assessing older adults - inspiring...
TRANSCRIPT

Assessing older adults
Julie Daltrey NP (Older Adult)
Juliedaltreywaikatodhbhealthnz
021 2235917
World Population Ageing 1950-2050 (United Nations 20022013)
bull UNPARALLELEC ENDURING
bull AGED ARE AGEING - 80+ age group triple
bull GLOBAL by 2047 8 our of 10 OA will live in developing world
bull ROOT CAUSES decrease fertility rates increase life expectancy
bull PUBLIC HEALTH SANITATION ndash people no longer dying of infections
Australia NZ India USA China
Life expectancy and cause of death in NZ
Life expectancy by age Cause of death
httpwwwworldlifeexpectancycomcountry-health-profilenew-zealand
Population ageing NZ
bull Between 1980 - 1998 mortality decreased
37 for the 75minus84
35 for 85 +
If we fix
bull Cancer uarr life expectancy by 37yr Male amp 39 yr Female
bull Ischaemic heart disease uarrlife expectancy by 36 yr M and 27 yr F
bull Stroke uarrlife expectancy 08 yr M and 13 yr F
Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
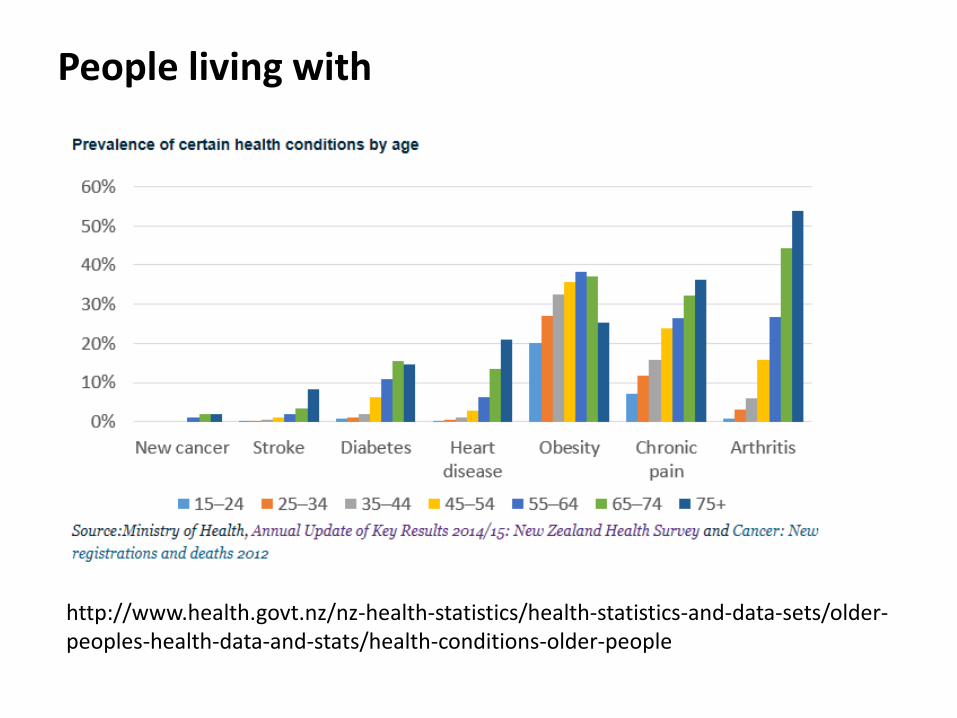
People living with
httpwwwhealthgovtnznz-health-statisticshealth-statistics-and-data-setsolder-peoples-health-data-and-statshealth-conditions-older-people
Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

World Population Ageing 1950-2050 (United Nations 20022013)
bull UNPARALLELEC ENDURING
bull AGED ARE AGEING - 80+ age group triple
bull GLOBAL by 2047 8 our of 10 OA will live in developing world
bull ROOT CAUSES decrease fertility rates increase life expectancy
bull PUBLIC HEALTH SANITATION ndash people no longer dying of infections
Australia NZ India USA China
Life expectancy and cause of death in NZ
Life expectancy by age Cause of death
httpwwwworldlifeexpectancycomcountry-health-profilenew-zealand
Population ageing NZ
bull Between 1980 - 1998 mortality decreased
37 for the 75minus84
35 for 85 +
If we fix
bull Cancer uarr life expectancy by 37yr Male amp 39 yr Female
bull Ischaemic heart disease uarrlife expectancy by 36 yr M and 27 yr F
bull Stroke uarrlife expectancy 08 yr M and 13 yr F
Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
People living with
httpwwwhealthgovtnznz-health-statisticshealth-statistics-and-data-setsolder-peoples-health-data-and-statshealth-conditions-older-people
Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Life expectancy and cause of death in NZ
Life expectancy by age Cause of death
httpwwwworldlifeexpectancycomcountry-health-profilenew-zealand
Population ageing NZ
bull Between 1980 - 1998 mortality decreased
37 for the 75minus84
35 for 85 +
If we fix
bull Cancer uarr life expectancy by 37yr Male amp 39 yr Female
bull Ischaemic heart disease uarrlife expectancy by 36 yr M and 27 yr F
bull Stroke uarrlife expectancy 08 yr M and 13 yr F
Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
People living with
httpwwwhealthgovtnznz-health-statisticshealth-statistics-and-data-setsolder-peoples-health-data-and-statshealth-conditions-older-people
Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Population ageing NZ
bull Between 1980 - 1998 mortality decreased
37 for the 75minus84
35 for 85 +
If we fix
bull Cancer uarr life expectancy by 37yr Male amp 39 yr Female
bull Ischaemic heart disease uarrlife expectancy by 36 yr M and 27 yr F
bull Stroke uarrlife expectancy 08 yr M and 13 yr F
Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
People living with
httpwwwhealthgovtnznz-health-statisticshealth-statistics-and-data-setsolder-peoples-health-data-and-statshealth-conditions-older-people
Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts
People living with
httpwwwhealthgovtnznz-health-statisticshealth-statistics-and-data-setsolder-peoples-health-data-and-statshealth-conditions-older-people
Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Population ageing amp service use NZ
