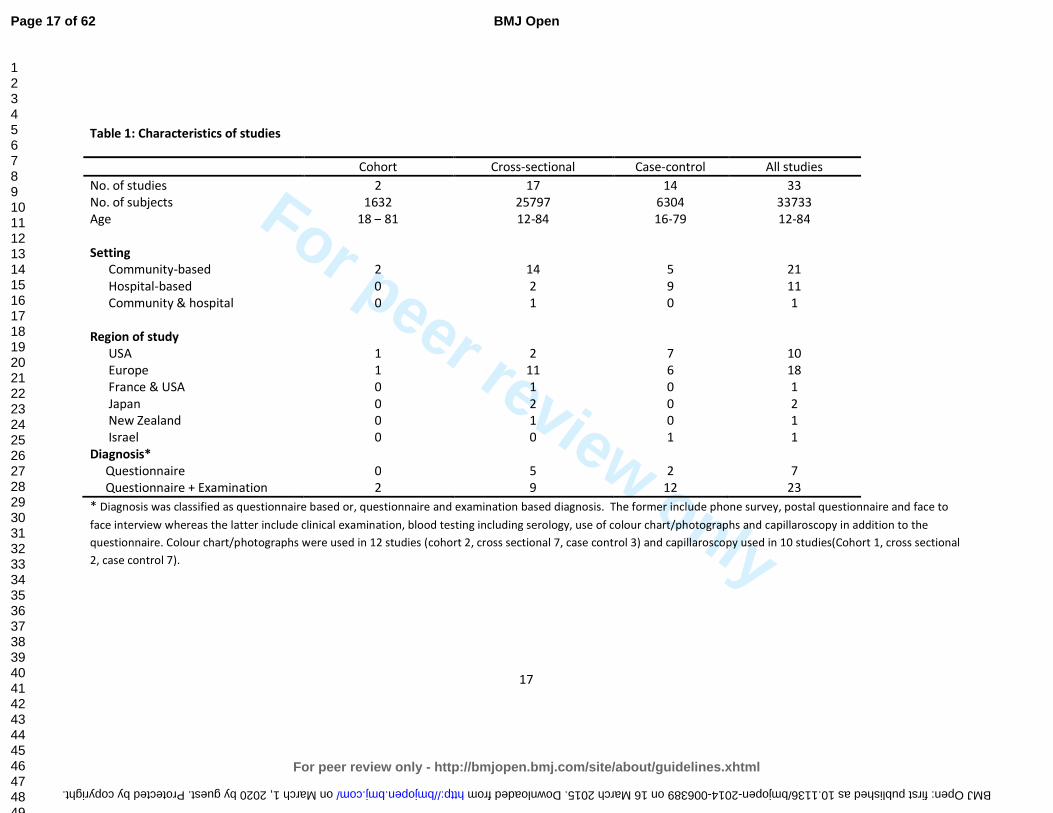
For peer review only
17
Table 1: Characteristics of studies
Cohort Cross-sectional Case-control All studies
No. of studies 2 17 14 33
No. of subjects 1632 25797 6304 33733
Age 18 – 81 12-84 16-79 12-84
Setting
Community-based 2 14 5 21
Hospital-based 0 2 9 11
Community & hospital 0 1 0 1
Region of study
USA 1 2 7 10
Europe 1 11 6 18
France & USA 0 1 0 1
Japan 0 2 0 2
New Zealand 0 1 0 1
Israel 0 0 1 1
Diagnosis*
Questionnaire 0 5 2 7
Questionnaire + Examination 2 9 12 23
* Diagnosis was classified as questionnaire based or, questionnaire and examination based diagnosis. The former include phone survey, postal questionnaire and face to
face interview whereas the latter include clinical examination, blood testing including serology, use of colour chart/photographs and capillaroscopy in addition to the
questionnaire. Colour chart/photographs were used in 12 studies (cohort 2, cross sectional 7, case control 3) and capillaroscopy used in 10 studies(Cohort 1, cross sectional
2, case control 7).
Page 17 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
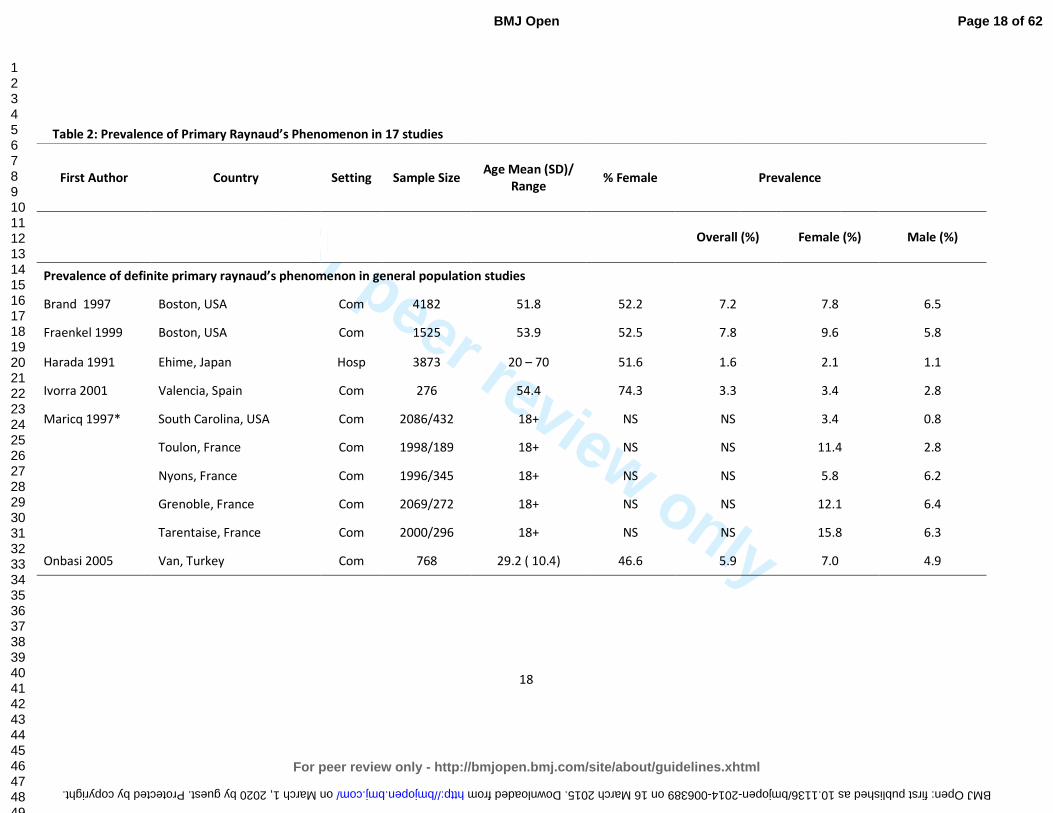
For peer review only
18
Table 2: Prevalence of Primary Raynaud’s Phenomenon in 17 studies
First Author Country Setting Sample Size
Age Mean (SD)/
Range
% Female
Prevalence
Overall (%)
Female (%) Male (%)
Prevalence of definite primary raynaud’s phenomenon in general population studies
Brand 1997 Boston, USA Com 4182 51.8 52.2 7.2 7.8 6.5
Fraenkel 1999 Boston, USA Com 1525 53.9 52.5 7.8 9.6 5.8
Harada 1991 Ehime, Japan Hosp 3873 20 – 70 51.6 1.6 2.1 1.1
Ivorra 2001 Valencia, Spain Com 276 54.4 74.3 3.3 3.4 2.8
Maricq 1997* South Carolina, USA Com 2086/432 18+ NS NS 3.4 0.8
Toulon, France Com 1998/189 18+ NS NS 11.4 2.8
Nyons, France Com 1996/345 18+ NS NS 5.8 6.2
Grenoble, France Com 2069/272 18+ NS NS 12.1 6.4
Tarentaise, France Com 2000/296 18+ NS NS 15.8 6.3
Onbasi 2005 Van, Turkey Com 768 29.2 ( 10.4) 46.6 5.9 7.0 4.9
Page 18 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
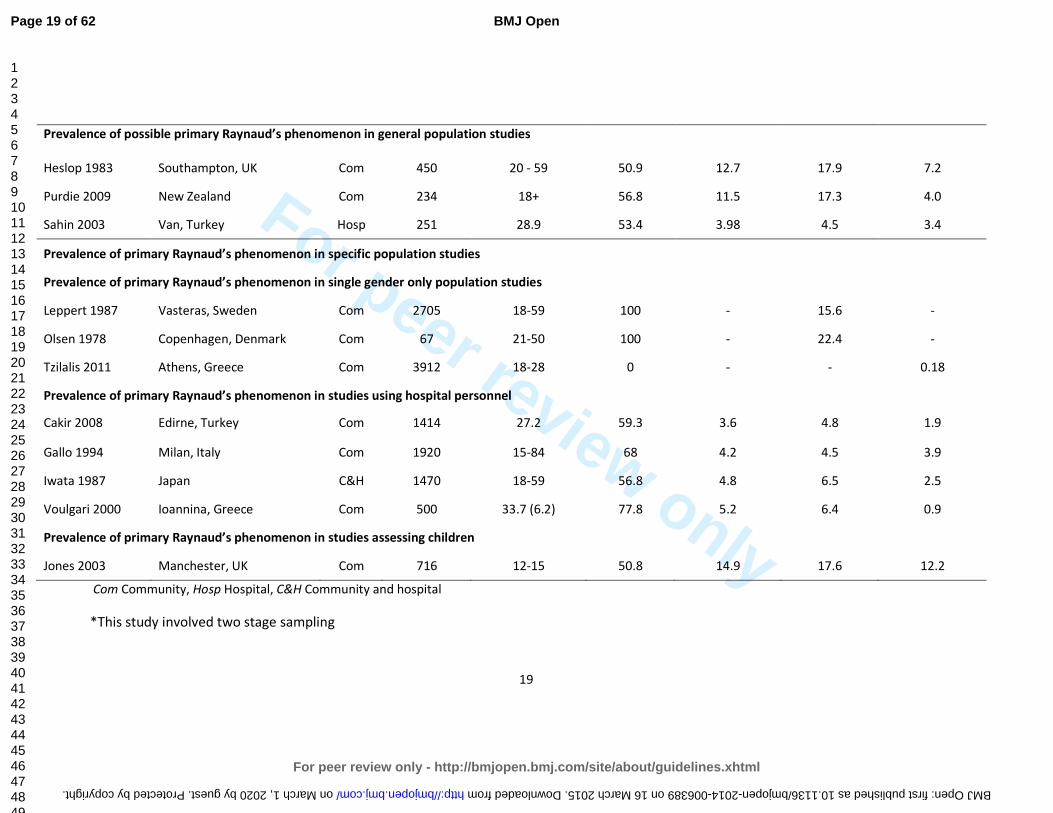
For peer review only
19
Prevalence of possible primary Raynaud’s phenomenon in general population studies
Heslop 1983 Southampton, UK Com 450 20 - 59 50.9 12.7 17.9 7.2
Purdie 2009 New Zealand Com 234 18+ 56.8 11.5 17.3 4.0
Sahin 2003 Van, Turkey Hosp 251 28.9 53.4 3.98 4.5 3.4
Prevalence of primary Raynaud’s phenomenon in specific population studies
Prevalence of primary Raynaud’s phenomenon in single gender only population studies
Leppert 1987 Vasteras, Sweden Com 2705 18-59 100 - 15.6 -
Olsen 1978 Copenhagen, Denmark Com 67 21-50 100 - 22.4 -
Tzilalis 2011 Athens, Greece Com 3912 18-28 0 - - 0.18
Prevalence of primary Raynaud’s phenomenon in studies using hospital personnel
Cakir 2008 Edirne, Turkey Com 1414 27.2 59.3 3.6 4.8 1.9
Gallo 1994 Milan, Italy Com 1920 15-84 68 4.2 4.5 3.9
Iwata 1987 Japan C&H 1470 18-59 56.8 4.8 6.5 2.5
Voulgari 2000 Ioannina, Greece Com 500 33.7 (6.2) 77.8 5.2 6.4 0.9
Prevalence of primary Raynaud’s phenomenon in studies assessing children
Jones 2003 Manchester, UK Com 716 12-15 50.8 14.9 17.6 12.2
Com Community, Hosp Hospital, C&H Community and hospital
*This study involved two stage sampling
Page 19 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
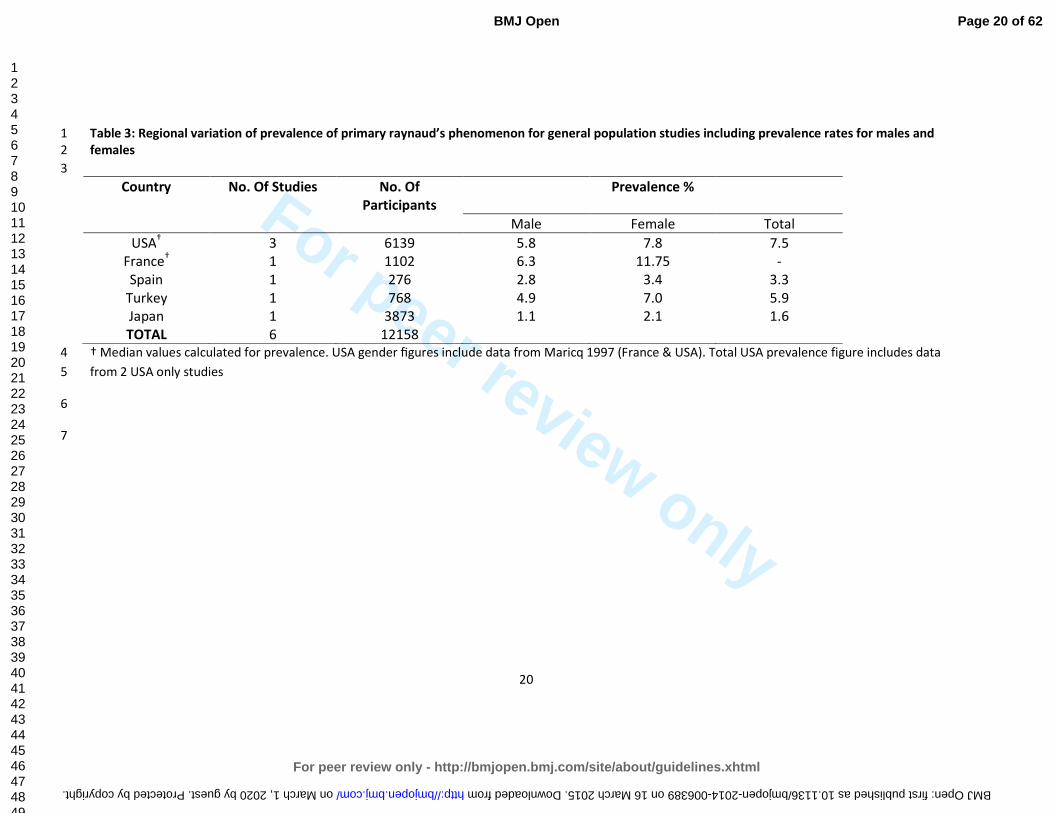
For peer review only
20
Table 3: Regional variation of prevalence of primary raynaud’s phenomenon for general population studies including prevalence rates for males and 1
females 2
3
Country No. Of Studies No. Of
Participants
Prevalence %
Male Female Total
USA† 3 6139 5.8 7.8 7.5
France† 1 1102 6.3 11.75 -
Spain 1 276 2.8 3.4 3.3
Turkey 1 768 4.9 7.0 5.9
Japan 1 3873 1.1 2.1 1.6
TOTAL 6 12158
† Median values calculated for prevalence. USA gender figures include data from Maricq 1997 (France & USA). Total USA prevalence figure includes data 4
from 2 USA only studies 5
6
7
Page 20 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
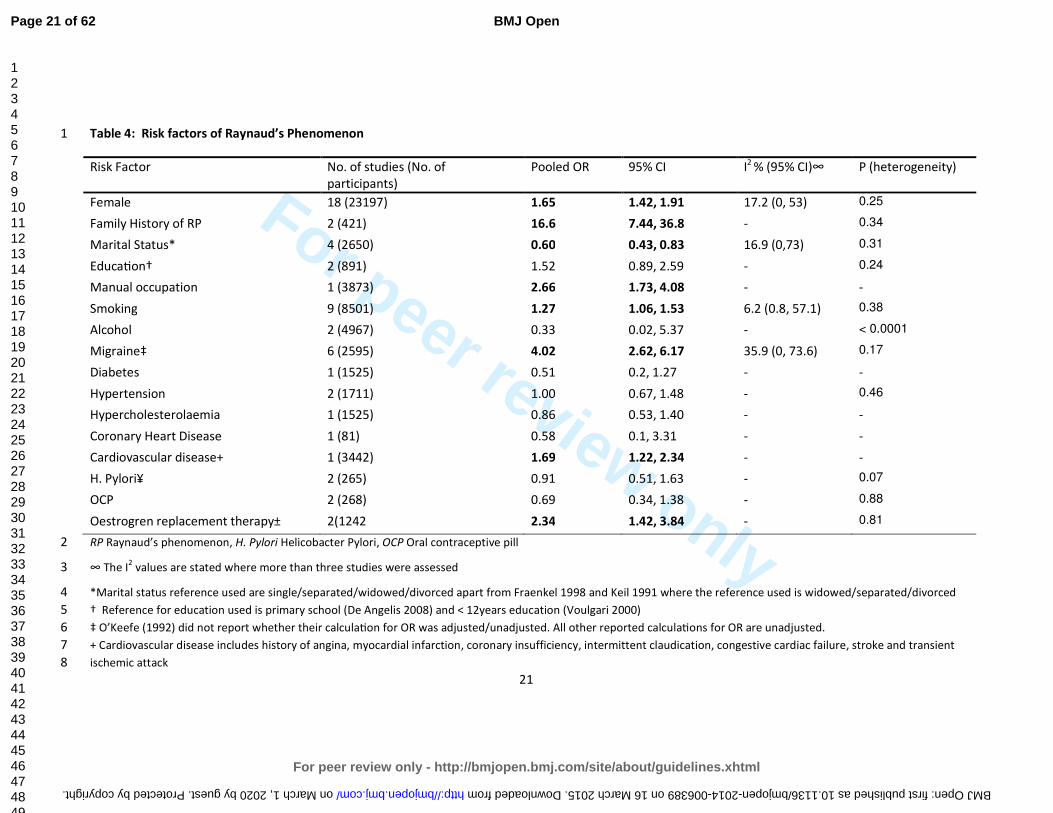
For peer review only
21
Table 4: Risk factors of Raynaud’s Phenomenon 1
Risk Factor No. of studies (No. of
participants)
Pooled OR 95% CI I2
% (95% CI)∞
P (heterogeneity)
Female 18 (23197) 1.65 1.42, 1.91 17.2 (0, 53) 0.25
Family History of RP 2 (421) 16.6 7.44, 36.8 - 0.34
Marital Status* 4 (2650) 0.60 0.43, 0.83 16.9 (0,73) 0.31
EducaWon† 2 (891) 1.52 0.89, 2.59 - 0.24
Manual occupation 1 (3873) 2.66 1.73, 4.08 - -
Smoking 9 (8501) 1.27 1.06, 1.53 6.2 (0.8, 57.1) 0.38
Alcohol 2 (4967) 0.33 0.02, 5.37 - < 0.0001
Migraine‡ 6 (2595) 4.02 2.62, 6.17 35.9 (0, 73.6) 0.17
Diabetes 1 (1525) 0.51 0.2, 1.27 - -
Hypertension 2 (1711) 1.00 0.67, 1.48 - 0.46
Hypercholesterolaemia 1 (1525) 0.86 0.53, 1.40 - -
Coronary Heart Disease 1 (81) 0.58 0.1, 3.31 - -
Cardiovascular disease+ 1 (3442) 1.69 1.22, 2.34 - -
H. Pylori¥ 2 (265) 0.91 0.51, 1.63 - 0.07
OCP 2 (268) 0.69 0.34, 1.38 - 0.88
Oestrogren replacement therapy± 2(1242 2.34 1.42, 3.84 - 0.81
RP Raynaud’s phenomenon, H. Pylori Helicobacter Pylori, OCP Oral contraceptive pill 2
∞ The I2 values are stated where more than three studies were assessed 3
*Marital status reference used are single/separated/widowed/divorced apart from Fraenkel 1998 and Keil 1991 where the reference used is widowed/separated/divorced 4
† Reference for education used is primary school (De Angelis 2008) and < 12years education (Voulgari 2000) 5
‡ O’Keefe (1992) did not report whether their calculaWon for OR was adjusted/unadjusted. All other reported calculaWons for OR are unadjusted. 6
+ Cardiovascular disease includes history of angina, myocardial infarction, coronary insufficiency, intermittent claudication, congestive cardiac failure, stroke and transient 7
ischemic attack 8
Page 21 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
22
¥ Positive investigation for Helicobacter pylori uses urea breath test (Savarino 2000) and serology (Herve 2006) 1
± Adjusted for age BMI alcohol cigarettes and B adrenoreceptor antagonists in study by Fraenkel (1998) 2
3
4
Figure 1: Flow chart diagram showing results of systematic literature search 5
6
7
8
9
10
11
12
Figure 2: Forest plot showing the pooled prevalence of definite Primary Raynauds Phenomenon for 5 general population studies 13
14
15
16
Box 1: Exclusion reasons for 1814 papers
Review (219), Case report (34), Letter (14), Webpage (5), Animal studies unrelated to RP (4), Connective tissue disease
(602), Vibration induced disease (169), Diagnosis/investigation of RP (11), Secondary progression from primary RP (4),
drugs related to RP (53), RA/inflammatory arthritis (21), Other musculoskeletal (37), Fibromyalgia (9)Genetics not
related to RP (11), Autoantibodies (13), Treatment involving sympathectomy (45), Ophthalmology studies (14),
Psychiatric conditions (11), Haematological disease (14), Infectious disease (24), cardiovascular disease (64), Respiratory
disease (17), Gastrointestinal disease (27), Renal disease (27), Dermatological (30), Endocrine disease (31), Neurological
disease (43), Cancer (106), Drugs not related to RP (63), Vascular intervention (64), Laser Doppler flowmetry (8), Breast
implant rupture (4)Others: including motor vehicles, dentists, seafarers, fishermen, aircrafts, breast feeding (17)
Box 2: Exclusion reasons for 64 papers
Letter to editor (1)
Review (5)
Diagnosis/Investigation of RP (14)
Secondary RP (39)
Treatment RP (1)
Same patient sample as is already included in another study used (3)
Case only study (1)
Page 22 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
23
REFERENCES
1 Allen E, Brown G. Raynaud disease: A critical review of minimal requisites for diagnosis. Am J Med
