are we up to speed?
TRANSCRIPT

T
J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 6 , N O . 1 1 , 2 0 1 3
ª 2 0 1 3 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 3 . 0 9 . 0 0 7
From Big Data to Rich Insights in CV Imaging for a Hyperconnected World
Are We Up to Speed?
Jagat Narula, MD, PHD
he first software implementation of the heatmap display was developed in 1991 (1) and
has been used since then as a mainstream toolin systems biology for communicating in-teractions among genes, proteins, and metabolitesthat define life processes. In general, heat maps areconsidered a flexible visualization tool for dataclusters and to explore patterns using rectangular,color-coded arrays that display the conceptual andstatistical linkages among variables plotted along thex and y axes. This issue of iJACC presents a view-point in which heat maps are suggested as a step toexplore the structure of big databases recordedduring the assessment of cardiac function (2). Theexamples of data interactions that distinguish thepattern of left ventricular deformation seen in pa-tients with constrictive pericarditis and restrictivecardiomyopathy illustrate the potential value of heatmap visualization, symbolizing the burgeoning in-terest in big data in health care (3,4). Cardiacimaging and radiology are generating multiple ter-abytes of images every year, and the picture archivingand communication system market is projected todouble in the next 5 years. Although several view-points have been recently published regarding theemerging role of big data in health care (3,4), it isworth questioning what healthcare big data one maypossibly find concealed in the images and how thisnew knowledge could be extracted despite the exist-ing challenges in healthcare information technology.
The term big data has evolved as a catchword forsmart, more insightful data analyses of both struc-tured and unstructured data. For cardiac imaging,big data analytics can refer to the informationaccrued from echocardiography, angiography, andmagnetic resonance imaging or computed tomog-raphy. One could further contemplate the specificinteractions of imaging data with electronic medicalrecords, home monitoring devices, genomic data,insurance claims, and drug information forimproving patient outcomes. Current economicconcerns, perhaps more than any other factor, aredriving more scrutiny and demands for big data
From the Icahn School of Medicine at Mount Sinai, New York,
New York.
applications. President Obama approved the $200million Big Data Research and DevelopmentInitiative (5), and both the National Institutes ofHealth and the National Science Foundation haveidentified big data as a program focus for solicitingproposals that emphasize collection, deidentifica-tion, validation, archiving, and dissemination oflarge volumes of imaging and associated genetic,pathological, and clinical data generated from clin-ical research projects and clinical trials with the aimof enabling meaningful organization of the data.Furthermore, the United States federal governmentand other public agencies have recently made avail-able their massive stores of healthcare knowledge,including data from clinical trials and informationon patients covered under public insurance pro-grams. The potential value of big data in health careand global economic trends in the utilization ofmobile applications and telemedicine has alsomotived global organizations. For example, theUnited Nations has prioritized a workforce calledGlobal Pulse that is currently working to connect thedots between data mining and humanitarianism, aneffort that may enable digitally mapping the devel-opment of a global healthcare ecosystem. The bigdata revolution, indeed, has been rightly referred toas our “planet developing a digital nervous system”;several real-time sensors and monitoring devices arein the commercial pipeline and are expected to movediagnostics into an individual’s own personal space,creating a hyperconnected world that liberateshealth-care monitoring and decisions from the wallsof the clinic or hospital into individuals’ commu-nities and homes.
