asthma and copd || pulmonary rehabilitation
TRANSCRIPT
713
C H A P T E R
Pulmonary Rehabilitation
INTRODUCTION
Pulmonary rehabilitation is nowadays a rec-ognized evidence-based therapy which can be applied to patients with lung diseases who are symptomatic and have reduced activities of daily living, despite optimal medical therapy [1, 2] . Unlike most drugs, pulmonary rehabilitation does not target the lungs directly, but aims at reversing or stabilizing the extra-pulmonary eff ects of lung diseases [1] .
Lung disease, especially chronic obstruc-tive pulmonary disease (COPD), is a poorly diagnosed, but a very prevalent problem in our society. More than half the patients with mild to moderate COPD remain undiagnosed until late in the disease [3] . Physical inactivity is a natural defense strategy to avoid the distressing symp-tom of exercise induced dyspnea. Unfortunately, inactivity inevitably leads to many of the s ystemic
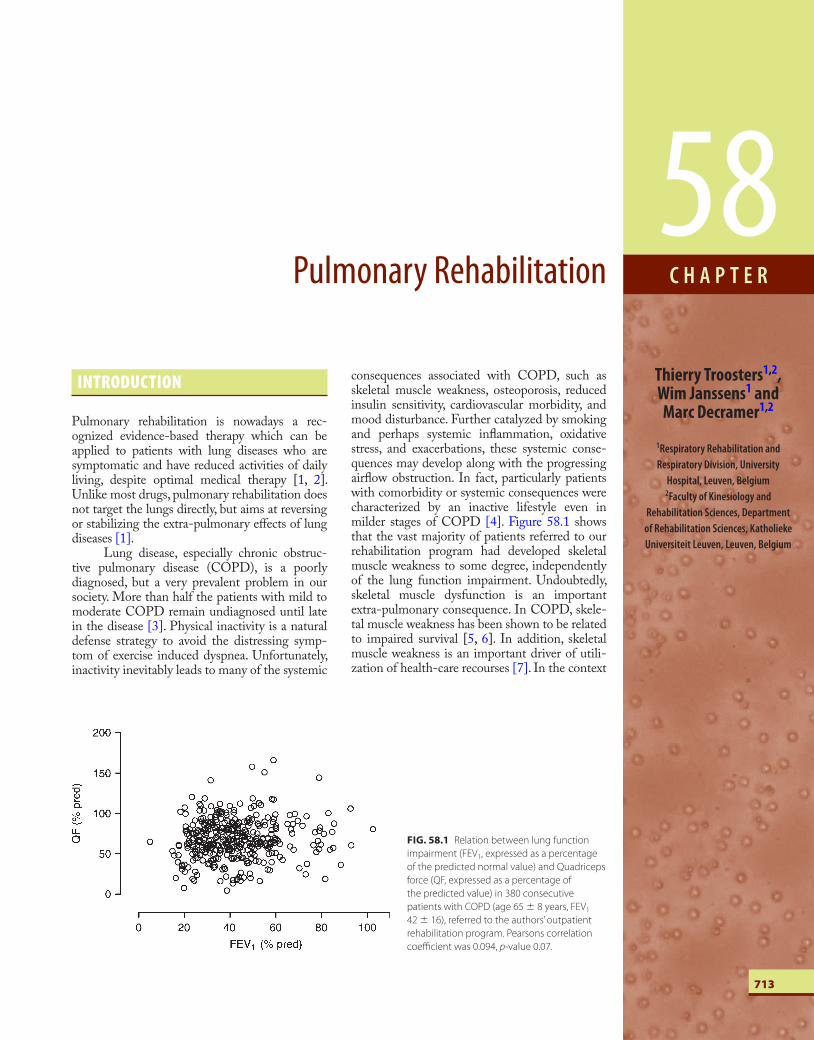
consequences associated with COPD, such as skeletal muscle weakness, osteoporosis, reduced insulin sensitivity, cardiovascular morbidity, and mood disturbance. Further catalyzed by smoking and perhaps systemic infl ammation, oxidative stress, and exacerbations, these systemic conse-quences may develop along with the progressing airfl ow obstruction. In fact, particularly patients with comorbidity or systemic consequences were characterized by an inactive lifestyle even in milder stages of COPD [4] . Figure 58.1 shows that the vast majority of patients referred to our rehabilitation program had developed skeletal muscle weakness to some degree, independently of the lung function impairment. Undoubtedly, skeletal muscle dysfunction is an important extra-pulmonary consequence. In COPD, skele-tal muscle weakness has been shown to be related to impaired s urvival [5, 6] . In addition, skeletal muscle weakness is an important driver of utili-zation of health-care recourses [7] . In the context
58 Thierry Troosters 1, 2 , Wim Janssens 1 and Marc Decramer 1 ,2
1 Respiratory Rehabilitation and Respiratory Division, University
Hospital, Leuven, Belgium 2 Faculty of Kinesiology and
Rehabilitation Sciences, Department of Rehabilitation Sciences, Katholieke Universiteit Leuven, Leuven, Belgium
FIG. 58.1 Relation between lung function
impairment (FEV1, expressed as a percentage
of the predicted normal value) and Quadriceps
force (QF, expressed as a percentage of
the predicted value) in 380 consecutive
patients with COPD (age 65 � 8 years, FEV1
42 � 16), referred to the authors ’ outpatient
rehabilitation program. Pearsons correlation
coeffi cient was 0.094, p -value 0.07.
Asthma and COPD: Basic Mechanisms and Clinical Management
714
of pulmonary rehabilitation, it is also important to recognize the non-physiological extra-pulmonary consequences of chronic lung disease. Depression, for example, is very preva-lent in stable patients [8] , and is signifi cantly related to the adverse outcome of COPD, particularly after acute exacerba-tions [9] . In the recent Global Initiative for Obstructive Lung Disease (GOLD), the systemic consequences of COPD were specifi cally noted as an important marker of morbidity, com-plicating the management of obstructive lung disease [10] .
As mentioned above, pulmonary rehabilitation targets the systemic consequences of lung diseases. It is now gener-ally recognized as an evidence-based and eff ective therapy for patients with lung diseases, who are symptomatic and have reduced participation the in activities of daily life. Th e evidence on the eff ectiveness of pulmonary rehabilitation is impressive, and has been reviewed in several recent documents. Table 58.1 summarizes the most important eff ects of rehabilitation and where applicable the strength of the evidence, as provided in the diff erent evidence-based reviews. To be successful, pulmo-nary rehabilitation is typically designed as a comprehensive intervention off ered by a team of health-care providers over a substantial period of time. Typically, rehabilitation programs are carried out for 6 weeks to 6 months, with longer programs yielding more substantial eff ects [14] . Patients participate in an individualized tailored program which takes into account the complexity of the presenting patient. Exercise training is the cornerstone of such a program. Several other interven-tions may complement the program to maximize its eff ective-ness. Pulmonary rehabilitation may serve many goals, which depend on the perspective one takes. Examples of the goals from the diff erent perspectives are as follows:
Patient’s perspective:
● Reduced symptoms of breathlessness or fatigue
● Enhanced exercise tolerance and skeletal muscle strength
● Improved physiological and emotional function
● Increased health-related quality of life.
Th e health-care provider’s perspective:
● Optimal self-management by the patient
● Optimal utilization of available recourses.