Sci 1932;183(2):187-200.
2 LeRoy E, Medsger T. Raynaud’s phenomenon: a proposal for classification. Clin Exp Rheumatol
1992;10:485-488.
3 Bowling J, Dowd P. Raynaud’s disease. Lancet 2003;361:2078-80.
4. Brennan P, Silman A, Black C, et al. Validity and reliability of three methods used in the diagnosis
of Raynaud's phenomenon. The UK Scleroderma Study Group. Br J Rheumatol 1993;32(5):357-61.
5 Maricq H, Weinrich M. Diagnosis of Raynaud’s phenomenon assisted by colour charts. J Rheumatol
1988;15(3):454-459.
6 Voulgari P, Alamanos Y, Papazisi D, et al. Prevalence of Raynaud's phenomenon in a healthy Greek
population. Ann Rheum Dis 2000;59(3):206-210.
7 Keil J, Maricq H, Weinrich M, et al. Demographic, social and clinical correlates of Raynaud
phenomenon. Int J Epidemiol 1991;20(1):221-224.
8 Freedman R, Mayes M. Familial aggregation of primary Raynaud's disease. Arthritis and
Rheumatism 1996;39(7):1189-1191.
9 Smyth AE, Hughes AE, Bruce IN, Bell AL. A case-control study of candidate vasoactive mediator
genes in primary Raynaud's phenomenon. Rheumatology (Oxford) 1999;38(11):1094-1098.
10 O'Keeffe S, Tsapatsaris N, Beetham W. Association between Raynaud's phenomenon and
migraine in a random population of hospital employees. J Rheumatol 1993;20(7):1187-1188.
11 O'Keeffe S, Tsapatsaris N, Beetham W. Increased prevalence of migraine and chest pain in
patients with primary Raynaud disease. Ann Intern Med 1992;116(12 Pt 1):985-989.
12 Stroup D, Berlin J, Morton S, et al. Meta-analysis of Observational Studies in Epidemiology
(Moose) group. JAMA 2000;283:2008-2012.
13 DerSimonian R, Laird N. Meta-analysis in Clinical Trials. Controlled Clinical Trials 1986;7:177-188.
14 Stuart A, Ord JK. Kendall's Advanced Theory of Statistics (6th edition). London: Edward Arnold
1994.
15 Whitehead A, Whitehead J. A general parametric approach to the meta-analysis of randomised
clinical trials. Stat Med 1991;10:1665-77.
16 Gavaghan D, Moore R, McQuay H. An evaluation of homogeneity tests in meta-analyses in pain
using simulations of individual patient data. Pain 2000;85:415-24.
17 Higgins J, Thomspon S, Deeks J, et al. Measuring inconsistency in meta-anlyses. BMJ
2003;327:557-60.
18 Egger M, Davey Smith G, Schneider M, et al. Bias in meta-anlysis detected by a simple, graphical
test. BMJ 1997;315:629-34.
19 Carpentier P, Satger B, Poensin D, et al. Incidence and natural history of Raynaud phenomenon: a
long-term follow-up (14 years) of a random sample from the general population. J Vasc Surg 2006;
44(5):1023-1028.
20 Suter L, Murabito J, Felson D, et al. The incidence and natural history of Raynaud's phenomenon
in the community. Arthritis Rheum 2005; 52(4):1259-1263.
21 Brand F, Larson M, Kannel W, et al. The occurrence of Raynaud's phenomenon in a general
population: the Framingham Study. Vasc Med 1997;2(4):296-301.
22 Cakir N, Pamuk O, Donmez S, et al. Prevalence of Raynaud's phenomenon in healthy Turkish
medical students and hospital personnel. Rheumatol Int 2008; 29(2):185-188.
23 Fraenkel L, Zhang Y, Chaisson C F et al. Different factors influencing the expression of raynaud's
phenomenon in men and women. Arthritis Rheum 1999;42(2):306-310.
24 Gallo E, Bianchi E, Motta A, et al. [The incidence of Raynaud's phenomenon in 1920 residents in
Milan]. [Italian] Incidenza del fenomeno di Raynaud in 1920 residenti in Milano. Minerva
Cardioangiol 1994;42(1-2):65-71.
Page 23 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
24
25 Harada N, Ueda A, Takegata S. Prevalence of Raynaud's phenomenon in Japanese males and
females. J Clin Epidemiol 1991;44(7):649-655.
26 Heslop J, Coggon D, Acheson E. The prevalence of intermittent digital ischaemia (Raynaud's
phenomenon) in a general practice. J R Coll Gen Pract 1983;33(247):85-89.
27 Ivorra J, Perales J, Carballido C, et al. Prevalence of Raynaud's phenomenon in general practice in
the East of Spain. Clin Rheumatol 2001;20(2):88-90.
28 Iwata H, Makimo S, Miyashita K. [Prevalence of Raynaud's phenomenon in individuals not using
vibrating tools]. Sangyo Igaku - Japanese Journal of Industrial Health 1987;29(6):500-503.
29 Jones G, Herrick A, Woodham S, et al. Occurrence of Raynaud's Phenomenon in Children Ages 12-
15 Years: Prevalence and Association with Other Common Symptoms. Arthritis Rheum
2003;48(12):3518-352.
30 Leppert J, Aberg H, Ringqvist I, et al. Raynaud's phenomenon in a female population: prevalence
and association with other conditions. Angiology 1987;38(12):871-877.
31 Maricq H, Carpentier P, Weinrich M, et al. Geographic variation in the prevalence of Raynaud's
phenomenon: A 5 region comparison. J Rheumatol 1997;24(5):879-889.
32 Olsen N, Nielsen S. Prevalence of primary Raynaud phenomena in young females. Scand J Clin Lab
Invest 1978;38(8):761-764.
33 Onbasi K, Sahin I, Onbasi O, et al. Raynaud's phenomenon in a healthy Turkish population. Clin
Rheumatol 2005;24(4):365-369.
34 Purdie G, Harrison A, Purdie D. Prevalence of Raynaud's phenomenon in the adult New Zealand
population. N Z Med J 2009;122(1306):55-62.
35 Sahin I, Onbasi K, Onbasi O, et al. Raynaud's Phenomenon in Healthy Population Who Admitted to
the Hospital in Van Region, Turkey [Turkish] Van Yoresinde Hastaneye Basvuran Saglikli
Populasyonda Raynaud Fenomeni. Ondokuz Mayis Universitesi Tip Dergisi 2003;20(2):73-77.
36 Tzilalis V, Panagiotopoulos N, Papatheodorou G, et al. Prevalence of Raynaud's phenomenon in
young Greek males. Clin Rheumatol 2011;30(1):57-59.
37 De Angelis R, Salaffi F, Grassi W. Health-related quality of life in primary Raynaud phenomenon. J
Clin Rheumatol 2008;14(4):206-210.
38 Fraenkel L, Zhang Y, Chaisson C, et al. The association of estrogen replacement therapy and the
Raynaud phenomenon in postmenopausal women. Ann Intern Med 1998;129(3):208-212.
39 Herve F, Cailleux N, Benhamou Y, et al. [Helicobacter pylori prevalence in Raynaud's disease].
[French] Prevalence des infections a Helicobacter pylori au cours de la maladie de Raynaud. Revue
de Medecine Interne 2006;27(10):736-741.
40 Koh K, Kim S, Lee K, et al. Does prevalence of migraine and Raynaud's phenomenon also increase
in Korean patients with proven variant angina? Int J Cardiol 1995; 51(1):37-46.
41 Savarino V, Sulli A, Zentilin P, et al. No evidence of an association between Helicobacter pylori
infection and Raynaud phenomenon. Scand J Gastroenterol 2000;35(12):1251-1254.
42 Shemirani A, Szomjak E, Balogh E, et al. Polymorphism of clotting factors in Hungarian patients
with Raynaud's. Blood Coagul Fibrinolysis 2011;22(1):56-59.
43 Susol E, MacGregor A, Barrett J, et al. A two-stage, genome-wide screen for susceptibility loci in
primary Raynaud's phenomenon. Arthritis Rheum 2000;43(7):1641-1646.
44 Suter L, Murabito J, Felson D, et al. Smoking, Alcohol Consumption, and Raynaud's Phenomenon
in Middle Age. Am J Med 2007;120(3):264-271.
45 Zahavi I, Chagnac A, Hering R, et al. Prevalence of Raynaud's phenomenon in patients with
migraine. Arch Intern Med 1984;144(4):742-744.
46 Shoenfeld Y, Gerli R, Doria A, et al. Accelerated atherosclerosis in autoimmune rheumatic
diseases. Circulation. 2005;112: 3337–3347.
47 Tyrrell P, Beyene J, Feldman B, et al. Rheumatic Disease and Carotid Intima-Media Thickness: A
Systematic Review and Meta-Analysis. Arterioscler Thromb Vasc Biol 2010;30:1014-1026.
Page 24 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
25
48 Schoenfeld S, Kasturi S, Costenbader K. The epidemiology of atherosclerotic cardiovascular
disease among patients with SLE: a systematic review. Semin Arthritis Rheum 2013:43(1):77-95 doi:
10.1016/j.semarthrit.2012.12.002. [published Online First 17 February 2013].
