biom30002 l3 2015 md
DESCRIPTION
Lecture Notes.TRANSCRIPT

Clinical aspects of Duchenne muscular
dystrophy
M2M 2015 Muscular Dystrophies Theme
Lecture 3

COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and communicated to you by or on behalf of the University of Melbourne pursuant to Part VB of the Copyright Act 1968 (the Act).
The material in this communication may be subject to copyright under the Act. Any further copying or communication of this material by you may be the subject of copyright protection under the Act and constitute an infringement.
Do Not Remove This Notice

DMD is caused by loss of dystrophin
normal
DMD/ mdx
Muscle immunohistochemical
staining for dystrophin
Author’s own

Dystrophinopathies
Duchenne muscular dystrophy
Becker muscular dystrophy
Familial cramps + myalgia syndrome
Other
– X-‐linked dilated cardiomyopathy
– Isolated elevated CK
– ManifesIng carrier females
– Isolated quadriceps myopathy
Guillaume-Benjamin Duchenne de Boulogne US National Library of Medicine

Onset
DMD: onset <5 years – Incidence 1/5000 boys – Clinical diagnosis typically 2-‐4 yrs
Wheelchair dependency <13 yrs
BMD: onset > 5yrs – Incidence 1/35 000 male births – Clinical onset variable
Wheelchair dependency >16 yrs

Clinical presentaIons of DMD
Delayed motor milestones – Mean age walking 18m (normal <18 months)
Gait difficulIes
– Broad-‐based, waddling gait, proximal weakness – Trouble climbing steps, Gowers’ manoeuvre
– Persistent toe-‐walking, flat feet FaIgability, frequent falls
– Inability to run or to keep up with peers Calf / thigh cramps, muscle enlargement
Speech delay, learning problems

Physical examinaIon
Waddling gait Proximal weakness Enlarged, rubbery muscles
– calves +/-‐ quads, gluteal, deltoid, even tongue – early hypertrophy, late pseudohypertrophy
Facial muscles spared Extra-‐ocular muscles always spared
Weak neck flexors Lumbar lordosis

Muscle hypertrophy
Muscles look larger but in fact this apparent enlargement is due to increased fat and fibrosis rather than an increase in true muscle Issue i.e. ‘pseudohypertrophy ‘

Muscle hypertrophy
http://neuromuscular.wustl.edu/musdist/dmd.html

Gowers’ sign (1)

Gowers’ sign (2)

Gowers’ sign (3)

Gowers’ sign (4)
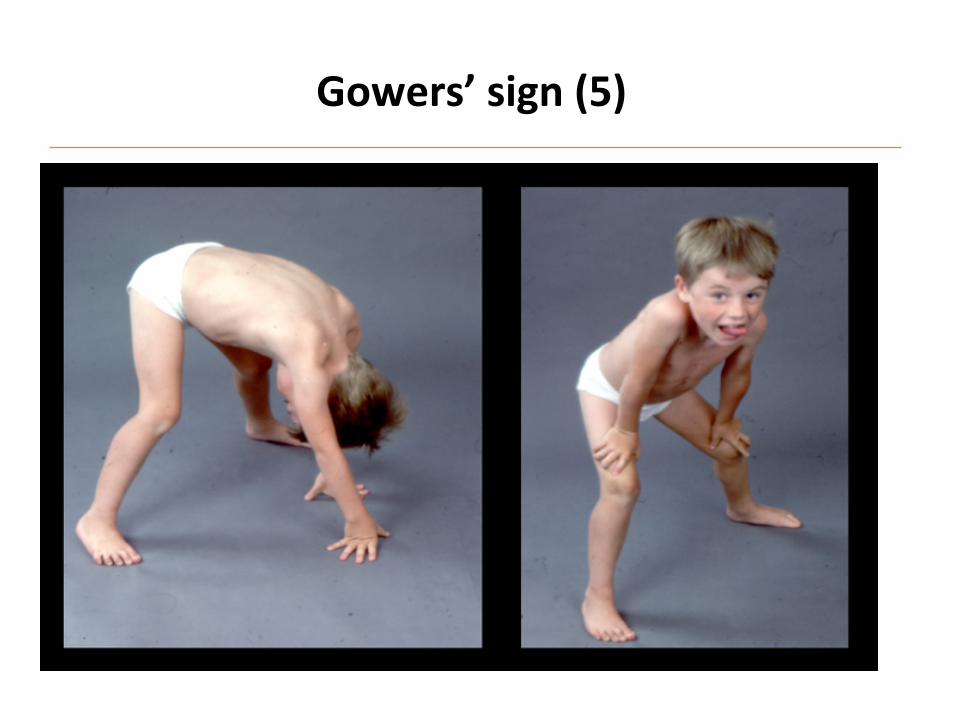
Gowers’ sign (5)

