approach to dysphagia
TRANSCRIPT

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Approach To DysphagiaApproach To Dysphagia
Fuad Ridha MahabotFuad Ridha Mahabot
1

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . IntroductionIntroduction
• is a general term used to describe the inability to move food from the
mouth to the stomach
• should be differentiated from disorders that prevent transfer of food to
the mouth or beyond the stomach but that are not characterized by
difficulty swallowing - e.g. feeding disorder/gastric outlet obstruction
• an average of 10 million Americans are evaluated for swallowing
disorders annually
2

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DefinitionDefinition
• dysphagia - difficulty in swallowing
• odynophagia - swallowing causes pain
• usually patient comes with the complaint of
throat discomfort
FB sensation
feel of hold up
absolute difficulty in swallowing
3
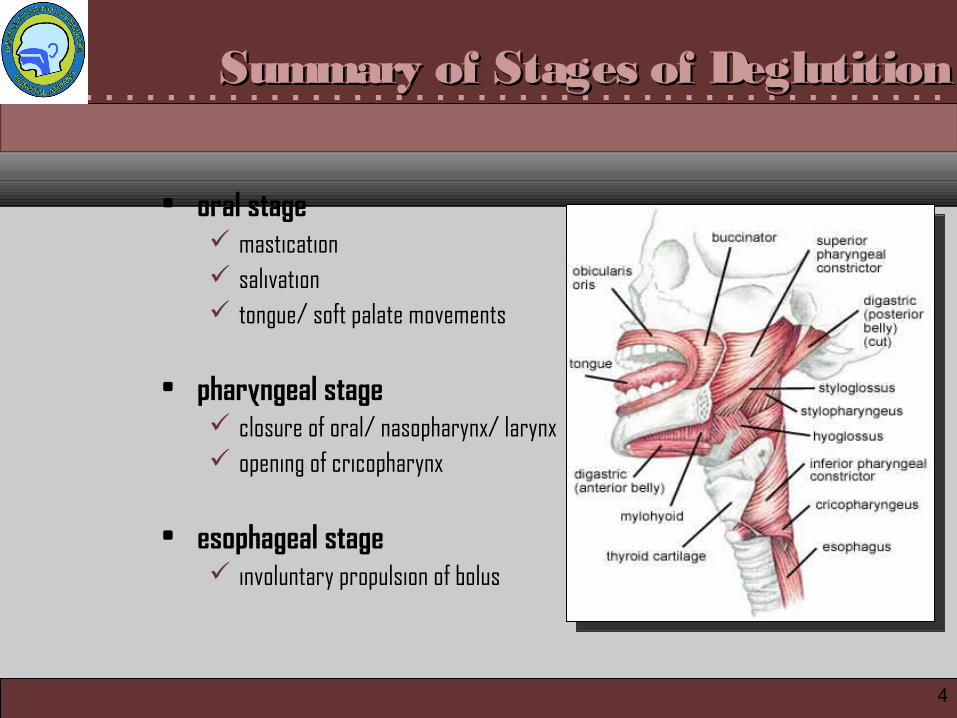
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Summary of Stages of DeglutitionSummary of Stages of Deglutition
• oral stage mastication salivation tongue/ soft palate movements
• pharyngeal stage closure of oral/ nasopharynx/ larynx opening of cricopharynx
• esophageal stage involuntary propulsion of bolus
4

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5stage Istage I stage IIstage II

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6
stage IIIstage III

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . AetiologyAetiology
• can de divided into:
pre-oesophageal (i.e. due to disturbance in the oral or pharyngeal phase of
deglutition)
oesophageal (when disturbance is in oesophageal phase)
7

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pre-oesophageal causes
• oral phase - normally, food must be masticated, lubricated with saliva,
converted into bolus by movement of tongue and then pushed into
pharynx by elevationof tongue against hard palate
• any disturbance in these events will cause dysphagia
• abnormalities are due to:
cannot hold food in the mouth anteriorly due to reduced lip closure
cannot form / hold a bolus or residue on the floor of the mouth due to reduced
range of tongue motion or coordination
8
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
unable to align teeth due to reduced mandibular movement
entry of food material into the anterior sulcus or the presence of residue in the
anterior sulcus due to reduced labial tension or tone
entry of food material into the lateral sulcus or the presence of residue in the
lateral sulcus due to reduced buccal tension or tone
abnormal hold position or material falls to the floor of the mouth due to tongue
thrust or reduced tongue control
delayed oral onset of swallow due to apraxia of swallow or reduced oral
sensation
searching motion or inability to organize tongue movements due to apraxia of
swallow
9

