antineoplastic therapy use in patients with advanced cancer admitted to an acute palliative care...
TRANSCRIPT
Antineoplastic Therapy Use in Patients WithAdvanced Cancer Admitted to an AcutePalliative Care Unit at A ComprehensiveCancer CenterA Simultaneous Care Model
David Hui, MD, MSc; Ahmed Elsayem, MD; Zhijun Li, MS; Maxine De La Cruz, MD; J. Lynn Palmer, PhD;
and Eduardo Bruera, MD
BACKGROUND: Cancer patients admitted to a palliative care unit generally have a poor prognosis. The role of anti-
neoplastic therapy (ANT) in these patients remains controversial. In the current study, the authors examined the fre-
quency and predictors associated with ANT use in hospitalized patients who required admission to an acute
palliative care unit (APCU). METHODS: Included in the study were all 2604 patients admitted over a 5-year period to
a 12-bed APCU located within a National Cancer Institute comprehensive cancer center, in which patients had access
to both palliative care and ANT. Institutional databases were used to retrospectively retrieve data regarding patient
demographics, cancer diagnosis, ANT use, length of hospital stay, and survival from time of admission. RESULTS: The
median hospital stay was 11 days, and the median survival was 22 days. During hospitalization, 435 patients (17%)
received ANT, including chemotherapy (N ¼ 297; 11%), hormonal agents (N ¼ 54; 2%), and targeted therapy (N ¼ 155;
6%). No significant change in the frequency of ANT use was detected over the 5-year period. Multivariate logistic
regression analysis revealed that younger age, specific cancer diagnoses, and longer admissions were independently
associated with ANT use. CONCLUSIONS: The use of ANT during hospitalization that included an APCU stay was lim-
ited to a small percentage of patients and did not increase over time. ANT use was associated with younger age, spe-
cific cancer diagnoses, and longer admissions. The APCU facilitates simultaneous care for patients receiving ANT.
Cancer 2010;116:2036–43. VC 2010 American Cancer Society.
KEYWORDS: neoplasms, therapeutics, antineoplastic agents, targeted agents, palliative care.
Patients with advanced cancer inevitably experience progressive functional decline and psychological distress. Aspatients transition from advanced to far advanced stages of disease (ie, expected survival of <3 months), palliative careplays an increasingly important role by providing symptom control and psychosocial counseling, and facilitating health-care decision making. Patients who require admission under palliative care generally have a poor prognosis, with a mediansurvival of weeks.1-5 During this critical end-of-life period, patients, family members, and the healthcare team are facedwith a multitude of complex healthcare decisions.
Some of the most challenging of these complex decisions concern the initiation, continuation, and withdrawal ofpalliative antineoplastic therapy (ANT).6 Because of a lack of clear guidance for the use of ANT at the end-of-life and thedifficulty in estimating survival for patients with advanced cancer, the decision to administer or withhold ANT is currentlybeing made on a case-by-case basis, taking into account patients’ wishes along with clinical, logistic, and financialconsiderations.7
DOI: 10.1002/cncr.24942, Received: April 21, 2009; Revised: July 8, 2009; Accepted: July 30, 2009, Published online February 16, 2010 in Wiley InterScience
(www.interscience.wiley.com)
Corresponding author: Eduardo Bruera, MD, Department of Palliative Care and Rehabilitation Medicine, Unit 008, The University of Texas M. D. Anderson Cancer
Center, 1515 Holcombe Boulevard, Houston, TX 77030; Fax: (713) 792-6092; [email protected]
Department of Palliative Care and Rehabilitation Medicine, The University of Texas M. D. Anderson Cancer Center, Houston, Texas
We thank Ms. Olubumi Akiwumi for her assistance with database management, and Ms. Tamara Locke for review of article.
2036 Cancer April 15, 2010
Original Article

The role of ANT for patients admitted to the acutepalliative care unit (APCU) is controversial. Some institu-tions have a policy of discontinuing all ANT on admissionto the APCU, which forces patients to choose betweencancer treatment and optimal palliative care. Others pro-pose a simultaneous care model in which patients receivepalliative care while receiving ANT.8-10 Lagman et aldescribed their experience with cancer patients admittedto an inpatient palliative care unit at the Cleveland Clinic,in which 13% were treated with radiotherapy, chemo-therapy, or both.11 Another retrospective study from aJapanese Cancer Center reported only 3 of 201 patientsadmitted to its palliative care unit receivedchemotherapy.12
To the best of our knowledge, there has been littledocumentation of the extent, trends, and predictors ofANT use in patients who require an APCU stay. A betterunderstanding of the current pattern of ANT use wouldprovide insights into how palliative care can be integratedinto oncology practice under a simultaneous care model.Using a retrospective cohort design, we examined the fre-quency, factors, and duration between admission anddeath associated with ANT use in hospitalized patientswho required an APCU stay.
MATERIALS AND METHODS
Subjects
The Institutional Review Board at The University ofTexas M. D. Anderson Cancer Center (MDACC)approved this study and waived informed consent. Allcancer patients admitted to the APCU at MDACCbetween September 1, 2003 and August 31, 2008 wereincluded in this retrospective cohort study. These dateswere chosen to correspond to the institution’s fiscal year,which begins on September 1 and ends on August 31 ofthe following year. For patients with multiple admissionsto the APCU, only the last available admission wasincluded for analysis because this admission is closest tothe end-of-life, providing insights into the extent of ANTuse in patients with far advanced cancer.
