australasian veterinary dermatology advisory panel …
TRANSCRIPT

ADVANCING VETERINARY PRACTICE IN DERMATOLOGY Summary guidelines for the diagnosis and management of pruritus in dogs
FOR HEALTHY SKIN
AUSTRALASIAN VETERINARY DERMATOLOGY ADVISORY PANEL (AVDAP)
SECOND EDITION

AUSTRALASIAN VETERINARY DERMATOLOGY ADVISORY PANEL
THE PANEL MEMBERS INCLUDE:
DR MANDY BURROWS BSc, BVMS, MANZCVS, FANZCVS
Associate Professor in Small Animal Medicine (Dermatology); Registered Specialist in Veterinary Dermatology, Perth WA
DR SAMANTHA CROTHERS BSc, BVMS, DipACVD
Specialist in Veterinary Dermatology Melbourne, VIC
Developed by the
DR PETER HILL (AVDAP Chair) BVSc (Hons), PhD, DVD DipACVD, Dip ECVD, MANZCVS
Professor of Veterinary Dermatology and Immunology, Adelaide, SA
DR MIKE SHIPSTONE BVSc (Hons), MACVSc, FACVSc, DipACVD
Specialist in Veterinary Dermatology Brisbane, QLD
DR REBECCA TRAUB BSc (Vet. Biol.), BVMS (Hons), PhD
Professor in Veterinary Parasitology, University of Melbourne, VIC
DR LINDA VOGELNEST BVSc (Hons), MANZCVS, FANZCVS
Specialist in Veterinary Dermatology Sydney, NSW
> Page 4 of full guidelines

CONTENTS
ABOUT THIS SUMMARY 5
Guideline objectives 5
Guideline website 5
INTRODUCTION TO PRURITUS 6
Overview of diagnosis and management 7
SECTION A: DIAGNOSTIC APPROACH
INITIAL ASSESSMENT OF THE PRURITIC DOG
Step 1: Take history and identify chief complaint 8
Step 2: Conduct a physical examination 9
Step 3: Use diagnostic tests to rule in/out differential diagnosis 12
PERFORMING AND INTERPRETING DIAGNOSTIC TESTS
Outline of diagnostic procedures for infection-based causes 14
Outline of diagnostic procedures for allergy-based causes 15
SECTION B: THERAPEUTIC APPROACH
MANAGEMENT OF PRURITUS 16
Acknowledging and managing owners’ expectations 16
Managing the skin condition 17
MONITORING PRURITUS TREATMENT AND PROGRESS 18
WHEN TO OFFER REFERRAL TO A DERMATOLOGIST 19
DOWNLOAD THE FULL GUIDELINES AT: www.zoetis.co.nz/derm
3AVDAP Summary Guidelines

4 AVDAP Summary Guidelines

ABOUT THIS SUMMARY
This summary is a companion to the full AVDAP guidelines for the diagnosis and management of pruritus in dogs. It provides an overview of the key elements related to pruritus in dogs including diagnostic tests and their interpretation, as well as the approaches for managing the condition.
More in-depth information on each topic can be found in the corresponding section of the full guidelines. Page numbers have been provided to facilitate navigation to the relevant section of the guidelines.
GUIDELINE OBJECTIVES
The purpose of these guidelines is to assist veterinary practitioners in the diagnosis and effective management of the pruritic dog with the aim of helping dogs and their owners live a better quality of life.
The AVDAP guidelines provides evidence- and expert opinion-based guidance translated into practical advice on the most effective strategies in the diagnosis and management of pruritus in dogs
DOWNLOAD THE FULL GUIDELINES AT: www.zoetis.co.nz/derm
GUIDELINE WEBSITE
5AVDAP Summary Guidelines

