behavioral health services for injured or ill workers – collaborative care analysis and...
TRANSCRIPT
Behavioral Health Services for Injured or Ill workers – Collaborative Care Analysis and Recommendations
January 22, 2015
Collaborative Care Review Informal IIMAC meetings to review data and discuss
psychiatric care issues (July – October 2013)
IIMAC recommended Focus on Collaborative Care (January 2014).
Requested Review to– update L&I data on claims with psychiatric treatment– identify current Washington state implementation– summarize currently well done literature reviews
Use Review and IIMAC feedback as a base for executive recommendations and next steps
2
3
4
5
Local Collaborative Care Implementation
1. Identified Models currently implemented in WA state– Group Health – Medicaid’s Community Health Plan of Washington (CHPW)
2. Conducted Semi-Structured interviews
3. Defined Core Components/Key Elements
4. Identified Key Contacts
5. Obtained and Summarized Detailed information
Outcome: Documented and understand local implementation status, potential for collaboration or coordination and key informant assistance (learnings), if move forward. 6
Key Collaborative Care Components
Identified key elements from the Medicaid/Group Health comparison for further investigation via a review of collaborative care studies
Conditions treated (mild, moderate or severe) Screening protocols and validated instruments Role of the care coordinator Typical providers participating Best practices for communication
(e.g., systematic protocols, timing, tools, technology)
Reported outcomes(e.g., clinical improvement, process measures) 7
Key Studies Identified
Five key studies related to collaborative care models for behavioral health in primary care were identified: 3 systematic reviews including a Cochrane review, 1 randomized controlled trial and 1 prospective study.
Archer, et.al. 2012, Cochrane Review, Collaborative care for depression and anxiety problems. A meta-analysis/systematic review.Gilbody, et.al. 2006, Arch Intern Med, Collaborative care for depression, A cumulative meta-analysis and review of longer-term outcomes.Williams, Jr., et.al. 2007, General Hospital Psychiatry, Systematic review of multifacted interventions to improve depression care.Unutzer, et.al. 2002, JAMA, Collaborative Care Management of Late-Life Depression in the Primary Care Setting. A randomized controlled trial
Katon, et.al. 2002, J Gen Intern Med, Long-term effects of a collaborative care intervention in persistently depressed primary care patients. A prospective cohort study.
8
Strong and consistent evidence•For example, the Williams review included 28 studies with over 1,800 clinicians and 11,000 patients where the majority of studies had low risk of bias; randomized by either patient, providers or practices; outcomes were assessed blind to treatment assignment; an intent to treat assignment was used; and interventions were generally well defined and compared to usual care where the clinician or patient was educated about the assessment of depression.
More rapid and sustained improvement in both short and longer term:
• mental health outcomes• employment rates, • functioning, • quality of life
Example: Unutzer 2002 found that at 12 months follow up, 45% of the intervention (collaborative care) patients had a 50% or greater reduction in symptoms from baseline as compared to 19% of patients in the usual care group (OR 3.45, p<0.001).
9
Review includes excellent analysis to organize further considerations.
Example: Williams provided a useful framework that groups the intervention into four categories1.Delivery system redesign (care management and enhanced mental health access) – structured assessment and regular monitoring Decision support (PCP and patient education) – educational materials; treatment algorithms; and/or patient specific feedback2.Information systems –electronic systems to track and monitor patient assessment and progress3.Self-management – educational materials, and half of the studies built self-management support into care manager functions
10
Review includes excellent analysis to develop focus group questions regarding program design, measures, outcomes, leading to better outcomes for example:
Sample of correlation found 1.Structured (proactive) care management2.support of medication management by primary care providers3.Supervision (regular/planned) of care managers (usually by psychiatrist)4.Case managers with a mental health background5.Strong clinical champion 6.Resources to support infrastructure, training, and care manager
Sample of lack of correlation1.Number of sessions with a case manager2.Addition of specific types of psychotherapy to medication management, or where antidepressants were prescribed at start.
11
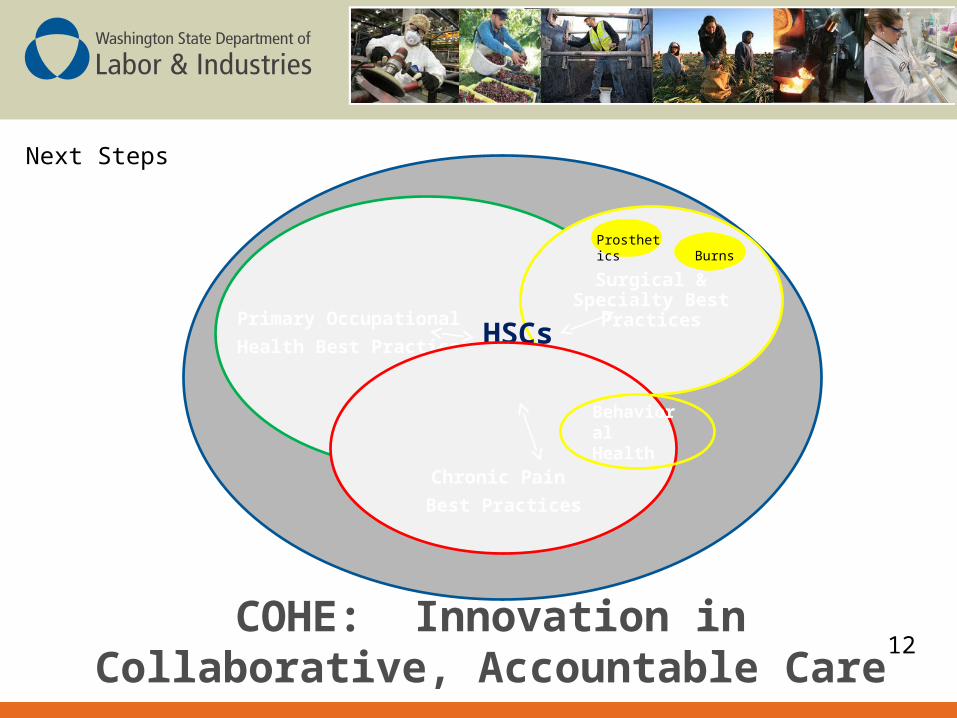
COHE: Innovation in Collaborative, Accountable Care
Primary Occupational
Health Best Practices
Surgical & Specialty Best Practices
HSCs OHMS
BurnsProsthetics
Chronic Pain
Best Practices
Behavioral Health
Next Steps
12