biology of anal squamous cell carcinoma
TRANSCRIPT

BiologyofAnalSquamousCellCarcinoma
ProfEricRaymond,MD,PhDHôpitaux ParisSaint-Joseph
January2017

TrendsinAnalCancerIncidencebyAgeGroups
Source:SurveillanceEpidemiologyandEndResults– http://seer.cancer.gov/data Accessed8/18/2013

Thomison 2008,HumanPathology,39:154
HPVINFECTIONANDANALDYSPLASIAANDANALCANCER
PreventionofAnalCancerandotherHPVrelateddisease
• Merck– GardasilandGardasil-9arebothFDAapprovedforuseinmalesandfemales9– 26yrsofage
• Dosingis0.5mlattime0,1monthand6months• Bothgardasil vaccineshavebeenshowntopreventHPVrelatedcytologic changesduetotypespecificHPVsub-types
• GSK– Cervarix isonlyFDAapprovedforfemalesfromage9– 25yrs ofage• Dosingis0.5mlattime0,1monthand6months
• CondomusemayreduceHPVtransmissionbutsignificantleveloftransmissiondoesoccureveninthesettingofconsistentcondomuse
ClinCancerRes 2016
Molecularbiologyofanalsquamoous cellcarcinomas(ASCCs)
• AnalysisofseverallargecohortsofASCCshaveshownthatthemajorityofASCCsharborhumanpapillomavirus(HPV)
• HPVassociatedASCCshaveincreasedsensitivitytoCRTandimproveddiseaseoutcomescomparedtonon-HPVassociatedtumors
• KRAS,NRAS,andHRASmutationsareunfrequentlyobserved
• immunohistochemistry(IHC)revealedhighlevelsofEGFRexpressionandfrequentmutationsinthePIK3CA/AKTpathwaypriortotherapy
ClinCancerRes 2016
ManagementandPrognosisofAnalCancer• TreatmentforAnalCancer1
• ChemotherapywithMitomycin-Cand5-Flouro-uracilandRadiation
• Abdomino-PelvicResectiononlyforresidualdiseasepostChemo-RT
• FiveyearsurvivalratesofanalcancerinUS2• Localdisease– 78%• Regionaldisease– 56%• Distantdisease– 18%
1. Ajani JAetal;2008:JAMA299(16):1914-212. JohnsonLGetal;2004:Cancer;101:281- 288

Thenumberoftotalmutationsincreasesinrecurrenttumorsafterradiochemotherapy
ClinCancerRes 2016

Afterradiochemotherapy
• Atotalof2980somaticmutations,including1875missense,170nonsense,30frameshift,and785silentmutationswereidentified
• Thisincludes• knownactivatingmutationsinPIK3CA,• alterationsintheKEAP-1bindingdomainofNFE2L2,• mutationsinTP63andEP300,genesinvolvedinsquamouscelldifferentiation
• Inadditionotherbiologicalpatternswereobserved:• activatingMAPK1and• inactivatingPTENmutations
• Interestingly,• singleHPVnegativecasedidnothaveaTP53mutation• HPVpositivecasesharboredTP53mutations
ClinCancerRes 2016

