asthma & copd - hadassah€¦ · -decreasing morbidity and related costs . 5 ... asthma/copd...
TRANSCRIPT

1
Asthma & COPD
2
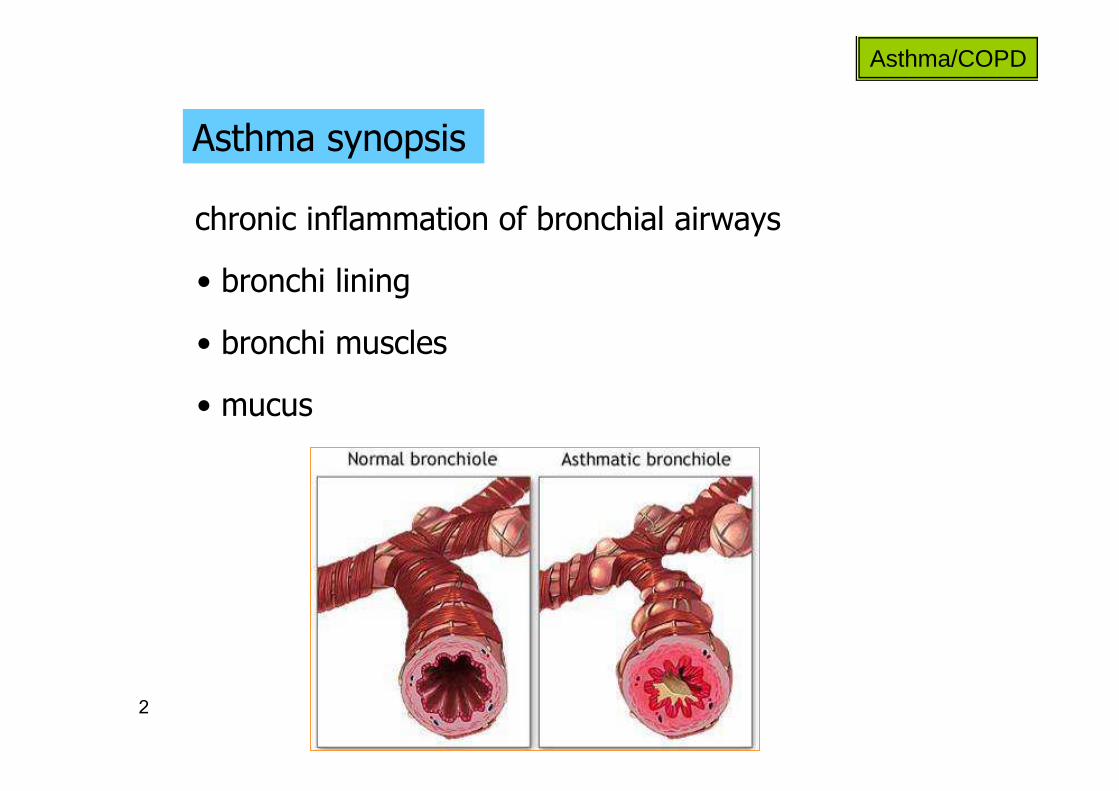
Asthma synopsis
Asthma/COPD
chronic inflammation of bronchial airways
• bronchi lining
• bronchi muscles
• mucus

3
Asthma synopsis
Asthma/COPD
acute broncho-constriction
cough
resolution?
shortness of breath
wheezing
chest tightness tachypnea

4
Asthma synopsis
Asthma/COPD
• generally not progressive
• remitting-relapsing
• M vs. M
• goals of therapy:
- relieving symptoms
- preventing recurrence
- preventing bronchial remodeling
- decreasing morbidity and related costs

5
Asthma pharmacotherapy
Asthma/COPD
oral vs. inhaled
inhalation Tx:
• main disadvantage -
• main advantage -

6
Asthma pharmacotherapy
Asthma/COPD
oral vs. inhaled

7
Asthma pharmacotherapy
Asthma/COPD
• corticosteroids
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• β2-adrenergic agonists

8
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists
9
Asthma pharmacotherapy
Asthma/COPD
Corticosteroids
inhaled corticosteroids (ICS) - 1st-line for:
rescue SABAs required> 2/wk
persistent asthma +
“ICS improve asthma control more effectively in both children and adults than … any other single, long-term control medication do.”[NHLBI guidelines 2007]
“ICS are currently the most effective anti-inflammatory medications for the treatment of persistent asthma [GINA report 2010]
10
Asthma pharmacotherapy
Asthma/COPD
ICS
• fluticasone (Flixotide®)
• budesonide (Budicort®)
• beclomethasone (Qvar®)