Th e societal perspective:
● Increased productivity and active participation of patients in society
● Reduction of cost associated with the management of the disease
● Enhanced coping of the family when a family member is suff ering from COPD.
It is important to realize that patients suff ering from other respiratory diseases, such as pulmonary sarcoidosis [15] , cystic fi brosis [16] , or after lung transplantation [17] , equally present systemic consequences of their disease. Consequently, pulmonary rehabilitation programs should not be restricted to patients with COPD, but should be open to any patient suff ering from extra-pulmonary consequences of lung dis-eases in general.
THE INDICATION FOR REHABILITATION AND SETTING
According to the defi nition of the American Th oracic Society and the European Respiratory Society, pulmonary
TABLE 58.1 An overview of the eff ects of pulmonary rehabilitation as reported in evidence-based practice guidelines [11] , a state of the art review [12] and
a Cochrane meta-analysis [13] .
Eff ect Evidence grade [11] Size of eff ect
Improvement of dyspnea 1A CRDQ-Dys: 1.06 (0.85 to 1.26) points [13]
Improvement of HRQoL 1A SGRQ total: � 6.11 ( � 8.98 to 3.24)% [13]
Reduction in hospital days and utilization of
health care recourses
2B
Survival None provided
Psychosocial benefi ts (self-effi cacy with exercise,
cognitive function, anxiety, depression)
2B
Exercise tolerance
Peak work rate 8W (3–13W) [13] � 18 (IQR 13–24) % baseline [12]
6MWD 48 min (32–65 min) [13] � 34 min if � 28 s, 50 min if � 28 s [12]
Whole body endurance � 87% of baseline [12]
Evidence grading 1A: Strong recommendation; 2B: Weak recommendation; CRDQ-Dys: Dyspnea subscale of the chronic respiratory disease questionnaire; SGRQ: saint Georges
Respiratory Questionnaire; 6MWD: six minute walking distance.

58Pulmonary Rehabilitation
715
re habilitation is aiming at reducing symptoms, optimizing function, increasing participation, and reducing health-care cost through stabilizing or reversing the systemic conse-quences of the disease [1] . Hence, theoretically, patients with an indication for the need of rehabilitation are those suff ering from extra-pulmonary consequences. Th is defi ni-tion is, however, not very practical as the systemic conse-quences that can be targeted by pulmonary rehabilitation are not defi ned. Clearly, not all “ systemic consequences ” of the disease are amendable to pulmonary rehabilitation. For example, osteoporosis and anemia are the recognized sys-temic consequences of COPD [18] , but it is unlikely that pulmonary rehabilitation would have a signifi cant impact on these outcomes. In addition, the spin-off of pulmonary rehabilitation may well be an enhanced self-management, which leads to more effi cient utilization of health care recourses and cost savings [19] , without altering the “ sys-temic consequences of the disease. ”
A more practical approach to identifying candidates for rehabilitation and guide the assessment of patients before enrollment in rehabilitation could be to select patients who are optimally pharmacologically treated, but still present with one of the following:
● Disabling symptoms due to deconditioning
● Skeletal or respiratory muscle weakness
● Poor health-related quality of life
● Repeated exacerbations or ineffi cient use of available recourses
● Depressed mood status
● Malnutrition (obesity of cachexia)
● Poor coping with the symptoms of their disease.
Th is allows to set up active screening for rehabilitation pro-grams, which typically includes assessment of exercise tol-erance, skeletal and respiratory muscle force, nutritional status, symptoms, health-related quality of life, and capability of self-management.
Depending on the complexity of the individual prob-lem, the program can be designed across a range of complex-ities. Programs can be as simple as an intervention consisting of exercise training in the home setting of patients with uncomplicated COPD [20] or as complex as an in-patient program in a mechanically ventilated patient [21] . On the basis of proper assessment the individual program, its setting and components can be designed, taking into account the available recourses in a given region, current best practice, and evidence. Several guidelines may help those setting up pulmonary rehabilitation facilities to structure their program [1, 11, 22, 23] .
Exercise training has now the status of the corner-stone of each program, and will be dealt with below. Exercise training has a strong evidence base. A program of exercise training of the muscles of ambulation is recommended and is a mandatory component of any pulmonary rehabilitation program [11] . For several other components of a rehabilita-tion program, however, evidence is also building up, particu-larly for specifi c subgroups of patients.
In depressed patients (some 40% (95% CI: 36–44%) of patients with COPD [24] ), for example, psychologi-cal c ounseling may be of benefi t in order to help reducing symptoms of depression or anxiety. Admittedly, a large trial to confi rm the point is currently still missing [25, 26] , but since depressive symptoms do signifi cantly impact on health-related quality of life [27] and even impact readmis-sion [9] in these patients, psychological counseling may well be worth the eff ort in patients who suff er from symptoms of depression, anxiety, or poor coping. It should be stressed, however, that exposure to exercise therapy may in itself have an anti-depressant eff ect [28] . Nutritional interven-tions have been shown to be unsuccessful in poorly selected COPD patients [29] . However, when nutritional interven-tions are successful in improving body mass in cachectic patients, they do spin-off in an important survival benefi t [30] . Besides patients suff ering from pulmonary cachectia, a less recognized role, but likely of equal importance, is the care for obese COPD patients . Clearly obesity is linked to increased pulmonary ventilation to carry out activities of daily living. Consequently, weight loss in obese patients might yield important functional benefi ts in activities car-ried out against gravity (e.g. stair climbing, walking). Th e authors believe that weight loss, particularly loss of fat mass, might be an important target in overweight COPD patients referred to pulmonary rehabilitation programs. Occupational therapists may be consulted within the context of a rehabilitation program [31] . Occupational therapists may advise patients on the mode and pace of carrying out activities of daily life. Oftentimes occupational therapists might advise on the use of wheeled walking aids (rolla-tors). Although many patients show poor compliance with the daily use of a rollator [32] , those who use it may sub-stantially and suddenly improve their exercise tolerance [33, 34] . Other potentially cost-eff ective components of a reha-bilitation program are interventions aiming at enhancing self-management. Generally, these interventions are super-vised by specially trained advanced practice nurses , who work integrated in the rehabilitation team. Interventions aiming at enhancing self-management have shown variable success [35] . Studies showing cost-eff ectiveness of these interven-tions focused at a subgroup of patients with at least one hospital admission [19] . Hence it seems reasonable to direct eff orts specifi cally to this subgroup of patients.
Another point to consider when a patient is referred to a pulmonary rehabilitation program is the setting of such a program. Programs have been successfully set up in a primary care (home) setting [20, 36] as an outpatient program in a rehabilitation center [37] or in the commu-nity [38, 38] , or as an in-patient program [39, 40] . Clearly each of these programs has advantages and disadvantages. One of the most important problems of home-based pro-grams is the limited staff and equipment, which makes it diffi cult to deal with more severe patients [41] . Th e most important problem of outpatient programs is the trans-portation to the center [42] . In-patient programs are costly and should be restricted to those patients with very limited mobility. Ideally, a reference rehabilitation center should have access to all modalities of rehabilitation. Th is can be done by establishing strong links between the diff erent lines of health care.

