barr body distribution and estrogen receptor protein in ... · barr body and estrogen receptor...
TRANSCRIPT

ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 7, No. 6Copyright (g) 1977, Institute for Clinical Science
Barr Body Distribution and Estrogen Receptor Protein in Mammary Carcinoma*PAUL PETER ROSEN, M.D.,f ANGELA SAVINO, CT (ASCP),t
CELIA MENENDEZ-BOTET, Ph .D.,* JEROME A. URBAN, M.D.,§ VALERIE MIKE, Ph .D.," MORTON K. SCHWARTZ, Ph .D.,*
and MYRON R. MELAMED, M.D.f
Departments of Pathology (Cytology Service), t Biochemistry t and Surgery (Breast Service),§
Memorial Hospital, and
Biostatistics Laboratory," Memorial Sloan-Kettering Cancer Center,
New York, NY 10021
ABSTRACT
This study was undertaken to investigate the relationship between Barr body distribution and estrogen receptor protein content of mammary carcinoma. The proportion of cells with one or more Barr body was determined in 105 specimens of mammary carcinoma from Guard stained imprints. Receptor protein content of the specimen was measured by the dextran charcoal method and compared with histopathologic features of the carcinomas. Primary carcinomas with Barr bodies in more than 10 percent of tumor cells were more likely to have higher levels of receptor protein than those with a lower proportion of Barr body containing cells (P < 0.005). The results obtained for primary carcinoma may explain why patients with carcinomas that have a high proportion of Barr body positive cells are more likely to respond to hormonal therapy. Furthermore, these observations, when correlated with other available data about ERP suggest that an X-chromosome is involved in the synthesis of and/or carries the locus of action for estrogen receptor protein.
Introduction
Assays of the content of receptor protein for estrogen12 in mammary carcinoma have proven to be clinically useful indicators of the likelihood of response to hormonal therapy in patients with recurrent mammary carcinoma.
* Address reprint requests to Paul Peter Rosen, M.D., Department of Pathology, Memorial Hospital, 1275 York Avenue, New York, NY 10021.
Complexes formed through interaction of receptor and hormone in the cytoplasm of potentially responsive cells are translocated to the nucleus. By binding with desoxyribonucleic acid (DNA) acceptor sites, the complexes influence the formation of specific ribonucleic acid (RNA) and ultimately protein synthesis.13,23 Non-histone protein components of chromatin are apparently important determinants of the specificity of binding sites,22 but there is
491

492 ROSEN, ET AL.
as yet no evidence as to which chromosome bears this locus of action or the locus for the synthesis of receptor protein.
It has been noted that patients whose tumors had a greater proportion of cells in which a distinct Barr body could be identified had a more favorable prog
nosis.7,24'29'34 Recurrent carcinomas with a higher proportion of Barr body positive cells were found to be more likely to regress in response to therapy.5,17'24'31 Women whose breast carcinoma contained a high proportion of Barr body positive cells derived some benefit from prophylactic oophorectomy, whereas those with Barr body negative tumors did not benefit.33
This study was undertaken to evaluate the relationship between the estrogen re
ceptor content and the proportion of Barr body positive cells in mammary car
cinoma.
Materials and Methods
One hundred and five specimens of primary or recurrent mammary carcinoma submitted for frozen section and for estrogen receptor protein (ERP)
f h%
9 %<#
F ig u r e 1. Photograph of mammary carcinoma cell in imprint preparation stained with Guard’s stain. Barr body is indicated by arrow (original magnification x570).
analysis were obtained from the Pathology Laboratory. Barr bodies (figure 1) were identified in Guard stained direct
imprints made from the tissue selected for ERP analysis. The procedure for
staining and counting cells was identical with that described in a prior report.29 A
minimum of 100 carcinoma cells from each tumor was studied. The number of cells with a Barr body was expressed as a
percentage of the total number. Cells with more than one Barr body were infrequent. When present, they were recorded as positive but were not listed separately. Four cases in which the preparation was unsatisfactory were excluded from analysis.
A detailed pathological review of the tissues was also undertaken, using a protocol developed in an earlier study of
morphological correlations with estrogen receptor protein.26 Results of biochemical, cytological and pathological investigations performed independently were combined at the time of data analysis. ERP was measured by the dextran char
coal method described in detail
elsewhere.20'26 Incubations were carried out at room temperature for 60 minutes.