bull 65-74 yrs visit GP 6-7 times a year
bull 85+ visit GP 9 times a year
bull 32 hospital admission are people aged 65 and over
bull For circulatory system disease amp MSK issues (amp gen unwell)
bull LOS has been decreasing with a corresponding increase in day cases
bull Impact of Population Ageing in New Zealand on the Demand for Health and Disability Support Services
and Workforce Implications Justine Cornwall and Judith A Davey 2004 httpswwwhealthgovtnzsystemfilesdocumentspublicationscornwallanddaveypdf
Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Assessment of complex elderly
bull Medically
bull Socially
bull Functionally
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts
It is a multidimensional multidisciplinary diagnostic
instrument designed to collect data on the medical
psychosocial and functional capabilities and limitations of
older adults in order to develop a coordinated and
integrated plan for treatment and long term follow up
bull Different from a standard medical evaluation in 3 ways
(1) focuses on older adults with complex problems
(2) emphasizes functional status and quality of life
(3) frequently uses an interdisciplinary team of providers
Comprehensive geriatric assessment
bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull OA in hospital less likely to (a) die or experience functional
deterioration (b) to be admitted to an institution and more
likely to be alive in their own homes at 12 month follow up
(Ellis)
bull Frail OA with coordinated care based on CGA have improved
outcomes amp darr unnecessary hospital admissions (Boult)
bull 75+ preventive home visits based on CGA less decline in
functional status amp prevent ARRC admission (huss)
Why Comprehensive geriatric assessment
bullEllis G Whitehead MA Robinson D OrsquoNeill D Langhorne P Comprehensive geriatric assessment for older adults admitted to hospital meta-analysis of randomised controlled trials BMJ
bullBoult C Green AF Boult LB Pacala JT Snyder C Leff B Successful models of comprehensive care for older adults with chronic conditions evidence for the Institute of Medicinersquos ldquoretooling for an aging Americardquo report J Am Geriatr Soc-
bullHuss A Stuck AE Rubenstein LZ Egger M Clough-Gorr KM Multidimensional geriatric assessment back to the future Multidimensional preventive home visit programs for community dwelling older adults a systematic review and meta-analysis of randomized controlled trials [published correction in 200964318] 63298-307
bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull develop treatment amp long-term follow-up plans
bull arrange for primary care amp rehabilitative services
bull organize amp facilitate case management
bull determine long-term care requirements amp optimal
placement
bull make the best use of health care resources
Goal of Comprehensive geriatric assessment
Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Process of Comprehensive geriatric assessment
1 Gather data
2 Discuss with team
3 Develop treatment plan
4 Implementation plan
5 Monitorevaluate response
6 Revise plan
(so itrsquos the nursing process)
Use of validated tools to gather a complete picture of the older personrsquos
ndash medical health
ndash physical function
ndash psychological function
ndash social function
bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull Medical health
Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Multiple morbidity in Hospitalised Older Patients Who Are the Complex Elderly (medically)
bull Retrospective UK study 2012-13 every hospital admission for 65+
bull MM common 63 ge 2 conditions
bull Multiple MM less common 5 ge 6 condition
bull MM (ge 2) more common with age 50 of 65-69 yr and 67 of 80-84 yr
Distinct groups
- Group 1 (MM le2) Ca andor metastasis
