associations between maternal fever and influenza and congenital heart defects
TRANSCRIPT

Associations Between Maternal Fever and Influenza andCongenital Heart Defects
Matthew E. Oster, MD, Tiffany Riehle-Colarusso, MD, Clinton J. Alverson, MS, and Adolfo Correa, MD, PhD
Objective To examine associations between maternal reports of prenatal fever or influenza and congenital heartdefects (CHDs), and to evaluate whether those associations varied with antipyretic use.Study designWe analyzed case infants with CHD (n = 2361) and control infants without CHD (n = 3435) from theBaltimore-Washington Infant Study (1981-1989). Participating mothers were asked whether they experienceda ‘‘fever of 101�F or higher,’’ had ‘‘influenza (flu),’’ or used an antipyretic agent (ie, acetaminophen, salicylate, or non-steroidal anti-inflammatory drug) during the period extending from 3 months before pregnancy through the end ofthe third month of pregnancy. We used logistic regression to compute ORs and 95% CIs while controlling for po-tential confounders.Results There were significant associations between fever and influenza and specific CHDs, namely right-sidedobstructive defects (fever: OR, 2.04; 95% CI, 1.27 to 3.27; influenza: OR, 1.75; 95% CI, 1.16 to 2.62) and atrioven-tricular septal defects in infantswithDown syndrome (fever: OR, 1.92; 95%CI, 1.10 to 3.38; influenza:OR, 1.66; 95%CI, 1.04 to 2.63). Maternal antipyretic use in the setting of fever or influenza tended to decrease these associations.Conclusions Prenatal maternal fever or influenza may be associated with right-sided obstructive lesions in allinfants and with atrioventricular septal defects in infants with Down syndrome. The use of antipyretics might atten-uate such associations. (J Pediatr 2011;158:990-5).
Despite numerous advances in the treatment of congenital heart disease during the past 30 years, congenital heart defects(CHDs) continue to be a leading cause of morbidity and mortality in children.1 Identification of risk factors for CHDsand subsequent efforts to prevent congenital heart disease remain important priorities for research.2
Examination of maternal exposures during pregnancy has offered some clues as to potential risk factors for CHD. Maternalfebrile illness and hyperthermia have been associated with a variety of birth defects, especially defects of the central nervoussystem.3-10 Associations of maternal fever and hyperthermia with CHD are less clear-cut, however.11-20 The association betweenCHD and some viral illnesses, particularly rubella, has been well documented,21,22 yet analyses of the role of influenza in the riskof CHD have yielded inconsistent findings.13,16,17,23 Previous reports of the associations between maternal fever or influenzaand CHD are summarized in Table I. Whether the variations in findings across studies reflect differences in studypopulations, methods, sampling variation, types of infections, or frequency and severity of febrile illness is unclear.
In the present study, we aimed to evaluate possible associations between reports of maternal fever and/or influenza dur-ing pregnancy and CHD. Furthermore, in an effort to ascertain whether any possible associations between maternal feverand/or influenza and CHD might be due to fever, we also examined the effects of antipyretic therapy on those associations.
AVSD Atrioventricular septal de
BMI Body mass index
BWIS Baltimore-Washington Inf
CHD Congenital heart defect
990
Methods
Cases and controls in this study were participants in the Baltimore-Washington Infant Study (BWIS), a population-based,case-control study among live births to residents of Maryland, Washington, DC, and northern Virginia between 1981 and1989. The BWIS data collection methods have been described in detail previously.24 Cases were infants born with structuralCHD confirmed by echocardiography, catheterization, surgery, or autopsy by 1 year of age; premature infants with patentductus arteriosus as an isolated heart defect and infants with arrhythmias in the absence of structural heart defects wereexcluded from the BWIS. Controls consisted of a random sample of live-born infants without birth defects born in theregion and frequency-matched to cases on month, year, hospital of birth, and age at interview. During the study period,
From the Division of Pediatric Cardiology, Children’sHealthcare of Atlanta, Emory University, (M.O.); and
4390 cases and 3572 controls were enrolled. Barriers to eligibility for a motherto be interviewed included a physician’s refusal to have the subject’s mothercontacted, failure to locate the mother, adoption, language barrier, death of
National Center on Birth Defects and DevelopmentalDisabilities, Centers for Disease Control and Prevention,Atlanta, GA (M.O., T.R.-C., C.A., A.C.)