Although the prospects of big data in health careare exciting, its use in cardiovascular imaging posesunique challenges, both for individual providersand at the institutional level. At the provider level,some physicians are likely to feel intimidated by thedecision-making prospects of big data science,arguing that intelligent machines and computa-tional algorithms may displace the traditional art ofmedicine and critical thinking. Perhaps theappropriate attitude would be to form a human-computer synergy that will surpass the capabilitiesof either alone, just as we use Google Maps to
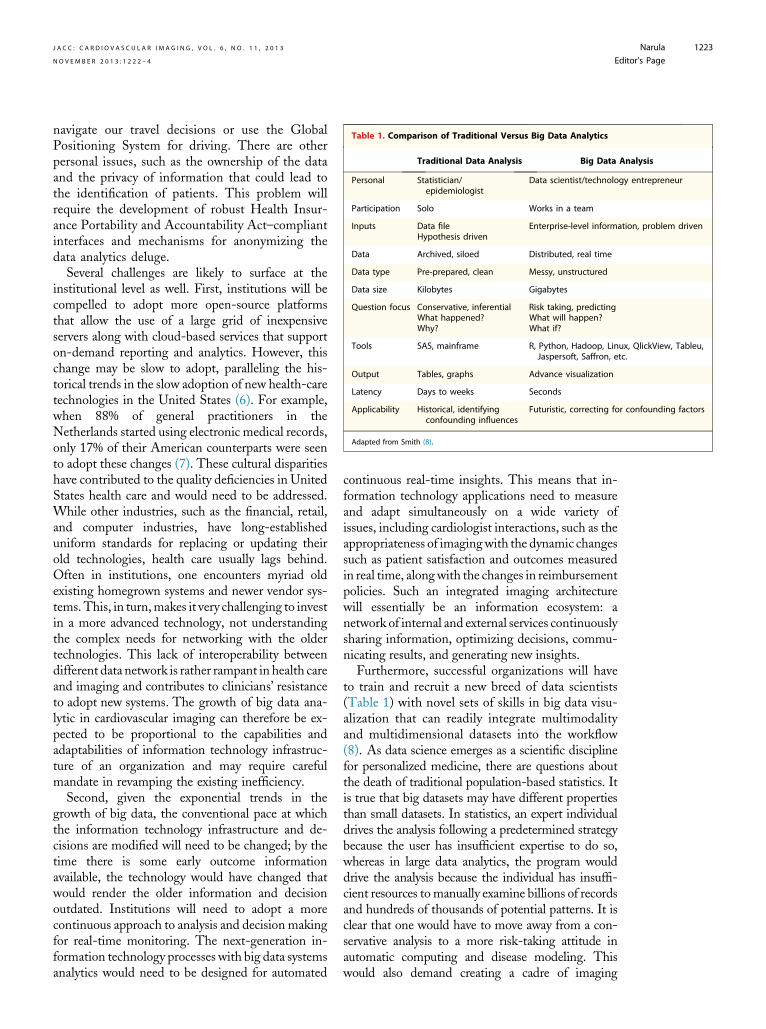
Table 1. Comparison of Traditional Versus Big Data Analytics
Traditional Data Analysis Big Data Analysis
Personal Statistician/epidemiologist
Data scientist/technology entrepreneur
Participation Solo Works in a team
Inputs Data fileHypothesis driven
Enterprise-level information, problem driven
Data Archived, siloed Distributed, real time
Data type Pre-prepared, clean Messy, unstructured
Data size Kilobytes Gigabytes
Question focus Conservative, inferentialWhat happened?Why?
Risk taking, predictingWhat will happen?What if?
Tools SAS, mainframe R, Python, Hadoop, Linux, QlickView, Tableu,Jaspersoft, Saffron, etc.
Output Tables, graphs Advance visualization
Latency Days to weeks Seconds
Applicability Historical, identifyingconfounding influences
Futuristic, correcting for confounding factors
Adapted from Smith (8).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3 Narula
N O V E M B E R 2 0 1 3 : 1 2 2 2 – 4 Editor’s Page
1223
navigate our travel decisions or use the GlobalPositioning System for driving. There are otherpersonal issues, such as the ownership of the dataand the privacy of information that could lead tothe identification of patients. This problem willrequire the development of robust Health Insur-ance Portability and Accountability Act–compliantinterfaces and mechanisms for anonymizing thedata analytics deluge.
Several challenges are likely to surface at theinstitutional level as well. First, institutions will becompelled to adopt more open-source platformsthat allow the use of a large grid of inexpensiveservers along with cloud-based services that supporton-demand reporting and analytics. However, thischange may be slow to adopt, paralleling the his-torical trends in the slow adoption of new health-caretechnologies in the United States (6). For example,when 88% of general practitioners in theNetherlands started using electronic medical records,only 17% of their American counterparts were seento adopt these changes (7). These cultural disparitieshave contributed to the quality deficiencies in UnitedStates health care and would need to be addressed.While other industries, such as the financial, retail,and computer industries, have long-establisheduniform standards for replacing or updating theirold technologies, health care usually lags behind.Often in institutions, one encounters myriad oldexisting homegrown systems and newer vendor sys-tems. This, in turn,makes it very challenging to investin a more advanced technology, not understandingthe complex needs for networking with the oldertechnologies. This lack of interoperability betweendifferent data network is rather rampant in health careand imaging and contributes to clinicians’ resistanceto adopt new systems. The growth of big data ana-lytic in cardiovascular imaging can therefore be ex-pected to be proportional to the capabilities andadaptabilities of information technology infrastruc-ture of an organization and may require carefulmandate in revamping the existing inefficiency.
