appendiceal intussusception induced by cecal ... · presentation is often non specific that...
TRANSCRIPT

21J Radiol Sci March 2014 Vol.39 No.1
Appendiceal intussusception is an unusual appendiceal pathologic entity with a slightly higher prevalence in adult female [1, 2]. It can be caused by anatomical and patholog-ical factors such as appendiceal or cecal neoplasm. Clinical presentation is often non specific that constitutes a pre-surgical diagnostic challenge for radiologists and surgeons. Among the five types of appendiceal intussusception which defined by McSwain [3], the complete type has the most specific image pattern. The “coiled-spring” sign in double-contrast barium enema [4]; a “finger-like” filling defect and absent appendix without previous appendectomy in both double-contrast barium enema and computed tomography (CT) have been documented [5]. Here we report a new CT character in a case of McSwain type V appendiceal intus-susception induced by cecal adenocarcinoma.
CASE REPORT
A 58-year-old male, who was previous healthy, visited his physician about defecating tarry stool for 10 days with
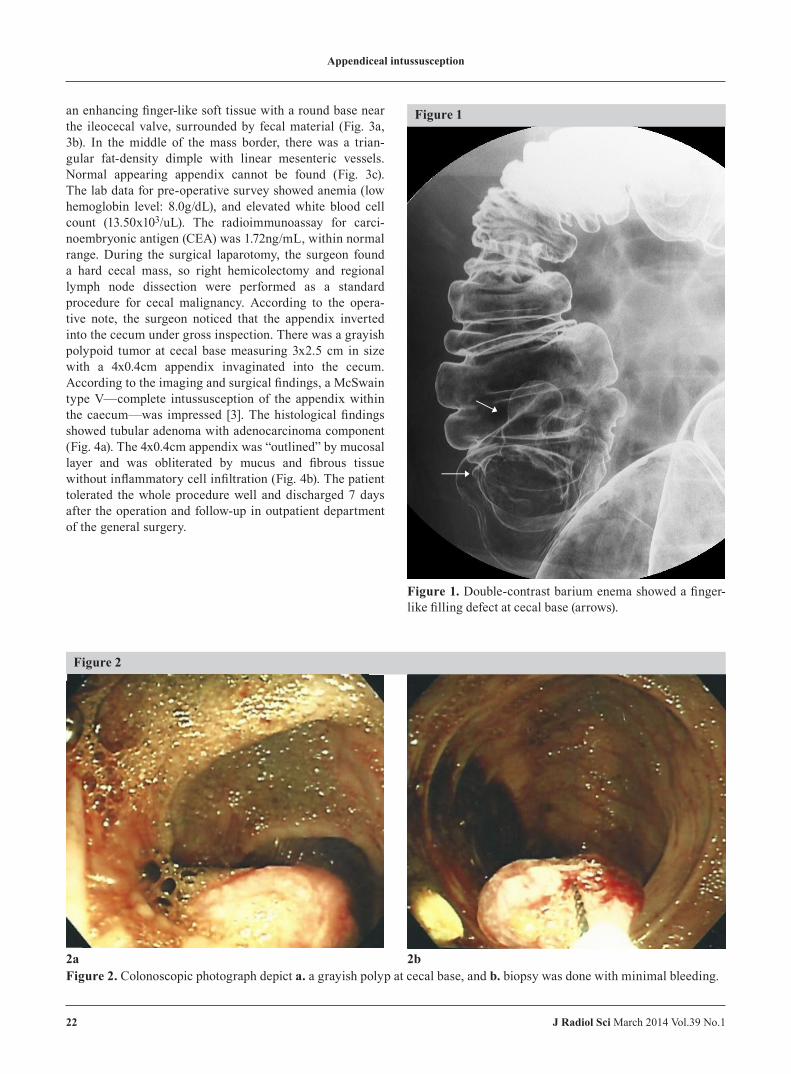
dizziness, general weakness. He denied abdominal pain, weight loss recently. No palpable mass, and no muscle guarding or rebounding tenderness was noted under physical examination. Under digital rectal examination, a grade II hemorrhoid was found, but the double contrast colon series were ordered to survey other possibility that causing gastrointestinal bleeding. There was an about 3 cm pedunculated, polyp-like lesion from cecal base and adjacent to the ileocecal region (Fig. 1). Then colonoscopy also found a polyp at cecum but difficult to remove by transrectal polypectomy, so the polyp was biopsied first (Fig. 2). The histological report of the 3 pieces of speci-mens revealed fibrino-inflammatory exudate composed of neutrophils, fibrin & exfoliated epithelial cells. Because of the possibility of malignancy by considering the size and morphology, so the patient was then admitted for further pre-operative evaluation.
