author(s): patrick carter, daniel wachter, rockefeller ... · pdf images/cdimage4.jpg...
TRANSCRIPT

Author(s):PatrickCarter,DanielWachter,RockefellerOteng,CarlSeger,2009-2010.License:Unlessotherwisenoted,thismaterialismadeavailableunderthetermsoftheCreativeCommonsAttribution3.0License:http://creativecommons.org/licenses/by/3.0/
WehavereviewedthismaterialinaccordancewithU.S.CopyrightLawandhavetriedtomaximizeyourabilitytouse,share,andadaptit.Thecitationkeyonthefollowingslideprovidesinformationabouthowyoumayshareandadaptthismaterial.Copyrightholdersofcontentincludedinthismaterialshouldcontactopen.michigan@umich.eduwithanyquestions,corrections,orclarificationregardingtheuseofcontent.Formoreinformationabouthowtocitethesematerialsvisithttp://open.umich.edu/education/about/terms-of-use.Anymedicalinformationinthismaterialisintendedtoinformandeducateandisnotatoolforself-diagnosisorareplacementformedicalevaluation,advice,diagnosisortreatmentbyahealthcareprofessional.Pleasespeaktoyourphysicianifyouhavequestionsaboutyourmedicalcondition.Viewerdiscretionisadvised:Somemedicalcontentisgraphicandmaynotbesuitableforallviewers.

CitationKeyformoreinformationsee:http://open.umich.edu/wiki/CitationPolicy
Use+Share+Adapt
MakeYourOwnAssessment
CreativeCommons–AttributionLicense
CreativeCommons–AttributionShareAlikeLicense
CreativeCommons–AttributionNoncommercialLicense
CreativeCommons–AttributionNoncommercialShareAlikeLicense
GNU–FreeDocumentationLicense
CreativeCommons–ZeroWaiver
PublicDomain–Ineligible:WorksthatareineligibleforcopyrightprotectionintheU.S.(USC17§102(b))*lawsinyourjurisdictionmaydiffer
PublicDomain–Expired:Worksthatarenolongerprotectedduetoanexpiredcopyrightterm.
PublicDomain–Government:WorksthatareproducedbytheU.S.Government.(USC17§105)
PublicDomain–SelfDedicated:Worksthatacopyrightholderhasdedicatedtothepublicdomain.
FairUse:UseofworksthatisdeterminedtobeFairconsistentwiththeU.S.CopyrightAct.(USC17 § 107)*lawsinyourjurisdictionmaydifferOurdeterminationDOESNOTmeanthatallusesofthis3rd-partycontentareFairUsesandweDONOTguaranteethatyouruseofthecontentisFair.Tousethiscontentyoushoulddoyourownindependentanalysis todeterminewhetherornotyourusewillbeFair.
{Contentthecopyrightholder,author,orlawpermitsyoutouse,shareandadapt.}
{ContentOpen.Michiganbelievescanbeused,shared,andadaptedbecauseitisineligibleforcopyright.}
{ContentOpen.MichiganhasusedunderaFairUsedetermination.}

Advanced Emergency Trauma Course
GhanaEmergencyMedicineCollaborativePatrickCarter,MD∙DanielWachter,MD∙RockefellerOteng,MD∙CarlSeger,MD
AirwayandVentilatorManagement
Presenter:DanielWachter,MD

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Essentials of Emergency Airway Management
Knowtheanatomy. Learntheequipment. Learnthetechniques-10and20. Developjudgment.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Compromise in Emergency Patients
CommonEtiologies:• Cardiacfailureandarrest• Respiratoryfailure(primary)• Neurologicaldiseases• Multipletrauma,headinjury,burns• Toxicologicalemergencies

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Indications for Emergency Airway Intervention
What are the indications?
Zen(flickr)

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Indications for Emergency Airway Intervention
Tocorrecthypoxemia(oxygenate)orhypercarbia(ventilate).
Toprovideapatent,secureairway. Tofacilitateotherinterventionsincriticallyillpatients(prophylactic).
Anticipateneedforintubationbasedonclinicalcourseandlikelihoodofdeterioration.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Management Options• Patencymaneuvers• Non-invasiveventilation• Endotrachealintubationwithorwithoutinductionandparalyticagents• Nasotrachealintubation• Adjunctairways• Surgicalairway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
O2 Delivery Devices VenturiMask HudsonMask Nonrebreather NasalCannula
www.rcsed.ac.uk/ journal/vol46_5/fig-2.gif

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
O2 Delivery Devices BiPAP/CPAP
Source Undetermined Rarely works in critical airway cases – is patient DNI?