The findings and conclusions in this report are those ofthe authors and do not necessarily represent the officialposition of the Centers for Disease Control and Preven-tion. The authors declare no conflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2011 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2010.11.058
fect
ant Study
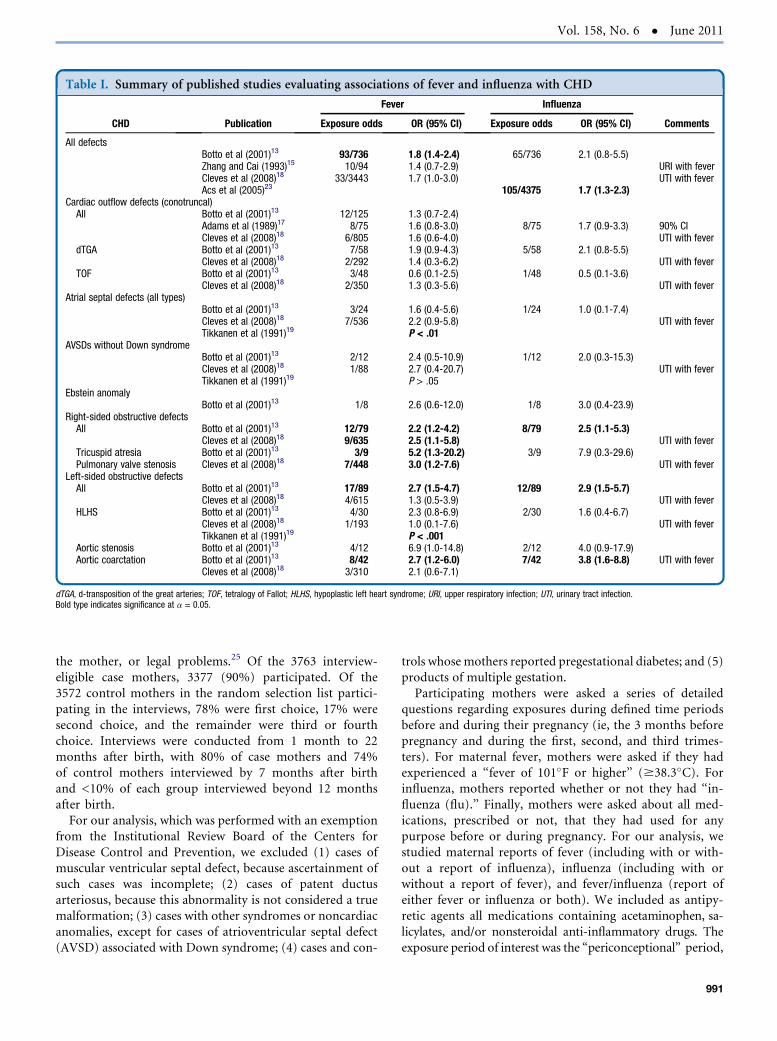
Table I. Summary of published studies evaluating associations of fever and influenza with CHD
CHD Publication
Fever Influenza
CommentsExposure odds OR (95% CI) Exposure odds OR (95% CI)
All defectsBotto et al (2001)13 93/736 1.8 (1.4-2.4) 65/736 2.1 (0.8-5.5)Zhang and Cai (1993)15 10/94 1.4 (0.7-2.9) URI with feverCleves et al (2008)18 33/3443 1.7 (1.0-3.0) UTI with feverAcs et al (2005)23 105/4375 1.7 (1.3-2.3)
Cardiac outflow defects (conotruncal)All Botto et al (2001)13 12/125 1.3 (0.7-2.4)
Adams et al (1989)17 8/75 1.6 (0.8-3.0) 8/75 1.7 (0.9-3.3) 90% CICleves et al (2008)18 6/805 1.6 (0.6-4.0) UTI with fever
dTGA Botto et al (2001)13 7/58 1.9 (0.9-4.3) 5/58 2.1 (0.8-5.5)Cleves et al (2008)18 2/292 1.4 (0.3-6.2) UTI with fever
TOF Botto et al (2001)13 3/48 0.6 (0.1-2.5) 1/48 0.5 (0.1-3.6)Cleves et al (2008)18 2/350 1.3 (0.3-5.6) UTI with fever
Atrial septal defects (all types)Botto et al (2001)13 3/24 1.6 (0.4-5.6) 1/24 1.0 (0.1-7.4)Cleves et al (2008)18 7/536 2.2 (0.9-5.8) UTI with feverTikkanen et al (1991)19 P < .01
AVSDs without Down syndromeBotto et al (2001)13 2/12 2.4 (0.5-10.9) 1/12 2.0 (0.3-15.3)Cleves et al (2008)18 1/88 2.7 (0.4-20.7) UTI with feverTikkanen et al (1991)19 P > .05
Ebstein anomalyBotto et al (2001)13 1/8 2.6 (0.6-12.0) 1/8 3.0 (0.4-23.9)
Right-sided obstructive defectsAll Botto et al (2001)13 12/79 2.2 (1.2-4.2) 8/79 2.5 (1.1-5.3)
Cleves et al (2008)18 9/635 2.5 (1.1-5.8) UTI with feverTricuspid atresia Botto et al (2001)13 3/9 5.2 (1.3-20.2) 3/9 7.9 (0.3-29.6)Pulmonary valve stenosis Cleves et al (2008)18 7/448 3.0 (1.2-7.6) UTI with fever
Left-sided obstructive defectsAll Botto et al (2001)13 17/89 2.7 (1.5-4.7) 12/89 2.9 (1.5-5.7)
Cleves et al (2008)18 4/615 1.3 (0.5-3.9) UTI with feverHLHS Botto et al (2001)13 4/30 2.3 (0.8-6.9) 2/30 1.6 (0.4-6.7)
Cleves et al (2008)18 1/193 1.0 (0.1-7.6) UTI with feverTikkanen et al (1991)19 P < .001
Aortic stenosis Botto et al (2001)13 4/12 6.9 (1.0-14.8) 2/12 4.0 (0.9-17.9)Aortic coarctation Botto et al (2001)13 8/42 2.7 (1.2-6.0) 7/42 3.8 (1.6-8.8) UTI with fever
Cleves et al (2008)18 3/310 2.1 (0.6-7.1)
dTGA, d-transposition of the great arteries; TOF, tetralogy of Fallot; HLHS, hypoplastic left heart syndrome; URI, upper respiratory infection; UTI, urinary tract infection.Bold type indicates significance at a = 0.05.