49 Peters M, Symmons D, McCarey D, et al. EULAR evidence-based recommendations for
cardiovascular risk management in patients with rheumatoid arthritis and other forms of
inflammatory arthritis. Ann Rheum Dis 2010;69: 325-331 doi: 10.1136/ard.2009.113696. [Published Online
First 22 September 2009].
50 Gabriel S, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and
comorbidity of the rheumatic diseases. Arthritis Res Ther 2009;11(3):229 doi: 10.1186/ar2669.
[published Online First 19 May 2009].
51 Lévy L, Fautrel B, Barnetche T, et al. Incidence and risk of fatal myocardial infarction and stroke
events in rheumatoid arthritis patients. A systematic review of the literature. Clin Exp Rheumatol
2008;26:673-9.
52 Avina-Zubieta J, Choi H, Sadatsafavi M, et al. Risk of cardiovascular mortality in patients with
rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum 2008;59:1690-7.
53 Burns D. Epidemiology of smoking-induced cardiovascular disease. Prog Cardiovasc
Dis. 2003;46(1):11-29.
54 De Backer G. Risk factors and prevention of cardiovascular disease: A review. Dialogues in
Cardiovascular Medicine 2008;13(2):83-99.
55 O’Donnell M, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic
stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010:376(9735):112-
123.
56 JBS3 Board. Joint British Societies’ consensus recommendations for the prevention of
cardiovascular disease (JBS3) Heart 2014;100(Suppl 2)::ii1–ii67.
57 British Cardiac Society, British Hyperlipidaemia Association, British Hypertension Society,
endorsed by the British Diabetic Association. Joint British recommendations on prevention of
coronary heart disease in clinical practice. Heart 1998;80(Suppl 2):S1–29.
58 Joint British Societies. JBS 2: Joint British Societies’ guidelines on prevention of
cardiovascular disease in clinical practice. Heart 2005;91(Suppl 5):v1–52.
59 Goff D, Lloyd-Jones D, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of
cardiovascular risk: a report of the American College of Cardiology/American Heart Association task
force on practice guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2935-59.
60 Gasparini C, Sutherland H, Griffiths L. Studies on the pathophysiology and genetic basis of
migraine. Curr Genomics 2013; 14:300-315.
61 Lipton R, Bigal M. Migraine: Epidemiology, impact and risk factors for progression. Headache
2005;45[Suppl 1]:S3-S13. 62 Rosamond W. Are migraine and coronary heart disease associated? An epidemiologic review.
Headache 2004; 44[Suppl 1]:S5-S12.
63 Miller D, Waters D, Warnica W, et al. Is variant angina the coronary manifestation of generalised
vasospastic disorder? N Engl J Med 1981;304:763-766.
Page 25 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
1
Prevalence, risk factors and associations of Primary Raynaud’s Phenomenon: Systematic 1
review and meta-analysis of observational studies 2
3
Rozeena Garner MBBS MRCP (Rheum) 2, Rakesh Kumari MBBS MD MRCP (Rheum)
2, Peter 4
Lanyon DM FRCP MRCGP DRCOG2, Michael Doherty MA MD FRCP
1, 2, Weiya Zhang BMed 5
MEpi PhD1 6
1Academic Rheumatology, University of Nottingham, UK;
2Department of Rheumatology, 7
Queens Medical Centre, UK 8
9
10
Correspondence to: 11
Dr Weiya Zhang 12
Academic Rheumatology 13
Clinical Sciences Building 14
Nottingham City Hospital 15
Nottingham NG5 1PB 16
UK 17
Telephone: +44 (0)115 823 1756 18
Fax: +44 (0)115 823 1757 19
Page 26 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
2
Email: [email protected] 1
2
Keywords: Primary Raynaud’s phenomenon, prevalence, incidence, risk factors, systematic 3
review 4
Word Count: Abstract: 244, main text: 3133 5
6
Page 27 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
3
Abstract 1
Objective: To systematically review the literature with regard to the prevalence, incidence, 2
risk factors and associations of primary Raynaud’s phenomenon (PRP). 3
Method: A systematic review of the literature of observational studies for PRP was 4
undertaken using five electronic databases. Any studies reporting prevalence, incidence and 5
risk factors of PRP were collected. Relative risk or odds ratio (OR) and 95% confidence 6
interval (CI) were extracted or calculated to present the association between risk factors 7
and PRP. Random effects model was used to pool the results. 8
Results: 33 articles assessing a total of 33, 733 participants were included in this analysis (2 9
cohort, 17 cross-sectional and 14 case-control studies). The pooled prevalence of PRP was 10
4.85% (95% CI 2.08%, 8.71%) in the general population. The pooled annual incidence of PRP 11
was 0.25% (95% CI 0.19, 0.32). Risk factors and associations for PRP included female gender 12
(OR 1.65, 95% CI 1.42, 1.91), family history (OR 16.6, 95% CI 7.44, 36.8), smoking (OR 1.27, 13
95% CI 1.06, 1.53), manual occupation (OR 2.66 95% CI 1.73, 4.08), migraine (OR 4.02, 95% 14
CI 2.62, 6.17), cardiovascular disease (OR 1.69, 95% CI 1.22, 2.34) and marital status 15
(married) (OR 0.60, 95% CI 0.43, 0.83). The definition of PRP varied considerably between 16
studies. 17
Conclusion: This is the first systematic review of the prevalence, incidence, risk factors and 18
associations of PRP. Further study using uniform strict criteria for the condition is required 19
to confirm these findings, particularly the possible association with cardiovascular disease. 20
21
Page 28 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
4
1
Strengths and limitations of this study 2
• This is the first meta-analysis of the literature for the global epidemiology of primary 3
Raynaud’s phenomenon (PRP). 4
• The prevalence and incidence of PRP in different countries were estimated. Female 5
gender, positive family history, smoking and migraines were found to be the major risk 6
factors for PRP. 7
• The lack of original data restricted an adequate estimation of the age-effect on PRP. 8
• Different definitions of PRP handicapped a comparison between countries 9
10
INTRODUCTION 11
In the 19th century, Maurice Raynaud first described Raynaud’s phenomenon (RP) as an 12
episodic, symmetrical, vasospastic disorder resulting in classic triphasic colour change, 13
trophic changes limited to the skin and uncomfortable sensory symptoms of the extremities 14
in the absence of arterial occlusion.[1] Further criteria have been suggested to distinguish 15
Primary RP (PRP) from secondary RP which include detail regarding symptom duration, 16
negative autoimmune serology, normal serum inflammatory markers and capillaroscopy, 17
and the clinical absence of any underlying disease.[1-4] Use of colour charts to aid 18
diagnosis has also been used.[4, 5] Despite this, there is no unifying definition that is used 19
worldwide for PRP. 20
21
There have been a number of studies performed in various countries reporting the 22
prevalence of RP. The reported prevalence ranges from less than 1% (in men) and up to 23
20% (in women) depending on definitions and population selected.[6] In contrast, few 24
studies have examined the incidence of PRP and the true burden of PRP in the general 25
population remains unclear. PRP is thought to be more common in women, particularly 26
when it develops at a young age.[7] There are also reports of a hereditary component and 27
Page 29 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
5
links with other vasospastic conditions such as migraine.[8-11] It is uncertain whether other 1
co-morbidities or risk factors particularly related to vascular diseases such as ischaemic 2
heart disease and/or smoking have an association with PRP. 3
4
The primary objective of this study was to perform a systematic review of observational 5
studies to summarise the literature with regard to the prevalence, incidence and risk 6
factors/associations of PRP. The secondary objective was to examine the current definitions 7
used to define PRP worldwide. 8
METHODS 9
1: Literature search – data sources and search strategy 10
A comprehensive systematic literature search was undertaken in June 2011 and re-run in 11
October 2014 using five databases: Medline, Embase, Cinahl, Amed and Pubmed. The 12
search terms for “Raynauds” or “Raynauds disease” were combined with the terms 13
“epidemiology” , “prevalence”, “risk” or “incidence” to generate the citations (see Appendix 14
1 for full details of search strategy). “Cross sectional”, “case-control” or “cohort” studies and 15
“systematic review” were also applied for types of studies. 16
Abstracts were reviewed and the full papers were sought where abstracts were felt to be 17
relevant. Any duplicate articles were excluded (Figure 1). Where there was difficulty in 18
article retrieval, the authors were contacted via email. The literature search and abstract 19
review was completed by RG and validated by WZ. Reference lists of the review articles 20
were also examined for relevant studies. 21
22
Page 30 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
6
2: Inclusion and Exclusion Criteria 1
Inclusion criteria: studies reporting the prevalence and/or incidence of PRP; studies 2
reporting potential risk factors associated with PRP; studies reporting human data on PRP in 3
people of any age; studies in any language (4 articles required translation – 1 Japanese, 1 4
Turkish, 1 French, 1 Italian). 5
Exclusion criteria (Figure 1): studies assessing treatment of PRP; studies involving 6
participants with RP secondary to other diseases; studies assessing RP in a specific 7
occupation e.g., people using vibration tools; unpublished material, case reports, editorials, 8
letters or reviews. 9
3. Data extraction and quality assessment 10
Study characteristics including age range, gender ratio and total number of participants in 11
the study were documented. The study design, country, setting (i.e. hospital or community 12
based) were also assessed and noted. If more than one article used the same study 13
population, the article where the data was felt to be presented most clearly was used in the 14
study. The definition of PRP and instruments used to confirm the condition were also 15
documented. The number of cases of PRP out of the number of people studied in a certain 16
time in the general population was documented as unadjusted crude prevalence. Incidence 17
figures were documented if the number of new cases of PRP in the population at risk 18
studied over a given period of time was stated. 19
Individual odds ratio (OR), relative risk (RR) or hazard ratio (HR) and their 95%confidence 20
interval (CI) were extracted or calculated for the following: 21
Page 31 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
7
o Constitutional: age, gender 1
o Environmental: employment, education, marital status, sex hormone 2
medications 3
o Genetic: family history in 1st
degree relatives 4
o Associations: smoking, alcohol, cardiovascular disease, migraine 5
6
All studies were reviewed by RG to assess study quality and for data extraction and were 7
validated by WZ. An independent reviewer (RK) assessed a random selection of articles to 8
ensure quality of data extraction. Study quality was assessed according to study design 9
(cohort, cross-sectional and case control), setting (community or hospital), sample size, case 10
definition, exposure definition, confounding factors and adjustment. Quality scoring for 11
studies was not performed as it is not possible or fair to assign equal weight to different 12
quality aspects related to the study. However, current consensus standards of reporting 13
meta-analysis of observational studies in epidemiology (MOOSE) [12] were followed, and 14
subgroup/sensitivity analysis was undertaken to examine the changes of the estimate 15
according to different quality aspects 16
4. Statistical analysis 17
Individual data for prevalence and incidence were derived from the original report either 18
directly or indirectly from the information provided in each study. The pooled proportion 19
was calculated as the back-transform of the weighted mean of the transformed proportion, 20
using inverse arcsine variance weights for the fixed effects model and DerSimonian-Laird 21
(1986) weights for the random effects model. [13, 14] Cumulative incidence and 95%CI were 22
Page 32 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
8
transformed into incidence rate data (i.e., incidence per 100 person-years) and pooled 1
incidence rate was estimated. Individual data for OR, RR and HR were pooled to present 2
the overall relative risk of all observational studies, as well as separately for each specific 3
risk measure or study design as appropriate. Random-effects mode was used to pool the 4
data.[15] Heterogeneity was examined using Forest plots, Cochran Q tests and I2
statistic as 5
a measure for inconsistency due to chance.[16, 17] Publication bias was assessed using 6
funnel plots and Eggers test or the Harbord test if the number of studies included in the 7
meta-analysis was too small (≤4).[18] All analyses were undertaken using StatsDirect© 8
Version 2.7.9. 9
10
RESULTS 11
1: Study characteristics 12
2378 citations were found in the initial literature search. 467 duplicates were removed and 13
1871 citations were excluded as they did not meet the inclusion criteria (Figure 1). The final 14
number of studies available for analysis was 33 (33, 733 subjects). There were 2 cohort 15
studies[19, 20] (1, 632 subjects), 17 cross-sectional studies[6, 21-36] (25, 797 subjects) and 16
14 case-control studies[7-11, 37-45] (6, 304 subjects) (Table 1). Data for incidence and 17
prevalence were taken from cohort and cross-sectional studies respectively. Data for risk 18
factors were taken from all studies as long as the results were reported. 19
Age ranges across different study designs were as follows: case-control (16-79 years), cohort 20
(18-81 years), cross sectional (12-84 years). 67% of the studies involved participants 21
recruited in a community based setting. The majority of studies were conducted in Europe 22
Page 33 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
9
(18)[6, 9, 19, 22, 24, 26, 27, 29, 30, 32, 33, 35-37, 39, 41-43] or the USA (10)[7-8, 10-11, 20-1
21, 23, 38, 40, 44], however other countries of origin included Japan (2)[25, 28], New 2
Zealand (1)[34] and Israel (1)[45]. One comparison study included participants from USA and 3
France.[31] 4
Participants were surveyed by means of phone, face-to-face interview, and/or postal 5
questionnaire. 26 studies included a physical examination which also included blood testing 6
(including serology), nail fold capillaroscopy and use of colour chart/photographs (Table 1) 7
10 studies used specific criteria to define PRP (3 studies [8, 21, 32] Allen & Brown[1], 3[9, 8
36, 37]Leroy & Medsger[2], 4[6, 22, 33-34] UK Scleroderma Study Group[4]). The remaining 9
studies used a combination of cold sensitivity, varying degrees of colour change and sensory 10
symptoms via questionnaire or interview to define PRP. Colour charts or photographs to 11
