approach to lymphadenopathy prof:akmal jamal fcps;frcsed: 2013
TRANSCRIPT

Approach to Lymphadenopathy
PROF:AKMAL JAMAL
FCPS;FRCSEd:
2013

Case 41 yo male school teacher presents to your office with right sided
cervical lymphadenopathy. His past medical history is significant for hypertension and dyslipidemia. He noticed the lump in his neck last week. He has not experienced any fevers, chills or weight loss. He denies any sore throat, ear pain or dental problems. His vital signs are stable. On physical exam he has a 2cm anterior cervical lymph node which is firm, non-tender and mobile. His HEENT exam is unremarkable. No skin lesions are evident. No other lymphadenopathy is found. How should you proceed with this patient?
A. Location and duration typical for viral etiology. Have your patient follow up for annual physical next year.
B. Proceed to fine needle aspiration.C. Check a CXR and cbc.D. Have patient follow up in 3-4 weeks.

Learning Objectives
Provide an approach to the patient with peripheral lymphadenopathy
Be able to differentiate between benign and serious illness
Knowledgeable of nodal distribution and anatomic drainage
Present a substantial differential diagnosis Indications for nodal biopsy

Objectives
Approach to Adenopathy Who to investigate When to investigate How to define risk for underlying malignancy

Definition: Lymphadenopathy
Lymph nodes that are abnormal in size consistency or number

Definitions
Pathologic Lymph Node >2cm in children is considered abnormal
Acute Lymphadenopathy < 2 weeks duration
Subacute Lymphadenopathy 2-6 weeks duration
Chronic Lymphadenopathy > 6 weeks duration

Classification: Lymphadenopathy
Generalized- if lymph nodes are enlarged in two or more noncontiguous areas
Localized- if only one area is involved.

Distinguishing between two is important in formulating a differential diagnosis.
3/4 of patients will present with localized lymphadenopathy
1/4 with generalized lymphadenopathy.

Why do lymph nodes enlarge?
Increase in the number of benign lymphocytes and macrophages in response to antigens
Infiltration of inflammatory cells in infection (lymphadenitis)
In situ proliferation of malignant lymphocytes or macrophages
Infiltration by metastatic malignant cells Infiltration of lymph nodes by metabolite
laden macrophages (lipid storage diseases)

The Lymphatic System
Normally palpable lymph nodes in healthy people?

The Lymphatic System Normally palpable lymph nodes in healthy people.
submandibular, axillary inguinal

Lymphatic System

Lymphatic System
Network that filters antigens from the interstitial fluid Primary site of immune response from tissue
antigens Lymphatic drainage in all organs of the body except
brain, eyes, marrow and cartilage Flaccid thin walled channelsprogressive caliber 600 lymph nodes in body Slow flow, low pressure system returns interstitial
fluid to the blood system

Lymph nodes
Capsular shell Fibroblasts and reticulin
fibers Macrophages Dendritic cells T cells B cells


anatomy
16

HISTOLOGYTWO ZONES:
A darkly staining cortexAnd a lightly staining medulla
17

18

function
They are centers of lymphocyte production. Both B-lymphocytes and T-lymphocytes are produced here by multiplication of pre-existing lymphocytes.
Filter the products from lymph such as bacteria and other particulate matter and to prevent their entry into systemic circulation.
The antibodies produced by the B-Lymphocytes are carried to the circulation… and indirectly help in mounting an immune response.
19

Peripheral lymphadenopathy
Most cases benign, self limited illness Primary or secondary manifestation of 100
illnesses The CHALLENGE is to decide if it is
representative of a serious illness…

Parameters to help distinguish between benign and serious
illness
Age
Character
Location

“Malignancy much more common in patients
greater 50 yrs of age”
Not exactly

Algorithm to evaluate Lymphadenopathy
History
Physical exam
Confirmatory testing
Indication for biopsy

History
Localizing symptoms or signs to suggest a specific site
Constitutional symptoms: B symptoms
(fever, night sweats, >10%body wt >6months) Epidemiologic clues: occupation, travel, high
risk behavior Medications

