b scan
TRANSCRIPT

ULTRASONOGRAPHY
(B-SCAN)
VASIUR RAHMANDr R. P. Centre, AIIMS
HISTORY
1793: Lazzaro Spallanzani (Italy) discovered that bats orient
themselves with the help of sound whistles while flying in
darkness. This was the basis of modern ultrasound application
Bats use ultrasounds to navigate in the darkness

INTRODUCTION
first used in the field of ophthalmology
by MUNDT and HUGHES.
Oksala et al report the sound velocities
in the various compartment of eye.
Contact Bscan was introduced by
Bronson and it being portable, become a
part of everyday use in ophthalmology.
physics
Ultrasound
○ Longitudinal wave
○ Alternating compressions and rarefactions of
molecules
>20khz (20,000 oscillations /sec) Ultrasound
Similar to sound waves
Reflected
Refracted

Low
frequency (1 to 5 MHz)
Longer
wavelength
Lower Resolution (abdominal and pelvic structure)
Abdominal ultrasound Ophthalmic ultrasound
High frequency (8 to 10 MHz)
Short wavelength (< 0.2mm)
Higher Resolution of minute ocular and orbital structure
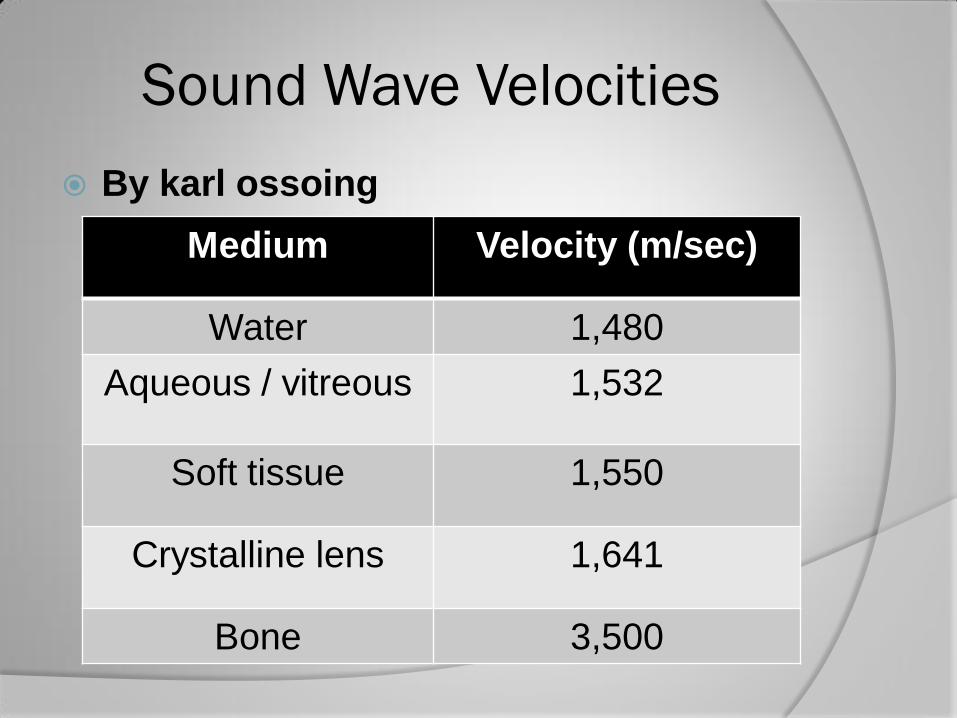
By karl ossoing
Sound Wave Velocities
Medium Velocity (m/sec)
Water 1,480
Aqueous / vitreous 1,532
Soft tissue 1,550
Crystalline lens 1,641
Bone 3,500
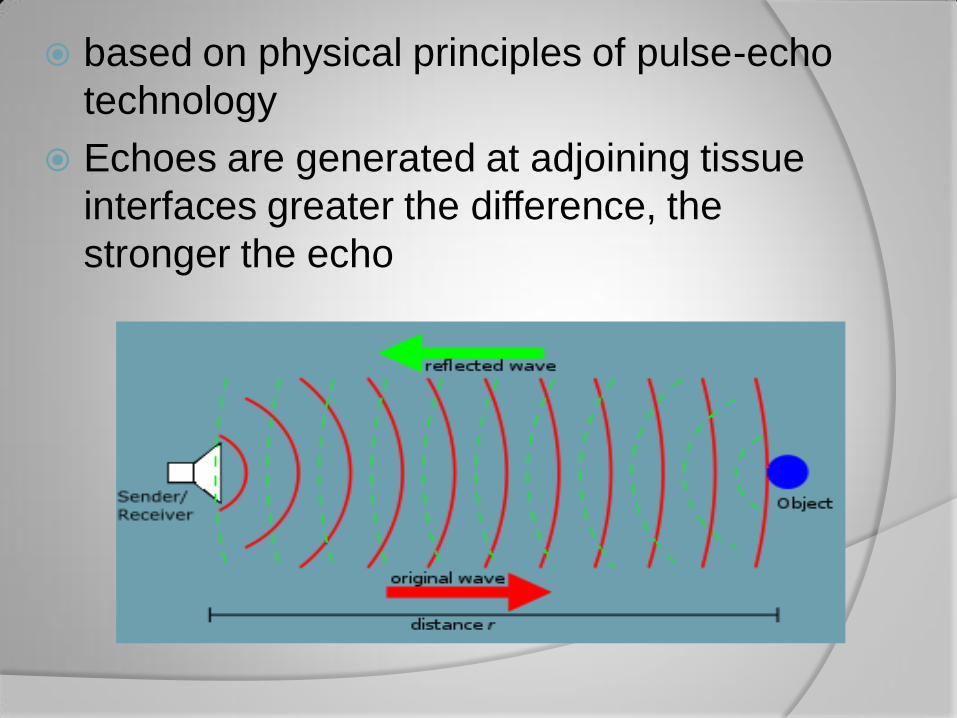
based on physical principles of pulse-echo
technology
Echoes are generated at adjoining tissue
interfaces greater the difference, the
stronger the echo

