arthroscopic synovectomy in hemophilic arthropathy of the knee
TRANSCRIPT

Scand J Haematol - Suppl40, Vol33, 1984,263-270
Arthroscopic Synovectomy in Hemophilic Arthropathy of the Knee
J. D. WIEDEL
Department of Orthopedics University of Colorado, School of Medicine, Denver, Colorado
Five patients with chronic hemophilic arthropathy of the knee underwent arthroscopic synovectomies between June of 1980 and June of 1981. Four of the five patients have had no spontaneous bleeds and have had no recurrence of synovial hypertrophy. Two of these patients did have a trauma-induced bleed. One patient, who did not have a posteromedial synovectomy, had a persistent posteromedial synovial hypertrophy which was the site of recurrent bleeds, requiring a repeat synovectomy. All patients obtained their preoperative range-of-motion, and only two patients required manipulation. No complications occurred as a result of these arthroscopic synovectomies. From this preliminary report, arthroscopic synovectomy in the hemophilic knee proved to be a safe and effective procedure.
Key words: Arthroscopy, Hemarthrosis, Joint motion, Recurrent bleeds Synovectomy, Synovial hypertrophy
Correspondence to: Jerome D. Wiedel, M.D., Associate Professor, 4200 East Ninth Avenue, Denver, Colorado 80262, USA
Synovectomy for chronic hemophilic synovitis is performed for the main pur- pose of stopping recurrent hemarthroses. The indications being those of frequent recurrent bleeds and synovial hyper- trophy, which persist in spite of adequate factor replacement therapy.
Traditionally, synovectomy of the knee is performed through medial and lateral parapatellar arthrotomy incisions. However, without posteromedial and posterolateral arthrotomies, only a limit- ed (subtotal) synovectomy is accomp- lished. Such an extensive surgical ap- proach causes considerable postoperative pain and significantly interferes with the patient’s attempt at regaining muscle con- trol and performing range-of-motion exercises. This, no doubt, contributes to the loss of motion frequently observed
after synovectomy. Although Storti and co-workers (1969) reported improved joint mobility in all their patients follow- ing knee synovectomy, other authors re- port a loss of motion in many patients (Arnold & Hilgartner 1977, Clark 1978, McCollough et a1 1979, Pietrogrande et a1 1972, Greer 1980). Even Storti & Ascari (1975) in a later publication, reported that knee mobility remained unchanged in 33 percent of his patients and even worsened in 12 percent. Other compli- cations reported have been wound heal- ing problems, infection, and fractures as- sociated with manipulation (Clark 1978).
These difficulties encountered follow- ing open synovectomy led to the consi- deration of alternatives. Because of the known low morbidity following arthro- scopic surgery, manifested mainly in the

264 WIEDEL
minimal pain and early return of knee motion, synovectomy by arthroscopic means was attempted in the hopes of sig- nificantly reducing these recognized complications.
This paper reports on five patients with hemophilia who have had arthro- scopic synovectomies performed on the knee between June of 1980 and June of 1981.
Four patients had classic hemophilia (F VIII deficiency) and one had F IX de- ficiency. The patients with F VIII defi- ciency all had less than 1 percent levels and the patient with F IX deficiency had a level of 1 percent.
The stage of knee joint involvement was classified radiographically as Stage 2 in one patient, Stage 3 in two patients, and Stage 4 in two patients.
All patients had symptoms of frequent hemarthrosis with persistent knee joint swelling. In addition, the patients with Stage 4 disease had symptoms of pain with activity.
Examination of the knees demon- strated marked synovial hypertrophy and effusion in the patients with Stage 2 and 3 disease (Figure 1) while the two patients with Stage 4 disease showed a moderate synovial hypertrophy plus crepitance with joint motion.
The range-of-motion was reduced slightly, particularly in flexion, in Stage 3 and Stage 4 (Table 1).
TABLE 1 .