As in earlier studies of ERP from this
hospital, specimens with less than 10
femtomoles of ERP per mg of cytosol protein and in which less than 60 percent of
the binding was inhibited by 1000 fold excess untritiated estradiol, diethylstil-
besterol or 20,000 fold excess CI628 were designated as ERP negative. Those with 10 femtomoles or more of ERP with at least 60 percent inhibition were designated as positive. Specimens with intermediate combinations were classified as positive if the specific ERP were greater than six. Those with a lesser specific ERP
were termed negative. Specific ERP was determined as the product of femtomoles per mg cytosol protein and percentage inhibition. The constant of dissociation (Kd) was determined from a Scratchard

BARR BODY AND ESTROGEN RECEPTO R PROTEIN 493
plot based on analysis of three estradiol concentrations (1,2 and 5nM). Among specimens found to be ERP positive on the basis of binding in femtomoles and percent inhibition at InM estradiol, all but two primary tumors and two metas- tases had a KD greater than 5 x 10~9 M. Statistical significance of the results was evaluated by the chi-square test and for small samples by the Fisher exact probability ratio test.
Buccal smears from 20 other women between the ages of 18 and 74 were also examined as controls. Four were hospital employees with no history of breast disease. The others were a consecutive series of women with breast disease seen in the office of one of the authors (JAU). Half had been treated for mammary carcinoma and half had clinically diagnosed fibrocystic disease or mastitis.
Results
The distribution of Barr body counts and the relationship of these counts to the estrogen receptor protein content of the specimen are shown in table I. The specimens were categorized according to the percentage of tumor cells with Barr bodies to obtain data comparable to a prior study in which similar groupings were used.29 The percentage distribution of specimens was not significantly different in the two series. Carcinomas with Barr bodies in more than 10 percent of cells were more likely to be ERP positive. The difference in the frequency of ERP positivity between all specimens of carcinoma with less than 10 percent and more than 10 percent Barr body positive cells was significant (P < 0.01).
P r im a r y a n d M e t a s t a t ic C a r c in o m a
Barr body counts ranged from zero to 30 percent. The distribution was uni- modal. Approximately two-thirds of the specimens were primary tumors. The
TABLE X
Relationship Between Barr Body Distribution and Estrogen Receptor Protein in All Specimens
ERP Of Specimen
Less
Barr Body
than 10% 10
Distribution
to 20% More than 20%
No.Spec.
%TotalSpec.
No.Spec.
%TotalSpec.
No.Spec-
TotalSpec.
Positive 6 18 25 51 11 58Negative _27 82 24_ 49 8 42
Total 33 49 19
P < 0.01Counts in the table are related to the EBP content
determined by the dextran charcoal method.
others were locally recurrent carcinoma or distant metastases. Analysis of these groups separately (table II) revealed a positive correlation between Barr body count and ERP among the primary tumors (P < 0.005) but not among the smaller number of recurrent tumors examined.
A g e
Thirty-four patients were less than 50 years old and 67 were older. As shown in table III, a greater percentage of the older women had Barr body counts over 10 percent than did younger women; this difference, however, was not statistically significant.
T u m o r M a r g in s
Fourteen primary carcinomas were considered to have circumscribed or pushing margins and 51 had irregular or infiltrative borders. Virtually the same percentages of tumors with pushing and infiltrating margins (35 percent and 31 percent, respectively) had Barr body counts below 10 percent.
L y m p h o id R e a c t io n
Intensity of the lymphoid reaction in and around primary carcinomas was characterized as minimal to moderate (1
494 ROSEN, E T AL.
Estrogen Receptor Protein and Barr Body D is tr ibu tion : Comparison o f Primary and Metastatic Breast Carcinoma
TABLE II
Barr Body Distribution in Carcinoma PRIMARY CARCINOMA METASTATIC CARCINOMA
Less % 10% % Less % 10% %ERP of than 10% Total or more Total than 10% Total or more TotalSpecimen No. Spec. Spec. No. Spec. Spec. No. Spec. Spec. No. Spec. Spec.
