25.05.2009 dr.h.n.sarker compressive and non compressive spinal cord syndrome dr. h.n. sarker mbbs,...
TRANSCRIPT
25.05.2009 Dr.H.N.Sarker
Compressive and non Compressive and non compressive spinal compressive spinal
cord syndromecord syndromeDr. H.N. Sarker Dr. H.N. Sarker
MBBS, FCPS (Medicine), MBBS, FCPS (Medicine), MACP(USA),MACP(USA),MRCP(UK), MRCP(UK),
MRCPS(GLASGO),FRCP(Edin) MRCPS(GLASGO),FRCP(Edin) Associate ProfessorAssociate Professor
MedicineMedicineSBMC, BarisalSBMC, Barisal

25.05.2009 Dr.H.N.Sarker
INTRODUCTIONINTRODUCTION
Spinal cord is a long , thin Spinal cord is a long , thin tubular structure of central tubular structure of central nervous system which extends nervous system which extends from foramen magnum to lower from foramen magnum to lower border of first lumbar vertebra. It border of first lumbar vertebra. It is covered by three meninges – is covered by three meninges – Dura, arachnoid, and pia Dura, arachnoid, and pia matters. matters.
25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
INTRODUCTION…. INTRODUCTION….
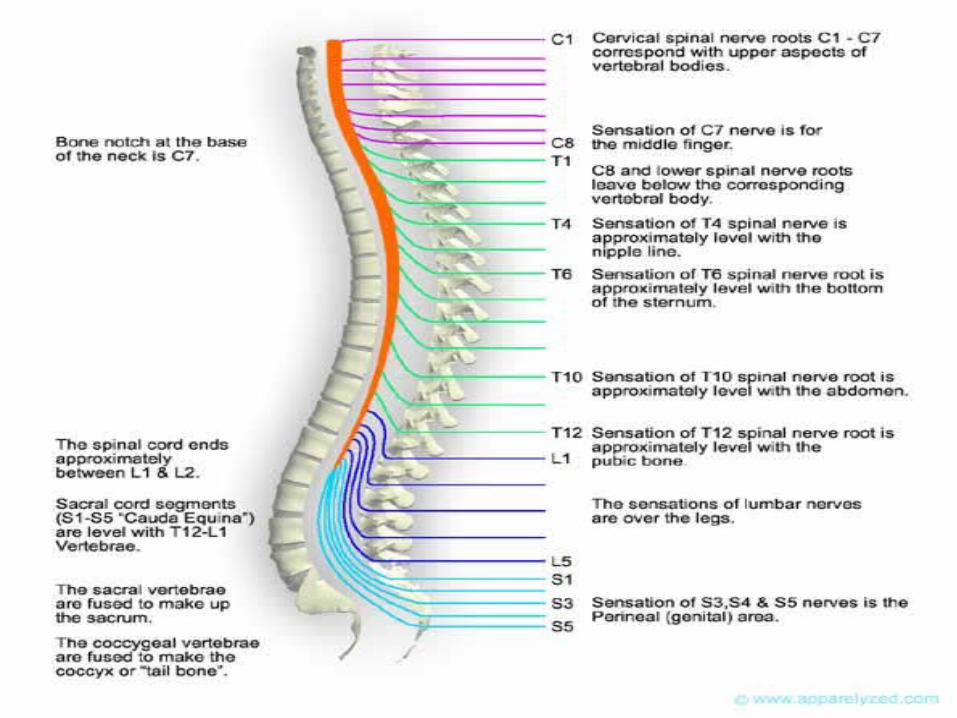
Spinal cord consists of 31 spinal Spinal cord consists of 31 spinal segments from which corresponding segments from which corresponding pair of spinal nerve arise. Since the pair of spinal nerve arise. Since the spinal cord is shorter than vertebral spinal cord is shorter than vertebral canal , spinal segment does not canal , spinal segment does not correspond with vertebra. correspond with vertebra.