11
Asthma pharmacotherapy
Asthma/COPD
ICS - Mechanism:
• anti-inflammatory effect
• airway smooth muscle dilation

12
Asthma pharmacotherapy
Asthma/COPD
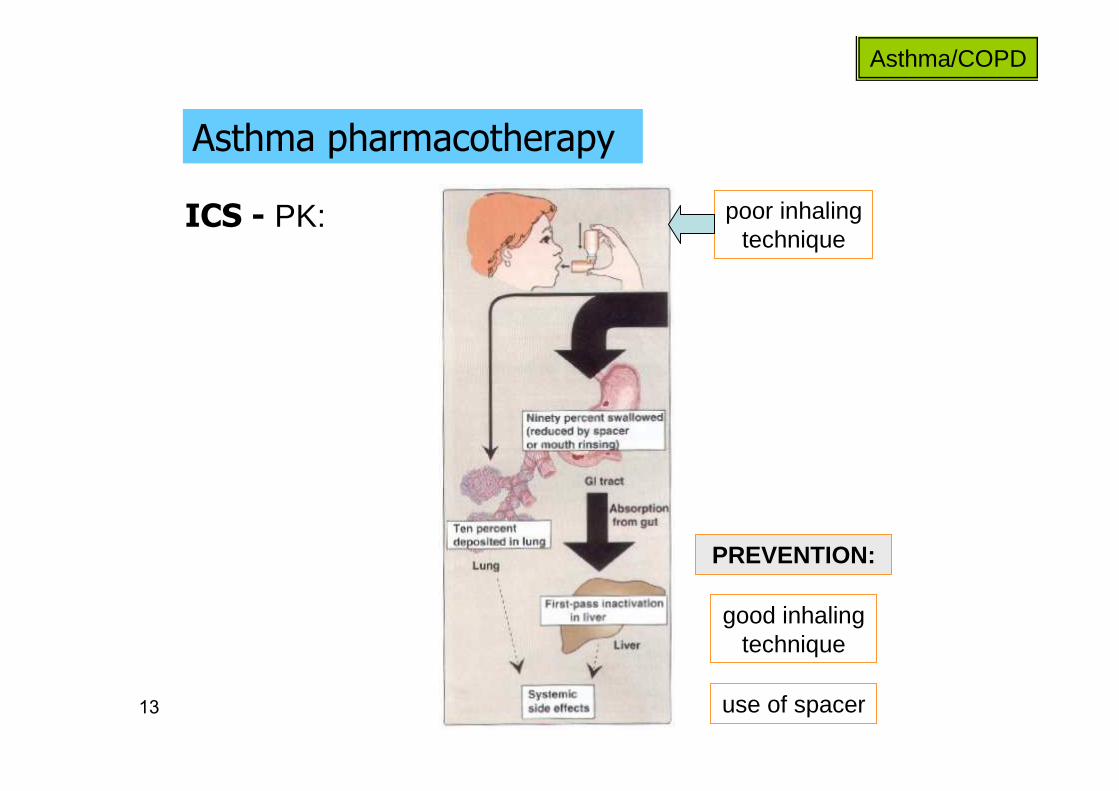
ICS - PK:
• fate of non-inhaled drug?
• proper inhalation reduces systemic exposure
• hepatic metabolism?
13
Asthma pharmacotherapy
Asthma/COPD
ICS - PK: poor inhaling technique
good inhaling technique
use of spacer
PREVENTION:
14
Asthma pharmacotherapy
Asthma/COPD
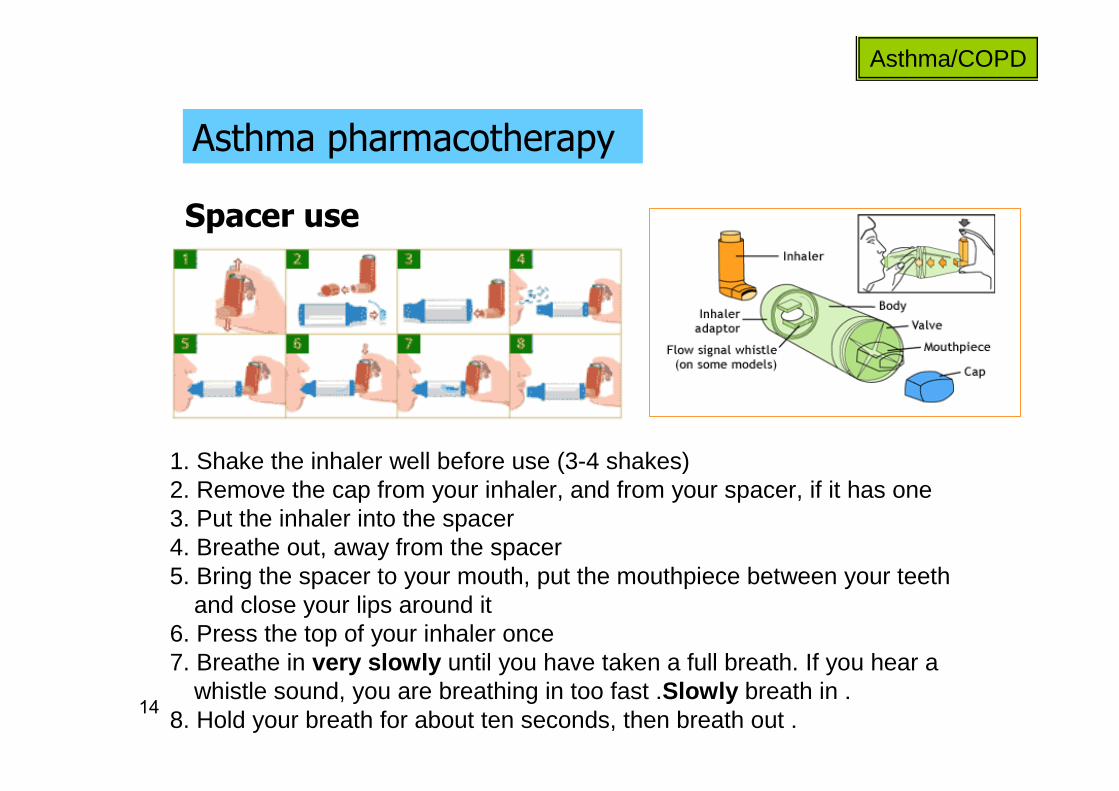
Spacer use
1. Shake the inhaler well before use (3-4 shakes)2. Remove the cap from your inhaler, and from your spacer, if it has one 3. Put the inhaler into the spacer 4. Breathe out, away from the spacer 5. Bring the spacer to your mouth, put the mouthpiece between your teeth
and close your lips around it 6. Press the top of your inhaler once 7. Breathe in very slowly until you have taken a full breath. If you hear a
whistle sound, you are breathing in too fast .Slowly breath in .8. Hold your breath for about ten seconds, then breath out .