having frequency greater than 20khz for
imaging the posterior segment-8 to 25 MHz
for imaging the anterior segment-50 MHz
Rule-greater the frequency lesser will be
penetration

Probe thick, with a mark
emit focussed sound beam at frequency 10mhz
mark on the Bscan probe indicates beam orientation-area towards which mark is directed appears at the top of the echogram on display screen

ULTRASOUND PRINCIPLES AND PHYSICS
Angle of incidence:
Perpendicularity to the
area of interest always
should be maintained to
achieve the strongest
echo.
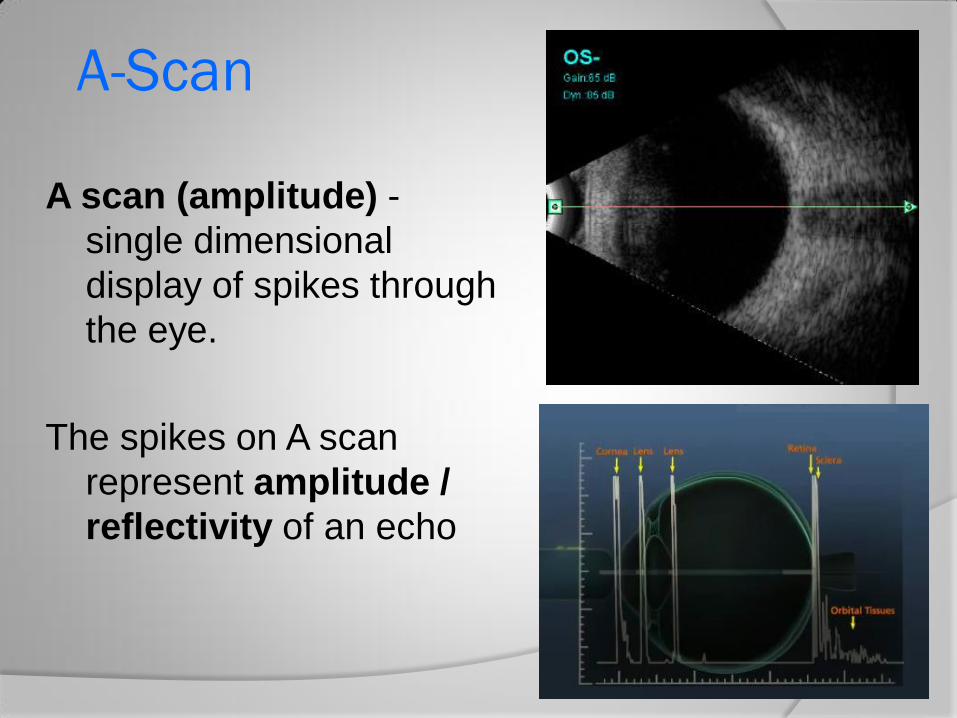
A scan (amplitude) -
single dimensional
display of spikes through
the eye.
The spikes on A scan
represent amplitude /
reflectivity of an echo
A-Scan