Asthma and COPD: Basic Mechanisms and Clinical Management
716
Screening of patients for rehabilitation
From the above it is clear that proper design of a rehabilita-tion program depends on a thorough screening of patients. Th is screening should answer the following questions:
1 Is there an indication for pulmonary rehabilitation in a given patient and what results can be expected?
2 Which components should be included in the program for a given patient and what will be the optimal setting of the program?
An example of the intake procedure in the authors ’ institute is given in Table 58.2 .
Indication and expected results
To establish the indication for a rehabilitation program, a formal exercise test should be carried out. Exercise intol-erance is indeed an important reason to refer a patient for rehabilitation. We found that patients with skeletal and res-piratory muscle weakness were most responsive to exercise training [43] , justifying the assessment of peripheral and respiratory muscle strength. Rehabilitation programs are oriented toward patients who are symptomatic and have reduced activities of daily life, encouraging to assess symp-toms and health-related quality of life, and physical activity. With evolving technology it becomes possible to assess the latter, rather than estimate physical activity levels with ques-tionnaires [44, 45] . In patients admitted to the hospital with a severe exacerbation of COPD, pulmonary r ehabilitation
TABLE 58.2 An example of the intake procedure for pulmonary rehabilitation at the authors ’ center.
Test Reason or consequence
Lung function assessment Disease severity
Exercise test
Incremental cycle ergometry Exercise intolerance/factors limiting exercise
6MWD Exercise intolerance, treatment eff ect
Constant work rate test Treatment eff ect
Muscle function
Quadriceps force, biceps, triceps Muscle weakness? Need for resistance training
Respiratory muscle force Need for inspiratory muscle training
Symptoms, Function
MRC Severity of impairement in daily life
PFSDQ Symptoms in daily life (occupational therapists)
HRQoL
CRDQ Indication for rehabilitation, identifi cation of problems in four domains
Activity monitoring
1 week of monitoring Actual physical activity level
Interview psychologist
HADS Psychological burden
Social anamnesis Social support
Nutritional anamnesis Calorie intake and nutritional � protein balance
Bioelectrical impedance Assessment of body composition
6MWD: six minute walking distance; MRC: medical council dyspnea scale; PFSDQ: Pulmonary functional status and dyspnea scale;
HRQoL: Health related quality of life with the Chronic Respiratory Disease Questionnaire (CRDQ); HADS: Hospital anxiety and depression scale.

58Pulmonary Rehabilitation
717
should be part of the proper after care. In these patients rehabilitation does reduce readmission rate by 75% and may even enhance survival [46] . In addition substantial and clinically relevant improvements in exercise tolerance and health-related quality of life were reported [47] .
Components of the rehabilitation program
To establish the components of the rehabilitation program and its optimal setting, a multidisciplinary assessment is needed. Th is consists of a nutritional assessment, including analysis of the fat free mass and a nutritional interview to estimate the caloric balance [48] . A thorough social interview to gain insight in the social network and available social sup-port is helpful since patients lacking social support are at risk to drop out from a program [49] . An intake by a psycholo-gist may allow to identify the large proportion of patients suff ering from signifi cant depressive symptoms or other psy-chiatric morbidity [50] . An important and often forgotten aspect may be the burden on the partner of the patient [51] . A fi rst screening for psychological morbidity can be done using questionnaires such as the Beck depression inventory or the Hospital Anxiety and Depression Scale. Lastly physi-cal activity levels of patients and symptoms during specifi c activities of daily living can be assessed using questionnaires such as the Pulmonary Functional Status and Dyspnea Questionnaire (PFSDQ) [52, 53] .
Depending on the complexity of the individual case one or more disciplines can be engaged in the rehabilita-tion process of the individual patient. Ideally the patient is referred to a program which optimally meets his needs and takes into account the motivation and social circumstances. Needless to say that a program should also be moduled along the possibilities of the health-care system in a given region.
Exercise training
Exercise training is undoubtedly the cornerstone of a pul-monary rehabilitation program. Programs aim at enhanc-ing exercise tolerance and skeletal muscle force. Skeletal muscle force can be enhanced by specifi c resistance training (weightlifting) exercise [54–56] . Improvement in exercise tolerance is essentially obtained through two main path-ways. First, the oxidative capacity of the skeletal muscle is enhanced [57] , leading to reductions in lactate production at identical work [58] . A second pathway involves an improve-ment in movement effi ciency, yielding less oxygen consump-tion to cover identical work rate. Both pathways are not mutually exclusive, and both lead to reductions in pulmonary ventilation, and dynamic hyperinfl ation during exercise. Th e reduction in pulmonary ventilation, the improved dynamic hyperinfl ation, and the desensitization (better tolerance to high ventilatory levels) are crucial to the improved exer-tional dyspnea, which is seen after exercise training [13] . To enhance the oxidative capacity of the skeletal muscle, exer-cise training should be conducted at relatively high training intensity [58] (see below). Improvement in movement effi -ciency is obtained by practicing specifi c exercises (e.g. walk-ing training will only improve walking effi ciency). For this pathway, the modality of the exercise is more crucial than the intensity at which the exercise is carried out.
In general, exercise training in patients with COPD follows the principles of exercise training in the healthy eld-erly [59] . Programs generally consist of a brief warm-up, a core program lasting at least 30 min of exercise and a cooling down. An example of an exercise training program is given in Table 58.3 . Close supervision and proper monitoring of the patients ensure the safety during the program [12] . In fact, very few exercise-related events and, as far as the authors are aware, no fatal events have been reported after pulmonary rehabilitation in the published literature.
TABLE 58.3 An overview of an outpatient rehabilitation session in the rehabilitation center of the authors.
Time Duration (min) Item Intensity
13:00 5 Brief contact with health care provider to check the health status. Resting saturation,
peak fl ow, and heart rate are recorded
13:05 10 Low intensity warm-up exercise on bicycle 20–30 W
13:15 32 Cycling exercises e.g. 8 blocks of 2 min interval training with 2 min of rest between the
intervals
75% Wmax
13:47 15 Resistance training exercises for the upper and lower limb. Typical muscle groups are
quadriceps, triceps, biceps and pectoral muscle
3 series of 8 repetitions
14:02 6 2 blocks of 2 min stair climbing separated by 2 min of rest Dyspnea 4–6/10
14:08 6 2 blocks of 2 min of arm ergometry separated by 2 min of rest Dyspnea 4–6/10
14:14 20 2 blocks of 8 min of treadmill walking 80% 6 MWs
14:34 30 Individual contact with another health care worker (psychologist, social worker, dietician)
15:04 End of session

Asthma and COPD: Basic Mechanisms and Clinical Management
718
Whole body exercise
Exercise training has been included in virtually all studies investigating the benefi ts of pulmonary rehabilitation. To suc-cessfully increase skeletal muscle properties and render meas-urable physiological benefi ts, it is important that patients do exercise at relative high work loads. To do so, the exercise train-ing intervention can be adapted to the individual exercise limi-tations of the patient. Th e conventionally used form to deliver exercise training to COPD patients is endurance training. In COPD patients with primarily moderate disease, exercise training conducted at approximately 75% of the peak work rate (60% of the diff erence between the lactate threshold and peak oxygen uptake) resulted in signifi cant physiological eff ects [58] . A similar training strategy was shown to be eff ective in patients with severe disease [60] . Others have confi rmed that high training intensity is required to elicit physiologic training eff ects [61, 62] .
