best of immuno-oncology
TRANSCRIPT

BEST OF IMMUNO-ONCOLOGY

Anticipating antibodies 4
The growing potential of CAR T-cell therapy 11
Personalized cancer therapy directed by immune-profiling 14
Making sense of immuno-oncology 16
Immuno-oncology—Gold rush or a golden age? 20
The importance of cancer neoepitope discovery 22
Contents Foreword
Immuno-oncology is not a new concept. Going back to at least the 17th century, the idea of enlisting the immune system in the fight against tumors has had a place in medicine. Of course, back then the strategy was to intentionally cause an infection in the vicinity of the tumor to prime the body to heal itself.
The late 1990s and early 2000s, thankfully, were a bit more refined in terms of cancer immunotherapy—bringing us our first monoclonal antibody therapies for cancer. And more recently—in 2017—the first approved chimeric antigen receptor T-cell (CAR T) therapy. There are also dendritic cell therapies and cytokine therapies prominent in recent immuno-oncology efforts.
Here in this eBook we provide you a quick peek into our most prominent and still-perti-nent coverage of cancer immunotherapeutic efforts in the drug discovery and develop-ment realm, with one special report, four guest commentaries and one research news roundup from DDN magazine between 2018 and 2020.
Surgery, chemotherapy, radiation therapy and other members of the “old guard” will no doubt continue to play necessary roles in cancer treatment, but the promise of less harmful—and hopefully more robust—results seems to lie in the realm of targeted chemical or biological attacks on tumors, and that is an arena in which immuno-oncology is definitely a rising star.
Drug Discovery News Best of Immuno-Oncology
Perform functional genestudies in primary cells
Carry out loss- or gain-of-function experiments in physiologically relevant cells. Screen in clinically relevant cell types to help avoid misleading hits from cell lines and
reduce the risk of downstream complications in your drug discovery pipeline.
horizondiscovery.com
Accell self-delivering siRNA • Silence gene expression in difficult-to-transfect cells
Synthetic and lentiviral CRISPR sgRNA • Knockout a gene with accuracy and efficiency
Pooled and arrayed T-cell screens • Elucidate genes that are crucial for T cell functionality and efficacy
Arrayed B-cell screens • Understand how genes contribute to Breg function in health and disease
Trusted CRISPR and RNAi reagents
RNA-based immune cellscreening services
CRISPRand RNAispecialists
©2020 The Horizon logo and other trademarks are the property of Horizon Discovery Limited, unless otherwise stated. DHARMACON is a trademark of Dharmacon Inc.
Contractresearchservices
4Drug Discovery News
ANTICIPATING ANTIBODIES Digging deeper into repertoires means tapping into Plan B (cell)BY RANDALL C WILLIS, DDN FEATURES EDITOR
As little as a decade ago, sitting through any session of the AACR or ASCO conferences, one could not help but be struck by the activity and potential for immunotherapies.
What started as a trickle of monoclonal antibody (mAb) therapies in the late 1990s became a steady flow in the 2000s and a torrent in the 2010s.
But even as more biotherapeutics were approved and more com-panies explored the space, the benchmarks of success rose almost as quickly as the price tags associated with treatment. And while the development of products like rituximab and trastuzumab could never be described as easy, many consider those first few antibody targets the low-hanging fruit of immuno-oncology.
In the push to enhance the precision of treatment or to develop follow-on biotherapies when the initial molecules cease to work, researchers have had to explore increasingly intractable targets that often represent increasingly smaller patient populations. The result of that extra work and those smaller markets is an increasing price tag that, in some cases, threatens to shift the cost-benefit analysis.
Unable to change the patient population, researchers are faced with having to increase the efficiency of antibody discovery and development, working to focus as much energy as possible on only those candidates with the best potential for success.
Higher-hanging fruit“I’ll be very honest and say it’s hard for me really to understand how we’re going to address costs, primarily because the discovery of these drugs is not simple and it’s not getting any simpler,” admits John Proctor, senior vice president of marketing at Berkeley Lights.
“For a long time, it was all about monoclonal antibodies, and there have been some amazing mAbs discovered,” he continues, adding that although people continue to explore mAb discovery, it
is often with an eye toward combining antibodies as bi- or trispe-cific molecules.
That, he points out, has introduced a level of complexity that is only now being realized. It is simple math.
“If you need two or potentially three antibodies to make one drug, then you need two to three times the number of campaigns than you did previously,” he says. “And, on top of that number of campaigns, you also have to be able to assess the diversity of antibodies generated against the particular target very quickly.”
For AbCellera CEO Carl Hansen, that perception of complexity has been an issue since the earliest days of the antibody therapeutics.
“If you roll back 30 years, therapeutic antibodies were not even on anyone’s radar,” he recounts. “In fact, when people first started doing them, the pharmaceutical industry dismissed it as being overly complex.
“Starting with some blockbusters in the 1990s, that field has grown into what is now probably north of [a] $120-billion market and has been consistently, for decades, the fastest-growing class of therapeutics.”
From his earliest days as a professor at the University of British Columbia (UBC), however, Hansen has monitored the develop-ment of the field, seeing opportunities in computation, genomics and microfluidics to address biomedical challenges.
“One of the dynamics we saw as the field has progressed was that pharmaceutical companies were being increasingly pushed toward targets that had proven to be difficult using conventional technology,” he says.
For Hansen, the best way to address these challenges was not to head to the bench to re-engineer what Mother Nature had perfected over 350 million years. Rather, he saw a need for methods that produced a better immune response and then to better screen that response to find the best molecules.
FROM 2020 SPECIAL REPORT

DDN Best of Immuno-Oncology
5Drug Discovery News
Another factor, he notes, was the birth of the biotech industry and the growth of specialized fields such as immuno-oncology, which has significantly layered on complexity to an already challenging task.
“These companies either have a new angle on biology or they have technologies that typically require some elements of antibody to make them work,” Hansen explains. “It could be CAR T. It could be bispecifics. It could be antibody-drug conjugates.”
It was in recognizing the changing landscape that Hansen’s academic interests took a more commercial turn.
“In 2012, we recognized that we could wrap those technologies together to make a best-in-world platform for searching deeply into natural immune systems to find antibodies that had the properties that made them suitable for development as therapeutics,” he recounts.
At the core of this advance was a focus on single-cell analysis.“Single-cell analysis was a theme that I worked on for over a
decade,” Hansen says. “And this was an opportunity to apply single-cell analysis to what is by far one of the most interesting things in biology: adaptive immunity. It is also one where the connection to a real problem in the industry—finding the next generation of drugs—allowed us to build a thriving business.”
Part of seizing on this opportunity meant seriously rethinking the technologies and methods that got the field to this point. Central to that was wondering if the limitations of hybridoma technology—a founding method of antibody discovery and devel-opment—had surpassed its benefits.
Aaron Winters and colleagues at Amgen Research and UBC offered their take on hybridomas in a recent paper.
The efficiency of immortalizing antibody-secreting cells through fusion with myeloma cells is quite low, they suggested. Even with optimized electrofusion protocols, as few as one in 5,000 input B cells manages to not only survive the fusion, but also become immortalized and secrete antibody.
“Additionally, hybridoma methods generally require extensive cell culture, which is labor intensive and dependent on mitosis, further slowing development timelines,” the authors continued.
This challenge, they argued, can lead to the identification of low-affinity antibodies, and often requires multiple rounds of resource-intensive affinity maturation to generate potent molecules.
In some ways, Hansen suggests, those limitations were accept-able in the early days because of the targets that researchers were tackling.
“Thirty years ago, that was fine,” he remarks. “There were easy targets, there wasn’t a lot of competition, and all you needed to find was any old antibody that happened to bind the target and block it.”
Hansen adds that another bonus was that it was pretty easy to mount immune responses against the chosen targets.
“Hybridoma, for that reason, has been the cornerstone from which we have had the blockbusters that we do today,” he continues.
“One of the big advantages of hybridoma is that it allows you to go after antibodies from natural immune responses, as compared to synthetic approaches—e.g., doing yeast or phage display—and they have been much more successful in getting through to the clinic,” he recalls. “I think 80 percent or more of the antibodies that have been approved have come from immunizations or from natural sources.”
However, Hansen is quick to highlight the inherent limitations of what he calls the Franken-cell approach and the loss of more than 99 percent of what was available in the animal starting material.
Implementing plan B“If you care about diversity, which is the thing that we really emphasize in our program, it is important to have a large number of antibodies so that you’re not just picking any antibodies that work, but rather you are picking the one that is most potent and has the properties that make it most quickly and easily developable into a drug,” Hansen notes. “You want to make sure that you cast as wide a net as possible.”
“We are in a numbers game,” adds Marian Rehak, vice president of research and development at Sphere Fluidics. “If you want to screen the whole repertoire, you need the technology that allows you to do that.”
With such challenges in mind, Winters and colleagues heralded the advent of microfluidic and microencapsulation technologies that permit the direct identification and characterization of anti-body-secreting B cells.
“These micro tools eliminate the need for immortalization, are species-agnostic, allow high-throughput sampling as well as
Therapeutics using antibodies for the treatment of cancer went from a trickle in the late 1990s to a torrent in the 2010s. But in the push to enhance the precision of treatment or to develop follow-on biotherapies when the initial molecules cease to work, researchers have had to explore increasingly intractable targets that often represent increasingly smaller patient populations.
“If you need two or potentially three antibodies to make one drug, then you need two to three times the number of campaigns than you did previously. And, on top of that number of campaigns, you also have to be able to assess the diversity of antibodies generated against the particular target very quickly.”
- John Proctor of Berkeley Lights

DDN Best of Immuno-Oncology
6Drug Discovery News
multiparameter phenotyping of the input cells, have reduced reagent consumption compared to hybridoma and display technologies, and maintain the ability to retain the native VH and VL pairings of the original antibody,” they noted.
Earlier this year, Rehak and colleagues at Sphere Fluidics and UCB described the application of Cyto-Mine in both antibody discovery and cell line development. In this proof-of-concept experiment, antibody-secreting CHO cells were monitored rather than hybridomas or B cells.