INTRODUCTION TO PRURITUS
Pruritus is defined as an “unpleasant sensation that triggers a desire to scratch.” 1
Itch, like pain, is one of the body’s basic defence mechanisms that signals a potential hazard.
Itch can manifest as an acute condition, or it can develop into a chronic, self-perpetuating pathologic state that requires a thorough diagnostic work-up to identify the underlying cause so that the most appropriate management strategy can be implemented.
> Page 9 of full guidelines
1. Ikoma A, Cevikbas F, Kempkes C, Steinhoff M. Anatomy and neurophysiology of pruritus, Semin Cutan Med Surg. 2011;30:64-70
Acutely pruritic patients should be effectively worked up and managed. Failure to do so may result in chronic allergic dermatitis that can be more time-consuming and costly to manage.
Chronic Atopic DermatitisImage courtesy of Peter Hill
6 AVDAP Summary Guidelines

Chronic Atopic DermatitisImage courtesy of Peter Hill
OVERVIEW OF DIAGNOSIS AND MANAGEMENT > Page 10 of full guidelines
Diagnosis and management of the pruritic dog can be divided into two components: (A) the diagnostic approach and (B) the therapeutic approach.
B: THERAPEUTIC APPROACH
STRATEGIC USE OF ANTI-PRURITIC THERAPY WHERE APPROPRIATEMay occur concurrently with diagnostic approach
IF NO RESPONSE TO THERAPY OR IT LOOKS UNUSUAL: BIOPSY, CULTURE AND/OR REFER
• Topical +/- systemic
MANAGE FLARE FACTORS E.G. PARASITES, PYODERMA, DIETARY INDISCRETION
AVOIDANCE OF DIETARY OR CONTACT ALLERGENS
LONG-TERM ANTI-PRURITICS FOR ATOPIC DERMATITIS
• Oclacitinib • Lokivetmab • Cyclosporin • Glucocorticoids
ALLERGEN SPECIFIC IMMUNOTHERAPY
ADJUNCTIVE TREATMENTS
MANAGE SKIN BARRIER (DIET, TOPICAL)
• e.g. medicated washes, systemic anti-fungal treatment.
ANTI-FUNGALS
PHYSICAL EXAM
PRIORITISE DIFFERENTIAL DIAGNOSES LIST AND PLAN DIAGNOSTIC TESTS
HISTORY• Breed, age of onset, seasonality, environment, previous medication and response, current flea control etc.
A: DIAGNOSTIC APPROACH
ALLERGIES Food, Atopic Dermatitis, Contact
If parasites and infection have been ruled out,and the skin condition remains, then Allergic
Dermatitis should be investigated
1 PARASITES
• Fleas• Demodex mite• Sarcoptes mite• Ear mites
Diagnostic tests to consider:• Flea comb• Wet paper• Skin scrape — superficial — deep• Trichogram• Squeeze tape impression• Flea & Sarcoptes
therapeutic trial
INFECTION
• Bacteria • Yeast
Diagnostic tests to consider:• Adhesive tape impression• Cotton bud• Glass slide impression
2
3
ATOPIC DERMATITIS
FOOD CONTACT
Diagnostic tests to consider:• Dietary
exclusion trial
Diagnostic tests to consider:• Intra-dermal
testing• Serology
Diagnostic tests to consider:• Avoidance and
re-challenge• Patch test
ANTIBIOTICSFLEA AND MITE TREATMENT AND
PREVENTION
7AVDAP Summary Guidelines