Medications That May Cause Lymphadenopathy
Allopurinol Atenolol (Tenormin) Captopril (Capozide) Carbamazepine Cephalosporins Gold Hydralazine
Penicillin Phenytoin Primidone Pyrimethamine Quinidine Sulfonamides Sulindac

Physical Examination

Lymph node character
Size Site Consistency Pain with palpation

Size
Greater than one centimeter generally considered abnormal
Exception inguinal area, lymph nodes commonly palpated (>1.5 cm)
Size does not indicate a specific disease process
Obese and thin population

Pain…..
Indication of rapid increase in size: stretch of capsular shell
NOT useful in determining benign vs malignant state
Inflammation, suppuration, hemorrhage

Consistency
Stone hard: typical of cancer usually metastatic
Firm rubbery: can suggest lymphoma Soft: infection or inflammation Shotty “buckshot under skin” Suppurated nodes: fluctuant Matted

Location, location, location

Post cervical: scalp, neck skin of arms thorax cervical and axillary nodes (lymphoma, head/neck ca)

Facial Papule with Adenopathy




Suppurative Lymphadenitis with Overlying cellulitis

Mycobacterial Lymphadenitis

Mycobacterial Lymphadenitis


Famous nodes
Virchows
Left supraclavicular (abdominal or thoracic ca) Sister Joseph
Para-umbilical (gastric adenoca) Delphian node
Prelaryngeal (thyroid or laryngeal ca) Node of Cloquet (Rosenmuller node)
Deep inguinal near femoral canal

Creating a Differential
CHICAGO

43

Chicago
Cancer Heme malignancies: Hodgkins, NHL, acute
and chronic leukemias, waldenstroms, multiple myeloma (plastmocytomas)
Metastatic: solid tumor breast, lung, renal, cell ovarian

cHicago
Hypersensitivity syndromes
Serum sickness Serum sickness like
illness
Drugs Silicone Vaccination Graft vs Host

Specific Medications
Cephalosporins Atenolol Captopril
Dilantin Sulfonamides Carbamazepine Primodine Gold Allupurinol

Chicago
Infections
Viral Bacterial Protozoan Mycotic Rickettsial (typhus) Helminthic (filariasis)

VIRAL
EBV…mono spot test CMV….cmv titers, immunsuppresed,
transplant recipient, recent blood transfusion HIV…IV drug use, high risk sexual behavior Hepatitis….IV drug use Herpes Zoster….superficial cutaneous
nodules

Bacterial
Staph/strep: cutaneous source, lymphadenitis Cat scratch: bartonella hensalae, two weeks
after inoculation Mycobacterium: TB and non-tb, host
characteristics (HIV, foreign born, low socioeconomic status, homeless)


Spirochete
Syphilis: Treponema pallidum Primary localized inguinal lymph nodes and secondary, non-treponemal, treponemal
Lyme disease

Protozoan
Toxoplasmosis: ELISA assay, intracellular protozoan toxoplasmosis gondii….bilateral, symmetrical, non-tender cervical adenopathy
…consider undercooked meat, reactivation in immuncompromised host

chicago
Connective Tissue Disease
Rheumatoid Arthritis SLE Dermatomyositis Mixed connective tissue disease Sjogren

chicago
Atypical lymphoproliferative disorders
Castleman’s disease Wegeners Angioimmuonplastic lymphadenopathy with
dysproteinemia

chicaGo
Granulomatous
Histoplasmosis Mycobacterial infections Cryptococcus Silicosis: coal, foundry, ceramics, glass Berylliosis: metal, alloys Cat Scratch

OTHER…….chicago
RARE Kikuchi Rosia Dorfman Kawasaki Transformation of germinal centers

Non-Infectious Lymphadenopathy

Kawasaki Disease Lymphomucocutaneous Disease Five Characteristics of Disease (4/5 for
diagnosis) Fever >5 days Cervical lymphadenopathy (usually unilateral) Erythema and edema of palms and soles with
desquamation of skin Nonpurulent Bilateral Conjunctivitis Strawberry Tongue
Treatment IVIG and Aspirin