Positive 4 1 9 29 66 2 17 7 29Negative 17 81 15 34 10 83 17 7 1
Total
P < 0.005Counts in the table are related to the ERP content determined by the dextran charcoal method.
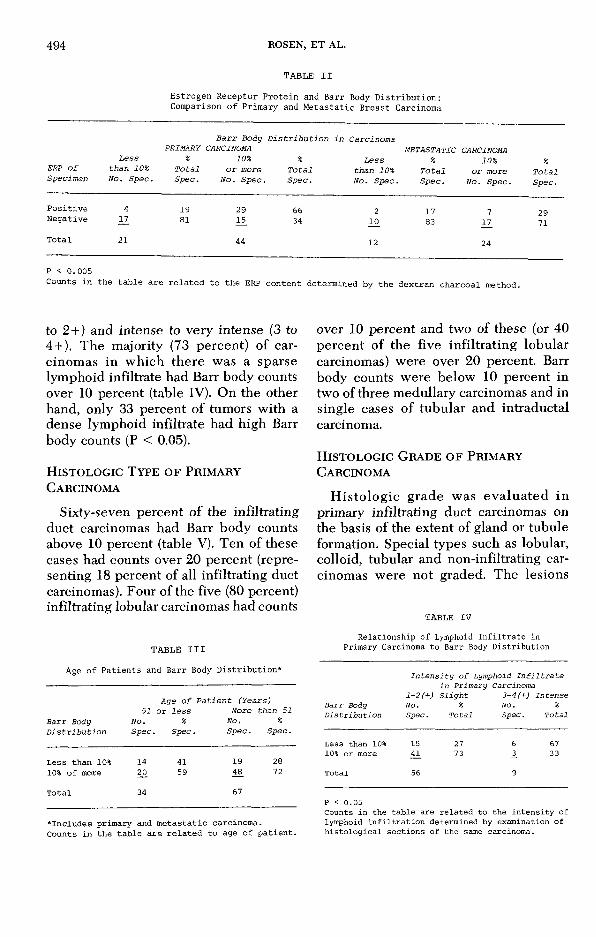
to 2+) and intense to very intense (3 to 4 + ). The majority (73 percent) of carcinomas in which there was a sparse lymphoid infiltrate had Barr body counts over 10 percent (table IV). On the other hand, only 33 percent of tumors with a dense lymphoid infiltrate had high Barr body counts (P < 0.05).
H i s t o l o g ic T y p e o f P r im a r y
C a r c in o m a
Sixty-seven percent of the infiltrating duct carcinomas had Barr body counts above 10 percent (table V). Ten of these cases had counts over 20 percent (representing 18 percent of all infiltrating duct carcinomas). Four of the five (80 percent) infiltrating lobular carcinomas had counts
T A B L E III
Age o f Patients and Barr Body D istribu tion*
Barr Body Distribution
51 N o . Spec.
Age of or less
%Spec.
Patient (Years)More than 51
No. % Spec. Spec.
Less than 10% 14 41 19 2810% of more 20. 59 48 72
Total 34 67
♦Includes primary and metastatic carcinoma.Counts in the table are related to age of patient.
over 10 percent and two of these (or 40 percent of the five infiltrating lobular carcinomas) were over 20 percent. Barr body counts were below 10 percent in two of three medullary carcinomas and in single cases of tubular and intraductal carcinoma.
H i s t o l o g ic G r a d e o f P r im a r y
C a r c in o m a
Histologic grade was evaluated in primary infiltrating duct carcinomas on the basis of the extent of gland or tubule formation. Special types such as lobular, colloid, tubular and non-infiltrating carcinomas were not graded. The lesions
TAB L E IV
Relationship of Lymphoid In f iltra te in Primary Carcinoma to Barr Body D istribution
Intensity of Lymphoid Infiltrate in Primary Carcinoma
1-2 (+) Slight 3-4 (+) IntenseBarr Body No. % No. %Distribution Spec. Total Spec. Total
Less than 10% 15 27 6 6710% or more 41_ 73 3_ 33
Total 56 9
P < 0.05Counts in the table are related to the intensity of lymphoid infiltration determined by examination of histological sections of the same carcinoma.