Our 12-bed APCU was opened at the MDACC in2002. Staffed by an interdisciplinary team of physicians,nurses, social workers, physiotherapists, and a chaplain, 1goal of the APCU is to provide symptommanagement forpatients with advanced cancer and severe physical and/orpsychosocial distress, and to provide emotional supportfor their families.13
Patient Characteristics and Duration BetweenAdmission and Death
We retrospectively retrieved patient demographics (age,sex, race, and religion), cancer diagnosis, and durations ofthe entire hospitalization and APCU stays from institu-tional databases. We also collected information regardingANT used between the dates of hospital admission anddischarge from our institutional pharmacy databases. Toensure consistency and accuracy of data, we conductedfurther reviews of patient electronic health records whenany discrepancy was detected. Survival outcome wasobtained from the Tumor Registry Vital Statistics Data-base, with further review of electronic chart records toobtain the date of last follow-up when necessary.
We examined ANTs use during the entire hospitali-zation period, rather than the APCU period alone,because the periods leading to APCU admission and im-mediately after APCU discharge were very much relatedto the APCU stay, with similar patient characteristics anddisease severity. Among patients with multiple cancerdiagnoses, the most responsible cancer diagnosis for hos-pitalization was used for analysis.
ANT Use
Decisions to initiate, continue, or withdraw ANT weremade on a case-by-case basis, with key guidance providedby the patients’ oncologists. Patients admitted to ourAPCU are able to receive ANT; however, our nurses arenot certified to administer cytotoxic or targeted therapiesintravenously. Thus, arrangements are made to facilitatethe administration of parenteral ANT, such as temporarytransfer to the outpatient chemotherapy unit or to an on-cology inpatient unit.
ANTs were categorized into chemotherapeuticagents, hormonal agents, and targeted therapy. In thisstudy, biologic agents such as interferon were classified astargeted therapy.
Megestrol acetate may be used either as anticancertherapy or as therapy for anorexia-cachexia. Thus, forpatients who received this medication, we reviewed theindications to determine whether it had been used asANT. Bisphosphonates and corticosteroids were notconsidered ANT in this study.
Statistical Analysis
We summarized baseline demographics, admission char-acteristics, and ANT utilization using descriptive statis-tics, including medians, means, standard deviations,ranges, and frequencies together with 95% confidence
Antineoplastic Agents in Palliative Care/Hui et al
Cancer April 15, 2010 2037

intervals. The chi-square test was used to determine theyearly trend of ANT utilization.
We compared the baseline and admission character-istics between patients who received ANT and those whodid not. Comparisons were made using the Student t testfor continuous variables that were normally distributed(ie, age); the Kruskal-Wallis test for continuous, nonpara-metric variables (eg, admission length); and the Pearsonchi-square test for categorical variables (eg, race, religion).Variables associated with a P value �.20 on univariateanalysis were then fitted in a logistic regression modelwith backward elimination to identify factors associatedwith ANT during hospitalization. A 2-sided P value<.05was considered to be statistically significant.
Survival analysis was plotted by using the Kaplan-Meier method.14 Overall survival was calculated from thetime of hospital admission to death from any cause ordate last known alive.
The Statistical Package for the Social Sciences (SPSSversion 16.0; SPSS Inc, Chicago, Ill) software was usedfor statistical analysis.
RESULTS
Baseline Characteristics
The characteristics of the 2604 patients who requiredadmission to the APCU during the study period areshown in Table 1. Respiratory, gastrointestinal, and geni-tourinary malignancies constituted greater than half of allcases. A total of 740 (28%) patients were admitted to anddischarged directly from the APCU; the remainder hadboth an oncology unit and APCU stay. The median dura-tion between admission and death for the entire cohortwas 22 days.
Frequency of ANT Use
During their hospitalization that included an APCU stay,435 patients received ANT, including chemotherapy (N¼ 297; 11%), hormonal agents (N ¼ 54; 2%), and tar-geted therapy (N ¼ 155; 6%). Among these patients, 58received both chemotherapeutic agents and targetedagents, 11 received both chemotherapeutic agents andhormonal agents, and 1 received all 3 classes of agents.Thirty-six patients (1%) received ANT as part of anexperimental clinical trial. Overall, 2169 (83%) patientsreceived no ANT during the APCU admission.