25.05.2009 Dr.H.N.Sarker
INTRODUCTION INTRODUCTION
There are two enlargements in There are two enlargements in spinal cord – spinal cord –
cervical (C4-T1) from which cervical (C4-T1) from which nerves nerves supplying the upper supplying the upper limbs arise limbs arise
lumbar (L1-S3) from which lumbar (L1-S3) from which nerves nerves supplying lower limbs supplying lower limbs arise.arise.
25.05.2009 Dr.H.N.Sarker
Blood SupplyBlood Supply
Spinal cord is supplied by Spinal cord is supplied by a single anterior spinal artery – a single anterior spinal artery –
which supplies anterior two which supplies anterior two thirds of spinal cord thirds of spinal cord
Two posterior spinal arteries- Two posterior spinal arteries- which, supplemented by which, supplemented by segmental arteries supply segmental arteries supply posterior one third of the cord.posterior one third of the cord.

25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Any lesion of the spinal cord Any lesion of the spinal cord produces effects involving the produces effects involving the spinal segment(s) and long spinal segment(s) and long tract(s) of the spinal cord. So, to tract(s) of the spinal cord. So, to understand the effect of any understand the effect of any lesion you should clearly lesion you should clearly understand anatomical understand anatomical arrangement of the spinal arrangement of the spinal segment and long tracts.segment and long tracts.
25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Each segment consists of Each segment consists of
central gray matter central gray matter peripheral white matterperipheral white matter

25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Central gray matter: Composed of nerve Central gray matter: Composed of nerve cells which are arranged as cells which are arranged as
anterior horn cell- lower motor neuronanterior horn cell- lower motor neuron Posterior horn cell- Posterior horn cell-
Sensory neuronSensory neuron Second order neuronSecond order neuron Fibre from this neurons crosses within the Fibre from this neurons crosses within the
segment to the opposite side to form segment to the opposite side to form lateral spinothalamic tract. First order lateral spinothalamic tract. First order neuron lies in dorsal root ganglion of neuron lies in dorsal root ganglion of spinal cord.spinal cord.

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Peripheral white matter: Peripheral white matter:
It contains bundles of fibres that It contains bundles of fibres that are called tracts.are called tracts.

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Long tracts:Long tracts: There are at least 10 tracts in There are at least 10 tracts in
spinal cord; But we are spinal cord; But we are interested in only three long interested in only three long tracts- corticospinal tract, tracts- corticospinal tract, spinothalamic tract and dorsal spinothalamic tract and dorsal column which subserves most of column which subserves most of the functions.the functions.

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Corticospinal tract: Corticospinal tract: It produces ipsilateral upper It produces ipsilateral upper
motor neuron lesion as the fibres motor neuron lesion as the fibres of the tract crosses at medullae of the tract crosses at medullae oblongata.oblongata.

25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Spinothalamic tract: Spinothalamic tract: It contains fibers for pain, crude It contains fibers for pain, crude
touch and temperature. Since touch and temperature. Since fibers of 2nd order neuron crosses fibers of 2nd order neuron crosses within the segment to opposite within the segment to opposite side , any lesion of the tract leads side , any lesion of the tract leads to loss of pain and temperature to loss of pain and temperature sensation of opposite site of the sensation of opposite site of the body below the lesion .body below the lesion .

25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
NeuroanatomyNeuroanatomy
Dorsal column: Dorsal column: It carries sense of position and It carries sense of position and
vibration and fine touch. As the vibration and fine touch. As the fibres croses midline at medullae fibres croses midline at medullae oblongata, so lesion in the tract oblongata, so lesion in the tract produce ipsilateral loss of sense produce ipsilateral loss of sense of position and vibration and fine of position and vibration and fine touch.touch.