INITIAL ASSESSMENT OF THE PRURITIC DOG> Page 13 of full guidelines
The 3 key steps to diagnosis:
Step 1: Take history and identify owner’s chief complaintStep 2: Conduct a thorough physical examinationStep 3: Use diagnostic tests to rule in/out differential diagnoses
STEP 1: TAKE HISTORY AND IDENTIFY CHIEF COMPLAINT
USE A DERMATOLOGY-BASED QUESTIONNAIRE TO FACILITATE INITIAL CONSULTATION
Refer to www.zoetis.co.nz/derm for an example and printable version of a questionnaire for general practice use
Questionnaires enable efficient gathering of detailed information, especially if skin cases are chronic or recurrent. Ideally these should be completed prior to the consultation to ease time pressures.
USE A SHORTER SET OF QUESTIONS IF TIME IS LIMITED
These questions capture the minimal historical information required to assist with an accurate diagnosis:
Question Areas of assessment: Specific questions for owner:
1Is the dog pruritic? Ask individually about multiple behaviours that owners may not interpret as itch
• Does your dog lick, bite, chew, rub, roll, scratch or scoot?
2 Age of onset/duration of itch • At what age did you first notice the itch/how long has your dog been itchy?
3 Assess distribution of itch • Where on the body is the itch?
4 Pattern of itch • Is the itch continuous, seasonal or intermittent?
5 Development of condition • What came first? The itch or rash/skin changes?
6 Medications used for itch and response to treatment
• Have you given any medications for itch or any other conditions?
• Did they resolve, reduce or make no change to the itch?
SECTION A: DIAGNOSTIC APPROACH
8 AVDAP Summary Guidelines

ASSESSMENT OF COAT QUALITY AND GENERAL BODY CONDITION
• Examine hair coat for density
• Screen body for signs of systemic disease
IDENTIFY ANY LESIONS OR PARASITES
• Look for grossly visible ectoparasites
• Clip hair to visualise subtle lesions
• Use a magnifying glass to check for small lesions
• Assess skin sensitivity with digital stimulation
• Check for abnormal odours
• Characterise and record skin lesions
STEP 2: CONDUCT A PHYSICAL EXAMINATION
Refer to page 15 of the full guidelines for more details on how to conduct the physical assessment and to understand how lesion distribution patterns can help in the diagnosis of pruritus.
MAJOR LESIONS OBSERVED IN A PRURITIC DOG > Page 17 of full guidelines
Changes in skin colour - erythema, hyperpigmentation
Rashes - erythematous macules, papules, pustules and staphylococcal rings
Alopecia - spontaneous or secondary to pruritus
Excessive scaling - scale, seborrhoea, epidermal collarette
Changes in skin thickness – lichenification, cutaneous atrophy
Defects in skin integrity - self-induced (excoriations, erosions, ulcers) or spontaneous (furunculosis)
There are three major aims when performing a dermatological examination. These are to:
1. Assess coat quality and general body condition
2. Identify any lesions or parasites e.g. fleas that are present
3. Determine distribution of lesions
9AVDAP Summary Guidelines
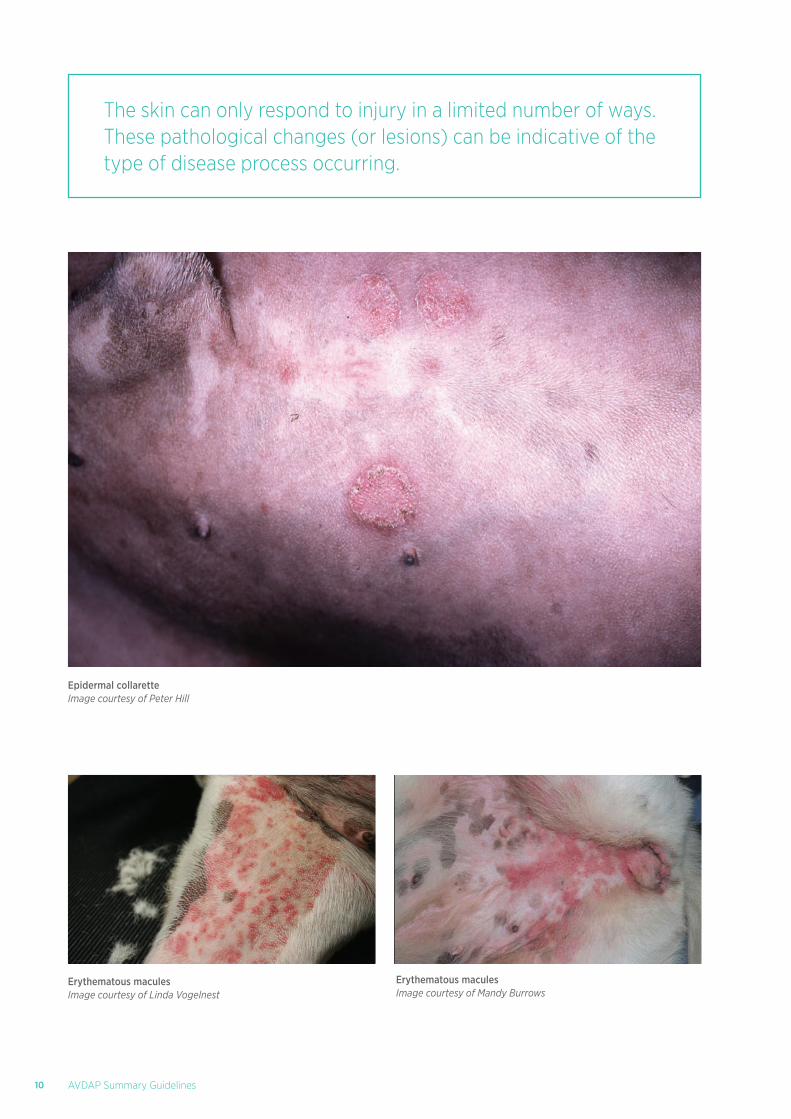
The skin can only respond to injury in a limited number of ways. These pathological changes (or lesions) can be indicative of the type of disease process occurring.
Erythematous macules Image courtesy of Linda Vogelnest
Epidermal collaretteImage courtesy of Peter Hill
Erythematous macules Image courtesy of Mandy Burrows
10 AVDAP Summary Guidelines

