articles intelligent technology for an aging population
TRANSCRIPT

■ Today, approximately 10 percent of the world’spopulation is over the age of 60; by 2050 this pro-portion will have more than doubled. Moreover,the greatest rate of increase is amongst the “oldestold,” people aged 85 and over. While many olderadults remain healthy and productive, overall thissegment of the population is subject to physicaland cognitive impairment at higher rates thanyounger people. This article surveys new technolo-gies that incorporate artificial intelligence tech-niques to support older adults and help them copewith the changes of aging, in particular with cog-nitive decline.
We are in the midst of a profound de-mographic shift, moving from aworld in which the majority of the
population is relatively young to one in whicha significant proportion of people are over theage of 65. This change poses both a challengeand an opportunity for the design of intelligenttechnology. While many older adults will re-main healthy and productive, overall this seg-ment of the population is subject to physicaland cognitive impairment at higher rates thanyounger people. It is important to keep in mindthat there is growth not just in the absolutenumber of older adults, but also in the propor-tion of the population that is over the age of65; there will thus be fewer young people tohelp older adults cope with the challenges ofaging. While human caregiving cannot and
will not be replaced, assistive technologies thatcan supplement human caregiving have thepotential to improve the quality of life for botholder adults and their caregivers. In particular,assistive technologies now being developedmay enable older adults to “age in place,” thatis, remain living in their homes for longer peri-ods of time. A large body of research has shownthat older Americans prefer to maintain inde-pendent households as long as possible(Hareven 2001). Additionally, institutionaliza-tion has an enormous financial cost, not onlyfor elders and their caregivers, but also for gov-ernments. In the United States, the federal gov-ernment, under the auspices of Medicaid andMedicare, pays for nearly 60 percent of the na-tion’s $132 billion annual nursing home bill(CMS Statistics 2003), and similar expenses areincurred throughout other nations. Thus tech-nology that can help seniors live at homelonger provides a “win-win” effect, both im-proving quality of life and potentially savingenormous amounts of money. Other technolo-gy can help those elders who are in assisted liv-ing or skilled nursing care facilities maintainmore independence there.
A range of artificial intelligence techniqueshas been used in the design of advanced assis-tive technologies. This article surveys thesetechnologies, focusing on systems that supportolder adults who are grappling with cognitivedecline.
Articles
SUMMER 2005 9Copyright © 2005, American Association for Artificial Intelligence. All rights reserved. 0738-4602-2005 / $2.00
Intelligent Technologyfor an Aging Population
The Use of AI to Assist Elders
with Cognitive Impairment
Martha E. Pollack

composition of a population. Popula-tion pyramids include a sequence ofhorizontal bars in which each bar rep-resents the number of the people with-in a particular age cohort; the numberof females within each cohort isshown to the right or the center line,while the number of males is shown tothe left. For example, figure 1 showsthe population pyramid for the UnitedStates in 1950. The source of the termpopulation pyramid is clear from the fig-ure, which has a pyramidal (or at leasttriangular) form, illustrating the factthat there tend to be relatively fewpeople in the oldest age cohorts, withincreasing numbers in successivelyyounger cohorts.
As we begin the twenty-first centu-ry, population pyramids have becomedistinctly less pyramidal. Figure 2shows the population pyramid for theUnited States in 2000, while figure 3shows the projected pyramid for 2030.The change in demographics is imme-diately clear: older adults make up anincreasingly greater proportion of thepopulation. In 2000, people aged 65and older made up 12.3 percent of theU.S. population, while by 2030, theywill constitute 19.2 percent, afterwhich growth is projected to level offso that this cohort represents 20.0 per-cent of the population in 2050. Themost rapid growth will occur within asubgroup of this cohort—the so-called“oldest old,” or people over the age of80. Today this group makes up 3.2 per-cent of the U.S. population, while by2030 that number will increase to 5.0percent, and by 2050, to 7.2 percent.Similar trends can be found world-wide, as illustrated in figure 4, whichpresents data for typical, selectedcountries. Although the shift is mostdramatic in the more industrialized re-gions of the world, a significantgrowth in the percentage of olderadults is expected in virtually everycountry.
A number of systems have been de-veloped to help people compensate forthe physical and sensory deficits thatmay accompany aging. Many of thesedo not rely on computer technology,for example liftchairs, which help peo-ple rise from seats, and ergonomichandles, which make it easier to opendoors. However, an increasing number
An Aging World To see just how dramatic the current demographic shiftis, it is useful to look at population pyramids: diagramstraditionally used by demographers to visualize the
Articles
10 AI MAGAZINE
80+75-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Male Female
Figure 1. Population Pyramid for the United States in 1950.
Source: U.S. Census Bureau
80+75-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Male Female
Figure 2. Population Pyramid for the United States in 2000.
Source: U.S. Census Bureau

of devices rely on AI and other ad-vanced computer-based technologies.Examples include text-to-speech sys-tems for people with low vision; a dig-ital programmable hearing aid that in-corporates a rule-based AI system tomake real-time decisions among alter-native signal-processing techniquesbased on current conditions (Flynn2004); and a jewelrylike device that al-lows people with limited mobility tocontrol household appliances usingsimple hand gestures (Starner et al.2000). In addition, significant researchhas been done to design obstacle-avoiding wheelchairs (see, for exam-ple, Yanco [2001] or Levine et al.[1999]).
Older adults can also be supportedwith technology that helps alleviatethe social isolation that may stemfrom mobility issues or from the needto care full time for a seriously illspouse or partner. For example, inter-actions between an older person andher family members and friends canbe facilitated by elder-friendly email1
and devices such as Dude’s Magic Box(Siio, Rowan, and Mynatt 2002), an in-novative system that allows childrento interact with grandparents who arefar away by placing their toys or otherobjects of interest into a box that pro-jects a picture onto a touch-sensitivescreen at the grandparents’ home.
In addition to sensory-motor andpsychosocial issues, a third area ofconcern for an aging population iscognitive decline. One widely citedstudy done in 1989 found that 10 per-cent of people over the age of 65 and50 percent of those over 85 hadAlzheimer’s disease, probably the best-known cause of severe cognitive im-pairment in elders (Hebert et al. 2003).A 2001 study that was restricted tocommunity-dwelling older adults—that is, excluding those living in nurs-ing homes and assisted-living facili-ties—showed that 23.4 percent of thepeople over 65 exhibited cognitive im-pairment that was short of dementia(CIND: cognitive impairment/no de-mentia), while another 4.8 percent ex-hibited full-fledged dementia. Thesame study found that of those over85, 38 percent exhibited CIND, while27 percent exhibited dementia (Un-verzagt et al. 2001). While the exact
rates of cognitive impairment reported differsomewhat from study to study, there is noquestion that cognitive impairment is a seriousproblem for many older adults and that theprevalence of this problem increases signifi-cantly with age, the “oldest old” having amuch greater rate of cognitive impairmentthan those in their late 60s and 70s.
This article will focus on the use of AI tech-niques in technology designed to support olderadults with cognitive impairment. It is not in-tended to be a complete survey of the relevantprojects but will instead provide a descriptionof the major goals of this class of technology,along with examples that illustrate the role ofAI for each class. LoPresti, Mihailidis, andKirsch (2004) provide a comprehensive survey,including discussion of many relatively simpledevices that do not include AI techniques.Haigh and Yanco (2002) and the proceedings ofa National Research Council workshop (Pewand Hemel 2004) provide information abouttechnologies that support sensory-motor andpsychosocial as well as cognitive problems inelders. Sixsmith (2002) gives a brief introduc-tion to “telecare” for cognitively impaired olderpeople, including a description of some of theethical issues raised by this technology. Finally,Czaja (1990) and Fisk et al. (2004) provide ex-cellent discussions of human-factors concernsin the design of technology for seniors.
Articles
SUMMER 2005 11
80+75-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Male Female
Figure 3. Population Pyramid for the United States in 2030.
Source: U.S. Census Bureau

