are psychological treatments of panic disorder...
TRANSCRIPT

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 1
Are psychological treatments of panic
disorder efficacious?
Peter Wilhelm
7.3 and 14.3.2018

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 2
Efficacy of Behavioral Treatment of Panic Disorder
First randomised controlled trial
Barlow and colleagues
Barlow, D. H., Craske, M. G., Cerny, J. A. & Klosko, J. S. (1989). Behavioral treatment of panic disorder. Behavior Therapy,
20, 261-282.
Craske, M. G., Brown, T. A. & Barlow, D. H. (1991). Behavioral treatment of panic disorder: A two-year follow-up. Behavior
Therapy, 22, 289-304.
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 3
Individual experiences recurrent unexpected panic attacks,
and is persistently concerned or worried about having more panic attacks,
or changes his or her behavior in maladaptive ways because of the panic attacks (e.g., avoidance of exercise or of unfamiliar locations).
Panic attacks are abrupt surges of intense fear or intense discomfort that reach a peak within minutes, accompanied by physical and/or cognitive symptoms:
• e.g. accelerated heart rate, sweating, trembling or shaking, shortness of breath, chest pain or discomfort.., fear of loosing control, fear of dying.
12 month prevalence: 2-3%, women vs men: 2:1
High comorbidity
Efficacy of Behavioral Treatment of Panic Disorder
Background: Panic Disorder, DSM 5 (p. 190)

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 4
State of the art treatment for panic disorder, in the1980s,
when the study was conducted:
• Panic attacks can effectively be treated with
psychoactive drugs (Benzodiazipines)
Behavioral therapy is effective in treating avoidance behavior
(via in vivo confrontation)
• Implicit assumption: Behavioral therapy is not an efficacious
treatment for panic disorder without agoraphobic avoidance
Efficacy of Behavioral Treatment of Panic Disorder
Background

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 5
Is cognitive behavioral therapy (CBT) efficacious for the
treatment of panic disorder without agoraphobic
avoidance?
State of research
• Several case studies in which CBT led to an improvement
(e.g. Gitlin et al., 1985; Clark, Salkovskis & Chalkley, 1985)
• 1 controlled pilot study (Biofeedback, PMR & cognitive Therapy
vs. waiting list control group), with 11 patients (Barlow, Cohen et
al., 1984)
Efficacy of Behavioral Treatment of Panic Disorder
Background

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 6
Objective:
Evaluating the efficacy of a newly developed CBT for the
treatment of panic disorder
Efficacy of Behavioral Treatment of Panic Disorder
Aim of the studie
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 7
Exposition & cognitive Therapy (E&C)
Cognitive restructuring: Acquiring skills for re-evaluating beliefs and appraisals about environmental and internal physiological cues
• analysis of faulty logic, reattribution, decatastrophizing, self instruction
Interoceptive exposure after the 5th session: • Anxiety hierarchy.
• Cognitive skills were applied to anxiety provocing situations through visualisation of anxiety scences and overbreathing.
Progressive Muscle Relaxation (R)
2x exercises per day. After 5th session: exercising the use of relaxation as a coping skill
Relaxation combined with exposition und cognitive therapy (Comb)
Wait list control group
Efficacy of Behavioral Treatment of Panic Disorder
Treatment conditions

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 8
Single Therapy: 1 x per week, 15 weeks
Treatment manuals: detailed description for evry session
Therapist: 10 doctoral students and psychologists, who were trained for all interventions
Weekly supervision
Treatment Integrity • All sessions were audiotaped
• 35 tapes were randomly selected: Two 5 min segments were selected and therapist behavior was rated
• Patients rated credibility and Logic of treatment (after 1. and last session, follow up)
Efficacy of Behavioral Treatment of Panic Disorder
Application of treatments
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 9
Patients of „Phobia and Anxiety Disorder Clinic“,
State University of New York
Panic Disorder without or only slight Agoraphobia
Efficacy of Behavioral Treatment of Panic Disorder
Participants

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 10
Inclusion Criteria
DSM III-R: Panic disorder, no or slight agoraphobic avoidance
Therapist Rating: Severity of disorder > 4 (Scale 0 to 8) (Anxiety Disorder Interview Schedule-Revised; ADIS-R)
At least 1 attack within the last 2 weeks (diary, 4 times daily)
Patients who already got other treatments not related to anxiety
Stable medication
Exclusion Criteria
Age 18 to 65;
Alcohol- or substance abuse
Major depression, psychosis, organic brain syndrome
Other therapies of anxiety /
Begin of Psychopharmacological treatment • less than 3 Mon. benzodiazepines,
• less than 6 Mon. MAO-Hemmer, tricyclic antidepressants)
Efficacy of Behavioral Treatment of Panic Disorder
Sample: Inclusion and exclusion criteria

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 11
Standardized Interviews (blind judges)
Hamilton Anxiety and Depression Scales
Standardized Self-Reports
State-Trait Anxiety Inventory (Spielberger, Gorusch, & Lushene, 1970)
Cognitive Somatic Anxiety Questionnaire, (Marks & Mathews, 1979),
Fear Questionnaire (Marks & Mathews, 1979)
Beck Depression Inventory (Beck et al., 1961)
Psychosomatic Rating Scale (Cox, Freundlich & Meyer, 1975)
Subjective Symptom Scale (Modification, Hafner & Marks, 1978)
Self-Observation: Structured diary (4 times daily) Anxiety Rating from 0 to 8; Panic yes/no; stressful events?
Efficacy of Behavioral Treatment of Panic Disorder
Meassurements