Systemic Manifestations of Kawasaki Disease

Kikuchi-Fujimoto disease Also known as necrotizing lymphadenitis Benign condition Affects young Japanese girls Associated Signs and Symptoms
Fever Nausea Weight loss Night Sweats Arthralgias Hepatosplenomegaly
Thought to have viral or autoimmune etiology The majority spontaneously regress within 6 months,
however some patients have recurrences

Rosai-Dorfman Massive, painless, bilateral cervical adenopathy Benign condition Generalized proliferation of sinusoidal histiocytes First decade of life with 2M:1F Associated signs and symptoms
Fever Neutrophilic leukocytosis Polyclonal hypergammaglobulinemia
Most patients will get a biopsy given the large adenopathy Characteristic biopsy showing sinus expansion with
histiocytes and phagocytosed lymphocytes (Foucar 1990) Treatment is supportive and most patients have
spontaneous regression
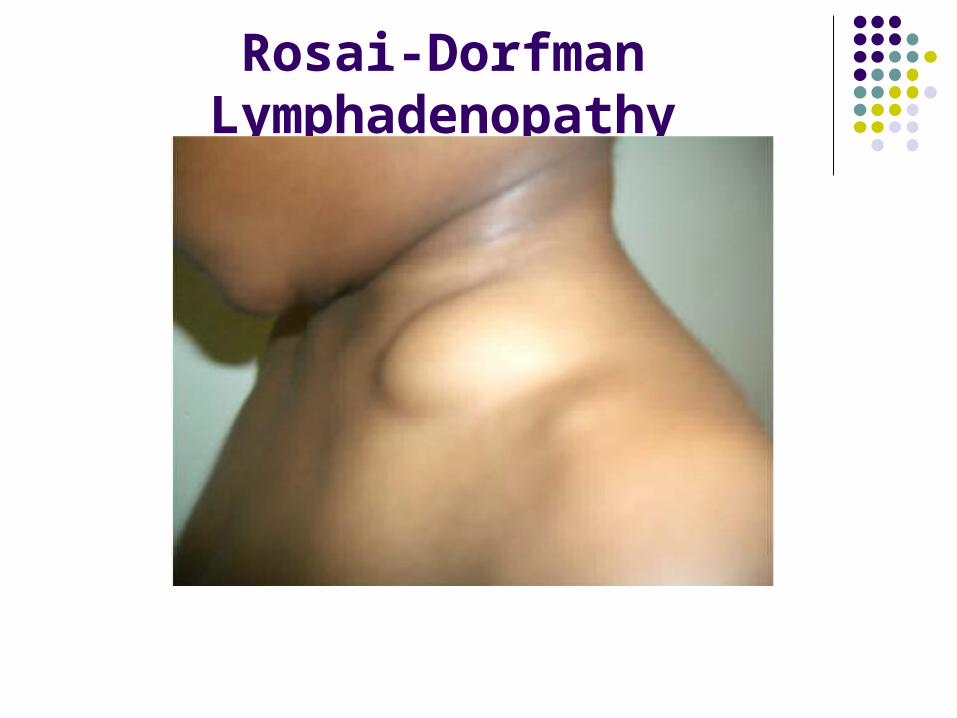
Rosai-Dorfman Lymphadenopathy

Langerhans Cell Histiocytosis Eosinophilic Granuloma
Solitary bone, skin, lung, or stomach lesions Hands-Schuller-Christian Disease
Diabetes Insipidus, Exophthalmos, Lytic bone lesions Letterer-Siwe disease
Life threatening multisystem disorder 50% 5 year survival
1/3 of patients will have background LAD Histopathology shows normal lymph node
architecture but increase sinusoidal Langerhans’ cells, macrophages, and eosinophils
Treatment with topical steroids, oral steroids, and even chemoradiation therapy