The post contrast whole abdominal computed tomog-raphy (CT) study (Siemens SOMATOM Sensation 16, 100mL angiografin IV push) with 2mm-thickness section and sagittal reconstruction from the axial section revealed
Appendiceal Intussusception Induced by cecal adenocarcinoma in Tubular Adenoma: a case report
Shih-hSuan Liang1 She-Meng Cheng1 Fei-Shih Yang1,2
Department of Radiology1, Mackay Memorial Hospital, Taipei, Taiwan Department of Radiological Technology2, Yuanpei University, Hsinchu, Taiwan
AbSTRACT
Intussusception of the appendix is rare in worldwide studies and is difficult to recognize before operation. We report a case of a 58-year-old, previous healthy male with defecating tarry stool for 10 days with dizziness, general weakness. Double contrast colon series and abdominal computed tomography (CT) revealed a 2.5 cm pedunculated, polyp-like lesion adjacent to the ileocecal region, and the appendix was not found. The pathological findings of biopsy tissues of colonoscopy only showed inflammatory change. Appendiceal intussusception was finally recognized during the operation. The pathological report of the specimen from right hemicolectomy revealed a cecal adenocarci-noma in tubular adenoma. Appendiceal intussusception is an interesting variation of the appendiceal diseases that the colonoscopist, radiologist, and general surgeon must know and better to identify before operation to avoid possible perforation during biopsy.
Correspondence Author to: She-Meng ChengDepartment of Radiology, Mackay Memorial Hospital, Taipei, TaiwanNo. 92, Sec. 2, Zhong-Shan N. Road, Taipei 104, Taiwan
J Radiol Sci 2014; 39: 21-24
Appendiceal intussusception
22 J Radiol Sci March 2014 Vol.39 No.1
an enhancing finger-like soft tissue with a round base near the ileocecal valve, surrounded by fecal material (Fig. 3a, 3b). In the middle of the mass border, there was a trian-gular fat-density dimple with linear mesenteric vessels. Normal appearing appendix cannot be found (Fig. 3c). The lab data for pre-operative survey showed anemia (low hemoglobin level: 8.0g/dL), and elevated white blood cell count (13.50x103/uL). The radioimmunoassay for carci-noembryonic antigen (CEA) was 1.72ng/mL, within normal range. During the surgical laparotomy, the surgeon found a hard cecal mass, so right hemicolectomy and regional lymph node dissection were performed as a standard procedure for cecal malignancy. According to the opera-tive note, the surgeon noticed that the appendix inverted into the cecum under gross inspection. There was a grayish polypoid tumor at cecal base measuring 3x2.5 cm in size with a 4x0.4cm appendix invaginated into the cecum. According to the imaging and surgical findings, a McSwain type V—complete intussusception of the appendix within the caecum—was impressed [3]. The histological findings showed tubular adenoma with adenocarcinoma component (Fig. 4a). The 4x0.4cm appendix was “outlined” by mucosal layer and was obliterated by mucus and fibrous tissue without inflammatory cell infiltration (Fig. 4b). The patient tolerated the whole procedure well and discharged 7 days after the operation and follow-up in outpatient department of the general surgery.