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 12
Treatment responder
20% Improvement in three of four measures:
Clinical rating of severity (> 2 points)
Fear Questionnaire (> 2 points)
Number of panic attacks per week
Subjective Symptom Scale Total score (> 8 points)
Treatment non-responder
Deterioration of 20% (Pre-Post) in any of the measures (independent of improvement in other variables)
End state functioning
absolute level of functioning at Post-Assessment(only completers) • low end state (LES) vs high end state (HES)
Efficacy of Behavioral Treatment of Panic Disorder
Composite measures of clinically significant change
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 13
Patients were randomly assigned to 4 conditions
Assessment : Pre – Post – Follow up: 3, 6, 12, 24 months
Efficacy of Behavioral Treatment of Panic Disorder
Research Design

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 14
Efficacy of Behavioral Treatment of Panic Disorder
Sample size and drop-outs (in %)
Comparison drop-outs vs. completers (ANOVAS)
Drop-outs: lower severity at pre treatment
Higher consumption of anxiolytics
Pre Post 6-Month 24-Month
Wait-list 16 15 (6%) - -
Exposition (E) &
Cognitive Therapie (C)
16 15 (6%) 8 15
Relaxation (R) 15 10 (33%*) 9 9
Combined (E & C & R) 20 16 (17%) 6 10
* signifikant

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 15
Efficacy of Behavioral Treatment of Panic Disorder
Change in sample size over time

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 16
Efficacy of Behavioral Treatment of Panic Disorder
„Treatment Responders“ at Post-Assessment
significant
N = 54; lacking information for n = 13

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 17
Efficacy of Behavioral Treatment of Panic Disorder
„High End-State Functioning“ at Post-assessment
significant
N = 53; lacking information for n = 14
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 18
Efficacy of Behavioral Treatment of Panic Disorder
Comparison: Pre-Post Assessment
Reduction in clinical rating of severity
• All treatment groups significantly improved but not CG
• All treatment groups were significantly better than CG
Reduction in Hamilton Anxiety Score
• All treatment groups significantly improved but not CG
• R and Combined G were significantly better than control
group
Psychosomatic Symptoms
• Only relaxation group significantly improved
• Only R was significantly better than CG
No significant differences in the other measures
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 19
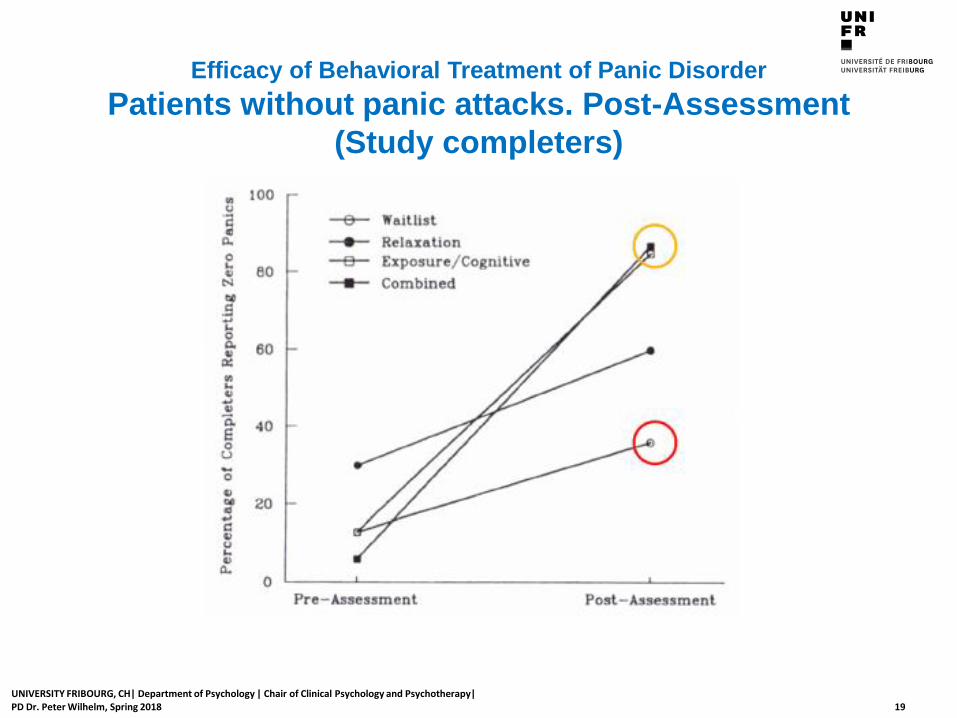
Efficacy of Behavioral Treatment of Panic Disorder
Patients without panic attacks. Post-Assessment
(Study completers)

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 20
Efficacy of Behavioral Treatment of Panic Disorder
Patients without panic attacks. Post-Assessment
(Intent to treat analysis with total sample)

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 21
Efficacy of Behavioral Treatment of Panic Disorder
24 Month Follow-Up: Summary
Maintainance of therapy success
Decrease of trait-anxiety and somatic symptoms
(Post vs. 24 months)
BDI-Scores
• Increase in R-group
• Decrease in E & C-group

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 22
Efficacy of Behavioral Treatment of Panic Disorder
Participants with high end state and without panic
(Excluding drop outs)