Vol. 158, No. 6 � June 2011
the mother, or legal problems.25 Of the 3763 interview-eligible case mothers, 3377 (90%) participated. Of the3572 control mothers in the random selection list partici-pating in the interviews, 78% were first choice, 17% weresecond choice, and the remainder were third or fourthchoice. Interviews were conducted from 1 month to 22months after birth, with 80% of case mothers and 74%of control mothers interviewed by 7 months after birthand <10% of each group interviewed beyond 12 monthsafter birth.
For our analysis, which was performed with an exemptionfrom the Institutional Review Board of the Centers forDisease Control and Prevention, we excluded (1) cases ofmuscular ventricular septal defect, because ascertainment ofsuch cases was incomplete; (2) cases of patent ductusarteriosus, because this abnormality is not considered a truemalformation; (3) cases with other syndromes or noncardiacanomalies, except for cases of atrioventricular septal defect(AVSD) associated with Down syndrome; (4) cases and con-
trols whose mothers reported pregestational diabetes; and (5)products of multiple gestation.Participating mothers were asked a series of detailed
questions regarding exposures during defined time periodsbefore and during their pregnancy (ie, the 3 months beforepregnancy and during the first, second, and third trimes-ters). For maternal fever, mothers were asked if they hadexperienced a ‘‘fever of 101�F or higher’’ ($38.3�C). Forinfluenza, mothers reported whether or not they had ‘‘in-fluenza (flu).’’ Finally, mothers were asked about all med-ications, prescribed or not, that they had used for anypurpose before or during pregnancy. For our analysis, westudied maternal reports of fever (including with or with-out a report of influenza), influenza (including with orwithout a report of fever), and fever/influenza (report ofeither fever or influenza or both). We included as antipy-retic agents all medications containing acetaminophen, sa-licylates, and/or nonsteroidal anti-inflammatory drugs. Theexposure period of interest was the ‘‘periconceptional’’ period,
991
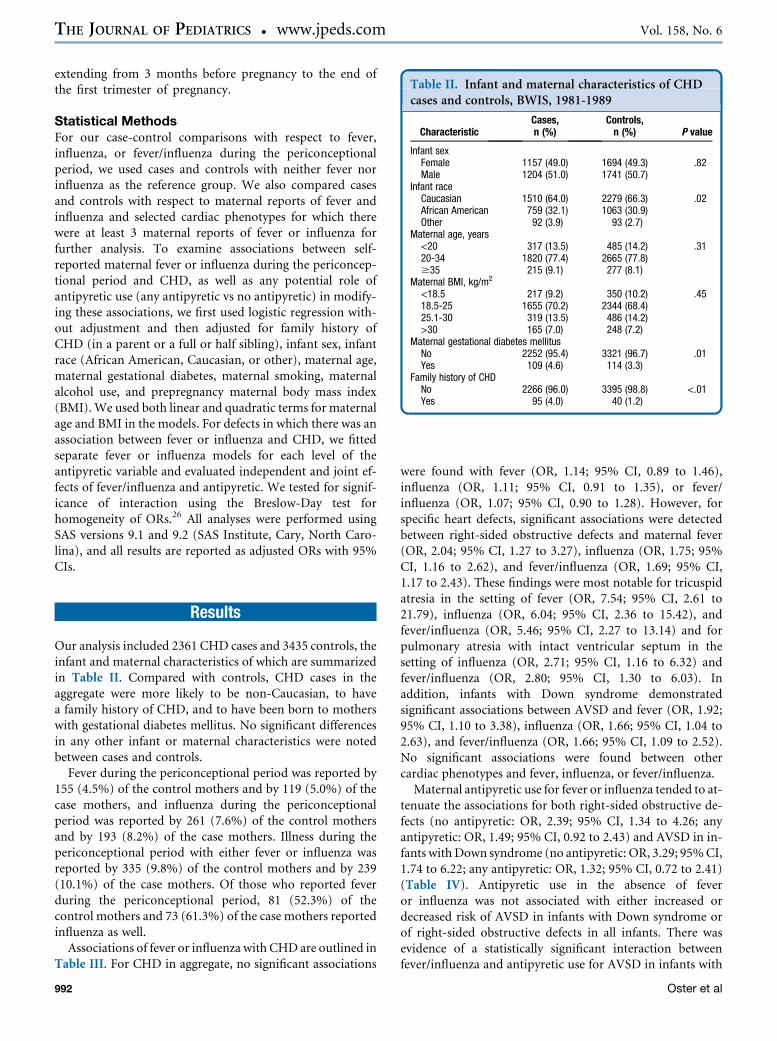
Table II. Infant and maternal characteristics of CHDcases and controls, BWIS, 1981-1989
CharacteristicCases,n (%)
Controls,n (%) P value
Infant sexFemale 1157 (49.0) 1694 (49.3) .82Male 1204 (51.0) 1741 (50.7)
Infant raceCaucasian 1510 (64.0) 2279 (66.3) .02African American 759 (32.1) 1063 (30.9)Other 92 (3.9) 93 (2.7)
Maternal age, years<20 317 (13.5) 485 (14.2) .3120-34 1820 (77.4) 2665 (77.8)$35 215 (9.1) 277 (8.1)
Maternal BMI, kg/m2
<18.5 217 (9.2) 350 (10.2) .4518.5-25 1655 (70.2) 2344 (68.4)25.1-30 319 (13.5) 486 (14.2)>30 165 (7.0) 248 (7.2)
Maternal gestational diabetes mellitusNo 2252 (95.4) 3321 (96.7) .01Yes 109 (4.6) 114 (3.3)
Family history of CHDNo 2266 (96.0) 3395 (98.8) <.01Yes 95 (4.0) 40 (1.2)
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 158, No. 6
extending from 3 months before pregnancy to the end ofthe first trimester of pregnancy.