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
forward tongue movement to start the swallow due to tongue thrust
residue of food on the tongue due to reduced tongue range of movement or
strength
disturbed lingual contraction (peristalsis) due to lingual discoordination
incomplete tongue-to-palate contact due to reduced tongue elevation
unable to mash material due to reduced tongue elevation
adherence of food to hard palate due to reduced tongue elevation or reduced
lingual strength
10

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aetiology of Oral Phase
congenital cleft palate, lingual thyroid
inflammatory stomatitis, glossitis, ulcer, sialadenitis, TMJ arthritis, ludwig’s angina, trismus, dental
trauma # maxilla/ mandible, cheek/ tongue bite, corrosive poisoning
neurological palsy: palatal/ lingual/ facial;spasm: trismus/ tetanus
neoplastic papilloma, salivary tumors, ranula, carcinoma, jaw tumors, etc.
miscellaneous xerostomia-nutritional/ radiotherapy
11

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12
tongue ulcertongue ulcer
Ludwing’s AnginaLudwing’s Angina

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
• pharyngeal phase - normally, food should enter the pharynx and then
be directed towards oesophageal opening
• all unwanted communications into the nasopharynx, larynx, oral cavity
should be closed
• abnormalities are due to
delayed pharyngeal swallow
nasal penetration during swallow due to reduced velopharyngeal closure
pseudoepiglottis (after total laryngectomy) - fold of mucosa at the base of the
tongue
14

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
cervical osteophytes
coating of pharyngeal walls after the swallow due to bilateral reduction
of pharyngeal contraction
vallecular residue due to reduced posterior movement of the tongue base
coating in a depression on the pharyngeal wall due to scar tissue or pharyngeal
pouch
residue at top of airway due to reduced laryngeal elevation
aspiration during swallow due to reduced laryngeal closure
stasis of residue in pyriform sinuses due to reduced anterior laryngeal
pressure
delayed pharyngeal transit time15

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Aetiology of Pharyngeal Phase
congenital pharyngeal diverticulum (Zenker’s diverticulum)
inflammatory pharyngitis, tonsillitis, quinsy, retro/ parapharyngeal abscess, TB laryngitis, acute epiglotitis, etc.
trauma FB, corrosive poisoning, iatrogenic trauma, road traffic accidents
neurological cricopharyngeal spasm, VC palsy (aspiration), tetanus, etc.
neoplastic benign: salivary tumors, papilloma, etc., malignant: ca. tonsil/ base tongue/ hypopharynx/ larynx, salivary tumors, etc.
miscellaneous Plummer-Wilson syndrome, globus hystericus
16

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Exudative TonsillitisExudative Tonsillitis Hypopharynx MalignancyHypopharynx Malignancy

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
• other causes of oropharyngeal dysphagia - neuromyogenic
stroke
head trauma
Parkinson's disease and parkinsonism
amyotrophic lateral sclerosis
multiple sclerosis
myasthenia gravis
myopathies (inflammatory, metabolic)
19

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Oesopharyngeal causes - lesion may lie in the lumen, on the wall or
outside the wall of oesophagus
i. structural disorders
inflammatory and/or fibrotic strictures
• peptic
• caustic
• pill-induced
• radiation-induced
20

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
mucosal rings and webs
• Schatzki's ring
• multiringed esophagus (eosinophilic esophagitis)
ii. carcinoma
primary (squamous, adenocarcinoma)
secondary (e.g. breast, melanoma)
21

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iii. disorders related to systemic diseases
pemphigus and pemphigoid conditions
Lichen planus
scleroderma (multifactorial)
intramural lesions
leiomyoma
granular cell tumor
22

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iv. extramural lesions
aberrant right subclavian artery (dysphagia lusoria)
mediastinal masses
bronchial carcinoma
v. anatomical abnormalities
hiatal hernia
esophageal diverticulum
23

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
vi. motility disorders
achalasia and achalasia-like disorders
idiopathic (classic) achalasia
atypical disorders of lower esophageal sphincter relaxation
Chaga’s disease
pseudoachalasia
24