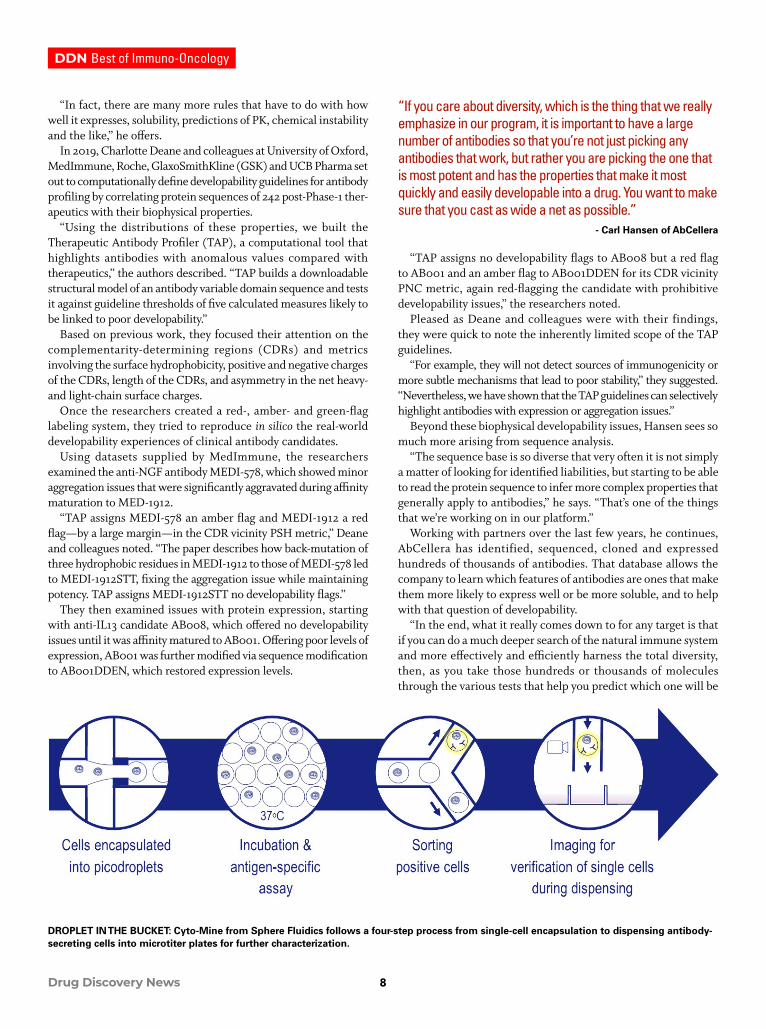
As the authors described, the process is basically broken down into four steps.
Initially, using a biocompatible surfactant, both cells and assay reagents are encapsulated with culture medium into picodroplets. These picodroplets, which can carry anywhere from zero to one to a few dozen cells as required, are then incubated to permit protein production and secretion.
Using a FRET-based assay to detect IgG production, picodroplet fluorescence is monitored and positive cells are collected and stored in a chilled microchamber or dispensed into a collection device, such as single cells into microtiter wells. Negative picodroplets, meanwhile, are diverted to waste.
The assay can be customized by the selection of appropriate FRET-based detection probes specific for the protein of interest, such as IgG, or for antigen-specific IgG using labeled antigen assays, Rehak and colleagues explained.
The picodroplets can then be interrogated a second time and verified for monoclonality.
“From all the experiments shown, there was no apparent difference in cell outgrowth rate between Cyto-Mine and manual [limiting dilution cloning],” the authors noted. “These data suggest that Cyto-Mine is a gentle and cell-friendly cloning technology.”
In this experiment, the picodroplets were approximately 450 pL in volume, which the authors suggested was about five to six orders of magnitude smaller than volumes used in assays done in a 96-well plate.
“This means that in the same time, the concentration of secreted antibodies from a single cell can be 5-6 orders of magnitude higher in picodroplets than in conventional vessels,” they explained. In a typical Cyto-Mine instrument run, between 100,000 and 40 million cells can be screened.
Thus, not only does the microfluidic system offer increased throughput at up to single-cell resolution, but it also offers significantly reduced reagent costs.
Rehak also points out that Cyto-Mine can be used to monitor cell-surface protein expression and even flag issues related to anti-body misfolding and aggregation.
Winters and colleagues had similar experiences working with Berkeley Lights’ Beacon platform in a process the Amgen team described as NanOBlast.
“Amgen was one of the earliest customers of Berkeley Lights, and they have been super-supportive of our work in developing applications for biopharma, both in antibody discovery and in cell line development,” says Berkeley Lights’ Proctor.
Rather than sequester B cells and reagents into picodroplets, the Beacon system uses microfluidics to move cells, reagents, beads
or other objects through the channels of a culturing microchip, and then optoelectronics to dispense single cells and reagents into any of hundreds or thousands of one-nanoliter reaction chambers called nanopens.
It is within these nanopens that the B cells produce antibodies, which can be assayed for IgG secretion or antigen-specific IgGs. Beyond these two basic assays, however, the system also allows researchers to perform more functional assays such as competi-tive binding, cell binding and ligand-receptor blocking. The key, according to Proctor, is to reveal functional characteristics as quickly as possible.
“If you’re able to ask basic questions, like ‘does this antibody bind my target,’ that’s informative,” he states. “But if you then have to re-express and do all of this analytical characterization downstream on, say, 1,000 antibodies because you weren’t able to assess function to find out you only have 100 on the backend, you’ve probably invested months of work and hundreds of thousands of dollars trying to answer that question.
“Because we can do these functional assays on-chip up front during the primary screen, we can find all 1,000 or however many hits would be target binders, but we could then tell you a priori that there’s only actually 100 functional ones.”
This effect was highlighted in a recent application note where 33,377 mouse plasma B cells were screened for binding to PD-L1 beads, resulting in 598 positives. These were then screened for bind-ing to PD-L1 expressed on the surface of CHO cells, reducing the positive hits to 273. A subsequent ligand-receptor blocking assay demonstrated that 46 leads not only bound PD-L1, but also blocked the interaction between fluorescently tagged PD-1 and PD-L1.
Thus, performing these assays within the same chip reduced the deeper characterization effort from 600 potential leads to 46.
Key to the platform and to maintaining cell viability are the optofluidics.
A “BEACON” OF HOPE: The Beacon system from Berkeley Lights uses microfluidics to move B cells through the channels of a culturing microchip and optoelectronics to dispense individual cells into any of hundreds or thousands of reaction chambers called nanopens, where they can be assayed for IgG production or for functional characteristics.
DDN Best of Immuno-Oncology
7Drug Discovery News
“At a very high level, we are using broad-spectrum light to activate a series of optical switches on a siliconized chip,” explains Proctor. “When we use light on that chip, the switches are essentially able to turn on and off.”
When that switch is on, he continues, it creates a dielectric force that essentially repels an object, whether it’s a microbead or a cell.
“If you just draw a box around it, so that there’s a force on all four sides, then you can move the box and the cell or object stays inside the box, and you can direct it wherever you would like on the chip,” he adds.
This progress in high-throughput B cell analysis, however, doesn’t mean that hybridomas have been completely abandoned.
Hybridoma hold-outs“We are seeing movement from hybridoma to B cells, but recently, we have also seen movement back to hybridomas,” says Rehak.
And many biopharma companies have long used and extensively validated hybridoma approaches.
Last year, Scott Dessain and colleagues at the Lankenau Insti-tute for Medical Research, FDA’s Center for Biologics Evaluation and Research, and Children’s Hospital of Pennsylvania acknowl-edged the opportunities still afforded from the technically straight-forward methods.
“They produce full-length, glycosylated mAbs that maintain their original heavy chain:light chain pairings without the need for recombinant gene expression,” the authors explained.
“However, their major shortcoming is that mAbs are secreted into the cell culture medium, so that hybridomas must be maintained in oligoclonal pools while their secreted mAbs are analyzed separately,” they acknowledged. “This impedes the discovery of rare mAbs because it imposes practical limits on the numbers of cells that can be analyzed, and is a disadvantage compared to yeast display methods, in which mAbs are expressed
on the cell surface and can be screened for antigen binding in bulk culture.”
Rather than abandon hybridomas, however, Dessain and colleagues looked for ways to mimic the cell surface expression capabilities of yeast display within the hybridoma screen. The result is the platform On-Cell mAb Screening (OCMS).
“OCMS transiently captures and displays mAbs on the hybridoma surface, while preventing mAbs from binding to cells that do not secrete them,” the authors explained.
The system relies on an anchor-linker strategy, whereby an anchor protein—an anti-rabbit IgG tandem scFv—is expressed in the fusion partner cell line and is maintained in the hybridoma. This is complemented with a rabbit anti-human IgG antibody (RAH) linker.
When RAH is added to the culture, it binds to the surface of the hybridoma cells, where it captures antibodies secreted by the cell to which it is bound. Excess RAH in the culture medium acts as a competitor to prevent secreted antibodies from one cell binding to neighboring hybridoma cells.
“This provides specificity to the reaction, so that mAbs secreted by cells within a heterogeneous population can be analyzed indi-vidually in association with the cells that make them,” Dessain and colleagues suggested. “Cells expressing mAbs with desired features can be identified by fluorescence imaging techniques.”
By mixing cells with different binding properties, the researchers showed that a given mAb was only bound by the cells that secreted that mAb. Beyond fluorescence microscopy, the researchers also demonstrated the utility of their platform with flow cytometry.
The researchers also noted how the analogy with yeast display extended beyond antibody capture at the cell surface.
“High-throughput competitive binding, epitope complemen-tation, and dissociation rate assays developed for yeast should be adaptable for screening mAbs expressed by OCMS hybridomas,” they proposed. “OCMS can also be used to assess mAb expression levels by individual cells in a heterogeneous population in real time, using either fluorescence imaging or flow cytometry.
“This feature should be useful to establish and monitor stable, high-expressing cell clones for master cell banks and bioreactor production runs.”
Earlier this year, the technology was licensed from Lankenau to be commercialized by new company OCMS Bio, for which Dessain serves as chief scientific officer.
Identifying and characterizing cells that produce antibodies against specific targets is still a long way from having some-thing that will work as an immunotherapy, however. Given that an antibody for clinical treatment faces many different stresses and strains than one in its natural immune environment, other molecular facets must be explored to determine whether a given molecule can be developed into a therapeutic.
Developability and design“The question of developability is an important one,” says Hansen.
Recognizing parallels with Lipinski’s Rules of Five in the small-molecule space, he suggests there are several metrics that they examine in the antibody space.
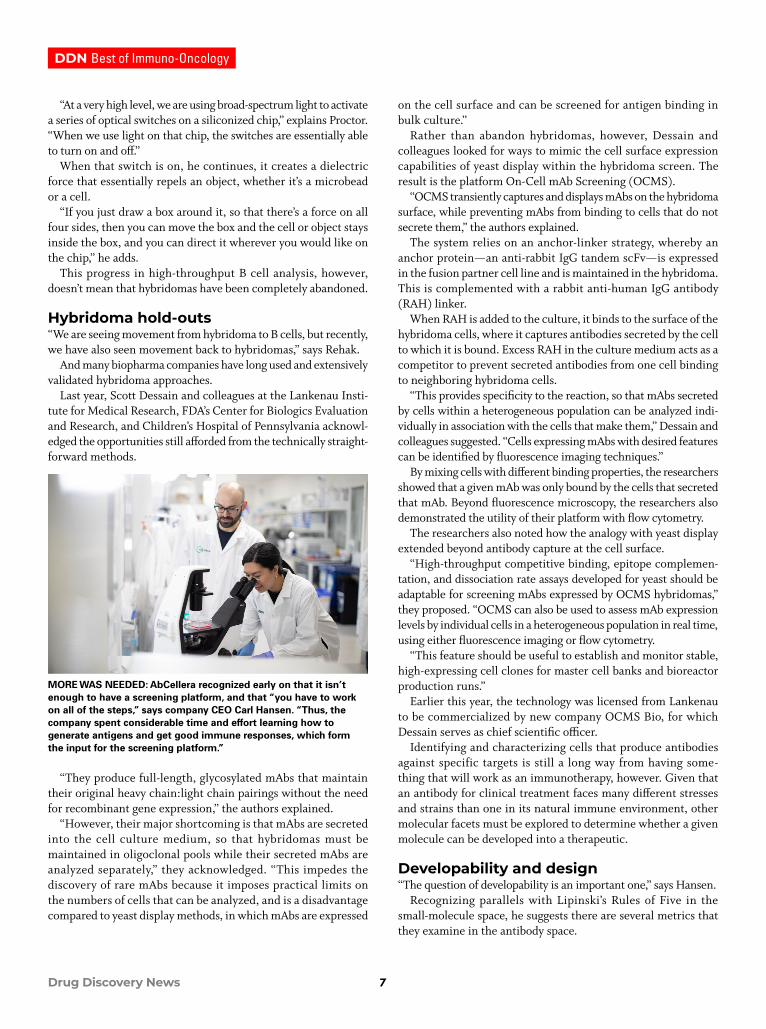
MORE WAS NEEDED: AbCellera recognized early on that it isn’t enough to have a screening platform, and that “you have to work on all of the steps,” says company CEO Carl Hansen. “Thus, the company spent considerable time and effort learning how to generate antigens and get good immune responses, which form the input for the screening platform.”