continual observation of her performance ofroutine activities.
In all three cases, it is essential that the sys-tem be able to observe and reason about the el-der’s performance of daily activities.3 This isprobably most obvious in the case of assurancesystems, which must recognize whether some-one has fallen, has eaten, has taken her medi-cine, and so on. But, as we will see later on, theability to recognize the performance of routineactivities is also essential for compensation sys-tems, so that they can provide useful assistancethat is tailored to the current needs of the user.Similarly, assessment systems work by reason-ing about how and when the user performs herdaily activities.
Activity monitoring is currently a very activeresearch topic. Work has been done to use sen-sors to recognize the execution status of partic-ular types of activities, such as handwashing(Mihailidis, Fernie, and Barbenel 2001), mealpreparation (Barger et al. 2002), and move-
Goals for Assistive Technology for Cognition
Assistive technology can assist older people2
with cognitive impairment in one or more ofthe following ways: (1) by providing assurancethat the elder is safe and is performing neces-sary daily activities, and, if not, alerting a care-giver; (2) by helping the elder compensate forher impairment, assisting in the performanceof daily activities; and (3) by assessing the el-der’s cognitive status.
Assurance systems aim primarily at ensuringsafety and well-being and at reducing caregiverburden, by tracking an elder’s behavior andproviding up-to-date status reports to a caregiv-er. Compensation systems provide guidance topeople as they carry out their daily activities,reminding them of what they need to do andhow to do it. Assessment systems attempt to in-fer how well a person is doing—what her cur-rent cognitive level of functioning is—based on
Articles
12 AI MAGAZINE
22.7%6.9%Colombia
25.9%7.8%Brazil
26.2%6.9%Mexico
25.5%16.1%United States
19.2%Slovenia
30.7%18.2%Netherlands
24.1%Italy
34.5%23.2%Germany
37.6%19.3%Belarus
20502000
5.3%3.9%Mali
7.7%4.6%Ethiopia
6.0%4.2%Botswana
19.0%4.6%Jordan
24.8%6.4%Iran
18.7%6.8%Egypt
22.7%5.7%Fiji
29.9%16.4%Australia
20.5%6.8%Myanmar
23.3%Japan
20.1%7.5%India
22.7%6.9%China
42.4%
21.4%10.0%
41.5%
40.6%
World
> Age 60
Figure 4. Population Statistics for Typical Selected Countries Worldwide.
Source: United Nations Population Division

ments around town (Liao, Fox, and Kautz2004). Additionally, several projects have at-tempted to do more general activity recogni-tion, using radio frequency identification(RFID) tags attached to household objects andgloves (Philipose et al. 2004) or networks of het-erogeneous sensors (Haigh et al. 2003, Glascockand Kutzik 2000). Figure 5 illustrates the rangeof sensor technologies that are being investigat-ed for activity monitoring. As shown there, re-searchers are exploring both environmentalsensors and biosensors. The former class in-clude motion detectors and RFID readers thatdetermine a person’s location, contact switcheson cabinets and refrigerator doors that indicatewhether they have been opened, pressure sen-sors that indicate whether a person is sitting ina bed or chair, and thermometers that indicatewhether a stove has been turned on. Biosensorsare generally worn by a person to measure vitalsigns such as heart rate and body temperature.This range of sensors can be used to determinewhere a person is and what household objectsshe has used, as well as to get a general sense ofher activity level. This information can be usedto infer specific daily activities performed, andin turn, that knowledge, perhaps combinedwith biometric information, leads to a generalassessment of health and well-being.
In general, Bayesian networks are the princi-pal technology used for performing activityrecognition. A typical approach is that taken inthe PROACT system (Philipose et al. 2004),which employs a dynamic Bayesian network(DBN) that represents daily activities such asmaking tea, washing, brushing teeth, and soon. The user of PROACT wears a specially de-signed glove that includes an RFID reader,which can then sense household objects likecups, toothbrushes, and socks that have RFIDtags affixed to them.4
Each activity type that PROACT is intendedto recognize is modeled as a linear series ofsteps, and each step is then associated with theobjects involved and the probability of seeingeach such object. For example, making tea ismodeled as a three-stage activity, in whichthere is high probability of using the tea kettlein the first stage (in which water is boiled), ahigh probability of using the box of tea bags inthe second stage (in which the tea is steeped),and medium probability of using milk, sugar,or lemon in the third step (in which flavoringis added to the tea). The probabilities are in-tended to capture three possible sources of er-ror: sensor noise, objects that are unknown inthe model, and objects that are only optionallyused for each stage. Once the model has beendesigned, it is converted into a DBN. PROACT
then treats information about objects used andtime elapsed as observed variables and treatsthe current activity as a hidden variable, em-ploying Bayes filtering techniques to derive aprobability distribution over possible currentactivities. In preliminary testing with 14 differ-ent activity types, 14 subjects, and 108 taggedobjects, PROACT demonstrated an average pre-cision of 88 percent and average recall of 73percent.
Assurance Systems Examples of assurance systems include re-search projects (Haigh et al. 2003, Kart et al.2002, Chan et al. 1999, Ogawa et al. 2002), ademonstration system being used in an elder-care residential setting (Stanford 2002), and ahandful of commercially marketed products.The typical architecture for an assurance sys-tem is depicted in figure 6. These systems in-clude sensors placed in the user’s home, com-municating via a short-range protocol such asX10 to a base station, which may in turn com-municate wirelessly to a controller; the con-troller then uses broadband or a “plain oldtelephone system” (POTS) to send informationto a monitoring station or directly to the care-giver. Caregivers can get status reports on a reg-ular basis, typically by checking a web page,and are also alerted to emergencies by phone,pager, or email.
In some cases, the sensor network used by anassurance system is extremely simple, consist-ing, say, of just contact switches on externaldoorways, so that a caregiver can be immedi-ately notified if a cognitively impaired elderleaves her home: wandering is a significantproblem for people with certain types of cogni-tive impairment. With these systems, very littleinference is actually required; instead, an alarmis simply generated whenever the contactswitch is triggered.
In other cases, the network may include awide range of sensors, which are continuallymonitored both to recognize deviations fromnormal trends that may indicate problems (forexample, failure to eat meals regularly, as deter-mined by lack of motion in the kitchen) and todetect emergencies that require immediate at-tention (for example, falls, as indicated by ces-sation of motion above a certain height). Thesophistication of the inference performed us-ing the collected sensor data varies from systemto system. In some systems, only a loose con-nection is established between the sensor sig-nal and the activity being reported on: ma-chine learning may be used to infer broadpatterns of sensor firings, which then serve as
Articles
SUMMER 2005 13

