being obese and diabetic: can we help?
TRANSCRIPT
REVIEW ARTICLE
Being obese and diabetic: can we help? Denise Thomas SRD MPhil, Chief Dietitian,
St James’ Hospital, Locksway Road, Portsmouth PO4 8LD, UK
This article discusses the current prob- lems met when treating obesity, not only when it occurs independently of other conditions, but most obviously when it occurs with diabetes. This view is per- sonal and from a dietetic standpoint. There are many invasive forms of treating obesity which will not be discussed here; the focus of this discourse is the art of the dietitian in giving dietary information that hopefully will help those who are overweight, to lose weight.
The heavy burden of weight reduction The use of a reduced energy diet is still one of the most effective means of weight reduction’. However, as with most forms of weight-reducing treatment, it is in- effective in terms of a long-term result2. Various papers have illustrated that those who successfully lose weight will usually regain it3.
For those who have diabetes, the prob- lem of weight reduction is quite a heavy burden. Although there is debate about the risks between obesity and cardio- vascular disease, it is still true that, for obese diabetics, a reduction in weight will benefit their diabetic state. Estimates of the prevalence of obesity range from 10 to 50% or more of the adult population in Europe, depending on the criteria used to define it*.
The question is, therefore, why do people persist in gaining weight the way they do? In 1984 the NACNE report was published5 and the general population was subjected to an overwhelming amount of nutritional information. Today, various forms of diets are available, videos to help with exercise, and the slimming industry is worth approximately 814 billion annually; yet some people remain fat.
Dietitians have been viewed as pur- veyors of treatment for those who require weight loss, and much debate has been made about whether dietitians are effec- tive in helping people lose weight6.
An audit of those referred for weight reduction to the Dietetic Department in Portsmouth (Table I ) showed that only 37% attended all appointments offered to them and they attained an average weight loss of 2.9kg over three months. This audit has made us question our practice.
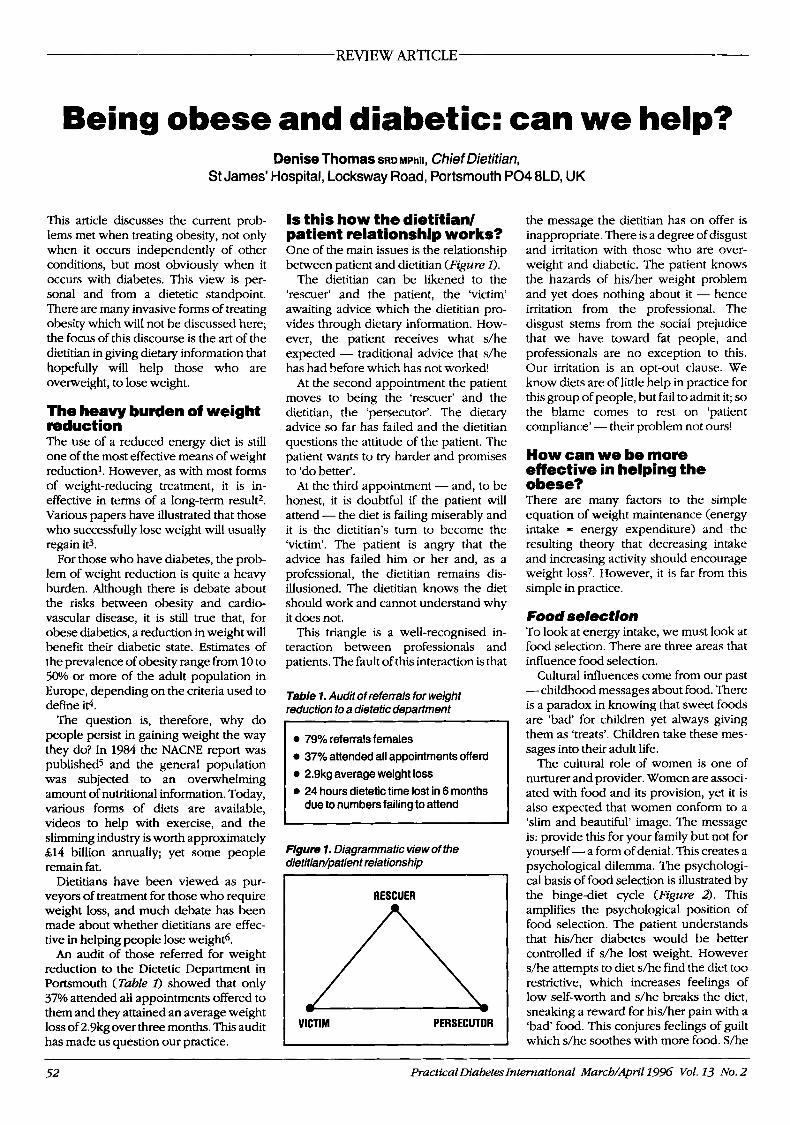
Is this how the dietitiad patient relationship works? One of the main issues is the relationship between patient and dietitian (Fgure I ) .