64
Unexplained lymphadenopathy without signs or symptoms of serious disease or malignancy can be observed for one month, after which
specific imaging or biopsy should be performed
fine-needle aspiration, excisional biopsy remains the initial diagnostic procedure of choice.
Modern cross-sectional imaging modalities such as ultrasound(US), computed tomography (CT) and magnetic resonance (MR)
imaging allow reliable detection of cervical lymph nodes. However,the differentiation between benign and malignant lymph
nodes remains challenging
Alternative imaging modalities such as single photonemission computed tomography (SPECT) and positron emissiontomography (PET) can help to differentiate between benign and
malignant lymph nodes

Limited Unexplained
Age Location History
Wait 3-4 weeks and reexamine No indication for empiric antibiotics or steroids Glucorticoids can be harmful and delay diagnosis
can obscure diagnosis due to lympholytic affect

Unexplained Generalized lymphadenopathy
Always requires an evaluation Start with CXR and CBC Review Medications PPD, RPR, Hepatitis screen, ANA, HIV No yield on above test: Biopsy most
abnormal node

Role of Ultrasound No radiation exposure Good for following the progress of an abscess Differentiate Reactive vs Malignant nodes
Reactive <1 cm Oval (S/L ratio <0.5cm) Normal hilar vascularity Low resistive index with high blood flow
Malignant >1 cm Round (S/L ratio >0.5cm) No echogenic hilus Cogaulative necrosis present High resistive index with low blood flow Extracapsular spread
Sensitivity 95% and Specificity 83% for differentiating reactive vs metastatic lymph nodes

The Role of FNA
Minimally invasive Low morbidity Not as reliable in children as in adults so you
can only trust FNA if it is positive (Twist 2000) Chau et al. 2003
Evaluated FNA of 289/550 patients referred with LAD
Sensitivity 49% and Specificity of 97% False negative rate of 45% 83% of false negatives were lymphomas

The Role of Excisional Biopsy
Still the gold standard for diagnosis Consider if FNA is inconclusive or if FNA is
negative but your suspicion for malignancy is high
You must excise the largest and firmest node that is palpable and must remove the node with the capsule intact (Twist 2000)

BIOPSY
Can be done by bedside, open surgery, mediastinocopy or by needle aspiration*
FNA not recommended cannot distinguish between lymphomas (nodal architecture needs to be intact)
FNA reserved for established diagnosis and to demonstrate recurrence

Diagnostic Yield
Ideally axillary and inguinal nodes are avoided as often demonstrate reactive hyperplasia
Preferred supraclavicular, cervical, axillary, epitrochlear, inguinal
Complications include vascular and nerve injury

Unexplained Lymphadenopathy
Localized Lymphadenopathy
When to biopsy ?

Unexplained Lymphadenopathy
Localized Lymphadenopathy
Patients with benign clinical history, an unremarkable physical examination no constitutional symptoms should be reexamined in three to four weeks
to see if the lymph nodes have regressed or disappeared.

Unexplained Lymphadenopathy
Localized Lymphadenopathy
Patients with unexplained localized lymphadenopathy who have
constitutional symptoms or signs, risk factors for malignancy or lymphadenopathy that persists for three to
four weeks should undergo a biopsy.

Fine Needle Aspirate
Convenient, less invasive, quicker turn-around time
Most patients with a benign diagnosis on FNA biopsy do not undergo a surgical biopsy

Case 41 yo male school teacher presents to your office with right sided
cervical lymphadenopathy. His past medical history is significant for hypertension and dyslipidemia. His medications include hctz and simvastatin. He has no known drug allergies. He believes he noticed the lump in his neck last week. He has not experienced any fevers, chills or weight loss. He denies a sore throat, ear pain or dental problems. His vital signs are stable. On physical exam he has a 2cm anterior cervical lymph node which is firm, non-tender and mobile. His HEENT exam is unremarkable. No skin lesions are evident. No other lymphadenopathy is found. How should you proceed with this patient?
A. Location and duration typical for viral etiology. Have your patient follow up for annual physical next year.
B. Proceed to fine needle aspiration C. Check a CXR and cbcD. Have patient follow up in 3-4 weeks.