biological threats outbreaks, attacks and accidents · observations (continued) the response from...
TRANSCRIPT
Biological Threats
Outbreaks, Attacks and Accidents
Prevent, Detect and Respond
A Global Health and National Security Imperative
Gerald W Parker, DVM, PhDAssociate Vice President Public Health Preparedness and Response
Texas A&M Health Science Center
Interim Director, Institute for Infectious Animal Diseases
Texas A&M AgriLife Research

Topics
Evolving Biological Threats and Policy
Lessons observed: 2 Cases
2001 Anthrax
2014 Ebola response
National Security Strategy
Global Health Security Agenda

Evolving Biological Threats
Threat Agents Traditional threats remain
Engineered and advanced threats
Emerging infectious diseases
Threat Events Accidental release
Deliberate elicit use by offensive weapons programs State
Non-state
Lone actor
Naturally-occurring, emerging trans-boundary infectious diseases (zoonotic)
Therapeutic resistance
DURC
Traditional
Threats
Emerging
ThreatsAdvanced
Threats
Popular Biology ~2025

“Pathogenic microbes can be resilient,
dangerous foes.
Although it is impossible to predict
their individual emergence in time
and place, we can be confident that
new microbial diseases will emerge.”
– IOM, 1992
Emerging Infectious
Diseases

Biodefense & Emerging Infectious Disease Highlights
Biological &
Toxin Weapons
Convention
Sarin
attack in
Tokyo by
Aum
Shinrikyo
H5N1
Pandemic
potential
CDC Laboratory
Response Network &
Strategic National
Stockpile
Al Qaeda 911
& Anthrax
letter attacks
CDC and NIH
Biodefense
preparedness
programs
expand rapidly
SARS
H5N1
Pandemic
potential
Project
BioShield
H5N1 Pandemic
Influenza Emergency
Supplemental
Appropriations
Hurricanes
Pandemic & All
Hazards
Preparedness Act
H1N1
Pandemic
Middle East
Coronavirus
Ebola
1972 1995 20161997 1999 2001 2003 2004 2005 2006 2009 2012 2014

ANTHRAX ATTACKS OF
2001

2001 Anthrax Attack
Observations
The 2001 attacks may be easiest type of bioterrorist strike to confront even so their impact was far-reaching:
Two branches of the Federal Government were temporarily shut down & U.S. Postal operations significantly disrupted
Only 22 individuals contracted anthrax (11 inhalational & 11 cutaneous)
More than 33,000 required post-exposure antibiotics
Direct economic cost (losses) ~ $3 Billion
Decontamination of Senate office building, Postal Process plant and AMI building cost ~$320 Million

Observations (Continued)
The response from medical, public health & law enforcement communities was massive.
1000 physicians, epidemiologists, public health official & medical practitioners.
U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID) performed 30,000 tests on 10,000 samples.
400 contractors & as many 400 government workers needed to decontaminate just the Hart U.S. Senate Office Building.
These attacks revealed weaknesses in almost every aspect of U.S. bio-preparedness.
The failure to communicate a clear message to the public was on of the greatest problems.
Key Lessons Learned
Establish clear chain of command for incident response
1. Develop check list of key immediate actions
2. Expand cooperation between medical, public health & law
enforcement communities
3. Establish reliable 1st responder communications
4. Exchange liaisons, increase 1st responder training & joint exercises

Key Lessons Learned Continued
Develop comprehensive communication strategies
1. Develop coordinated media strategy
2. Prepare public messages in advance
3. Establish joint information center for sharing data
Improve ability to detect a biological attack early
1. Expand environmental detection systems
2. Improve clinical & forensic diagnostic capabilities
3. Alert medical community immediately
Key Lessons Learned Continued
Develop local distribution plans for antibiotics, vaccine
administration & provision of treatment of mass casualties
1. Develop stockpile and mass delivery strategies
2. Incorporate mental health needs into response plans
3. Strengthen civil defense
4. Need Anthrax Vaccine and surge capability
Expand local & regional surge capacities for mass-casualty care.
Improve large-area decontamination capabilities