overall trends in the elder’s activity for the pastmonth. Future plans are to extend the systemso that when the caregiver touches one of theicons, more detailed information is providedabout the elder’s activities that day: whethershe took her medicine, ate meals, and so on.
Compensation Systems Where assurance systems monitor a person andprovide alarms and status reports, they do notactually intervene and assist someone in ac-complishing her daily activities. In contrast, asecond class of systems is designed precisely tohelp an older adult compensate for any cogni-tive impairment he or she has experienced.These systems can help compensate for impair-ment in the ability to navigate, to manage adaily schedule, to complete a multistep task, torecognize faces, and to locate objects. Examplesof systems providing the first three types of as-sistance are discussed below.
Navigational Support Several systems have been developed to helpolder adults navigate successfully around their
the basis of establishing deviations from thenorm that constitute grounds for issuing awarning. For example, the system may learnthat a particular user is generally active in thekitchen between 7:30 and 8:15 AM, and maythen indicate a potential problem if no such ac-tivity is detected one day. This contrasts withthe kind of fine-grained activity recognitiondone by PROACT and related systems.
In addition to the question of how to deter-mine what information to report, research hasaddressed the question of exactly how to pre-sent the information. One particularly interest-ing approach is that of the Digital Family Por-trait project (Mynatt et al. 2001). Themotivation behind this work is to have a con-tinually up-to-date information display that isunobtrusive and provides a balance betweenthe elder’s privacy and the caregiver’s need forinformation. In this system, the adult child ofan elder keeps a picture of the elder in a digitalpicture frame, which has a pattern of 28 attrac-tive icons (for example, butterflies or trees). Thesize of each icon provides a general sense of theelder’s activity level on a given day; this way,the caregiver can immediately get a sense of the
Articles
14 AI MAGAZINE
Figure 5. Sensors for Activity Monitoring.
Monitor What?
The Environment • Motion sensors • GPS • RFID • Contact switches • Load sensors • Light sensors • Thermometers • Water sensors • Video cameras
The Person • Biosensors
To Identify
Location
Interaction with Household Objects
Amount of Movement
Biological Function
and Infer
ActivitiesPerformed
Health andWell-being

environments. Most of these systems aim to as-sist people who can no longer safely find theirway around, because of either sensory difficul-ties such as diminished vision or mobility im-pairments that make walking difficult. A majorgoal of these systems is obstacle avoidance. Lesswork has been done on systems that providenavigational support to people with cognitiveimpairment, but one interesting example ofsuch a system is the intelligent mobility plat-form (IMP) (Morris et al. 2003). IMP consists ofa standard commercial walker augmented witha laser range-finder, a handheld computer pro-viding a touchscreen interface for the user, anactive drive mechanism, and intelligent navi-gation software. The goal of the IMP projecthas been to design a device that can help a po-tentially confused user find her way around asetting, such as a large assisted-living facility, inwhich she might otherwise become lost.
During an installation phase, IMP is driventhrough the user’s environment via joystickand uses simultaneous localization and map-ping (SLAM) technology (Leonard et al. 2002)to create a map based on the readings obtainedby the laser range-finder. Individual regions of
the map such as the dining room, commonsroom, exercise room, and the user’s bedroomare then hand-labeled. Subsequently, the usercan select a destination from the on-board in-terface, and IMP will plan a path from theuser’s current location to that destination,guiding the user along that path by displayinga large red arrow that points the way; as theuser moves along the path, the arrow shifts toshow where she should turn.
Although IMP was designed primarily to pro-vide navigational guidance, a study was alsocompleted to determine whether the informa-tion that IMP has about a person’s locationthroughout the day is sufficient to support ac-tivity recognition. The approach taken in-volves constructing a hierarchical semi-Markovmodel with three layers: a low-level positionallayer, which represents the person’s metric po-sition (x, y, ?-coordinates); an intermediatetopological layer, which represents her locationin terms of the mapped regions (for example,in the dining room); and a top-level activitylayer, which represents the activity in whichshe is currently engaged (for example, eatingdinner). Model parameters are learned from la-
Articles
SUMMER 2005 15
Figure 6. Architecture of an Assurance System.
sensor
sensor
sensorbase station
Elderís HomeCaregiver’sHome, Office,or Telephone
controller
Broadband or Telephone Service (POTS)
802.11
RF or
X10
Monitoring Station

Autominder system (Pollack et al. 2003, Pollack2002) has aimed at enhancing schedule man-agement in several ways. Autominder providesa useful example of the value of AI technolo-gies in assistive technology, so we describe it insome detail.
Autominder. To understand how Automin-der works, it is instructive to consider an exam-ple of its interaction with a typical user: a for-getful, 80-year-old diabetic woman we’ll callMrs. Jones, who is supposed to eat a meal orsnack every four hours, and who currently hasan infection that requires her to take antibi-otics on a full stomach. With an alarm-clock-like system, one would have to specify the ex-act time at which Mrs. Jones had to take hermedicine. In contrast, using Autominder, Mrs.Jones or her caregiver would simply specifythat she has to take her medicine within anhour of eating breakfast and dinner. Once Au-tominder recognizes that Mrs. Jones has eatenbreakfast, it will know to remind her to take hermedicine within the next hour, should she for-get to do so. Similarly, rather than telling Auto-minder that Mrs. Jones has to eat at, say 7 AM,11 AM, 3 PM, and 7 AM, it would instead be giventhe upper bound of four hours between mealsor snacks. If Autominder then recognizes thatMrs. Jones has eaten lunch at 11:10, it willknow to remind her to eat again at 3:10—ormaybe a little earlier if her favorite TV show ison from 3:00 to 3:30.
To achieve this kind of behavior, Automin-der must maintain an accurate and up-to-datemodel of its user’s daily plan, monitor the exe-cution of that plan, and decide about issuingreminders accordingly. As depicted in figure 7,Autominder’s architecture includes three maincomponents, one dedicated to each of thesetasks. The Plan Manager stores the user’s planof daily activities in the client plan, and is re-sponsible for updating it and identifying andresolving any potential conflicts in it. It is thecomponent of the system responsible for an-swering the question “What is the user sup-posed to do?” The second module, the ClientModeler, uses information about the user’s ob-served activities to track the execution of theclient plan, storing beliefs about the executionstatus in the client model. The Client Modeleraddresses the question “What is the user do-ing?” Finally, the third main module is a re-minder-generation component called the Intel-ligent Reminder Generator (IRG), whichreasons about any disparities between what theuser is supposed to do and what she is doing,and makes decisions about whether and whento issue reminders. The Intelligent ReminderGenerator answers the question “What actions
beled data, and Bayesian filtering is then usedto recognize activities from sensed location in-formation. Preliminary results are very impres-sive, although more extensive testing, with agreater range of activities is required (Glover,Thrun, and Matthews 2004).
While IMP guides a person in an indoor facil-ity, another recent system, called OpportunityKnocks, has been designed to provide outdoornavigational guidance to less severely impairedpeople who may still be traveling around theircommunities (Liao, Fox, and Kautz 2004). Op-portunity Knocks, which is deployed on a cellphone enhanced with a global positioning sys-tem (GPS) chip and Bluetooth, learns its user’sstandard routes around town. Like IMP, itmakes use of a hierarchical probabilistic model(a dynamic Bayesian network) to attempt to in-fer where its user is currently traveling, and,having done so, it can then detect whether theuser has made an error, for example, by gettingon the wrong bus. In that case, it alerts the userto her error, by making a knocking sound—hence the system’s name—and provides infor-mation about how to get back to where theuser is supposed to be. The user can also man-ually enter her destination and have the systemguide her there.
Schedule Management A second type of compensation system helpsusers who have suffered from memory declinethat makes them prone to forgetfulness aboutroutine daily activities. In particular, schedule-management systems remind people when totake their medicine, when to eat meals, whento take care of personal hygiene, when to checkin with their adult children, and so on. Earlyschedule-management systems used alarmclocks, calendars, and buzzers (Harris 1978,Jones and Adams 1979, Wilson and Moffat1994), while later systems employed wirelessdevices including pagers, cell phones, andpalmtop computers (Hersh and Treadgold1994, Kim et al. 2000, Wilson et al. 1997). Re-gardless of the delivery platform, these earlysystems—like most commercially available re-minder systems today—function like glorifiedalarm clocks: they issue fixed reminders for ac-tivities at prespecified times. Unfortunately,this characteristic greatly limits their effective-ness, because older adults, like younger ones,do not live their lives according to unchangingschedules. To be useful, schedule-managementsystems need to be much more flexible.
The PEAT system (Levinson 1997) was thefirst system to use AI planning techniques tointroduce flexibility into a schedule-manage-ment system. More recently, research on the
Articles
16 AI MAGAZINE