15
Asthma pharmacotherapy
Asthma/COPD
ICS - benefits
• reduces airway hyper-responsiveness to various
bronchial stimulators
• oral-corticosteroids sparing
• the most effective Tx for long-term control of
asthma in children and adults
chronic use:

16
Asthma pharmacotherapy
Asthma/COPD
Systemic corticosteroids
• refractory cases may need PO support for certain periods
• long-term PO use rarely required
(persistent-severe uncontrolled asthma)
• upon improvement - tapering off over 1-2wk
• IV/PO: may be required in acute, severe exacerbations
(“status asthmaticus”)

17
Asthma pharmacotherapy
Asthma/COPD
Corticosteroids - general short-term ADEs
• increase appetite
• nervousness
• anxiety
• adrenal suppression
• growth retardation (children)
• insomnia
• Cushing’s syndrome
18
Asthma pharmacotherapy
Asthma/COPD
Corticosteroids - general long-term ADEs
• osteoporosis
• diabetes
• weight gain
• adrenal suppression
• growth retardation (children)
• peptic ulcers
• HTN
• immuno-suppression
• ↑↑↑↑ triglycerides, cholesterol
• infection masking
• skin thinning
• Cushing’s syndrome
• hypokalemia • more ……..

19
Asthma pharmacotherapy
Asthma/COPD
ICS - general ADEs
• overall, ADEs risk significantly reduced with ICS
• importance of . . . . . .
• local infections in mouth and pharynx
• long-term high-dose ICS:
- cataract (monitor)
- osteoporosis (monitor, consider Ca+++vit. D)
• cough
- easy bruising

20
Asthma pharmacotherapy
Asthma/COPD
Corticosteroids - DDIs
• ↓↓↓↓ by CYP-450 inducers (phenytoin, phenobarbital, rifampin)
• antacids (↓↓↓↓ oral absorption)
• ↓↓↓↓/↑↑↑↑ anticoagulant effect
• estrogen (↑↑↑↑ clearance)
• live-attenuated vaccines (immuno-suppression)
• hypokalemic drugs, digoxin
• generally insignificant with ICS

21
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists

22
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
• anti-inflammatory?
• bronchodilation?