indicate colour change were used in 12 studies[6-7, 9-10, 19-20, 25, 28-29, 31, 33, 35] and 12
nailfold capillaroscopy was performed as part of the examination in 10 studies.[8-9, 19, 31, 13
36, 37, 39, 41-43] In 15 studies, blood testing including serology and/or inflammatory 14
markers were performed.[6, 8-9, 11, 24, 30, 33, 36-37, 39-44] 15
Studies with clear definition of PRP or clear exclusion criteria for secondary RP were 16
categorised as “definite PRP” in this study. Studies with less clear definition of PRP were 17
categorised as “possible PRP”. Studies with clear definition of secondary RP were excluded. 18
Page 34 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
10
2: Prevalence of PRP 1
The overall prevalence for definite PRP varied from 1.6 – 7.2% in 6 cross sectional studies in 2
the general population (women: 2.1-15.8% and men 0.8-6.5%).[21, 23, 25, 27, 29, 33] The 3
pooled prevalence was 4.85% (95% CI 2.08%, 8.71%) (Figure 2), with 5.74% (95% CI 2.74, 4
9.75) in women and 4.12% (95% CI 1.60, 7.74) in men. We used the Harbord test to detect 5
publication bias (1.59 92.5% CI -21.6,24.8, P=0.87) 6
The overall prevalence for possible PRP ranges from 3.98% to 12.7% (women: 4.5-17.9% and 7
men: 3.4-7.2%) in three cross sectional studies.[26, 34-35] The prevalence in specific 8
populations varies depending on the studies (Table 2) 9
In 6 studies assessing the general population we found the lowest prevalence of PRP in 10
Japan with an overall prevalence of 1.6 (2.1% in women, 1.1% in men).[25] Highest overall 11
prevalence figures were found in the USA with a median prevalence of 7.5% (7.8% in 12
women, 5.8% in men,).[21, 23] A study from France also showed high prevalence figures of 13
11.75% in women and 6.3% in men (median values).[31] (Table 3) 14
Five studies reported prevalence of PRP by age.[6, 28-30, 34]. Three did not find any age-related 15
prevalence (Leppert1987, Iwata 1987 and Voulgari 2000). Purdie (2009) reported a higher 16
prevalence of PRP in younger compared to older age groups, whereas Fraenkel (1999) reported 17
higher prevalence in older age groups in men (adjusted OR=2.3, 95%CI 1.0 to 5.2 highest vs. lowest 18
tertile) but not in women (adjusted OR=0.9, 95%CI 0.4 to 1.6). Jones (2003) also showed a slight 19
increase in prevalence by age in yearly increments between ages 12-15 years. 20
21
22
Page 35 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
11
3: Incidence of Primary Raynauds Phenomenon 1
Only two studies reported incidence rates.[19-20] Carpentier et al reported an annual 2
incidence rate of 0.25% (95% CI 0.17, 0.33), with 0.24% in women and 0.26% in men and 3
Suter et al reported a 7-year incidence of 1.87% (2.2% in women and, 1.5% in men), which 4
was converted to an annual incidence rate of 0.26% (95%CI 0.17, 0.39). The pooled annual 5
incidence rate of these two studies was therefore 0.25% (95%CI 0.19, 0.32). 6
7
4: Risk factors and associations 8
In 18 studies (23, 197 participants), there was a positive association between female gender 9
and PRP (OR 1.65, 95% CI 1.42, 1.91).[6-7, 9, 20-29, 33-35, 37, 44] Family history, assessed in 10
2 studies looking at 1st degree relatives, also had a positive significant association with PRP 11
(OR 16.6, 95%CI 7.44, 36.8).[8-9] No significant association was found with education 12
beyond primary school age.[6, 37] (Table 4). Manual occupation (not including vibration 13
tool use) had an OR of 2.66 (95% CI 1.73, 4.08) in 1 study of 3873 participants.[25] In 4 14
studies, being married was associated with a lower risk of PRP with OR of 0.60 (95% CI 0.43, 15
0.83) compared with being single/divorced/widowed.[6-7, 23, 37] Smoking was found to 16
have an association in 9 studies giving a pooled OR of 1.27 (95% CI 1.06, 1.53).[7, 9-11, 20, 17
22-23, 32, 44] Alcohol use,[23, 44] participants with positive Helicobacter Pylori 18
investigations[39, 41] and those with conditions such as diabetes,[23] hypertension[11, 23] 19
and hypercholesterolaemia[23] did not have a significant association with PRP. 20
Migraine had a positive significant association with a pooled OR of 4.02 (95% CI 2.62, 6.17) 21
in 6 studies.[6, 9-11, 22, 45] One study of 3442 participants reported a positive association 22
Page 36 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
12
of cardiovascular disease with PRP with an OR of 1.69 (95% CI 1.22, 2.34).[44] 1
Cardiovascular disease in this study included a history of ischaemic heart disease, 2
intermittent claudication, congestive cardiac failure and cerebrovascular disease. A single 3
study using 81 participants did not show a positive significant association of coronary heart 4
disease with PRP.[40] 5
A positive association was found in participants taking oestrogen replacement therapy alone 6
in two studies with an OR of 2.34 (95% CI 1.42, 3.84).[23, 38] However no significant 7
association was found in combined oestrogen and progesterone replacement therapy[38] in 8
postmenopausal women or in oral contraceptive pill[10-11] use in two other studies. A 9
study by Smyth et al looking at allele frequencies of known polymorphisms of candidate 10
vasoactive mediator genes (eNOS, BKRG, ET01 and ETA receptor genes) did not show any 11
association.[9] Shemirani et al looked at clotting factors in participants with PRP and found a 12
significant association with methyltetrahydrofolate reductase C677T mutations (OR 0.4, 95% 13
CI 0.2, 0.9) but no difference in other thrombosis-associated alleles (FVLeiden, prothrombin 14
G20210A).[42] 15
16
DISCUSSION 17
This is the first meta-analysis of the literature for the prevalence, incidence, risk factors and 18
associations of PRP. Overall the pooled mean prevalence of PRP in the general population 19
was 4.85% (95% CI 2.08%, 8.71%) (Figure 2) and the mean incidence was 0.25% (95% CI 20
0.17, 0.33) per annum.[19] Major risk factors/associations of PRP include female gender, 21
Page 37 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
13
family history of PRP, migraine, smoking, cardiovascular disease, manual occupation, 1
oestrogren replacement therapy and possibly marital status. (Table 4). 2
Variations in prevalence were observed between countries (Table 3) though this could 3
reflect use of different diagnostic criteria rather than real differences in prevalence. The 4
heterogeneity of prevalence figures may also reflect the differences in the way the studies 5
were conducted, the selection of participants (e.g., age and gender), and the disease 6
definition. All studies (except for Maricq 1997) demonstrate a higher prevalence of PRP in 7
women. This may be due to a relationship with female hormones as two studies found an 8
association between PRP and use of oestrogen replacement therapy alone,[23, 38] although 9
no association was found between combined oestrogen and progesterone replacement or 10
the oral contraceptive pill.[10-11, 38] In contrast, prevalence of PRP does not increase with 11
age in five published studies with a wide age range of participants from 12 years up to 84 12
years.[6, 28-30, 34] This accords with the clinical observation that PRP usually starts in 13
teenage years and that later development, which is far less common, is characteristic of 14
secondary RP. While the former may be driven predominantly by genetic risk factors, later 15
onset “primary” Raynaud’s may be predominantly influenced by environmental exposures 16
such as vascular microtrauma from manual usage and vibrating tools. In terms of other 17
environmental factors we did find a weak negative association between marital status and 18
PRP with an OR of 0.60 (95%CI 0.43, 0.83) in those that are married vs. 19
single/separated/widowed/divorced.[6-7, 23, 37] However, there is no plausible biological 20
explanation for this and the reported data may not be free from confounding bias. 21
The association of cardiovascular disease and autoimmune disease is well documented and 22
thought to be due to accelerated atherosclerosis as a result of chronic inflammation, 23
Page 38 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
14
treatment such as glucocorticoids as well as the traditional risk factors for cardiovascular 1
disease.[46-52] A link between cardiovascular disease and PRP has been shown in only one 2
study[44] and a reason for this association is not known. It is unlikely to be due to an 3
inflammatory process or related to medication and with PRP having predominance for the 4
female population and onset at a young age it not clear if traditional cardiovascular risk 5
factors play a part. However, smoking was found to have positive association with PRP in 6
our study (OR 1.27, 95% CI 1.06, 1.53). It is well known that smoking is one of three 7
(smoking, hypertension and hyperlipidaemia) main risk factors for cardiovascular and 8
cerebrovascular disease.[53-59] Smoking may be the same risk factor for PRP and CVD. 9
Whether smoking causes PRP first then CVD is an interesting question which deserves 10
further research. More interestingly, we found a very strong association between migraine 11
and PRP (OR 4.02, 95%CI 2.62, 6.17). It has been previously shown that migraine is due to a 12
cascade of vascular and neural events.[46-47] However, a review by Rosamund suggested 13
migraine was not shown to be linked with coronary heart disease but possibly shares a 14
common underlying pathophysiology with Raynaud’s phenomenon and other vasospastic 15
disorders such as variant angina.[60-61] It is thought there may be other factors that may 16
affect the underlying mechanism for these vasospastic conditions as episodes occur at 17
different times with differing precipitants.[62-63] Further study may help clarify whether 18
PRP is a benign vasospastic disorder or whether there is underlying pathology affecting the 19
vascular wall associated with traditional risk factors seen in cardiovascular disease. 20
There are number of caveats to this study. Firstly, it was striking that there was no uniform 21
definition for diagnosis of PRP. Only 39% of studies looking at prevalence had a precise 22
definition for PRP, thereby reducing the number of studies we used to assess pooled 23
Page 39 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
15
prevalence. It is possible that the variation in definition of PRP together with the way 1
participants were recruited and assessed may have led to under- or over-estimation of the 2
true prevalence of PRP in the general population. We feel that an amalgamation of the 3
generally more commonly used definitions would ensure that the diagnosis is clear by 4
assessing symptoms, using colour chart or photographs for confirmation of colour change 5
and carefully exclude underlying conditions including checking for digital infarcts/ulceration, 6
nailfold capillaroscopy and assessing autoimmune screen and inflammatory markers. 7
Secondly, as our objective was to specifically examine the epidemiology of PRP a large 8
proportion of studies were excluded because they focused on secondary Raynaud’s 9
phenomenon, especially related to connective tissue diseases and vibration white finger. In 10
addition we also excluded studies that looked at investigation or treatment of PRP. This left 11
only a small number of studies to assess. From the studies included, there was a great deal 12
of variation in the population of participants used. 9 out of the 17 studies used investigated 13
participants in the general population whereas the remainder examined specific populations 14
such as single gender, children or hospital/medical personnel. Furthermore, there was 15
considerable variation in the risk factors addressed in each study and this may have affected 16
the significance and association, or lack of association between the risk factors and PRP. We 17
tried to extract as many risk factors from each study as possible to use in our analysis. In the 18
future, a larger multinational population study may help us to get a better understanding of 19
the disease. This would be particularly useful if standardised criteria were used to include 20
participants in the studies, using strict definition for PRP (as mentioned previously) and data 21
was collected in a similar fashion assessing a wide variety of possible risk factors 22
Page 40 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
16
(particularly related to cardiovascular disease and vasospastic disoders) for more accurate 1
data analysis. 2
3
CONCLUSION 4
This first systematic review summarises the burden of PRP in the general population using 5
published literature. It is not a rare condition (prevalence 4.85% and annual incidence 6
0.25%). It starts at a young age, is more common in women and associates with a family 7
history and with smoking. In addition, people with PRP are 4 times more likely to have 8
migraine than those without this condition. 9
10
ACKNOWLEDGEMENT: Our sincere thank you to Joanna Ramowski and Helen Richardson for 11
article retrieval and support. Also special thank you to Anu Suokas, Karin Tatsumoa, 12
Professor Tiraje Truncer, Ana Valdes and Maggie Wheeler for language translation. 13
14
AUTHOR CONTRIBUTIONS 15
Study conception and design: Dr Zhang, Professor Doherty, Dr Lanyon, Dr Garner 16
Acquision of data: Dr Garner, Dr Kumari, Dr Zhang 17
Statistical Analysis: Dr Garner, Dr Zhang 18
Analysis and interpretation of data: Dr Garner, Dr Zhang, Professor Doherty, Dr Lanyon 19
Manuscript preparation and final approval of manuscript: Dr Garner, Dr Zhang, Professor 20
Doherty, Dr Lanyon 21
Page 41 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
17
Funding No funding 1
Competing interests None 2
Ethical approval and patient consent Not required 3
Data sharing statement No unpublished data were used in this study. No additional data 4
available. 5
6
7
8
9
10
11
Page 42 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
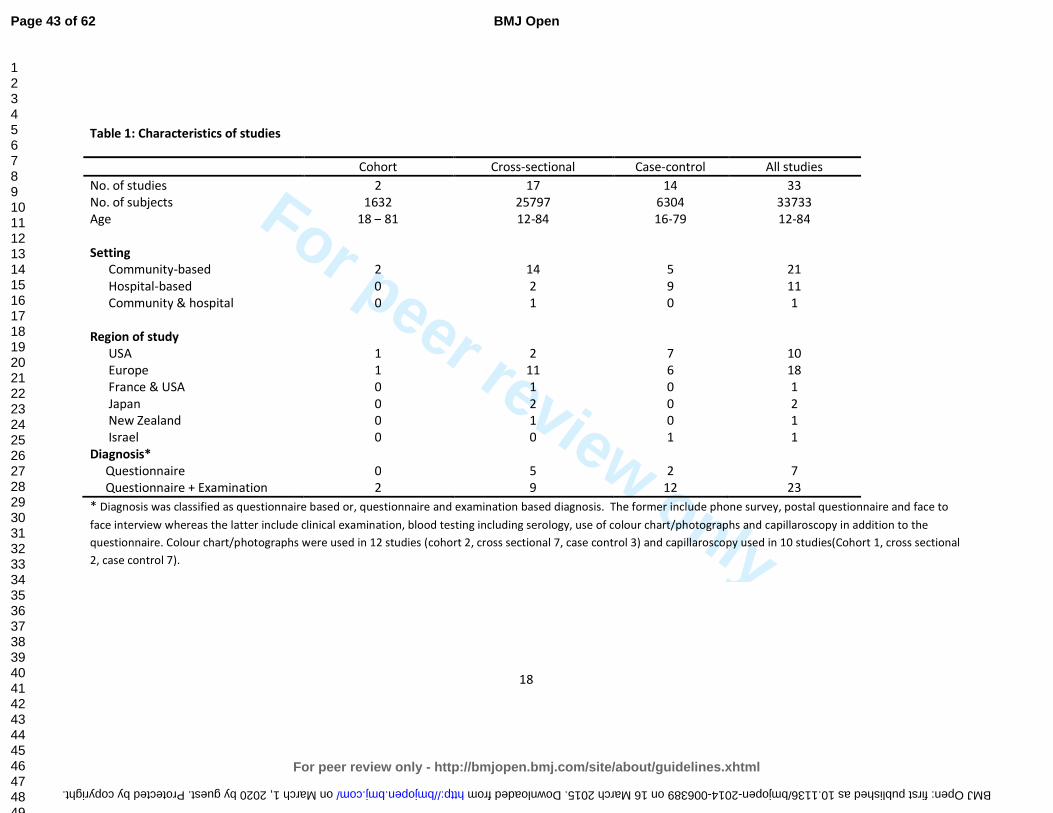
For peer review only
18
Table 1: Characteristics of studies
Cohort Cross-sectional Case-control All studies
No. of studies 2 17 14 33
No. of subjects 1632 25797 6304 33733
Age 18 – 81 12-84 16-79 12-84
Setting
Community-based 2 14 5 21
Hospital-based 0 2 9 11
Community & hospital 0 1 0 1
Region of study
USA 1 2 7 10
Europe 1 11 6 18
France & USA 0 1 0 1
Japan 0 2 0 2
New Zealand 0 1 0 1
Israel 0 0 1 1
Diagnosis*
Questionnaire 0 5 2 7
Questionnaire + Examination 2 9 12 23
* Diagnosis was classified as questionnaire based or, questionnaire and examination based diagnosis. The former include phone survey, postal questionnaire and face to
face interview whereas the latter include clinical examination, blood testing including serology, use of colour chart/photographs and capillaroscopy in addition to the
questionnaire. Colour chart/photographs were used in 12 studies (cohort 2, cross sectional 7, case control 3) and capillaroscopy used in 10 studies(Cohort 1, cross sectional
2, case control 7).