The median number of ANT administered duringthe entire hospitalization was 1 (interquartile range [Q1-Q3], 1-2), with a median number of 2 doses (Q1-Q3, 1-
2) per patient. The most commonly used chemotherapeu-tic agents included cytarabine (intravenous/intrathecal; N¼ 58), gemcitabine (N ¼ 52), paclitaxel (N ¼ 44),hydroxyurea (N ¼ 40), carboplatin (N ¼ 30), cisplatin(N ¼ 27), methotrexate (intravenous/intrathecal; N ¼22), doxorubicin (N ¼ 22), and cyclophosphamide (N ¼22). The top 3 hormonal agents were anastrozole (N ¼10), letrozole (N ¼ 10), and leuprolide (N ¼ 9). The tar-geted therapies used were erlotinib (N ¼ 28), rituximab(N ¼ 22), gefitinib (N ¼ 19), bevacizumab (N ¼ 14),bortezomib (N ¼ 9), sorafenib (N ¼ 8), cetuximab (N ¼
Table 1. Characteristics of 2604 Cancer Patients WhoRequired APCU Admission
Characteristic No. (%a)
Median age (range), y 59 (18-101)
Female sex 1273 (48.9)
RaceCaucasian 1745 (67.0)
Black 422 (16.2)
Hispanic 307 (11.8)
Others 130 (5.0)
Religionb
Christian 2119 (94)
Others 135 (5.9)
Cancer diagnosisRespiratory 595 (22.9)
Gastrointestinal 512 (19.7)
Hematologic 304 (11.7)
Gynecologic 271 (10.4)
Genitourinary 217 (8.3)
Breast 207 (8.0)
Head and neck 155 (6.0)
Sarcoma 104 (4.0)
Dermatologic 99 (3.8)
Primary unknown 92 (3.5)
CNS 26 (1.0)
Endocrine 22 (0.8)
Admission typeAPCU only 740 (28.4)
Oncology ward and APCU 1864 (71.6)
Median admission durationMDACC hospital stay (Q1-Q3), d 11 (8-17)
APCU stay (Q1-Q3), d 7 (4-10)
Antineoplastic agent use during admissionc
Chemotherapeutic agents 297 (11.4)
Hormonal agents 54 (2.1)
Targeted agents 155 (6.0)
APCU indicates acute palliative care unit; CNS, central nervous system;
MDACC, The University of Texas M. D. Anderson Cancer Center; Q, inter-
quartile range.aUnless otherwise stated.bInformation regarding religion was not available for 350 patients.cOf the 435 patients who received antineoplastic therapy, 69 patients
received 2 classes of agents, and 1 patient received all 3 classes.
Original Article
2038 Cancer April 15, 2010
7), trastuzumab (N¼ 6), imatinib (N¼ 4), and sunitinib(N¼ 4).
During their APCU stay, 82 (3%), 35 (1%), and 58(2%), respectively, patients received chemotherapy, hor-monal agents, and targeted therapy. A total of 382 (15%)patients had ANT initiated while they were admittedunder an oncology service, and 53 (2%) received their firstdose after transfer to the APCU. Among the patients whowere treated with chemotherapeutic, hormonal, and tar-geted agents during hospitalization, 10%, 26%, and 12%,respectively, received the ANT after they were transferredto the APCU.
Yearly Trends of ANT Use
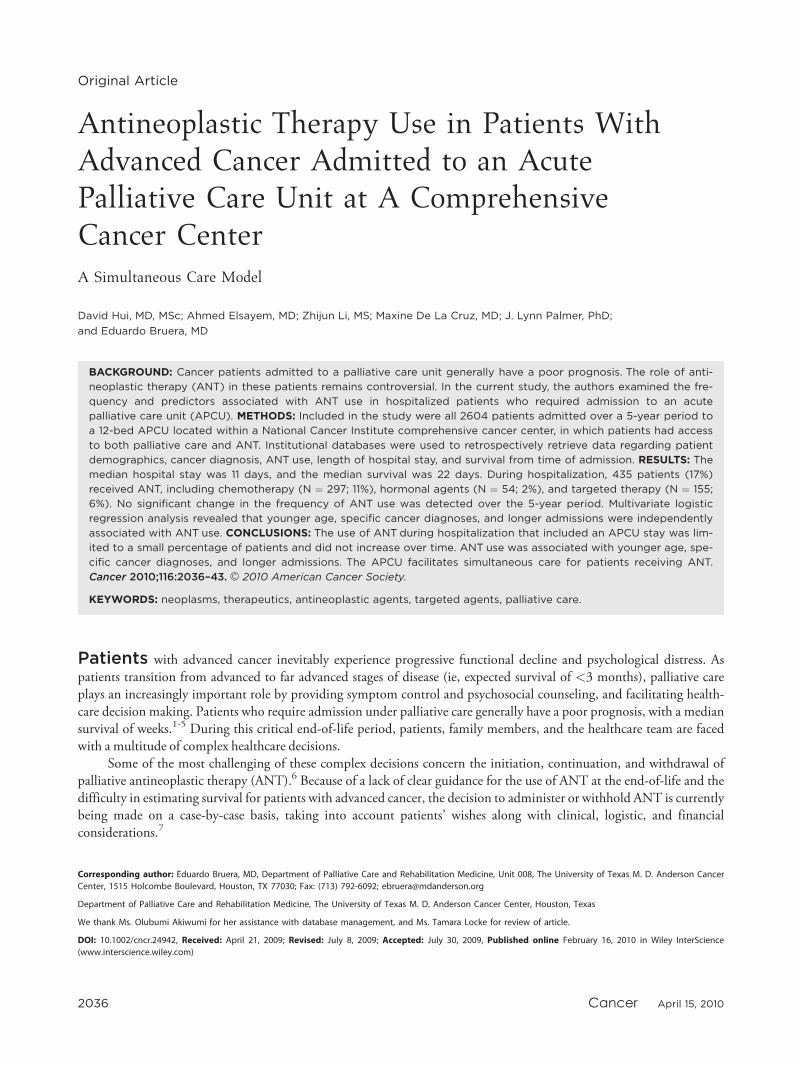
The frequency of ANT use during the entire hospitaliza-tion over the 5-year period is shown in Figure 1. Overall,no significant variation in the frequency of use was notedfor chemotherapy, hormonal therapy, and targeted agents.We also examined the yearly trend of ANT use duringAPCU admission and found no significant changes overtime (data not shown).