Pat. Age Factor Joint Range of Motion Deficiency Stage Extension Flexion
1 , 13 VIII &l%) I1 O0 150'
3. 1 5 VlII (<l%) 111 Oo 125' 4. 18 VIII (<l%) IV 5' 115'
2 . 13 VIII (51%) 111 oo 125O
5 . 36 IX ( 1%) IV 5 0 l l o o
Figure 1 . Marked synovial hypertrophy and effusion of left knee in a 13-year-old male with Stage 2 hemo- philic arthropathy.
All of the patients had a preoperative evaluation in the comprehensive hemo- philia clinic, at which time a factor level and an inhibitor study was performed. The presence of an inhibitor was consi- dered a contraindication to surgery.
Throughout hospitalization, the hema- tology and orthopaedic services jointly cared for the patients. One hour before surgery the patient received the appro- priate factor replacement in the amount to produce a 100 percent plasma factor level. This was repeated in 12 hours. The dose was then reduced to half and re- peated every 12 hours for approximately 7-10 days, and then the frequency was decreased to a daily dose. The length of time that a scheduled dose of factor re- placement was given depended upon the individual case, with special considera- tion given to the intensity of the physical therapy and the status of the knee. Every other day, factor replacement was given for 2-3 weeks if physical therapy was prolonged. Usually, by 3-4 weeks, fac-

ARTHROSCOPIC SYNOVECTOMY 265
tor replacement was given only on a need basis.
The surgical procedure required a stan- dard arthroscopic surgery setup. A tour- niquet was used but generally not inflated until after the diagnostic examination was completed.
To assure adequate distention of the joint and good fluid flow, two 3-liter bags of sterile saline, located at least one meter above the level of the knee, were attached to a large inflow cannula at least 4 mm in diameter via Y-tubing (TUR tubing).
For viewing, a 30 degree and 70 degree arthroscope with a video system was used. It was necessary to use a high inten- sity light source when using the video to assure good visualization.
Examination of the joint was accomp- lished through an inferolateral portal, using a 30 degree arthroscope. Once this was accomplished, the tourniquet was in- flated and the synovectomy begun, using motorized instruments. Four anterior in- sertion sites were routinely used: the standard inferomedial and inferolateral sites plus medial and lateral suprapatellar sites. Three of these sites were used si- multaneously: one for the inflow cannu- la, one for the arthroscope, and one for the shaver.
In addition to these four anterior por- tals, a posteromedial approach was used to remove synovium from the postero- medial compartment. Either two portals were used, one for the arthroscope and the other for the shaver, or if the 70 de- gree arthroscope could be inserted through the intercondylar notch to ob- serve the posterior compartments, then a single posterior portal was used for inser- tion of the synovial resector. Occasional-
ly, a posterolateral portal was used if satisfactory removal of synovium was not accomplished through the anterior inferolateral portal.
Various types of cartilage and meniscal shavers were used to most effectively remove synovium. Shavers with the larg- est windows and variable speed control, including the 5.5 mm synovial resector, performed best on large surfaces, whereas, smaller meniscal cutters worked better in small spaces like the notch and posterior compartments and along bony margins, such as erosions, osteophytes, and adjacent to the articular surfaces.
The synovium most accessible was re- moved first. This was usually the supra- patellar pouch and the medial and lateral recesses. Synovectomy in the posterior compartments was performed next. A problem of bleeding was frequently en- countered after removal of synovium from the fat pad area, making visualiza- tion more difficult when attempting synovectomy in the posterior compart- ments. Therefore, complete excision of the synovium from the infrapatellar fat pad and anterior intercondylar notch area was generally performed last.
The procedure requires meticulous technique, patience, and time. Initially, between 2 and 3 hours were required to accomplish these synovectomies. If the tourniquet was deflated before comple- tion, which was done any time the pro- cedure extended past 90 minutes, the joint was easily cleared once the tourni- quet was reinflated and continuous irri- gation reestablished. A decrease in the total operating time was possible once larger and more aggressive synovial re- sectors became available.