Page 43 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
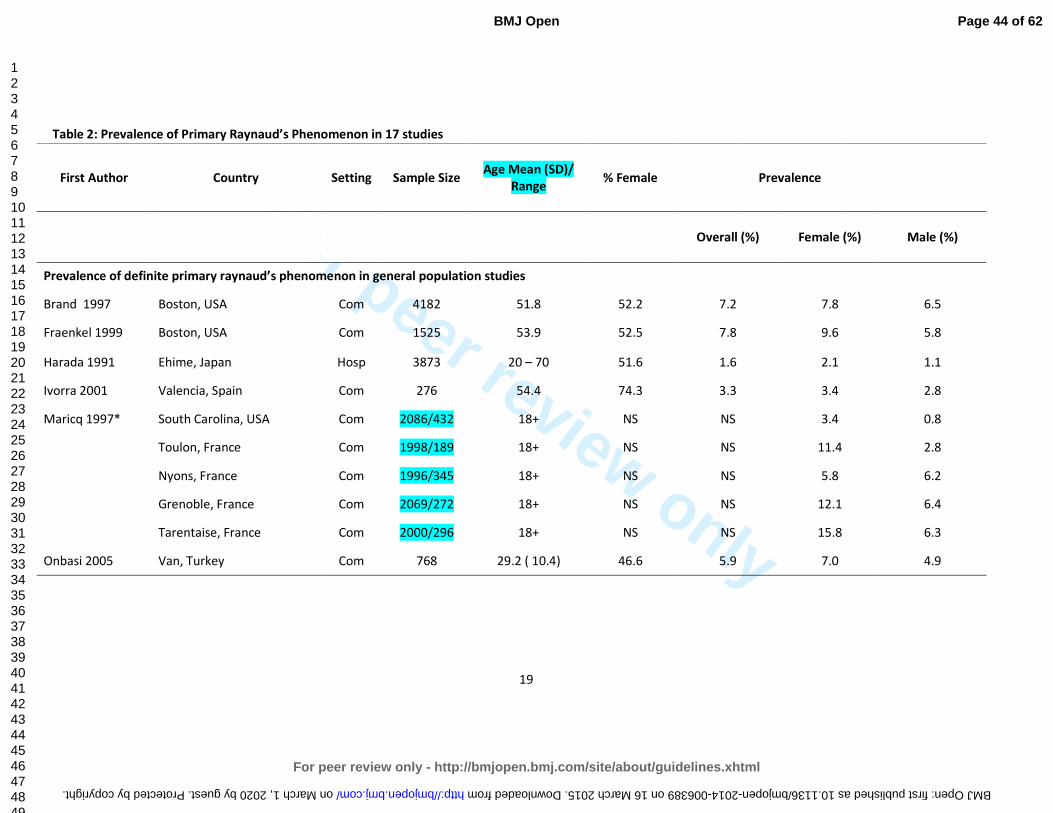
For peer review only
19
Table 2: Prevalence of Primary Raynaud’s Phenomenon in 17 studies
First Author Country Setting Sample Size
Age Mean (SD)/
Range
% Female
Prevalence
Overall (%)
Female (%) Male (%)
Prevalence of definite primary raynaud’s phenomenon in general population studies
Brand 1997 Boston, USA Com 4182 51.8 52.2 7.2 7.8 6.5
Fraenkel 1999 Boston, USA Com 1525 53.9 52.5 7.8 9.6 5.8
Harada 1991 Ehime, Japan Hosp 3873 20 – 70 51.6 1.6 2.1 1.1
Ivorra 2001 Valencia, Spain Com 276 54.4 74.3 3.3 3.4 2.8
Maricq 1997* South Carolina, USA Com 2086/432 18+ NS NS 3.4 0.8
Toulon, France Com 1998/189 18+ NS NS 11.4 2.8
Nyons, France Com 1996/345 18+ NS NS 5.8 6.2
Grenoble, France Com 2069/272 18+ NS NS 12.1 6.4
Tarentaise, France Com 2000/296 18+ NS NS 15.8 6.3
Onbasi 2005 Van, Turkey Com 768 29.2 ( 10.4) 46.6 5.9 7.0 4.9
Page 44 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
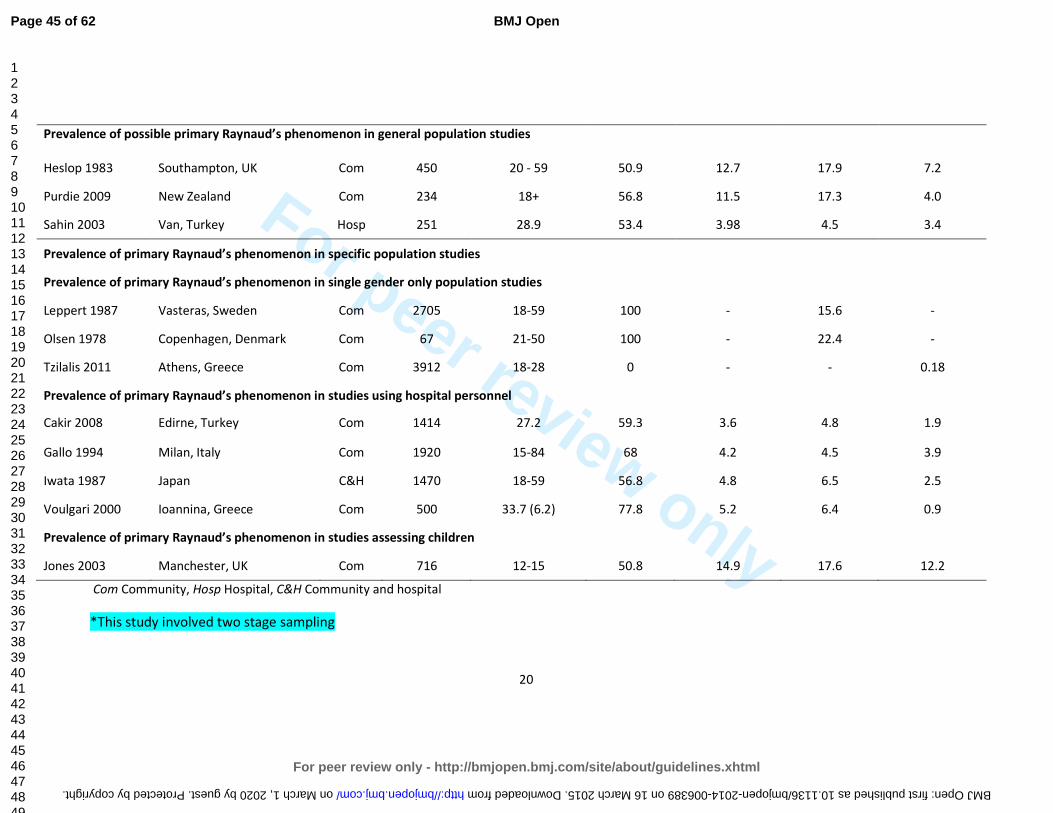
For peer review only
20
Prevalence of possible primary Raynaud’s phenomenon in general population studies
Heslop 1983 Southampton, UK Com 450 20 - 59 50.9 12.7 17.9 7.2
Purdie 2009 New Zealand Com 234 18+ 56.8 11.5 17.3 4.0
Sahin 2003 Van, Turkey Hosp 251 28.9 53.4 3.98 4.5 3.4
Prevalence of primary Raynaud’s phenomenon in specific population studies
Prevalence of primary Raynaud’s phenomenon in single gender only population studies
Leppert 1987 Vasteras, Sweden Com 2705 18-59 100 - 15.6 -
Olsen 1978 Copenhagen, Denmark Com 67 21-50 100 - 22.4 -
Tzilalis 2011 Athens, Greece Com 3912 18-28 0 - - 0.18
Prevalence of primary Raynaud’s phenomenon in studies using hospital personnel
Cakir 2008 Edirne, Turkey Com 1414 27.2 59.3 3.6 4.8 1.9
Gallo 1994 Milan, Italy Com 1920 15-84 68 4.2 4.5 3.9
Iwata 1987 Japan C&H 1470 18-59 56.8 4.8 6.5 2.5
Voulgari 2000 Ioannina, Greece Com 500 33.7 (6.2) 77.8 5.2 6.4 0.9
Prevalence of primary Raynaud’s phenomenon in studies assessing children
Jones 2003 Manchester, UK Com 716 12-15 50.8 14.9 17.6 12.2
Com Community, Hosp Hospital, C&H Community and hospital
*This study involved two stage sampling
Page 45 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from

For peer review only
21
Table 3: Regional variation of prevalence of primary raynaud’s phenomenon for general population studies including prevalence rates for males and 1
females 2
3
Country No. Of Studies No. Of
Participants
Prevalence %
Male Female Total
USA† 3 6139 5.8 7.8 7.5
France† 1 1102 6.3 11.75 -
Spain 1 276 2.8 3.4 3.3
Turkey 1 768 4.9 7.0 5.9
Japan 1 3873 1.1 2.1 1.6
TOTAL 6 12158
† Median values calculated for prevalence. USA gender figures include data from Maricq 1997 (France & USA). Total USA prevalence figure includes data 4
from 2 USA only studies 5
6
7
8
9
10
11
12
13
Page 46 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
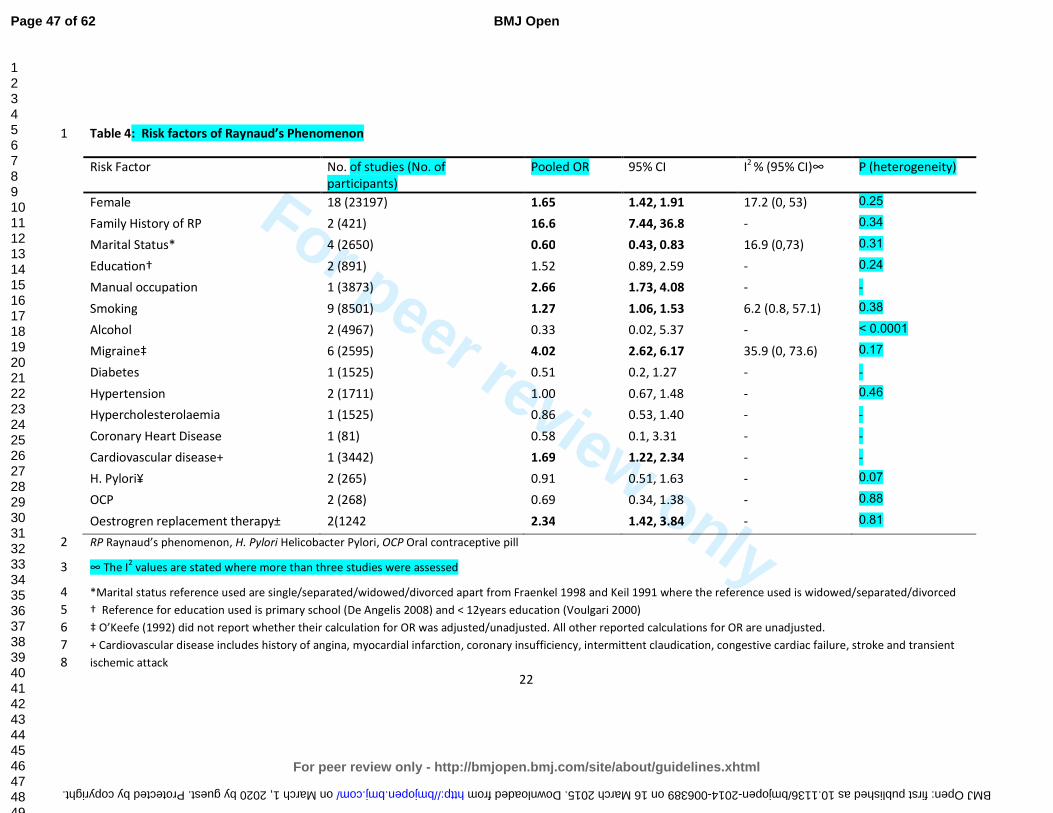
For peer review only
22
Table 4: Risk factors of Raynaud’s Phenomenon 1
Risk Factor No. of studies (No. of
participants)
Pooled OR 95% CI I2
% (95% CI)∞
P (heterogeneity)
Female 18 (23197) 1.65 1.42, 1.91 17.2 (0, 53) 0.25
Family History of RP 2 (421) 16.6 7.44, 36.8 - 0.34
Marital Status* 4 (2650) 0.60 0.43, 0.83 16.9 (0,73) 0.31
EducaWon† 2 (891) 1.52 0.89, 2.59 - 0.24
Manual occupation 1 (3873) 2.66 1.73, 4.08 - -
Smoking 9 (8501) 1.27 1.06, 1.53 6.2 (0.8, 57.1) 0.38
Alcohol 2 (4967) 0.33 0.02, 5.37 - < 0.0001
Migraine‡ 6 (2595) 4.02 2.62, 6.17 35.9 (0, 73.6) 0.17
Diabetes 1 (1525) 0.51 0.2, 1.27 - -
Hypertension 2 (1711) 1.00 0.67, 1.48 - 0.46
Hypercholesterolaemia 1 (1525) 0.86 0.53, 1.40 - -
Coronary Heart Disease 1 (81) 0.58 0.1, 3.31 - -
Cardiovascular disease+ 1 (3442) 1.69 1.22, 2.34 - -
H. Pylori¥ 2 (265) 0.91 0.51, 1.63 - 0.07
OCP 2 (268) 0.69 0.34, 1.38 - 0.88
Oestrogren replacement therapy± 2(1242 2.34 1.42, 3.84 - 0.81
RP Raynaud’s phenomenon, H. Pylori Helicobacter Pylori, OCP Oral contraceptive pill 2
∞ The I2 values are stated where more than three studies were assessed 3
*Marital status reference used are single/separated/widowed/divorced apart from Fraenkel 1998 and Keil 1991 where the reference used is widowed/separated/divorced 4
† Reference for education used is primary school (De Angelis 2008) and < 12years education (Voulgari 2000) 5
‡ O’Keefe (1992) did not report whether their calculation for OR was adjusted/unadjusted. All other reported calculations for OR are unadjusted. 6
+ Cardiovascular disease includes history of angina, myocardial infarction, coronary insufficiency, intermittent claudication, congestive cardiac failure, stroke and transient 7
ischemic attack 8
Page 47 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
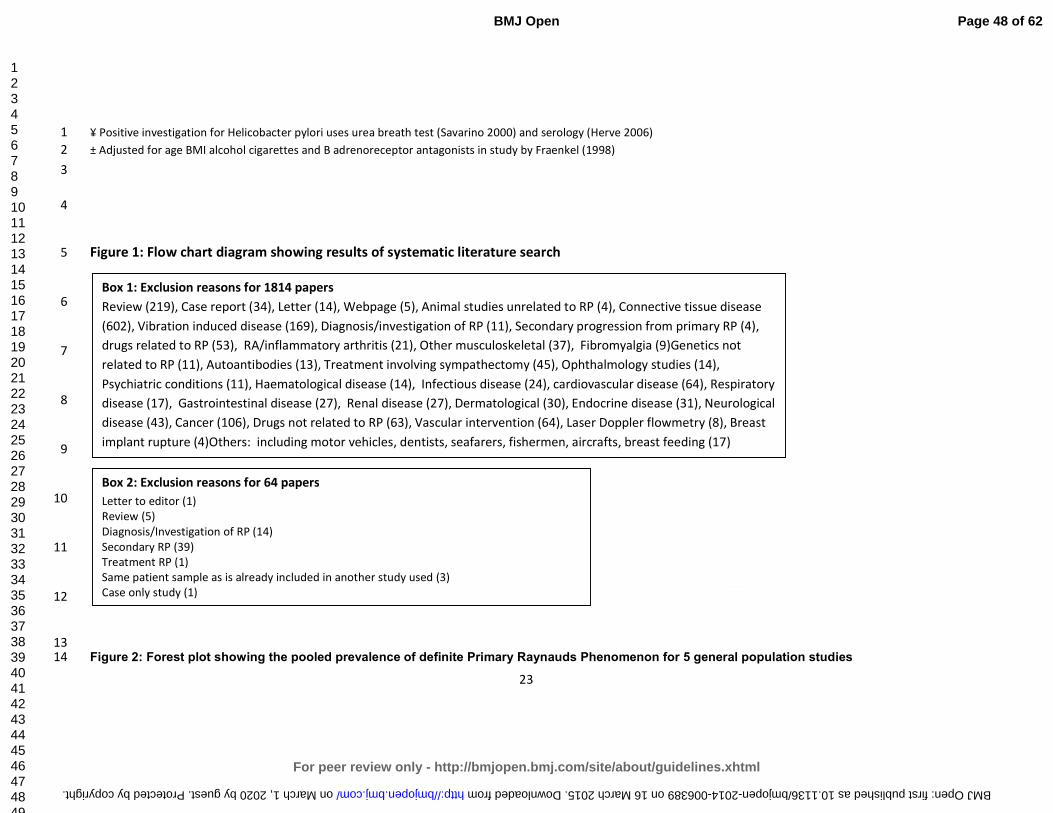
For peer review only
23
¥ Positive investigation for Helicobacter pylori uses urea breath test (Savarino 2000) and serology (Herve 2006) 1
± Adjusted for age BMI alcohol cigarettes and B adrenoreceptor antagonists in study by Fraenkel (1998) 2
3
4
Figure 1: Flow chart diagram showing results of systematic literature search 5
6
7
8
9
10
11
12
13 Figure 2: Forest plot showing the pooled prevalence of definite Primary Raynauds Phenomenon for 5 general population studies14
Box 1: Exclusion reasons for 1814 papers
Review (219), Case report (34), Letter (14), Webpage (5), Animal studies unrelated to RP (4), Connective tissue disease
(602), Vibration induced disease (169), Diagnosis/investigation of RP (11), Secondary progression from primary RP (4),
drugs related to RP (53), RA/inflammatory arthritis (21), Other musculoskeletal (37), Fibromyalgia (9)Genetics not
related to RP (11), Autoantibodies (13), Treatment involving sympathectomy (45), Ophthalmology studies (14),
Psychiatric conditions (11), Haematological disease (14), Infectious disease (24), cardiovascular disease (64), Respiratory
disease (17), Gastrointestinal disease (27), Renal disease (27), Dermatological (30), Endocrine disease (31), Neurological
disease (43), Cancer (106), Drugs not related to RP (63), Vascular intervention (64), Laser Doppler flowmetry (8), Breast
implant rupture (4)Others: including motor vehicles, dentists, seafarers, fishermen, aircrafts, breast feeding (17)
Box 2: Exclusion reasons for 64 papers
Letter to editor (1)
Review (5)
Diagnosis/Investigation of RP (14)
Secondary RP (39)
Treatment RP (1)
Same patient sample as is already included in another study used (3)
Case only study (1)
Page 48 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
24
REFERENCES
1 Allen E, Brown G. Raynaud disease: A critical review of minimal requisites for diagnosis. Am J Med
Sci 1932;183(2):187-200.