Factors Associated With ANT Use
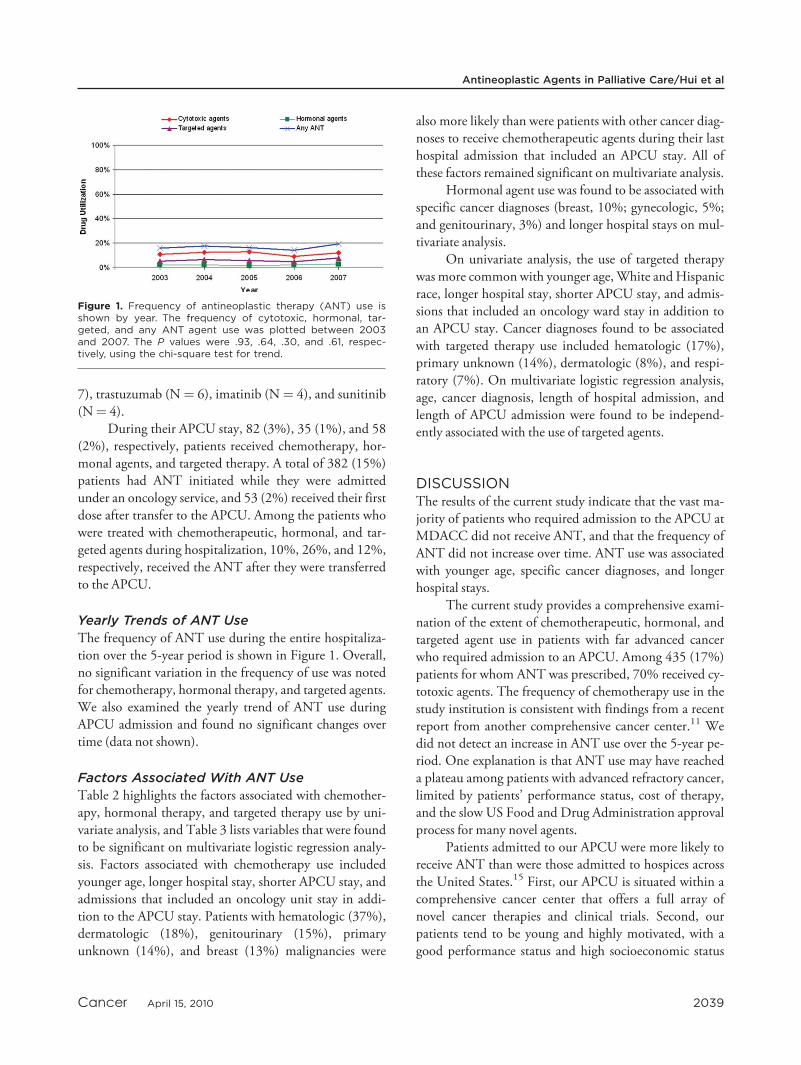
Table 2 highlights the factors associated with chemother-apy, hormonal therapy, and targeted therapy use by uni-variate analysis, and Table 3 lists variables that were foundto be significant on multivariate logistic regression analy-sis. Factors associated with chemotherapy use includedyounger age, longer hospital stay, shorter APCU stay, andadmissions that included an oncology unit stay in addi-tion to the APCU stay. Patients with hematologic (37%),dermatologic (18%), genitourinary (15%), primaryunknown (14%), and breast (13%) malignancies were
also more likely than were patients with other cancer diag-noses to receive chemotherapeutic agents during their lasthospital admission that included an APCU stay. All ofthese factors remained significant on multivariate analysis.
Hormonal agent use was found to be associated withspecific cancer diagnoses (breast, 10%; gynecologic, 5%;and genitourinary, 3%) and longer hospital stays on mul-tivariate analysis.
On univariate analysis, the use of targeted therapywas more common with younger age,White andHispanicrace, longer hospital stay, shorter APCU stay, and admis-sions that included an oncology ward stay in addition toan APCU stay. Cancer diagnoses found to be associatedwith targeted therapy use included hematologic (17%),primary unknown (14%), dermatologic (8%), and respi-ratory (7%). On multivariate logistic regression analysis,age, cancer diagnosis, length of hospital admission, andlength of APCU admission were found to be independ-ently associated with the use of targeted agents.
DISCUSSIONThe results of the current study indicate that the vast ma-jority of patients who required admission to the APCU atMDACC did not receive ANT, and that the frequency ofANT did not increase over time. ANT use was associatedwith younger age, specific cancer diagnoses, and longerhospital stays.
The current study provides a comprehensive exami-nation of the extent of chemotherapeutic, hormonal, andtargeted agent use in patients with far advanced cancerwho required admission to an APCU. Among 435 (17%)patients for whom ANT was prescribed, 70% received cy-totoxic agents. The frequency of chemotherapy use in thestudy institution is consistent with findings from a recentreport from another comprehensive cancer center.11 Wedid not detect an increase in ANT use over the 5-year pe-riod. One explanation is that ANT use may have reacheda plateau among patients with advanced refractory cancer,limited by patients’ performance status, cost of therapy,and the slow US Food and Drug Administration approvalprocess for many novel agents.