DDN Best of Immuno-Oncology
8Drug Discovery News
“In fact, there are many more rules that have to do with how well it expresses, solubility, predictions of PK, chemical instability and the like,” he offers.
In 2019, Charlotte Deane and colleagues at University of Oxford, MedImmune, Roche, GlaxoSmithKline (GSK) and UCB Pharma set out to computationally define developability guidelines for antibody profiling by correlating protein sequences of 242 post-Phase-1 ther-apeutics with their biophysical properties.
“Using the distributions of these properties, we built the Therapeutic Antibody Profiler (TAP), a computational tool that highlights antibodies with anomalous values compared with therapeutics,” the authors described. “TAP builds a downloadable structural model of an antibody variable domain sequence and tests it against guideline thresholds of five calculated measures likely to be linked to poor developability.”
Based on previous work, they focused their attention on the complementarity-determining regions (CDRs) and metrics involving the surface hydrophobicity, positive and negative charges of the CDRs, length of the CDRs, and asymmetry in the net heavy- and light-chain surface charges.
Once the researchers created a red-, amber- and green-flag labeling system, they tried to reproduce in silico the real-world developability experiences of clinical antibody candidates.
Using datasets supplied by MedImmune, the researchers examined the anti-NGF antibody MEDI-578, which showed minor aggregation issues that were significantly aggravated during affinity maturation to MED-1912.
“TAP assigns MEDI-578 an amber flag and MEDI-1912 a red flag—by a large margin—in the CDR vicinity PSH metric,” Deane and colleagues noted. “The paper describes how back-mutation of three hydrophobic residues in MEDI-1912 to those of MEDI-578 led to MEDI-1912STT, fixing the aggregation issue while maintaining potency. TAP assigns MEDI-1912STT no developability flags.”
They then examined issues with protein expression, starting with anti-IL13 candidate AB008, which offered no developability issues until it was affinity matured to AB001. Offering poor levels of expression, AB001 was further modified via sequence modification to AB001DDEN, which restored expression levels.
“TAP assigns no developability flags to AB008 but a red flag to AB001 and an amber flag to AB001DDEN for its CDR vicinity PNC metric, again red-flagging the candidate with prohibitive developability issues,” the researchers noted.
Pleased as Deane and colleagues were with their findings, they were quick to note the inherently limited scope of the TAP guidelines.
“For example, they will not detect sources of immunogenicity or more subtle mechanisms that lead to poor stability,” they suggested. “Nevertheless, we have shown that the TAP guidelines can selectively highlight antibodies with expression or aggregation issues.”
Beyond these biophysical developability issues, Hansen sees so much more arising from sequence analysis.
“The sequence base is so diverse that very often it is not simply a matter of looking for identified liabilities, but starting to be able to read the protein sequence to infer more complex properties that generally apply to antibodies,” he says. “That’s one of the things that we’re working on in our platform.”
Working with partners over the last few years, he continues, AbCellera has identified, sequenced, cloned and expressed hundreds of thousands of antibodies. That database allows the company to learn which features of antibodies are ones that make them more likely to express well or be more soluble, and to help with that question of developability.
“In the end, what it really comes down to for any target is that if you can do a much deeper search of the natural immune system and more effectively and efficiently harness the total diversity, then, as you take those hundreds or thousands of molecules through the various tests that help you predict which one will be
DROPLET IN THE BUCKET: Cyto-Mine from Sphere Fluidics follows a four-step process from single-cell encapsulation to dispensing antibody-secreting cells into microtiter plates for further characterization.
“If you care about diversity, which is the thing that we really emphasize in our program, it is important to have a large number of antibodies so that you’re not just picking any antibodies that work, but rather you are picking the one that is most potent and has the properties that make it most quickly and easily developable into a drug. You want to make sure that you cast as wide a net as possible.”
- Carl Hansen of AbCellera
DDN Best of Immuno-Oncology
9Drug Discovery News
a good drug, you can stand the attrition,” Hansen explains. “You can leave the ones that don’t have the right properties behind and still make sure that you have a robust pipeline that gets all the way to the end so that you have multiple leads that you can finally bring into clinical trials.”
The reduced candidates achieved with lower-throughput systems like hybridoma or other microfluidic systems, he contrasts, reduce your chances of finding antibodies with the right potency or developable properties.
“In the end, what that means is that you need to start circling back and doing protein engineering, and that leads to inefficiencies and delays in getting to the clinic,” he remarks.
Seeing the whole boardAbCellera recognized early on that it isn’t enough to have a screening platform, Hansen says. Rather, you have to work on all of the steps.
Thus, the company spent considerable time and effort learning how to generate antigens and get good immune responses, which form the input for the screening platform.
“If you don’t get the right input, it’s unlikely you’re going to find what you’re looking for in a drug,” he states.
“Once you’ve done that for many targets and you have a throughput like ours—we can easily screen through a million cells in an afternoon—then the challenge is no longer can I find an antibody against my target, but rather how can I get the most information content in that screen,” he suggests.
Those screens allow them to go from those thousands of hits down to a much smaller and manageable number—say, 100—that have the other properties important to turning a lead into a drug.
Hansen offers the example of a screen to determine not only if an antibody binds to the target, but also to look at cross-reactivity against eight different targets at once.
“That can help when you want to find an antibody you can test in a non-human primate or in other animals,” he explains. “It can
also help when you want an antibody that hits one receptor but misses another isoform.”
“We can do experiments to select for antibodies that have higher affinity, that recognize certain epitopes, that block ligands,” he continues. “There is a lot of functional information that can be gained.”
Each piece of information advises the next step of moving through development, starting with cloning, moving through expression, and into further testing that is simply better performed in microtiter plates.
According to Hansen, “I don’t think you’re ever going to be able to do all of those at the single-cell level. I think you want to bring some number through so that you’re doing your tests in a rigorous way.”
In March, however, Berkeley Lights announced their effort to try to expand what was possible at the single-cell level, introducing Opto Cell Line Development 2.0.
In support of this effort, Jennitte Stevens and colleagues at Amgen Research recently used GFP- and RFP-expressing CHO cells to compare clonality assurance with the Beacon platform and industry-standard FACS-assisted cell deposition and limiting dilution seeding.
“When comparing between growing colonies, the Beacon cloning and confirmation process calls 94 percent of exported cultures as positive that they were clonally derived,” the authors noted. “This is compared to 45 percent for a FACS and 17 percent for a limiting dilution process.”
“Additionally, Beacon clones that have been selected for export into 96-well microtiter plates have a higher recovery rate (56 percent) (positive + negative / attempts) compared to FACS (24 percent) and limiting dilution (33 percent) in the same plate format,” they added.
Whatever the method used, the ability to screen broader repertoires of cells earlier and more thoroughly, and failing or adjusting tempting candidates without expending as many resources, is sure to change the landscape of antibody development and immunotherapy more broadly from initial exploration to, perhaps, a patient’s bedside.
A MARATHON, NOT A SPRINT: Identifying and characterizing cells that produce antibodies against specific targets is still a long way from having something that will work as an immunotherapy, though. Given that an antibody for clinical treatment faces many different stresses and strains than one in its natural immune environment, other molecular facets must be explored to determine whether a given molecule can be developed into a therapeutic.
“Once you’ve done that for many targets and you have a throughput like ours—we can easily screen through a million cells in an afternoon—then the challenge is no longer can I find an antibody against my target, but rather how can I get the most information content in that screen."
- Carl Hansen of AbCellera
DDN Best of Immuno-Oncology
10Drug Discovery News
Going wide to go deep
To explore the greatest possible repertoire of antibody candidates or to find leads against heretofore intractable targets, there is growing interest in looking beyond the
usual sources.“The lion’s share of discovery is still done from rodents,” says Ab-
Cellera CEO Carl Hansen. “Of course, there are wildtype rodents, but there are now methods for taking antibodies from a rodent and then humanizing them into an antibody that looks like a human antibody.”
Looking to reduce this process even further, companies like Trianni have developed transgenic mouse lines that produce fully human antibodies directly.
For some targets or functional epitopes, however, evolutionary con-servation between humans and mice can make it difficult to mount an immune response, explained Torben Gjetting and colleagues at Symphogen (now part of Servier) in 2019.
“One solution to overcome this limitation is to use divergent animal species that are evolutionarily more distant to mammals,” the authors wrote, introducing the chicken as one such species.
“Chickens may not only be able to raise antibodies against very conserved targets, but also against novel human functional epitopes that are masked in mice due to sequence conservation,” they conti-nued. “Furthermore, antibodies against human targets generated in chicken are often cross-reactive to the mouse orthologous target.”
To test their thinking, the researchers generated a large antibody repertoire against the immune checkpoint protein PD1 in chickens. They then humanized the antibodies and compared the best candida-tes for PD1 binding affinity and functional activity to the commercial anti-PD1 immunotherapies pembrolizumab and nivolumab.
“The epitope of Sym021 was particularly interesting since it allowed for exceptionally strong cross-reactivity to both human, cy-nomolgus monkey, and mouse PD1,” the authors noted. “Moreover, Sym021 shows potent PD-L1 and PD-L2 blocking activity in reporter cell assays and was at least as efficient as nivolumab and pemb-rolizumab reference antibodies in enhancing T cell responses and cytokine production in vitro.”
The researchers also tested Sym021 for its ability to activate T cells in vivo and its impact on tumor growth in four mouse models.
“Sym021 treatment was found to induce significant tumor growth inhibition in several syngeneic tumor models and even complete tumor eradication in the Sa1N mouse fibrosarcoma model,” they reported.
Given these results, Sym021 was further subjected to toxicology testing in cynomolgus monkeys and is currently in a Phase 1 clinical
trial as a monotherapy or in combination with anti-LAG-3 or anti--TIM-3 leads vs. solid tumor malignancies or lymphomas.
To the authors’ knowledge, this was the first in-human study of a chicken-derived therapeutic antibody.
Alternatively, you may switch species to explore antibodies structurally distinct from those in humans, such as camelids.