- Group 2 (MM of 3 4 or 5) COPD lung disease rheumtm amp osteoporosis
- Group 3 (MM ge6) HF CVA DM HTN amp MI
Concluded
bull Group 2 and 3 complex elderly ndash if can predict can target resource
Ruiz M Bottle A Long S Aylin P (2015) Multi-Morbidity in Hospitalised Older Patients Who Are the Complex Elderly PLoS ONE 10(12) e0145372 ttpsdoiorg101371journalpone0145372
Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Multi morbidity is associated with elevated risk of death disability poor functional status poor quality of life and adverse drug events (USA epidemiology study)
bull Marcel E Salive Multimorbidity in Older Adults Epidemiol Rev 2013 35 (1) 75-83 doi 101093epirevmxs009
bull So what if we identified them at triage (hospital primary care)
Identifying vulnerable older adults (triage screen) tick
Known cognitive impairment mental health condition
Require assistance with showering dressing
Poor mobility
2 or more ED presentations in last 6 months
A progressive neurological condition
brittle social support system lives alone
Multiple morbidity
Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Why do older people with multi-morbidity experience unplanned hospital admissions from community a RCA (Reed R
Isherwood L Ben-Tovim D (2015) BMC Health Services Research 15525
bull 36 pts 70+yrs ndash interviews family GPs specialists amp hosp records review
1 a consequence of minimal care 2 progression of disease 3 home care accessibility 4 high complexity 5 clinical error 6 delayed care-seeking by the patient
Previous Systematic review reason for ED visit by Older Adultsrsquo
1 perceived and actual poor health status
2 previous hospitalED use
3 Lack primary health care access
McCusker J Karp I Cardin S Durand P Morin J Determinants of emergency department visits by
older adults a systematic review Acad Emerg Med 200310(12)1362ndash70
Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Patient‐Centered Care for Older Adults with Multiple Chronic Conditions A Stepwise Approach from the American Geriatrics Society
1 Primary concern
2 current treatment working
3 Patient prefs
4 Is there relevant evident
5 Consider prognosis
6 Interactions between treatment and conditions
7 Benefits and harms
8 Communicate decide
9 Reassess
Journal of the American Geriatrics Society Volume 60 Issue 10 pages 1957-1968 19 SEP 2012 DOI 101111j1532-5415201204187x httponlinelibrarywileycomdoi101111j1532-5415201204187xfulljgs4187-fig-0001
bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull Physical function
Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Life and Living in Advanced Age a Cohort Study in New Zealand ndash Te Puā waitanga O Ngā Tapuwae Kia Ora Tonu (LiLACS - BOP) Age Māori (80+) amp non-Māori (85+) (functionally complex)
Ability - Disability bull 95 independent PC (5 need help) bull 70 independent Home chores (30 need help)
Health ndash last 12 months bull 98 saw GP bull 42 hospital admission almost half of those 2 or more admissions
Eating bull 76 full or partial dentures (Maori less likely) bull 24 chewing difficulty (dentures issues or missing teeth) bull lt ⅓ visited a dentist in the previous 12 months (Māori 18)
Falls ndash last 12 months bull 37 at least one fall - 20 of those had to go to hospital bull 20 of people had fallen more than once
httpswwwfmhsaucklandacnzenfacultylilacsresearchpublicationshtmla00ebcc370896771990ac4e394b2a762
Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Geriatric syndromes
Multifactorial health condition that occur when the accumulated effect of impairments in multiple systems render and older person vulnerable to situational changes
bull Multiple risk factors (for getting syndrome)
bull Multiple organ systems involved
bull Diagnostic studies to identify cause can be ineffective burdensome dangerous and costly