It is important to adjust and increase the training load in every training session. Trained personnel should be available to ensure close supervision on the training intensity. Training intensity can be monitored using 10-point Borg symptom scales. A score around 4–6 is generally advised as an appropri-ate training intensity, provided the patients are familiar with the scale. Interestingly, a given Borg symptom score is generally chosen by a patient at an identical relative work rate. Hence as patients improve during training, the same Borg rating will be achieved at higher absolute work rates [63] . Since most patients are not limited by the cardiovascular system, using heart fre-quency to guide exercise training is not to be advised.
In patients who reach a ventilatory limitation during exercise, it is diffi cult to obtain a high training intensity for sustained periods of time. Several strategies may help clini-cians to ensure high intensity training in more severe COPD. Interval exercise training has been used and showed to result in physiological benefi ts, comparable to those of endurance training [64–67] . Th e advantage of interval training is that the ventilatory requirements remain relatively limited [68] . Interval training is achieved by breaking down the long exer-cise bouts into smaller bouts of exercise separated by periods of active recovery (low work rate) or rest.
An intervention that minimizes the ventilatory burden during exercise training is the use of supplemental oxygen. Oxygen, dose dependently, reduces the ventilation for a given exercise intensity [69, 70] . Th e application of oxygen supple-ments hence allows training at higher training intensity [71] . Non-invasive mechanical ventilation reduces the work of breathing and has been used successfully in severe COPD as an adjunct to exercise training [72–74] . In less severe COPD the impact of using non-invasive mechanical ventilation was not signifi cant [75] . Lastly, the required ventilation can be reduced simply by reducing the amount of muscles set at work. If exercise is confi ned to one leg, ventilation is con-siderably reduced, allowing a signifi cant increase in training load [76] . A recent trial confi rmed that in severe patients, single leg exercise training resulted in 20% more increase in peak oxygen consumption and peak work rate compared to conventional cycling training (two legs) [77] . In the latter study, however, no patient centered outcomes were assessed. Hence, although interesting from a physiological perspective, it is too early to judge whether single leg exercise training is
ready for wide clinical use [78] . Similarly, during cycling less muscles are recruited compared to walking exercises; hence it is not surprising that for a given oxygen consumption, cycling is more fatiguing for the quadriceps muscle [79] . It would be interesting to conduct a head-to-head comparison study on the physiological eff ects of cycling versus walking exercises. On the basis of the larger potential to elicit mus-cle fatigue, cycling would be a form of exercise training that may result in larger physiological eff ects, compared to walk-ing. However, such a study is currently unavailable.
All the above techniques reduce the ventilatory bur-den. Another complementary option is to enhance the ven-tilatory capacity. Obviously optimal bronchodilator therapy does also allow for larger pulmonary ventilation and less dynamic hyperinfl ation during exercise. In one study, a potent long-term anti-cholinergic drug showed to enhance exercise training eff ects compared to the use of short acting bronchodilators only [80] . Breathing gases with light density (e.g. helium and oxygen, HELIOX) also enhance the venti-latory capacity. One study suggests that maximal ventilation is enhanced by 16% when breathing 21% oxygen and 79% helium [81] . Although this would technically allow training at higher intensity, it is doubtful whether this intervention is currently ready for clinical routine. A last intervention which enhances peak ventilatory capacity is bracing the arms. During walking, this can be applied using a wheeled walking aid (rollator). Our group showed that bracing the arms on a rollator enhanced maximal voluntary ventilation by 8 l/min, which partly explained the acute benefi cial eff ect of a rollator [82] . During treadmill walking, bracing of the arms can also easily be achieved.
Resistance training
Another form of conventional training is resistance training. Th is form of exercise, generally consisting of weight lifting, can be used as the only form of training [55, 56, 83] , or in combination with whole body exercises [54, 55, 84] . In all the latter studies, muscle strength was signifi cantly more increased when resistance training was added to the exercise regimen. Increased muscle strength is an important treat-ment objective in patients with COPD suff ering from mus-cle weakness, as activities of daily life do require strength apart from muscle endurance. As mentioned above, muscle weakness is an important factor related to morbidity and even mortality in COPD. It follows that patients suff ering from muscle weakness may be particularly good candidates to a resistance training program.
Resistance training is easy to apply in clinical practice. Patients are instructed to lift weights (generally on a multi-gym device). Th e weight imposed and the number of rep-etitions ensure overload of the skeletal muscle. In patients with COPD and several other chronic diseases, resistance training is started at approximately 70% of the weight a patient can lift once (i.e. the one repetition maximum). Th e eff ects of resistance training programs may be enhanced in male hypogonadal patients by testosterone replacement therapy. In one study, [85] weekly intramuscular injections with testosterone, aiming at restoring testosterone levels to normal values in initially hypogonadal men, did enhance skeletal muscle force more than either of the interventions
58Pulmonary Rehabilitation
719
alone. Further studies are required to investigate the long-term safety of this intervention. However, since skeletal muscle dysfunction is in itself a negative prognostic factor, a short-term use of testosterone may be benefi cial to result in a rapid restoration of this potentially harmful situation.
Neuromuscular electrical stimulation
Another intervention used to specifi cally stimulate the peripheral muscles is medium to high-frequency neu-romuscular electrical stimulation (NMES). Four studies have investigated successfully the eff ects of this intervention [86–89] . All studies in COPD used transcutaneous electri-cal stimulation with stimulation frequencies of 35 [89] to 50 Hz [86, 87, 90] . In patients with congestive heart failure, low-frequency (10–15 Hz) transcutaneous electrical stimu-lation was successfully applied [91, 92] . Studies showed that there was more strength gain in the skeletal muscles treated with electrical stimulation, either as mono-therapy or in combination with general exercise training [89] . Th is intervention may prove to be attractive in patients who have diffi culties to take part in regular rehabilitation, such as patients admitted to hospital with acute exacerbations.