The dietitian can be likened to the ‘rescuer’ and the patient, the ‘victim’ awaiting advice which the dietitian pro- vides through dietary information. How- ever, the patient receives what s/he expected - traditional advice that s/he has had before which has not worked!
At the second appointment the patient moves to being the ‘rescuer’ and the dietitian, the ‘persecutor’. The dietary advice so far has failed and the dietitian questions the attitude of the patient. The patient wants to try harder and promises to ‘do better’.
At the third appointment - and, to be honest, it is doubtful if the patient will attend - the diet is failing miserably and it is the dietitian’s turn to become the ‘victim’. The patient is angry that the advice has failed him or her and, as a professional, the dietitian remains dis- illusioned. The dietitian knows the diet should work and cannot understand why it does not.
This triangle is a well-recognised in- teraction between professionals and patients. The fault of this interaction is that
Table 1. Audit ofreferrals for weight reduction to a dietetic department
0 79% referralsfemales 0 37% attended all appointments offerd 0 2.9kg average weight loss 0 24 hours dietetic time lost in 6 months
due to numbers failing to attend
Figure 1. Diagrammatic view of the dietitiadpatient relationship
I RESCUER I
I I VICTIM PERSECUTOR
the message the dietitian has on offer is inappropriate. There is a degree of disgust and irritation with those who are over- weight and diabetic. The patient knows the hazards of hidher weight problem and yet does nothing about it - hence irritation from the professional. The disgust stems from the social prejudice that we have toward fat people, and professionals are no exception to this. Our irritation is an opt-out clause. We know diets are of little help in practice for this group of people, but fail to admit it; so the blame comes to rest on ‘patient compliance’ - their problem not ours!
How can we be more effective in helping the obese? There are many factors to the simple equation of weight maintenance (energy intake = energy expenditure) and the resulting theory that decreasing intake and increasing activity should encourage weight loss7. However, it is far from this simple in practice.
Food selection To look at energy intake, we must look at food selection. There are three areas that influence food selection.
Cultural influences come from our past -childhood messages about food. There is a paradox in knowing that sweet foods are ‘bad for children yet always giving them as ‘treats’. Children take these mes- sages into their adult life.
The cultural role of women is one of nurturer and provider. Women are associ- ated with food and its provision, yet it is also expected that women conform to a ‘slim and beautiful’ image. The message is: provide this for your family but not for yourself - a form of denial. This creates a psychological dilemma. The psychologi- cal basis of food selection is illustrated by the binge-diet cycle (Figure 2). This amplifies the psychological position of food selection. The patient understands that his/her diabetes would be better controlled if s/he lost weight. However s/he attempts to diet s/he find the diet too restrictive, which increases feelings of low self-worth and s/he breaks the diet, sneaking a reward for his/her pain with a ‘bad’ food. This conjures feelings of guilt which s/he soothes with more food. S/he
52 PracticalDiabetes International March/April1996 Vol. 13 No. 2
REVIEW ARTICLE Being oheseand diabetic: can we help?
Figure 2. The binge-diet cycle
“I am overweight.” “I am diabetic.”
\ Failure.
Increased disappointment with self.
I I
Attempts to re-establish control.
h \
“I should lose weight.” “I would be happy and
healthy.“
i Attempt to diet.
/ Binge eats. /
Diet too restrictive. Breaks diet. - resolves to try again tomorrow, to do better than before, but it never reaches that - the diet is well and truly broken. S/he is in the spiral of increased dis- appointment and failure, increased con- solation with food.
The third influence on food selection is biological. This centres around the neuro- transmitter serotonin (5HT). Table 2 shows the times and types of women who have been shown to have a higher intake of snacks and desserts - all of these abnor- malities of feeding are linked to mood and the metabolism of serotonin. Serotonin produces satiety in the brain and its production is decreased when a person is on a diet. Therefore there is a disturbance in the ability to maintain satiety when a person is undereating. The brains of obese people are more susceptible to periods of carbohydrate craving, and females have a higher rate of synthesis of 5HT and are therefore more sensitive to changes of that neurotransmitter in the brains.