Statistical MethodsFor our case-control comparisons with respect to fever,influenza, or fever/influenza during the periconceptionalperiod, we used cases and controls with neither fever norinfluenza as the reference group. We also compared casesand controls with respect to maternal reports of fever andinfluenza and selected cardiac phenotypes for which therewere at least 3 maternal reports of fever or influenza forfurther analysis. To examine associations between self-reported maternal fever or influenza during the periconcep-tional period and CHD, as well as any potential role ofantipyretic use (any antipyretic vs no antipyretic) in modify-ing these associations, we first used logistic regression with-out adjustment and then adjusted for family history ofCHD (in a parent or a full or half sibling), infant sex, infantrace (African American, Caucasian, or other), maternal age,maternal gestational diabetes, maternal smoking, maternalalcohol use, and prepregnancy maternal body mass index(BMI). We used both linear and quadratic terms for maternalage and BMI in the models. For defects in which there was anassociation between fever or influenza and CHD, we fittedseparate fever or influenza models for each level of theantipyretic variable and evaluated independent and joint ef-fects of fever/influenza and antipyretic. We tested for signif-icance of interaction using the Breslow-Day test forhomogeneity of ORs.26 All analyses were performed usingSAS versions 9.1 and 9.2 (SAS Institute, Cary, North Caro-lina), and all results are reported as adjusted ORs with 95%CIs.
Results
Our analysis included 2361 CHD cases and 3435 controls, theinfant and maternal characteristics of which are summarizedin Table II. Compared with controls, CHD cases in theaggregate were more likely to be non-Caucasian, to havea family history of CHD, and to have been born to motherswith gestational diabetes mellitus. No significant differencesin any other infant or maternal characteristics were notedbetween cases and controls.
Fever during the periconceptional period was reported by155 (4.5%) of the control mothers and by 119 (5.0%) of thecase mothers, and influenza during the periconceptionalperiod was reported by 261 (7.6%) of the control mothersand by 193 (8.2%) of the case mothers. Illness during thepericonceptional period with either fever or influenza wasreported by 335 (9.8%) of the control mothers and by 239(10.1%) of the case mothers. Of those who reported feverduring the periconceptional period, 81 (52.3%) of thecontrol mothers and 73 (61.3%) of the case mothers reportedinfluenza as well.
Associations of fever or influenza with CHD are outlined inTable III. For CHD in aggregate, no significant associations
992
were found with fever (OR, 1.14; 95% CI, 0.89 to 1.46),influenza (OR, 1.11; 95% CI, 0.91 to 1.35), or fever/influenza (OR, 1.07; 95% CI, 0.90 to 1.28). However, forspecific heart defects, significant associations were detectedbetween right-sided obstructive defects and maternal fever(OR, 2.04; 95% CI, 1.27 to 3.27), influenza (OR, 1.75; 95%CI, 1.16 to 2.62), and fever/influenza (OR, 1.69; 95% CI,1.17 to 2.43). These findings were most notable for tricuspidatresia in the setting of fever (OR, 7.54; 95% CI, 2.61 to21.79), influenza (OR, 6.04; 95% CI, 2.36 to 15.42), andfever/influenza (OR, 5.46; 95% CI, 2.27 to 13.14) and forpulmonary atresia with intact ventricular septum in