Cellular&MolecularComponentsoftheCarcinomaMicroenvironment
EndothelialcellsPericytesVEGFR-PDGFR
Tcells(CD4-Treg)CD4:PD1-CTLA4-CD28Treg:CD73-CD39
DendriticcellsPDL1-PD1-MSHII-CD80/86
TumorassociatedmacrophagesCXCR4-TGFβR
TumorcellsTGFβR-MET-PDL1
FibroblastsFGFR
TGFβHGFFGF19IL8IL10
SDF1/CXCL12
MHC
PD-L1
PD-1
PD-1
T-cellreceptor
PD-L2
Tcell
NFκB
Other
PI3K
Tumorcell
IFNγ
IFNγR
Shp-2
Nivolumab
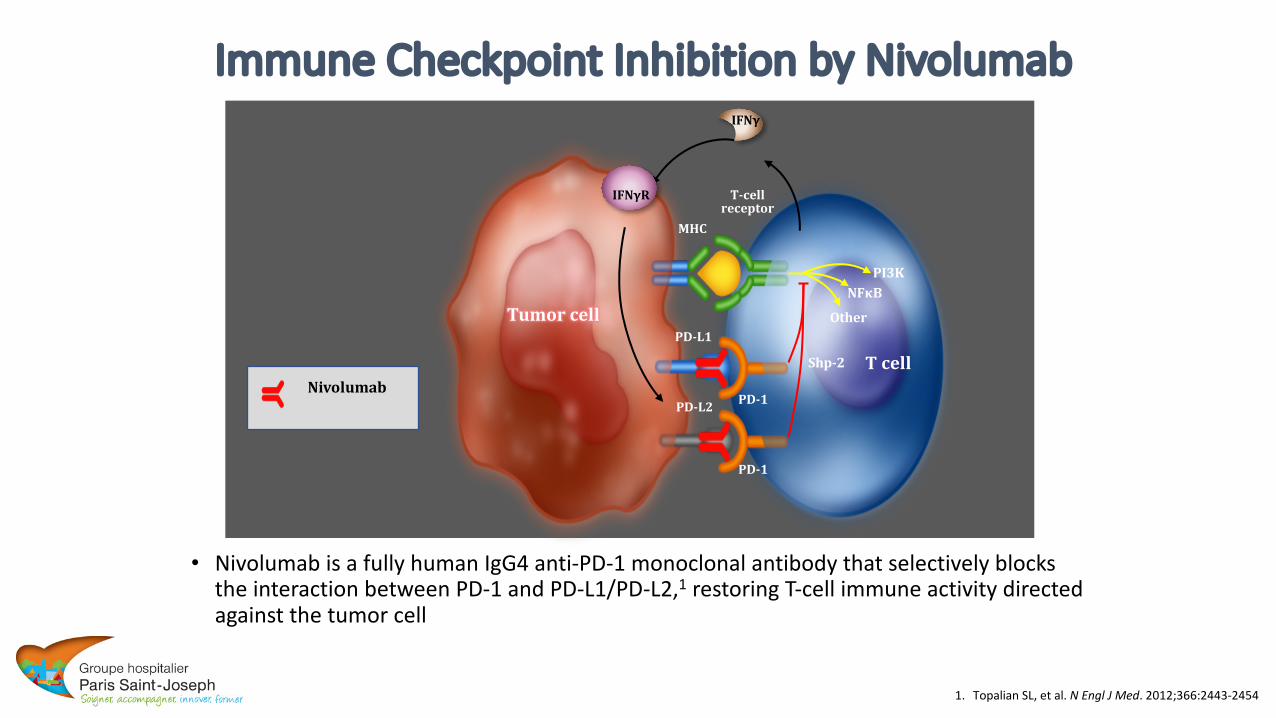
ImmuneCheckpointInhibitionbyNivolumab
• Nivolumab isafullyhumanIgG4anti-PD-1monoclonalantibodythatselectivelyblockstheinteractionbetweenPD-1andPD-L1/PD-L2,1 restoringT-cellimmuneactivitydirectedagainstthetumorcell
1. Topalian SL,etal.NEnglJMed.2012;366:2443-2454