“They have antibodies that have a single heavy chain, and that allows you to have a single polypeptide that can be generated within the animal’s immune system, which specifically recognizes the target and makes it very amenable to protein engineering,” Hansen explains.
“One of the big advantages of camelid antibodies is that they are modular and can be combined with simple linkers and protein engineering methods to make a variety of different molecular constructs that would otherwise be very challenging to produce and to manufacture,” he adds.
But even without changing species, the full antibody reper-toire is spread across the multiple immune compartments—e.g., spleen, lymph nodes and bone marrow—which cannot be equal-ly accessed by all methods.
For example, B cells from bone marrow have not been histori-cally amenable to fusion with myeloma cells to form hybridomas, explains John Proctor, senior vice president of marketing at Berkeley Lights.
“They seem to be overly sensitive to the process and don’t survive,” he continues. “So, hybridoma for a long time has been limited to just splenocytes.”
Likewise, immunization and epitope localization can differ across the immune compartments and thereby produce a differ-ent immune response.
“Even just immunizing the same target over and over, you’ll see different immune responses,” Proctor adds. “By accessing all compartments, we’re able to scan that diversity every time to do the screen.”
Given the increasing complexity and demands of newer im-munotherapy approaches, starting with the broadest array of op-tions can only help to increase the chances of success.
DDN Best of Immuno-Oncology
11Drug Discovery News
THE GROWING POTENTIAL OF CAR T-CELL THERAPYBY ANDREA TOELL OF LONZA BIOSCIENCES
IntroductionThe rising global incidence of cancer1 highlights the importance of developing more effective therapeutic strategies. Amid a wealth of innovative anticancer research, new therapeutic tools continue to emerge in the field of immuno-oncology. However, these approaches, which are focused on boosting the ability of a patient’s immune system to target and eliminate cancer cells, are not without risk, and many immunotherapies can trigger poten-tially harmful side effects. Given the need for greater treatment efficacy, safety and specificity, innovative immunotherapeutic strategies that more closely target cancers and minimize the risk of adverse responses are being developed using genetic engineering approaches that modify the patient’s own immune cells.
T lymphocytes (T cells) play a key role in cell-mediated immune responses to cancer, making them prime candidates for ex-vivo genetic modification. One such modification is the transfer of chi-meric antigen receptor (CAR) transgene cassettes into a patient’s primary T cells. This produces CAR T cells that express CARs specific to the tumor of interest. Following characterization and expansion, these cells are re-infused into the patient. The ability of CAR T cells to effectively treat hematopoietic malignancies such as lymphoblastic leukemia2 has fueled interest in advancing this technology. Further progress in gene transfer strategies is improving the safety and efficacy of CAR T cells in the treatment of blood cancers, and a major question now is whether CAR T-cell therapy can be applied to solid tumors. This will require novel strategies to address the considerable challenges involved in both avoiding autoimmune side-effects and overcoming the hostile tumor microenvironment.
CAR T cells and their success against B cell malignanciesCancer immunotherapy relies on reinforcing the body’s natural immune response to tumor-associated antigens (TAA). T cell par-ticipation in cell-mediated immune responses to cancer begins when T cells encounter B cells or dendritic cells that have digest-ed TAAs and display antigen peptide fragments that are bound to major histocompatibility complex (MHC) molecules (anti-gen-MHC). T cell receptors (TCRs) recognize and bind with the antigen-MHC complex, stimulating T cell maturation to produce T cells that either regulate the immune response or become cyto-toxic “killer” T cells capable of attacking cancerous cells directly. Major challenges to the effectiveness of this immune response include the ability of cancer cells to create an immunologically tolerant microenvironment and to employ a variety of immuno-suppressive mechanisms.3,4 Growing tumors are also known to down-regulate specific effector T cell responses and induce resis-tance to T cell killing.5
Early strategies for T cell modification involved engineering the TCR. However, down-regulation of antigen presentation to the TCR in the cancer limits their efficacy. CAR T cells have advantages here, as CARs are highly specific targeting molecules that combine the binding properties of a monoclonal antibody with signaling through the TCR complex. When expressed by T cells, CARs target TAAs in their native conformation, independent of the MHC complex. This allows them to bypass human leucocyte antigen (HLA) recognition and thereby avoid some of the key mechanisms that facilitate tumor escape from TCR-mediated immunity.
CAR T cells are currently the subject of more than 100 clinical trials,6 with B-lineage antigens such as CD19 the most investi-gated to date. Two therapies are FDA approved: one is for the treatment of diffuse large B cell lymphoma, and the second is for
FROM 2019 COMMENTARY
12Drug Discovery News
DDN Best of Neuroscience
certain types of adult non-Hodgkin lymphoma.7 The application of CAR technology in cancer therapy is currently the focus of intense study. However, the safety and efficacy of the resulting treatments largely depends on the methods used to generate the CAR T cells and, as such, understanding how to engineer them is critically important.
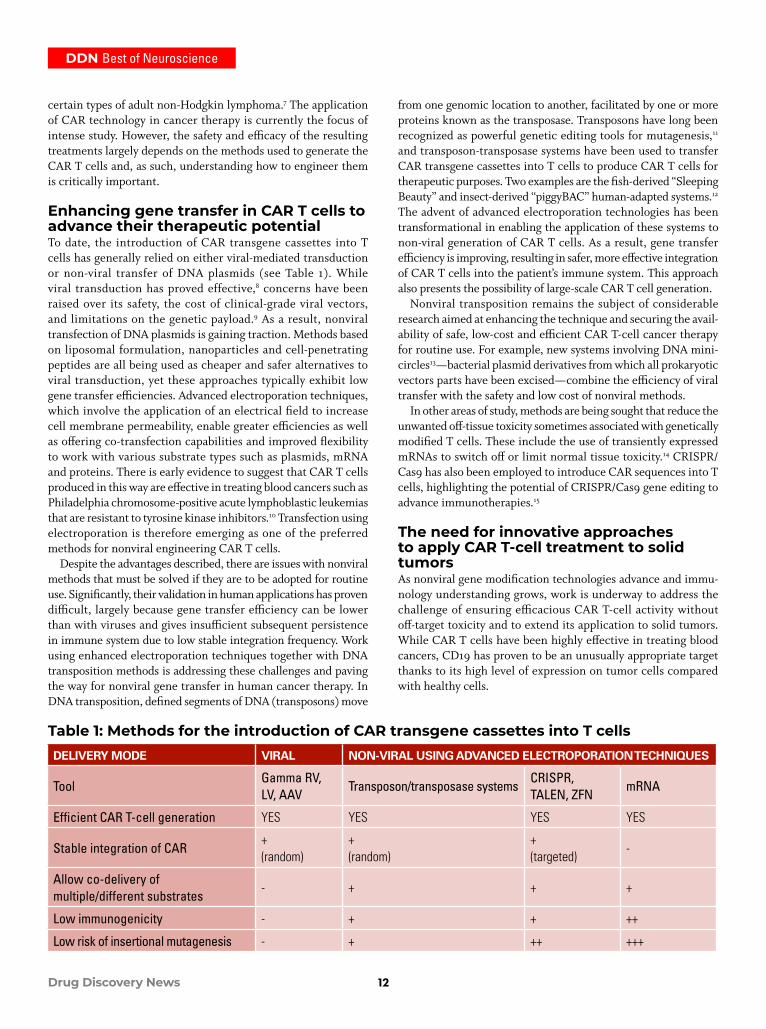
Enhancing gene transfer in CAR T cells to advance their therapeutic potentialTo date, the introduction of CAR transgene cassettes into T cells has generally relied on either viral-mediated transduction or non-viral transfer of DNA plasmids (see Table 1). While viral transduction has proved effective,8 concerns have been raised over its safety, the cost of clinical-grade viral vectors, and limitations on the genetic payload.9 As a result, nonviral transfection of DNA plasmids is gaining traction. Methods based on liposomal formulation, nanoparticles and cell-penetrating peptides are all being used as cheaper and safer alternatives to viral transduction, yet these approaches typically exhibit low gene transfer efficiencies. Advanced electroporation techniques, which involve the application of an electrical field to increase cell membrane permeability, enable greater efficiencies as well as offering co-transfection capabilities and improved flexibility to work with various substrate types such as plasmids, mRNA and proteins. There is early evidence to suggest that CAR T cells produced in this way are effective in treating blood cancers such as Philadelphia chromosome-positive acute lymphoblastic leukemias that are resistant to tyrosine kinase inhibitors.10 Transfection using electroporation is therefore emerging as one of the preferred methods for nonviral engineering CAR T cells.
Despite the advantages described, there are issues with nonviral methods that must be solved if they are to be adopted for routine use. Significantly, their validation in human applications has proven difficult, largely because gene transfer efficiency can be lower than with viruses and gives insufficient subsequent persistence in immune system due to low stable integration frequency. Work using enhanced electroporation techniques together with DNA transposition methods is addressing these challenges and paving the way for nonviral gene transfer in human cancer therapy. In DNA transposition, defined segments of DNA (transposons) move
from one genomic location to another, facilitated by one or more proteins known as the transposase. Transposons have long been recognized as powerful genetic editing tools for mutagenesis,11 and transposon-transposase systems have been used to transfer CAR transgene cassettes into T cells to produce CAR T cells for therapeutic purposes. Two examples are the fish-derived “Sleeping Beauty” and insect-derived “piggyBAC” human-adapted systems.12 The advent of advanced electroporation technologies has been transformational in enabling the application of these systems to non-viral generation of CAR T cells. As a result, gene transfer efficiency is improving, resulting in safer, more effective integration of CAR T cells into the patient’s immune system. This approach also presents the possibility of large-scale CAR T cell generation.
Nonviral transposition remains the subject of considerable research aimed at enhancing the technique and securing the avail-ability of safe, low-cost and efficient CAR T-cell cancer therapy for routine use. For example, new systems involving DNA mini-circles13—bacterial plasmid derivatives from which all prokaryotic vectors parts have been excised—combine the efficiency of viral transfer with the safety and low cost of nonviral methods.
In other areas of study, methods are being sought that reduce the unwanted off-tissue toxicity sometimes associated with genetically modified T cells. These include the use of transiently expressed mRNAs to switch off or limit normal tissue toxicity.14 CRISPR/Cas9 has also been employed to introduce CAR sequences into T cells, highlighting the potential of CRISPR/Cas9 gene editing to advance immunotherapies.15
The need for innovative approaches to apply CAR T-cell treatment to solid tumorsAs nonviral gene modification technologies advance and immu-nology understanding grows, work is underway to address the challenge of ensuring efficacious CAR T-cell activity without off-target toxicity and to extend its application to solid tumors. While CAR T cells have been highly effective in treating blood cancers, CD19 has proven to be an unusually appropriate target thanks to its high level of expression on tumor cells compared with healthy cells.