0
20
40
60
80
100
0 1 2 3 4 5 6 7 8
Time after Attack (days)
Perc
en
t In
fecte
d i
n I
ncu
bati
on
Pe
rce
nt W
e C
an
Sa
ve
w
ith
Ora
l A
nti
bio
tic
sDetect
Decide
Distribute
Dispense
Baccam, P. & Boechler, M, “Public Health Response to an Anthrax Attack: An Evaluation of Vaccination Policy Options,”
Biosecuirty and Bioterrorism: Biodefense Strategy, Practice and Science Vol 5, #1, 2007 pp. 26-34.
Saving Lives Requires Fast, Effective Response

Summary
2001 anthrax letter attacks demonstrated biological risk is real
Even small scale attacks can have national & international impacts;
Defense against biological attacks requires extensive preparation, coordination & vigilance;
Must be underpinned by robust research foundation
Saving lives after an attack requires effective response that is fast with robust logistics to deliver medical countermeasures
Microbial forensics established as a new science
Laboratory biosecurity, personal reliability, and biosafety

Current Concern: Aerosol ReleasePast Experience: 2001 Anthrax Attacks
Number that received
antibiotic treatment
30,000
Number of illnesses 22
Number of deaths 5
Decontamination 3 Buildings ~$320 M
Direct Economic Cost >$1 B
Number that will need antibiotic treatment 1.9-3.4 M
Number of illnesses ~450,000
Number of deaths ~380,000
Decontamination City wide
Projected Economic Cost >$1.8 T
1 gm via letters 1-2 kg via cropduster
The Simplest Versus the
Most Realistic Attack Scenario

Comprehensive Biodefense
Strategy
THREAT
AWARENESS
PREVENTION AND
PROTECTION
SURVEILLANCE
AND DETECTION
RESPONSE AND
RECOVERY
BW related
intelligence
Proactive
prevention
(vaccination)
Critical
infrastructure
protection
(collective
protection)
Attack warning
(biosurveillance)
Attribution
(forensics)
Response planning
Mass casualty care
(surge medical care)
(rapid distribution of
medical
countermeasures)
Risk communication
Medical counter-
measure development
Decontamination
HSPD-10
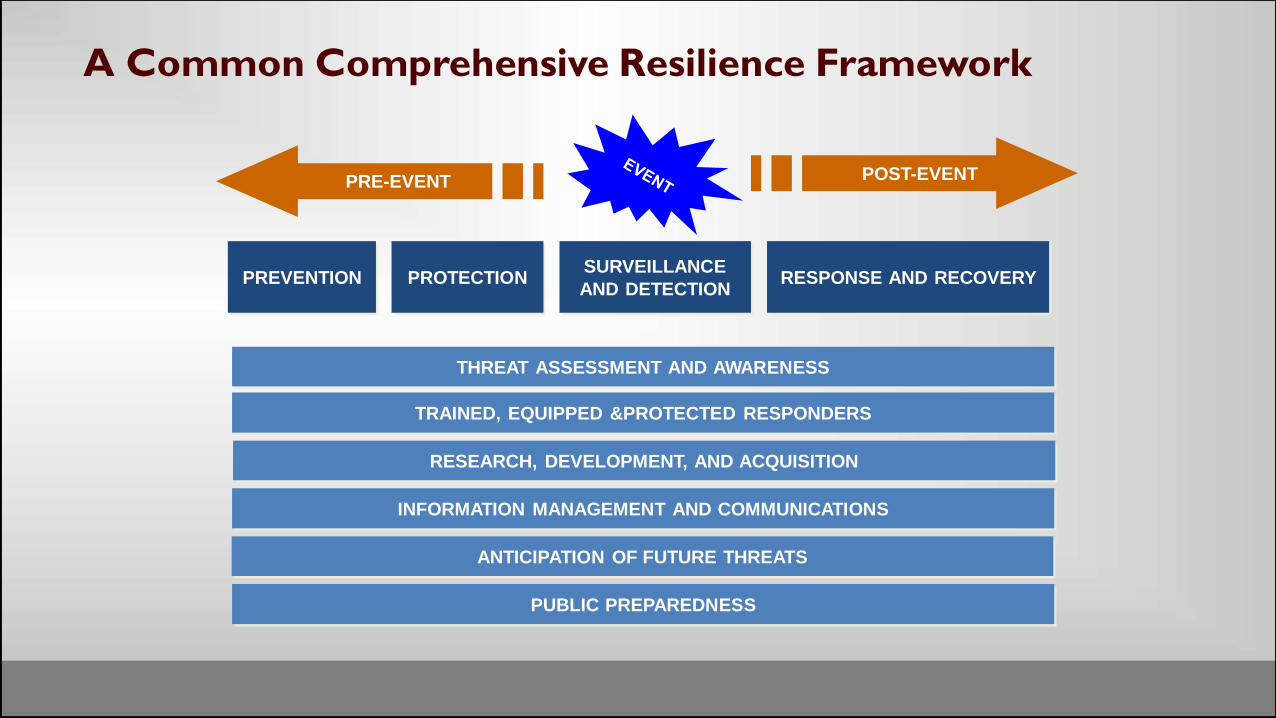
A Common Comprehensive Resilience Framework
PREVENTION PROTECTIONSURVEILLANCE
AND DETECTIONRESPONSE AND RECOVERY
ANTICIPATION OF FUTURE THREATS
INFORMATION MANAGEMENT AND COMMUNICATIONS
TRAINED, EQUIPPED &PROTECTED RESPONDERS
RESEARCH, DEVELOPMENT, AND ACQUISITION
THREAT ASSESSMENT AND AWARENESS
PUBLIC PREPAREDNESS
POST-EVENTPRE-EVENT