Transverse scan
Longitudinal
Axial
B-scan Probe Orientations
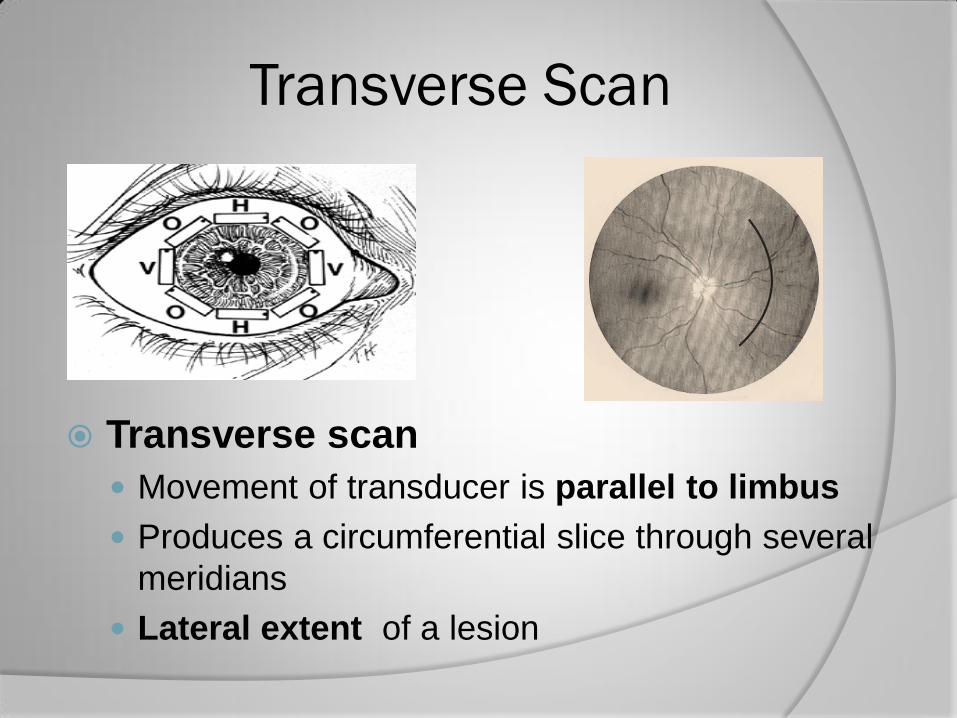
Transverse scan
Movement of transducer is parallel to limbus
Produces a circumferential slice through several
meridians
Lateral extent of a lesion
Transverse Scan
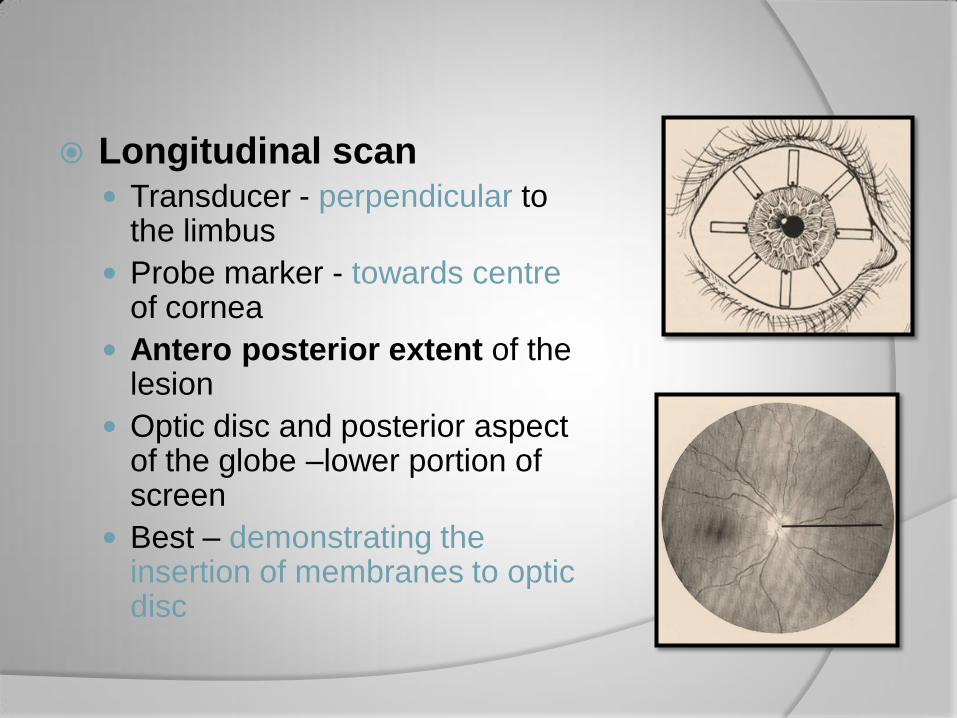
Longitudinal scan Transducer - perpendicular to
the limbus
Probe marker - towards centre of cornea
Antero posterior extent of the lesion