CA209-040:Response KineticsORR:around15%- MedianDurationresponse17months
TimeSinceFirstDose,Months
Chan
geinTa
rgetLe
sion
From
Baseline,%
180
0 3 6 9 12 15 18 21
-100
-80
-60
-40
-20
0
20
40
60
80
100 Months,range
Uninfected(n=21)
HCV(n=11)
HBV(n=10)
TotalEvaluable(n=42)
DOR 7.2*– 12.5* 1.4*– 8.3* 11.9 1.4*– 12.5*
DurationofSD 1.1*– 17.3* 2.9† – 14.0 2.7*– 6.9* 1.1*– 17.3*
*Censored†Patient with resolved HCV infectionFirst occurrence of new lesion
11
+
AnthonyB.El-Khoueiry etal.ASCO2015
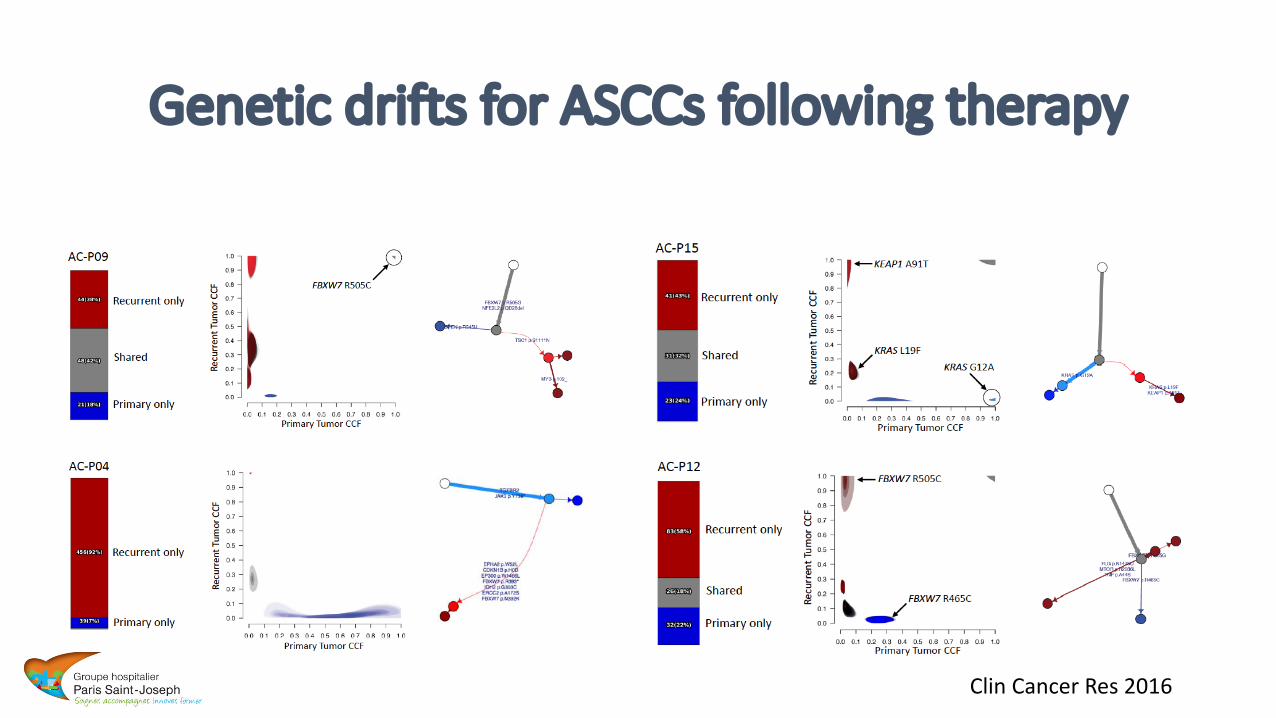
GeneticdriftsforASCCsfollowingtherapy
ClinCancerRes 2016

GeneticalterationsleadtomTOR pathwayactivation
ActivationofthemTOR pathwayClinCancerRes 2016

AnalogyAnalSquamousCellCarcinoma
Head&NeckSquamousCellCarcinoma

InHNSCC,thePI3K/mTORpathwayisactivated>70%oftumorsandyieldspoorprognosis
PI3k gene amplification (40-50%)
or mutation (11-40%)
Receptor activationEGFR >90%
PTEN Loss of function:
gene mutation (10-15%), deletion
or promoter methylation
Faivre etal.NatRevDrugDisc,2006
(No RAS mutation)
Everolimus
Conclusions
• Analsquamouscellcarcinomasareraretumorsofincreasingincidence• VaccinationofHPV16-18forcancerpreventioninimmunocompromisedpatients(HIV,chronicsteroids,immunosuppressivemedicationposttransplantation,…)
• Understandingtumorbiologyatthelevelofcancercellmutationsandchangesintumormicroenvironmentmayhelpidentifyingpoorprognosticpatientsanddevelopnovelanticancerdrugs
• Noveltherapeuticstrategiesmayinvolve:• Immunotherapies• mTOR inhibitors• Drugsinhibitingkeystepsinepithelial-to-mesenchymaltransition(MET,TGF-beta,CXCR4,etc…)