Table 1: Methods for the introduction of CAR transgene cassettes into T cellsDELIVERY MODE VIRAL NON-VIRAL USING ADVANCED ELECTROPORATION TECHNIQUES
ToolGamma RV, LV, AAV
Transposon/transposase systemsCRISPR, TALEN, ZFN
mRNA
Efficient CAR T-cell generation YES YES YES YES
Stable integration of CAR+ (random)
+ (random)
+ (targeted)
-
Allow co-delivery of multiple/different substrates
- + + +
Low immunogenicity - + + ++
Low risk of insertional mutagenesis - + ++ +++

DDN Best of Immuno-Oncology
13Drug Discovery News
In contrast with its use against hematopoietic malignancies, applying CAR T-cell treatments to fight solid tumors is more com-plex. Firstly, the potential for autoimmune side-effects is much greater, as there is often a lack of specifically targetable antigens.16 In solid tumors, antigens are generally not tumor-selective but are simply overexpressed. This is increasing the focus on those anti-gens that are preferentially expressed in certain types of cancer. Other strategies under investigation are aimed at increasing tar-geting specificity, including dual antigen recognition techniques.
Secondly, there are significant issues in overcoming the hos-tile microenvironment in solid tumors. Potential strategies to combat these challenges include “armored CAR” T cells, which are engineered to be resistant to immunosuppression, as well as combination therapy approaches such as those based on check-point inhibitors. Ongoing efforts to tackle these major challenges are beginning to yield novel and innovative CAR T-cell therapy treatments for solid tumors. One recent review17 has highlighted encouraging results in pediatric neuroblastoma, HER2-positive sarcoma and disseminated glioblastoma, and also noted that more than one-third of CAR T cell trials registered at the U.S. National Library of Medicine are investigating solid tumor indications.
ConclusionCAR T cells are currently the focus of considerable research and development efforts in the field of immuno-oncology, with some notable therapeutic successes in the treatment of blood cancers. Work to improve gene transfer technologies is helping to ensure robust and sustained CAR T-cell activity and increase the safety and efficacy of CAR T-cell treatments for B-cell malignancies.
Despite this success, however, widening the scope of CAR T-cell therapy to solid tumors presents a variety of more com-plex challenges that include identifying unique TAAs, avoiding autoimmune side-effects and overcoming the immunosuppressive tumor microenvironment. Consequently, researchers are no lon-ger simply searching for the next novel biomarker, but are looking to improve the underlying issues around treatment specificity and efficacy. The encouraging progress that has been made using innovative solutions suggests CAR T cells have the potential to usher in a new generation of effective cancer treatments.
References1. Cancer Research UK, 2014. Worldwide cancer incidence sta-
tistics. Available at: https://www.cancer.gov/news-events/cancer-currents-blog/2018/tisagenlecleucel-fda-lymphoma
2. Dai H, Wang Y, Lu X, Han W. Chimeric Antigen Receptors Modified T Cells for Cancer Therapy. J Natl Cancer Inst. 2016; 108(7). DOI: 10.1093/jnci/djv439
3. Zou W. Immunosuppressive networks in the tumour envi-ronment and their therapeutic relevance. Nature Reviews Cancer. 2005; 5(4), 263–274.
4. Rabinovich GA, Gabrilovich D. Sotomayor EM. Immuno-suppressive Strategies that are Mediated by Tumor Cells. Annual Review of Immunology. 2007; 25(1), 267–296.
5. Wu AA, Drake V. Huang HS, Chiu S, Zheng L. Repro-gramming the tumor microenvironment: tumor-induced
immunosuppressive factors paralyze T cells. Oncoimmu-nology. 2015; 4(7), e1016700.
6. Hay KA, Turtle CJ. Chimeric Antigen Receptor (CAR) T Cells: Lessons Learned from Targeting of CD19 in B-Cell Malignancies. Drugs. 2017; 77(3), 237–245.
7. National Cancer Institute. FDA Approves Second CAR T Cell Therapy for Lymphoma. Cancer Currents Blog. Pub-lished May 2018 updated 1 Dec 2018. Available at: https://www.cancer.gov/news-events/cancer-currents-blog/2018/tisagenlecleucel-fda-lymphoma
8. Melero I, Gaudernack G, Gerritsen W, Huber C, Parmiani G, Scholl S, Thatcher N, Wagstaff J, Zielinski C, Faulk-ner I, Mellstedt H. Therapeutic vaccines for cancer: an overview of clinical trials. Nat Rev Clin Onc. 2014; 11(9), 509–524.
9. Dotti G, Gottschalk S, Savoldo B, Brenner MK. Design and Development of Therapies using Chimeric Antigen Receptor-Expressing T cells. Immunol Rev. 2014; 257(1), DOI: 10.1111/imr.12131
10. Saito S, Nakazawa Y, Sueki A, Matsuda K, Tanaka M, Yan-agisawa R, Maeda Y, Sato Y, Okabe S, Inukai T, Sugita K, Wilson MH, Rooney CM, Koike K. Anti-leukemic potency of piggyBac-mediated CD19-specific T cells against refrac-tory Philadelphia chromosome–positive acute lympho-blastic leukemia. Cytotherapy. 2014; 16(9), 1257–1269.
11. Ivics Z, Hackett PB, Plasterk RH, Izsvák Z. Molecular Reconstruction of Sleeping Beauty, a Tc1-like Transposon from Fish, and Its Transposition in Human Cells. Cell. 1997; 91(4), 501–510.
12. Singh H, Moyes JS, Huls MH, Cooper LJ. Manufacture of T cells using the Sleeping Beauty system to enforce expression of a CD19-specific chimeric antigen receptor. Cancer Gene Therapy. 2015; 22(2), 95–100.
13. Monjezi, R. et al., 2017. Enhanced CAR T-cell engineering using non-viral Sleeping Beauty transposition from mini-circle vectors. Leukemia, 31(1), pp.186–194. http://www.nature.com/leu/journal/v31/n1/full/leu2016180a.html
14. Caruso HG, Torikai H, Zhang L, Maiti S, Dai J, Do KA, Singh H, Huls H, Lee DA, Champlin RE, Heimberger AB, Cooper LJ. Redirecting T Cell Specificity to EGFR Using mRNA to Self-limit Expression of Chimeric Anti-gen Receptor. Journal of Immunotherapy. 2016; 39(5), 205–217.
15. Su S, Hu B, Shao J, Shen B, Du J, Du Y, Zhou J, Yu L, Zhang L, Chen F, Sha H, Cheng L, Meng F, Zou Z, Huang X, Liu, B.Su, CRISPR-Cas9 mediated efficient PD-1 disruption on human primary T cells from cancer patients. Nature Scientific Reports. 2016; 6, 20070.
16. D’Aloia MM, Zizzari IG, Sacchetti B, Pierelli L, Aliman-di M. CAR-T cells: the long and winding road to solid tumors. Cell Death & Disease. 2018; 9, 282.
17. Schmidts A, Maus MV. Making CAR T Cells a Solid Option for Solid Tumors. Frontiers in Immunology. 2018; DOI: 10.3389/fimmu.2018.02593
DDN Best of Immuno-Oncology
14Drug Discovery News
PERSONALIZED CANCER THERAPY DIRECTED BY IMMUNE-PROFILINGBY STEPHEN M. ANDERTON OF CONCEPT LIFE SCIENCES AND MICHAEL MILLAR OF AQUILA BIOMEDICAL
The successful use of monoclonal antibodies that target CTLA-4-expressing cells, or that interrupt PD-1 signaling, has heralded a new era of cancer immunotherapy. However,
not all types of cancer are sensitive to these approaches and, in those that are, too many patients do not respond. To broaden efficacy, the hunt is on for additional immune pathways that can be manipulated to improve response rates, particularly when used in combination with PD-1-blockade. Earlier this year, the reported failure of the IDO-inhibitor Epacadostat to enhance the response rate to anti-PD-1 treatment brought disappointment, highlighting the continuing inability to predict the clinical fortunes of what seem scientifically sound approaches.
How can this be improved? A widely held view is that we need to better understand a patient’s immune landscape, and particularly the immune landscape within their tumor(s). There are currently three main approaches to characterizing the immune landscape of solid tumors: transcriptional profiling, single-cell cytometric analyses and histology.
Transcriptional profilingTranscriptional profiling allows collection of the broadest datasets. These can come from the use of commercially supplied packages, including “immunology,” “oncology” or “immune-oncology” panels, or from unbiased RNA-sequencing. Single-cell next-generation sequencing (NGS) currently provides the deepest insight into gene expression and is particularly powerful for discovery science.
However, whilst there will undoubtedly be interesting targets that are missed using defined panels, the ease and speed of data analysis (over the relatively cumbersome bioinformatics required for NGS) mean the more targeted analyses are likely to have great-est utility for day-to-day immune profiling. Recent advances have
combined RNA and protein analyses from the same sample, such as NanoString’s nCounter system, which comes with the advan-tage of being able to handle FFPE-preserved material.
Whilst transcriptional analyses can provide breadth of information, in general this does not include information on levels of expression of particular genes in defined cell populations. Taking molecular profiling in the setting of PD-1 blockade as an exemplar, the ligand PDL-1 can be expressed by tumor cells, by infiltrating innate immune cells, or by PD-1+ T cells themselves. FACS sorting [fluorescence-activated cell sorting] to provide individual populations for downstream transcriptional analyses is feasible, but requires some a priori decisions regarding the cells of interest, as the number of cell populations that can be sorted from a single sample is limited. It also only tells us about expression at the population level, rather than at the individual cell level.
Single-cell NGS can bring the necessary resolution but, as discussed above, is unlikely to be widely used as a routine. Recently launched platforms seek to balance breadth of gene expression with single-cell detail and also functionality. For example, BD’s Rhapsody system uses microwells to capture RNA from individual cells on uniquely barcoded beads, prior to pooling, multiplex PCR and sequencing. Available gene panels provide coverage of hundreds of genes from thousands of sampled cells.
Cytometry in multiple dimensions: From light to mass to four-letter codingFlow cytometry has been the workhorse technique of cellular immunology for decades, and fluorescently labeled antibodies remain the most widely used platform. The range of cell populations identifiable in a sample has been limited by the numbers of colors available. Although the most advanced cytometers can now confidently handle around 20 colors, newer
FROM 2019 COMMENTARY

DDN Best of Immuno-Oncology
15Drug Discovery News
technologies are pushing the boundaries further. Utilizing metal-conjugated antibodies, CyTOF combines flow cytometry with time-of-flight mass spectrometry to deliver powerful data-sets on the expression of dozens of molecules. But even CyTOF has so far remained in the double-digit range and will be restricted by the numbers of metals available for conjugation. It is also relatively slow (around 1,000 cells per second, less than 1/10th the pace of traditional FACS) and it is considerably more expensive.
The consensus is that DNA barcoding offers a solution to really scale up molecular profiling. Antibodies are tagged with unique DNA sequences, labeled cells are lysed and the barcodes read on a DNA sequencer. This approach has the potential to be nuanced to include transcriptional analysis of the same sample. Although some other current technologies combine protein and mRNA profiling on the same sample (e.g. NanoString), these only provide data at the sample level rather than the single-cell level, so a technology that can offer this would be a step forward.
Next-generation histologyWhilst utilization of the methods described above can provide information on which cells are expressing what molecule, they cannot tell us where those cells are. Sticking with the example of PD-1 blockade, how valuable is it to know which cells are expressing PDL-1, if we do not know how close they are to T cells (that are or are not) expressing PD-1?