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Ca OesophagusCa Oesophagus Gastro Oesophageal Reflux DiseaseGastro Oesophageal Reflux Disease

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
foreign bodyforeign bodyAchalasia CardiaAchalasia Cardia

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . History Takings and EvaluationHistory Takings and Evaluation
• taking a careful history is vital for the evaluation of dysphagia.
• the history will yield the likely underlying
pathophysiologic process
anatomic site of the problem in most patients - 80%
crucial for determining whether subsequently detected radiographic or
endoscopic 'anomalies' are relevant or incidental
27

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Three fundamental aims should be met when taking a dysphagia
history
i. to establish whether or not dysphagia is actually present; that is, to distinguish
true dysphagia from
• globus sensation (in between meals)
• xerostomia - loose the lubrication properties and stimulus
• odynophagia - transient than dysphagia, and persists only during the 15–
30 secs that a bolus takes to traverse the esophagus
28

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ii. to determine whether the site of the problem is esophageal or pharyngeal
iii. to distinguish a structural abnormality from a motor disorder.
These avenues of enquiry are outlined below in an order that corresponds to that of a
highly effective diagnostic algorithm.
• history will also dictate whether the next diagnostic procedure should
be endoscopy, a barium swallow or esophageal manometry
• in some difficult cases, all three diagnostic techniques may need to be
performed to establish an accurate diagnosis
29

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Where is the site of bolus hold-up?
• retrosternal bolus hold-up indicates that the disorder lies within the
esophagus.
• however, the patient's perception of an apparent bolus hold-up in the
neck has low diagnostic specificity, and cervical localization per se
does not help the clinician to distinguish pharyngeal from esophageal
causes of dysphagia.
30

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
• owing to viscerosomatic referral, in 30% of cases the perceived site of
hold-up is above the suprasternal notch when the actual hold-up is
within the esophageal
31

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Does the patient report symptoms that are predictive of oropharyn-
geal dysfunction
• there are four symptoms that have high specificity for oropharyngeal
dysfunction:
delayed or absent oropharyngeal swallow initiation
deglutitive postnasal regurgitation or egress of fluid through the nose during
swallowing
deglutitive cough indicative of aspiration
the need to swallow repetitively to achieve satisfactory clearance of swallowed
material from the hypopharynx32

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
• if one or more of these four symptoms are present then the cause of
dysphagia is probably oropharyngeal, either structural or
neuromyogenic
33

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Oropharyngeal vs. Oesophageal DysphagiaOropharyngeal vs. Oesophageal Dysphagia
34

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Oesophageal differentiation - mechanical vs. motility disorder
i. is the dysphagia for the solids or liquids?
patients who have a motor disorder will describe dysphagia for liquids and
solids
whereas patients who have structural disorders will describe dysphagia for
solids only
once a solid bolus becomes impacted, the patient will report dysphagia for
liquids and solids
35

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ii. motility - features
three cardinal features of dysmotility
• dysphagia (for solids and liquids)
• chest pain
• regurgitation
regurgitation during meals, as well as spontaneous regurgitation between meals
or at night, is highly suggestive of dysmotility
unlike regurgitation that is related to GERD, the regurgitated fluid in patients
with esophageal dysmotility is generally not noxious to taste
36
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
in addition, spasm or achalasia typically cause chest pain. Although this chest
pain is frequently described as 'heavy' or 'crushing', it can be indistinguishable
from the typical 'heartburn' of reflux.
the pain frequently occurs during meals, but it can be quite unpredictable and
sporadic or nocturnal.
sipping antacids or even water can relieve the pain related to dysmotility, which
further confuses its distinction from reflux-related pain.
37

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How long has dysphagia been present? Is it intermittent? Is it
progressive?
• slowly progressive, long-standing dysphagia, particularly against a
background of reflux, is suggestive of a peptic stricture.
• severity of heartburn correlates poorly with esophageal mucosal
damage. For example, patients who have severe mucosal changes,
including strictures and Barrett's mucosa, could have had minimal or
no heartburn in the immediate past.
38

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
• a short history of dysphagia — particularly with rapid progression
(weeks or months) and associated weight loss — is highly suggestive of
esophageal cancer
• long-standing, intermittent, nonprogressive dysphagia purely for solids
is indicative of a fixed structural lesion such as distal esophageal ring
or proximal esophageal mucosal web
39