Gowers’ sign (6)


Gowers’ sign
‘Climbing up’ legs on arising from ground IndicaIve of proximal weakness in older children (>4 yrs)
Normal in younger children <3 yrs
Non-‐specific i.e. seen in any muscle disorder causing proximal weakness – DMD, BMD
– Myotonic dystrophy – Congenital myopathies
– Muscle disorders of adulthood including steroid myopathy

Muscle atrophy
Author’s own

Diagnosis of DMD
Serum creaIne kinase level – Enzyme released by damaged muscle cells into blood
– Normal <200 IU/L, DMD >10 000
Thyroid funcIon tests ( blood) – Hypothyroidism can look very much like DMD
GeneIc tesIng (by MLPA) for DMD – PosiIve in 65-‐70% cases – DeleIons 65%, duplicaIons 5%, point mutaIons 10-‐15%
Muscle biopsy
– High suspicion of DMD, geneIc tests are negaIve – Necessary in about 1/3 of cases

Serum CK (creaIne kinase) levels Normal (< 200 U/L)
Elevated
(200-‐ 800 U/L) Markedly elevated
(>1000 U/L)
Congenital myopathies Congenital myopathies + muscular dystrophies
Congenital muscular dystrophies
Endocrine myopathies Endocrine myopathies FSH MD
Myotonic dystrophy Myotonic dystrophy Duchenne + Becker MD
DermatomyosiIs DermatomyosiIs Limb girdle MD
Metabolic myopathies Metabolic myopathies
Myasthenic syndromes Idiopathic
SMA SMA
Pompe disease
Neuropathies Motor neuropathies

Natural history of DMD
3-‐6 yrs: ‘honeymoon’ phase – Mild weakness but overall strength and funcIon may increase
– Increasing disparity between affected child and his peers 8 yrs: difficulty climbing stairs, walking
– Increasing faIgability, inability to run and jump
– Increasingly prominent lumbar lordosis
– Progressive contractures Achilles, ITBs, hips ~ 10-‐13yrs: transiIon to wheelchair use Respiratory or cardiac failure late teens-‐early 20s


Duchenne muscular dystrophy Course
Some variability in course
AmbulaIon lost anywhere between 8-‐14 years
Gradual decline in upper limb funcIon
– Difficulty bringing hands to mouth by 16-‐18years
Death average approx. 25 years
Death is usually from respiratory failure
Cardiac death in about 10%
– Cardiomyopathy or arrhythmias


Natural history of Becker MD
Onset amer age 5 yrs – Commonly 5-‐15 yrs – Occasionally as late as 3rd or 4th decade
Progressive limb-‐girdle weakness Calf pain and myalgias common
Able to walk amer 15 yrs Respiratory failure amer 4th decade Cardiomyopathy is MORE common than in DMD
– Greater strain on heart caused by greater exercise and acIvity
Duchenne muscular dystrophy Respiratory deficit
Weakness of intercostal muscles > diaphragm
In the early years, vital capacity increases with age and growth
In the early teens, vital capacity plateaus and then declines steadily (5-‐10%/ year)
Respiratory failure typically occurs in the late teens or early 20s

Sleep-‐disordered breathing
Muscle weakness causes restricIve lung disease In all neuromuscular disorders, respiratory muscle funcIon is worst in sleep
– Decreased respiratory muscle tone and central drive This sleep-‐disordered breathing (SDB) is worst in REM sleep
May manifest with sleepiness, headache etc
– FaIgability, poor exercise tolerance, poor school performance – Symptoms relate to CO2 retenIon, not to hypoxia
– Does not cause shortness of breath or cough Progresses to nocturnal and then also dayIme hypovenIlaIon
Early recogniIon enables appropriate treatment