Once the procedure was completed,
266 WIEDEL
two one-eighth inch drainage tubes were inserted through the inferior medial and lateral portals by means of a sharp trocar, then passed superiorly into the supra- patellar pouch and out through the skin and attached to a suction system.
The incisions were closed with either subcuticular absorbable suture or a steri- strip tape. A sterile dressing was then ap- plied, followed by a long leg compression dressing with medial and lateral plaster splints holding the knee in extension.
Postoperatively, within the first 24 hours, the patient started physical thera- py, consisting of isometrics and leg lifts. Range-of-motion exercises began when the compression dressing was removed, which was 48-72 hours postoperatively and 24 hours after removal of the drains. The drains were removed in 24-48 hours, depending upon the amount of drainage, but never left in place more than 48 hours. Whirlpool baths were in- stituted to assist in range-of-motion exer- cises after 72 hours or when all incisions were dry.
RESULTS
The hospitalization time averaged 17 days, ranging from 5-30 days.
Two of the five patients required mani- pulation; one, with Stage 3 , at 14 days, and the other, with Stage 4, at 27 days. Manipulation was considered if the pa- tient was not showing a progressive in- crease in range-of-motion and had not passed 60 to 70 degrees by 14 days.
All patients in followup regained com- pletely their preoperative range-of-mo- tion.
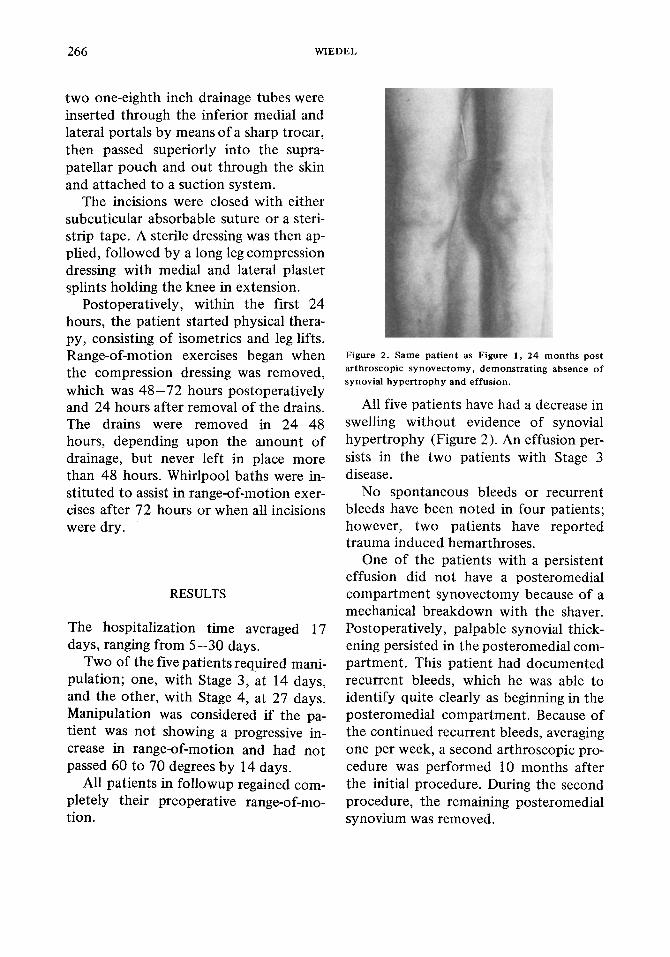
Figure 2. Same patient as Figure 1 , 24 months post arthroscopic synovectomy, demonstrating absence of synovial hypertrophy and effusion.
All five patients have had a decrease in swelling without evidence of synovial hypertrophy (Figure 2). An effusion per- sists in the two patients with Stage 3 disease.
No spontaneous bleeds or recurrent bleeds have been noted in four patients; however, two patients have reported trauma induced hemarthroses.