Patients admitted to our APCU were more likely toreceive ANT than were those admitted to hospices acrossthe United States.15 First, our APCU is situated within acomprehensive cancer center that offers a full array ofnovel cancer therapies and clinical trials. Second, ourpatients tend to be young and highly motivated, with agood performance status and high socioeconomic status
Figure 1. Frequency of antineoplastic therapy (ANT) use isshown by year. The frequency of cytotoxic, hormonal, tar-geted, and any ANT agent use was plotted between 2003and 2007. The P values were .93, .64, .30, and .61, respec-tively, using the chi-square test for trend.
Antineoplastic Agents in Palliative Care/Hui et al
Cancer April 15, 2010 2039

relative to the general oncology patient population. Third,our palliative care program provides simultaneous care inboth the outpatient and inpatient settings, in whichpatients can access both palliative care and ANT.
We found that younger age, specific cancer diagno-ses, and longer hospital admissions were associated withANT use. In particular, hematologic malignancy was a
strong predictor of chemotherapy and targeted therapyuse. Indeed, studies from our institution and from othershave shown that patients with hematologic malignanciesare more likely to be treated aggressively, to die in inten-sive care units, and to have delayed referrals to palliativecare compared with patients with solid tumors.16-18 Notsurprisingly, breast, genitourinary, and gynecologic
Table 2. Factors Associated With Antineoplastic Therapy Use During Hospital Admission That Included an APCU Stay
Chemotherapeutic Agents Hormonal Agents Targeted Agents
NoChemotherapy(N52307)
Chemotherapy(N5297)
Pa NoHormones(N52550)
Hormones(N554)
Pa NoTargetedTherapy(N52449)
TargetedTherapy(N5155)
Pa
Mean age (SD), y 58.9 (13.4) 54.0 (14.9) <.001 58.3�13.6 59.1�13.6 .66 58.6�13.6 53.8�14.6 <.001
GenderFemale 1123 (88.2%) 150 (11.8%) .55 1231 (96.7%) 42 (3.3%) <.001 1195 (93.9%) 78 (6.1%) .71
Male 1184 (89%) 147 (11%) 1319 (99.1%) 12 (0.9%) 1254 (94.2%) 77 (5.8%)
RaceWhite 1543 (88.4%) 203 (11.6%) .77 1712 (98.1%) 34 (1.9%) .83 1646 (94.3%) 100 (5.7%) .018
Black 374 (88.6%) 48 (11.4%) 413 (97.9%) 9 (2.1%) 390 (92.4%) 32 (7.6%)
Hispanic 272 (88.6%) 35 (11.4%) 300 (97.7%) 7 (2.3%) 297 (96.7%) 10 (3.3%)
Others 118 (91.5%) 11 (8.5%) 125 (96.9%) 4 (3.1%) 116 (89.9%) 13 (10.1%)
ReligionChristian 1886 (89.0%) 233 (11.0%) .27 2075 (97.9%) 44 (2.1%) .28 2001 (94.4%) 118 (5.6%) .21
Non-Christian 116 (85.9%) 19 (14.1%) 134 (99.3%) 1 (0.7%) 124 (91.9%) 11 (8.1%)
Cancer typesb
Hematologic 191 (62.8%) 113 (37.2%) <.001 300 (98.7%) 4 (1.3%) .23 250 (82.2%) 54 (17.8%) <.001
Solid tumors 2116 (92.0%) 184 (8.0%) 2250 (97.8%) 50 (2.2%) 2199 (95.6%) 101 (4.4%)
Dermatologic 81 (81.8%) 18 (18.2%) 99 (100%) 0 (0%) 91 (91.9%) 8 (8.1%)
Genitourinary 230 (84.9%) 41 (15.1%) 262 (96.7%) 9 (3.3%) 256 (94.5%) 15 (5.5%)
Primary unknown 79 (85.9%) 13 (14.1%) 90 (97.8%) 2 (2.2%) 79 (85.9%) 13 (14.1%)
Breast 180 (87.0%) 27 (13.0%) 186 (89.9%) 21 (10.1%) 198 (95.7%) 9 (4.3%)
Endocrine 20 (90.9%) 2 (9.1%) 22 (100%) 0 (0%) 22 (100%) 0 (0%)
Gynecologic 199 (91.7%) 18 (8.3%) 207 (95.4%) 10 (4.6%) 215 (99.1%) 2 (0.9%)
Gastrointestinal 482 (94.1%) 30 (5.9%) 510 (99.6%) 2 (0.4%) 498 (97.3%) 14 (2.7%)
Head and neck 148 (95.5%) 7 (4.5%) 155 (100%) 0 (0%) 148 (95.5%) 7 (4.5%)
Respiratory 572 (96.1%) 23 (3.9%) 589 (99%) 6 (1%) 555 (93.3%) 40 (6.7%)
Sarcoma 100 (96.2%) 4 (3.8%) 104 (100%) 0 (0%) 103 (99.0%) 1 (1.0%)
CNS 25 (96.2%) 1 (3.8%) 26 (100%) 0 (0%) 26 (100%) 0 (0%)
Admission typeAPCU only 720 (97.3%) 20 (2.7%) <.001 728 (98.4%) 12 (1.6%) .31 712 (96.2%) 28 (3.8%) .003
Oncology ward/APCU 1587 (85.1%) 277 (14.8%) 1822 (97.7%) 42 (2.3%) 1737 (93.2%) 127 (6.8%)
Median MDACC hospital
admission length
(Q1-Q3), d
7 (11-16) 18 (11-26) <.001 11 (8-17) 13.5 (9-21) .051 11 (8-17) 15 (10-26) <.001
Median APCU admission
length (Q1-Q3), d
7 (4-10) 7 (4-9) .003 7 (4-10) 7 (5-9) 1.0 7 (4-10) 6 (4-9) .11
APCU indicates acute palliative care unit; SD, standard deviation; CNS, central nervous system; MDACC, The University of Texas M. D. Anderson Cancer Cen-
ter; Q, interquartile range.aComparisons were made between patients who received antineoplastic therapy and those who did not. The chi-square test was used for categorical varia-
bles, the Student t test was used for age, and the Mann-Whitney U test was used for median hospital admission and APCU admission length.bComparisons were made between all solid tumors and hematogic malignancies using the chi-square test for chemotherapy and targeted agents, and the
Fisher exact test for hormonal agents.