Optic disc and posterior aspect of the globe –lower portion of screen
Best – demonstrating the insertion of membranes to optic disc
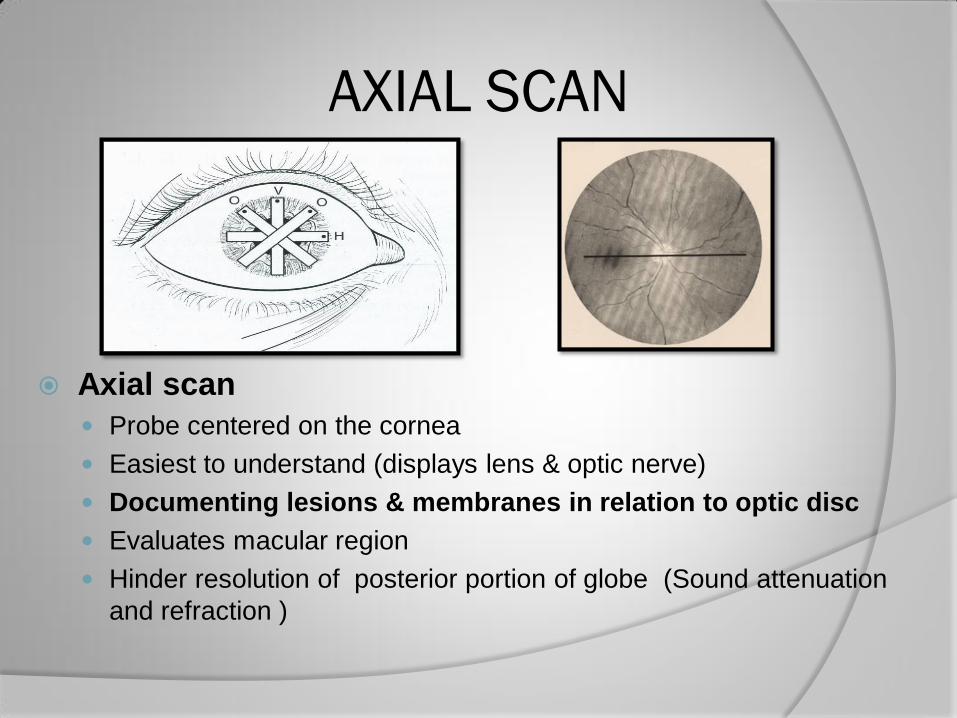
Axial scan
Probe centered on the cornea
Easiest to understand (displays lens & optic nerve)
Documenting lesions & membranes in relation to optic disc
Evaluates macular region
Hinder resolution of posterior portion of globe (Sound attenuation
and refraction )
AXIAL SCAN