One of the patients with a persistent effusion did not have a posteromedial compartment synovectomy because of a mechanical breakdown with the shaver. Postoperatively, palpable synovial thick- ening persisted in the posteromedial com- partment. This patient had documented recurrent bleeds, which he was able to identify quite clearly as beginning in the posteromedial compartment. Because of the continued recurrent bleeds, averaging one per week, a second arthroscopic pro- cedure was performed 10 months after the initial procedure. During the second procedure, the remaining posteromedial synovium was removed.
ARTHROSCOPIC SYNOVECTOMY 26 7
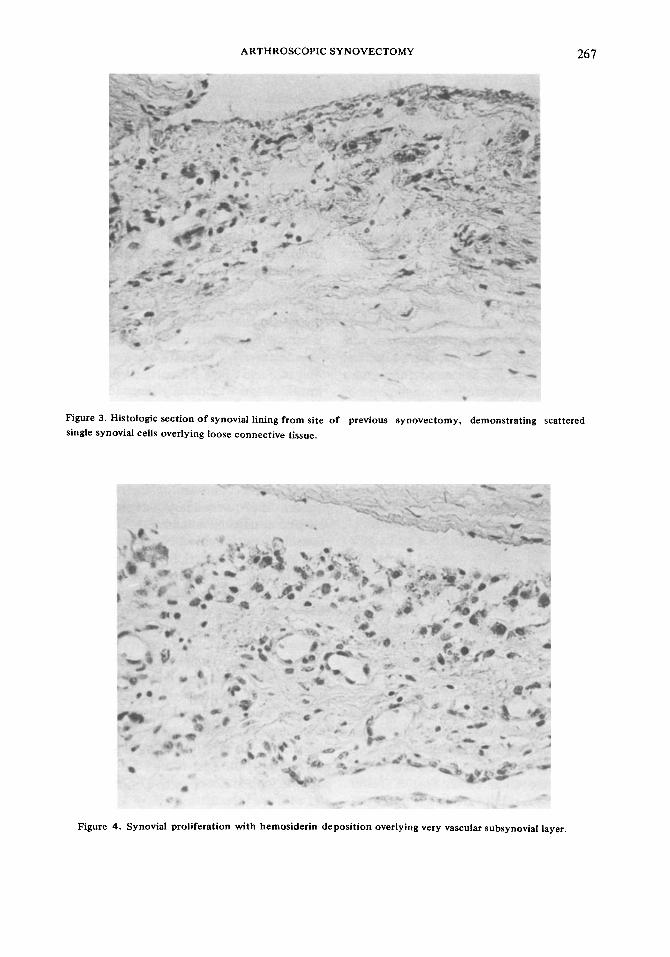
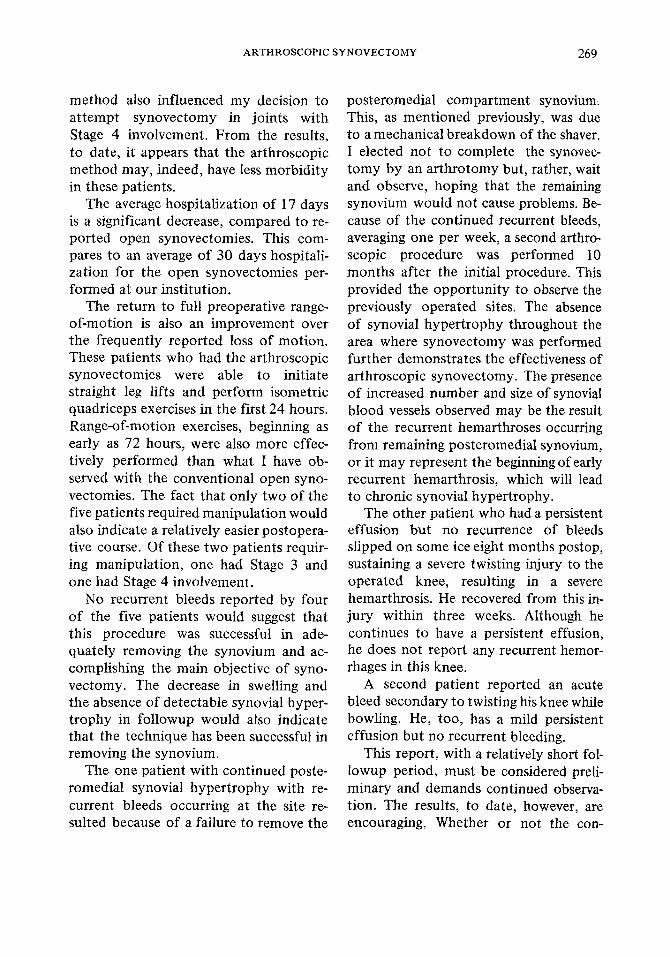
Figure 3. Histologic section of synovial lining from site of previous synovectomy, demonstrating scattered single synovial cells overlying loose connective tissue.