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
O2 Delivery Devices Endotrachealtube
Source Undetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Patient Risk Factors for Airway Compromise Whyaretheseguysscaryairwaypatients?• Externalanatomy• AirwayAnatomy
SpoonyMushroom(flickr) http://commons.wikimedia.org/wiki/File:Glidescope_02.JPG

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
External Anatomy DifficultBag/MaskVentilation• Edentulous• Obese• HistoryofSnoring/SleepApnea• Beard• Age>55• Anatomicallyabnormalfacies• Facial/necktrauma• Obstructiveairwaydisease• 3rdtrimesterpregnancy

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
External Anatomy DifficultIntubation• Necktrauma• Prominentincisors• Recedingmandible• Cervicalspineimmobilization
Eg.bamboospine,fusion• Short,thinneck• Anatomicallyabnormalfacies• Morbidobesity

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Anatomy Mustknowtheanatomycold• Anatomicrelationship:
Tongue Vallecula Epiglottis VocalCords
Source Undetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Review of Airway Anatomy
Nasopharynx Oropharynx Hypopharynx Larynx–Laryngoscopicview• Musthavethisburnedintoyourbraininordertobeanairwayexpert

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Anatomy
www.aap.org/nrp/ images/CDIMAGE4.JPG
www.medword.com/ pics/Anatomy/Fig956.gif
arytenoids & aryepiglottic folds

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Anatomy YouMUSTknowtheanatomy Maybedistorted……..
www.bgsm.edu/voice/ images www.bgsm.edu/voice/ images

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
http://www.childrensmemorial.org/cme/online/article.asp?articleID=179
http://www.childrensmemorial.org/cme/online/article.asp?articleID=179

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse Source Undetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Assessment Decidingwhoneedsactiveairwaymanagement• Historyofpriordifficultyintubations• PhysicalExamFeatures
Obesity Shortneck Macroglossia Micrognathia Largeteeth SmallMouth
• ClinicalCondition Stablevs.Unstable ActiveBleeding Vomiting Needforprocedures OtherInterventions

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Physical Assessment of Airway Status
VitalSigns• RespiratoryRate,O2sat,BloodPressure,Heartrate
MentalStatus• Agitation,Somnolence,Coma
AirwayPatency• Secretions,Stridor,Obstruction,Edema
Ventilation• BreathSounds,AccessoryMuscleuse,Retractions,Rales,Wheezing

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Assessment Techniques MallampatiScore MouthOpening• 3fingersbetweenincisors
ThyromentalDistance• >6cm=“3fingers”• Predictslaryngoscopicgeometry
AdequateNeckExtension• Assumingnotrauma
Evaluateforobstruction

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Mallampati Classification
I 2
3 4http://www.bartleby.com/107/illus1201.html

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Techniques Patency Maneuvers
Fingersweepoforopharynx
Academy of Health Sciences, United States Army Medical Department

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Techniques Patency Maneuvers
Heimlichmaneuverorchestthrusts
Rama(Wikipedia)

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Techniques Patency Maneuvers
Headtiltwithchinlift,orjaw-thrustmaneuver
SourceUndetermined
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Techniques Patency Maneuvers
Suctioningofupperairway
www.anesth.uiowa.edu/

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Oral Airway
Preventstonguefromoccludingairway Requiresabsentgagreflex Canbeusedasabiteblock Placecarefullyoverthetongue Ifpatientcantolerateoralairway,theylikelyneedtobeintubated

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Nasal Airway Device
Pliable Goodforsonorouspatients Lubricatetip;placeinmostpatentnostril Gointheinferiorandmedialportionofthenostrilandhorizontaltothehardpalate

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Bag-Valve-Mask Ventilation Very important skill to know
May provide temporary or definitive airway management.
One person - importance of a good seal.
Two person technique more effective.
In EMS setting may be as useful as endotracheal intubation.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Bag-Valve-Mask Ventilation
SourceUndetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Oral Endotracheal Intubation The BASICS:
• Use of laryngoscope to provide visualization.
• Passage of a plastic air conduit through the vocal cords and into the trachea.
Very difficult (and inadvisable) to do without pharmacological aids • Except in patients who are in cardiorespiratory
arrest, deeply comatose, or neonates.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Learn the equipment
SourceUndetermined SourceUndetermined
SourceUndeterminedSourceUndetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Equipment and Preparation
Laryngoscope handle and blade
Endotracheal tube
Bag-Valve-Mask
Suction - large bore
Meds and good IV line
Monitor, O2 sat