Histological examination has always been central to understanding tumor heterogeneity, and advances in multiplex staining, whole-slide scanning and image analysis permit extraction of qualitative or quantitative information with 2D integrity maintained. Tissue microarrays allow high-throughput screening, and slide scanning allows the morphological, pathological, spatial distribution and temporal changes resulting from treatment to be visualized across large areas of tissue.
Advances in multiplex detection technologies allow simul-taneous detection of multiple immune biomarkers in a similar manner to flow cytometry, but with the added value that spatial visualization brings. There are currently two main approaches for high-plex staining. The SIMPLE method uses direct (no signal amplification) or indirect (low/moderate signal amplification) staining of individual targets. Once imaged, the sections undergo a combination of chromogen bleaching or fluorescence quenching and antibody stripping.
This process repeats iteratively until the required number of images is acquired, before merging the datasets into a rendered multiplex image. Alternatively, the highly-sensitive Tyramide-based detection methods employ a sequential approach for target detection, signal amplification and antibody stripping. Currently there can be six cycles of staining before imaging using a spectral imaging platform, but this should soon increase to nine. Tyramide detections currently deliver 7-plex staining, and can be combined with RNAScope for mRNA detection.
Both of the approaches outlined above have advantages and disadvantages, and both share the complexities of target validation and staining sequence. However, robotic staining systems and whole-slide scanners favor Tyramide-based approaches within
a consistent high-throughput environment, as opposed to the SIMPLE method which is more interventionist and laborious. Ultra-high-plex approaches of the future may again call on DNA barcoding to raise the technical bar. The reagents and technologies supporting this field are evolving rapidly, and will require a new generation of skilled histotechnologists to deliver.
Which approach to choose?Each of the approaches discussed here brings benefits and has limitations: NGS brings the greatest depth, but at a population level; single-cell analyses by can bring detail on relative expression of proteins or mRNA, but with reduced depth and a lack spatial information; histology brings that information, but here “multi-plexing” currently means the number of markers available in a fairly standard flow cytometry run. As ever, choice is dictated by the questions that need to be answered. Personalized medicine is delivered by asking, “What is the best (available) treatment for this patient?” For cancer immunotherapy, it is obvious that an understanding of the extent and quality of the immune infiltrate in a tumor will help to guide the clinician and patient. For simplicity, tumors have been divided into three categories determined by the presence and location of T cells—notably, “immune deserts,” “immune-excluded” or “inflamed.” Logically, and in broad terms, this order reflects sensitivity to current immunotherapies.
Spatial information from histology can have prognostic value. Using numbers and location of CD3+ and CD8+ T cells, HalioDx’s Immunoscore Colon test on resected tumors has shown value in predicting relapse risk for stage I-III colon cancer. This has not been extended to predictions of response to immunotherapy. Two immunohistochemistry tests for PDL-1 expression have been FDA-approved to accompany Keytruda (anti-PD-1) and Tecentriq (anti-PDL-1), and the search for other companion diagnostic tests will remain intense, particularly for the alternative immunother-apies currently in clinical trials.
Depending on the target pathways, these might well be better characterized by transcriptional or cytometric analyses than by histology. There are now some commercial providers offering CyTOF for broader characterization of immune cell populations in tumors, for example.
It is important to remember that we are dealing with an immune response. As such, ex-vivo characterization can only tell us so much and a great deal more can be learned by functionally testing that response; for example, a T cell’s response to T cell receptor activation, or an innate immune cell’s response to toll-like receptor activation (with or without addition of drug). Functional readouts might then be cytometric or biochemical characterization, changes in transcription, multiplexed analysis of secreted products or, of course, cytotoxic activity against tumor targets.
It is likely that the high-end, complex and expensive approaches discussed here will be best deployed to provide preclinical datasets. The true benefit will come from distilling the salient information from these to enable development of directed, validated and robust tests. This is in the distance, but a lack of technology will not be the obstacle.
DDN Best of Immuno-Oncology
16Drug Discovery News
MAKING SENSE OF IMMUNO-ONCOLOGYA news roundup showcasing notable cancer immunotherapy researchBY JEFFREY BOULEY, DDN CHIEF EDITOR
We’ve covered a lot of stories over the years in DDN magazine related to immuno-oncology, particularly in the past several years. But, of course, much of
that news has been of collaboration deals, specific companies’ proprietary discovery efforts, clinical trial results and the like. But we also have more “evergreen” news that is, if not timeless, at least more likely to be broadly interesting to you and useful to your knowledge long-term.
In that vein, here are six immuno-oncology news stories pulled from the pages of the magazine between 2018 and 2020.
Is CD40 the key to three-drug combos in immuno-oncology treatments?Emerging three-drug combinations are poised to redefine the immuno-oncology treatment paradigm in advanced malignancies with high unmet need, according to a 2020 report from data and analytics company GlobalData, which added that the oncology market is “saturated” with new drugs that target the immune system; “however, these only target part of the problem caused by cancer’s ability to hide from the immune system.”
Noted Miguel Ferreira, an oncology and hematology analyst at GlobalData: “To achieve the full potential of this strategy, new targets that independently trigger immune activation in addition to blocking cancer-mediated suppression of the immune system are needed.”
One of the current strategies using checkpoint inhibitors in certain cancer types involves treating with a PD-1 inhibitor, which blocks the ability of the cancer to silence necessary immune cells, and adding a second drug, such as an angiogenesis inhibitor, to help stabilize the response by disrupting the tumor microenvironment.
What is currently missing is a third component, a drug targeting a co-stimulatory T cell receptor which must directly and independently activate T cells to initiate an immune response.
“CD40 has been identified as the leading stimulatory receptor in T cells that would allow for a three-drug combination strategy by being the agent involved in directly activating the immune response,” said Ferreira. “As a single drug treatment, the dose required to get a sufficient effect might be too high and therefore too toxic, but when used in combination, a lower dose can contribute to the potential synergism between drugs targeting different aspects of the immune system against cancer.”
Removing cancer’s protective barrier could boost immunotherapy treatmentsScientists may have found a way to pull down the protective wall that surrounds tumors, potentially re-exposing them to the killing power of the immune system and immunotherapy treatments, according to a study partly funded by Cancer Research UK and published in EBioMedicine in 2019.
Although this was still from early research in the lab, the findings suggest this approach could help to boost the effects of innovative cancer treatments, such as CAR T therapy, which so far haven’t been used successfully to tackle solid tumors.
Dr. Francis Mussai and Dr. Carmela De Santo, based at the University of Birmingham, studied immune cells, called myeloid-derived suppressor cells or MDSCs, taken from the blood of 200 adults and children newly diagnosed with cancer before they had started treatment.
These cells send out a barrage of chemical signals that shield tumor cells from the immune system and the effects of treatment, and prevent the activation of T cells that can kill tumors.
When MDSCs are present in higher numbers, the outlook for patients is worse as their cancer can become resistant to treatment and is more likely to spread to other parts of the body. Researchers showed that an antibody drug that is already available for leukemia
FROM 2018-2020

DDN Best of Immuno-Oncology
17Drug Discovery News
was able to destroy these immune cells, which protect the solid tumor from the immune system.
“Treatments that work with the immune system to kill cancer often fail because it can be difficult for our body’s defences to get access to the tumor cells,” said Mussai, lead author of the study and Cancer Research UK Clinical Scientist Fellow at the University of Birmingham. “Our research indicates that giving this antibody drug alongside immunotherapies could dramati-cally increase the number of patients benefitting from the latest innovations in treatment.”
Previously, researchers in another group had found a way to break the protective layer around tumors in mice by using antibod-ies that attach to the MDSC cell surface, marking it for destruction by the immune system. But translating this into clinical trials has been challenging because researchers have been unable to find a drug target that is present on human MDSCs.
In this latest study, the team used blood samples taken from patients and showed that a protein called CD33 is present on the surface of MDSCs across a wide range of cancers.
By using an antibody drug called gentuzumab ozogamicin that targets CD33, which is already used to treat acute myeloid leuke-mia, the researchers were able to kill the MDSCs in the samples and restore the ability of T cells to attack the tumor cells.
The researchers also showed that active MDSCs prevented CAR T cells from working; however, when they added the antibody drug, it boosted the activity of the CAR T cells.
“This is the first time we’ve been able to effectively target the immune cells that form a barrier around solid tumors,” noted Mus-sai. “If this approach works in patients it could improve treatments for many different types of cancer, in both adults and children. We envision our approach will have the most impact in CAR T therapy, which despite showing lots of promise in blood cancer, so far it’s had limited success in solid tumors.”
Added Dr. Emily Farthing, research information manager at Cancer Research UK: “Although this is early research, it’s increased our understanding of the way tumors interact with the immune
system, and has given us a tantalizing insight into how we could make immunotherapies work for more patients in the future. But we are still a long way off in getting this treatment to patients. The next step will be to learn more about the side effects of the antibody drug, and how it works in the body.”
A nanoparticle nudgeGiven cancer’s ability to constantly mutate to avoid immune cells or even engage such cells to protect tumors, harnessing or tweaking immune functions could hold the key to more effective treatments—to that end, the Fred Hutchinson Cancer Research Center in 2019 produced a potential new tool for such efforts. The study, “Genetic programming of macrophages to perform anti-tumor functions using targeted mRNA nanocarriers,” was published in Nature Communications.
Some approaches for “recalibrating” the immune system entail training T cells to recognize certain proteins or enzymes on the surface of tumor cells, replicating those T cells in the lab, and then reintroducing the trained cells into the body. The Fred Hutch discovery offers a more specialized method of reprogramming immune cells that they say avoids toxicities seen in similar approaches.
Their method uses nanotechnology, specifically using “minuscule, dissolving polymer particles [that] can ferry genetic instructions that temporarily rewire certain immune-suppressing cells into cancer fighters without causing body-wide toxicities,” according to a press release authored by Sabrina Richards of the Fred Hutch News Service.
The cells in question are macrophages, a type of white blood cell. Macrophages are generally grouped as either M1 or M2 macrophages. As explained in the Nature Communications study, “Just like in healthy tissues, where macrophages have a remarkable ability for responding to environmental cues, TAMs are educated by the tumor microenvironment they experience. This produces multiple phenotypes that have a broad range of functions. TAM phenotypes can be described along a linear scale, where M1 and M2 phenotypes represent the two extremes (comparable to the T
H1–T
H2 classification). M1 macrophages are recognized as
classically activated macrophages that can phagocytose pathogens. More importantly, these cells have anti-tumoral properties.”
“Unfortunately, other macrophages are polarized into the M2 phenotype,” the authors continue. “These decrease inflammation, encourage tissue repair, and provide pro-tumoral effects. In established progressive tumors in humans, TAMs usually express an M2-like phenotype, and thus promote tumor progression, metastasis, and resistance to chemotherapy. It is therefore of key interest in cancer research to create strategies that can reprogram TAMs from a pro-tumoral (M2-like) to an anti-tumor (M1-like) phenotype and thereby induce immune effects that can bring about tumor regression. However, as yet there are no methods that can enable physicians to rationally and selectively reprogram TAMs for therapeutic purposes.”