Figure

268 WIEDEL
This second procedure also allowed me to directly observe the synovial lining from the previous synovectomy. There was not evidence of hypertrophic pig- mented synovial tissue. The lining of the joint appeared white and glistening; how- ever, there were numerous large vessels appearing on the surface. In some areas there were noted small hemorrhages from these vessels.
A biopsy was taken of the surface membrane in the suprapatellar pouch where the previous synovectomy had been accomplished.
A thin synovial layer with underlaying loose connective tissue appeared in most places (Figure 3). Scattered throughout the biopsy area were very small areas of synovial proliferation but no villous formation (Figure 4).
Presently, this patient is not reporting any recurrent bleeding into this joint.
Other than this problem, no complica- tions occurred as a result of the arthro- scopic synovectomies.
DISCUSSIONS
The main objectives of synovectomy for chronic hemophilic arthropathy are to stop recurrent hemarthroses and, hope- fully, prevent further destruction of ar- ticular cartilage. To accomplish this, synovectomy should be done before ad- vanced joint changes have occurred.
Most authors agree that the results are better when the synovectomy is per- formed early, before radiographic evid- ence of cartilage involvement (Arnold & Hilgartner 1977, Dyszy-Laube et a1 1974, Pietrogrande et a1 1972, Post & Telfer 1978). These results are based upon the number of postoperative bleeds and joint
mobility. The followup of our patients is still
too short to determine if synovectomy will, indeed, prevent further cartilage destruction.
Although radiographic changes have traditionally been used to stage the disease process, actual articular cartilage involvement is impossible to determine unless directly observed. In fact, in this group of patients, joints which are classi- fied radiographically as Stage 2 and 3 had more advanced articular cartilage changes when directly observed than what the classification indicates.
In this series of patients, one had Stage 2 and two had Stage 3 involvement of their knees. Stage 3 is usually considered the latest stage at which arthropathy is still reversible with treatment. Two patients had Stage 4 involvement of the knee. Both of these patients complained of discomfort with activity, probably related to the advanced nature of their disease process and secondary degenerative arthritic condition. In addition, these pa- tients had documented recurrent bleeds with palpable synovial thickening. Both patients felt the recurrent bleeds inter- fered enough with their activity that they were willing to undergo synovec- tomy, knowing the risks of possible loss of joint mobility.
These two patients were also highly motivated individuals, which aided in making the decision to perform the synovectomy. This aspect of the patient’s pscyhological makeup is an extremely important preoperative evaluation. With- out a doubt, the best results are seen in patients who are cooperative, motivated, and who are tolerant to pain.
Lower morbidity with the arthroscopic
ARTHROSCOPIC SYNOVECTOMY 269
method also influenced my decision to attempt synovectomy in joints with Stage 4 involvement. From the results, to date, it appears that the arthroscopic method may, indeed, have less morbidity in these patients.
The average hospitalization of 17 days is a significant decrease, compared to re- ported open synovectomies. This com- pares to an average of 30 days hospitali- zation for the open synovectomies per- formed at our institution.