Enhancing physical activity
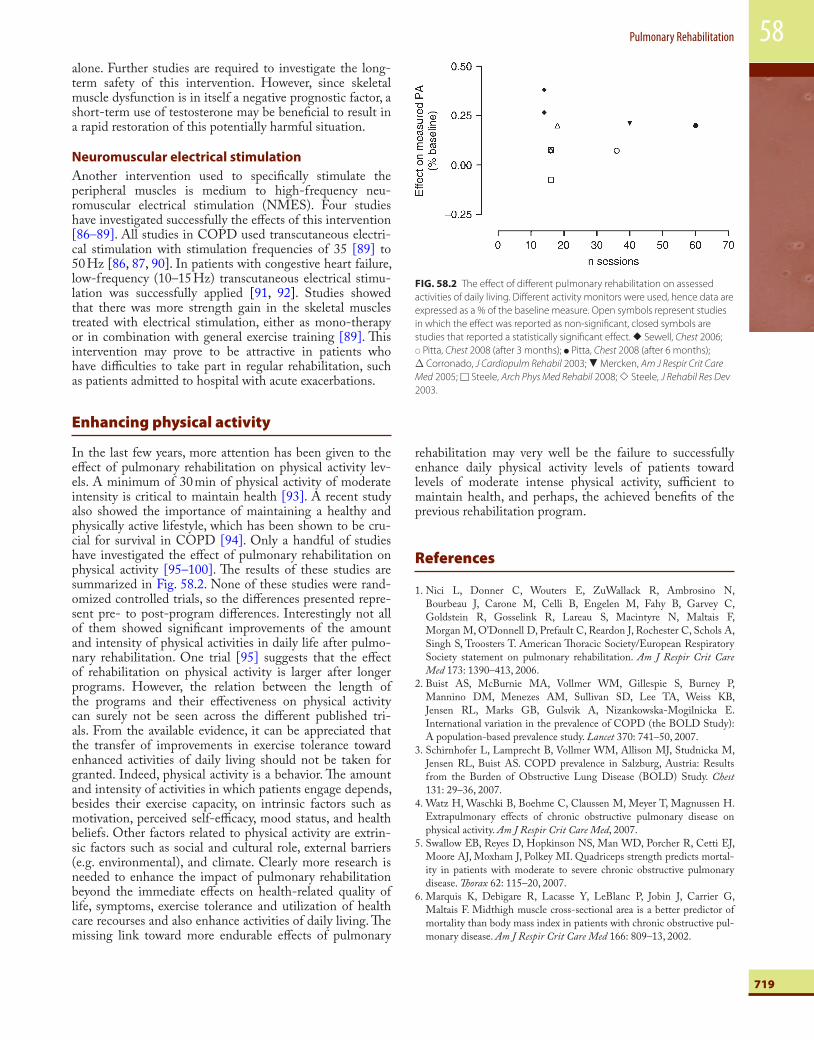
In the last few years, more attention has been given to the eff ect of pulmonary rehabilitation on physical activity lev-els. A minimum of 30 min of physical activity of moderate intensity is critical to maintain health [93] . A recent study also showed the importance of maintaining a healthy and physically active lifestyle, which has been shown to be cru-cial for survival in COPD [94] . Only a handful of studies have investigated the eff ect of pulmonary rehabilitation on physical activity [95–100] . Th e results of these studies are summarized in Fig. 58.2 . None of these studies were rand-omized controlled trials, so the diff erences presented repre-sent pre- to post-program diff erences. Interestingly not all of them showed signifi cant improvements of the amount and intensity of physical activities in daily life after pulmo-nary rehabilitation. One trial [95] suggests that the eff ect of rehabilitation on physical activity is larger after longer programs. However, the relation between the length of the programs and their eff ectiveness on physical activity can surely not be seen across the diff erent published tri-als. From the available evidence, it can be appreciated that the transfer of improvements in exercise tolerance toward enhanced activities of daily living should not be taken for granted. Indeed, physical activity is a behavior. Th e amount and intensity of activities in which patients engage depends, besides their exercise capacity, on intrinsic factors such as motivation, perceived self-effi cacy, mood status, and health beliefs. Other factors related to physical activity are extrin-sic factors such as social and cultural role, external barriers (e.g. environmental), and climate. Clearly more research is needed to enhance the impact of pulmonary rehabilitation beyond the immediate eff ects on health-related quality of life, symptoms, exercise tolerance and utilization of health care recourses and also enhance activities of daily living. Th e missing link toward more endurable eff ects of pulmonary
rehabilitation may very well be the failure to successfully enhance daily physical activity levels of patients toward levels of moderate intense physical activity, suffi cient to maintain health, and perhaps, the achieved benefi ts of the previous rehabilitation program.
References
1 . Nici L , Donner C , Wouters E , ZuWallack R , Ambrosino N , Bourbeau J , Carone M , Celli B , Engelen M , Fahy B , Garvey C , Goldstein R , Gosselink R , Lareau S , Macintyre N , Maltais F , Morgan M , O’Donnell D , Prefault C , Reardon J , Rochester C , Schols A , Singh S , Troosters T . American Th oracic Society/European Respiratory Society statement on pulmonary rehabilitation . Am J Respir Crit Care Med 173 : 1390 – 413 , 2006 .
2 . Buist AS , McBurnie MA , Vollmer WM , Gillespie S , Burney P , Mannino DM , Menezes AM , Sullivan SD , Lee TA , Weiss KB , Jensen RL , Marks GB , Gulsvik A , Nizankowska-Mogilnicka E . International variation in the prevalence of COPD (the BOLD Study): A population-based prevalence study . Lancet 370 : 741 – 50 , 2007 .
3 . Schirnhofer L , Lamprecht B , Vollmer WM , Allison MJ , Studnicka M , Jensen RL , Buist AS . COPD prevalence in Salzburg, Austria: Results from the Burden of Obstructive Lung Disease (BOLD) Study . Chest 131 : 29 – 36 , 2007 .
4 . Watz H , Waschki B , Boehme C , Claussen M , Meyer T , Magnussen H . Extrapulmonary eff ects of chronic obstructive pulmonary disease on physical activity . Am J Respir Crit Care Med , 2007 .
5 . Swallow EB , Reyes D , Hopkinson NS , Man WD , Porcher R , Cetti EJ , Moore AJ , Moxham J , Polkey MI . Quadriceps strength predicts mortal-ity in patients with moderate to severe chronic obstructive pulmonary disease . Th orax 62 : 115 – 20 , 2007 .
6 . Marquis K , Debigare R , Lacasse Y , LeBlanc P , Jobin J , Carrier G , Maltais F . Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pul-monary disease . Am J Respir Crit Care Med 166 : 809 – 13 , 2002 .
FIG. 58.2 The eff ect of diff erent pulmonary rehabilitation on assessed
activities of daily living. Diff erent activity monitors were used, hence data are
expressed as a % of the baseline measure. Open symbols represent studies
in which the eff ect was reported as non-signifi cant, closed symbols are
studies that reported a statistically signifi cant eff ect. � Sewell, Chest 2006;
� Pitta, Chest 2008 (after 3 months); � Pitta, Chest 2008 (after 6 months);
Δ Corronado, J Cardiopulm Rehabil 2003; � Mercken, Am J Respir Crit Care
Med 2005; � Steele, Arch Phys Med Rehabil 2008; � Steele, J Rehabil Res Dev
2003.

Asthma and COPD: Basic Mechanisms and Clinical Management
720
7 . Decramer M , Gosselink R , Troosters T , Verschueren M , Evers G . Muscle weakness is related to utilization of health care resources in COPD patients . Eur Respir J 10 : 417 – 23 , 1997 .
8 . van Manen JG , Bindels PJ , Dekker FW , IJzermans CJ , van der Zee JS , Schade E . Risk of depression in patients with chronic obstructive pul-monary disease and its determinants . Th orax 57 : 412 – 16 , 2002 .
9 . Ng TP , Niti M , Tan WC , Cao Z , Ong KC , Eng P . Depressive symp-toms and chronic obstructive pulmonary disease: Eff ect on mortality, hospital readmission, symptom burden, functional status, and quality of life . Arch Intern Med 167 : 60 – 67 , 2007 .
10 . Rabe KF , Hurd S , Anzueto A , Barnes PJ , Buist SA , Calverley P , Fukuchi Y , Jenkins C , Rodriguez-Roisin R , van WC , Zielinski J . Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary . Am J Respir Crit Care Med 176 : 532 – 55 , 2007 .
11 . Ries AL , Bauldoff GS , Carlin BW , Casaburi R , Emery CF , Mahler DA , Make B , Rochester CL , ZuWallack R , Herrerias C . Pulmonary rehabilitation: Joint ACCP/AACVPR evidence-based clinical practice guidelines . Chest 131 : 4S – 42S , 2007 .