Previous efforts to do so, they note, have been “nonspecific and elicit systemic inflammation.”
Stephan and his team were looking to tackle this issue with a bioengineering twist. Their nanoparticles can be packed with
TRIPLE THREAT: “CD40 has been identified as the leading stimulatory receptor in T cells that would allow for a three-drug combination strategy [for cancer] by being the agent involved in directly activating the immune response,” noted Miguel Ferreira of GlobalData.

DDN Best of Immuno-Oncology
18Drug Discovery News
genetic instructions to control cell functions, and they dissolve once in the cell.
“The nanoparticles are designed to be nonimmunogenic and not activate the immune system by themselves. They’re not designed to release a drug,” Stephan explained. “We’re programming the immune system from within.”
In this study, Stephan and Dr. Fan Zhang, a postdoctoral fellow on Stephan’s team, focused on synthetic mRNA molecules—specifically, in vitro-transcribed mRNA—as the genetic instructions to be included. The mRNA nanoparticles contain instructions for the production of two macrophage-stimulating proteins, which, as noted in Richards’ piece, “allows them to reprogram macrophages without touching their DNA.” Also included were molecules to ensure the nanoparticles would reach and be “eaten” by macrophages.
The team tested the nanoparticles in mice with ovarian cancer, administering them once a week via abdominal catheter for nine weeks—and the results were promising. Forty percent of mice saw complete clearance of tumors in the nanoparticle group, and mice in this group also lived an average of 142 days, compared to an average of 60 days for the control group. Mice with the mRNA-laden nanoparticles presented with increased populations of inflammatory macrophages, and also saw more T cells penetrate their tumors. When tested in mice with glioblastoma and metastatic melanoma, three intravenous infusions a week for three weeks led to comparable increases in survival times as those seen in the mice with ovarian cancer.
Stephan explained that immature macrophages are being intercepted before they can be co-opted by the tumors, adding that “We are targeting these cells that the tumor wants to recruit and we make sure that they don’t turn into suppressor cells, but they turn into the exact opposite.”
“We show that we can affect a lot of different immune cells, and we haven’t seen any of the toxicities that could be associated with treatments that modulate the immune system throughout the body, such as checkpoint inhibitors,” he said.
While this has obviously yet to be translated into humans, the team did demonstrate that nanoparticles with mRNA that encode human proteins were also capable of reprogramming the macrophages.
The authors report that there could be potential for using this nanoparticle approach in combination with other treatments, saying “Although we will test IRF5/IKKβ NPs as a monotherapy first, our platform could ultimately reveal its full potential when used in synergy with existing immunotherapies, (e.g., T cell therapies, cancer vaccines, or checkpoint blockade inhibitors) by creating a therapeutic window for patients, thus stimulating a stronger overall immune response ... Considering the substantial role TAMs play in cancer proliferation, angiogenesis, invasion, and metastasis, we suspect that our platform could be used to its best advantage as a companion therapeutic for patients that are refractory to other treatments such as immune checkpoint inhibitors, cancer vaccines, T cell therapies, or antibody approaches.”
Two-pronged antibodies draw immune killers directly to cancer cellsIn the lab of biochemist and immunologist Dr. Christoph Rader, an associate professor at The Scripps Research Institute (TSRI), scientists in 2018 engineered a new type of anticancer antibody that is intended to enhance nature’s cancer-fighting strategies by attracting killer T cells directly to cancer cells covered with a distinctive protein.
Referred to as “T cell-engaging bi-specific antibodies,” these novel weapons in the fight against cancer were designed to attack malignant cells but leave healthy cells untouched—all thanks to their selective targeting system. That targeting system homes in on ROR1 specifically, a protein found on the surface of several types of cancer cells.
“Once the T cells are recruited and activated, they release cytotoxic molecules that penetrate the target cells and kill them,” Rader said. “Natural antibodies can’t do this. You have to engineer them in a bispecific fashion to do this.”
Granted, bispecific antibodies themselves aren’t a new area of research, but this particular antibody and potential therapeutic may be more versatile than most.
As Rader explained, ROR1 is an excellent target for a “smart” cancer-fighting system because it is seen only in mature cells that are malignant. Rader first discovered ROR1’s activity in leukemia a decade before while working at the National Cancer Institute.
“ROR1 is expressed during embryogenesis, and then it is tightly down-regulated after birth. It later reappears in both blood cancers and solid malignancies,” Rader said, adding that it has been found on malignant cells, including lung, breast, ovarian and blood-based cancers. “One of the most unique aspects of this bi-specific anti-body is that it can work in so many different cancer indications.”
Also on the more novel side of bispecific antibody R&D is the duration of activity for this particular antibody. Rader credits Dr. Junpeng Qi, first author of the study on their bispecific ROR1 work and a postdoctoral associate at TSRI, with engineering a group of bispecific antibodies that stay active in animal models for about five days—which he points out is a feat compared with current approaches. The one U.S.-approved bispecific antibody therapeutic for cancer right now—against B cell acute lymphoblastic leukemia—stays active for a couple of hours, Rader said.
“Junpeng used a component of natural antibodies for this bispecific antibody that gives it not only a larger size, but also the ability to be recycled and stay in the blood longer,” Rader explained. “They are not there eternally, though. You get rid of them eventually, which is important for avoiding systemic toxicity.”
The scientists’ work was described in the article “Potent and Selective Antitumor Activity of a T-Cell Engaging Bispecific Antibody Targeting a Membrane-Proximal Epitope of ROR1,” which appeared online for the journal Proceedings of the National Academy of Sciences.
Also worth noting is that Rader is particularly interested in applying his bispecific antibodies to HER2-negative breast cancer, a type of breast cancer with fewer treatment options than many other cancers. “If you look at ROR1 expression in breast cancer,

DDN Best of Immuno-Oncology
19Drug Discovery News
you see that the patients who are HER2-negative are often ROR1-positive,” he noted. “These breast cancer patients might benefit.”
Survivin research opens up new avenues for cancer immunotherapy2018 research from Roswell Park Comprehensive Cancer Center and MimiVax LLC showed that one of the most commonly occurring molecules in cancer cells may be an attractive target for a broad range of immunotherapy approaches, including CAR T therapy. The study, “Survivin Monoclonal Antibodies Detect Survivin Cell Surface Expression and Inhibit Tumor Growth in vivo,” was published in Clinical Cancer Research, a journal of the American Association for Cancer Research.
Survivin is a cell-survival protein highly expressed by many types of cancer, including many glioma, lung, pancreatic, breast and neuroendocrine tumors and some forms of multiple myeloma, lymphoma and leukemia. Emerging vaccine approaches developed at Roswell Park and targeting the survivin protein may be more effective than standard therapy alone for some patients with glioblastoma.
Previously, survivin was thought to be present only inside the cancer cell, where some types of immunotherapy could not reach it. This preclinical study is the first to report that survivin can be found on the surface of cancer cells, which means that certain forms of immunotherapy targeting the protein could be effective against cancer cells. This observation suggests that antibody-based treatment approaches, including survivin CAR T cell therapy, could be used to target both solid and liquid tumors—a finding that could help broaden the applications for CAR T therapies.
“We’ve shown through our clinical trials of SurVaxM immunotherapy that survivin-targeting vaccines will stimulate both T-lymphocyte and antibody responses against survivin,” said senior author Dr. Michael Ciesielski, an assistant professor in the Department of Neurosurgery at Roswell Park. “Through this latest study, we have now discovered that antibodies that target cell-surface survivin have distinct therapeutic potential.”
Immune-stimulating cells shrink breast tumorsA research team at BriaCell Therapeutics Corp., an immuno-oncology-focused biotechnology company with a proprietary targeted immunotherapy technology, in 2018 published a paper that shed light on the potentially unique mechanism of action of BriaCell’s lead product candidate, Bria-IMT, in the journal Frontiers in Immunology.
The paper, titled “SV-BR-1-GM, a Clinically Effective GM-CSF-Secreting Breast Cancer Cell Line, Expresses an Immune Signature and Directly Activates CD4+ T Lymphocytes,” focused on the mechanism of action of Bria-IMT, also referred to as SV-BR-1-GM, and may explain impressive early clinical data on tumor shrinkage observed in some patients with metastatic breast cancer.
As summarized in the peer-reviewed publication, a body of evidence suggests immune-stimulating actions of SV-BR-1-GM which the paper’s authors believe are unique to Bria-IMT compared with other similar approaches. Bria-IMT (SV-BR-1-GM), the company’s lead product candidate, is derived from a specific breast cancer cell line. It is genetically engineered to release granulocyte-macrophage colony-stimulating factor (GM-CSF), a substance that activates the immune system, and the compound is thought to help the body recognize and kill tumor cells by activating both T cells that directly attack tumor cells, and, potentially, B cells that produce antitumor antibodies.
Specifically, Bria-IMT contains several factors, including HLA Class II molecules, molecules which typically are involved in start-ing an immune response. These molecules directly activate CD4+ “helper” T cells, a key component of the immune system, which can produce a strong immune response against tumor cells result-ing in tumor size reduction—also known as clinical regression. Complete or even partial regressions are difficult to achieve in advanced breast cancer patients who have failed the standard of care. BriaCell has previously reported such responses in patients with metastatic breast cancer, not only in soft tissue and visceral areas but even in the brain, a difficult site to treat.
FATAL ATTRACTION: Work at The Scripps Research Institute resulted in a new type of anticancer antibody intended to enhance nature’s cancer-fighting strategies by attracting killer T cells directly to cancer cells covered with a distinctive protein.

DDN Best of Immuno-Oncology
20Drug Discovery News
IMMUNO-ONCOLOGY—GOLD RUSH OR A GOLDEN AGE?BY DR. ANDY KINLEY OF NOVELLA CLINICAL
The last few years saw the success of checkpoint inhibitor drugs like pembrolizumab and nivolumab in treating cancer and brought on a whole new meaning to the field
of immunotherapy. Modulating the immune system to kill tumor cells became a main focus of many drug sponsors and the term “immuno-oncology” became a new buzzword. Estimates show1 that currently hundreds of clinical trials involving immuno-oncology therapies are being carried out with the recruitment of over a hundred thousand patients.
As excitement builds in the field, concerns have also arisen about poorly designed trials, patient safety and inefficient use of research funds and patient volunteers. In this commentary, we take a deeper look at the status of the crowded immuno-oncology field and explain how drug sponsors (and the scientific world in general) can derive the best benefit from a multitude of clinical trials and the information so gathered.
IntroductionA feverish hype has surrounded the field of immuno-oncology (IO) over the past decade with the discovery and approval of several checkpoint inhibitors. Keytruda (pembrolizumab), perhaps the most notable checkpoint inhibitor, has been approved for the treatment of melanoma, lung cancer, head and neck cancer and several other cancer types.
The concept of cancer immunotherapy is not new, and the beginnings of the field can be traced back to findings made more than a century ago. However, incredible progress has been made recently, and with the success of drugs like Keytruda, which generated greater than $1 billion in sales in the third quarter of 2017 alone, the business case for industry focus on immuno-oncology therapeutics is clear.