The return to full preoperative range- of-motion is also an improvement over the frequently reported loss of motion. These patients who had the arthroscopic synovectomies were able to initiate straight leg lifts and perform isometric quadriceps exercises in the first 24 hours. Range-of-motion exercises, beginning as early as 72 hours, were also more effec- tively performed than what I have ob- served with the conventional open syno- vectomies. The fact that only two of the five patients required manipulation would also indicate a relatively easier postopera- tive course. Of these two patients requir- ing manipulation, one had Stage 3 and one had Stage 4 involvement.
No recurrent bleeds reported by four of the five patients would suggest that this procedure was successful in ade- quately removing the synovium and ac- complishing the main objective of syno- vectomy. The decrease in swelling and the absence of detectable synovial hyper- trophy in followup would also indicate that the technique has been successful in removing the synovium.
The one patient with continued poste- romedial synovial hypertrophy with re- current bleeds occurring at the site re- sulted because of a failure to remove the
posteromedial compartment synovium. This, as mentioned previously, was due to a mechanical breakdown of the shaver. I elected not to complete the synovec- tomy by an arthrotomy but, rather, wait and observe, hoping that the remaining synovium would not cause problems. Be- cause of the continued recurrent bleeds, averaging one per week, a second arthro- scopic procedure was performed 10 months after the initial procedure. This provided the opportunity to observe the previously operated sites. The absence of synovial hypertrophy throughout the area where synovectomy was performed further demonstrates the effectiveness of arthroscopic synovectomy. The presence of increased number and size of synovial blood vessels observed may be the result of the recurrent hemarthroses occurring from remaining posteromedial synovium, or it may represent the beginning of early recurrent hemarthrosis, which will lead to chronic synovial hypertrophy.
The other patient who had a persistent effusion but no recurrence of bleeds slipped on some ice eight months postop, sustaining a severe twisting injury to the operated knee, resulting in a severe hemarthrosis. He recovered from this in- jury within three weeks. Although he continues to have a persistent effusion, he does not report any recurrent hemor- rhages in this knee.
A second patient reported an acute bleed secondary to twisting his knee while bowling. He, too, has a mild persistent effusion but no recurrent bleeding.
This report, with a relatively short fol- lowup period, must be considered preli- minary and demands continued observa- tion. The results, to date, however, are encouraging. Whether or not the con-

270 WlEDEL
tinued absence of recurrent bleeds and no recurrence of synovial hypertrophy will compare with those of the reported open synovectomies remains to be seen.
REFERENCES
Arnold W & Hilgartner M (1977) Hemophilic arthro- pathy: Current concepts of pathogenesis and management. J B o n e Joint Surg 59A, 287- 305.
Clark M (1978) Knee synovectomy in hemophilia. Orthopedics 1, 285-290.
Dyszy-Laube B, Kaminski W, Gizycka I, Kaminska D, Sekowska-Zmuda J & Ludert, E (1 974) Synovec- tomy in the treatment of hemophilic arthropathy. J P e d i a t S u r g 9 , 123-125.
Greer R, I11 (1980) Operative Management of hemo- philic arthropathy - An overview. Orthopedics 3, 135- 138.
McCollough N, 111, Enis J , Lovitt J , Chun-Yet Lian E Niemann K & Loughlin E, Jr (1979) Synovectomy or total replacement of the knee in hemophilia. J Bone Jo in t Surg 61A, 69-75.
Pietrogrande V, Dioguardi N & Mannucci P (1972) Short-term evaluation of synovectomy in haerno- philia.BritMed J 2 , 378-381.
Post M & Telfer M (1975) Surgery in hemophilic patients. J B o n e Jo in t Surg S I A , 1136-1145.
Storti E & Ascari E (1975) Surgical and chemical synovectomy. Ann N Y Acad Sci 240, 316-327.
Storti E, Traldi A, Tosatti E & Davoli P (1969) Syno- vectomy - A new approach t o haemophilic arthro- pathy. Acta Haemat 41, 193-205.