should I (the Autominder system) take to en-sure that the user successfully performs her dai-ly activities?”
Each of Autominder’s components makesheavy use of AI technology. At the core of thePlan Manager is a temporal constraint-satisfac-tion processing engine, which performs dy-namic reasoning about the times at which ac-tivities are to be performed. (See sidebar.) Likethe other systems described above for monitor-ing and recognizing an elder’s activities, Auto-minder’s Client Modeler relies on Bayesian in-ference techniques.5 In some regards, the mostinteresting component of Autominder is theIntelligent Reminder Generator. To decidewhether and when to issue a reminder, the IRGmust balance four goals: (1) ensuring that theuser is aware of planned activities; (2) achiev-ing a high level of user and caregiver satisfac-tion; (3) avoiding introducing inefficiency intothe user activities; and (4) avoiding making theuser overly reliant on the reminder system,
which would have the detrimental effect of de-creasing, rather than increasing user indepen-dence.
It would be straightforward to generate re-minders if only the first criterion were of con-cern: one could simply issue a reminder forevery activity at its earliest possible start time,perhaps repeating the reminder at regular inter-vals if the activity is not performed. However,such a policy might do a potentially poor job ofsatisfying the other criteria. Two alternative ap-proaches have thus been taken in Autominderto producing reminders that achieve all fourgoals. The first (McCarthy and Pollack 2002)adopts a local-search approach based on theplanning-by-rewriting paradigm (Ambite andKnoblock 2001). It begins by creating an initialreminder plan that includes a reminder foreach activity in the user plan at its earliest pos-sible start time and then performs local search,using a set of plan rewrite rules to generate al-ternative candidate reminding plans. For ex-
Articles
SUMMER 2005 17
Preferences
ActivityInformation
ClientPlan
ClientModel
ClientModeler
PlanManager
PlanUpdates
Inferred Activity
Activity Information
SensorData
SmartHome
IntelligentReminderGenerator
ClientModel
Information
Reminders
Figure 7. Autominder’s Architecture.

To provide flexible, adaptive re-minders to a user, the Autominder sys-tem must maintain an up-to-datemodel of the user’s plan. This is doneby the Plan Manager. The Plan Manag-er, like most automated planning sys-tems, models plans as 4-tuples, < S, O,L, B >, where S are steps in the plans,and O, L, and B are temporal orderingconstraints, causal links, and bindingconstraints over those steps. However,we have found that temporal con-straints are particularly important inproviding schedule-management sup-port, and so we augment the set oftemporal constraints allowed: specifi-cally, we make use of the language ofdisjunctive temporal problems (DTPs)(Stergiou and Koubarakis 2000,Tsamardinos and Pollack 2003). For-mally, a DTP is a conjunctive set of dis-junctive inequalities: each orderingconstraint has the form
lb1 ≤ X1 – Y1 ≤ ub1 � . . . � lbn≤ Xn – Yn ≤ ubn
where the Xi and Yi refer to the start orend points of steps in the plan, andthe lower and upper bounds (lbi andubi) are real numbers.
Figure A gives an example of fourDTP constraints representing a typical
morning routine for an elderly user: 1. Mrs. Jones should breakfast be-tween 7 and 8, reserving 20–30 min-utes to eat.
2. She should take her medicinewithin an hour of eating.
3. She should bathe after 7 AM, re-serving 30–40 minute for this activity.
4. She should finish breakfast and
her bath by 8:30 (perhaps becausesomeone is coming to pick her up todrive her to the doctor).
The graph in figure A includes twonodes for each activity, one with sub-script S to indicate its start, and onewith E to indicate its end. The allow-able interval between any two activi-ties is indicated by [l, u], denoting thelower (upper) bounds on the interval
Articles
18 AI MAGAZINE
Temporal Reasoning in
Autominder’s Plan Manager
[0,510]
[20,30] [0,60]
[420,480]
[30,40]
[0,510]
BthE
EatE MedSEatS
BthS
TR
0 ≤ EatS – BthE ≤ ∞or0 ≤ BthS – EatE ≤ ∞
[420,∞]
Figure A. An Example Plan as a DTP in Autominder.
rank is selected, and the process iterates, withrewrite rules now being applied to the selectedplan. Iteration continues until either some re-minder plan is judged to have quality exceed-ing a prespecified threshold, or there is an in-terrupt indicating that there has been a changeto the user plan or to the user model. In the lat-ter case, the entire reminder plan generationprocess is restarted.
Although this approach has been satisfacto-ry for the initial version of Autominder and iswhat is being used in the current field testing,it has three key limitations:
First, it is very difficult to handcraft goodrules and evaluation functions.
Second, partly as a consequence of the first
ample, one rewrite rule deletes reminders foractivities that have low importance and thatare seldom forgotten by the user. Another ruleshifts the time of a reminder for an activity toits expected time, that is, the time by whichthe user usually performs the activity. Yet an-other rule spaces out reminders for activitiesfor the same type of action: for instance, in-stead of issuing eight reminders in a row todrink water, application of this rule would re-sult in the reminders being spaced out throughthe day. The newly generated reminder plansare evaluated using a heuristic function thattakes into account factors such as the numberof reminders, their timing, and their relativespacing. The reminder plan with the highest
limitation, the rules and evaluation functionthat have been developed handle only a smallsubset of the types of interface control ques-tions that might be addressed. To date, reason-ing is only done about which activities in theclient plan warrant reminders and, for those ac-tivities, when to issue the reminders. Reason-ing is not done about other types of interactionwith the client, for example, when to requestconfirmation about whether she has in factcompleted some activity, nor about the bestmeans of issuing reminders: all the remindersin the current version of Autominder are sim-ple text strings.
Third, and perhaps most importantly, theIRG’s rules and evaluation functions are fixed:
they do not change over time. Yet, typically thecapabilities and needs of intended users of sys-tems such as Autominder will change overtime. As an elder’s cognitive capacities dimin-ish, she may require additional or more de-tailed reminders. Even over shorter time spans,a user’s needs may change, for instance, duringa period of illness.
The second approach being investigated inAutominder for intelligently generating re-minders addresses these limitations. It uses re-inforcement learning (RL) to induce an interac-tion policy, a function from features of thecurrent state (for example, the time of day, thetiming of the previous interaction, the user’smood, and the actions she is supposed to per-
Articles
SUMMER 2005 19
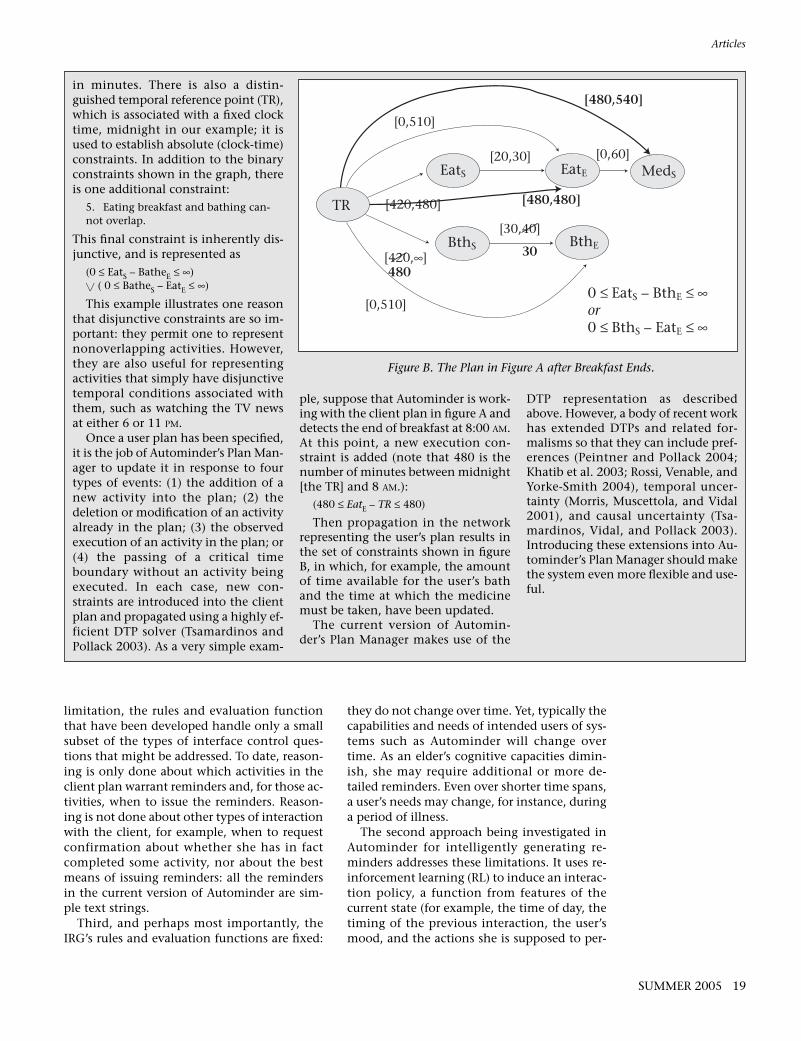
in minutes. There is also a distin-guished temporal reference point (TR),which is associated with a fixed clocktime, midnight in our example; it isused to establish absolute (clock-time)constraints. In addition to the binaryconstraints shown in the graph, thereis one additional constraint:
5. Eating breakfast and bathing can-not overlap.
This final constraint is inherently dis-junctive, and is represented as
(0 ≤ EatS – BatheE ≤ ∞) � ( 0 ≤ BatheS – EatE ≤ ∞)
This example illustrates one reasonthat disjunctive constraints are so im-portant: they permit one to representnonoverlapping activities. However,they are also useful for representingactivities that simply have disjunctivetemporal conditions associated withthem, such as watching the TV newsat either 6 or 11 PM.
Once a user plan has been specified,it is the job of Autominder’s Plan Man-ager to update it in response to fourtypes of events: (1) the addition of anew activity into the plan; (2) thedeletion or modification of an activityalready in the plan; (3) the observedexecution of an activity in the plan; or(4) the passing of a critical timeboundary without an activity beingexecuted. In each case, new con-straints are introduced into the clientplan and propagated using a highly ef-ficient DTP solver (Tsamardinos andPollack 2003). As a very simple exam-
ple, suppose that Autominder is work-ing with the client plan in figure A anddetects the end of breakfast at 8:00 AM.At this point, a new execution con-straint is added (note that 480 is thenumber of minutes between midnight[the TR] and 8 AM.):
(480 ≤ EatE – TR ≤ 480)
Then propagation in the networkrepresenting the user’s plan results inthe set of constraints shown in figureB, in which, for example, the amountof time available for the user’s bathand the time at which the medicinemust be taken, have been updated.
The current version of Automin-der’s Plan Manager makes use of the
DTP representation as describedabove. However, a body of recent workhas extended DTPs and related for-malisms so that they can include pref-erences (Peintner and Pollack 2004;Khatib et al. 2003; Rossi, Venable, andYorke-Smith 2004), temporal uncer-tainty (Morris, Muscettola, and Vidal2001), and causal uncertainty (Tsa-mardinos, Vidal, and Pollack 2003).Introducing these extensions into Au-tominder’s Plan Manager should makethe system even more flexible and use-ful.
[0,510]
[20,30] [0,60]
[420,480]
[30,40]
[0,510]
BthE
EatE MedSEatS
BthS
TR
0 ≤ EatS – BthE ≤ ∞or0 ≤ BthS – EatE ≤ ∞
[420,∞]
[480,540]
[480,480]
30
480
Figure B. The Plan in Figure A after Breakfast Ends.