BARR BODY AND ESTROGEN RECEPTOR PROTEIN 495
were distributed on a scale of 1 (low- grade, well differentiated) to 4 (high grade, poorly differentiated). Grades 1 and 2 were compared with grades 3 and4. Forty-seven percent of carcinomas with counts below 10 percent and 42 percent of those with higher Barr body counts were in the group of better differentiated lesions. The differences between low and high grade carcinomas were not significant.
St a t u s o f A x il l a r y L y m p h N o d e s
There was no correlation between Barr body count in primary carcinomas and the presence or absence of axillary lymph node métastasés. Thus, patients with tumors that had low Barr body counts were not more likely to have axillary lymph node métastasés.
C o n t r o l s
Counts of Barr body positive cells in buccal smear preparations from control patients ranged from 7 to 19 percent. The mean count of Barr body positive cells in female buccal smears in this laboratory has been about 12. The average proportion of Barr body positive cells in buccal smear preparations was 13 percent for patients with breast carcinoma and the same for women with benign breast disease. This result is almost identical with the average result obtained in this laboratory for buccal smears in “normal” women.
Discussion
The nuclear sex chromatin or Barr body has been the subject of intense study since it was described in 1949 by Barr and Bertram.2 Graham and Barr originally proposed that this structure represented a condensation of the heterochromatic portions of both x-chromosomes.8 However subsequent investigations have shown
TABLE VHistologic Type of Primary Carcinoma
and Barr Body D istribution
Number of Cases with IndicatedPercentage of Cells with Barr Body
% of Caseswith Counts
Histologic Type Less 10% or of 10%of Carcinoma than 10% More or More
Infiltrating duct 16 38 67Infiltrating lobular 1 4 80Medullary 2 1 33Colloid 0 1Tubular 1 0Intraductal 1 0
that the nuclear chromatin body is one rather than both x-chromosomes. As a rule, it has been observed that the x-chromosomes complement of a normal cell is one more than the number of Barr bodies.
Moore and Barr21 reviewed, in 1957, several studies of the distribution of sex chromatin in normal tissues and neoplasms. Most benign and malignant tumors were found to have a sex chromatin distribution similar to that of the normal tissues of the host. Carcinoma of the female breast was a notable exception.21,32 In a substantial number of carcinomas, the proportion of tumor cells with a Barr body was lower than or higher than in normal tissues. In this and two prior reports from this institution29,34 and in other studies,14 the distribution of cases has been essentially unimodal.
There is surprisingly little information available about the relationship between the Barr body and the actual chromosome complement of neoplastic cells. In a study of cervical carcinoma, Atkin1 found a normal nuclear chromatin pattern in 80 percent of tumors which were “near diploid.” Chromatin bodies were present in nuclei of only 20 percent of “near tetra- ploid” carcinomas. Gropp and Wolf s9 studies indicated that nuclei in carcinomas composed of small, uniform cells

496 ROSEN, E T AL.
were more likely to contain a Barr body than nuclei in tumors composed of larger cells.
Kallenberger et al15 correlated the DNA content of Feulgen stained imprints with the Barr body incidence in mammary carcinoma. An increased frequency of polyploidy was found in tumors with low chromatin body counts. Other investigators have described the DNA content and chromosome constitution of benign16 and malignant15,16,18,19 breast lesions. Many of these reports were summarized by Ludwig et al18 in 1973 who concluded that most mammary carcinomas were aneuploid. None of these studies provide any information about the relationship between the Barr body and x-chromo- some content of mammary carcinoma cells.
Little attention has been given to correlating the Barr body distribution in breast carcinoma with histologic characteristics of the tumors. Kimel17 concluded that Barr body count and tumor differentiation, as described by nuclear grade, were inversely related. However, in a prior study29 from this institution and in the current investigation, there was no association between Barr body count and tumor grade as expressed in terms of the degree of glandular differentiation. Several authors7,17,29 have failed to find a significant correlation between the presence or absence of axillary lymph node métastasés and Barr body count in the primary tumor. Evidently the positive correlation between Barr body count in the primary tumor and survival7,24,29,34 is not due to differences in the frequency of métastasés between tumors with high and low Barr body counts.