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Laryngoscope Blades Miller Blade - (straight blade) -lifts the epiglottis. MacIntosh Blade (curved) - placed in vallecula
and tilts epiglottis anteriorly.
Kalumet(Wikipedia)Ignis(Wikipedia)

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Laryngoscope Blades AgeandBladeSizeandType:• PrematureInfant-0Miller• TermInfant-1Miller• UptoAge2-2MillerorMac• Olderchildren(age>12),smalladults-3MillerorMac• Largeradults-4MillerorMac

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Tube Sizing Premature - 2.5 mm
Term - 3.0 mm
Age 6 months - 3.5 mm
Age 1 year - 4.0 mm
Formula: 4 + age/4 = tube size
“Age 8 is enough for a cuff”

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Intubation The Mechanics
Adequate bed height and patient positioning.
Open mouth and remove dentures.
Hold blade in left hand!
Sweep tongue from right to left.
Avoid the teeth.
Airway can be externally manipulated by person holding cricoid pressure. BURP maneuver.
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
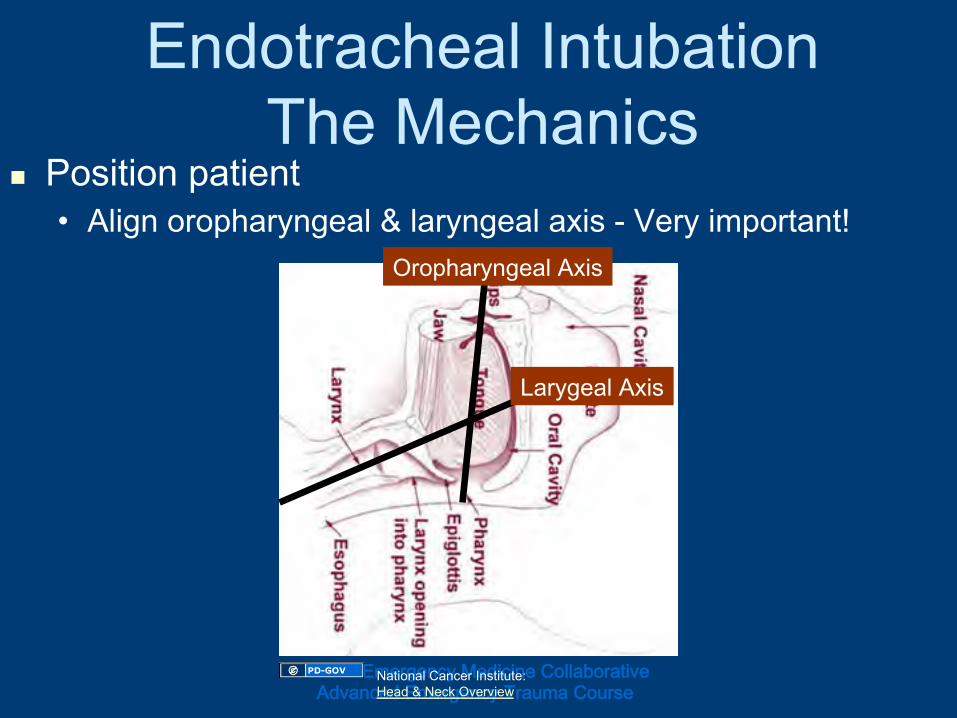
Endotracheal Intubation The Mechanics
Position patient • Align oropharyngeal & laryngeal axis - Very important!
LarygealAxis
OropharyngealAxis
NationalCancerInstitute:Head&NeckOverview