CLOCK HOUR
PROBE POSITION
CLOCK AREA
SCREENED
3-limbus 9-posterior
3-equator 9-equator
3-firnix 9-anterior
6-limbus 12-posterior
6-equator 12-equator
6-fornix 12-anterior
Why we need B-scan..????
Evaluation of intraocular details
Evaluation of retrochoroidal lesions
especially tumors
Examination of retrobulbar soft tissue
masses
Identification, localization and
measurement of foreign bodies
Assessment of damage in trauma cases

PROCEDURE
mostly the Bscanning is done
transpalpebrum
Lesions must place at the centre of scanning
beam
Lowest possible decibel gain consistent with
the maintenance of adequate intensity
should be used

Measured in decibels
Higher gain –
Display weaker echos like
vitreous opacities
Lower gain
Stronger echoes (retina and
sclera)
Better resolution
Gain
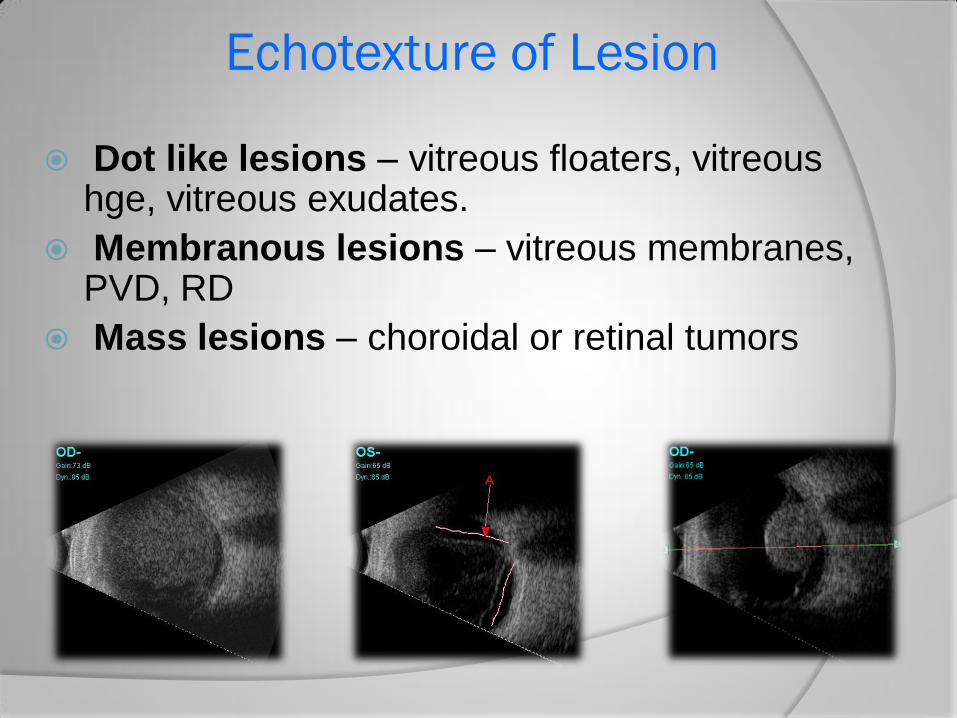
Dot like lesions – vitreous floaters, vitreous hge, vitreous exudates.
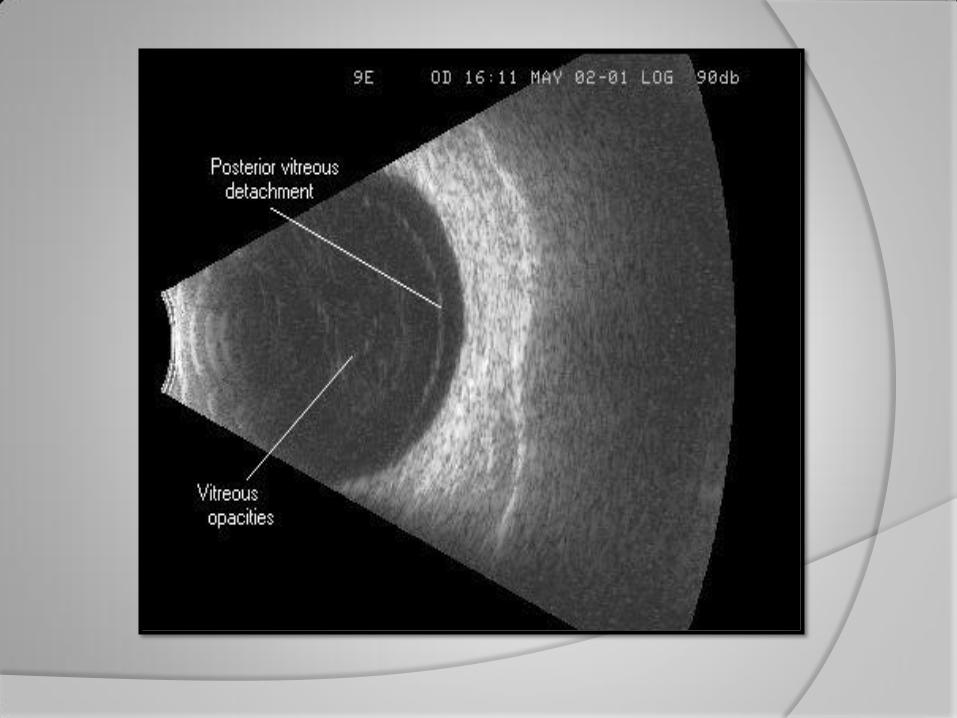
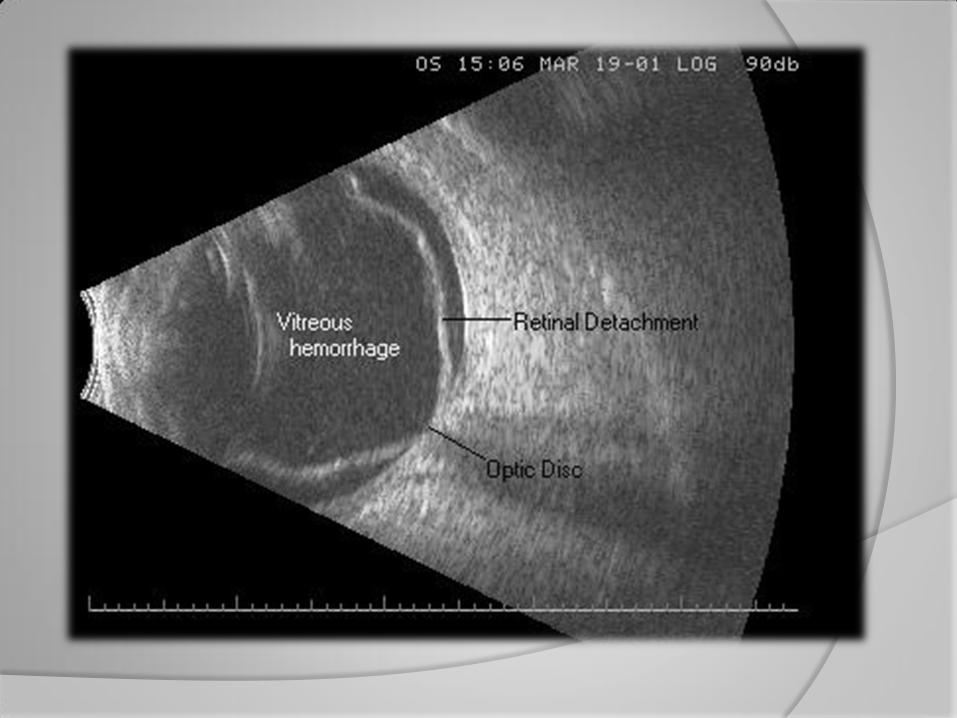
Membranous lesions – vitreous membranes, PVD, RD
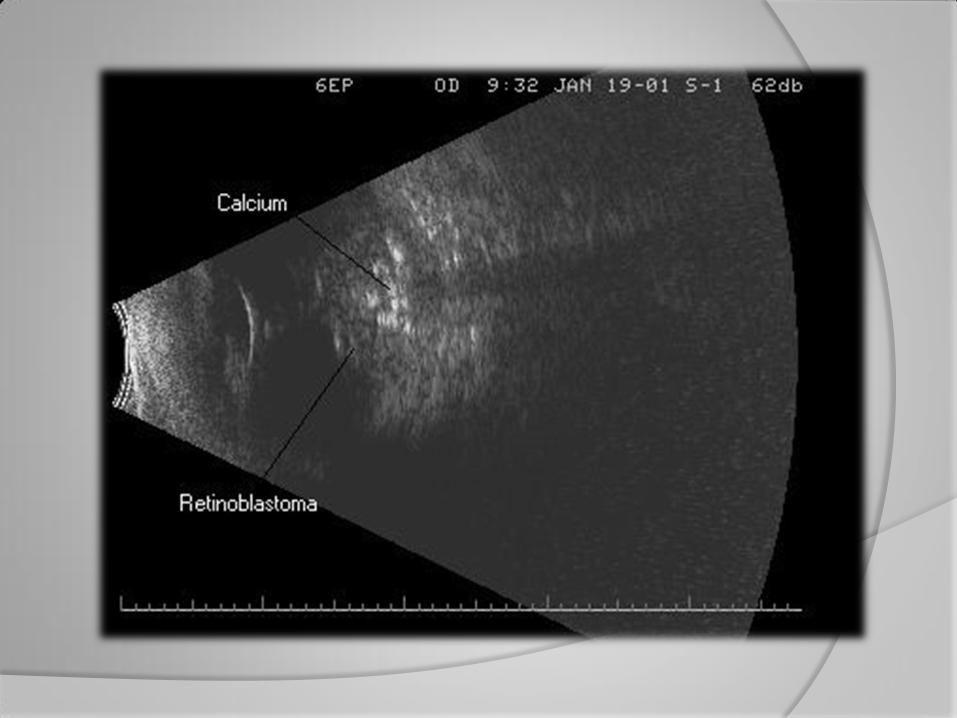
Mass lesions – choroidal or retinal tumors
Echotexture of Lesion
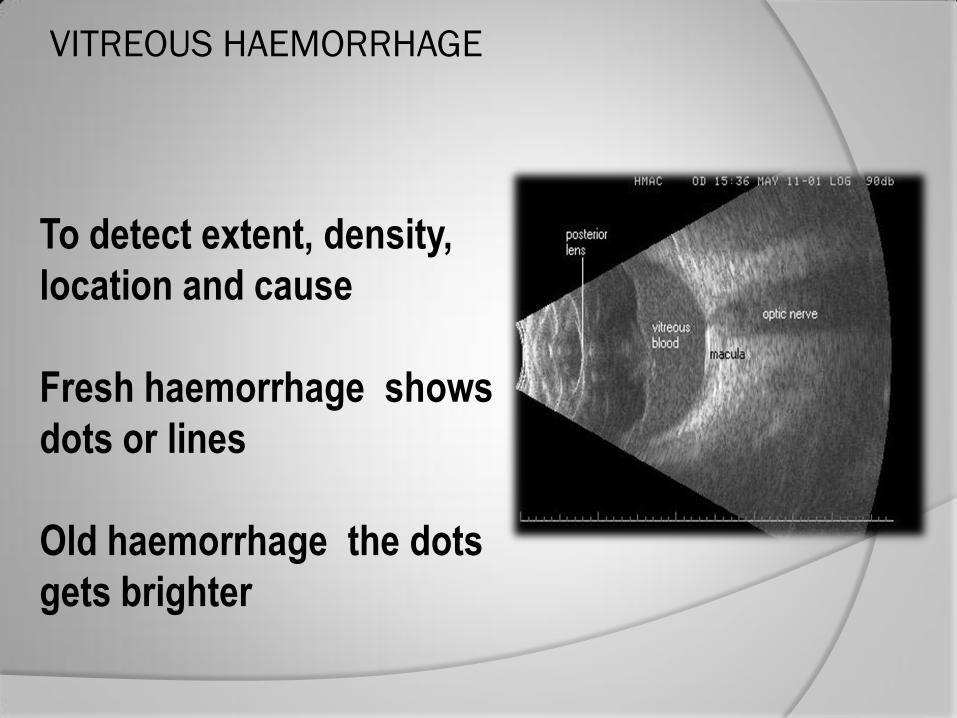
VITREOUS HAEMORRHAGE
To detect extent, density,
location and cause
Fresh haemorrhage shows
dots or lines
Old haemorrhage the dots
gets brighter