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 23
Efficacy of Behavioral Treatment of Panic Disorder
Participants with high end state and without panic
(Including drop outs)
significant for „Panic-Free“
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 24
Efficacy of Behavioral Treatment of Panic Disorder
24 months Follow-Up:
Other Psychological Treatments
Alternative Psychotherapy:
R 83%, E&C 33%, COMB 40%
Psychopharmaca
R 71%, E&C 17%, COMB 43%

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 25
Efficacy of Behavioral Treatment of Panic Disorder
Summary of results
Post Assessment: (R, E&C, E&C&R) > Wait list
In relaxation group, less patients were panic free,
However anxiety and psychosomatic symptoms were reduced.
Follow up: Maintenance of therapy success over 2 years
For patients with interoceptive exposer and cognitive restructuring
Patients in relaxation group less stable patterns
• Highest drop out rate
• Highest rate of additional treatment
Cognitive behavioral therapy with relaxation (E&C&R) was not more efficacious than E&C

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 26
Efficacy of Behavioral Treatment of Panic Disorder
Conclusions
Panic disorder without agoraphobic avoidance can be efficaciously treated with a combination of interoceptive exposer + cognitive restructuring
Directly after treatment, relaxation is as efficacious as interoceptive exposer + cognitive restructuring, but in the long run it is less efficacious.
Relaxation is not a necessary component of an efficacious treatment of panic disorder. Interoceptive exposer + cognitive restructuring is sufficient.
Compared to results in the literature, long term effects of interoceptive exposer and cognitive restructuring seem to better than pharmacological treatment
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 27
Cognitive-behavioral therapy, pharmacotherapy, or their combination for
treating panic disorder (PD): A randomized controlled trial (RCT)
(Barlow, Gorman, Shear, & Woods, 2000)
Barlow, D. H., Gorman, J. M., Shear, M. K., & Woods, S. W. (2000). Cognitive behavioral therapy, imipramine, or their
combination for panic disorder: A randomized controlled trial. Journal of the American Medical Association, 283,
2529–2536.
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 28
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Background
Background: Well established efficacy for two PD treatments
Psychological treatment: CBT
Pharmacological treatment with Imipramine (Tofranil)
• First tricyclic antidepressant, discovered 1951 by Ciba Geigy (today Novartis)
• increases the extracellular level of neurotransmitters (serotonin, norepinephrine ) by limiting their reabsorption (reuptake) into the presynaptic cells
• Broad range of effects
Improves mood, reduces symptoms of agitation and anxiety
side effects: dry mouth, drowsiness, dizziness, blurred vision, low blood pressure, rapid heart rate, increased sweating, diarrhea, stomach cramps, increase of appetite, weight gain
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 29
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Objectives
Relative and combined efficacies of drug and PT treatment for PD have not been evaluated
Objectives: To evaluate, whether
• drug and PT for PD are each more efficacious than placebo
• one treatment is more efficacious than the other
• combined therapy is more efficacious than either therapy alone?

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 30
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Study design
312 panic disorder patients were randomly assigned to five groups (double blind)
CBT
Imipramine
Drug placebo
CBT + Imipramine
CBT + Drug placebo

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 31
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Treatments (acute phase)
Treatments were manualized for each condition
Acute treatment phase: 11 sessions during 12 weeks for each condition
CBT • individual 50-minute sessions
Interoceptive exposure, cognitive restructuring, and breathing training
Psychopharmacotherapy (Imipramine or Placebo) + Clinical Management • individual 30-minute contacts
monitor adverse effects, clinical state, and physical/mental condition
maximize compliance
proscribe specific interventions included in CBT (cognitive restructuring of anxiety and panic symptoms)
Imipramine treatment was slowly titrated up to a maximum of 300 mg/day
Blood levels were assessed at 6 and 12 weeks
Combined Treatment (Imipramine or Placebo + CBT) • individual contacts with 2 therapists for about 75 minutes per week.
Benzodiazepine screening of urine samples
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 32
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Treatments (maintenance phase)
Responders to acute treatment entered a 6-month maintenance phase without breaking the study blind.
6 monthly appointments in which treatment similar to the acute treatment was continued
After maintenance phase treatment was stopped
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 33
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Therapists
Therapists providing CBT were doctoral level clinicians who underwent extensive training
Pharmacotherapists were experienced psychiatrists who underwent additional training
Ongoing supervision, biweekly
Adherence and competence ratings were collected after listening to a sample of audiotaped sessions

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 34
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Assessment
at baseline
after acute phase (3 months after baseline)
after maintenance phase (9 months after baseline)
after follow-up phase (15 months after baseline)
Trained evaluators (blind to treatment assignment) judged patients on
• Panic Disorder Severity Scale (PDSS)
clinician-rated scale of PD severity
Response was defined > 40% reduction of PD symptoms
• Clinical Global Impression Scale (CGI),
7-point ratings on 2 items: overall improvement and severity
Definition of responders:
• CGI much improved (≤ 2) while being rated as mild or less (≤ 3) on CGI severity
• Patients who received nonstudy treatment for anxiety = nonresponders

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 35
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Patients
Inclusion criteria:
Potential participants met DSM-III-R or DSM-IV criteria for PD with no more than mild agoraphobia (ADIS-R avoidance scale ≤ 18)
Panic attack(s) in the 2 weeks before treatment
Patients with comorbid unipolar depression were not excluded
Patients were permitted to take benzodiazepines until end of acute phase
Exclusion criteria
psychotic, bipolar, or significant medical illnesses,
suicidality, significant substance abuse,
contraindications to either treatment,
prior nonresponse to similar treatments,
concurrent competing treatment or pending disability claims