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Intubation The Mechanics
Scissormouth BladeLhand
SourceUndetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Intubation The Mechanics
Sweeptongue Avoidteeth
SourceUndetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Intubation The Mechanics
Elevateepiglottis-liftinaxisoflaryngoscopehandle.
SourceUndetermined
http://www.cpp.usmc.mil/schools/fmss/_borders/intub8.jpg
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
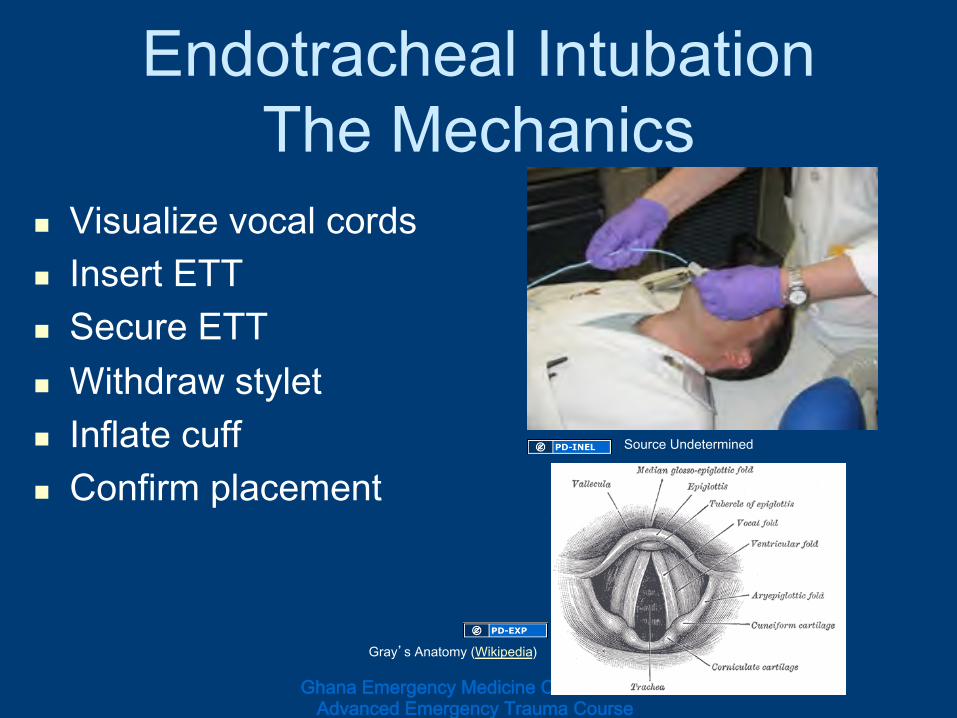
Endotracheal Intubation The Mechanics
Visualizevocalcords InsertETT SecureETT Withdrawstylet Inflatecuff Confirmplacement
Gray’sAnatomy(Wikipedia)
SourceUndetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Endotracheal Intubation The Mechanics
KEY POINTS Position the patient correctly
When you see the cords, do not look away; have assistant give you everything you need.
Place the tube, remove stylet, inflate cuff.
Hold the tube until secured.
Tube depth in centimeters = Tube number x 3; or F - 21 cm, M - 23 cm at mouth corner.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Rapid Sequence Induction (RSI) Endotracheal Intubation
Use of drugs to improve intubating conditions by eliminating patient resistance and providing muscular relaxation.
Co-administration of a potent sedative and a neuromuscular blocking agent.
Given in rapid sequence to decrease time of unprotected airway.
Assumes full stomach in emergency patient.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Induction Agents Etomidate
0.2-0.3 mg/kg IV
Decreases intracranial pressure and intragastric pressure.
Minimal hemodynamic effects.
Can lead to adrenal suppression after one dose - unclear clinical significance.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Induction Agents Ketamine
1-2 mg/kg IV Dissociative anesthetic, like PCP.
Catecholamine release leads to increased BP and HR and bronchodilation, increased secretions.
Good for asthma, bad for head injury or MI.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
RSI Paralytics - Succinylcholine 1.5 - 2 mg/kg IV Fasciculation and skeletal muscle paralysis
within 45 seconds. Potential side effects
Bradyarrhythmias Increased IG, IO, and IC pressure Increased potassium Malignant hyperthermia Prolonged paralysis.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Depolarizing – Binds to Nm receptor, opens Na channel causing depolarization.
Non-Depolarizing – Competes with Ach, does not activate Nm receptor
http://commons.wikimedia.org/wiki/File:Synapse_diag4.png

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
RSI Paralytics Non-Depolarizing Agents
E.g. Rocuronium 1 mg/kg IV Good choice if there is a clear
contraindication to succinylcholine. Non-depolarizing agents are usually
used to maintain paralysis rather than as RSI agents.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
RSI Pretreatment Medications Lidocaine 1.5 mg/kg IV
Head injury and MI - recommended, not essential
Fentanyl 3 mcg/kg IV Head injury and MI. - recommended, not
essential.
Atropine 0.02 mg/kg IV for kids < 5 y/o Decrease succinlycholine-related bradycardia.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
RSI - the Seven P’s Prepare t-10
Preoxygenate t-5
Pretreatment t-3
Paralysis after sedation
Protect - Sellick’s maneuver
Place tube
Post-intubation check

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Confirming Endotracheal Tube Placement
See tube go through cords. Watch for tube condensation.
Pulse oximetry and end tidal CO2 detector. Do not rely on capnometry in arrest/shock states
Auscultate stomach and lungs.
Chest X-ray for tube positioning in trachea.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Success Rates Method Intubations (%) Success Rate
RSI 67 99%
Oral, sedation 7 92%
Oral, no meds 18 93%
Nasotracheal 7 86%
from the NEAR II study (National Emergency Airway Registry)