thesetting of influenza (OR, 2.71; 95% CI, 1.16 to 6.32) andfever/influenza (OR, 2.80; 95% CI, 1.30 to 6.03). Inaddition, infants with Down syndrome demonstratedsignificant associations between AVSD and fever (OR, 1.92;95% CI, 1.10 to 3.38), influenza (OR, 1.66; 95% CI, 1.04 to2.63), and fever/influenza (OR, 1.66; 95% CI, 1.09 to 2.52).No significant associations were found between othercardiac phenotypes and fever, influenza, or fever/influenza.Maternal antipyretic use for fever or influenza tended to at-
tenuate the associations for both right-sided obstructive de-fects (no antipyretic: OR, 2.39; 95% CI, 1.34 to 4.26; anyantipyretic: OR, 1.49; 95% CI, 0.92 to 2.43) and AVSD in in-fants withDown syndrome (no antipyretic: OR, 3.29; 95%CI,1.74 to 6.22; any antipyretic: OR, 1.32; 95% CI, 0.72 to 2.41)(Table IV). Antipyretic use in the absence of feveror influenza was not associated with either increased ordecreased risk of AVSD in infants with Down syndrome orof right-sided obstructive defects in all infants. There wasevidence of a statistically significant interaction betweenfever/influenza and antipyretic use for AVSD in infants with
Oster et al
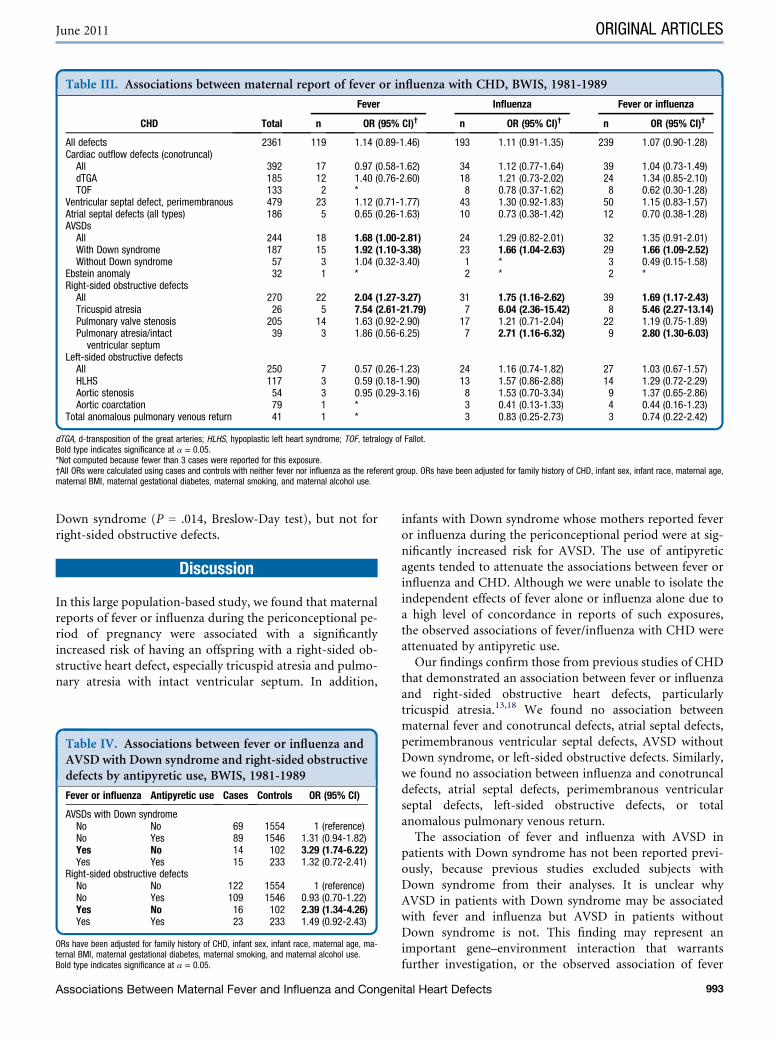
Table III. Associations between maternal report of fever or influenza with CHD, BWIS, 1981-1989
CHD Total
Fever Influenza Fever or influenza
n OR (95% CI)† n OR (95% CI)† n OR (95% CI)†
All defects 2361 119 1.14 (0.89-1.46) 193 1.11 (0.91-1.35) 239 1.07 (0.90-1.28)Cardiac outflow defects (conotruncal)All 392 17 0.97 (0.58-1.62) 34 1.12 (0.77-1.64) 39 1.04 (0.73-1.49)dTGA 185 12 1.40 (0.76-2.60) 18 1.21 (0.73-2.02) 24 1.34 (0.85-2.10)TOF 133 2 * 8 0.78 (0.37-1.62) 8 0.62 (0.30-1.28)
Ventricular septal defect, perimembranous 479 23 1.12 (0.71-1.77) 43 1.30 (0.92-1.83) 50 1.15 (0.83-1.57)Atrial septal defects (all types) 186 5 0.65 (0.26-1.63) 10 0.73 (0.38-1.42) 12 0.70 (0.38-1.28)AVSDsAll 244 18 1.68 (1.00-2.81) 24 1.29 (0.82-2.01) 32 1.35 (0.91-2.01)With Down syndrome 187 15 1.92 (1.10-3.38) 23 1.66 (1.04-2.63) 29 1.66 (1.09-2.52)Without Down syndrome 57 3 1.04 (0.32-3.40) 1 * 3 0.49 (0.15-1.58)
Ebstein anomaly 32 1 * 2 * 2 *Right-sided obstructive defectsAll 270 22 2.04 (1.27-3.27) 31 1.75 (1.16-2.62) 39 1.69 (1.17-2.43)Tricuspid atresia 26 5 7.54 (2.61-21.79) 7 6.04 (2.36-15.42) 8 5.46 (2.27-13.14)Pulmonary valve stenosis 205 14 1.63 (0.92-2.90) 17 1.21 (0.71-2.04) 22 1.19 (0.75-1.89)Pulmonary atresia/intact
ventricular septum39 3 1.86 (0.56-6.25) 7 2.71 (1.16-6.32) 9 2.80 (1.30-6.03)
Left-sided obstructive defectsAll 250 7 0.57 (0.26-1.23) 24 1.16 (0.74-1.82) 27 1.03 (0.67-1.57)HLHS 117 3 0.59 (0.18-1.90) 13 1.57 (0.86-2.88) 14 1.29 (0.72-2.29)Aortic stenosis 54 3 0.95 (0.29-3.16) 8 1.53 (0.70-3.34) 9 1.37 (0.65-2.86)Aortic coarctation 79 1 * 3 0.41 (0.13-1.33) 4 0.44 (0.16-1.23)
Total anomalous pulmonary venous return 41 1 * 3 0.83 (0.25-2.73) 3 0.74 (0.22-2.42)
dTGA, d-transposition of the great arteries; HLHS, hypoplastic left heart syndrome; TOF, tetralogy of Fallot.Bold type indicates significance at a = 0.05.*Not computed because fewer than 3 cases were reported for this exposure.†All ORs were calculated using cases and controls with neither fever nor influenza as the referent group. ORs have been adjusted for family history of CHD, infant sex, infant race, maternal age,maternal BMI, maternal gestational diabetes, maternal smoking, and maternal alcohol use.