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 36
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Allocation of Patients

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 37
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Drop outs during acute phase
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 38
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
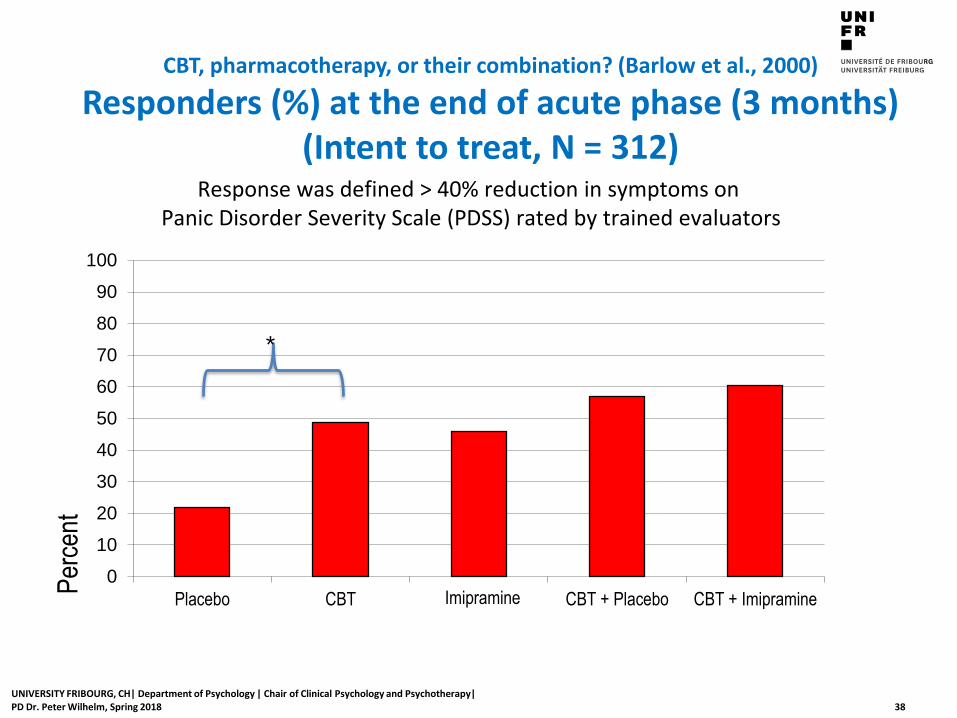
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (Intent to treat, N = 312)
*
Imipramine
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 39
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
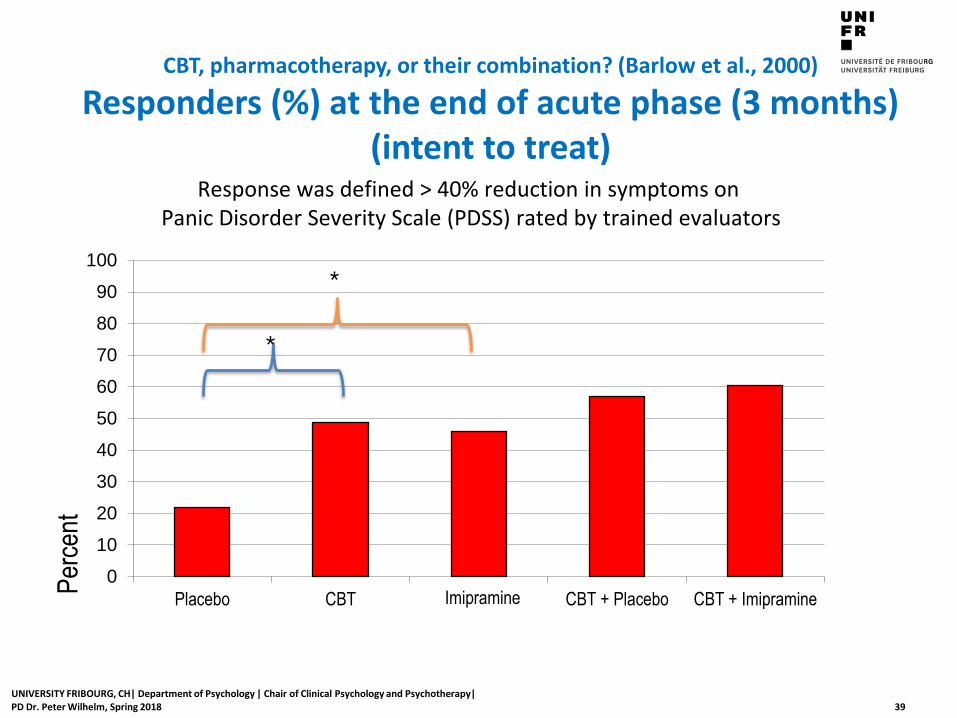
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (intent to treat)
*
*
Imipramine
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 40
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
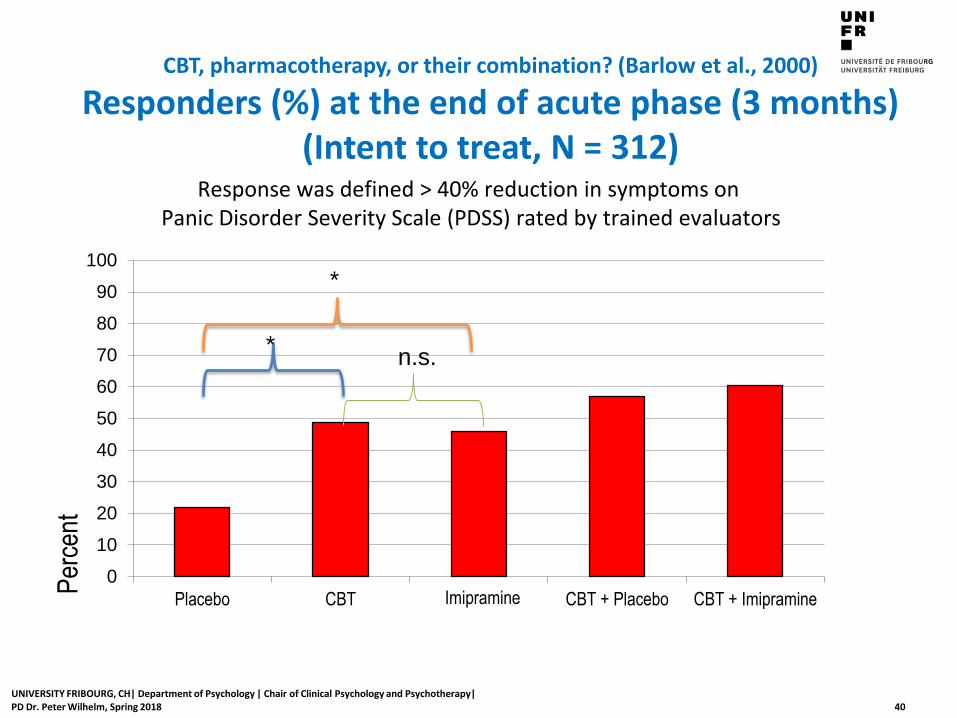
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
n.s.
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (Intent to treat, N = 312)
*
*
Imipramine