recognizes a problem—for instance, that thesubject is using the towel before wetting herhands—a prerecorded verbal prompt is provid-ed. In a field test with 10 subjects with moder-ate-to-severe dementia, COACH was shown toincrease by 25 percent the number of hand-washing steps that subjects could complete suc-cessfully without assistance from caregivers.
Assessment Systems So far we have described assurance systems andcompensation systems. A third use for AI tech-nology in the care of older adults with cogni-tive impairment is to provide continual, natu-ralistic assessment of their cognitive status.Several studies have shown that cognitive im-pairment frequently remains undiagnosed forsubstantial periods of time (Boise, Neal, andKaye 2004; Ross et al. 1997; Callahan, Hendrie,and Tierney 1995), an unfortunate situationsince there exist a range of medical and behav-ioral means of helping cognitively impaired pa-tients, as well as social support services for theirfamilies. Currently, most cognitive assessmentis done in the clinical setting, when a personvisits her physician. This means thatassessment is only done infrequently and onthe basis of limited information: it is quite pos-sible that the person is having a particularly“good” or “bad” day when she happens to havea doctor’s appointment. Additionally, the veryfact that the assessment is being done outsideof the person’s normal living environment maybias the assessment, for instance if the personfinds the doctor’s visit to be stressful.
Several researchers have thus begun to ex-plore the possibility of using sensor-basedmonitoring, combined with sophisticatedanalysis algorithms, to assess a person’s level offunctioning as she goes about her routine activ-ities in her home. An example is Wired Inde-pendence Square, a project in which sensorsare placed in a kitchen and used to collect tim-ing data while a patient at risk for cognitive im-pairment performs a task such as making tea(Carter and Rosen 1999). The hypothesis, as yetunconfirmed, is that objective data such as thiswill be shown to correlate with assessmentsmade with standard diagnostic batteries suchas the Assessment of Motor and Process Skills(AMPS), a tool used by occupational therapiststo measure the quality of a person’s perfor-mance of activities of daily living. Althoughthe initial version of this system was installedin an in-hospital setting—a kitchen used by oc-cupational therapists for observation and as-sessment of patients at the National Rehabilita-tion Hospital—the researchers hope to move to
form) to interface actions, including if andwhen to issue a reminder to perform a certainactivity. Although this approach has so far onlybeen tested in simulation, initial results showthat it is possible to learn strategies that canpersonalize to an individual user and adapt toboth short- and long-term changes in herneeds and preferences (Rudary, Singh, and Pol-lack 2004).
Autominder has been deployed in prototypeform on three platforms: a mobile robot, theIMP intelligent walker described above, and ahandheld computer (a personal digital assis-tant) that communicates wirelessly with a basestation. The mobile robot, which is namedPearl and is depicted in figure 8, includes a dif-ferential drive system, two on-board comput-ers, laser range-finders, sonar sensors, micro-phones for speech recognition, speakers forspeech synthesis, a touch-sensitive graphicsdisplay, a custom-designed actuated head unit,and stereo camera systems (Pineau et al.2003).6
Preliminary field tests of Autominder havebeen conducted with both older adults and pa-tients with traumatic brain injury, but system-atic studies of its effectiveness have not yetbeen completed.
Activity-Guidance Systems Where schedule-management systems providea user with prompts to perform multiple activ-ities during the course of her day, activity-guid-ance systems are geared towards providing re-minders about consecutive steps in individualactivities. As such, these systems tend to beaimed at people with more severe cognitive im-pairment.
An example is COACH (Mihailidis, Fernie,and Barbenel 2001), a system designed to assista person with severe dementia who has difficul-ty remembering the proper sequence of every-day activities or how to use the tools that arepart of those activities. The current version ofCOACH assists a person with handwashing;this task was chosen because studies haveshown that caregivers of dementia patientsfind that providing assistance with bathroomactivities is one of their most stressful tasks.The COACH system uses a video camera to ob-serve the user as she attempts to wash herhands. The video image is processed to identifythe two-dimensional (x, y) coordinates of atracking bracelet worn by the subject, and aplan-recognition algorithm is then invoked todetermine what step in the activity the subjectis attempting (for example, turning on the wa-ter, using soap, drying hands). If the system
Articles
20 AI MAGAZINE