Original Article
2040 Cancer April 15, 2010
malignancies were associated with hormonal therapy usein our cohort.
The overall length of hospital stay increased withANT use, which could be explained by the extra timeneeded for treatment administration and for patients torecover from therapy. The administration of ANT wasalso associated with a shorter stay in the APCU; thus,patients who received ANT spent a proportionally largeramount of time in the oncology ward. It is interesting tonote that neither race nor religion was a key considerationin the frequency of ANT use.
Both the American Society of Clinical Oncology19-21
and the National Quality Forum22 have stated thatchemotherapy use within 14 days of death is an indicatorof poor end-of-life care. Only 5.5% of patients in the cur-rent study cohort met this criterion. Although the principleof minimizing aggressive therapies in dying patients isfundamentally sound, survival estimation is extremely diffi-cult, with to our knowledge no standard prognostic toolsavailable for advanced cancer patients.23-26 More researchis necessary to establish predictors of survival in this popu-lation. Until highly accurate prognostic models such as theAcute Physiology and Chronic Health Evaluation(APACHE) Score27 in the critical care setting becomeavailable for advanced cancer patients, the application ofthe duration between chemotherapy and death as an indi-
cator of quality of care is challenging. Other reasons forthe administration of ANT close to the end-of-life includeheightened expectations and the hope of prolonging lifeand symptom control.7,28-35 Some patients may have anarrow window of opportunity for therapeutic interven-tion, and a trial of ANT may appear to be reasonable.Another reason is the increasing availability of new ANTover the past decade. Many of these agents are associatedwith fewer adverse effects than older agents, making it pos-sible for patients to receive ANT later in the trajectory ofillness.
One of the problems with chemotherapy adminis-tration close to the end-of-life is that it poses a barrier forpatients with far advanced cancer to receive palliative careand hospice services, because they frequently have to ‘‘giveup’’ ANT before enrollment onto these programs.36 Inthe current series, all patients who received chemotherapyhad access to both palliative care and oncology teams,highlighting a key advantage of an integrated palliativecare program. Indeed, a strong integration of palliativecare into oncology practice under the simultaneous caremodel may enhance the care of advanced cancer patientswho require ANT.10,37 First, optimal symptom manage-ment would support patients through treatments, andhelp maintain their quality of life. Second, the simultane-ous model would allow palliative care to be introduced
Table 3. Multivariate Logistic Regression Analysis for Factors Associated With Antineoplastic Agent Use During HospitalAdmission That Included an APCU Stay
ChemotherapeuticAgents OR(95% CI)
P HormonalAgents OR(95% CI)
P TargetedAgents OR(95% CI)
P
Age, per y 0.98 (0.97-0.99) <.001 — — — 0.97 (0.96-0.99) <.001
Cancer types — — <.001 — — <.001 — — .001
Hematologic 8 (4.8-13.2) <.001 0.95 (0.3-3.7) .95 1.6 (0.9-2.6) .11
Dermatologic 4 (2.0-7.9) <.001 — — — 1 (0.4-2.4) 1
Genitourinary 4.4 (2.6-7.6) <.001 3.3 (1.2-9.4) .024 0.57 (0.28-1.18) .14
Primary unknown 3.5 (1.7-7.4) <.001 2.1 (0.4-10.6) .37 0.67 (0.23-2.0) .47
Breast 3.3 (1.8-5.9) <.001 11.4 (4.5-28.6) <.001 0.57 (0.3-1.2) .15
Endocrine 2.1 (0.4-9.9) .35 — — — — — —
Gynecologic 1.8 (0.9-3.5) .077 4.7 (1.7-13.2) .003 0.12 (0.03-0.51) .004
Gastrointestinal 1.5 (0.8-2.6) .19 0.4 (0.08-1.9) .24 .32 (0.16-0.65) .001
Head and neck 1.2 (0.5-2.9) .69 — — — 0.39 (0.14-1.1) .08
Respiratory 1 (Reference) — 1 (Reference) — 1 (Reference) —
Sarcoma 0.6 (0.2-1.9) .41 — — — — — —
CNS 0.6 (0.08-5.0) .67 — — — — — —
APCU only admission 0.31 (0.19-0.51) <.001 — — — — — —
MDACC hospital admission
length, per d
1.04 (1.03-1.06) <.001 1.02 (1.0-1.05) .035 1.03 (1.02-1.05) <.001
APCU admission length, per d 0.96 (0.93-0.99) 0.01 — — — 0.94 (0.90-0.98) .007
APCU indicates acute palliative care unit; OR, odds ratio; 95% CI, 95% confidence interval; CNS, central nervous system; MDACC, The University of Texas