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 41
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
n.s.
n.s.
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (Intent to treat, N = 312)
*
*
Imipramine

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 42
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
n.s.
n.s.
n.s.
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (Intent to treat, N = 312)
*
*
Imipramine
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 43
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
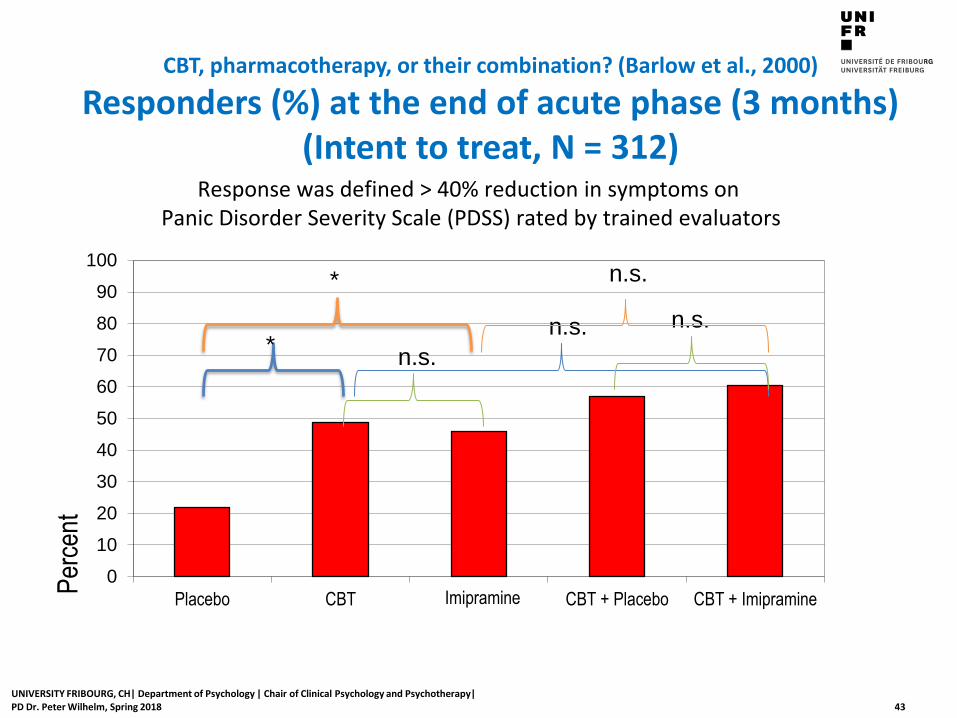
Response was defined > 40% reduction in symptoms on Panic Disorder Severity Scale (PDSS) rated by trained evaluators
n.s.
n.s. n.s.
n.s.
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (Intent to treat, N = 312)
*
*
Imipramine
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 44
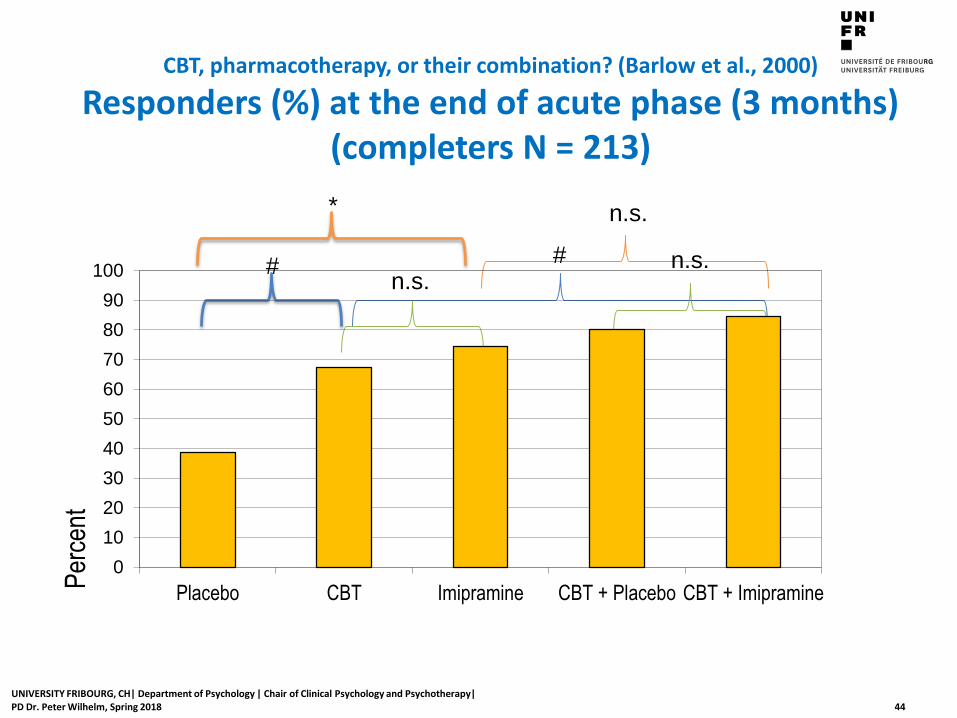
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of acute phase (3 months) (completers N = 213)
*
#
#
n.s.
n.s. n.s.
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT Imipramine CBT + Placebo CBT + Imipramine
Per
cent