Filovirus Emergence
Since 1976
Martines RB, et al. J Pathol 10-9-2014 E-pub ahead of print

WHO Sit Rep
Guinea
Liberia
Sierra Leone
01/06/2016

Current Outbreak In West Africa
• Liberia declared EVD free
Jan 2016
• Sierra Leone declared EVD free
• Guinea declared EVD free
Nov / Dec 2015
• Mali declared EVD free
Jan 2015
• Senegal & Nigeria declared EVD free
Oct 2014
• WHO declares “public health emergency of
international concern”
• Outbreak spreads to include Guinea, Liberia, Sierra Leone, Senegal, Nigeria, and Mali
Aug 2014
• WHO notified of rapidly evolving situation.
• MSF -unprecedentedand warned of difficulties combating EVD
March 2014
• Epidemic began in Guinea -index patient thought to be a 2 year old child
Dec 2013

Why was this outbreak so bad?
2013-2016 Ebola epidemic is the largest in history
> 28,000 cases, >11,000 deaths

N Engl J Med Oct 16, 2014; 371(16):1481-1495
Contributing factors
Delayed recognition, diagnosis, and public health response
Epicenter located on a 3 border region
First cases: Gueckedou and Macenta Highly interconnected populations
Easy connections by roads: rural and urban areas
EVD spread to cities
Overcrowding and poor sanitation
Cultural and social factors
Distrust of government authorities
Inadequate health care infrastructure