Articles
SUMMER 2005 21
Courtesy Carnegie Mellon University Robotics Institute.
Figure 8. “Pearl” the Robot.

systems are still largely emerging. Researchchallenges abound, and in designing technolo-gy to support an aging population, there arecompelling reasons to employ a number of dif-ferent AI technologies, including plan genera-tion and execution monitoring, reasoning un-der uncertainty, machine learning, naturallanguage processing, and robotics and machinevision. Additional challenges will require col-laboration with colleagues having expertise insensor-network architectures, privacy and secu-rity, and human-machine interaction. Thecomedienne Lucille Ball is said to have re-marked, “The secret to staying young is to livehonestly, eat slowly, and lie about your age.”With continued research, we can perhaps add afourth injunction: “use AI technology.”
AcknowledgementsThis article was written in part with supportfrom the National Science Foundation, GrantIIS-0085796, and from the Intel Corporation,Grant #13109. The Autominder system hasbeen developed with the efforts of a number ofpast and present graduate students, includingLaura Brown, Dirk Colbry, Colleen McCarthy,Michael Moffitt, Cheryl Orosz, Bart Peintner,Sailesh Ramakrishnan, Peter Schwartz, Joe Tay-lor, and Ioannis Tsamardinos. Thanks are alsodue to Jacqueline Dunbar-Jacob, JudithMatthews, and Sebastian Thrun, my fellowmembers of the original “Nursebot” project.
Notes1. Generations on Line, www.generationsonline. com.
2. And others; although this paper concentrates ontechnology for older adults, this same technologycan also be useful for younger people with cognitiveimpairment, including people with mental retarda-tion and victims of traumatic brain injury.
3. The disability literature classifies certainfundamental activities such as eating, dressing, andbathing as activities of daily living (ADLs) while oth-er, somewhat more complicated activities such aspreparing meals, light housework, and paying billsare classified as instrumental activities of daily living(IADLs). Additional categories for classification aresometimes also introduced. In this article, we willsimply refer to “daily” or “routine” activities to referto the variety of things that a person must do to func-tion autonomously in her home.
4. In the current prototype, the glove is somewhat awk-ward; it would need to be redesigned for an actually de-ployed system, but it suffices for a proof of concept.
5. In the versions of Autominder that we have beentesting in the field to date, we have not employedsensors, instead relying on the user to tap a screen toindicate that she has completed an activity. This isobviously just a temporary approach; we are current-ly investigating sensor-based activity-recognition al-gorithms in the laboratory and aim to develop a ver-
installations within individual homes in thenear future.
A related project attempts to measure cogni-tive performance by monitoring a person asshe interacts with her home computer (Jimi-son, Pavel, and Pavel 2003). In initial studies,each user was monitored as she played anadapted version of the FreeCell solitaire game;this was selected both because interviews witholder adults showed that they enjoyed this ac-tivity and because it is one that incorporates as-pects of cognition such as short-term memoryand strategic planning that are directly relevantto the performance of activities of daily living.Each time the user played FreeCell, her perfor-mance was compared to a standard establishedby an automated solver. Analysis was thendone to track the user’s relative performanceover time; the goal is to identify declines in per-formance that may be indicative of more gen-eral cognitive decline.
In this latter project, one can already see theuse of AI technology in the automated solverthat determines the optimal solution to eachFreeCell game. However, in both this and thepreceding project, as well as in other efforts todo continual, naturalistic assessment, one canenvision a larger and more central role for AItechniques: specifically, in the use of machine-learning methods to induce a person’s normallevel of functioning and to identify changesfrom that norm.
Conclusion Interest in intelligent assistive technology forolder adults is growing rapidly. Within the pastfive to eight years, research groups investigat-ing the use of AI techniques for such technolo-gy have formed at more than a dozen differentuniversities and industrial research laborato-ries. Workshops have been held at major AIconferences as well as at gerontology confer-ences (Haigh 2002; Rogers et al. 2002; SpryFoundation 2003; Gerontological Society2003); the National Research Council spon-sored a workshop resulting in a book on thistopic (Pew and Hemel 2004); an online infor-mation clearinghouse has been created (Centerfor Aging Services Technology—CAST)7; andthe United States Senate Special Committee hasheld a hearing on the assistive technology forelders (U. S. Senate 2004).
This article has provided a survey of intelli-gent technology to support elders with cogni-tive decline. Assurance systems are alreadyavailable as commercial products; compensa-tion systems mainly exist as research proto-types; and ideas about developing assessment
Articles
22 AI MAGAZINE