12 . Troosters T , Casaburi R , Gosselink R , Decramer M . Pulmonary reha-bilitation in chronic obstructive pulmonary disease . Am J Respir Crit Care Med 172 : 19 – 38 , 2005 .
13 . Lacasse Y , Goldstein R , Lasserson TJ , Martin S . Pulmonary rehabilita-tion for chronic obstructive pulmonary disease . Cochrane Database Syst Rev , 2006 , CD003793.
14 . Salman GF , Mosier MC , Beasley BW , Calkins DR . Rehabilitation for patients with chronic obstructive pulmonary disease . J Gen Intern Med 18 : 213 – 21 , 2003 .
15 . Spruit M , Th omeer M , Gosselink R , Troosters T , Kasran A , Debrock A , Demedts M , Decramer M . Skeletal muscle weakness in patients with sarcoidosis and its relationship with exercise intolerance and reduced health status . Th orax 60 : 32 – 38 , 2005 .
16 . Troosters T , Langer D , Vrijsen B , Segers J , Wouters K , Janssens W , Gosselink R , Decramer M , Dupont LJ . Skeletal muscle weakness, exer-cise tolerance and physical activity in adults with cystic fi brosis . Eur Respir J , 2007 , Revised.
17 . Maury G , Langer D , Verleden G , Dupont L , Gosselink R , Decramer M , Troosters T . Skeletal muscle force and functional exercise tolerance before and after lung transplantation, a cohort study . Am J Transplant , 2008 , in press.
18 . Fabbri LM , Rabe KF . From COPD to chronic systemic infl ammatory syndrome? Lancet 370 : 797 – 99 , 2007 .
19 . Bourbeau J , Julien M , Maltais F , Rouleau M , Beaupre A , Begin R , Renzi P , Nault D , Borycki E , Schwartzman K , Singh R , Collet JP . Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: A disease-specifi c self-management intervention . Arch Intern Med 163 : 585 – 91 , 2003 .
20 . Strijbos JH , Postma DS , van Altena R , Gimeno F , Koeter GH . A com-parison between an outpatient hospital-based pulmonary rehabilitation program and a home-care pulmonary rehabilitation program in patients with COPD. A follow-up of 18 months . Chest 109 : 366 – 72 , 1996 .
21 . Nava S . Rehabilitation of patients admitted to a respiratory intensive care unit . Arch Phys Med Rehabil 79 : 849 – 54 , 1998 .
22 . National Institute for Clinical Excellence (NICE) . Chronic obstructive pulmonary disease: National clinical guidline for the management of COPD in adults in primary and secondary care . Th orax 59 ( Suppl 1 ) , 2004 .
23 . Société de Pneumologie de Langue Française de Pneumologie . Recommandations de la Société de Pneumologie de Langue Française sur la réhabilitation du malade atteint de BPCO . Rev Mal Respir 22 : 7S8 – 7S14 , 2005 .
24 . Yohannes AM , Baldwin RC , Connolly MJ . Depression and anxiety in elderly patients with chronic obstructive pulmonary disease . Age Ageing 35 : 457 – 59 , 2006 .
25 . Coventry PA , Hind D . Comprehensive pulmonary rehabilitation for anxiety and depression in adults with chronic obstructive pulmonary disease: Systematic review and meta-analysis . J Psychosom Res 63 : 551 – 65 , 2007 .
26 . Coventry PA , Gellatly JL . Improving outcomes for COPD patients with mild-to-moderate anxiety and depression: A systematic review of cognitive behavioural therapy . Br J Health Psychol , 2007 .
27 . Oga T , Nishimura K , Tsukino M , Sato S , Hajiro T , Mishima M . Longitudinal deteriorations in patient reported outcomes in patients with COPD . Respir Med , 2006 .
28 . Craft LL , Perna FM . Th e benefi ts of exercise for the clinically depressed . Prim Care Companion J Clin Psychiatry 6 : 104 – 11 , 2004 .
29 . Ferreira IM , Brooks D , Lacasse Y , Goldstein RS . Nutritional support for individuals with COPD: A meta-analysis . Chest 117 : 672 – 78 , 2000 .
30 . Schols AM , Slangen J , Volovics L , Wouters EF . Weight loss is a revers-ible factor in the prognosis of chronic obstructive pulmonary disease . Am J Respir Crit Care Med 157 : 1791 – 97 , 1998 .
31 . Lorenzi CM , Cilione C , Rizzardi R , Furino V , Bellantone T , Lugli D , Clini E . Occupational therapy and pulmonary rehabilitation of disa-bled COPD patients . Respiration 71 : 246 – 51 , 2004 .
32 . Gupta RB , Brooks D , Lacasse Y , Goldstein RS . Eff ect of rollator use on health-related quality of life in individuals with COPD . Chest 130 : 1089 – 95 , 2006 .
33 . Gupta R , Goldstein R , Brooks D . Th e acute eff ects of a rollator in indi-viduals with COPD . J Cardiopulm Rehabil 26 : 107 – 11 , 2006 .
34 . Probst V , Heyvaert H , Coosemans I , Pitta F , Spruit M , Troosters T , Gosselink R , Decramer M . Eff ects of a rollator on exercise capacity, gas exchange and ventilation in COPD patients . Am J Respir Crit Care Med 167 : A669 , 2003 , Abstract.
35 . Effi ng T , Monninkhof EM , van der Valk PD , van der Palen J , van Herwaarden CL , Partidge MR , Walters EH , Zielhuis GA . Self-m anagement education for patients with chronic obstructive pulmo-nary disease . Cochrane Database Syst Rev , 2007 , CD002990.
36 . Wijkstra PJ , Ten Vergert EM , van Altena R , Otten V , Kraan J , Postma DS , Koeter GH . Long term benefi ts of rehabilitation at home on quality of life and exercise tolerance in patients with chronic obstruc-tive pulmonary disease . Th orax 50 : 824 – 28 , 1995 .
37 . Troosters T , Gosselink R , Decramer M . Short- and long-term eff ects of outpatient rehabilitation in patients with chronic obstructive pulmo-nary disease: A randomized trial . Am J Med 109 : 207 – 12 , 2000 .
38 . Griffi ths TL , Burr ML , Campbell IA , Lewis-Jenkins V , Mullins J , Shiels K , Turner-Lawlor PJ , Payne N , Newcombe RG , Ionescu AA , Th omas J , Tunbridge J , Lonescu AA . Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: A randomised controlled trial . Lancet 355 : 362 – 68 , 2000 .
39 . Goldstein RS , Gort EH , Stubbing D , Avendano MA , Guyatt GH . Randomised controlled trial of respiratory rehabilitation . Lancet 344 : 1394 – 97 , 1994 .
40 . Franssen FM , Broekhuizen R , Janssen PP , Wouters EF , Schols AM . Eff ects of whole-body exercise training on body composition and functional capacity in normal-weight patients with COPD . Chest 125 : 2021 – 28 , 2004 .
41 . Wedzicha JA , Bestall JC , Garrod R , Garnham R , Paul EA , Jones PW . Randomized controlled trial of pulmonary rehabilitation in severe chronic obstructive pulmonary disease patients, stratifi ed with the MRC dyspnoea scale . Eur Respir J 12 : 363 – 69 , 1998 .