25.05.2009 Dr.H.N.Sarker
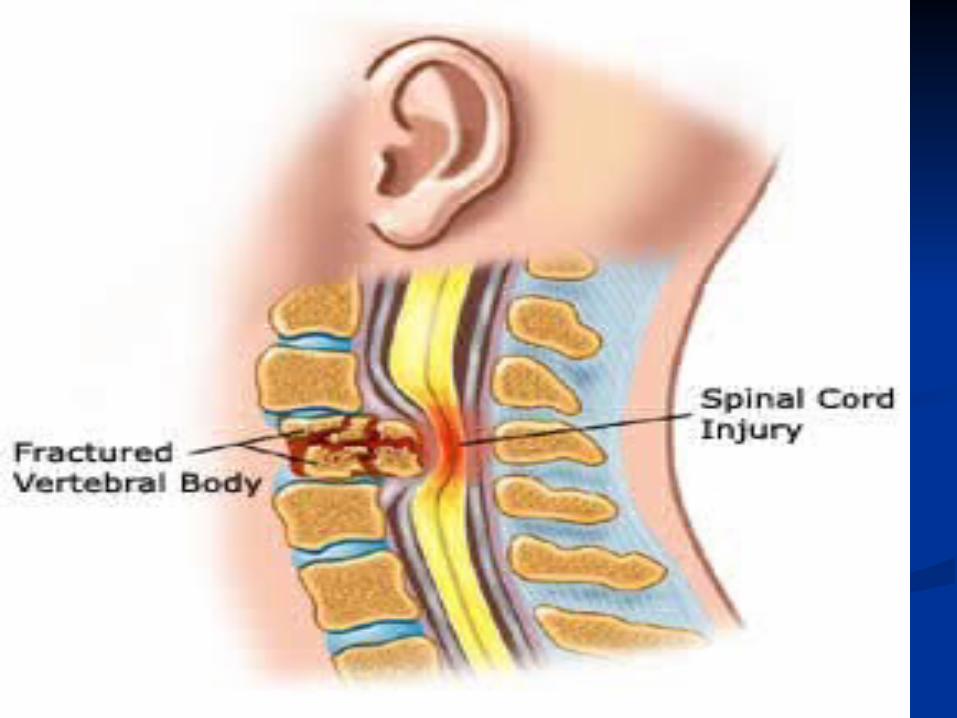
Compressive Spinal cord lesion: Compressive Spinal cord lesion: Common causesCommon causes
SiteSite FrequencyFrequency CausesCauses
VertebralVertebral 80%80% Trauma (extradural) Trauma (extradural) Intervertebral disc Intervertebral disc prolapse prolapse Metastatic carcinoma Metastatic carcinoma (e.g. breast, prostate, (e.g. breast, prostate, bronchus) Myelomabronchus) MyelomaTuberculosisTuberculosis
Meninges (intradural Meninges (intradural extramedullaryextramedullary
15%15% Tumours (e.g. Tumours (e.g. meningioma, meningioma, neurofibroma, neurofibroma, ependymoma, ependymoma, metastasis, lymphoma, metastasis, lymphoma, leukaemia)leukaemia)
Spinal cord (intradural Spinal cord (intradural intramedullaryintramedullary
5%5% Epidural abscessEpidural abscess
Tumours (e.g. glioma, Tumours (e.g. glioma, ependymoma, ependymoma, metastasismetastasis

25.05.2009 Dr.H.N.Sarker
Compressive Spinal cord Compressive Spinal cord lesionlesion
Clinical features: Clinical features: Onset is usually slow (over weeks) Onset is usually slow (over weeks)
but can be acute as a result of but can be acute as a result of trauma or metastases.trauma or metastases.
25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
SYMPTOMS OF SPINAL CORD SYMPTOMS OF SPINAL CORD COMPRESSIONCOMPRESSION
Pain:Pain:
Localised over the spine or in a root Localised over the spine or in a root distribution, which may be aggravated distribution, which may be aggravated by coughing, sneezing or strainingby coughing, sneezing or straining
Sensory:Sensory:
Paraesthesia, numbness or cold Paraesthesia, numbness or cold sensations, especially in the lower sensations, especially in the lower limbs, which spread proximally, often limbs, which spread proximally, often to a level on the trunkto a level on the trunk

25.05.2009 Dr.H.N.Sarker
SYMPTOMS OF SPINAL CORD SYMPTOMS OF SPINAL CORD COMPRESSIONCOMPRESSION
Motor :Motor :
Weakness, heaviness or stiffness of Weakness, heaviness or stiffness of the limbs, most commonly the legsthe limbs, most commonly the legs
Sphincters:Sphincters:
Urgency or hesitancy of micturition, Urgency or hesitancy of micturition, leading eventually to retention.leading eventually to retention.