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Physical ExaminationPhysical Examination
Physical examination for dysphagia:
patient's level of alertness and cognitive status, including vital signs
examination of cranial nerves V and VII-XII
complete examination of neck and chest including assessment of cervical lymph
nodes (if present)
assessement of voice
direct observation of lip closure, jaw closure, chewing and mastication, tongue
mobility and strength, palatal and laryngeal elevation, salivation, and oral
sensitivity
inspection the oral cavity and pharynx
41

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
examination of soft palate for position and symmetry during phonation and at
rest
evaluation of pharyngeal elevation by placing 2 fingers on the larynx and
assessing movement during a volitional swallow
examination of gag reflex by stroking the pharyngeal mucosa with a tongue
depressor
direct observation of the act of swallowing. At a minimum, watch the patient
while he/she drinks a few ounces of water. If possible, assess the patient's
eating of various food textures. After the swallow, observe the patient for 1
minute or more to see if a delayed cough response is present
42

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
skin should be examined for features of connective tissue disorders,
particularly scleroderma and CREST (calcinosis, Raynaud's phenomenon,
esophageal dysmotility, sclerodactyly and telangiectasia) syndrome.
muscle weakness or wasting might be evident if myositis is present, and
myositis can overlap with other connective tissue disorders that affect the
esophagus
signs of malnutrition, weight loss and pulmonary complications from aspiration
should be looked for
43

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . InvestigationsInvestigations
Blood Investigations – to screen for
infectious or inflammatory conditions
nutritional status
fluid-electrolyte imbalance
thyroid function - in detecting dysphagia associated with hypothyroidism or
hyperthyroidism
Radiography
i. chest x-ray - mediastinum, cardiac and pulmonary status, aspiration
pneumonia, also to rule out secondaries
44

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ii. lateral x-ray soft tissue neck - to detect any soft tissue lesions of post
cricoid or retropharyngeal space, prevertebral widening, osteophytes, foreign
bodies, etc.
iii. barium swallow
iv. CT scan - to evaluate mass lesions in the neck
v. MRI • useful when neurologic disorders are suspected• delineate mass lesions in the brain• evaluate degenerative processes in the brain and spinal cord
45

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Barium Swallow Barium Swallow in Achalasia in Achalasia CardiaCardia

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Endoscopies
i. direct laryngoscopy
ii. flexible nasopharyngoscopy
iii. bronchosocpy
iv. oesophagoscopy
give direct examination of pharyngeal as well as oesophageal mucosa
permits biopsy
47

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Special Tests
i. Videofluoroscopic Swallowing Study (VFSS)
• a.k.a Modified Barium Swallow (MBS)
• definitive study for evaluation of the swallowing mechanism
• uses different barium consistencies and simulated foods
• assess pharyngeal anatomy and motility and may evaluates all phases of
swallowing• superior to FEES for evaluating the oral phase and aspiration
48

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ii. Fiberoptic endoscopic evaluation of swallowing (FEES)
• using transnasal laryngoscope
• food colored with blue liquid dye viewed directly via scope
• advantages - for detection premature bolus loss, laryngeal penetration,
tracheal aspiration, and pharyngeal residue
• disadvantages - not demonstrate the motion of essential food pathway
structures
• FEES may be helpful when VFSS is not feasible (e.g. in critically ill patient,
patients in ICU who cannot be transferred to the fluoroscopy room)
49

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iii. Oesophageal Manometry
• to assess motor function of the esophagus
• a catheter with several electronic pressure probes is passed into the
stomach to measure esophageal contractions and to define upper and
lower esophageal responses to swallowing
• advantages:
– senses the activity of the muscles
– identifies subtle failures of pressure generation or hyperfunctioning of the
sphincters
– helps accurately diagnose the site of dysfunction
50

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iv. Oesophageal pH Monitoring
• standard criteria for diagnosing reflux disease
• a nasogastric probe is inserted into the patient's esophagus to record pH
levels
• these levels are compared with the patient's record of symptoms over 24
hours to determine whether acid reflux contributes to his/her symptoms
v. Swallowing and Laryngeal Electromyography
vi. Scintigraphy
51

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Swallow Carefully!!!Swallow Carefully!!!Thank YouThank You
52