23
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
short acting (SABAs):
• terbutaline (Bricalin®, Terbulin®)
• salbutamol=albuterol (Ventolin®)
• drugs of choice for mild asthma

24
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
short acting (SABAs):
• moderate duration (3-6hr)
• suitable for . . . .
• proper inhalation technique minimizes ADEs
• ADEs: tachycardia, hyperglycemia, hypokalemia, tremor
• rapid peak effect (0.5-2hr)

25
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
long acting (LABAs):
• formoterol (Foradil®, Oxis®)
• salmeterol (Serevent®)

26
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
long acting:
• long duration (12hr)
• acute vs. chronic use?
• ADEs generally similar to those of short-acting
• delayed peak effect (3-4hr)

27
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
Long-term safety concerns
Controversy has surrounded the use of beta-agonists in asthma
patients ever since their introduction over 50 years ago.
Numerous studies over many years have shown regular use of beta-agonists are associated with worsening of disease control.
Observational studies have consistently shown that the risk of life threatening and fatal asthma attacks increase with the use of
these medications .

28
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
Long-term safety concerns
SMART, Chest 2006;129:15-26.

29
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
Long-term safety concerns - SMART
• >6,100 centers
• >26,000 patients (of 60,000 intended)
• 28 weeks
• early termination

30
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
Long-term safety concerns - SMART

31
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
management:
• use LABAs in accordance with guidelines:
- not 1st-line!
- not for mild asthma!
- consider patient characteristics! (adherence, follow-up)
- not as monotherapy!
Long-term safety concerns - conflicting meta-analyses,

32
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
LABAs:
• Use of a LABA alone without use of a long-term asthma control medication, such as an inhaled corticosteroid, is contraindicated (absolutely advised against) in the treatment of asthma.
• Use of a LABA alone without use of a long-term asthma control medication, such as an inhaled corticosteroid, is contraindicated (absolutely advised against) in the treatment of asthma.
• LABAs should not be used in patients whose asthma is adequatelycontrolled on low or medium dose inhaled corticosteroids.• LABAs should not be used in patients whose asthma is adequatelycontrolled on low or medium dose inhaled corticosteroids.
June 2nd 2010

33
Asthma pharmacotherapy
Asthma/COPD
β2-adrenergic agonists
LABAs:
• LABAs should only be used as additional therapy for patients with asthma who are currently taking but are not adequately controlled on a long-term asthma control medication, such as an ICS.
• LABAs should only be used as additional therapy for patients with asthma who are currently taking but are not adequately controlled on a long-term asthma control medication, such as an ICS.
• Once asthma control is achieved and maintained, patients should be assessed at regular intervals and step down therapy should begin (e.g., discontinue LABA), if possible without loss of asthma control, and the patient should continue to be treated with a long-term asthma control medication, such as an ICS.
• Once asthma control is achieved and maintained, patients should be assessed at regular intervals and step down therapy should begin (e.g., discontinue LABA), if possible without loss of asthma control, and the patient should continue to be treated with a long-term asthma control medication, such as an ICS.
June 2nd 2010

34
Asthma pharmacotherapy
Asthma/COPD
Inhaled LABA-CS combinations
- salmeterol/fluticasone (Seretide®)
• for patients requiring both classes
- formoterol/budesonide (Symbicort®)
• adherence promotion