The reported positive correlation between response to therapy and Barr body count might be explained by the finding now being reported, that there was a highly significant relationship between the ERP content and Barr body count in
primary mammary carcinomas. However, it was a surprise to find that this relationship was not true for specimens of metastatic carcinoma although there was a slightly higher percentage of metastatic carcinomas with positive ERP and Barr body counts over 10 percent. No readily apparent explanation is available for the difference between the two groups of specimens. However, the frequency of ERP positive specimens is lower, overall, among metastases than it is in primary tumors.26
Several observations about ERP, Barr body count and characteristics of the tumors or patients appear to be interrelated. Primary carcinomas in post menopausal patients are more likely to be estrogen receptor positive than are carcinomas in younger or premenopausal women. In the current study, it has been noted that primary tumors in older patients were also more likely to have higher Barr body counts. ERP26 and Barr body count both were negatively correlated with lymphoid infiltration in the primary lesion. The relationships previously reported between histologic type of mammary carcinoma and ERP26 were similar to those between Barr body count and histologic type. Medullary carcinomas tended to have low Barr body counts and to be ERP negative. A significantly high proportion of infiltrating lobular carcinomas were ERP positive and they tended to have high Barr body counts.
These differences in the ERP properties of lobular and medullary carcinoma parallel the finding noted by Gropp and WoIP that tumor cells with small, uniform nuclei were likely to have higher Barr body counts. Lobular carcinoma is characterized by the relatively small size and uniformity of its nuclei whereas medullary carcinoma features larger more anaplastic nuclei.
In view of the foregoing, it seems unlikely that the correlation between ERP and Barr body count in primary mammary

BARR BODY AND ESTROGEN RECEPTOR PROTEIN 497
carcinomas is simply coincidental. The cytoplasmic complex of estrogen and ERP have been shown to be translocated to the nucleus where they are bound to “acceptor” sites in the chromatin. Many of the biochemical steps have been studied in great detail,4,22 butthe chromosomal site of this activity remains to be identified. Nor is it known which chromosomes carry the information for the synthesis of receptor protein.
The direct correlation between E RP and the Barr body content of these cells suggests that one or more x-chromosome is involved in the synthesis of ERP and/or may carry locus for estrogen-ERP action. This possibility is supported by our observation that those morphological properties of primary mammary carcinomas which were significantly associated with ERP bore a similar relationship to the Barr body count. On the other hand, factors that did not relate significantly to receptor protein also proved not to correlate with Barr body counts in the primary carcinoma.
Salih et al28 have suggested that the estrogen sensitivity of breast cancer can be assayed by a histochemical method for measuring dehydrogenase activity of the pentose shunt pathway. They observed that the dehydrogenase concentration tended to increase when samples of a breast carcinoma were incubated in vitro with hormones that influence the growth of breast cancer.11 Increased activity of glucose-6-phosphate dehydrogenase, (G-6-PD) an x-linked enzyme3,6 under the influence of estrogen is additional evidence that one or more loci involved in estrogen-ERP activity may be located on an x-chromosome.
As noted previously, in the normal female somatic cell only one of the two x-chromosomes is active. As a consequence, in an individual heterozygous for the G-6-PD gene, either the fast or slow varient would be expressed in a given cell. Tumors found to contain one isoen
zyme are thought to arise from a single cell (clonal origin). When a mixture of enzymes is present, it has been postulated that the tumor had a multicellular origin.
Limited data previously reported indicated a mixed pattern of G-6-PD in mammary carcinoma. Recent studies of the enzyme content of mammary carcinoma revealed higher levels of G-6-PD in comparison to non-carcinomatous mammary tissue10 owing especially to an increased proportion of the faster migrating isoenzyme G-6-PD-I. Increased G-6-PD-I activity has been observed after estrogen exposure25 in the rodent mammary tumor. While the mean level of G-6-PD activity was lower in human mammary carcinomas characterized as estrogen receptor positive,30 this result did not necessarily reflect the levels of enzyme that would have been found in an ERP positive tumor after hormone stimulation. No report has been found that compared G-6-PD activity in ERP positive and negative human mammary carcinomas after hormone stimulation.