2 LeRoy E, Medsger T. Raynaud’s phenomenon: a proposal for classification. Clin Exp Rheumatol
1992;10:485-488.
3 Bowling J, Dowd P. Raynaud’s disease. Lancet 2003;361:2078-80.
4. Brennan P, Silman A, Black C, et al. Validity and reliability of three methods used in the diagnosis
of Raynaud's phenomenon. The UK Scleroderma Study Group. Br J Rheumatol 1993;32(5):357-61.
5 Maricq H, Weinrich M. Diagnosis of Raynaud’s phenomenon assisted by colour charts. J Rheumatol
1988;15(3):454-459.
6 Voulgari P, Alamanos Y, Papazisi D, et al. Prevalence of Raynaud's phenomenon in a healthy Greek
population. Ann Rheum Dis 2000;59(3):206-210.
7 Keil J, Maricq H, Weinrich M, et al. Demographic, social and clinical correlates of Raynaud
phenomenon. Int J Epidemiol 1991;20(1):221-224.
8 Freedman R, Mayes M. Familial aggregation of primary Raynaud's disease. Arthritis and
Rheumatism 1996;39(7):1189-1191.
9 Smyth AE, Hughes AE, Bruce IN, Bell AL. A case-control study of candidate vasoactive mediator
genes in primary Raynaud's phenomenon. Rheumatology (Oxford) 1999;38(11):1094-1098.
10 O'Keeffe S, Tsapatsaris N, Beetham W. Association between Raynaud's phenomenon and
migraine in a random population of hospital employees. J Rheumatol 1993;20(7):1187-1188.
11 O'Keeffe S, Tsapatsaris N, Beetham W. Increased prevalence of migraine and chest pain in
patients with primary Raynaud disease. Ann Intern Med 1992;116(12 Pt 1):985-989.
12 Stroup D, Berlin J, Morton S, et al. Meta-analysis of Observational Studies in Epidemiology
(Moose) group. JAMA 2000;283:2008-2012.
13 DerSimonian R, Laird N. Meta-analysis in Clinical Trials. Controlled Clinical Trials 1986;7:177-188.
14 Stuart A, Ord JK. Kendall's Advanced Theory of Statistics (6th edition). London: Edward Arnold
1994.
15 Whitehead A, Whitehead J. A general parametric approach to the meta-analysis of randomised
clinical trials. Stat Med 1991;10:1665-77.
16 Gavaghan D, Moore R, McQuay H. An evaluation of homogeneity tests in meta-analyses in pain
using simulations of individual patient data. Pain 2000;85:415-24.
17 Higgins J, Thomspon S, Deeks J, et al. Measuring inconsistency in meta-anlyses. BMJ
2003;327:557-60.
18 Egger M, Davey Smith G, Schneider M, et al. Bias in meta-anlysis detected by a simple, graphical
test. BMJ 1997;315:629-34.
19 Carpentier P, Satger B, Poensin D, et al. Incidence and natural history of Raynaud phenomenon: a
long-term follow-up (14 years) of a random sample from the general population. J Vasc Surg 2006;
44(5):1023-1028.
20 Suter L, Murabito J, Felson D, et al. The incidence and natural history of Raynaud's phenomenon
in the community. Arthritis Rheum 2005; 52(4):1259-1263.
21 Brand F, Larson M, Kannel W, et al. The occurrence of Raynaud's phenomenon in a general
population: the Framingham Study. Vasc Med 1997;2(4):296-301.
22 Cakir N, Pamuk O, Donmez S, et al. Prevalence of Raynaud's phenomenon in healthy Turkish
medical students and hospital personnel. Rheumatol Int 2008; 29(2):185-188.
23 Fraenkel L, Zhang Y, Chaisson C F et al. Different factors influencing the expression of raynaud's
phenomenon in men and women. Arthritis Rheum 1999;42(2):306-310.
24 Gallo E, Bianchi E, Motta A, et al. [The incidence of Raynaud's phenomenon in 1920 residents in
Milan]. [Italian] Incidenza del fenomeno di Raynaud in 1920 residenti in Milano. Minerva
Cardioangiol 1994;42(1-2):65-71.
Page 49 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
25
25 Harada N, Ueda A, Takegata S. Prevalence of Raynaud's phenomenon in Japanese males and
females. J Clin Epidemiol 1991;44(7):649-655.
26 Heslop J, Coggon D, Acheson E. The prevalence of intermittent digital ischaemia (Raynaud's
phenomenon) in a general practice. J R Coll Gen Pract 1983;33(247):85-89.
27 Ivorra J, Perales J, Carballido C, et al. Prevalence of Raynaud's phenomenon in general practice in
the East of Spain. Clin Rheumatol 2001;20(2):88-90.
28 Iwata H, Makimo S, Miyashita K. [Prevalence of Raynaud's phenomenon in individuals not using
vibrating tools]. Sangyo Igaku - Japanese Journal of Industrial Health 1987;29(6):500-503.
29 Jones G, Herrick A, Woodham S, et al. Occurrence of Raynaud's Phenomenon in Children Ages 12-
15 Years: Prevalence and Association with Other Common Symptoms. Arthritis Rheum
2003;48(12):3518-352.
30 Leppert J, Aberg H, Ringqvist I, et al. Raynaud's phenomenon in a female population: prevalence
and association with other conditions. Angiology 1987;38(12):871-877.
31 Maricq H, Carpentier P, Weinrich M, et al. Geographic variation in the prevalence of Raynaud's
phenomenon: A 5 region comparison. J Rheumatol 1997;24(5):879-889.
32 Olsen N, Nielsen S. Prevalence of primary Raynaud phenomena in young females. Scand J Clin Lab
Invest 1978;38(8):761-764.
33 Onbasi K, Sahin I, Onbasi O, et al. Raynaud's phenomenon in a healthy Turkish population. Clin
Rheumatol 2005;24(4):365-369.
34 Purdie G, Harrison A, Purdie D. Prevalence of Raynaud's phenomenon in the adult New Zealand
population. N Z Med J 2009;122(1306):55-62.
35 Sahin I, Onbasi K, Onbasi O, et al. Raynaud's Phenomenon in Healthy Population Who Admitted to
the Hospital in Van Region, Turkey [Turkish] Van Yoresinde Hastaneye Basvuran Saglikli
Populasyonda Raynaud Fenomeni. Ondokuz Mayis Universitesi Tip Dergisi 2003;20(2):73-77.
36 Tzilalis V, Panagiotopoulos N, Papatheodorou G, et al. Prevalence of Raynaud's phenomenon in
young Greek males. Clin Rheumatol 2011;30(1):57-59.
37 De Angelis R, Salaffi F, Grassi W. Health-related quality of life in primary Raynaud phenomenon. J
Clin Rheumatol 2008;14(4):206-210.
38 Fraenkel L, Zhang Y, Chaisson C, et al. The association of estrogen replacement therapy and the
Raynaud phenomenon in postmenopausal women. Ann Intern Med 1998;129(3):208-212.
39 Herve F, Cailleux N, Benhamou Y, et al. [Helicobacter pylori prevalence in Raynaud's disease].
[French] Prevalence des infections a Helicobacter pylori au cours de la maladie de Raynaud. Revue
de Medecine Interne 2006;27(10):736-741.
40 Koh K, Kim S, Lee K, et al. Does prevalence of migraine and Raynaud's phenomenon also increase
in Korean patients with proven variant angina? Int J Cardiol 1995; 51(1):37-46.
41 Savarino V, Sulli A, Zentilin P, et al. No evidence of an association between Helicobacter pylori
infection and Raynaud phenomenon. Scand J Gastroenterol 2000;35(12):1251-1254.
42 Shemirani A, Szomjak E, Balogh E, et al. Polymorphism of clotting factors in Hungarian patients
with Raynaud's. Blood Coagul Fibrinolysis 2011;22(1):56-59.
43 Susol E, MacGregor A, Barrett J, et al. A two-stage, genome-wide screen for susceptibility loci in
primary Raynaud's phenomenon. Arthritis Rheum 2000;43(7):1641-1646.
44 Suter L, Murabito J, Felson D, et al. Smoking, Alcohol Consumption, and Raynaud's Phenomenon
in Middle Age. Am J Med 2007;120(3):264-271.
45 Zahavi I, Chagnac A, Hering R, et al. Prevalence of Raynaud's phenomenon in patients with
migraine. Arch Intern Med 1984;144(4):742-744.
46 Shoenfeld Y, Gerli R, Doria A, et al. Accelerated atherosclerosis in autoimmune rheumatic
diseases. Circulation. 2005;112: 3337–3347.
47 Tyrrell P, Beyene J, Feldman B, et al. Rheumatic Disease and Carotid Intima-Media Thickness: A
Systematic Review and Meta-Analysis. Arterioscler Thromb Vasc Biol 2010;30:1014-1026.
Page 50 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
26
48 Schoenfeld S, Kasturi S, Costenbader K. The epidemiology of atherosclerotic cardiovascular
disease among patients with SLE: a systematic review. Semin Arthritis Rheum 2013:43(1):77-95 doi:
10.1016/j.semarthrit.2012.12.002. [published Online First 17 February 2013].
49 Peters M, Symmons D, McCarey D, et al. EULAR evidence-based recommendations for
cardiovascular risk management in patients with rheumatoid arthritis and other forms of
inflammatory arthritis. Ann Rheum Dis 2010;69: 325-331 doi: 10.1136/ard.2009.113696. [Published Online
First 22 September 2009].
50 Gabriel S, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and
comorbidity of the rheumatic diseases. Arthritis Res Ther 2009;11(3):229 doi: 10.1186/ar2669.
[published Online First 19 May 2009].
51 Lévy L, Fautrel B, Barnetche T, et al. Incidence and risk of fatal myocardial infarction and stroke
events in rheumatoid arthritis patients. A systematic review of the literature. Clin Exp Rheumatol
2008;26:673-9.
52 Avina-Zubieta J, Choi H, Sadatsafavi M, et al. Risk of cardiovascular mortality in patients with
rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum 2008;59:1690-7.
53 Burns D. Epidemiology of smoking-induced cardiovascular disease. Prog Cardiovasc
Dis. 2003;46(1):11-29.
54 De Backer G. Risk factors and prevention of cardiovascular disease: A review. Dialogues in
Cardiovascular Medicine 2008;13(2):83-99.
55 O’Donnell M, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic
stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010:376(9735):112-
123.
56 JBS3 Board. Joint British Societies’ consensus recommendations for the prevention of
cardiovascular disease (JBS3) Heart 2014;100(Suppl 2)::ii1–ii67.
57 British Cardiac Society, British Hyperlipidaemia Association, British Hypertension Society,
endorsed by the British Diabetic Association. Joint British recommendations on prevention of
coronary heart disease in clinical practice. Heart 1998;80(Suppl 2):S1–29.
58 Joint British Societies. JBS 2: Joint British Societies’ guidelines on prevention of
cardiovascular disease in clinical practice. Heart 2005;91(Suppl 5):v1–52.
59 Goff D, Lloyd-Jones D, Bennett G, et al. 2013 ACC/AHA guideline on the assessment of
cardiovascular risk: a report of the American College of Cardiology/American Heart Association task
force on practice guidelines. J Am Coll Cardiol 2014;63(25 Pt B):2935-59.
60 Gasparini C, Sutherland H, Griffiths L. Studies on the pathophysiology and genetic basis of
migraine. Curr Genomics 2013; 14:300-315.
61 Lipton R, Bigal M. Migraine: Epidemiology, impact and risk factors for progression. Headache
2005;45[Suppl 1]:S3-S13.
62 Rosamond W. Are migraine and coronary heart disease associated? An epidemiologic review.
Headache 2004; 44[Suppl 1]:S5-S12.
63 Miller D, Waters D, Warnica W, et al. Is variant angina the coronary manifestation of generalised
vasospastic disorder? N Engl J Med 1981;304:763-766.