For women, the biological effect has a major effect on food selection. When
Table 2. Food selection. Times and types of women who have a higher intake ofsnacks and desserts
0 Luteal phase of menstrual cycle 0 Those with Pre-Menstrual Syndrome
0 Seasonal Affective Disorder 0 Obese carbohydrate cravers 0 Food binges in bulimia
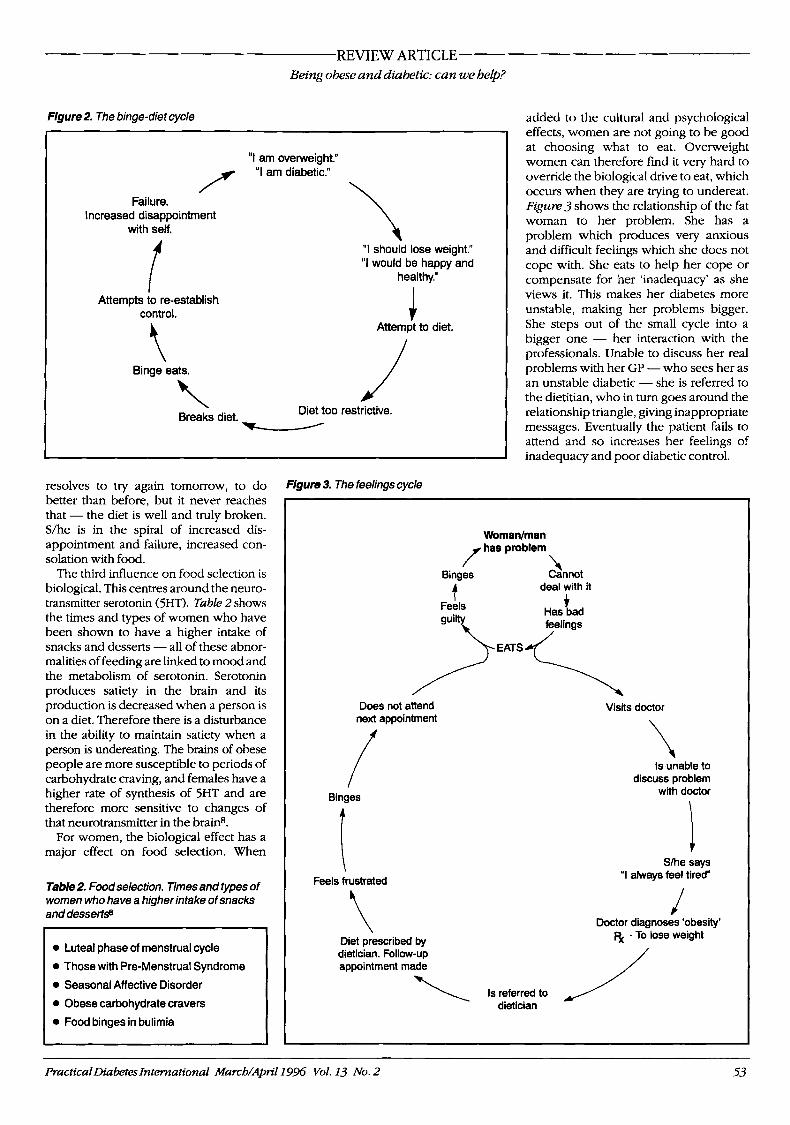
Figure 3. The feelings cycle
added to the cultural and psychological effects, women are not going to be good at choosing what to eat. Overweight women can therefore find it very hard to override the biological drive to eat, which occurs when they are trying to undereat. Figure 3 shows the relationship of the fat woman to her problem. She has a problem which produces very anxious and difficult feelings which she does not cope with. She eats to help her cope or compensate for her ‘inadequacy’ as she views it. This makes her diabetes more UnStdbk, making her problems bigger. She steps out of the small cycle into a bigger one - her interaction with the professionals. Unable to discuss her real problems with her GP -who sees her as an unstable diabetic - she is referred to the dietitian, who in turn goes around the relationship triangle, giving inappropriate messages. Eventually the patient fails to attend and so increases her feelings of inadequacy and poor diabetic control.
Woman/man
\ Binges Cannot deal with it A
Does not attend next appointment
Binges
I Feels frustrated
\ Diet prescribed by dietician. Follow-up appointment made
Visits doctor
Is unable to discuss problem
with doctor
Slhe says “I always feel tired“
J Doctor diagnoses ‘obesity’
5( - To lose weight
PracticalDiabetes International March/April 1936 Vol. 13 No. 2 53

REVIEW ARTICLE
Breaking the cycle Alter our own attitudes The first approach to changing this cycle is to alter the attitude of the professionals. We have to acknowledge that we are not immune to social prejudice toward fat people. Breaking down this psychologi- cal barrier is beneficial as it allows develop- ment of a therapeutic relationship and opts out of the relationship triangle.
In addition, we must acknowledge that diets may not have worked previously for the patient and therefore may have been of little benefit. This is illustrated by the patient’s history. By using this history you can show the metabolic effect of dieting, the possible link to emotional problems and the way s/he uses food.