CHOROIDAL DETACHMENT KISSING CHOROIDS

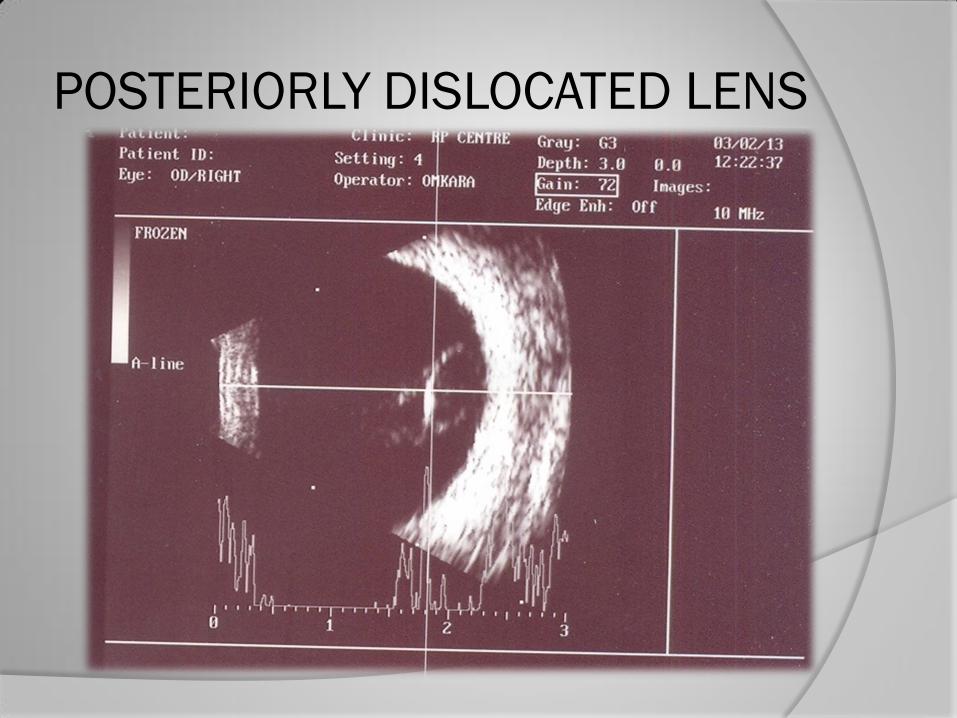
POSTERIORLY DISLOCATED LENS
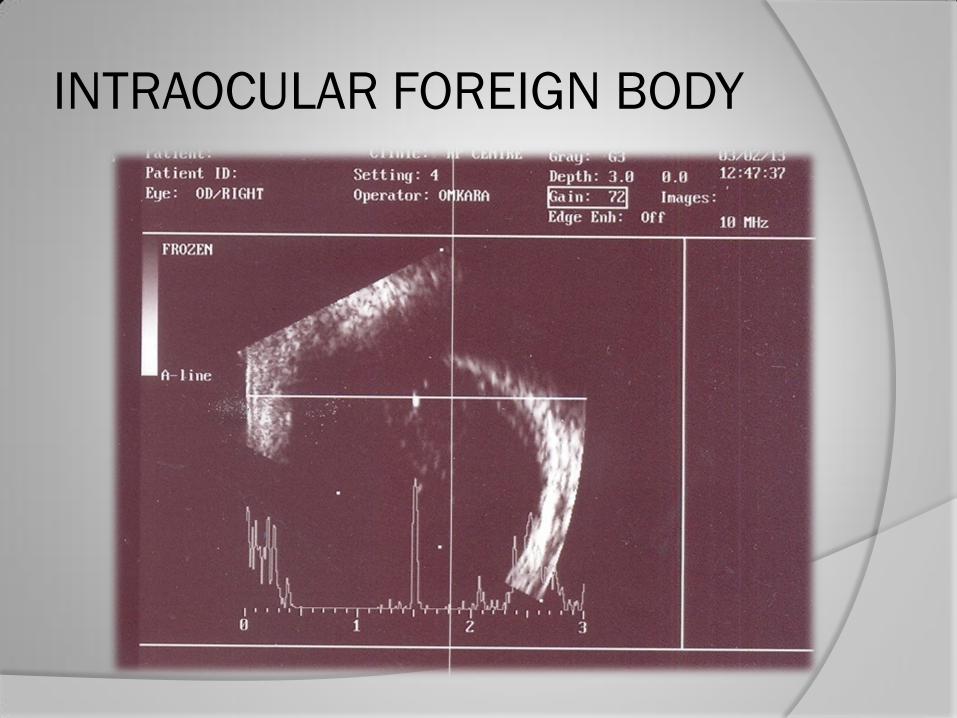
INTRAOCULAR FOREIGN BODY
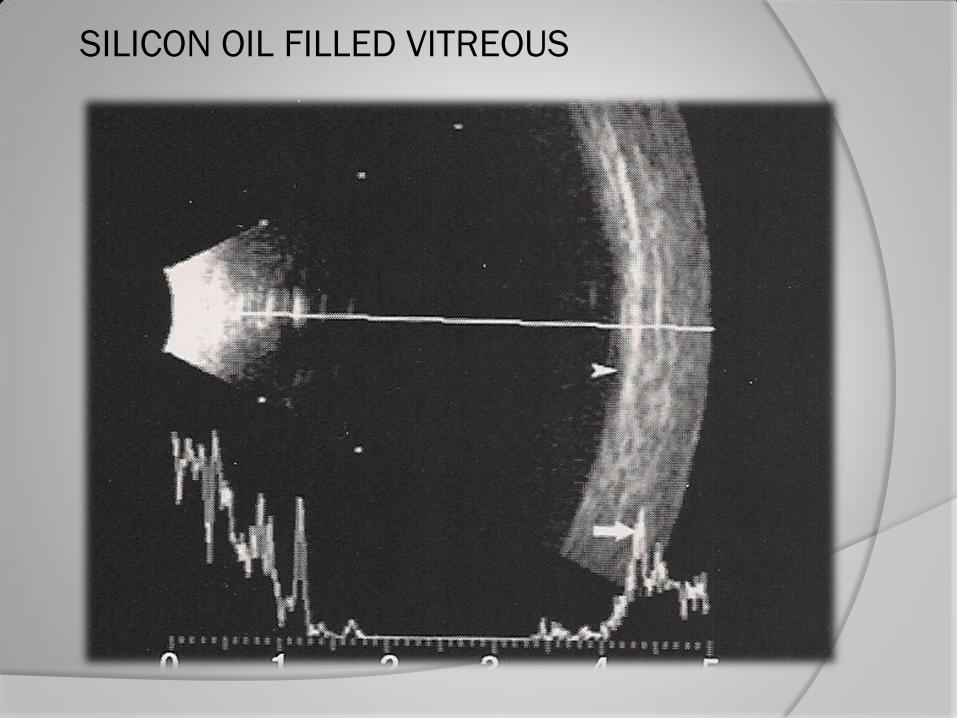
SILICON OIL FILLED VITREOUS
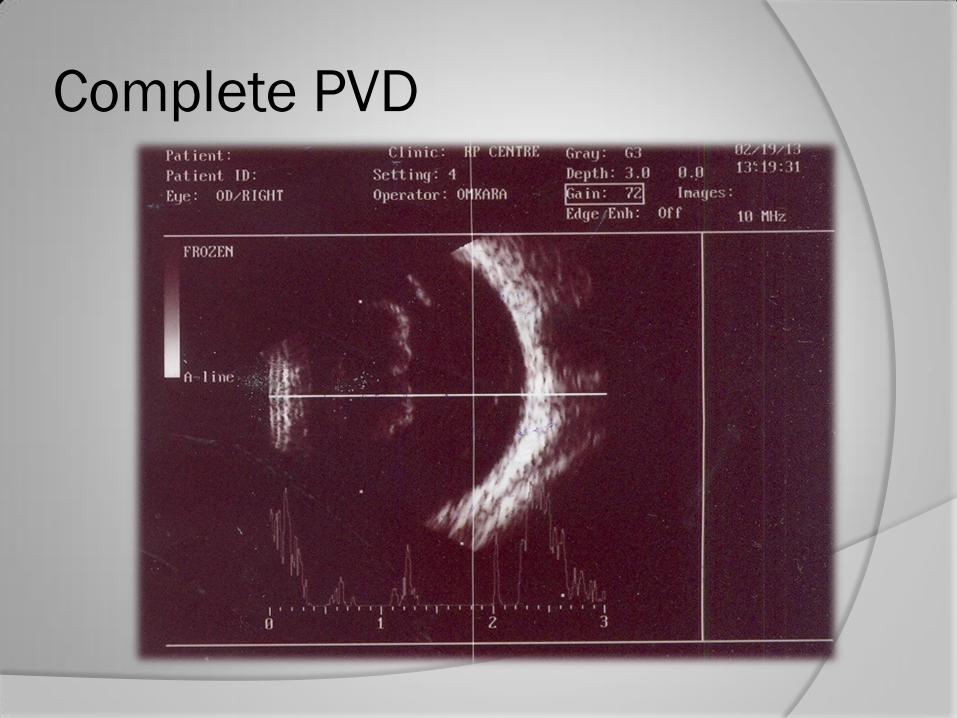
Complete PVD
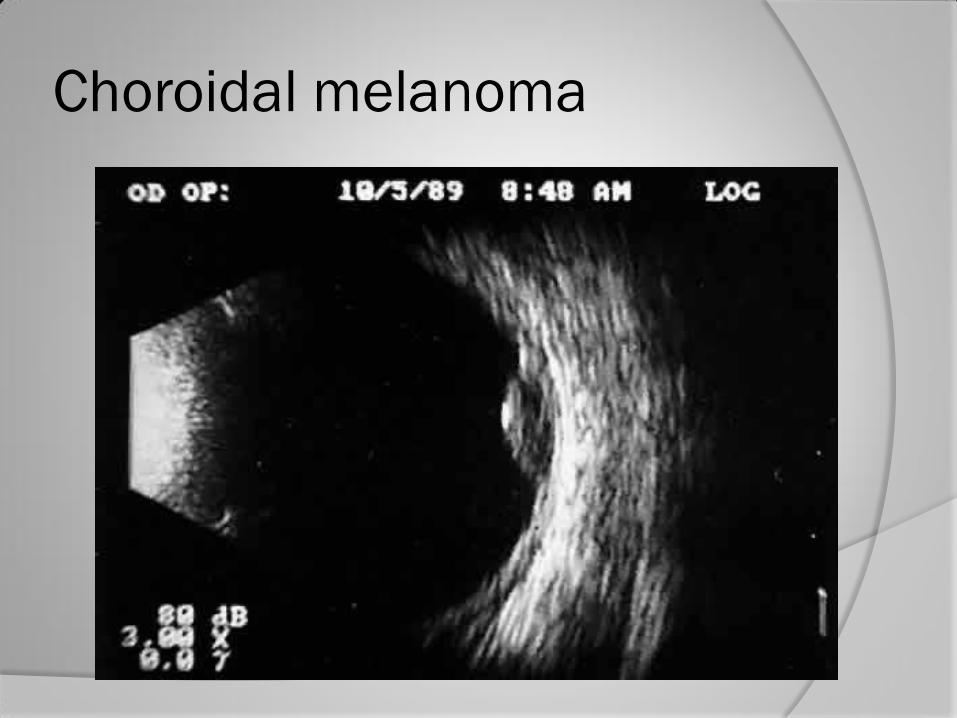
Choroidal melanoma

Endophthalmitis

Intra ocular foreign body
Non invasive
Performed in an office setting
Does not expose to radiation
High resolution echography provides
reliable and accurate assessment
Ideal for follow up of lesion
Advantages:

Disadvantages
High frequency sounds waves have limited penetration

THANK YOU