M. D. Anderson Cancer Center.
Antineoplastic Agents in Palliative Care/Hui et al
Cancer April 15, 2010 2041

earlier in the patientapos;s disease trajectory, and in theprocess significantly increase its effectiveness throughtimely symptom control, psychosocial interventions, andtransition of care. This is in contrast to the traditionaldichotomized model of active treatment and palliativecare/hospice, which results in fragmented care, delayedpalliative care referrals, the need to sacrifice quality of lifefor potential gain in quantity of life, and significantemotional distress.34
The current study had several limitations. First, thisstudy was only able to examine treatments given duringhospital admissions that included an APCU stay. Due tothe short survival in the current study cohort, we believethe likelihood of ANT use after APCU discharge is mini-mal. However, further studies are required to addressANT use before and after admission. Second, severalpotential determinants of ANT, such as education level,socioeconomic status, cancer stage, location of metastases,symptom profile, and performance status were not avail-able. Indeed, universal documentation of symptoms andperformance status during the APCU admission wouldhelp to assess the potential impact of palliative care onphysical and psychosocial distress at the end of life.Finally, patients who are treated at our comprehensivecancer center and the treatments that they received maynot be representative of cancer patients and treatmentsthroughout the United States; thus, the results may not begeneralizable.
In summary, our APCU served patients withadvanced cancer who had unique clinical characteristicsand treatment needs, and facilitated simultaneous care. Inthe era of personalized medicine, we need to develop notonly novel therapeutics targeting specific mutationswithin the cancer, but also symptom management strat-egies and psychosocial interventions tailored to ourpatients’ needs and their disease trajectory. Identificationof clinical and pathologic markers to better predict clinicalbenefits and adverse effects associated with ANT, coupledwith improved prognostication skills and treatment-deci-sion tools, would allow us to better customize therapeuticdecisions. The further integration of palliative care intothe practice of oncology under a simultaneous care modelwill improve patient access to palliative care, and hope-fully improve their quality of life.
CONFLICT OF INTEREST DISCLOSURESDr. Bruera is supported in part by the National Institutes ofHealth (Grants RO1CA1RO10162-01A1, RO1CA1222292-01,and RO1CA124481-01). Dr. Hui is funded by the Clinician In-
vestigator Program, Royal College of Physicians and Surgeons ofCanada.
REFERENCES1. Rees E, Hardy J, Ling J, Broadley K, A’Hern R. The use of
the Edmonton Symptom Assessment Scale (ESAS) within apalliative care unit in the UK. Palliat Med. 1998;12:75-82.
2. Lam PT, Leung MW, Tse CY. Identifying prognostic fac-tors for survival in advanced cancer patients: a prospectivestudy. Hong Kong Med J. 2007;13:453-459.
3. Moro C, Brunelli C, Miccinesi G, et al. Edmonton Symp-tom Assessment Scale: Italian validation in 2 palliative caresettings. Support Care Cancer. 2006;14:30-37.
4. Costantini M, Toscani F, Gallucci M, et al. Terminal can-cer patients and timing of referral to palliative care: a multi-center prospective cohort study. Italian CooperativeResearch Group on Palliative Medicine. J Pain SymptomManage. 1999;18:243-252.
5. Paci E, Miccinesi G, Toscani F, et al. Quality of life assess-ment and outcome of palliative care. J Pain Symptom Man-age. 2001;21:179-188.
6. Browner I, Carducci MA. Palliative chemotherapy: historicalperspective, applications, and controversies. Semin Oncol.2005;32:145-155.
7. Matsuyama R, Reddy S, Smith TJ. Why do patients choosechemotherapy near the end of life? A review of the perspec-tive of those facing death from cancer. J Clin Oncol.2006;24:3490-3496.
8. Meyers FJ, Linder J, Beckett L, Christensen S, Blais J, Gan-dara DR. Simultaneous care: a model approach to the per-ceived conflict between investigational therapy and palliativecare. J Pain Symptom Manage. 2004;28:548-556.
9. Meyers FJ, Linder J. Simultaneous care: disease treatmentand palliative care throughout illness. J Clin Oncol.2003;21:1412-1415.
10. Lagman R, Walsh D. Integration of palliative medicine intocomprehensive cancer care. Semin Oncol. 2005;32:134-138.
11. Lagman R, Rivera N, Walsh D, LeGrand S, Davis MP.Acute inpatient palliative medicine in a cancer center: clini-cal problems and medical interventions-a prospective study.Am J Hosp Palliat Care. 2007;24:20-28.
12. Sato K, Miyashita M, Morita T, Sanjo M, Shima Y, Uchi-tomi Y. Quality of end-of-life treatment for cancer patientsin general wards and the palliative care unit at a regionalcancer center in Japan: a retrospective chart review. SupportCare Cancer. 2008;16:113-122.