35
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists

36
Asthma pharmacotherapy
Asthma/COPD
Theophylline (Theotrim®, Theotard®)
• methylxanthine derivative
• structurally-related to caffeine
• originally isolated from tea (1888)
• administered orally (sustained release)
37
Asthma pharmacotherapy
Asthma/COPD
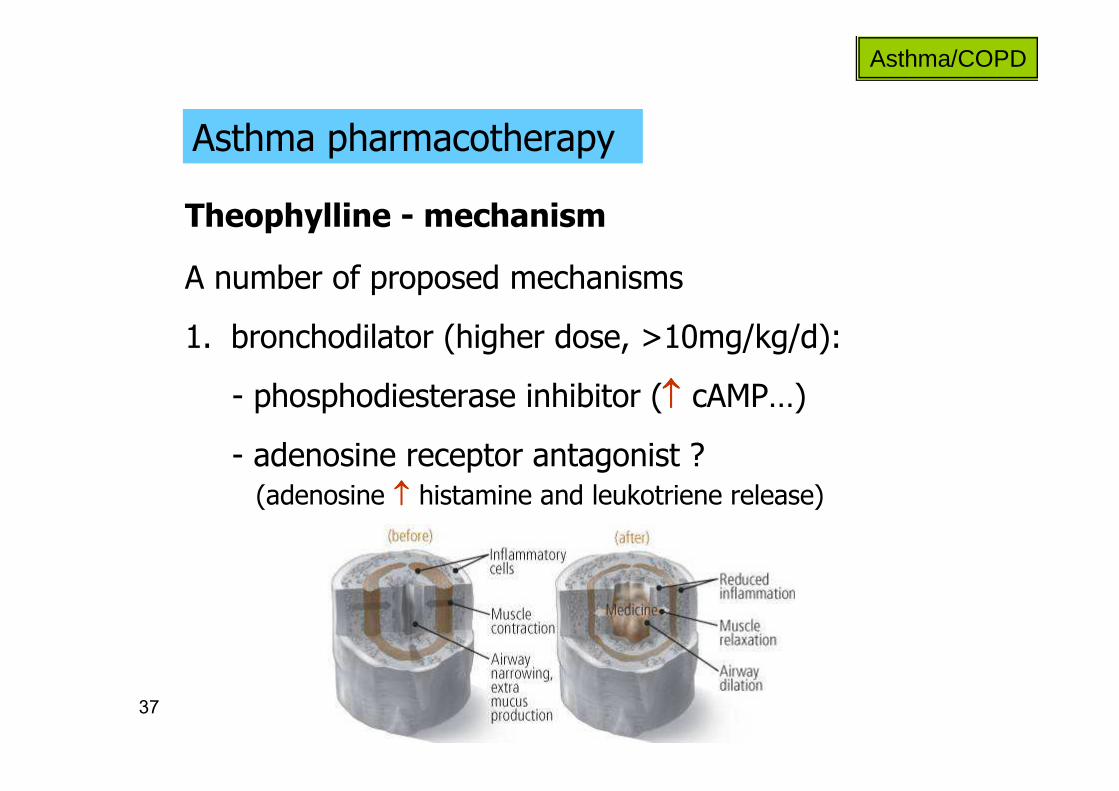
Theophylline - mechanism
A number of proposed mechanisms
- adenosine receptor antagonist ? (adenosine ↑↑↑↑ histamine and leukotriene release)
- phosphodiesterase inhibitor (↑↑↑↑ cAMP…)
1. bronchodilator (higher dose, >10mg/kg/d):

38
Asthma pharmacotherapy
Asthma/COPD
Theophylline - mechanism
A number of proposed mechanisms
2. anti-inflammatory (lower dose):
histone deacetylase
low-dose theophylline
active inflammatory gene transcription site
inflammatory process
acetylated core histones
inflammatory gene transcription
corticosteroids recruitment inhibition
increased activity

39
Asthma pharmacotherapy
Asthma/COPD
Theophylline - PK
• near-complete absorption
• significant hepatic metabolism
• mainly hepatic elimination (varies due to multiple effects)
• T1/2: adults - 8hr, smokers - 5hr, elderly - 12hr …

40
Asthma pharmacotherapy
Asthma/COPD
Theophylline - ADEs
adverse reactionsserum concentration
GI – nausea, vomiting, pain,CNS – insomnia, headache, agitation,
tremor, nervousness15-25 mcg/L
CV – tahcycardia, occasional PVBs25-35 mcg/L
VT, frequent PVBs, seizures>35 mcg/L
• narrow therapeutic index: target of 10-20 mcg/ml
• ADEs generally concentration-dependent:
TDM: 2hr post-oral dose

41
Asthma pharmacotherapy
Asthma/COPD
Theophylline - DDIs
↓↓↓↓ theophylline effect↑↑↑↑ theophylline effect
antacids (absorption), phenytoin, phenobarbital, rifampin, cigarette smoke, ritonavir, ketoconazole, more …..
cimetidine, corticosteroids, macrolides (erythromycin), quinolones (ciprofloxacin), CCBs, BBs, loop diuretics, more …

42
Asthma pharmacotherapy
Asthma/COPD
Theophylline - place in therapy
• decreasing use (ADEs, DDIs, better options); 3rd-line
• combination with ICS (steroid-sparing)
• refractory cases
• possible comeback as low-dose practice (anti-inflammatory)?