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 45
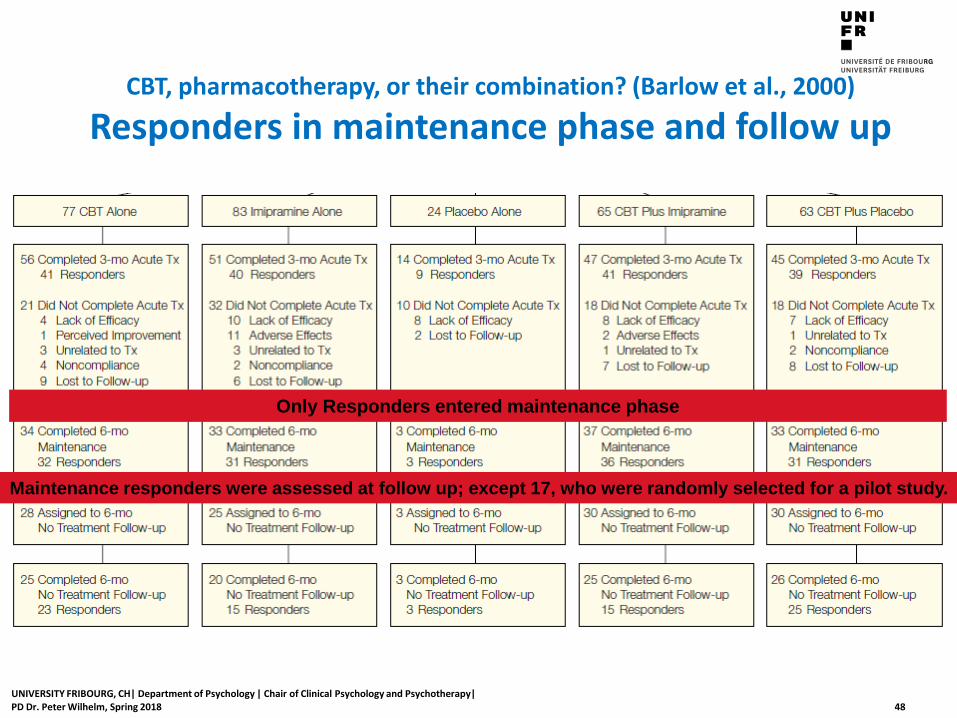
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders in maintenance phase and follow up
Only Responders entered maintenance phase

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 46
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of 6-month maintenance phase (Intention to continue maintenance N = 170)
*
#
#
n.s.
n.s. n.s.
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT Imipramine CBT + Placebo CBT + Imipramine
Per
cent

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 47
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of 6-month maintenance phase (Intent to treat, N = 312)
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
Imipramine
*
*
*
*
After 6-month maintenance phase: responders continued medication or monthly CBT
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 48
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders in maintenance phase and follow up
Only Responders entered maintenance phase
Maintenance responders were assessed at follow up; except 17, who were randomly selected for a pilot study.