sion of Autominder that fully integratessensor networks in the near future.
6. Pearl was designed and built at CarnegieMellon University by Sebastian Thrun andhis students.
7. Center for Aging Services Technology(CAST), www.agingtech.org/.
References Ambite, J. L., and Knoblock, C. A. 2001.Planning by Rewriting. Journal of ArtificialIntelligence Research 15: 207–261.
Barger, T.; Alwan, M.; Kell, S.; Turner, B.;Wood, S.; and Naidu, A. 2002. ObjectiveRemote Assessment of Activities of DailyLiving: Analysis of Meal Preparation Pat-terns. Medical Automation Research Cen-ter, University of Virginia Health System,Charlottesville, VA (http: //marc.med.vir-ginia.edu/pdfs/library/ADL.pdf).
Boise, L.; Neal, M. B.; and Kaye, J. 2004. De-mentia Assessment in Primary Care: Resultsfrom a Study in Three Managed Care Sys-tems. The Journals of Gerontology Series A:Biological Sciences and Medical Sciences59: M621–M626.
Callahan, C. M.; Hendrie, H. C.; and Tier-ney, W. M. 1995. Documentation andEvaluation of Cognitive Impairment in El-derly Primary Care Patients. Annals of Inter-nal Medicine 122(6): 422–429.
Carter, J., and Rosen, M. 1999. UnobtrusiveSensing of Activities of Daily Living: A Pre-liminary Report. In Proceedings of the FirstJoint Biomedical Engineering Society and Engi-neers in Medicine and Biology Conference,678. Piscataway, NJ Institute of Electricaland Electronics Engineers.
Chan, M.; Bocquet, H.; Campo, E.; Val, T.;and Pous, J. 1999. Alarm CommunicationNetwork to Help Carers of the Elderly forSafety Purposes: A Survey of a Project. Inter-national Journal of Rehabilitation Research22(2): 131–136.
CMS Statistics. 2003. U.S. Department ofHealth and Human Services. Centers forMedicare and Medicaid Services 2003 CMSStatistics. Washington, D.C.: GovernmentPrinting Office (www.cms.hhs.gov/ re-searchers/pubs/03cmsstats.pdf).
Czaja, S. 1990. Human Factors ResearchNeeds for an Aging Population. Washington,DC: National Academic Press.
Fisk, A. D.; Rogers, W. A.; Charness, N.; Cza-ja, S. J.; and Sharit, J. 2004. Designing forOlder Adults: Principles and Creative HumanFactors Approaches. Boca Raton, FL: CRCPress.
Flynn, M. 2004. Maximizing the Voice-to-Noise Ratio (VNR) via Voice Priority Pro-cessing. Hearing Journal (April 2004): 54–59.
Gerontological Society. 2003. Gerontologi-cal Society of America Formal InterestGroup on Technology and Aging Work-shop. Washington, DC: Gerontological So-ciety of America (www.stockton.edu/bur-dickd/tagupdates.html).
Glascock, A., and Kutzik, D. 2000. Behav-ioral Telemedicine: A New Approach to theContinuous Nonintrusive Monitoring ofActivities of Daily Living. Telemedicine Jour-nal 6(1): 33–44.
Glover, J.; Thrun, S.; and Matthews, J. T.2004. Learning User Models of Mobility-Re-lated Activities through InstrumentedWalking Aids. In Proceedings of the IEEE In-ternational Conference on Robotics and Au-tomation. Piscataway, NJ: Institute of Elec-trical and Electronics Engineers.
Haigh, K., ed. 2002. Automation as Caregiver:The Role of Intelligent Technology as Elder Care.Papers from the AAAI Workshop. TechnicalReport WS-02-02, American Association forArtificial Intelligence, Menlo Park, CA.
Haigh, K. Z.; Kiff, L. M.; Myers, J.; Guralnik,V.; Kirschbaum, K.; Phelps, J.; Plocher, T.;and Toms, D. 2003. The IndependentLifestyle Assistant (ILSA): Lessons Learned.Technical Report ACSPO3023, HoneywellLaboratories, Minneapolis, MN.
Haigh, K. Z., and Yanco, H. 2002. Automa-tion as Caregiver: A Survey of Issues andTechnologies. In Automation as Caregiver:The Role of Intelligent Technology in ElderCare. Papers from the AAAI Workshop,35–53. Technical Report WS-02-02, Ameri-can Association for Artificial Intelligence,Menlo Park, CA.
Hareven, T. K. 2001. Historical Perspectiveson Aging and Family Relations. In Hand-book of Aging and the Social Sciences, 5th ed.,ed. R. Binstock and L. George, 141–159.New York: Elsevier Science.
Harris, J. 1978. External Memory Aids. InPractical Aspects of Memory, ed. M. M.Gruneberg, P. N. Morris, and R. N. Sykes.London: Academic Press.
Hebert, L. E.; Scherr, P. A.; Bienias, J. L.;Bennett, D.; and Evans, D. A. 2003.Alzheimer Disease in the U.S. Population:Prevalence Estimates Using the 2000 Cen-sus. Archives of Neurology 60(8): 1119–1122.
Hersh, N. A., and Treadgold, L. 1994. Neu-ropage: The Rehabilitation of Memory Dys-function by Prosthetic Memory and Cue-ing. NeuroRehabilitation 4(3):187–197.
Jimison, H. B.; Pavel, M.; and Pavel, J. 2003.Adaptive Interfaces for Home Health. Paperpresented at the Second InternationalWorkshop on Ubiquitous Computing forPervasive Healthcare. Seattle, WA, October12 (www.healthcare.pervasive.dk/ubicomp2003/papers/).
Jones, M., and Adams, J. 1979. Toward a
Prosthetic Memory. Bulletin of the BritishPsychological Society 32(2): 165–167.
Kart, C.; Kinney, J.; Murdoch, L.; and Ziem-ba, T. 2002. Crossing the Digital Divide: Fam-ily Caregiver’s Acceptance of Technology. Tech-nical Report, Scripps Gerontology Center,Miami University, Oxford, OH.
Khatib, L.; Morris, P.; Morris, R.; and Ven-able, K. B. 2003. Tractable Pareto OptimalOptimization of Temporal Preferences. InProceedings of the Eighteenth InternationalJoint Conference on Artificial Intelligence,1289–1294. San Francisco: Morgan Kauf-mann Publishers.
Kim, H.; Burke, D.; Dowds, M.; Boone, K.A.; and Parks, G. J. 2000. Electronic Memo-ry Aids for Outpatient Brain Injury: Follow-up Findings. Brain Injury 14(2):187–196.
Leonard, J.; Tardós, J. D.; Thrun, S.; andChoset, H., eds. 2002. IEEE InternationalConference on Robotics and AutomationWorkshop on Concurrent Mapping and Local-ization for Mobile Robots. Piscataway, NJ: In-stitute of Electrical and Electronics Engi-neers.
Levine, S. P.; Bell, D. A.; Jaros, L. A.; Simp-son, R. C.; Koren, Y.; and Borenstein, J.1999. The Navchair Assistive WheelchairNavigation System. IEEE Transactions of Re-habilitation Engineering 7(4): 443–451.
Levinson, R. 1997. PEAT—The Planningand Execution Assistant and Trainer. Jour-nal of Head Trauma Rehabilitation12(2)(April): 85–91.
Liao, L.; Fox, D.; and Kautz, H. 2004. Learn-ing and Inferring Transportation Routines.In Proceedings of the Nineteenth NationalConference on Artificial Intelligence, 348–353.Menlo Park, CA: AAAI Press.
LoPresti, E. F.; Mihailidis, A.; and Kirsch, N.2004. Assistive Technology for CognitiveRehabilitation: State of the Art. Neuropsy-chological Rehabilitation 14(1/2):5–39.
McCarthy, C. E., and Pollack, M. E. 2002. APlan-Based Personalized Cognitive Orthot-ic. In Proceedings of the Sixth InternationalConference on AI Planning and Scheduling,213–222. Menlo Park, CA: AAAI Press.
Mihailidis, A.; Fernie, G. R.; and Barbenel, J.2001. The Use of Artificial Intelligence inthe Design of an Intelligent Cognitive Or-thosis for People with Dementia. AssistiveTechnology 13(1): 23–39.
Morris, A.; Donamukkala, R.; Kapuria, A.;Steinfeld, A.; Matthews, J.; DunbarJacobs,J.; and Thrun, S. 2003. A Robotic WalkerThat Provides Guidance. In Proceedings ofthe IEEE International Conference on Roboticsand Automation. Piscataway, NJ: Institute ofElectrical and Electronics Engineers.
Morris, P.; Muscettola, N.; and Vidal, T.2001. Dynamic Control of Plans with Tem-poral Uncertainty. In Proceedings of the Sev-
Articles
SUMMER 2005 23