bull Therapeutic management can be helpful without firm diagnosis
bull Donrsquot fit specific disease categories
Syndrome signs amp symptoms with a single underlying cause
Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Why are Geriatric syndromes important
bull Lead to
ndash increased mortality and disability
ndash decreased financial and personal resources
ndash longer hospitalizations
ndash can diminish quality of life
bull OrsquoHara Geriatric syndromes and their implications for nursing Nursing 43(1)1-3 January
2013
What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

What are Geriatric syndromes
American Geriatric Society bull Frailty bull Visual and Hearing impairment bull Dizziness and Syncope bull Malnutrition bull Urinary incontinence bull Gait impairment bull Falls bull Osteoporosis bull Dementia bull Delirium bull Sleep problems bull Pressure ulcers bull Constipation
Classic 5 in literature
bull Pressure ulcers
bull Falls
bull Incontinence
bull Functional decline
bull Delirium
bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull High prevalence of frailty among geriatric inpatients suggests that evaluation for frailty should be considered a part of the comprehensive geriatric assessment
Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Frailty ndash no internationally agreed defn
bull A state of multiple system decline from age-related physiological changes to the extent that an individuals cellular repair mechanism can not maintain homeostasis
ndash Cause cumulative cellular damage may be inflammatory
ndash Most physiological system lose homeostatic reserve with age but can loose about 30 and they will still function
bull Physiological state of heighten vulnerability
bull May become one of the worlds leading health issues as mortality global mortality is moving from infectious disease to age-related disease
bull Affects +- quarter of ge 85 year olds to some degree
bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull Itrsquos a multiple morbidity state unrelated diseases
bull Itrsquos a distinct physiological process resulting from dysregulation of multiple systems that interact and impair each other Deregulated systems reduce ability to maintain homeostasis in the face of stressors so people are vulnerable to adverse outcomes from ldquoroutinerdquo conditions
Frailty ndash cause theories
Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Frailty
bull Fried component of frailty ndash from cardiovascular health study index 3 or more
ndash Weight loss unintentional weight loss ge45kg in last 12 mth
ndash Exhaustion - self reported
ndash Low levels of physical activity
ndash Slowness ndash slowed walking speed
ndash Weakness ndash grip strength
(0 none frail prefrail 1-2 frail 3-5)
Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Clinical Frailty Index Rockwood et al Canadian Study of Health and Aging
Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

Edmonton frail scale
bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull 67 yr female
bull Renal impairment DMT2 cataracts mild cognitive impairment HTN hypothyroid
bull History of homelessness and couch hoping drug abuse
bull No family contact ndash disowned
bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull 85 yr female
bull COPD HTN Memory loss OA and spinal stenosis
bull Care giver son since husband died
bull Recurrent UTI dependant for PC can feed self standtransfer walks few steps
bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts

bull 91 yr male
bull CVA and falls ndash left hip and distal fibular aortic stenosis renal impairment IHD HTN AF
bull Meds include warfarin codeine paracetamol
bull Supportive son and daughter in law
bull Walks with frame and mobility scooter
bull Enjoys a drink (6 Jugs daily at club)
bull Hearing loss ++ cataracts