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Alternatives to Standard Endotracheal Intubation
Nasotracheal intubation
Intubating laryngeal mask airway (LMA)
Transtracheal Jet Ventilation (TTJV)
Others Retrograde, Digital, Lighted stylet, Fiberoptic-assisted.
Cricothyrotomy or Tracheostomy
ALL require advanced/additional training
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Nasotracheal Intubation Pt. cooperative and upright.
Good for oxygenation and ventilation problems - CHF, asthma, COPD
Anesthetize nose, lubricate tube, use tube 0.5 - 1 mm smaller than for oral use
Most patent nare, go medial and inferior, listen, advance - timing and rhythm are key.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Nasotracheal Intubation
faculty.washington.edu/pcolley/
http://commons.wikimedia.org/wiki/File:Chapter5figure69b-nasotracheal_intubation.jpg

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cricothyrotomy - Indications
Definitiveairwaycontrolwhennonsurgicalmethodsfail.
Upperairwayobstructionduetotrauma,edema,foreignbody,infection.
Source Undetermined

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cricothyrotomy Relative Contraindications
Age < 8 years old Bleeding disorder
Infections of neck or airway
Transection of airway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cricothyrotomy - Procedure Locate cricothyroid membrane.
Vertical skin incision 3-4 cm.
Stabilize thyroid cartilage with hand or hook.
Horizontal incision through inferior portion of membrane.
Insert instrument to widen hole.
Place tube, inflate cuff, secure.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cricothyrotomy - Procedure
www.theairwaysite.com
www.theairwaysite.com
www.theairwaysite.com
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Cricothyrotomy: Complications Early
Bleeding
Trauma to adjacent structures
Tube misplacement.
Later Infection
Subglottic stenosis.
Loss of the airway.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Pediatric Airway Management Airway smaller.
U-shaped floppy epiglottis.
Larynx more anterior and cephalad.
Narrowest point is cricoid cartilage.

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Pediatric Airway Management Use Broselow-Luten tape.
“At age 2, #2 (Mac or Miller).
“Below age 5, atropinize.”
“8 is enough for cut and cuff.”

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Case #1 Analcohol-intoxicatedmanhadaseizureinthepark.
Vitalsigns:• 140/100,P120,R18,Pulseox-93%,roomair.
Exam:Nosignsoftrauma;intactgagreflex;maceratedtongue;sonorousrespirations;clearlungs;non-focalneuroexam.
Whatistheappropriateairwaymanagement?

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Management
Options• Patencymaneuvers• Non-invasiveventilation• Endotrachealintubationwithorwithoutinductionandparalyticagents• Nasotrachealintubation• Surgicalairway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Case #2 78y.o.male,historyofMI,awakensSOB.BroughtbywifetoED.
Vitalsigns:• 210/120,P120,R32,Pulseox-88%,roomair.
Exam:• Diaphoretic,restless,confused,dusky,lungsverywet,positiveJVD.S3present.
Whatistheappropriateairwaymanagement?

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Management
Options• Patencymaneuvers• Non-invasiveventilation• Endotrachealintubationwithorwithoutinductionandparalyticagents• Nasotrachealintubation• Surgicalairway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Case #3 A36y.o.womanisbroughttoEDbyherhusbandafteringesting90Elaviltablets,“Downers”,Paxiltablets,andEtOHinasuicideattempt.
Vitalsigns:• 90/60,P136,R16,Pulseox-96%,roomair.
Exam:Uncooperative,somewhatdrowsy,hyperreflexic,lungsclear.
Whatistheappropriateairwaymanagement?

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Management
Options• Patencymaneuvers• Non-invasiveventilation• Endotrachealintubationwithorwithoutinductionandparalyticagents• Nasotrachealintubation• Surgicalairway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Airway Management Case #4 A3y.o.girlwasrunningwithasharptoyinhermouthandfell.Sustainedoropharyngealtrauma.
Vitalsigns:• 90/65,P145,R36,Pulseox-89%,roomair.
Exam:• Crying,child,somewhatcyanotic,drooling,hasstridor,obvioussubmentaledema.Tracheamidline.
Whatistheappropriateairwaymanagement?

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Emergency Airway Management
Options• Patencymaneuvers• Non-invasiveventilation• Endotrachealintubationwithorwithoutinductionandparalyticagents• Nasotrachealintubation• Surgicalairway

GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Special thanks to Richard Taylor, MD Brian Zink, MD
For developing slides and content For the UM ED M4 Airway Lecture
GhanaEmergencyMedicineCollaborativeAdvancedEmergencyTraumaCourse
Questions?
Dkscully(flickr)