antidepressant / anxiolytic antidepressant / anxiolytic escitalopram (lexapro) tri-cyclic...
TRANSCRIPT

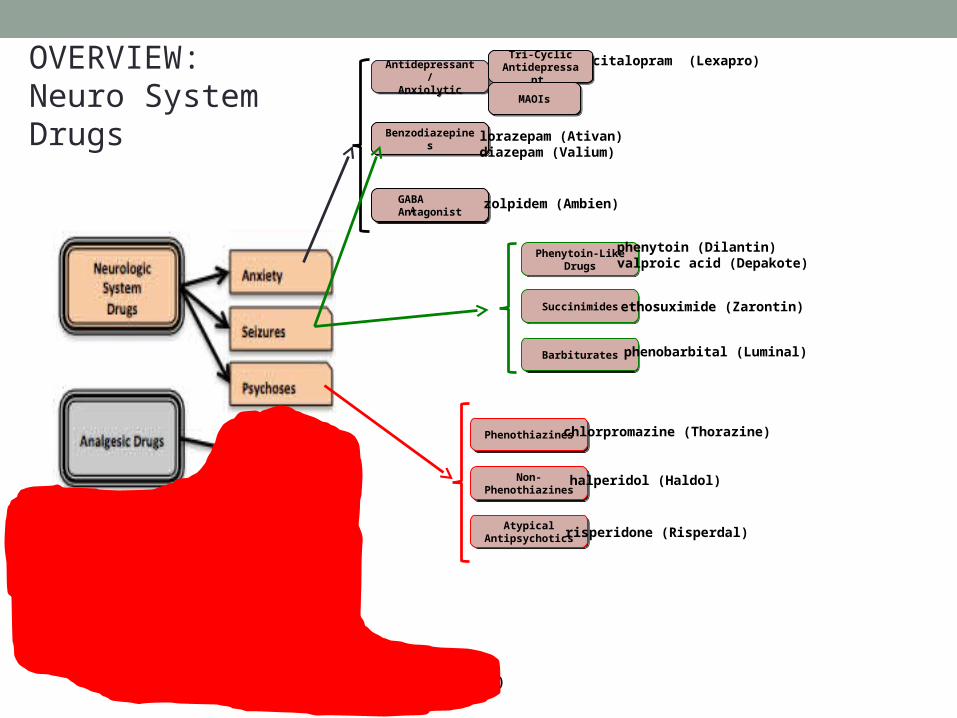
Antidepressant /Anxiolytic
Antidepressant /Anxiolytic
escitalopram (Lexapro)Tri-Cyclic Antidepressant
Tri-Cyclic Antidepressant
MAOIsMAOIs
BenzodiazepinesBenzodiazepines lorazepam (Ativan)diazepam (Valium)
GABA AntagonistGABA
AntagonistA zolpidem (Ambien)
Phenytoin-LikeDrugs
Phenytoin-LikeDrugs
SuccinimidesSuccinimides
BarbituratesBarbiturates phenobarbital (Luminal)
phenytoin (Dilantin)valproic acid (Depakote)
ethosuximide (Zarontin)
PhenothiazinesPhenothiazines chlorpromazine (Thorazine)
Non-Phenothiazines
Non-Phenothiazines
halperidol (Haldol)
Atypical Antipsychotics
Atypical Antipsychotics risperidone (Risperdal)
OpioidsOpioids
Opioid Antagonists
Opioid Antagonists
naloxone (Narcan)
morphine (Infumorph)
SalicylatesSalicylates aspirin (ASA)
NSAIDsNSAIDs ibuprofen (Motrin)
Non-OpioidNon-Opioid acetaminophen (Tylenol)
Central ActingCentral Acting tramadol (Ultram)
Anti-MigraineAnti-Migraine ergotamine (Cafergot)Sumatriptan (Imitrex)
OVERVIEW:Neuro SystemDrugs

Pain Assessment
• Subjective experience for clients• Numerical scales and surveys assist in assessment.• Effective pharmacotherapy depends on
• Assessment of degree of pain • Determining underlying disorders
Acute Pain
• Intense• Defined period of time

Chronic Pain
• Over six months’ duration• Interferes with daily activities
Nociceptive Pain
• Due to injury to tissues• Sharp, localized• Dull, throbbing, aching
Neuropathic Pain
• Due to injury to nerves• Burning, shooting, numbing
Pain Transmission
• Nociceptor stimulation• Spinal cord receives pain impulse through
• ∂ fibers – believed to signal sharp, well-defined pain• C fibers – believed to conduct dull, poorly localized pain

Endogenous Opioids
• May modify sensory information, interrupting pain transmission
• Endorphins, dynorphins, ekaphalins