25.05.2009 Dr.H.N.Sarker
SIGNS OF SPINAL CORD SIGNS OF SPINAL CORD COMPRESSIONCOMPRESSION
Signs depends on site of lesion Signs depends on site of lesion and completeness of and completeness of involvement.involvement.
25.05.2009 Dr.H.N.Sarker
SIGNS OF SPINAL CORD SIGNS OF SPINAL CORD COMPRESSIONCOMPRESSION
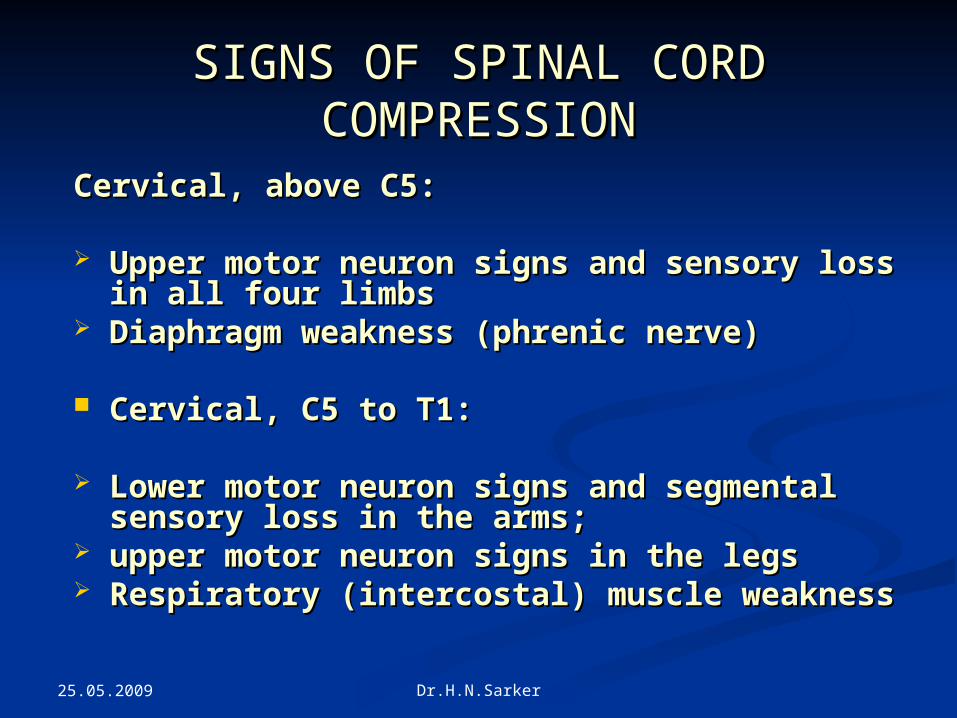
Cervical, above C5:Cervical, above C5:
Upper motor neuron signs and sensory loss Upper motor neuron signs and sensory loss in all four limbs in all four limbs
Diaphragm weakness (phrenic nerve)Diaphragm weakness (phrenic nerve)
Cervical, C5 to T1:Cervical, C5 to T1:
Lower motor neuron signs and segmental Lower motor neuron signs and segmental sensory loss in the arms; sensory loss in the arms;
upper motor neuron signs in the legs upper motor neuron signs in the legs Respiratory (intercostal) muscle weaknessRespiratory (intercostal) muscle weakness