Distribution of skin lesions is one of the most important clinical features used to prioritise the differential diagnosis list
DETERMINE DISTRIBUTION OF LESIONS > Page 27 of full guidelines
• A lesion distribution diagram is quick and easy to perform
• Provides a visual reference that is useful for monitoring progress
• Valuable when cases are seen by more than one clinician
An example of a completed lesion distribution diagram is shown below:
11AVDAP Summary Guidelines

STEP 3: USE DIAGNOSTIC TESTS TO RULE IN/OUT DIFFERENTIAL DIAGNOSES > Page 37 of full guidelines
PRIORITISATION OF THE DIFFERENTIAL DIAGNOSES
Based on the information derived from the history and physical examination the differential diagnosis list can be prioritised.
HISTORICAL FEATURES
Some distinctive/important historical features of common pruritic diseases in dogs will aid formulation of a prioritised differential list:
• Signalment
– All of the differential diagnoses for pruritus can be seen in young animals. If the pruritus commences in middle or older age, parasitic or infectious causes are more likely
– Breed predispositions: recognised for atopic dermatitis, and some infections (e.g. Malassezia dermatitis) – check predispositions for the breed
• Pattern of pruritus
– Sudden onset of severe continuous pruritus: consider Sarcoptes, and flea allergy if pruritus focused on back half of body
– Intermittent or waxing/waning pruritus: most consistent with seasonal parasitoses or atopic dermatitis
• Lesions
– Lesions before itch: exclude parasitic and infectious causes first
• Response to previous medications
– Complete resolution of skin condition with oclacitinib (Apoquel®) or glucocorticoids (anti-inflammatory doses): most consistent with allergy
– Partial resolution of pruritus with oclacitinib (Apoquel®) or glucocorticoids (anti-inflammatory doses): non-specific
– Poor response to oclacitinib (Apoquel®) or glucocorticoids: exclude demodicosis, scabies and infections
PHYSICAL EXAMINATION FEATURES
Important physical examination features in pruritic dogs that provide helpful clues to aid formulation of an accurate prioritised differential list, include:
• Lesions:
– Papules: exclude parasites, bacterial pyoderma, flea allergy
– Pustules/epidermal collarettes: bacterial pyoderma likely
– Alopecia
› Complete, well-demarcated foci/regions: exclude demodicosis, pyoderma
› Patchy/consistent with self-trauma: any pruritic disease
› Partial diffuse/moth-eaten: exclude bacterial pyoderma/folliculitis
12 AVDAP Summary Guidelines