Interruption of Pain Transmission
• Several target areas• Peripheral level• CNS level
• Pharmacological• Nonpharmacological

Nonpharmacologic Techniques for Pain Management
• Used alone or in conjunction with pharmacotherapy• May allow for lower doses and possibly fewer drug-related
adverse effects
Nonpharmacological Therapies
• Acupuncture• Biofeedback• Massage; therapeutic or physical touch• Heat or cold• Meditation or prayer• Relaxation• Art or music therapy• Chiropractic manipulation• Hypnosis• TENS• Energy therapies such a Reiki and Qi gong

Treatment for Intractable Cancer Pain
• Radiation or chemotherapy• Relieving nerve stimulation• Surgery • Nerve block
A natural or synthetic morphine-like substance responsible for reducing moderate to severe pain
Opioids

Opioid Receptors
• Receptors: mu, kappa, sigma, delta, epsilon• For pain management mu and kappa receptors are most important
• Opioid agonist drugs: stimulate receptors• Opioid antagonist drugs: block receptors
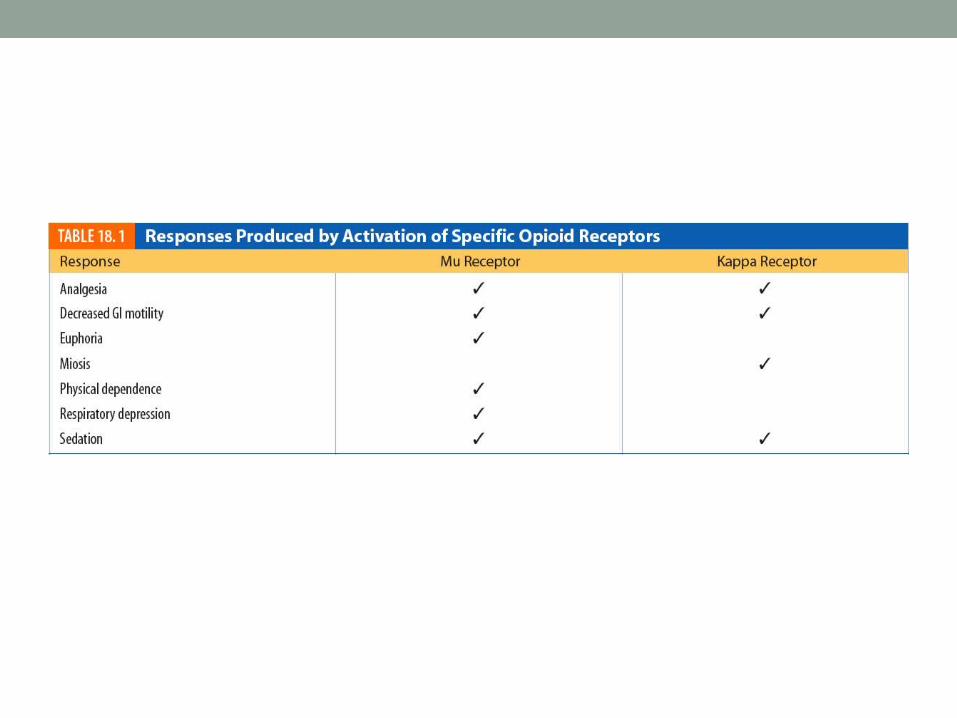