From Liberia to Dallas
Depart Liberia 19 September
Arrive Dallas 20 September
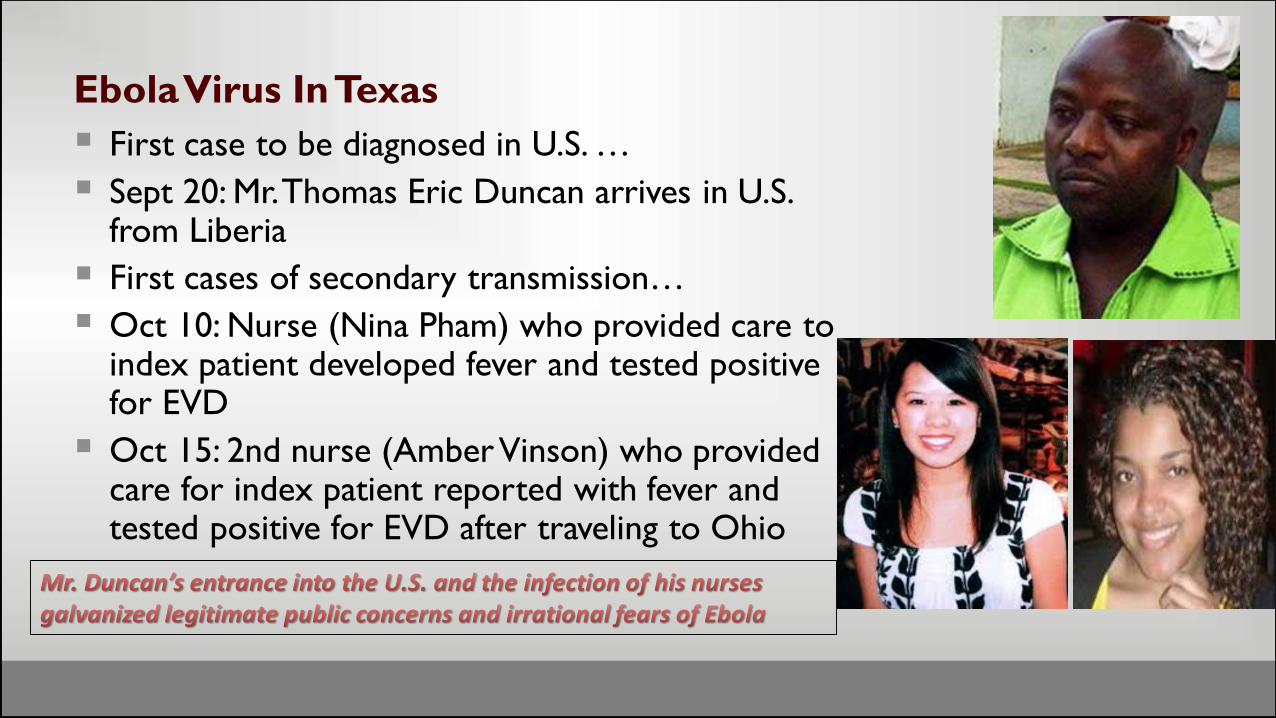
Ebola Virus In Texas
First case to be diagnosed in U.S. …
Sept 20: Mr. Thomas Eric Duncan arrives in U.S. from Liberia
First cases of secondary transmission…
Oct 10: Nurse (Nina Pham) who provided care to index patient developed fever and tested positive for EVD
Oct 15: 2nd nurse (Amber Vinson) who provided care for index patient reported with fever and tested positive for EVD after traveling to Ohio

First Ebola Virus Disease Diagnosis in U.S. Occurs in Texas
Texas has sophisticated and one of the nation’s best emergency management system, but
Texas faced unique public health emergency that required extraordinary efforts from public health experts, health care workers, emergency responders, and private sector partners, as well as local, state, and federal leaders
Disaster response requires coordinated response among state and local governments, community support organizations, and multidisciplinary responders Emergency management, public health, search & rescue, law enforcement,
transportation oversight, environmental controls, communications, and logistics
Public health is a team sport

Forensics of the Ebola Response
Decision Making: Who’s in charge?
HazMat: How clean is “clean”?
Communications: media, media, media
Contact tracing & monitoring
The lack of vaccines and therapies
Health care worker protection
Irrational, but legitimate public fear
Ethics: individual, local, national, global
Hospital surge capability & capacity Laboratory testing

Disasters Are Managed Locally
Trial By Ebola. Vanity Fair; February 2015

1. Hospital care
2. Identification and isolation triage
3. Hospital Preparedness Program
4. Education and training
5. Hospital care – experimental drugs
6. Personal protective equipment
7. Control order authority
8. Epi monitoring and contact tracing
9. Disposition of deceased
10. Housing and social services
11. Laboratory testing and sample transport
12. Guidelines for monitoring HCW
13. Incident command
14. Decontamination and waste removal
15. Communications
16. Care of domestic animals
17. Task Force future role
Texas Task Force Infectious Disease Preparedness
& Response