PustulesImage courtesy of Mandy Burrows
Crusted papules and pustulesImage courtesy of Peter Hill
– Lichenification/hyperpigmentation: chronic, non-specific change
– Coat changes (dull, coarse hair coat/poor regrowth after clipping): common with extended glucocorticoid therapy
• Lesion Distribution (once infections excluded):
– Face, ears, paws, axillae, ventral abdomen: atopic dermatitis, food allergy, Malassezia dermatitis, trombicula/Ixodes ticks
– Otitis externa/pinnal lesions: atopic dermatitis, food allergy, scabies
– Caudal trunk, caudal/medial hind limbs, ventral abdomen: flea allergy
– Contact regions (sparsely haired muzzle, feet, ventrum): contact allergy, atopic dermatitis, food allergy
Refer to page 37 of the full guidelines for a list of the major and less common differential diagnoses.
13AVDAP Summary Guidelines

PERFORMING AND INTERPRETING DIAGNOSTIC TESTS
Formulating a prioritised differential list prior to reaching for diagnostic tests will guide the most important tests to perform for each patient.
> Page 41 of full guidelines
Refer to page 41 of the full guidelines for detailed instructions on the differential diagnosis and diagnostic work-up using these techniques, including the culturing of bacterial and fungal samples.
Infection/Infestation Indications
Coat combing
page 44 of full guidelinesFor identifying parasites: fleas, Cheyletiella, lice, trombiculid mites
Adhesive tape impression
page 45 of full guidelines
For superficial bacterial pyoderma and Malassezia dermatitis; can also be diagnostic for dermatophytosis and surface dwelling mites (e.g. Cheyletiella), reveal inflammatory cell types (e.g. eosinophils to support parasitic or allergic disease), and may support diagnosis of immune-mediated diseases (e.g. acantholytic cells in Pemphigus foliaceus)
Glass slide impression/ear smears for microbes
page 52 of full guidelines
For sampling erosive to ulcerative skin lesions, gently punctured pustules, and for ear canal cytology; helpful to evaluate for infectious organisms (bacteria, yeast, other fungi), inflammatory cells (neutrophils, eosinophils, macrophages) and neoplastic cells
Skin-scraping – superficial
page 54 of full guidelinesFor superficial ectoparasites, including Sarcoptes, Otodectes, environmental mites (e.g. trombiculids)
Skin-scraping – deep
page 56 of full guidelines
For demodicosis due to Demodex canis (more typical follicular mite), or Demodex injai (long-tailed mite)
Squeeze-tape impression
page 58 of full guidelines
Useful whenever Demodex is suspected, and for monitoring response to therapy
Particularly useful for difficult sites e.g. around eyes, face, feet
Ear smear for otic parasites
page 59 of full guidelines
When there is evidence of otitis or pruritus of the ears and/or adjacent skin, especially in younger dogs or when exposure to young dogs or cats, and with dark granular ear discharge
Trichogram
page 60 of full guidelines
Allows evaluation for infectious agents (Demodex mites) and causes of hair loss (trauma or shedding)
OUTLINE OF DIAGNOSTIC PROCEDURES FOR INFECTION-BASED CAUSES
14 AVDAP Summary Guidelines

Food allergies Diagnostic approach
Food-elimination diet (for up to 8 weeks)
page 64 of full guidelines
Communicate with the owner the importance of this diagnostic step, including the length of the trial, how important it is to strictly adhere to the diet and how the pruritus will be managed in the interim
Establish what food the dog has been exposed to previously
Select an appropriate diet containing novel protein and carbohydrate (ones which the dog has never previously eaten)
Treat the dog with antipruritics. Oclacitinib (Apoquel®) or prednisolone may be considered at the start of the diet trial depending on the severity of the pruritus
Rechallenge with the original diet for up to two weeks whilst not receiving antipruritics to confirm diagnosis
Atopic dermatitis Diagnostic approach
Intradermal allergy test
page 67 of full guidelines
Tests presence of hypersensitivity to various environmental allergens based on skin reactivity
IgE serology test
page 68 of full guidelines
Requires a blood sample to be taken and sent off to an appropriate laboratory
The serum is assayed for allergen-specific IgE
Contact dermatitis Diagnostic approach
Contact avoidance trial (10-day duration)
page 70 of full guidelines
Owner advised to restrict the animal’s access to certain areas. This may involve avoidance of outdoor areas where plants are present (grass, trees, weeds, poison ivy, poison oak, Tradescantia (Wandering jew), dandelion leaves, cedar wood)
OUTLINE OF DIAGNOSTIC PROCEDURES FOR ALLERGY-BASED CAUSES
15AVDAP Summary Guidelines