42 . Taylor R , Dawson S , Roberts N , Sridhar M , Partridge MR . Why do patients decline to take part in a research project involving pulmonary rehabilitation? Respir Med 101 : 1942 – 46 , 2007 .
43 . Troosters T , Gosselink R , Decramer M . Exercise training in COPD: How to distinguish responders from nonresponders . J Cardiopulm Rehabil 21 : 10 – 17 , 2001 .
44 . Pitta F , Troosters T , Spruit M , Decramer M , Gosselink R . Activity monitoring for assessment of physical activities of daily life in patients with COPD . Arch Phys Med Rehabil 86 : 1979 – 85 , 2005 .
45 . Pitta F , Troosters T , Probst VS , Spruit MA , Decramer M , Gosselink R . Quantifying physical activity in daily life with questionnaires and motion sensors in COPD . Eur Respir J 27 : 1040 – 55 , 2006 .
46 . Puhan MA , Scharplatz M , Troosters T , Steurer J . Respiratory rehabili-tation after acute exacerbation of COPD may reduce risk for readmis-sion and mortality – a systematic review . Respir Res 6 : 54 , 2005 .
58Pulmonary Rehabilitation
721
47 . Man WD , Polkey MI , Donaldson N , Gray BJ , Moxham J . Community pulmonary rehabilitation after hospitalisation for acute exacerbations of chronic obstructive pulmonary disease: Randomised controlled study . BMJ 329 : 1209 , 2004 .
48 . Brug J , Schols A , Mesters I . Dietary change, nutrition education and chronic obstructive pulmonary disease . Patient Educ Couns 52 : 249 – 57 , 2004 .
49 . Young P , Dewse M , Fergusson W , Kolbe J . Respiratory rehabilitation in chronic obstructive pulmonary disease: Predictors of nonadherence . Eur Respir J 13 : 855 – 59 , 1999 .
50 . Wagena EJ , Arrindell WA , Wouters EF , van Schayck CP . Are patients with COPD psychologically distressed? Eur Respir J 26 : 242 – 48 , 2005 .
51 . Unger DG , Jacobs SB . Couples and chronic obstructive airway diseases: Th e role of gender in coping and depression . Womens Health 1 : 237 – 55 , 1995 .
52 . Lareau SC , Breslin EH , Meek PM . Functional status instruments: Outcome measure in the evaluation of patients with chronic obstructive pulmonary disease . Heart Lung 25 : 212 – 24 , 1996 .
53 . Lareau SC , Meek PM , Roos PJ . Development and testing of the modi-fi ed version of the pulmonary functional status and dyspnea question-naire (PFSDQ-M) . Heart Lung 27 : 159 – 68 , 1998 .
54 . Bernard S , Whittom F , LeBlanc P , Jobin J , Belleau R , Berube C , Carrier G , Maltais F . Aerobic and strength training in patients with chronic obstructive pulmonary disease . Am J Respir Crit Care Med 159 : 896 – 901 , 1999 .
55 . Ortega F , Toral J , Cejudo P , Villagomez R , Sanchez H , Castillo J , Montemayor T . Comparison of eff ects of strength and endurance train-ing in patients with chronic obstructive pulmonary disease . Am J Respir Crit Care Med 166 : 669 – 74 , 2002 .
56 . Spruit MA , Gosselink R , Troosters T , De Paepe C , Decramer M . Resistance versus endurance training in patients with COPD and skel-etal muscle weakness . Eur Respir J 19 : 1072 – 78 , 2002 .
57 . Maltais F , LeBlanc P , Simard C , Jobin J , Berube C , Bruneau J , Carrier L , Belleau R . Skeletal muscle adaptation to endurance training in patients with chronic obstructive pulmonary disease . Am J Respir Crit Care Med 154 : 442 – 47 , 1996 .
58 . Casaburi R , Patessio A , Ioli F , Zanaboni S , Donner CF , Wasserman K . Reductions in exercise lactic acidosis and ventilation as a result of exer-cise training in patients with obstructive lung disease . Am Rev Respir Dis 143 : 9 – 18 , 1991 .
59 . American College of Sports Medicine Position Stand. Exercise and phys-ical activity for older adults. Med Sci Sports Exerc 30: 992–1008, 1998.
60 . Casaburi R , Porszasz J , Burns MR , Carithers ER , Chang RS , Cooper CB . Physiologic benefi ts of exercise training in rehabilitation of patients with severe chronic obstructive pulmonary disease . Am J Respir Crit Care Med 155 : 1541 – 51 , 1997 .
61 . Puente-Maestu L , Sanz ML , Sanz P , Ruiz de Ona JM , Rodriguez-Hermosa JL , Whipp BJ . Eff ects of two types of training on pulmonary and cardiac responses to moderate exercise in patients with COPD . Eur Respir J 15 : 1026 – 32 , 2000 .
62 . Gimenez M , Servera E , Vergara P , Bach JR , Polu JM . Endurance train-ing in patients with chronic obstructive pulmonary disease: A compari-son of high versus moderate intensity . Arch Phys Med Rehabil 81 : 102 – 9 , 2000 .
63 . Mahler DA , Ward J , Mejia-Alfaro R . Stability of dyspnea ratings after exercise training in patients with COPD . Med Sci Sports Exerc 35 : 1083 – 87 , 2003 .
64 . Vogiatzis I , Nanas S , Roussos C . Interval training as an alternative modality to continuous exercise in patients with COPD . Eur Respir J 20 : 12 – 19 , 2002 .
65 . Vogiatzis I , Terzis G , Nanas S , Stratakos G , Simoes DC , Georgiadou O , Zakynthinos S , Roussos C . Skeletal muscle adaptations to interval training in patients with advanced COPD . Chest 128 : 3838 – 45 , 2005 .
66 . Coppoolse R , Schols AM , Baarends EM , Mostert R , Akkermans MA , Janssen PP , Wouters EF . Interval versus continuous training in patients with severe COPD: A randomized clinical trial . Eur Respir J 14 : 258 – 63 , 1999 .
67 . Puhan MA , Busching G , Schunemann HJ , VanOort E , Zaugg C , Frey M . Interval versus continuous high-intensity exercise in chronic obstructive pulmonary disease: A randomized trial . Ann Intern Med 145 : 816 – 25 , 2006 .
68 . Sabapathy S , Kingsley RA , Schneider DA , Adams L , Morris NR . Continuous and intermittent exercise responses in individuals with chronic obstructive pulmonary disease . Th orax 59 : 1026 – 31 , 2004 .
69 . Porszasz J , Emtner M , Goto S , Somfay A , Whipp BJ , Casaburi R . Exercise training decreases ventilatory requirements and exercise-induced hyperinfl ation at submaximal intensities in patients with COPD . Chest 128 : 2025 – 34 , 2005 .
70 . Somfay A , Porszasz J , Lee SM , Casaburi R . Dose–response eff ect of oxygen on hyperinfl ation and exercise endurance in nonhypoxaemic COPD patients . Eur RespirJ 18 : 77 – 84 , 2001 .
71 . Emtner M , Porszasz J , Burns M , Somfay A , Casaburi R . Benefi ts of supplemental oxygen in exercise training in non-hypoxemic COPD patients . Am J Respir Crit Care Med 168 : 1034 – 42 , 2003 .