13. Elsayem A, Swint K, Fisch MJ, et al. Palliative care inpa-tient service in a comprehensive cancer center: clinical andfinancial outcomes. J Clin Oncol. 2004;22:2008-2014.
14. Kaplan EL, Meier P. Nonparametric estimation fromincomplete observations. J Am Stat Assoc. 1958;53:457-481.
15. Mintzer DM, Zagrabbe K. On how increasing numbers ofnewer cancer therapies further delay referral to hospice: theincreasing palliative care imperative. Am J Hosp Palliat Care.2007;24:126-130.
16. Cheng WW, Willey J, Palmer JL, Zhang T, Bruera E.Interval between palliative care referral and death amongpatients treated at a comprehensive cancer center. J PalliatMed. 2005;8:1025-1032.
17. Fadul N, Elsayem A, Palmer JL, Zhang T, Braiteh F, BrueraE. Predictors of access to palliative care services among
Original Article
2042 Cancer April 15, 2010

patients who died at a comprehensive cancer center. J PalliatMed. 2007;10:1146-1152.
18. McGrath P. Are we making progress? Not in haematology!Omega (Westport). 2002;45:331-348.
19. Cancer care during the last phase of life. J Clin Oncol.1998;16:1986-1996.
20. McNiff KK, Neuss MN, Jacobson JO, Eisenberg PD,Kadlubek P, Simone JV. Measuring supportive care in med-ical oncology practice: lessons learned from the quality on-cology practice initiative. J Clin Oncol. 2008;26:3832-3837.
21. Earle CC, Park ER, Lai B, Weeks JC, Ayanian JZ, Block S.Identifying potential indicators of the quality of end-of-lifecancer care from administrative data. J Clin Oncol. 2003;21:1133-1138.
22. National Quality Forum. A National Framework and Pre-ferred Practices for Palliative and Hospice Care Quality.Washington, DC: National Quality Forum; 2006.
23. Lamont EB, Christakis NA. Some elements of prognosis interminal cancer. Oncology (Williston Park). 1999;13:1165-1170; discussion 1172-1174, 1179-1180.
24. Lamont EB, Christakis NA. Physician factors in the timingof cancer patient referral to hospice palliative care. Cancer.2002;94:2733-2737.
25. Glare PA, Sinclair CT. Palliative medicine review: prognos-tication. J Palliat Med. 2008;11:84-103.
26. Maltoni M, Caraceni A, Brunelli C, et al. Prognostic factorsin advanced cancer patients: evidence–based clinical recom-mendations–a study by the Steering Committee of the Euro-pean Association for Palliative Care. J Clin Oncol. 2005;23:6240-6248.
27. Zimmerman JE, Kramer AA, McNair DS, Malila FM.Acute physiology and chronic health evaluation (APACHE)IV: hospital mortality assessment for today’s critically illpatients. Crit Care Med. 2006;34:1297-1310.
28. Grunfeld EA, Ramirez AJ, Maher EJ, et al. Chemotherapyfor advanced breast cancer: what influences oncologists’ de-cision-making? Br J Cancer. 2001;84:1172-1178.
29. Doyle C, Crump M, Pintilie M, Oza AM. Does palliativechemotherapy palliate? Evaluation of expectations, out-comes, and costs in women receiving chemotherapy foradvanced ovarian cancer. J Clin Oncol. 2001;19:1266-1274.
30. Koedoot CG, De Haes JC, Heisterkamp SH, Bakker PJ, DeGraeff A, De Haan RJ. Palliative chemotherapy or watchfulwaiting? A vignettes study among oncologists. J Clin Oncol.2002;20:3658-3664.
31. Geels P, Eisenhauer E, Bezjak A, Zee B, Day A. Palliativeeffect of chemotherapy: objective tumor response is associ-ated with symptom improvement in patients with metastaticbreast cancer. J Clin Oncol. 2000;18:2395-2405.
32. Shanafelt TD, Loprinzi C, Marks R, Novotny P, Sloan J.Are chemotherapy response rates related to treatment-induced survival prolongations in patients with advancedcancer? J Clin Oncol. 2004;22:1966-1974.
33. Grunfeld EA, Maher EJ, Browne S, et al. Advanced breastcancer patients’ perceptions of decision making for palliativechemotherapy. J Clin Oncol. 2006;24:1090-1098.
34. Koedoot CG, de Haan RJ, Stiggelbout AM, et al. Palliativechemotherapy or best supportive care? A prospective studyexplaining patients’ treatment preference and choice. Br JCancer. 2003;89:2219-2226.
35. Harrington SE, Smith TJ. The role of chemotherapy at theend of life: ‘‘when is enough, enough?’’ JAMA. 2008;299:2667-2678.
36. Ford DW, Nietert PJ, Zapka J, Zoller JS, Silvestri GA. Bar-riers to hospice enrollment among lung cancer patients: asurvey of family members and physicians. Palliat SupportCare. 2008;6:357-362.
37. Golan H, Bielorai B, Grebler D, Izraeli S, Rechavi G,Toren A. Integration of a palliative and terminal care centerinto a comprehensive pediatric oncology department. PediatrBlood Cancer. 2008;50:949-955.
Antineoplastic Agents in Palliative Care/Hui et al
Cancer April 15, 2010 2043