Finally, our failure to find a significant correlation between ERP and Barr body count in metastases is puzzling. It has been reported elsewhere by us that metastases of mammary carcinoma may differ in their ERP properties from those of the primary tumor in nearly a third of instances when the specimens compared were not obtained simultaneously.27 The mean interval between the treatment of a primary tumor and the appearance of a metastasis was 9.6 months in cases in which there was no discrepancy and 19.3 months when the ERP differed between the primary and metastasis. Discrepancies were observed in 26 percent of cases in which non-simultaneous metastases were compared with one another and in 15 percent when simultaneously occurring but anatomically separate specimens were compared.27
498 ROSEN, E T AL.
It remains to be determined whether these differences in ERP are the result of genotypic alterations in mammary carcinoma cells that may occur with the passage of time or if they are a consequence of the origin of metastases from cells with existing differences in their ERP properties. Of course, these mechanisms would not be mutually exclusive. Whatever its origin, this variability may prove to be responsible for the lack of association between Barr body distribution and ERP in metastatic carcinoma.
Acknowledgment
Thanks are extended to Abraham Port for his assistance in evaluation of the data by computer.
References
1. At k in , N . B.: Sex chrom atin in female breast
cancer. Lancet 71:1145-1146, 1967.2. Ba r r , M. L. and Be r t r a m , E. G.: A mor
phological distinction between neurones of the male and female and the behavior of the nucleolar satellite during accelerated nucleopro- tein synthesis. Nature 163:676-677, 1949.
3. Be u t l e r , E., C o l l in s , Z., and I r w in , L. E.: Value o f genetic variants of glucose-6 - phosphate dehydrogenase in tracing the origin of malignant tumors. New Eng. J. Med. 276:389-391, 1967.
4. C l a r k , J. H. and Pe c k , J r ., E. J.: Nuclear retention of receptor-estrogen complex and nuclear acceptor sites. Nature 260:635-636,1976.
5. E h l e r s , P. N. and H e in z , H . A.: Zelkern- morphologisches Geschlecht und Hormonelle Beeinfluszbarkeit des Mamma-Carcinoma. Langenbecks Arch. 288:484-498, 1958.
6 . F ia l k o w , P. J.: Genetic marker studies in neoplasia. Genetic Concepts and Neoplasia. Proceedings of 23rd Annual Symposium on Cancer Research. University of Texas, M.D. Anderson Hospital, Baltimore, Williams and Wilkins, 1970.
7. G h o s h , S. N. and Sh a h , P. N.: Prognosis and incidence of sex chromatin in breast cancer. A preliminary report. Acta Cytologica 19:58-61,1975.
8. G r a h a m , M . A. and Ba r r , M . L .: Sex differ
ence in m orpho logy o f m etabo lic nuc le i in
somatic cells o f cat. Anat. Rec. 112 :709-723, 1952.
9. GROPP, H. and W OLF, W .: Uber den cytogene- tischen Z u s a m m e n h a n g Zwischen sexchromatin und Chromosomenstatus bein mammacarcinoma. Langenbeck’s Arch. Chir. 313:400-405, 1965.
10. H i l f , R ., Re c t o r , W. D., and O r l a n d o , R . A.: Multiple molecular forms of lactate dehydrogenase and glucose-6 -phosphate dehydrogenase in normal and abnormal human breast tissues. Cancer 37:1825-1830, 1976.
11. H o b b s , J. R., D e So u z a , I., Sa l ih , H ., and Ra g g a t t , P.: Selection of hormone-dependent breast cancers. Brit. J. Surg. 61:785-786, 1974.
12. Je n s e n , E. V.: Some newer endocrine aspects of breast cancer. New Eng. J. Med. 291:1252- 1253, 1974.
13. Je n s e n , E. V., M o h l a , S., G o r e l l , T. A., and D e So m b r e , E. R.: The role of estrophilin in estrogen action. Vitamins Hormones 32:89- 127, 1974.
14. KALLENBERGER, V. A.: Geschlechtschromatin bei Mammakarzinomen. Schw. med. Wochensch. 942:1450-1458, 1964.
15. Ka l l e n b e r g e r , A., H a g m a n n , A., and D e s c o e u d r e s , C.: The interpretation of abnormal sex chromatin incidence in human breast tumors on the basis of DNA measurements. Europ. J. Cancer 3 :439-448, 1968.