43
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists

44
Asthma pharmacotherapy
Asthma/COPD
Cromolyn/nedocromil
• “mast-cell stabilizers”

45
Asthma pharmacotherapy
Asthma/COPD
Cromolyn/nedocromil
• “mast-cell stabilizers”
↓↓↓↓ histamine (+ leukotriene) release
↓↓↓↓ inflammatory response
block mast-cell calcium channels
↓↓↓↓ mast cell degranulation

46
Asthma pharmacotherapy
Asthma/COPD
Cromolyn/nedocromil
“mast-cell stabilizers” for acute asthma attacks:
47
Asthma pharmacotherapy
Asthma/COPD
Cromolyn/nedocromil
• only effective as prophylaxis (ineffective for acute episodes)
• given as inhalation
• minimal systemic effects (local: irritation, bitter taste, dry mouth)
• useful in prevention of allergen-induced asthma
• safe in children, pregnancy
48
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists

49
Asthma pharmacotherapy
Asthma/COPD
Ipratropium (Atrovent®)
• anticholinergic agent (atropine derivative)
• blocks vagally-mediated contraction of smooth muscle
• peak effect: 1.5-2hr
• duration of effect: 4-6hr
• negligible ADEs (does not penetrate BBB)
• for preventive Tx
• rarely used for asthma

50
Asthma pharmacotherapy
Asthma/COPD
• β2-adrenergic agonists
• corticosteroids
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
51
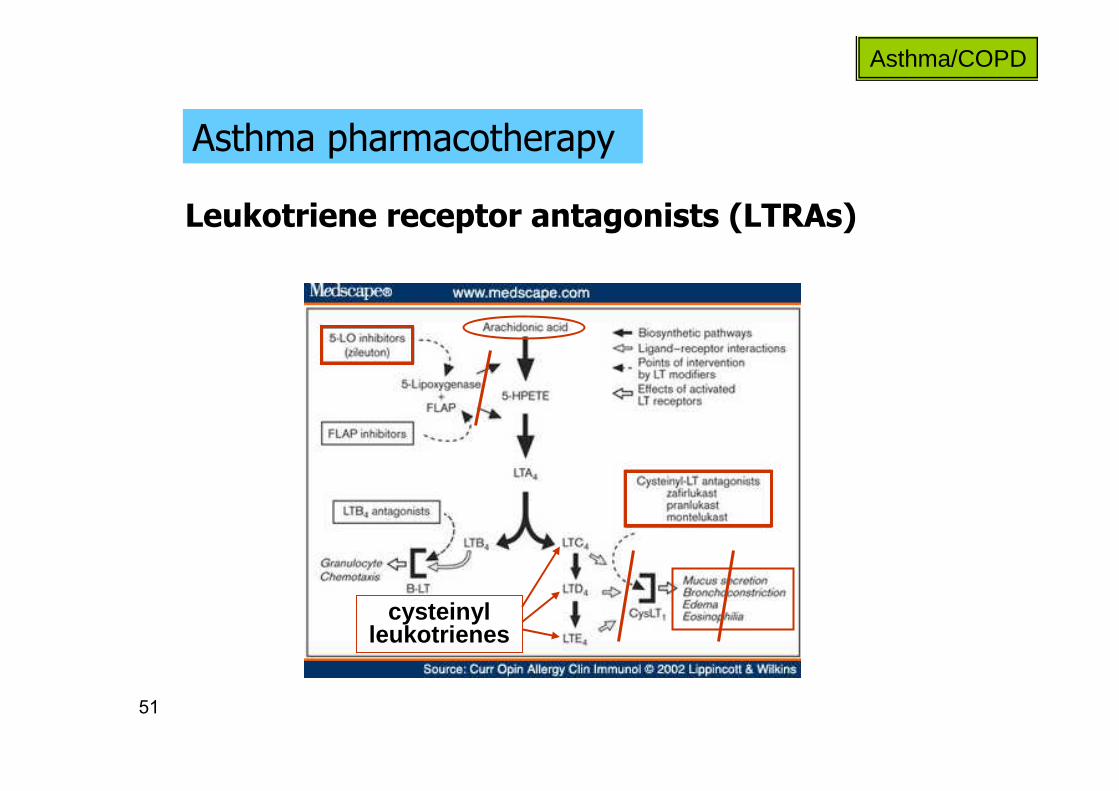
Asthma pharmacotherapy
Asthma/COPD
Leukotriene receptor antagonists (LTRAs)
cysteinyl leukotrienes

52
Asthma pharmacotherapy
Asthma/COPD
Leukotriene receptor antagonists (LTRAs)
montelukast (Singulair®)
• selective, reversible antagonist of cysteinyl-1 receptor
• for long-term control
• once-daily (evening) oral administration (chewable)
• extensive hepatic metabolism
• fecal excretion

53
Asthma pharmacotherapy
Asthma/COPD
Leukotriene receptor antagonists (LTRAs)
montelukast (Singulair®)
• selective, reversible antagonist of cysteinyl-1 receptor
• once-daily (evening) oral administration (chewable)
• extensive hepatic metabolism
• fecal excretion
• ADEs: headache (18%), impaired LFTs, dyspepsia, cough
• DDIs: ↓↓↓↓ 40% by phenobarbital (rifampin?)