31
Transportation assures rapid global spread of emerging diseases
Emergence of new, virulent pathogens
(50 appeared since 1973)
The Natural Threat
SARSH7N9
WHO calls Middle Eastern virus,
MERS, ‘threat to the entire world’
May 29, 2013
West Nile virus: Dallas declares
state of emergency
August 16, 2012
The Modern Reality of Emerging Infectious Diseases

Major Emerging and Reemerging Infectious-Disease
Outbreaks, Epidemics, and Pandemics, 2002 through 2015.
: Figure 1 From Sands, et al., The Neglected Dimension of Global Security—A Framework for Countering Infectious
Disease Crises, NEW ENGLAND J. OF MEDICINE (Jan. 13, 2016)

Bioterrorism Report Card:
U.S. unprepared
October 12, 2011
Syria, North Korea,
Iran, Egypt, etc.
Iraq arrests five in 'al-Qaeda
chemical weapons plot‘Al-Qaeda planned to strike targets in Iraq,
Europe and North America with chemical
weapons…
June 2, 2013
33
The Escalating Threat of CBRN Attack

A Common Comprehensive Resilience Framework
PREVENTION PROTECTIONSURVEILLANCE
AND DETECTIONRESPONSE AND RECOVERY
ANTICIPATION OF FUTURE THREATS
INFORMATION MANAGEMENT AND COMMUNICATIONS
TRAINED, EQUIPPED &PROTECTED RESPONDERS
RESEARCH, DEVELOPMENT, AND ACQUISITION
THREAT ASSESSMENT AND AWARENESS
PUBLIC PREPAREDNESS
POST-EVENTPRE-EVENT

The effective dissemination of a lethal
biological agent within a population
center would endanger the lives of
hundreds of thousands of people and
have unprecedented economic, societal,
and political consequences.
We must continue to work at home with
first responders and health officials to
reduce the risk associated with
unintentional or deliberate outbreaks of
infectious disease and to strengthen our
resilience across the spectrum of high-
consequence biological threats.
National Security Strategy 2010

Global Health Security Agenda 2014
A NATIONAL
BLUEPRINT FOR
BIODEFENSE: LEADERSHIP AND REFORM NEEDED
TO OPTIMIZE EFFORTS
BIPARTISAN REPORT OF THE BLUE RIBBON
STUDY PANEL AND BIODEFENSEOCTOBER 2015
Institute Sponsors: Hudson Institute Inter University Center
For Terrorism Studies

Essential Tasks in Responding to a Biological Incident of
Potential National Significance:
Priority Considerations, Decisions & Actions
Save Lives Ensuring rapid identification of attack, diagnosis and confirmation
Providing medical care
Distributing & administrating medical countermeasures as needed and in time
Maintain Order and Continuity of Operations Ensuring coordinated multi-disciplinary response
Ensuring security of assets
Ensuring security and operation of critical infrastructure
Manage the Crises and Prepare for Future Incident Sharing essential information and intelligence
Enhancing protection
Increasing detection capabilities

Local Public Health and Emergency Management Are On
the Frontline of Global Biologial Threats
Source: Kilpatrick AM, et al. Drivers, dynamics, and control of emerging vector-borne zoonotic diseases. The Lancet 380:9857, 1-7 Dec 2012, pp. 1946-55. www.sciencedirect.com/science/article/pii/S0140673612611519Note: Air traffic to most places in Africa, regions of South America, and parts of central Asia is low. If travel increases in these regions, additional introductions of vector-borne pathogens are probable.

Biological Threats
Outbreaks, Attacks and Accidents
Prevent, Detect and Respond
A Global Health and National Security Imperative
Gerald W Parker, DVM, PhDAssociate Vice President Public Health Preparedness and Response
Texas A&M Health Science Center
Interim Director, Institute for Infectious Animal Diseases
Texas A&M AgriLife Research