16. Ka l l e n b e r g e r , A.: Chromosomal anomalies in benign and premalignant breast lesions. Characterization of Human Tumors. Davis, W. and Maltoni, C., eds. Amsterdam, Elsevier Publishing Co., pp. 171-177, 1973.
17. K im EL, V.: Clinical-cytological correlations of mammary carcinoma based upon sex chromatin counts—a preliminary study. Cancer 10:922-927, 1957.
18. L u d w ig , A. S., O k a g a k i, T., R ic h a r t , R. M., and L a t t e s , R .: Nuclear DNA content of lobular carcinoma in situ of the breast. Cancer 31:1553-1560, 1973.
19. M a r k , J.: Two pseudodiploid human breast carcinomas studied with G-band technique. Europ. J. Cancer 11:815-819, 1975.
20. M e n e n d e z -Bo t e t , C. J., N is s e l b a u m , J. S.,
F l e is h e r , M ., R o s e n , P. P., F r a c c h ia , A., R o b b in s , G., Ur b a n , J. A., and Sc h w a r t z , M .
K.: Correlation between estrogen receptor protein and carcinoembryonic antigen in normal and carcinomatous human breast tissue. Clin. Chem. 22:1366-1371, 1976.
21. M o o r e , K. L. and Ba r r , M. L.: The sex chromatin in human malignant tumors. Brit. J. Cancer 11:384-392, 1957.
22. O ’M a l l e y , B. W.: Steroid hormone regulation of gene expression. Adv. Pathobiol. 2:84-137,1976.
23. O ’M a l l e y , B. W. and M e a n s , A. R.-. Female steroid hormones and target cell nuclei. Science 183:610-620, 1974.
24. Pe r r y , M.: Evaluation of breast tumor sex chromatin (Barr body) as an index of survival and response to pituitary ablation. Brit. J. Surg. 59:731-734, 1972.
25. R ic h a r d s , A. H . and H i l f , R.-. Effect of estrogen administration on gIucose-6 -phosphate dehydrogenase and lactate dehydrogenase isoenzymes in rodent mammary tumors and normal mammary glands. Cancer Res. 32:611-616, 1972.

BARR BODY AND ESTROGEN R ECEPTO R PROTEIN 499
26. R o s e n , P. P., M e n e n d e z -Bo t e t , C. J., N is-
s e l b a u m , J. S., U r b a n , J. A., M i k e , V., F r a c c h ia , A., and S c h w a r t z , M . K.: 30.Pathological review of breast lesions analyzedfor estrogen receptor protein. Cancer Res. 35:3187-3194, 1975.
27. R o s e n , P. P., M e n e n d e z -Bo t e t , C. J., U r b a n , J. A., F r a c c h ia , A., and Sc h w a r t z ,
M. K.: Estrogen receptor protein (ERP) in multiple tumor specimens from individual patients with breast carcinoma. Cancer 39:2194-2200,
1977‘ 33,28. Sa l ih , H., F l a x , H., and H o b b s , J. R.: In vitro
sensitivity of breast cancer tissue as a possible screening method for hormonal treatment. Lancet 7:1198-1202, 1972. 3 4
29. S a v in O , A. and K O SS , L. G.: The evaluation of sex chromatin as a prognostic factor in car-
cinoma of the breast. A preliminary report. Acta Cytologica 15:372^374, 1971.Sa v l o v , E . D ., W it t l if f , J. L ., H i l f , R., and H a l l , T . C.: Correlations between certain biochemical properties of breast cancer and response to therapy: A preliminary report. Cancer 33:303-309, 1974.Sh ir l e y , R . L.: The nuc lea r sex of breast
cancer. Surg. G ynec . O bstet. 725:737—740,1967.Ta v a r e s , A. S.: Sex chromatin in tumor cells. Acta Cytologica 6:90-94, 1962.Ve r d e r b e r , W ., W a s l , H ., Ka u f m a n n , F., and R e g e l e , H .: Zur Frage des Sex- Chromatins beim Mammacarcinom. Langen- beck’s Arch. Clin. Chir. 373:406-408, 1965. W a c k e r , B. and M il e s , C. P.: Sex chromatin incidence and prognosis in breast cancer. Cancer 79:1651-1654, 1966.