54
Asthma pharmacotherapy
Asthma/COPD
LTRAs
montelukast (Singulair®)
• LABA/ICS sparing
• additional indication:
prophylaxis of exercise-induced bronchospasm
• for long-term control

55
Asthma pharmacotherapy
Asthma/COPD
• cromolyn/nedocromil
• ipratropium
• leukotriene modifiers
• omalizumab
• theophylline
• corticosteroids
• β2-adrenergic agonists

56
Asthma pharmacotherapy
Asthma/COPD
Omalizumab (Xolair®)
recombinant DNA-derived selective IgE monoclonal antibody
USA 2003 data: 60% of asthma – allergen-induced

57
Asthma pharmacotherapy
Asthma/COPD
Omalizumab (Xolair®)
recombinant DNA-derived selective IgE monoclonal antibody
• peak serum concentrations after 7-8 days
• tissue elimination (intracellular)
• SC administration every 2 or 4 weeks
• T1/2 - 26 days
• anaphylactic reactions in 0.2%
• ↑ cancer?

58
Asthma pharmacotherapy
Asthma/COPD
Omalizumab (Xolair®)
• poorly controlled moderate-severe persistent asthma
• year-round allergies (proven allergic reaction)
• inadequate control despite routine ICS use
indicated for children over 12 and adults with:
• free circulating IgE reduced by 96%
• decreased incidence of asthma exacerbations
in these patients:
59
Asthma pharmacotherapy
Asthma/COPD
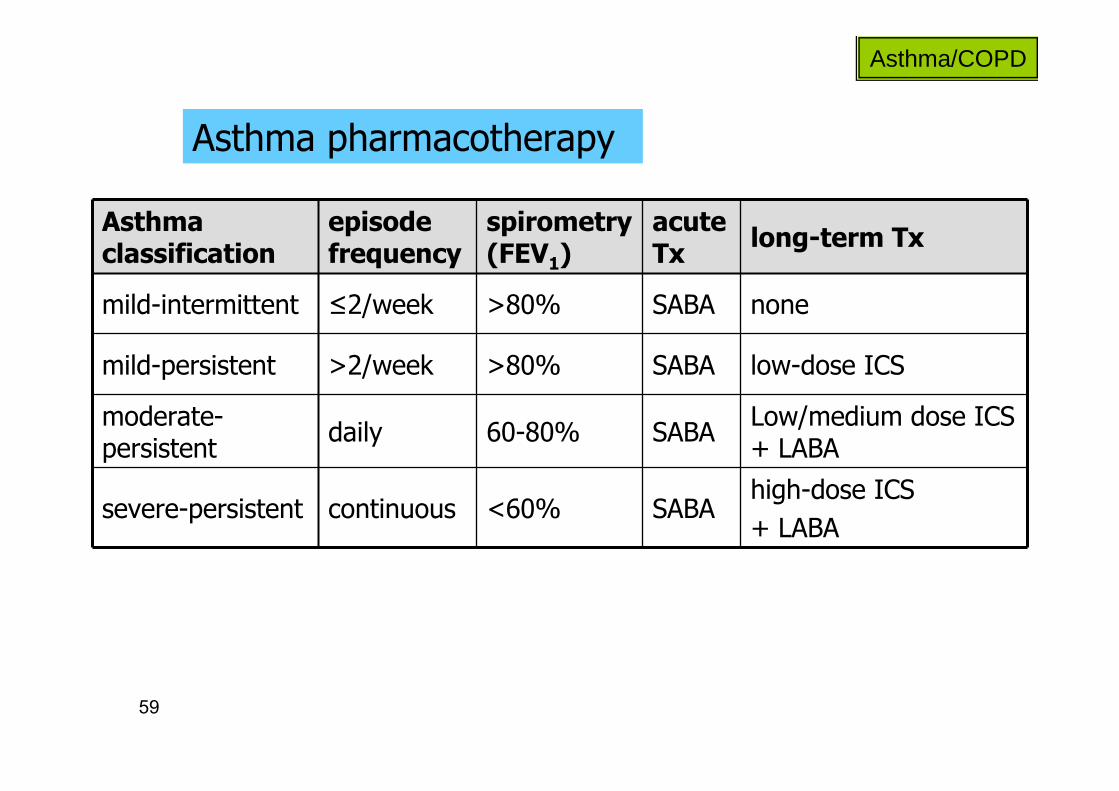
long-term Txacute Tx
spirometry (FEV1)
episode frequency
Asthma classification
noneSABA>80%≤2/weekmild-intermittent
low-dose ICSSABA>80%>2/weekmild-persistent
Low/medium dose ICS + LABA
SABA60-80%dailymoderate-persistent
high-dose ICS
+ LABASABA<60%continuoussevere-persistent