Typical forms of lung disease
Obstruc(ve lung disease – Increased resistance to airflow due to parIal or complete obstrucIon at any
level (trachea, bronchi, terminal or respiratory bronchioles)
– Lung funcIon tests show decreased maximal airflow rates during forced expiraIon, usually measured by forced expiratory volume in 1 sec (FEV1)
Restric(ve lung disease
– Reduced expansion of lung parenchyma and decreased total lung capacity.
– Lung funcIon tests show a reduced total lung capacity (TLC), and an expiratory flow rate that is normal or reduced proporIonately to TLC.
– RestricIve defects occur in two general condiIons
(1) chest wall disorders e.g. neuromuscular diseases, severe obesity, kyphoscoliosis
(2) chronic inters((al and infiltra(ve diseases, e.g. pneumoconioses and intersIIal fibrosis

Advanced Duchenne muscular dystrophy Respiratory deficit
Progresses to nocturnal and then also dayIme hypovenIlaIon
Hypoxia occurs late in the disease course
Development of atelectasis, pneumoniIs
– Pump failure-‐ poor inflaIon and emptying of lungs
Loss of respiratory reserve correlates with severity of kyphoscoliosis
– Scoliosis is caused by weakness of paraspinal muscles
Diaphragm relaIvely spared Ill late in disease

Cardiac involvement in DMD and BMD
Dilated cardiomyopathy > hypertrophic > conducIon defects Cardiomyopathy
– Decreased lem ventricular contracIlity , occasional cardiac failure – Commonly asymptomaIc/ subclinical
– 1/3 teenage yrs, ½ by 18 yrs, all >18 yrs – Symptoms omen minimal unIl late owing to musculoskeletal limitaIons
Myocardial fibrosis, sinus tachycardia, ectopic rhythms – 90% abnormal ECG
Cardiac death in 10% of cases
Cardiomyopathy more common in Becker MD

Dilated cardiomyopathy most common in DMD
(NB: Images differ slightly from those in presentation)
© 2011 UpToDate ®

Orthopaedic involvement in DMD
Early toe-‐walking common Achilles tendon and ilioIbial band (ITB) contractures
Progressive contractures: hips, knees, elbows, wrists
– More problemaIc amer wheelchair-‐bound, immobile Scoliosis
– Increases rapidly amer non-‐ambulant
Leitao et al. Sao Paulo Medical Journal 113: 995 – 999, 1995

Scoliosis repair stabilises but does not improve respiratory funcIon
http://www.uofmhealth.org/News/884surgical+approach+to+treat+scoliosis+
CNS involvement
Non-‐progressive (staIc) cogniIve impairment – Affects verbal > performance IQ – Mean IQ shimed 1SD, approx. 80 (normal: 100) – No good correlaIon with locaIon of deleIons
Two major types – Reduced verbal IQ – Reduced total IQ < 80
Occasional auIsm

3
810
11
32
20
12
9
3
0
3
6
9
12
15
18
21
24
27
30
33
36
<50 50-59 60-69 70-79 80-89 90-99 100-109 110-119 120+
TOTA
L N
o. O
F C
ASE
S
IQ RANGE
Normal IQ distribuIon PMD Cases TOTAL -106
MEAN IQ = 86.1
DistribuIon of IQ scores in boys with DMD
Cohen et al. Dev Med.Child Neurol 1968; 10:754-‐765.

CogniIve issues in DMD
Degree of cogniIve involvement is variable – 1/3 significant learning difficulIes
SelecIve impairment of verbal working memory skills leads to increased risk of learning difficulty
Greater difficulty remembering stories, difficulty manipulaIng verbal informaIon that requires immediate memory storage, difficulty with comprehension
Profile similar in subjects with DMD regardless of whether high or low intelligence

CogniIve problems in DMD may be mulIfactorial
Altered dystrophin expression in brain – StaIc intellectual deficits
Effect of chronic illness
– School absences Psychosocial effects
– Anxiety – Depression – Behavioural problems (increased by steroids)
Effect upon family
– Parental expectaIons – Parental mood problems

DMD: Summary: clinical findings
Boys appear relaIvely normal for first few years of life Then: rapid loss of muscle strength and funcIon MulIple systems involved
– Musculoskeletal
– Respiratory – Cardiac – CNS – Orthopaedic
Management must address all affected systems