Page 51 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from

For peer review only
Figure 1: Flow chart diagram showing results of systematic literature search
Initial search: n=2378
n = 1911
n = 97
Final number of relevant articles
Definite= 33
Further exclusion after paper
retrieval: n = 64
See box 2 for exclusion reasons
Duplicates = 467
Reviews, Case reports, Non-RP,
treatment, progression etc = 1814
See box 1 for exclusion reasons
aSee table 1 for exclusion reasons
Page 52 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
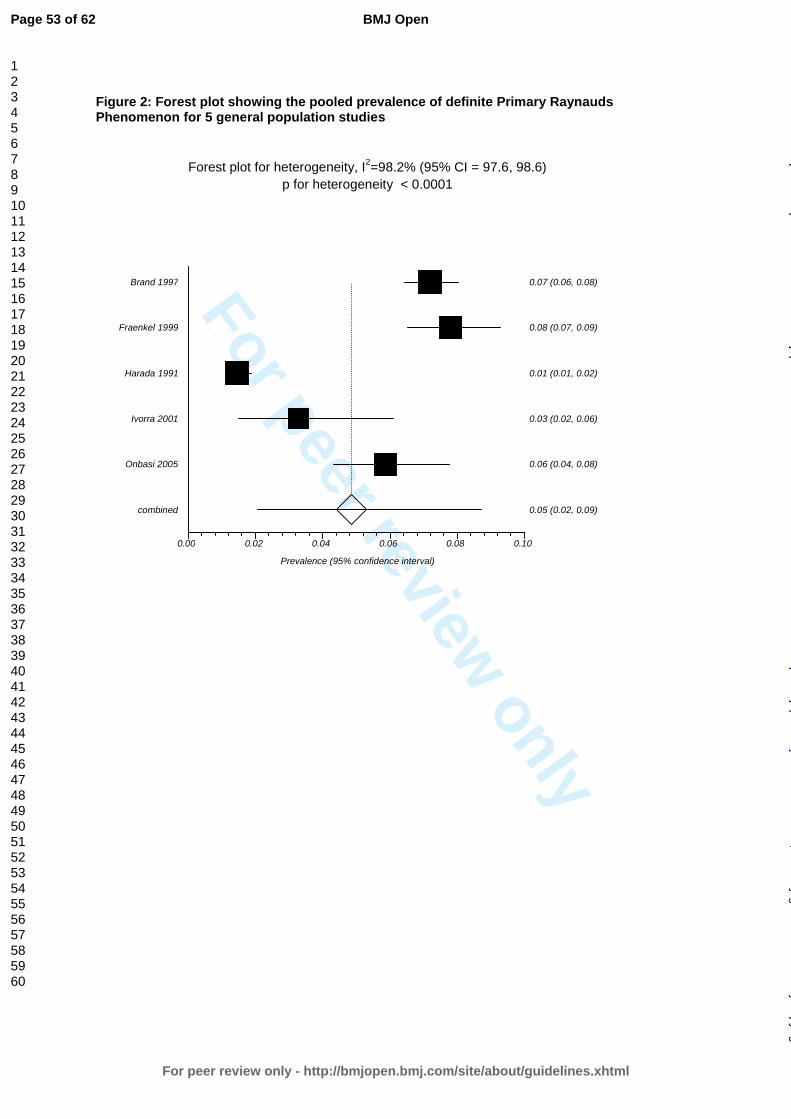
For peer review only
Figure 2: Forest plot showing the pooled prevalence of definite Primary Raynauds Phenomenon for 5 general population studies
0.00 0.02 0.04 0.06 0.08 0.10
combined 0.05 (0.02, 0.09)
Onbasi 2005 0.06 (0.04, 0.08)
Ivorra 2001 0.03 (0.02, 0.06)
Harada 1991 0.01 (0.01, 0.02)
Fraenkel 1999 0.08 (0.07, 0.09)
Brand 1997 0.07 (0.06, 0.08)
Prevalence (95% confidence interval)
Forest plot for heterogeneity, I2=98.2% (95% CI = 97.6, 98.6)
p for heterogeneity < 0.0001
Page 53 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
For peer review only
Page 54 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
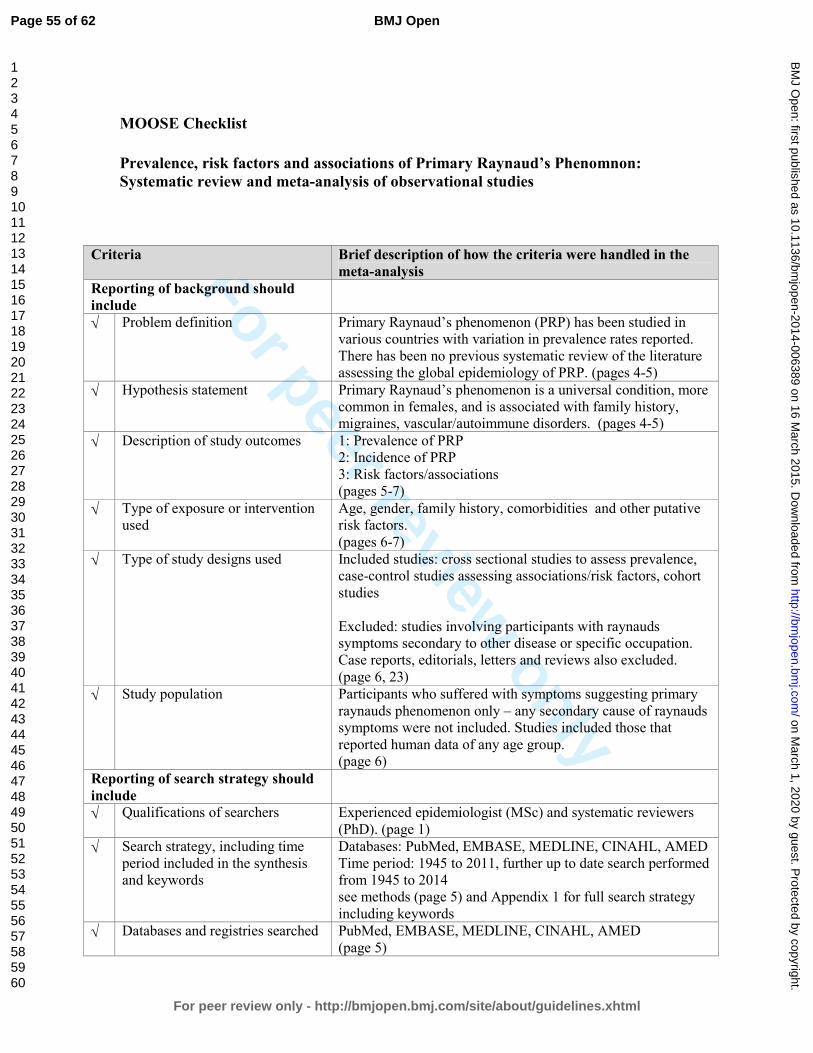
For peer review only
MOOSE Checklist
Prevalence, risk factors and associations of Primary Raynaud’s Phenomnon:
Systematic review and meta-analysis of observational studies
Criteria Brief description of how the criteria were handled in the
meta-analysis
Reporting of background should
include
√ Problem definition Primary Raynaud’s phenomenon (PRP) has been studied in
various countries with variation in prevalence rates reported.
There has been no previous systematic review of the literature
assessing the global epidemiology of PRP. (pages 4-5)
√ Hypothesis statement Primary Raynaud’s phenomenon is a universal condition, more
common in females, and is associated with family history,
migraines, vascular/autoimmune disorders. (pages 4-5)
√ Description of study outcomes 1: Prevalence of PRP
2: Incidence of PRP
3: Risk factors/associations
(pages 5-7)
√ Type of exposure or intervention
used
Age, gender, family history, comorbidities and other putative
risk factors.
(pages 6-7)
√ Type of study designs used Included studies: cross sectional studies to assess prevalence,
case-control studies assessing associations/risk factors, cohort
studies
Excluded: studies involving participants with raynauds
symptoms secondary to other disease or specific occupation.
Case reports, editorials, letters and reviews also excluded.
(page 6, 23)
√ Study population Participants who suffered with symptoms suggesting primary
raynauds phenomenon only – any secondary cause of raynauds
symptoms were not included. Studies included those that
reported human data of any age group.
(page 6)
Reporting of search strategy should
include
√ Qualifications of searchers Experienced epidemiologist (MSc) and systematic reviewers
(PhD). (page 1)
√ Search strategy, including time
period included in the synthesis
and keywords
Databases: PubMed, EMBASE, MEDLINE, CINAHL, AMED
Time period: 1945 to 2011, further up to date search performed
from 1945 to 2014
see methods (page 5) and Appendix 1 for full search strategy
including keywords
√ Databases and registries searched PubMed, EMBASE, MEDLINE, CINAHL, AMED
(page 5)
Page 55 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
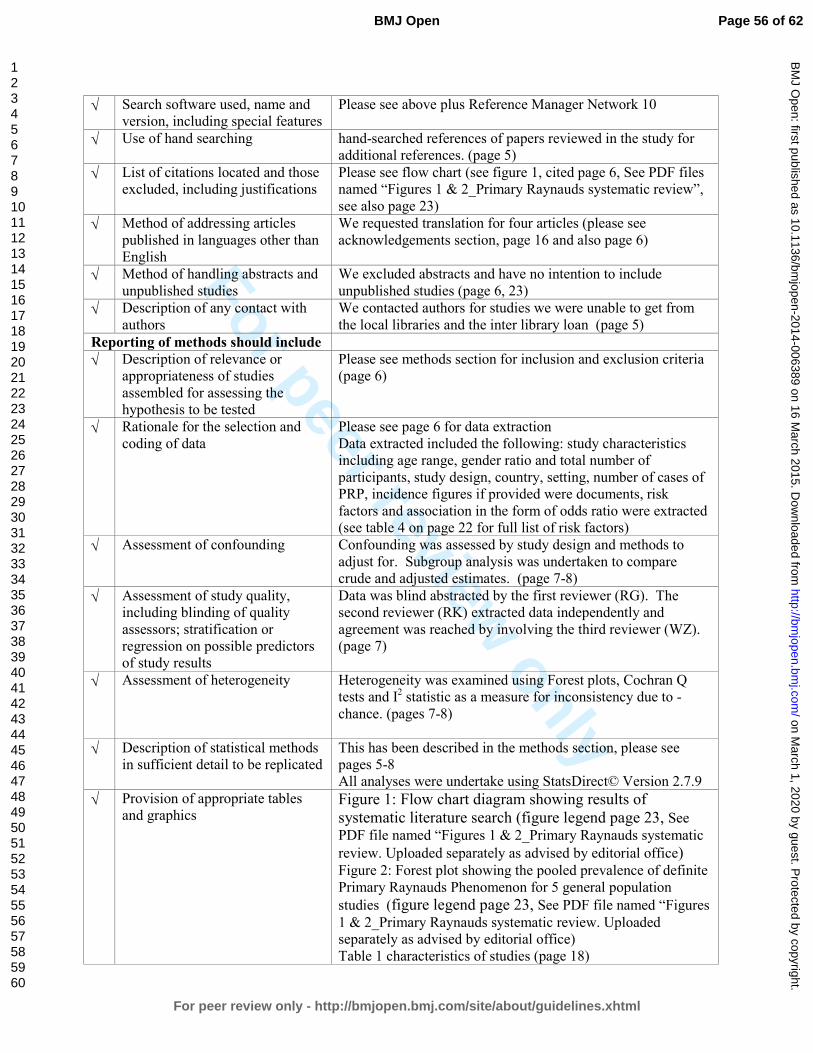
For peer review only
√ Search software used, name and
version, including special features
Please see above plus Reference Manager Network 10
√ Use of hand searching hand-searched references of papers reviewed in the study for
additional references. (page 5)
√ List of citations located and those
excluded, including justifications
Please see flow chart (see figure 1, cited page 6, See PDF files
named “Figures 1 & 2_Primary Raynauds systematic review”,
see also page 23)
√ Method of addressing articles
published in languages other than
English
We requested translation for four articles (please see
acknowledgements section, page 16 and also page 6)
√ Method of handling abstracts and
unpublished studies
We excluded abstracts and have no intention to include
unpublished studies (page 6, 23)
√ Description of any contact with
authors
We contacted authors for studies we were unable to get from
the local libraries and the inter library loan (page 5)
Reporting of methods should include
√ Description of relevance or
appropriateness of studies
assembled for assessing the
hypothesis to be tested
Please see methods section for inclusion and exclusion criteria
(page 6)
√ Rationale for the selection and
coding of data
Please see page 6 for data extraction
Data extracted included the following: study characteristics
including age range, gender ratio and total number of
participants, study design, country, setting, number of cases of
PRP, incidence figures if provided were documents, risk
factors and association in the form of odds ratio were extracted
(see table 4 on page 22 for full list of risk factors)
√ Assessment of confounding Confounding was assessed by study design and methods to
adjust for. Subgroup analysis was undertaken to compare
crude and adjusted estimates. (page 7-8)
√ Assessment of study quality,
including blinding of quality
assessors; stratification or
regression on possible predictors
of study results
Data was blind abstracted by the first reviewer (RG). The
second reviewer (RK) extracted data independently and
agreement was reached by involving the third reviewer (WZ).
(page 7)
√ Assessment of heterogeneity Heterogeneity was examined using Forest plots, Cochran Q
tests and I2 statistic as a measure for inconsistency due to -
chance. (pages 7-8)
√ Description of statistical methods
in sufficient detail to be replicated
This has been described in the methods section, please see
pages 5-8
All analyses were undertake using StatsDirect© Version 2.7.9
√ Provision of appropriate tables
and graphics Figure 1: Flow chart diagram showing results of
systematic literature search (figure legend page 23, See PDF file named “Figures 1 & 2_Primary Raynauds systematic
review. Uploaded separately as advised by editorial office) Figure 2: Forest plot showing the pooled prevalence of definite
Primary Raynauds Phenomenon for 5 general population
studies (figure legend page 23, See PDF file named “Figures
1 & 2_Primary Raynauds systematic review. Uploaded
separately as advised by editorial office)
Table 1 characteristics of studies (page 18)
Page 56 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
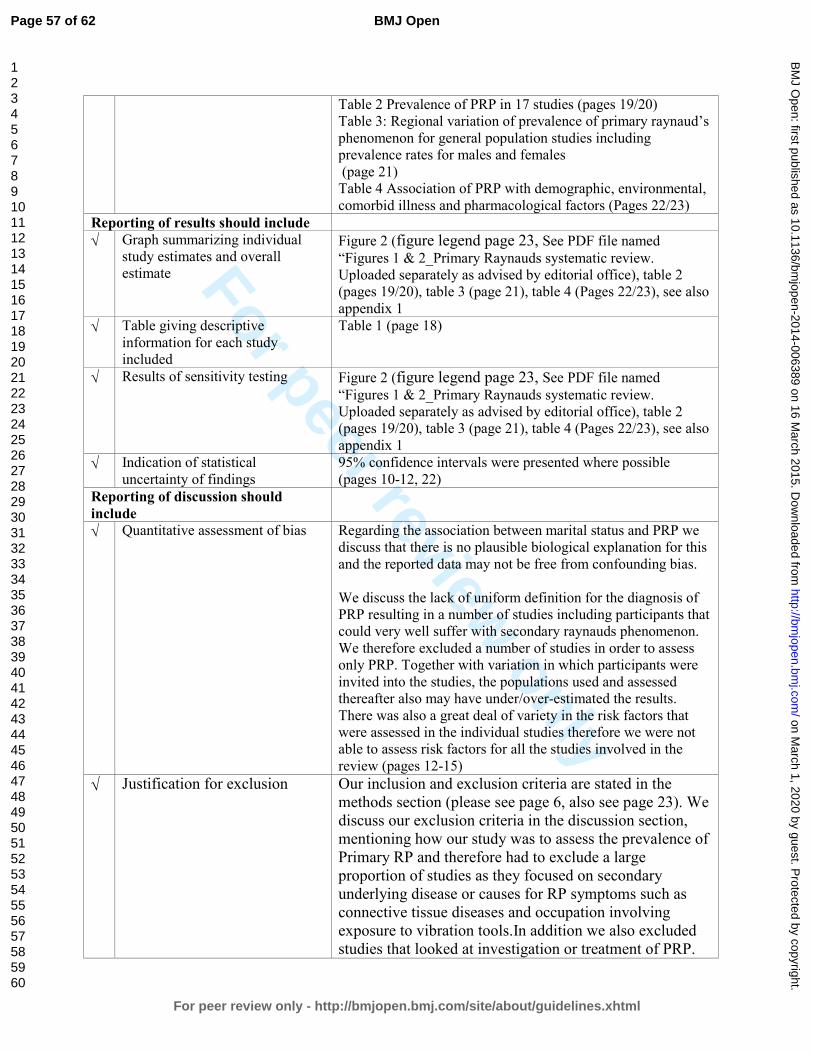
For peer review only
Table 2 Prevalence of PRP in 17 studies (pages 19/20)
Table 3: Regional variation of prevalence of primary raynaud’s
phenomenon for general population studies including
prevalence rates for males and females
(page 21)
Table 4 Association of PRP with demographic, environmental,
comorbid illness and pharmacological factors (Pages 22/23)
Reporting of results should include
√ Graph summarizing individual
study estimates and overall
estimate
Figure 2 (figure legend page 23, See PDF file named
“Figures 1 & 2_Primary Raynauds systematic review.
Uploaded separately as advised by editorial office), table 2
(pages 19/20), table 3 (page 21), table 4 (Pages 22/23), see also
appendix 1
√ Table giving descriptive
information for each study
included
Table 1 (page 18)
√ Results of sensitivity testing
Figure 2 (figure legend page 23, See PDF file named
“Figures 1 & 2_Primary Raynauds systematic review.
Uploaded separately as advised by editorial office), table 2
(pages 19/20), table 3 (page 21), table 4 (Pages 22/23), see also
appendix 1
√ Indication of statistical
uncertainty of findings
95% confidence intervals were presented where possible
(pages 10-12, 22)
Reporting of discussion should
include
√ Quantitative assessment of bias Regarding the association between marital status and PRP we
discuss that there is no plausible biological explanation for this
and the reported data may not be free from confounding bias.
We discuss the lack of uniform definition for the diagnosis of
PRP resulting in a number of studies including participants that
could very well suffer with secondary raynauds phenomenon.