60
Asthma pharmacotherapy
Asthma/COPD

61
Asthma pharmacotherapy
Asthma/COPD
Pharmacological markers for uncontrolled asthma
• acute SABA required >2/wk
• oral CS bursts required >2/yr
62
Asthma pharmacotherapy
Asthma/COPD
http://www.nhlbi.nih.gov/guidelines/asthma/asthsumm .pdf
Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asth ma –
Summary Report 2007
http://www.ginasthma.org/

63
COPD chronic obstructive pulmonary disease
Asthma/COPD
chronic, irreversible airflow obstruction
• two entities:
-
-
• slowly-progressive airway damage
• symptoms appear after years of exposure

64
COPD chronic obstructive pulmonary disease
Asthma/COPD
chronic, irreversible airflow obstruction
• 4th leading cause of death (USA)
• deadlier than asthma
• morbidity and mortality rising
• estimated USA annual cost >$30,000,000,000

65
COPD chronic obstructive pulmonary disease
Asthma/COPD
chronic, irreversible airflow obstruction
causes:

66
COPD chronic obstructive pulmonary disease
Asthma/COPD
chronic, irreversible airflow obstruction
symptoms/diagnosis:
• chronic cough (productive/non-productive)
• excessive mucus production
• shortness of breath (mild exertion)
• frequent throat-clearing
• chest tightness
• respiratory function tests (spirometry)
67
COPD chronic obstructive pulmonary disease
Asthma/COPD
Non-pharmacological Tx
avoid triggers
• smoking
• dust/chemicals
• air-pollution
[get better genes]

68
COPD chronic obstructive pulmonary disease
Asthma/COPD
Pharmacotherapy
non-curable, non-reversible: control symptoms
• 1st-line: inhaled bronchodilators
- SABAs/LABAs (LABAs advantageous for nocturnal episodes)
- anticholinergic (tiotropium = Spiriva®)
- combination
once-daily anticholinergic bronchodilator
69
COPD chronic obstructive pulmonary disease
Asthma/COPD
Pharmacotherapy
non-curable, non-reversible: control symptoms
• 2nd-line: ICS
- moderate-severe COPD uncontrolled with 1st-line
- modest effect in most COPD patients
- differing efficacy in asthma vs. COPD related to different inflammatory mediators
70
COPD chronic obstructive pulmonary disease
Asthma/COPD
Pharmacotherapy
non-curable, non-reversible: control symptoms
- presently lost favor (ADEs)
• 2nd/3rd-line: theophylline
- past 1st-line
- option for those unable to optimally operate inhalers

71
COPD chronic obstructive pulmonary disease
Asthma/COPD
Pharmacotherapy
Long-term TxFEV1Severity
SABA, as needed>80%mild
SABA/LABA/anticholinergic ± ICS30-80%moderate
as in moderate,
- antibiotics for acute exacerbations
- O2
<30%severe

72
COPD chronic obstructive pulmonary disease
Asthma/COPD
Pharmacotherapy
http://www.nhlbi.nih.gov/health/public/lung/copd/campaign-materials/html/providercard.htm

73
COPD chronic obstructive pulmonary disease
Asthma/COPD
COPD vs. asthma
COPDasthma
adulthood (>40s)childhood - young adulthoodtypical onset
respiratory infectionsallergen, exercise, cold airexacerbation
LABA (→ ICS)ICS → LABATx sequence
nearly daily symptomssymptom-free periodsTx effect
74
• inhaled corticosteroids – fluticasone• beta-2 adrenergic agonists
- short-acting: salbutamol - long-acting: salmeterol
• theophylline• cromolyn• ipratropium/tiotropium• montelukast• omalizumab
Pharmacotherapy – asthma/COPD
DRUGS FOR EXAM
Asthma/COPD