Figure 1
Figure 1. Double-contrast barium enema showed a finger-like filling defect at cecal base (arrows).
Figure 2
2a 2bFigure 2. Colonoscopic photograph depict a. a grayish polyp at cecal base, and b. biopsy was done with minimal bleeding.

Appendiceal intussusception
23J Radiol Sci March 2014 Vol.39 No.1
DISCUSSION
Due to low prevalence and non-specific clinical presen-tation, pre-surgical diagnosis of appendiceal intussusception
remains difficult. In addition, bleeding and perforation risk may rise when colonoscopic “polypectomy” done on an invaginated appendix with patent appendiceal lumen [6]. This emphasized the role of imaging diagnosis.
Figure 3
Figure 3. Contrast enhanced whole abdomen CT. a. axial section, b. sagittal reconstruction showed a well-enhanced tubular soft tissue mass (arrows) outlined by fecal material at cecal base. c. Focal magnified view showed a triangular fat-density dimple (arrowhead) with linear mesenteric vessels (arrow) at mass border. Absent appendix was also noted.
3a
3b 3c

Appendiceal intussusception
24 J Radiol Sci March 2014 Vol.39 No.1
Retrospectively reviewed the image studies of our case, a finger-like filling defect at cecum and absent appendix in both double-contrast barium enema and CT are compat-ible with the previous case reports of the McSwain type V appendiceal intussusception. The inverted appendix was not swollen or inflamed, also consistent with McSwain’s finding that “a markedly inflamed, indurated appendix cannot become intussuscepted” [3]. Therefore, the intussus-cipien is smaller than that of an ileocolic intussusception. Presence of a central mass in the cecum with a 6 mm outer diameter to the concentric configuration is suggestive of appendiceal intussusception under CT scan [7].
Further more, there are silk-like mesenteric vessels connecting to the fatty indentation on mass border, repre-sent mesoappendix folding into the cecum along with the inverted appendix. This finding could only be found in the 2mm thin-sliced axial CT section and was not mentioned before. Advancing CT scanner in recent years helps identi-fying details, not only the 4-millimeter inverted appendix itself but also the 1-millimeter vessels.
In conclusion, if there is a finger-like polyp at cecal base with a fatty dimpling on the margin associating small mesenteric vessels on thin-slice axial section of CT scan, appendiceal intussusception is highly suspected. It is impor-tant for radiologist to warn the surgeon in order to prevent perforation during colonoscopic biopsy. Undergo surgery is appropriate approach to direct en block resection and to prove the occult neoplasm which was easily overlooked in the leading point of intussusception.
REFERENCES
1. Collins DC. 71,000 human appendix specimens. A final report, summarizing forty years’ study. Am J Proctol 1963; 14: 265-281
2. Chaar CI, Wexelman B, Zuckerman K, Longo W. Intus-susception of the appendix: comprehensive review of the literature. Am J Surg 2009; 198: 122-128
3. McSwain B. Intussusception of the appendix. South Med J 1941; 34: 263-271
4. Levine SL, Trenker SW, Herlinger H. Coiled-spring sign of appendiceal intussusception. Radiology 1985; 155: 41-44
5. Swanger R, Davis S, McBride W, Rachlin S, Sonke PY, Brudnicki A. Multimodality imaging of an appendiceal intussusception. Pediatr Radiol 2007; 37: 929-932
6. Eric KJ, Maria EA, Scott RS. Appendiceal Inversion: a Diagnostic and Therapeutic Dilemma. JSLS- J Soc Laparoend 2009; 13: 92-95
7. Koumanidou C, Vakaki M, Theofanopoulou M. Appen-diceal and appendiceal-ileocolic intussusception: sono-graphic and radiographic evaluation. Pediatr Radiol 2001; 31: 180-183
Figure 4
4a 4bFigure 4. a. Microscopic examination demonstrated well-differentiated adenocarcinoma adjacent to the tubular adenoma. b. Section of the appendix showed thin-walled appendix with fibrous obliteration.