We therefore excluded a number of studies in order to assess
only PRP. Together with variation in which participants were
invited into the studies, the populations used and assessed
thereafter also may have under/over-estimated the results.
There was also a great deal of variety in the risk factors that
were assessed in the individual studies therefore we were not
able to assess risk factors for all the studies involved in the
review (pages 12-15)
√ Justification for exclusion Our inclusion and exclusion criteria are stated in the
methods section (please see page 6, also see page 23). We
discuss our exclusion criteria in the discussion section,
mentioning how our study was to assess the prevalence of
Primary RP and therefore had to exclude a large
proportion of studies as they focused on secondary
underlying disease or causes for RP symptoms such as
connective tissue diseases and occupation involving
exposure to vibration tools.In addition we also excluded
studies that looked at investigation or treatment of PRP.
Page 57 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
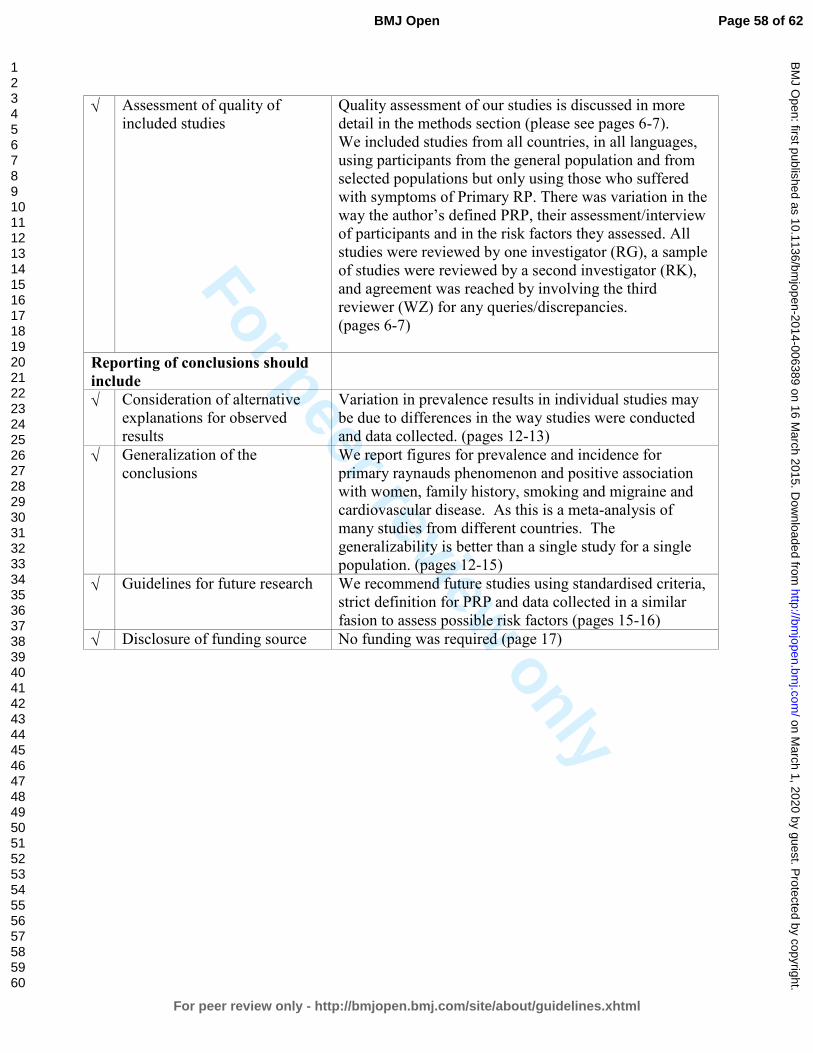
For peer review only
√ Assessment of quality of
included studies
Quality assessment of our studies is discussed in more
detail in the methods section (please see pages 6-7).
We included studies from all countries, in all languages,
using participants from the general population and from
selected populations but only using those who suffered
with symptoms of Primary RP. There was variation in the
way the author’s defined PRP, their assessment/interview
of participants and in the risk factors they assessed. All
studies were reviewed by one investigator (RG), a sample
of studies were reviewed by a second investigator (RK),
and agreement was reached by involving the third
reviewer (WZ) for any queries/discrepancies.
(pages 6-7)
Reporting of conclusions should
include
√ Consideration of alternative
explanations for observed
results
Variation in prevalence results in individual studies may
be due to differences in the way studies were conducted
and data collected. (pages 12-13)
√ Generalization of the
conclusions
We report figures for prevalence and incidence for
primary raynauds phenomenon and positive association
with women, family history, smoking and migraine and
cardiovascular disease. As this is a meta-analysis of
many studies from different countries. The
generalizability is better than a single study for a single
population. (pages 12-15)
√ Guidelines for future research We recommend future studies using standardised criteria,
strict definition for PRP and data collected in a similar
fasion to assess possible risk factors (pages 15-16)
√ Disclosure of funding source No funding was required (page 17)
Page 58 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2014-006389 on 16 M
arch 2015. Dow
nloaded from
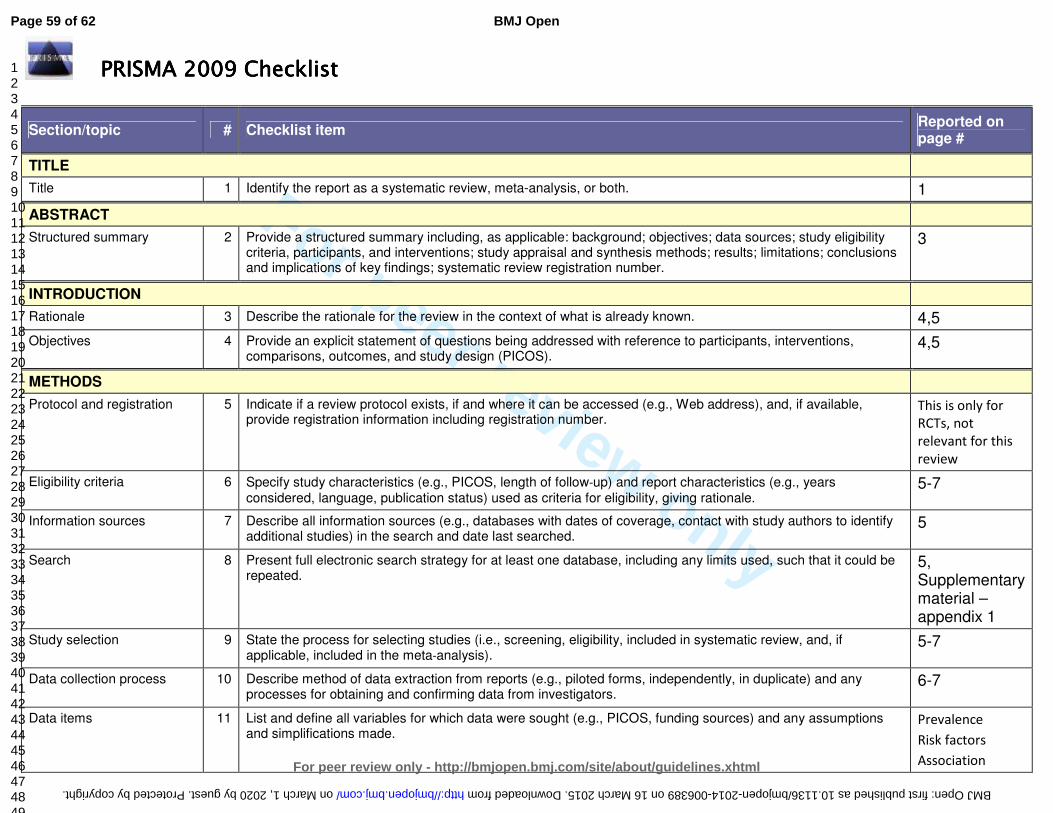
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
Section/topic # Checklist item Reported on page #
TITLE
Title 1 Identify the report as a systematic review, meta-analysis, or both. 1
ABSTRACT
Structured summary 2 Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number.
3
INTRODUCTION
Rationale 3 Describe the rationale for the review in the context of what is already known. 4,5
Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS).
4,5
METHODS
Protocol and registration 5 Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number.
This is only for
RCTs, not
relevant for this
review
Eligibility criteria 6 Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale.
5-7
Information sources 7 Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched.
5
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated.
5, Supplementary material – appendix 1
Study selection 9 State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis).
5-7
Data collection process 10 Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators.
6-7
Data items 11 List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made.
Prevalence
Risk factors
Association
Page 59 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
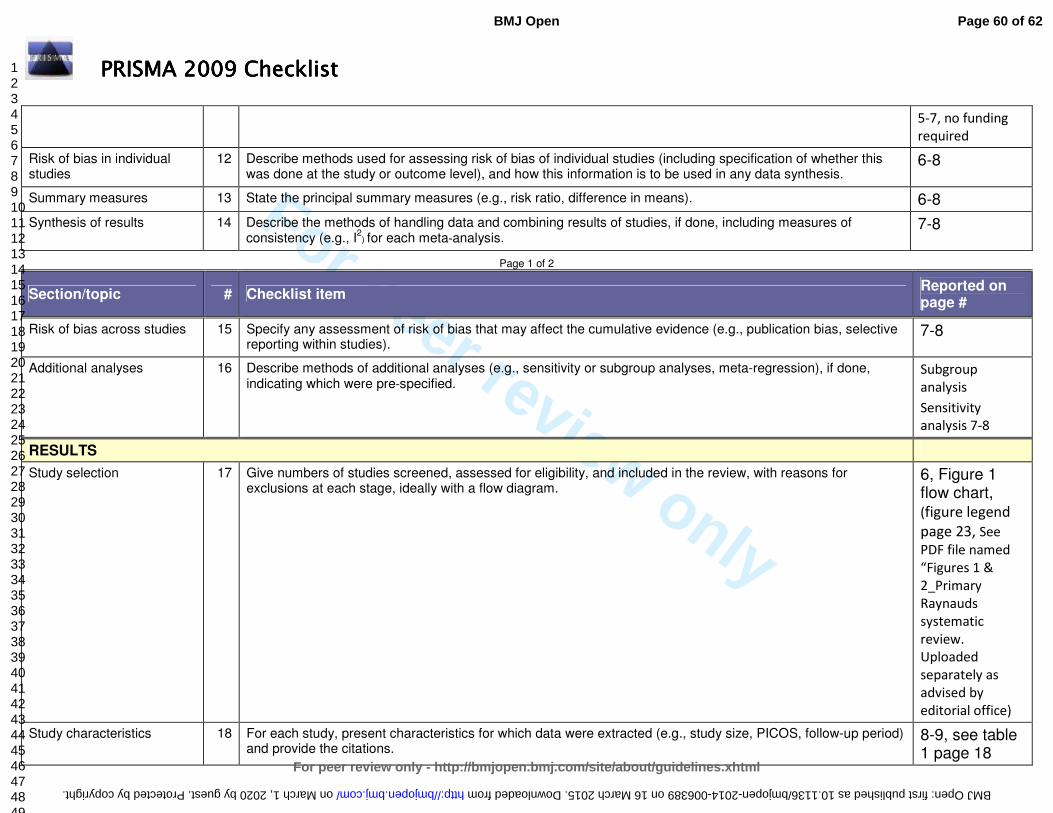
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
5-7, no funding
required
Risk of bias in individual studies
12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis.
6-8
Summary measures 13 State the principal summary measures (e.g., risk ratio, difference in means). 6-8
Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I
2) for each meta-analysis.
7-8
Page 1 of 2
Section/topic # Checklist item Reported on page #
Risk of bias across studies 15 Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies).
7-8
Additional analyses 16 Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified.
Subgroup
analysis
Sensitivity
analysis 7-8
RESULTS
Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram.
6, Figure 1 flow chart, (figure legend
page 23, See
PDF file named
“Figures 1 &
2_Primary
Raynauds
systematic
review.
Uploaded
separately as
advised by
editorial office)
Study characteristics 18 For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations.
8-9, see table 1 page 18
Page 60 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
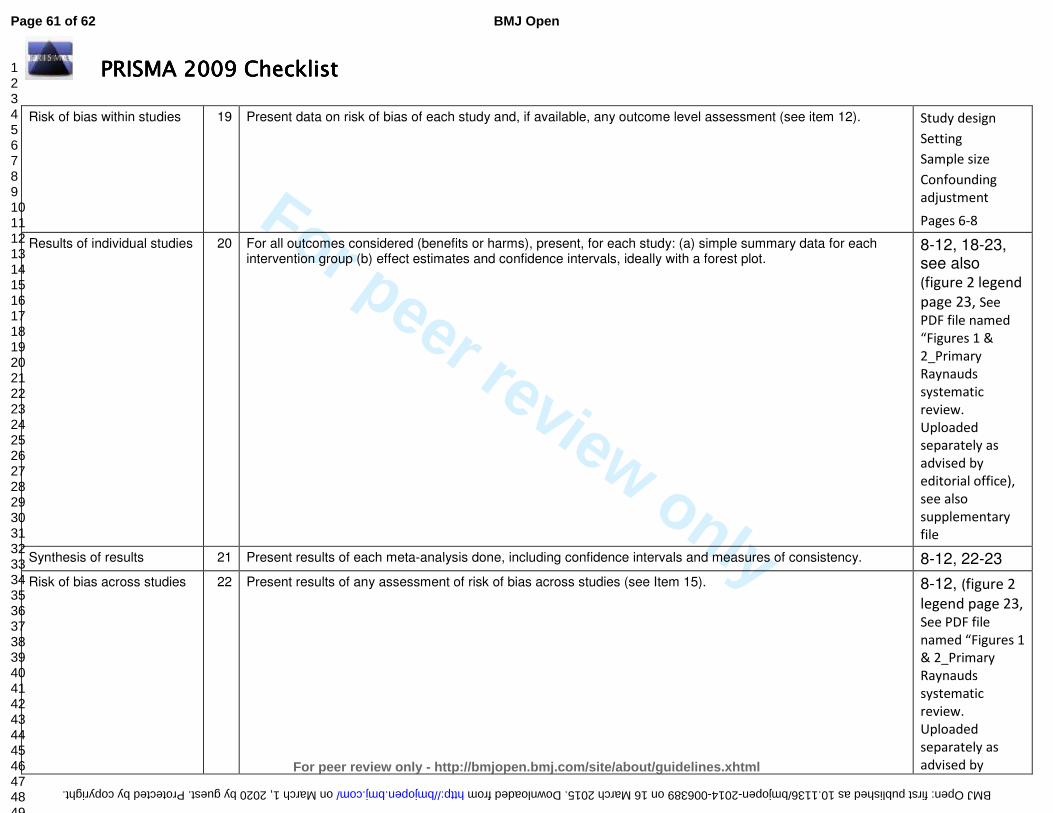
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
Risk of bias within studies 19 Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). Study design
Setting
Sample size
Confounding
adjustment
Pages 6-8
Results of individual studies 20 For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot.
8-12, 18-23, see also (figure 2 legend
page 23, See
PDF file named
“Figures 1 &
2_Primary
Raynauds
systematic
review.
Uploaded
separately as
advised by
editorial office),
see also
supplementary
file
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency. 8-12, 22-23
Risk of bias across studies 22 Present results of any assessment of risk of bias across studies (see Item 15). 8-12, (figure 2
legend page 23,
See PDF file
named “Figures 1
& 2_Primary
Raynauds
systematic
review.
Uploaded
separately as
advised by
Page 61 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from
For peer review only
PRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 ChecklistPRISMA 2009 Checklist
editorial office)
Additional analysis 23 Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]).
8-12, see also supplementary file
DISCUSSION
Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers).
12-15
Limitations 25 Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias).
12-15
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research.
13-15
FUNDING
Funding 27 Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review.
No funding required.
RG time half day
per week from
the NHS
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
For more information, visit: www.prisma-statement.org.
Page 2 of 2
Page 62 of 62
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on March 1, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2014-006389 on 16 March 2015. Downloaded from