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 49
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at the end of 6-month follow up phase (Intention to continue follow up: N = 116)
n.s.
n.s.
**
n.s.
* #
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT Imipramine CBT + Placebo CBT + Imipramine
Per
cent
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 50
0
10
20
30
40
50
60
70
80
90
100
Placebo CBT IPT CBT + Placebo CBT + Imipramine
Per
cent
#
Imipramine
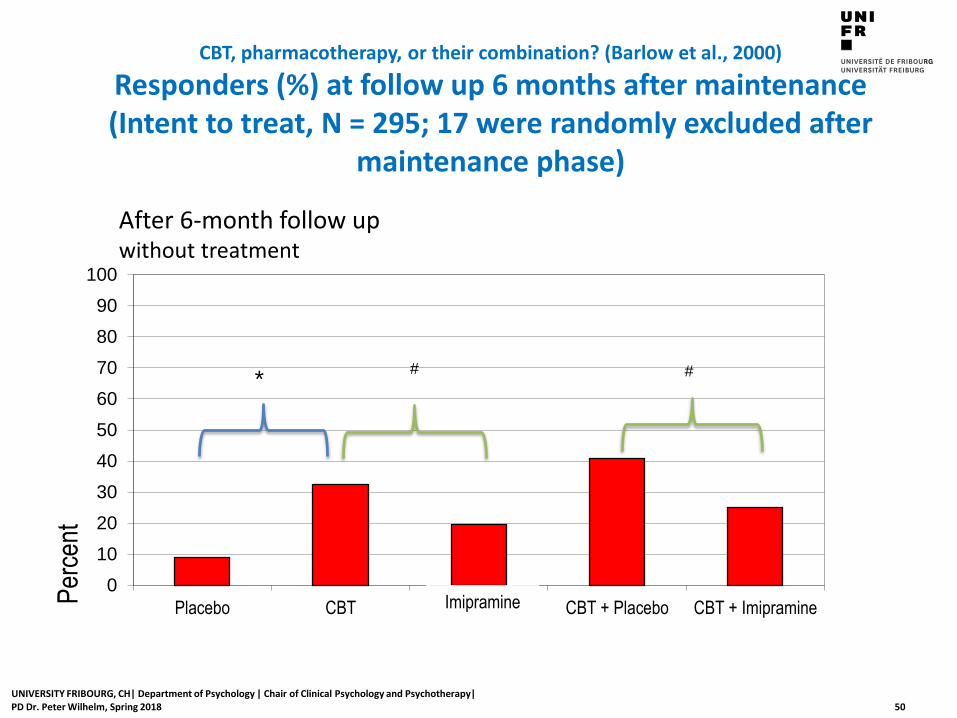
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Responders (%) at follow up 6 months after maintenance (Intent to treat, N = 295; 17 were randomly excluded after
maintenance phase)
* #
After 6-month follow up without treatment

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 51
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Summary and conclusions of the authors
Both imipramine and CBT are better than pill placebo for treatment of PD (post acute, post maintenance)
High attrition in placebo group; weak and non durable response
Imipramine produced a superior quality of response until end of maintenance
CBT had more durability and was somewhat better tolerated
• Relapse 4% for CBT, 25% for Imipramine
Coadministration of Imipramine and CBT resulted in limited benefit over monotherapy
• Improvement after maintenance
• addition of imipramine appeared to reduce long-term durability of CBT
Potential underestimation of benefits of medication by using a tricyclic antidepressant instead of an SSRI

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 52
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
What are limitations and problems of this study?

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 53
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
What are limitations and problems of this study?
Design is in favor of pharmacotherapy
• Pharmacotherapy = drug (placebo) + clinical management Imipramine and Placebo condition: Every week 30-minute contact with psychiatrist; recommendations and prescription
of exposure (not typical for usual psychiatric drug treatment) Combined treatment (Imipramine or Placebo + CBT), individual contacts with 2 therapists for about 75 minutes per week
(higher dosage of treatment than CBT alone)
• Assessment only based on external interviewer ratings of current symptoms and improvement. Patients perspective was not assessed, which shows usually less difference to placebo No adverse effects of treatment were assessed (side effects)
Pharmacotherapists were experienced psychiatrists; CBT therapists were doctoral level clinicians, prior
experience was not required
Placebo effect was probably underestimated • Blinding did probably not work for many patients because placebo did neither produce positive effects nor
side effects • Blinding did probably not work for doctors -> lower positive expectations
High and selective drop out rates impair interpretation of results
• Drop outs in placebo group: post = 58%, maintenance and follow up = 88% • Drop outs imipramine: post = 39%, maintenance = 52%, follow up = 68% • Drop outs CBT: post = 27%, maintenance = 47%, follow up = 62%
• -> underestimation of placebo effect in ITT analyses

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 54
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
What are limitations and problems of this study?
Selected patients who accept drug treatment
Many patients who were eligible refused participation in the study
• unwilling to start treatment with imipramine (30.6% and 47.4%), or
discontinue their current medication (22.6% and 35.1%).
“Results from comparative treatment outcome studies are limited
not only to people who meet the study criteria but also to those who
are willing to begin a medication treatment and discontinue their
current medication.” (Hofmann et al., 1998, p. 43)
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 55
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
What are limitations and problems of this study?
Design is in favor of pharmacotherapy
• Pharmacotherapy = drug (placebo) + clinical management
Imipramine and Placebo condition: Every week 30-minute contact with psychiatrist; recommendations and prescription of exposure
Combined treatment (Imipramine or Placebo + CBT), individual contacts with 2 therapists for about 75 minutes per week (higher dosage of treatment than CBT alone)
• Blinding did probably not work for many patients because Placebo did neither produce positive effects nor side effects
• Blinding did probably not work for doctors
• Assessment is only based on external interviewer ratings of current symptoms and improvement. Patients perspective was not assessed
• No adverse effects of treatment were assessed (side effects)
High drop out rates
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 56
CBT, pharmacotherapy, or their combination? (Barlow et al., 2000)
Conclusion drawn from the Barlow et al. (2000) study (APA practice guidelines, 2009, p. 52)
This study provided evidence for the short- and long-term efficacy of CBT
CBT is largely equivalent in short-term efficacy to imipramine and combination treatments,
CBT may produce more durable effects than imipramine or the combination of CBT and imipramine

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 57
Conclusions about efficacy of CBT treatments for panic disorder (APA practice guidelines, 2009, p. 51)
There are numerous controlled trials demonstrating the efficacy of CBT for panic disorder
Meta-analyses of clinical trials support the conclusion that effects of CBT for panic disorder are robust and durable.