June 2011 ORIGINAL ARTICLES
Down syndrome (P = .014, Breslow-Day test), but not forright-sided obstructive defects.
Discussion
In this large population-based study, we found that maternalreports of fever or influenza during the periconceptional pe-riod of pregnancy were associated with a significantlyincreased risk of having an offspring with a right-sided ob-structive heart defect, especially tricuspid atresia and pulmo-nary atresia with intact ventricular septum. In addition,
Table IV. Associations between fever or influenza andAVSD with Down syndrome and right-sided obstructivedefects by antipyretic use, BWIS, 1981-1989
Fever or influenza Antipyretic use Cases Controls OR (95% CI)
AVSDs with Down syndromeNo No 69 1554 1 (reference)No Yes 89 1546 1.31 (0.94-1.82)Yes No 14 102 3.29 (1.74-6.22)Yes Yes 15 233 1.32 (0.72-2.41)
Right-sided obstructive defectsNo No 122 1554 1 (reference)No Yes 109 1546 0.93 (0.70-1.22)Yes No 16 102 2.39 (1.34-4.26)Yes Yes 23 233 1.49 (0.92-2.43)
ORs have been adjusted for family history of CHD, infant sex, infant race, maternal age, ma-ternal BMI, maternal gestational diabetes, maternal smoking, and maternal alcohol use.Bold type indicates significance at a = 0.05.
Associations Between Maternal Fever and Influenza and Congen
infants with Down syndrome whose mothers reported feveror influenza during the periconceptional period were at sig-nificantly increased risk for AVSD. The use of antipyreticagents tended to attenuate the associations between fever orinfluenza and CHD. Although we were unable to isolate theindependent effects of fever alone or influenza alone due toa high level of concordance in reports of such exposures,the observed associations of fever/influenza with CHD wereattenuated by antipyretic use.Our findings confirm those from previous studies of CHD
that demonstrated an association between fever or influenzaand right-sided obstructive heart defects, particularlytricuspid atresia.13,18 We found no association betweenmaternal fever and conotruncal defects, atrial septal defects,perimembranous ventricular septal defects, AVSD withoutDown syndrome, or left-sided obstructive defects. Similarly,we found no association between influenza and conotruncaldefects, atrial septal defects, perimembranous ventricularseptal defects, left-sided obstructive defects, or totalanomalous pulmonary venous return.The association of fever and influenza with AVSD in
patients with Down syndrome has not been reported previ-ously, because previous studies excluded subjects withDown syndrome from their analyses. It is unclear whyAVSD in patients with Down syndrome may be associatedwith fever and influenza but AVSD in patients withoutDown syndrome is not. This finding may represent animportant gene–environment interaction that warrantsfurther investigation, or the observed association of fever
ital Heart Defects 993

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 158, No. 6
with AVSD in patients with Down syndrome may bespurious. Conversely, given the small number of patientswith AVSD without Down syndrome, the present studymight have been underpowered to detect an association offever and influenza with AVSD in this population.
Our results differ appreciably from those in previousreports in two ways. First, even though some previous studieshave noted almost a 2-fold increase in the risk of CHD inaggregate in association withmaternal fever13 and influenza,23
we found no statistically significant association between CHDin the aggregate and maternal reports of fever or influenza.Second, in contrast to studies that reported an increased riskof left-sided lesions in association with fever13,19 andinfluenza,13 we found no such evidence.
With respect to fever, two factors might potentiallyaccount for the differences between our findings andprevious reports. First, in the present study, exposure to feverwas specifically defined as a report of temperature of$101�F,whereas in previous studies fever either was not specificallydefined13 or encompassed a broader temperature range (ie,$38�C [100.4�F]).19 Second, the results of our study, whichinvolved a large number of subjects, are similar to those ofanother large study18 as opposed to smaller studies with con-trasting findings, which might have been influenced bygreater sampling variability.13,19
With respect to influenza, we did not find an associationwith left-sided obstructive defects as was noted in another,smaller study.13 In contrast to our study, a previous largerstudy found an increased risk for CHD in aggregate followingmaternal exposure to influenza.23 We would have liked tocompare the defect-specific exposures to see in which areasour results agreed with or differed from those in the earlierstudy, but defect-specific results were not reported in thatstudy. Interestingly, although that study’s investigators didnot report any associationwith fever, they didnote a decreasedrisk of CHD when exposed mothers were treated with antipy-retic agents, suggesting that any possible association with in-fluenza might be related to the concomitant occurrence offever.23
The role of maternal antipyretic use in the development ofCHD remains controversial. Some studies have suggesteda possible association between antipyretic use and CHD, es-pecially in animals,27 whereas others have found no increasedrisk of CHD in the offspring of mothers who used antipyreticagents during pregnancy.11 For those cardiac phenotypes as-sociated with maternal fever or influenza, we found that an-tipyretic use might offer a protective effect. This finding is inagreement with that of two previous studies of mothers inHungary23,28 and suggests that symptomatic treatment of fe-brile illness and influenza in pregnant women might havebeneficial effects on the developing fetus. The National BirthDefects Prevention Study found a possible decreased risk ofnoncardiac malformation in offspring of women who tookacetaminophen for a febrile illness during the first trimesterof pregnancy.29