72 . Hawkins P , Johnson LC , Nikoletou D , Hamnegard CH , Sherwood R , Polkey MI , Moxham J . Proportional assist ventilation as an aid to exer-cise training in severe chronic obstructive pulmonary disease . Th orax 57 : 853 – 59 , 2002 .
73 . Costes F , Agresti A , Court-Fortune M , Roche F , Vergnon JM , Barthelemy JC . Noninvasive ventilation during exercise training improves exercise tolerance in patients with chronic obstructive pulmo-nary disease . J Cardiopulm Rehabil 23 : 307 – 13 , 2003 .
74 . van ‘ t HA , Gosselink R , Hollander P , Postmus P , Kwakkel G . Training with inspiratory pressure support in patients with severe COPD . Eur Respir J 27 : 65 – 72 , 2006 .
75 . Bianchi L , Foglio K , Porta R , Baiardi R , Vitacca M , Ambrosino N . Lack of additional eff ect of adjunct of assisted ventilation to pulmonary rehabilitation in mild COPD patients . Respir Med 96 : 359 – 67 , 2002 .
76 . Dolmage TE , Goldstein RS . Response to one-legged cycling in patients with COPD . Chest 129 : 325 – 32 , 2006 .
77 . Dolmage TE , Goldstein RS . Eff ects of one-legged exercise training of patients with COPD . Chest 133 : 370 – 76 , 2008 .
78 . Mador MJ . Exercise training in patients with COPD: One leg is better than two? Chest 133 : 337 – 39 , 2008 .
79 . Pepin V , Saey D , Whittom F , LeBlanc P , Maltais F . Walking versus cycling: Sensitivity to bronchodilation in chronic obstructive pulmo-nary disease . Am J Respir Crit Care Med , 2005 .
80 . Casaburi R , Kukafka D , Cooper CB , Witek TJ Jr. , Kesten S . Improvement in exercise tolerance with the combination of tiotro-pium and pulmonary rehabilitation in patients with COPD . Chest 127 : 809 – 17 , 2005 .
81 . Eves ND , Petersen SR , Haykowsky MJ , Wong EY , Jones RL . Helium-hyperoxia, exercise, and respiratory mechanics in chronic obstructive pulmonary disease . Am J Respir Crit Care Med 174 : 763 – 71 , 2006 .
82 . Probst V , Troosters T , Coosemans I , Spruit M , Pitta F , Decramer M , Gosselink R . Mechanisms of improvement in exercise capacity using a rollator in COPD . Chest 126 : 1102 – 7 , 2004 .
83 . Simpson K , Killian K , McCartney N , Stubbing DG , Jones NL . Randomised controlled trial of weightlifting exercise in patients with chronic airfl ow limitation . Th orax 47 : 70 – 75 , 1992 .
84 . Mador MJ , Bozkanat E , Aggarwal A , Shaff er M , Kufel TJ . Endurance and strength training in patients with COPD . Chest 125 : 2036 – 45 , 2004 .
85 . Casaburi R , Bhasin S , Cosentino L , Porszasz J , Somfay A , Lewis M , Fournier M , Storer T . Anabolic eff ects of testosterone replacement and strength training in men with COPD . Am J Respir Crit Care Med 170 : 870 – 78 , 2004 .
86 . Neder JA , Sword D , Ward SA , Mackay E , Cochrane LM , Clark CJ . Home based neuromuscular electrical stimulation as a new rehabilita-tive strategy for severely disabled patients with chronic obstructive pul-monary disease (COPD) . Th orax 57 : 333 – 37 , 2002 .
87 . Bourjeily-Habr G , Rochester C , Palermo F , Snyder P , Mohsenin V . Randomised controlled trial of transcutaneous electrical muscle stimu-lation of the lower extremities in patients with chronic obstructive pul-monary disease . Th orax 57 : 1045 – 49 , 2002 .

Asthma and COPD: Basic Mechanisms and Clinical Management
722
88 . Zanotti E , Felicetti G , Maini M , Fracchia C . Peripheral muscle strength training in bed-bound patients with COPD receiving mechanical ven-tilation: Eff ect of electrical stimulation . Chest 124 : 292 – 96 , 2003 .
89 . Vivodtzev I , Pepin JL , Vottero G , Mayer V , Porsin B , Levy P , Wuyam B . Improvement in quadriceps strength and dyspnea in daily tasks after 1 month of electrical stimulation in severely deconditioned and malnourished COPD . Chest 129 : 1540 – 48 , 2006 .
90 . Dal CS , Napolis L , Malaguti C , Gimenes AC , Albuquerque A , Nogueira CR , De Fuccio MB , Pereira RD , Bulle A , McFarlane N , Nery LE , Neder JA . Skeletal muscle structure and function in response to electrical stimulation in moderately impaired COPD patients . Respir Med , 2006 .
91 . Maillefert JF , Eicher JC , Walker P , Dulieu V , Rouhier-Marcer I , Branly F , Cohen M , Brunotte F , Wolf JE , Casillas JM , Didier JP . Eff ects of low-frequency electrical stimulation of quadriceps and calf muscles in patients with chronic heart failure . J Cardiopulm Rehabil 18 : 277 – 82 , 1998 .
92 . Harris S , LeMaitre JP , Mackenzie G , Fox KA , Denvir MA . A ran-domised study of home-based electrical stimulation of the legs and conventional bicycle exercise training for patients with chronic heart failure . Eur Heart J 24 : 871 – 78 , 2003 .
93 . Haskell WL , Lee IM , Pate RR , Powell KE , Blair SN , Franklin BA , Macera CA , Heath GW , Th ompson PD , Bauman A . Physical activity and public health. Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association . Circulation , 2007 .
94 . Garcia-Aymerich J , Lange P , Benet M , Schnohr P , Anto JM . Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: A population-based cohort study . Th orax , 2006 .
95 . Pitta F , Troosters T , Probst V , Langer D , Decramer M , Gosselink R . Are patients with COPD more active after pulmonary rehabilitation . Chest , 2008 , E-pub ahead of Print.
96 . Sewell L , Singh SJ , Williams JE , Collier R , Morgan MD . Can indi-vidualized rehabilitation improve functional independence in elderly patients with COPD? Chest 128 : 1194 – 200 , 2005 .
97 . Mercken EM , Hageman GJ , Schols AM , Akkermans MA , Bast A , Wouters EF . Rehabilitation decreases exercise-induced oxidative stress in chronic obstructive pulmonary disease . Am J Respir Crit Care Med 172 : 994 – 1001 , 2005 .
98 . Steele BG , Belza B , Cain KC , Coppersmith J , Lakshminarayan S , Howard J , Haselkorn JK . A randomized clinical trial of an activity and exercise adherence intervention in chronic pulmonary disease . Arch Phys Med Rehabil 89 : 404 – 12 , 2008 .
99 . Coronado M , Janssens JP , de Muralt B , Terrier P , Schutz Y , Fitting JW . Walking activity measured by accelerometry during respiratory rehabilitation . J Cardiopulm Rehabil 23 : 357 – 64 , 2003 .
100 . Steele BG , Belza B , Hunziker J , Holt L , Legro M , Coppersmith J , Buchner D , Lakshminaryan S . Monitoring daily activity during pul-monary rehabilitation using a triaxial accelerometer . J Cardiopulm Rehabil 23 : 139 – 42 , 2003 .