25.05.2009 Dr.H.N.Sarker
SIGNS OF SPINAL CORD SIGNS OF SPINAL CORD COMPRESSIONCOMPRESSION
Thoracic cord :Thoracic cord :
Spastic paraplegia with a sensory Spastic paraplegia with a sensory level on the trunklevel on the trunk
Conus medullaris: Conus medullaris:
Lesions at the end of the spinal cord Lesions at the end of the spinal cord cause sacral loss of sensation and cause sacral loss of sensation and extensor plantar responses extensor plantar responses

25.05.2009 Dr.H.N.Sarker
SIGNS OF SPINAL CORD SIGNS OF SPINAL CORD COMPRESSIONCOMPRESSION
Cauda equina :Cauda equina :
Spinal cord ends at Spinal cord ends at approximately the T12/L1 spinal approximately the T12/L1 spinal level and spinal lesions below level and spinal lesions below this level can only cause lower this level can only cause lower motor neuron signs by affecting motor neuron signs by affecting the cauda equine.the cauda equine.
25.05.2009 Dr.H.N.Sarker
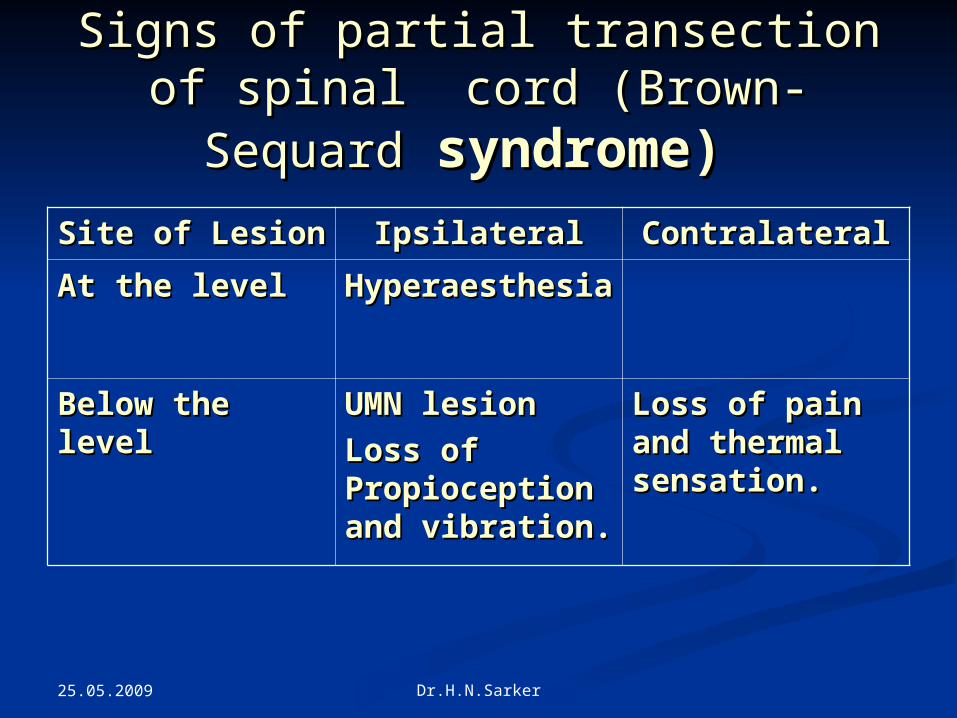
Signs of partial transection of Signs of partial transection of spinal cord (Brown- Sequardspinal cord (Brown- Sequard
syndrome)syndrome) Site of LesionSite of Lesion IpsilateralIpsilateral ContralateralContralateral
At the levelAt the level HyperaesthesiHyperaesthesiaa
Below the Below the levellevel
UMN lesionUMN lesion
Loss of Loss of Propioception Propioception and vibration.and vibration.
Loss of pain Loss of pain and thermal and thermal sensation.sensation.