Is IO experiencing a gold rush?Keytruda is one of six FDA-approved checkpoint inhibitors2 for the treatment of a wide variety of cancers. Due to their market and medical success, there has been great interest from both academia and pharmaceutical companies in these classes of drugs. This interest has translated into a populous drug development pipeline for cancer immunotherapeutics: 50 checkpoint inhibitors are being evaluated in 1,502 studies, 1,105 of which are in combination with other treatments.3 Thought leaders in the field, however, have criticized the massive number of trials, calling it a “gold rush”4 with pharmaceutical companies seeking to take advantage of the clinical and commercial success of these drugs.
Do these criticisms hold merit? Many claim that this rush has led to hastily planned trials that lack sufficient scientific rationale and/or preclinical investigation. These types of trials, as experts note, do not advance our scientific understanding of how these therapeutics work or cancer’s ability to develop resistance. The failed ECHO-301 study5 of IDO inhibitor epacadostat in combination with pembrolizumab in advanced melanoma is often highlighted as an example of rushing into a (Phase 3) clinical trial without robust early-phase and efficacy data.
One additional criticism of the excessive number of trials being run is that they are quickly exhausting oncology’s most precious and important resource—eligible patients.6 Many trials call for a very specific patient type—patients who have relapsed, are in a specific stage or have a specific biomarker—and enrolling them in trials that are essentially testing similar drugs could make it difficult for other trials studying more innovative and novel ther-apies to find enough subjects.
So, it may be worth asking the question: Since there are already six FDA-approved checkpoint inhibitors, five of which inhibit the
FROM 2018 COMMENTARY

DDN Best of Immuno-Oncology
21Drug Discovery News
same PD-1 signaling pathway, do patients really need additional treatment options that have a similar mechanism of action?
Not a gold rush, but a golden age?Answering this question, like studying cancer, is no easy task. Cancer is a complex disease capable of altering a patient’s immune system in a variety of ways. While researchers and clinicians have gained deep insights over the past century, there are still many unanswered questions. Preclinical research and tumor models can help to answer some of these questions; however, they may not be a good predictor of safety or efficacy in humans. Thus, performing well-designed clinical trials allows researchers to formulate a more unifying hypothesis for how different cancers, and the immunotherapies that treat them, work.
For this reason, other thought leaders in immuno-oncology have taken a view opposing those criticizing the “gold rush,” calling the current era a “golden age of oncology drug development.”7 Only 10 to 30 percent of patients respond to checkpoint inhibitors, and with the extraordinary cost of drugs like Keytruda, which is priced at $150,000 a year, it seems there is plenty of room for innovation to create more effective drugs, or combinations, that are cheaper for patients.
In addition, some of the critiques of the IO “gold rush” may not be 100-percent accurate. With the massive number of trials and the seemingly small number of eligible patients, it is easy to believe that patients are being enrolled in trials that will not necessarily provide additional information or simply repeat similar studies. However, about 60 percent of the 1,500 studies mentioned above are small, single-site trials. Many of these are dose-escalation or expansion studies, and while they can expand to include a large number of patients, typically enrollment is gated, based on preliminary safety and efficacy data. These exploratory trials usually involve only 15 to 20 patients in each treatment arm and will not expand to enroll more. Therefore, trial databases may artificially overestimate patient demand.
One additional argument for companies developing their own PD-L1 inhibitors is financial. PD-L1 inhibitors are the foundation for the treatment of many types of cancer. Their continuously growing success in a variety of indications and their use in combi-nation with other treatments means that any emerging company looking to break into the immunotherapy market will either need to partner with large pharmaceutical companies with approved PD-L1 therapies, or develop their own checkpoint inhibitor.
Beyond checkpoint inhibitors to novel therapiesThe crowded IO field can also lead to the development of innova-tive new approaches for the treatment of cancer. A few years ago, researchers proposed a framework called the Cancer-Immunity Cycle8 for thinking about the steps by which immune cells (spe-cifically T cells) are primed to attack cancer cells, infiltrate the tumor microenvironment,9 recognize which cells are cancerous and kill them. This framework has helped researchers identify new targets and pathways that could be exploited by novel cancer therapeutic strategies.
Many inventive companies have done just that, exploring second- and third-generation therapies. Some of these are a new wave of checkpoint inhibitors, either antibodies or small molecules, that “release the brakes” of the immune system by inhibiting molecules which prevent immune attacks against cancer cells (i.e., TIM-3, VISTA, LAG-3, IDO or KIR). Simultaneously, there is also active research into molecules that “step on the gas” by stimulating cellular targets (i.e. CD40, GITR, OX40, CD137 and ICOS) to kill cancer cells.
A gold standardWith the hype and activity in the immuno-oncology field increasing, there are sure to be additional successes and failures, adding fuel to the fire for each side of this argument. One thing that both sides can agree on is that clinicians and researchers want clinical trials to be run with solid, scientific rationales that have the greatest potential to benefit patients. As we’ve described above, there is certainly a “gold rush” in the field, but it may not be as bad for patients as some have pointed out. The activity in this area has helped, and will continue to help, answer critical research questions and push revolutionary cancer therapeutics to market.
References1. https://www.ft.com/
content/00092dde-578c-11e7-9fed-c19e2700005f2. https://www.cancer.org/treatment/treatments-and-side-
effects/treatment-types/immunotherapy/immune-check-point-inhibitors.html
3. https://www.cancerresearch.org/news/2017/cri-immuno-oncology-landscape-analysis-publication
4. https://www.thelancet.com/journals/lanonc/article/PIIS1470-2045(17)30521-1/fulltext
5. https://lifescivc.com/2018/04/life-after-echo-301-lessons-learned-about-modulating-ido-tdo-to-treat-cancer/
6. https://www.nytimes.com/2017/08/12/health/cancer-drug-trials-encounter-a-problem-too-few-patients.html
7. https://www.focr.org/news/science-too-much-good-thing8. https://www.cell.com/immunity/fulltext/
S1074-7613(13)00296-39. https://www.nature.com/articles/nature21349
The next generations of immuno-oncology therapies are already on the way to break through cancer's defenses.
DDN Best of Immuno-Oncology
22Drug Discovery News
THE IMPORTANCE OF CANCER NEOEPITOPE DISCOVERYBY DR. RENATE SEKUL OF PEPPERPRINT GMBH
Significant advances in cancer diagnosis and treatment have improved the outcomes in many types of cancer. Therapies targeting more selectively tumor-specific features such as
tumor-associated antigens are part of the clinical routine. However, efficient treatments for advanced and highly aggressive neoplastic diseases are still missing.
Novel immune-modulatory approaches focus on the tumor microenvironment and try to activate the patient’s immune response to cancer tissue. A major breakthrough in cancer immunotherapy has been achieved with the introduction of checkpoint inhibitors. Checkpoint inhibition blocks signaling of the T cell surface receptors cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) or programmed death 1 (PD1), thereby increasing the T cell response towards tumor cells and ideally causing tumor regression. Checkpoint inhibitors are already approved for such cancers as metastasized melanoma or non-small cell lung cancer; clinical studies in other malignancies are ongoing. Regardless of these achievements, though, only a part of the affected patient population responds to checkpoint inhibition—thus, reliable predictive biomarkers for patient stratification are urgently needed.
Other immune treatments aim to target more specifically selected tumor-specific antigens and neoantigens. A variety of therapeutic cancer vaccines based on peptides, proteins or RNA show promising results in clinical trials. Adoptive T cell transfer uses tumor-infiltrating lymphocytes from tumor tissues, which are then stimulated and amplified with tumor antigens ex vivo and transferred back to patients to induce an effective antitumor response. Both approaches require the precise knowledge of tumor antigens and the underlying immunogenic epitopes.
Tumor neoepitopesNeoantigens are tumor-specific antigens that originate from somatic mutations in cancer cells. In recent years, high-throughput gene sequencing of normal and cancer tissues revealed tens of thousands of somatic mutations in major cancer types. Each tumor type exhibits an individual mutation profile, with shared and unique mutations between cancer patients. Because neoantigens are absent in healthy tissues, they are considered ideal targets for novel immunotherapies.
Furthermore, the risk of autoimmune side effects will be sig-nificantly lower than addressing naïve tumor-associated anti-gens. Shared mutations can be addressed by more conventional approaches, such as treatment with monoclonal antibodies direct-ed against such neoantigens, while unique mutations can form the basis for individualized therapies.
Tumor neoantigens can elicit strong immune responses with detectable antibody levels in patient sera. However, not every mutation can stimulate an immune reaction. Computer-assisted epitope prediction tools can help to select relevant MHC class I and class II neoepitopes for further validation in biological assays.
Whereas MHC class I prediction software such as NetMHC works reasonably well, the accurate prediction of MHC class II epitopes is still a challenge. The experimental analysis of antibody signatures in patient sera and the determination of the corresponding neoepitopes can be a very valuable alternative. High-resolution antibody profiling towards the complete set of neoepitopes will provide information on relevant MHC class II epitopes, even without knowing the patient’s HLA status. Analyzing the antibody fingerprint response against neoepitopes can be performed in a rapid fashion, even against large numbers of epitope peptides, and can help to precisely distinguish between immunogenic and non-immunogenic mutations.
FROM 2018 COMMENTARY

DDN Best of Immuno-Oncology
23Drug Discovery News
Cancer neoepitope discovery on peptide arraysArray-based technologies are ideally suited for analyzing antibody signatures. Thousands to tens of thousands of antigens can be screened simultaneously in a single experiment, requiring only minute amounts of patient sera. Bound antibodies are typically detected by a standard immunoassay using appropriately labeled detection antibodies.
High-density peptide microarrays are the method of choice for the epitope mapping of neoantigen proteins or peptides in a high-throughput mode. Personalized neoepitope libraries with thousands of peptides can be generated in a fast and economic fashion by on-chip synthesis technology, giving the complete neo-epitope information within six weeks.
Combining high-throughput genomic sequencing technology with personalized peptide arrays for neoepitope discovery allows the straightforward discovery of immunogenic neoepitopes, patient by patient. Neoepitope targets can be identified within the shortest time frame, enabling the rapid translation of neoepi-tope information into high-precision cancer immunotherapies.
Immune responses to cancer neoepitopes will be a rich source of predictive biomarkers for patients, who will most likely benefit from current and future immunotherapies. Antibody responses to neoepitopes can guide immune modulatory therapies and indicate clinical responses to immune modulating therapies.
The described screening platform offers a high potential for the discovery of novel biomarkers for cancer diagnostic, disease monitoring and vaccine candidate selection.
Renate Sekul, Ph.D., received her doctorate in biochemistry in 1989 from the University of Cologne in Germany. Since then, she has worked in different pharmaceutical and biotech companies in the field of peptide and small-molecule drug discovery in various indication areas. She is an expert in preclinical drug discovery, and her research fields comprise peptide synthesis and characterization, protein biochemistry, biochemical assay development and profiling of drug candidates—as well as the development of array-based screening techniques. She has a great deal of expertise in array-based screening of pharmaceutical target proteins and antibodies using small-molecule and peptide microarrays. Sekul is co-inventor and owner of several patents for peptide and small-molecule drugs.