MANAGEMENT OF PRURITUS> Page 73 of full guidelines
The role of the veterinarian is to provide rapid, symptomatic relief of the pruritus for the dog, to determine the underlying cause, and to instigate appropriate management.
ACKNOWLEDGING AND MANAGING OWNERS’ EXPECTATIONS
Poor communication is one of the main reasons why owners seek a second opinion. The importance of effective communication should not be underestimated
SECTION B: THERAPEUTIC APPROACH
16 AVDAP Summary Guidelines

MANAGING THE SKIN CONDITION
Summary: management of pruritus
IDENTIFY TRIGGERS
• Implement flea and mite control
• Evaluate and treat for skin and ear infections
• Institute elimination diet if pruritus is continual/present all year round
• Identify allergens with allergy testing (note: oclacitinib and lokivetmab can be used to keep the patient comfortable whilst allergy testing is being undertaken)
TREAT PRURITUS (can be done in parallel with identifying the triggers)
• Oclacitinib, lokivetmab, cyclosporin, systemic glucocorticoids, +/- antihistamines
• Topical glucocorticoids
ALLERGEN SPECIFIC IMMUNOTHERAPY
BARRIER FUNCTION (can be done in parallel with identifying the triggers)
• Bathing
• Oral fatty acids
17AVDAP Summary Guidelines

MONITORING PRURITUS TREATMENT AND PROGRESSRefer to page 99 of the full guidelines for further details on monitoring approaches.
• Pruritus visual analogue scale score (PVAS) Indicates the severity of pruritus a dog is experiencing
• Photos of lesions A series of photographs comparing the dog's lesions to baseline photographs
prior to commencing management protocols
• Lesion distribution recording Whilst assessing the type of lesions, the clinician must also record their distribution
Overview of approaches to monitoring pruritus and associated lesions
Keeping the owner informed of progress helps get their buy-in to the management protocol. It is also important for the veterinarian to monitor progress and response to different therapies, which will enable the treatment protocol to be adapted for best results
18 AVDAP Summary Guidelines
WHEN TO OFFER REFERRAL TO A DERMATOLOGISTRefer to page 101 of the full guidelines for further details on when to refer to a dermatologist and tips for the referral process.
Reasons for referral to a veterinary dermatologist might include:
Intradermal testing and desensitisation in the management of atopic dermatitis
Diagnosis and management of a more complex skin disease
Judicious advice for a chronic common skin problem
Biopsy/histopathological evaluation
Management of otitis, including the use of video-otoscopy and advanced imaging of the bulla (e.g. CT or MRI)
Management of autoimmune or neoplastic skin diseases
If the owner requests a second opinion or referral
A veterinary dermatologist is specialised in diseases of the skin, ears, claws, mucous membranes, hair coat and subcutaneous tissues and their aetiology
19AVDAP Summary Guidelines

FULL GUIDELINES AVAILABLE FROM ZOETIS www.zoetis.co.nz/derm
Zoetis New Zealand Limited. Tel: 0800 963 847; www.zoetis.co.nz. APOQUEL and CYTOPOINT are registered trademarks of Zoetis. ACVM No. A10963, A11348, A11443, A11444 and A11445. RVM; Available only under Veterinary Authorisation. © 2018 Zoetis Inc. All rights reserved. June 18. MM-03546. CA2297