The possible mechanisms underlying the associationsobserved between maternal fever or influenza and specific
994
types of CHD are unclear. Numerous studies have suggestedthat hyperthermia may lead to cell death.4,30,31 Specifically,hyperthermia has been shown to lead to vascular abnormal-ities in chick embryos.32,33 Similarly, influenza infection hasbeen shown to lead to cell death in human cells in vitro34 andin mice in vivo,35 but this has not been as well studied as hy-perthermia in pregnancy.The present study has several strengths. We evaluated the
associations of maternal fever with CHD in the aggregate aswell as with specific cardiac defects diagnosed by objectivemethods. Because our survey instrument asked specificallywhether mothers had a temperature of$101�F, respondentswere unlikely to misinterpret tactile hyperthermia as truefever.36 The study also has several limitations. First, we mighthave incorrectly estimated the number of case and controlmothers actually affected by fever, influenza, or antipyreticuse. For fever, we might have misclassified mothers as havingno fever when in fact they had a temperature of $101�F butdid not use a thermometer to record an elevated temperature.Conversely, for influenza, we might have misclassified caseand control mothers, given that mothers were asked subjec-tively whether they had influenza, with no confirmatory diag-nostic assessment required. For antipyretic use, somemothers might have failed to recall which medications thatthey used. Regardless of these issues, however, the net effectof such exposure misclassifications occurring independentof case–control status would be to attenuate any real associa-tions between the exposures of interest and cardiac defects.Second, the BWIS questionnaire categorized exposures into3-month intervals before and during pregnancy, limitingour ability to identify the precise timing of events. We at-tempted to minimize this limitation by including exposuresthat might have occurred before a mother knew she was preg-nant and by not including exposures occurring after the firsttrimester. Third, because our survey instrument did not allowfor ascertainment of the duration of fever, the magnitude oftemperature elevation, or the number of instances of feverin the period of interest, we were unable to assess any poten-tial dose–response associations between fever and CHD thatmight exist. Finally, recall bias is always a concern in case-control studies involving interviews on prenatal exposuresconducted after birth. Although recall bias cannot beexcluded with certainty, if recall bias for fever or influenzawere a significant factor, then we would expect to see signifi-cant associations of fever or influenza with CHD in theaggregate or with various other specific defects in additionto right-sided obstructive defects and AVSD.Our findings provide additional evidence that maternal
fever or influenza during the periconceptional period of 3months before conception to 3 months after conceptionmay be associated with the development of certain CHD phe-notypes, most notably right-sided obstructive lesions andAVSD in infants with Down syndrome. Future studies arewarranted to corroborate these findings and to elucidatethe possible reasons for the associations of maternal feveror influenza with CHD. In the meantime, efforts to preventinfluenza and other febrile illnesses in pregnant women and
Oster et al

June 2011 ORIGINAL ARTICLES
to treat women with such illnesses with antipyretic agentsmay help decrease the prevalence of some types of CHD. n
Submitted for publication Jul 2, 2010; last revision received Oct 22, 2010;
accepted Nov 22, 2010.
Reprint requests: Matthew Oster, MD, Division of Pediatric Cardiology,
Children’s Healthcare of Atlanta, 1405 Clifton Road NE, Atlanta, GA 30322.
E-mail: [email protected]
References
1. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB,
Flegal K, et al. Heart disease and stroke statistics—2009 update: a report
from the American Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Circulation 2009;119:480-6.
2. Jenkins KJ, Correa A, Feinstein JA, Botto L, Britt AE, Daniels SR,
et al. Noninherited risk factors and congenital cardiovascular defects:
current knowledge. A scientific statement from the American Heart
Association Council on Cardiovascular Disease in the Young: en-
dorsed by the American Academy of Pediatrics. Circulation 2007;
115:2995-3014.
3. Chambers CD, Johnson KA, Dick LM, Felix RJ, Jones KL. Maternal fever
and birth outcome: a prospective study. Teratology 1998;58:251-7.
4. Edwards MJ. Apoptosis, the heat shock response, hyperthermia, birth
defects, disease and cancer: where are the common links? Cell Stress
Chaperones 1998;3:213-20.
5. Edwards MJ. Review: hyperthermia and fever during pregnancy. Birth
Defects Res A Clin Mol Teratol 2006;76:507-16.
6. Graham JM, Jr., Edwards MJ, Edwards MJ. Teratogen update:
gestational effects of maternal hyperthermia due to febrile illnesses and
resultant patterns of defects in humans. Teratology 1998;58:209-21.
7. Lynberg MC, Khoury MJ, Lu X, Cocian T. Maternal flu, fever, and the
risk of neural tube defects: a population-based case-control study. Am
J Epidemiol 1994;140:244-55.
8. Moretti ME, Bar-Oz B, Fried S, Koren G.Maternal hyperthermia and the
risk for neural tube defects in offspring: systematic review and meta-
analysis. Epidemiology 2005;16:216-9.
9. Smith MS, Edwards MJ, Upfold JB. The effects of hyperthermia on the
fetus. Dev Med Child Neurol 1986;28:806-9.
10. Shahrukh Hashmi S, Gallaway MS, Waller DK, Langlois PH, Hecht JT.
Maternal fever during early pregnancy and the risk of oral clefts. Birth
Defects Res A Clin Mol Teratol 2010;88:186-94.