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 58
Take home message
With an RCT Barlow & colleagues (1989) could show that • Relaxation is not a necessary component for treating panic disorder, relaxation is sufficient • Cognitive restructuring and interoceptive exposer is an efficacious treatment for panic
disorder and an alternative to pharmacotherapy
With another RCT Barlow et al. (2000) could show
• that CBT is as efficacious as Imipramine for the treatment of panic disorder directly after treatment
• After treatment has been stopped CBT is more efficacious than imipramine.
CBT is recommended as a first line treatment for panic disorder in national guidelines:
• American Psychiatric Association (APA) (2009). https://www.psychiatry.org/psychiatrists/practice/clinical-practice-guidelines
• National Institute for Health and Care Excellence (NICE) (2011, 2015). https://www.nice.org.uk/guidance/cg113
• Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF) http://www.awmf.org/leitlinien/detail/ll/051-028.html
• Compare guidelines with critical Cochrane review (Imai, Tajika, Chen, Pompoli, & Furukawa, 2016).

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 59
Take home message: Methodological issues
Drop outs are a common problem in therapy outcome studies
“Intent to treat analysis” (ITT) (e.g. last value carried forward) is a method to deal with drop outs
• ITT might change the pattern of results suggested by completer analyses
• When drop out rates are different for different conditions, ITT may lead to biased results
Long term follow up assessments are essential to demonstrate the sustainability of treatment effects
There might be problems with the generalization of results
• Treatments are not applied as in clinical practice
• Patients are highly selected
UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 60
References
American Psychiatric Association (2009). Practice guideline for the treatment of patients With panic disorder (2nd ed.). American Psychiatric Association. Retrieved 20.3.2018 from https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/panicdisorder.pdf
American Psychiatric Association [APA] (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Association.
Bandelow, B., Wiltink, J., Alpers, G. W., Benecke, C., Deckert, J., Eckhardt-Henn, A., ... Beutel, M. E. (2014). Deutsche S3-Leitlinie Behandlung von Angststörungen. Retrieved 20.3.2018 from http://www.awmf.org/uploads/tx_szleitlinien/051-028l_S3_Angstst%C3%B6rungen_2014-05_2.pdf
Barlow, D. H., Craske, M. G., Cerny, J. A. & Klosko, J. S. (1989). Behavioral treatment of panic disorder. Behavior Therapy, 20, 261-282.
Barlow, D. H., Gorman, J. M., Shear, M. K., & Woods, S. W. (2000). Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: A randomized controlled trial. Journal of the American Medical Association, 283, 2529–2536.
Craske, M. G., Brown, T. A. & Barlow, D. H. (1991). Behavioral treatment of panic disorder: A two-year follow-up. Behavior Therapy, 22, 289-304.
Hofmann, S. G., Barlow, D. H., Papp, L. A., Detweiler, M. F., Ray, S. E., Shear, M. K., ... Gorman, J. K. (1998). Pretreatment attrition in a comparative treatment outcome study on panic disorder. American Journal of Psychiatry, 155 (1), 43-47.
Imai, H., Tajika, A., Chen, P., Pompoli, A., & Furukawa T. A. (2016). Psychological therapies versus pharmacological interventions for panic disorder with or without agoraphobia in adults. Cochrane Database of Systematic Reviews, 10, Art. No.: CD011170. DOI: 10.1002/14651858.CD011170.pub2.
National Institute for Health and Care Excellence [NICE] (2011). Generalised anxiety disorder and panic disorder in adults: management. Clinical guideline. Retrieved 20.3.2018 from https://www.nice.org.uk/guidance/cg113/resources/generalised-anxiety-disorder-and-panic-disorder-in-adults-management-pdf-35109387756997
National Institute for Health and Care Excellence [NICE] (2015). Generalised anxiety disorder and panic disorder (with or without agoraphobia) in adults: Management in primary, secondary and community care. Recommendation for Guidance Executive. Retrieved 20.3.2018 from https://www.nice.org.uk/guidance/cg113/evidence/surveillance-review-decision-july-2015-pdf-2482902685

UNIVERSITY FRIBOURG, CH| Department of Psychology | Chair of Clinical Psychology and Psychotherapy| PD Dr. Peter Wilhelm, Spring 2018 61
Links to Practice Guidelines
United States • American Psychiatric Association (APA)
https://www.psychiatry.org/psychiatrists/practice/clinical-practice-guidelines
United Kingdom • National Institute for Health and Care Excellence (NICE)
https://www.nice.org.uk/
Germany • Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V.
(AWMF) http://www.awmf.org/leitlinien/leitlinien-suche.html
Cochrane Society • “Global independent network of researchers, professionals, patients, carers, and
people interested in health” • “Cochrane contributors - 37,000 from more than 130 countries - work together to
produce credible, accessible health information that is free from ccommercial sponsorship and other conflicts of interest.” Retrieved 21.3.2018 from http://www.cochrane.org/about-us
• http://www.cochrane.org/