2002 Revision Population Database. NewYork, NY (http://esa.un.org/unpp/).
Unverzagt, F. W.; Gao, G.; Baiyewu, O.;Ogunniyi, A. O.; Gureje, O.; Perkins, A.;Emsley, C. L.; Dickens, J.; Evans, R.; Musick,B.; Hall, K. S.; Hui, S. L.; and Hendrie, H. C.2001. Prevalence of Cognitive Impairment:Data from the Indianapolis Study of Healthand Aging. Neurology 57(9): 1655–1662.
United States Department of Commerce.Bureau of the Census. Population Division,International Programs Center (IPC) Inter-national Data Base (IDB). (/www.census.gov/ipc/www/idbpyr.html).
United States Senate, Special Committee onAging 2004. Assistive Technologies and In-dependent Aging: Opportunities and Chal-lenges. A Hearing of the United States Sen-ate Special Committee on Aging, Serial No.108-33. Washington, DC: U.S. GovernmentPrinting Office.
Wilson, B. A., and Moffat, M., eds. 1994.Clinical Management of Memory Problems.Rockville, MD: Aspen Systems Corporation.
Wilson, B. A.; Evans, J. J.; Emslie, H.; andMalinek, V. 1997. Evaluation of Neuropage:A New Memory Aid. Journal of Neurology,Neurosurgery and Psychiatry 63(1): 113–115.
Yanco, H. A. 2001. Development and testingof a robotic wheelchair system for outdoornavigation. In Proceedings of the 2001 Confer-ence of the Rehabilitation Engineering and Assis-tive Technology Society of North America.
Martha E. Pollack is aprofessor in the Depart-ment of Electrical Engi-neering and ComputerScience at the Universityof Michigan, where she isalso associate chair forcomputer science and en-gineering. Pollack was
previously professor of computer scienceand professor and director of the IntelligentSystems Program at the University of Pitts-burgh, and, before that, she was a seniorcomputer scientist at the Artificial Intelli-gence Center at SRI International in MenloPark, California. She received her B.A. degreefrom Dartmouth College and her Ph.D. fromthe University of Pennsylvania. A Fellow ofthe AAAI, Pollack recently completed a termas editor-in-chief of the Journal of Artificial In-telligence Research. She has done research andpublished papers in the areas of automatedplanning and execution monitoring, tempo-ral reasoning, and natural-language process-ing, as well as on assistive technology forcognitively impaired people. In April of2004, she testified before the United StatesSenate Special Committee on Aging, dis-cussing the potential value of assistive tech-nology in an aging world.
Rossi, F.; Venable, K. B.; and Yorke-Smith,N. 2004. Controllability of Soft TemporalConstraint Problems. In Proceedings of theTenth International Conference on Principlesand Practice of Constraint Programming.Springer Lecture Notes in Computer Sci-ence Series, Volume 3258, 588–603. Berlin:Springer-Verlag.
Rudary, M.; Singh, S. B.; and Pollack, M. E.2004. Adaptive Cognitive Orthotics: Com-bining Reinforcement Learning and Con-straint-Based Temporal Reasoning. In Pro-ceedings of the Twenty-First InternationalConference on Machine Learning, 719–726.New York: Association for Computing Ma-chinery.
Siio, I.; Rowan, J.; and Mynatt, E. 2002.Peek-a-Drawer: Communication by Furni-ture. In Extended Abstracts of the ACM Con-ference on Human Factors in Computing Sys-tems, 582–583. New York: Association forComputing Machinery.
Sixsmith, A. J. 2002. New Technology forthe Care of Cognitively Impaired OlderPeople. In Geriatric Psychiatry, 2nd ed., ed. J.R. M. Copeland, M. T. Abou-Saleh, and D.G. Blazer, 685–687. New York: Wiley.
Spry Foundation 2003. Computer BasedTechnology and Caring for Older Adults. Tech-nical Report. Spry Foundation NationalConference, Washington, DC, October 2–3(www. spry.org/).
Stanford, V. 2002. Using Pervasive Com-puting to Deliver Elder Care. IEEE Distrib-uted Systems Online. New York: Institute ofElectrical and Electronics Engineers (dson-line.computer.org/0203/departments/bp1app.htm).
Starner, T.; Auxier, J.; Ashbrook, D.; andGandy, M. 2000. The Gesture Pendant: ASelf-Illuminating, Wearable, Infared Com-puter Vision System for Home AutomationControl and Medical Monitoring. In Pro-ceedings of the IEEE International Symposiumon Wearable Computing, 87–94. Piscataway,NJ: Institute of Electrical and ElectronicsEngineers.
Stergiou, K., and Koubarakis, M. 2000.Backtracking Algorithms for Disjunctionsof Temporal Constraints. Artificial Intelli-gence 120(1): 81–117.
Tsamardinos, I., and Pollack, M. E. 2003. Ef-ficient Solution Techniques for DisjunctiveTemporal Problems. Artificial Intelligence151(12): 43–89.
Tsamardinos, I.; Vidal, T.; and Pollack, M. E.2003. CTP: A New, Constraint-based For-malism for Conditional, Temporal, Plan-ning. Constraints: An International Journal8(4):365–388.
United Nations. 2002. Department of Eco-nomic and Social Affairs. Population Divi-sion. World Population Prospects: The
enteenth International Joint Conference on Ar-tificial Intelligence, 494– 499. San Francisco:Morgan Kaufmann Publishers.
Mynatt, E. D.; Rowan, J.; Craighill, S.; andJacobs, A. 2001. Digital Family Portraits:Providing Peace of Mind of Extended Fam-ily Members. In Proceedings of the ACM Con-ference on Human Factors in Comuting Sys-tems, 333–340. New York: Association forComputing Machinery.
Ogawa, M.; Suzuki, R.; Izutsu, T.; Iwaya, T.;and Togawa, T. 2002. Long Term RemoteBehavioral Monitoring of Elderly by UsingSensors Installed in Ordinary Housing. InProceedings of the Second Annual Internation-al IEEE -EMBS Special Topic Conference onMicrotechnologies in Medicine and Biology,322–325. Piscataway, NJ: Institute of Elec-trical and Electronics Engineers.
Peintner, B., and Pollack, M. E. 2004. Low-Cost Addition of Preferences to DTPs andTCSPs. In Proceedings of the Nineteenth Na-tional Conference on Artificial Intelligence,723–728. Menlo Park, CA: AAAI Press.
Pew, R., and Hemel, S. V., eds. 2004. Tech-nology for Adaptive Aging. Washington, DC:National Academies Press.
Philipose, M.; Fishkin, K. P.; Perkowitz, M.;Patterson, D. J.; Hahnel, D.; Fox, D.; andKautz, H. 2004. Inferring ADLs from Inter-actions with Objects. IEEE Pervasive Com-puting 3(4): 50–57.
Pineau, J.; Montemerlo, M.; Pollack, M. E.;Roy, N.; and Thrun, S. 2003. Towards Ro-botic Assistants in Nursing Homes: Chal-lenges and Results. Robotics and Au-tonomous Systems 42(3–4): 273–282.
Pollack, M. E. 2002. Planning Technologyfor Intelligent Cognitive Orthotics. In Pro-ceedings of the Sixth International Conferenceon AI Planning and Scheduling, 322–331.Menlo Park, CA: AAAI Press.
Pollack, M. E.; Brown, L.; Colbry, D.; Mc-Carthy, C. E.; Orosz, C.; Peintner, B.; Ra-makrishnan, S.; and Tsamardinos, I. 2003.Autominder: An Intelligent Cognitive Or-thotic System for People with Memory Im-pairment. Robotics and Autonomous Systems44(3–4): 273–282.
Rogers, W. A.; Charness, N.; Fisk, A. D.; andCzaja, S., eds. 2002. The Fourth Interna-tional Conference on Gerontechnology.Gerontechnology 2(1) (www.gerontechnolo-gy.info/).
Ross, G. W.; Abbott, R. D.; Petrovitch, H.;Morens, D. M.; Grandinetti, A.; Tung, K.;Tanner, C.; Masaki, K.; Blanchette, P.; Curb,J. D.; Popper, J. S.; and White, L. R. 1997.Frequency and Characteristics of Silent De-mentia among Elderly Japanese-AmericanMen: The Honolulu Study. Journal of theAmerican Medical Association 277(10):800–805.
Articles
24 AI MAGAZINE