11. Cleves MA, Savell VH, Jr., Raj S, Zhao W, Correa A, Werler MM, et al.
Maternal use of acetaminophen and nonsteroidal anti-inflammatory
drugs (NSAIDS), and muscular ventricular septal defects. Birth Defects
Res A Clin Mol Teratol 2004;70:107-13.
12. Lipson AH, EdwardsMJ.Maternal sauna and hyperthermia during preg-
nancy and cardiovascular and other malformations in offspring. Eur J
Epidemiol 1993;9:676-8.
13. Botto LD, Lynberg MC, Erickson JD. Congenital heart defects, maternal
febrile illness, andmultivitamin use: a population-based study. Epidemi-
ology 2001;12:485-90.
14. Botto LD, Erickson JD, Mulinare J, Lynberg MC, Liu Y. Maternal fever,
multivitamin use, and selected birth defects: evidence of interaction? Ep-
idemiology 2002;13:485-8.
15. Zhang J, Cai WW. Association of the common cold in the first trimester
of pregnancy with birth defects. Pediatrics 1993;92:559-63.
16. Erickson JD. Risk factors for birth defects: data from the atlanta birth de-
fects case-control study. Teratology 1991;43:41-51.
Associations Between Maternal Fever and Influenza and Congen
17. Adams MM, Mulinare J, Dooley K. Risk factors for conotruncal cardiac
defects in Atlanta. J Am Coll Cardiol 1989;14:432-42.
18. Cleves MA, Malik S, Yang S, Carter TC, Hobbs CA. Maternal urinary
tract infections and selected cardiovascular malformations. Birth Defects
Res A Clin Mol Teratol 2008;82:464-73.
19. Tikkanen J, Heinonen OP. Maternal hyperthermia during pregnancy
and cardiovascular malformations in the offspring. Eur J Epidemiol
1991;7:628-35.
20. Czeizel AE. Specified critical period of different congenital abnormali-
ties: a new approach for human teratological studies. Congenit Anom
(Kyoto) 2008;48:103-9.
21. Rosenberg HS. Cardiovascular effects of congenital infections. Am J Car-
diovasc Patholo 1987;1:147-56.
22. Oster ME, Riehle-Colarusso T, Correa A. An update on cardiovascular
malformations in congenital rubella syndrome. Birth Defects Res A
Clin Mol Teratol 2009;88:1-8.
23. Acs N, Banhidy F, Puho E, Czeizel AE. Maternal influenza during preg-
nancy and risk of congenital abnormalities in offspring. Birth Defects Res
A Clin Mol Teratol 2005;73:989-96.
24. Ferencz C, Loffredo CA, Correa-Villasenor A, Wilson PD. Genetic and
Environmental Risk Factors of Major Congenital Heart Disease: The
Baltimore-Washington Infant Study, 1981-1989. Perspectives in
Pediatric Cardiology. Mount Kisco, NY: Futura Publishing; 1997.
25. Correa-VillasenorA,McCarter R,Downing J, FerenczC, Baltimore-Wash-
ington Infant StudyGroup.White-black differences in cardiovascularmal-
formations in infancy and socioeconomic factors. Am J Epidemiol 1991;
134:393-402.
26. Breslow NE, Day NE. Statistical Methods in Cancer Research, Vol I:
Analysis of Case-Control Studies. Lyon, France: IARC Science Pub-
lishers; 1980. p. 338.
27. Burdan F, Szumilo J, Dudka J, Korobowicz A, Klepacz R. Congenital
ventricular septal defects and prenatal exposure to cyclooxygenase
inhibitors. Brazil J Med Biol Res 2006;39:925-34.
28. Czeizel AE, Puho EH, Acs N, Banhidy F. High-fever–related maternal
diseases as possible causes of multiple congenital abnormalities:
a population-based case-control study. Birth Defects Res A Clin Mol
Teratol 2007;79:544-51.
29. Feldkamp ML, Meyer RE, Krikov S, Botto LD. Acetaminophen use in
pregnancy and risk of birth defects: findings from the National Birth De-
fects Prevention Study. Obstet Gynecol 2010;115:109-15.
30. Mirkes PE, Cornel LM, Park HW, Cunningham ML. Induction of ther-
motolerance in early postimplantation rat embryos is associated with in-
creased resistance to hyperthermia-induced apoptosis. Teratology 1997;
56:210-9.
31. Roulston A, Marcellus RC, Branton PE. Viruses and apoptosis. Annu
Rev Microbiol 1999;53:577-628.
32. Nilsen NO. Vascular abnormalities due to hyperthermia in chick
embryos. Teratology 1984;30:237-51.
33. Nilsen NO. Endothelial changes and microvascular leakage due to
hyperthermia in chick embryos. Virchows Archiv 1984;46:165-74.
34. Takizawa T, Ohashi K, Nakanishi Y. Possible involvement of double-
stranded RNA-activated protein kinase in cell death by influenza virus
infection. J Virol 1996;70:8128-32.
35. Mori I, Komatsu T, Takeuchi K, Nakakuki K, SudoM, Kimura Y. In vivo
induction of apoptosis by influenza virus. J Gen Virol 1995;76(Pt 11):
2869-73.
36. Singh M, Pai M, Kalantri SP. Accuracy of perception and touch for
detecting fever in adults: a hospital-based study from a rural,
tertiary hospital in central India. Trop Med Int Health 2003;8:
408-14.
ital Heart Defects 995