25.05.2009 Dr.H.N.Sarker

25.05.2009 Dr.H.N.Sarker
InvestigationInvestigation
Plain X-rays of spine Plain X-rays of spine MRI of spine or myelography MRI of spine or myelography Chest X-rays Chest X-rays CSF CSF Serum B12Serum B12

25.05.2009 Dr.H.N.Sarker
ManagementManagement
General measuresGeneral measures Care of skin:Care of skin: Meticulous attention must be Meticulous attention must be
paid to cleanliness and to paid to cleanliness and to turning pt two hrlyturning pt two hrly
Inspect pressure areas regularlyInspect pressure areas regularly Use pressure mattressUse pressure mattress Treat any pressure soreTreat any pressure sore

25.05.2009 Dr.H.N.Sarker
ManagementManagement
General measures…….General measures…….
Care of Bladder:Care of Bladder: Self catheterization or reflex bladder Self catheterization or reflex bladder
emptying emptying
Care of Bowel:Care of Bowel: Constipation and fecal impacation must Constipation and fecal impacation must
be avoidedbe avoided..
25.05.2009 Dr.H.N.Sarker
ManagementManagement
General measures……General measures……
Care of paralysed limbs:Care of paralysed limbs: Passive physiotherapy to prevent Passive physiotherapy to prevent
contracture.contracture. Severe spasticity may be helped by Severe spasticity may be helped by
beclofen or diazepambeclofen or diazepam..

25.05.2009 Dr.H.N.Sarker
ManagementManagement
Specific measure: Specific measure:
Treatment of the underlying cause Treatment of the underlying cause e.g. anti TB in pott’s disease.e.g. anti TB in pott’s disease.
RehabilitationRehabilitation

25.05.2009 Dr.H.N.Sarker
Non compressive spinal cord Non compressive spinal cord syndromesyndrome
causecause conditionsconditions
Hereditary Hereditary Hereditary spastic Hereditary spastic paraplegia, Friedreich’s paraplegia, Friedreich’s ataxiaataxia
Infective/inflammatory Infective/inflammatory Transverse myelitis, Transverse myelitis,
MS, SyphilisMS, Syphilis
Vascular Vascular Anterior spinal artery Anterior spinal artery infarct Spinal AVMinfarct Spinal AVM
Metabolic Metabolic Vitamin B12 deficiency Vitamin B12 deficiency (subacute combined (subacute combined degeneration degeneration
Degenerative Degenerative Motor neuron disease, Motor neuron disease, SyringomyeliaSyringomyelia

25.05.2009 Dr.H.N.Sarker
Acute Transverse MyelitisAcute Transverse Myelitis
Acute Transverse Myelitis is an Acute Transverse Myelitis is an acute, often monophasic acute, often monophasic inflammatory demyelinating inflammatory demyelinating disease affecting the spinal cord disease affecting the spinal cord over a variable number of over a variable number of segments.segments.

25.05.2009 Dr.H.N.Sarker
AetiologyAetiology
Multiple SclerosisMultiple Sclerosis Post infectious e.g. CMVPost infectious e.g. CMV Post vaccinationPost vaccination Trauma Trauma SurgerySurgery

25.05.2009 Dr.H.N.Sarker
Clinical FeatureClinical Feature
Any age Any age Subacute onsetSubacute onset May be severe neck or back painMay be severe neck or back pain Spastic paraparesis Spastic paraparesis Definite sensory level Definite sensory level Sphincter involvement- Initially Sphincter involvement- Initially
urinary retention later on urinary retention later on incontinenceincontinence

25.05.2009 Dr.H.N.Sarker
InvestigationInvestigation
MRIMRI CSF studyCSF study

25.05.2009 Dr.H.N.Sarker
ManagementManagement
General measuresGeneral measures
As for a paralysed patientAs for a paralysed patient
Specific measure: Specific measure:
High dose intravenous methyl High dose intravenous methyl prednisolone.prednisolone.

25.05.2009 Dr.H.N.Sarker
PrognosisPrognosis
VariableVariable One third recovered completelyOne third recovered completely One third remains with residual One third remains with residual
disabilitydisability One third bed ridden.One third bed ridden.

25.05.2009 Dr.H.N.Sarker