Second, given the exponential trends in thegrowth of big data, the conventional pace at whichthe information technology infrastructure and de-cisions are modified will need to be changed; by thetime there is some early outcome informationavailable, the technology would have changed thatwould render the older information and decisionoutdated. Institutions will need to adopt a morecontinuous approach to analysis and decision makingfor real-time monitoring. The next-generation in-formation technology processes with big data systemsanalytics would need to be designed for automated
continuous real-time insights. This means that in-formation technology applications need to measureand adapt simultaneously on a wide variety ofissues, including cardiologist interactions, such as theappropriateness of imagingwith the dynamic changessuch as patient satisfaction and outcomes measuredin real time, alongwith the changes in reimbursementpolicies. Such an integrated imaging architecturewill essentially be an information ecosystem: anetwork of internal and external services continuouslysharing information, optimizing decisions, commu-nicating results, and generating new insights.
Furthermore, successful organizations will haveto train and recruit a new breed of data scientists(Table 1) with novel sets of skills in big data visu-alization that can readily integrate multimodalityand multidimensional datasets into the workflow(8). As data science emerges as a scientific disciplinefor personalized medicine, there are questions aboutthe death of traditional population-based statistics. Itis true that big datasets may have different propertiesthan small datasets. In statistics, an expert individualdrives the analysis following a predetermined strategybecause the user has insufficient expertise to do so,whereas in large data analytics, the program woulddrive the analysis because the individual has insuffi-cient resources to manually examine billions of recordsand hundreds of thousands of potential patterns. It isclear that one would have to move away from a con-servative analysis to a more risk-taking attitude inautomatic computing and disease modeling. Thiswould also demand creating a cadre of imaging

Narula J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 6 , N O . 1 1 , 2 0 1 3
Editor’s Page N O V E M B E R 2 0 1 3 : 1 2 2 2 – 4
1224
specialists who focus upon database processing algo-rithms for integrating new understanding into theknowledge domain.In summary, imaging big data will prompt orga-
nizations to rethink their basic assumptions aboutthe relationships among imagers, data scientists, andinformation technology professionals and theirrespective roles.Although the questions and potentialsolutions may be varied, there is little doubt aboutthe manifold value that imaging big data will
potentially provide, with new insights into disease,treatment, and interventions. This was essentially thepurpose of highlighting an intuitive and futuristicviewpoint (2) by displaying the heat map on the coverpage.
Address for correspondence: Dr. Jagat Narula, IcahnSchool of Medicine at Mount Sinai, Mount Sinai Heart,One Gustave L. Levy Place, Mailbox 1030, New York,New York 10029. E-mail: [email protected].
R E F E R E N C E S
1. United States Patent and Trademark Of-fice. Registration #75263259. September 1,1993.
2. Sengupta PP. Intelligent platforms fordisease assessment: novel approaches infunctional echocardiography. J Am CollCardiol Img 2013;6:1206–11.
3. Larson EB. Building trust in thepower of “big data” research to servethe public good. JAMA 2013;309:2443–4.
4. Murdoch TB, Detsky AS. The inevi-table application of big data to healthcare. JAMA 2013;309:1351–2.
5. Kalil T, Zhao F. Unleashing thepower of big data. Available at: http://www.whitehouse.gov/blog/2013/04/18/unleashing-power-big-data. AccessedSeptember 17, 2013.
6. Poon EG, Jha AK, Christino M, et al.Assessing the level of healthcare infor-mation technology adoption in the
United States: a snapshot. BMC MedInform Decis Making 2006;6:1.
7. Harris Interactive. European physiciansespecially in Sweden, Netherlands andDemark, lead U.S. in use of electronicmedical records. Health Care News2002;2:1–3.
8. Smith D. Statistics vs data science vs BI.Available at: http://blog.revolutionanalytics.com/2013/05/statistics-vs-data-science-vs-bi.html. Accessed September 17, 2013.