Assess the patient properly The second phase of the new approach is a good assessment of each individual. Look at body size, shape and the extent of the problem. Examine their weight and dieting history. Figure 4 shows a classifi- cation that has not been evaluated but is a guideline for assessment.
Of note are the terms ‘static’ and ‘dynamic’ obesity (in categories 3 and 4). An obese person will eat 2-3 times more food than somebody who is lean. S/he will also eat food 2-3 times fasteP. People who have maintained a weight, even if that is overweight, for a period of time adopt ‘static obesity’. They start to have the same mannerisms as lean people. They eat more slowly and selectively choose less food. It is therefore important to en- courage static obesity in categories 3 and 4 to allow behdvioural work to take place.
Dynamic obesity is an inability to maintain a constant weight. This does not produce the thermic effect of food which is beneficial to energy need, and the person has difficulty experiencing and recognising hunger. In class 4 there is a place for some psychololgicdl work to look into the reason why the fat is there. An example of this is the woman who protects herself with her fat as a means of avoiding sexual advances and feelings of promiscuity.
Being obese and diabetic: can we help?
Figure 4. The four categories of fat people (6Mi=body mass index)
1. ‘The Dieter’ BMI = 25 Diets at least twice per year Help: .Knowledge about harm of yo-yo dieting
2.’The Welght Galner’ BMI =28-30 Diets cyclically Help: 0 Discuss why it has gone wrong 0 Set a realistic target 0 Aim for static obesity
3. ‘The Binge - Dieter’ BMI = 30+ In diet-binge cycle Help: 0 Knowledge that diets do not work 0 Triggers that perpetuate binge-eating 0 Realistic target 0 Static obesity - behavioural work
4. ‘The Classically Obese’ BMI = 35 and upwards Dynamic obesity Fear of dieting and hirn/herself Help: 0 Look at why weight is there 0 Help hidher to be fat in a thin world 0 Education and knowledge
Use behawioural programmes for weight reduction The third part of the new approach is a. recognition that diets do not always work. Therefore investigate patterns of eating - how, where and why people eat. Behavi- oural programmes for weight reduction have been shown to be one of the most effective in a follow-up studylo
He/p improve the patient’s self-esteem The fourth part of the new approach is the improvement of self-esteem. It is difficult to counteract the ‘slim is beautiful’ ethic; however, we must try to help the fat person take a valued place in society. As professionals we have to enable people to break through the social stereotype of ideal body size.
Fat women have an equal right in our society. Why is it that women are targeted more than men for weight reduction? Four out of five dietitic referrals for weight reduction are for women, yet this ratio does not apply when we look at statistics for overweight people in the UK. There is a need to dissolve social and sexual barriers that predetermine the ideal woman’s size.
Summary The treatment of obesity, whether in conjunction with diabetes or independent of it, lies in an examination of what the problem means to both patient and professional. A thorough assessment and an open approach by professionals are necessary to help improve the lifestyle as well as the medical state of obese diabetic people.
References 1. Garrow JS. Treatment of obesity. Lumel1992;
340: 403-13 2. Hughes JM, Stock w. Long-term (2 year) fol-
low-up of successful dimmers. IutJObesity1990; 14: 905
3. Bennett W. Dietary treatments of obesity. Ann WAcudScil987; 4 9 9 350-63
4. vonGaalL Body fat and fat distribution: eating patterns and endocrine factors. In: Eating patterns and weight control. International Monitor. Nether- lands: Medicor Europe, 1993 6-11
5. National Advisory Committee on Nutrition Education. Proposals for nutritional guidelines for health education in Britain. London Health Edu- cation Council, 1983
6 . PrenticeAM,BlackAE,MurgabmydPR,efaL Metabolism or appetite: questions of energy balance with particular reference to obesity. JHum NutrDiet 1989; 2: 95-104
7. Ravussin E, S w h b u r n BA. Pathophysiology of obesity. Lancet 1992; 340: 404-8
8. Wurtman w, WurtmanJJ. Dietary carbohy- drates, mood and obesity. In: Anderson GH and Ken- nedy SH, eds. Biology of feast and famine: relevance to eating disorders. London: Academic Press Inc, 1992: 151-6
9. Guy-Grand B. Stitt Y. Gustative alliesthesia: evidence supporting the ponderostatic hypothesis for obesity. In: Howard A, ed. Recent advances for obesity research. London: Newman, 1975: 238-42
10. Bjorvell H, Rossner S. Long-term treatment of Severe obesity: four year follow-up of results. Combined Behavioural Modification Programme. BMJ1985; 291: 37942
54 PracticaIDiabetes International March/April19% Vol. 13 No. 2