Figure 18.2 Opioid receptors

Opioid Antagonists
• Block opioid activity• Compete for opioid receptor
• Reverse symptoms of addiction, toxicity, and overdose• Naxalone (Narcan) may be used to reverse
respiratory depression and other acute symptoms• Also used to diagnose overdose
Opioid Dependence
• Potential to cause physical and psychologic dependence
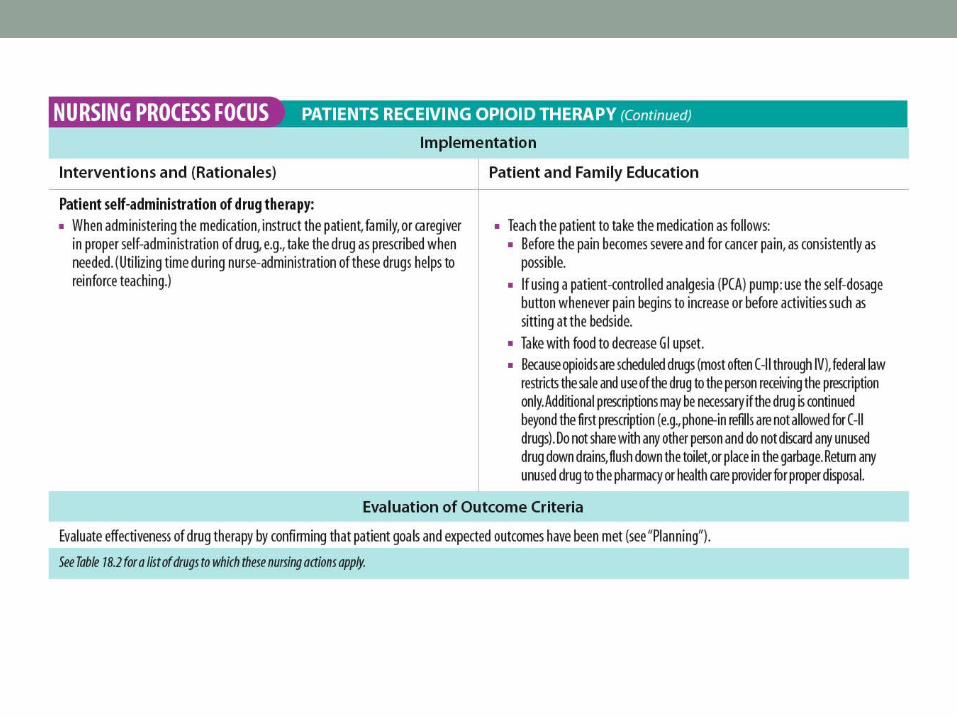
• Patient-controlled analgesia (PCA)• Combinations with nonnarcotic analgesics
Treatment for Opioid Dependence
• Switch from IV and inhalation forms to methadone, the oral form
• Methadone maintenance• Does not cure but avoids withdrawal symptoms• Treatment may continue for many months and years

Newer Treatment
• Early treatment: buprenorphine (Subutex)• Mixed opioid agonist-antagonist• Sublingual route
• Later maintenance: Suboxone
Role of Nurse
• Careful monitoring of client’s condition• Providing education• Obtaining medical history• Obtaining list of allergies• Assessing client’s pain level• Obtaining history of medications and alcohol and CNS-
depressant use
Opioid Therapy
• Assess potential for opioid dependency• Have narcotic antagonists available to reverse negative
effects
• Assist with activity• Monitor urine output for retention• Monitor client’s bowel habits for constipation
Opioid Antagonist Therapy
• Continue careful monitoring of client’s condition• Especially respiratory status
• Have resuscitative equipment available

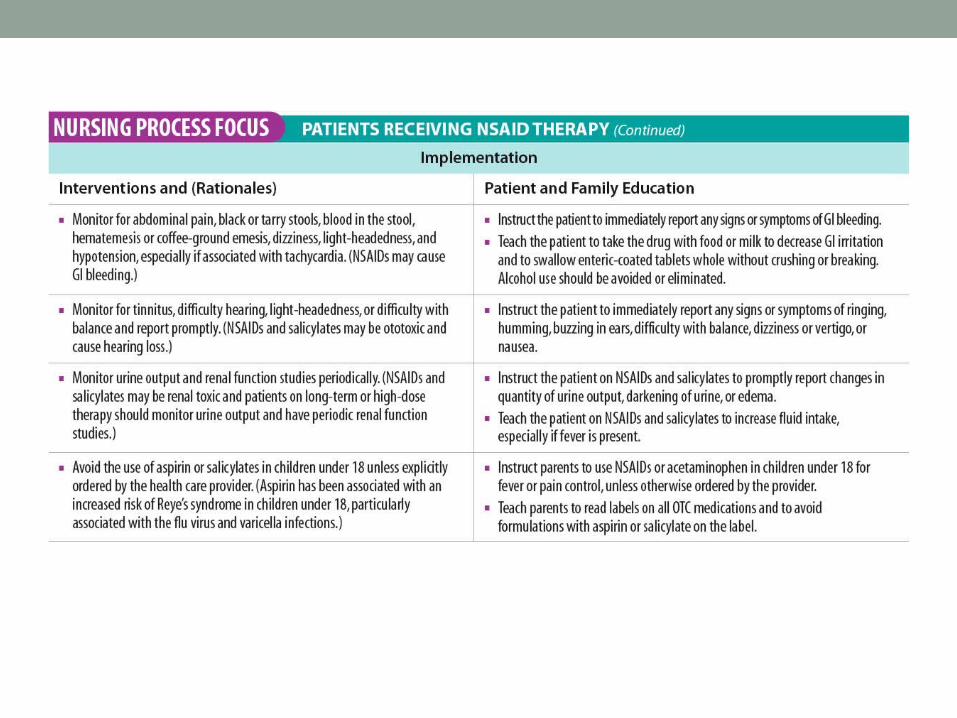
Nonopioid Analgesics
• Careful monitoring of client’s condition and providing education is necessary
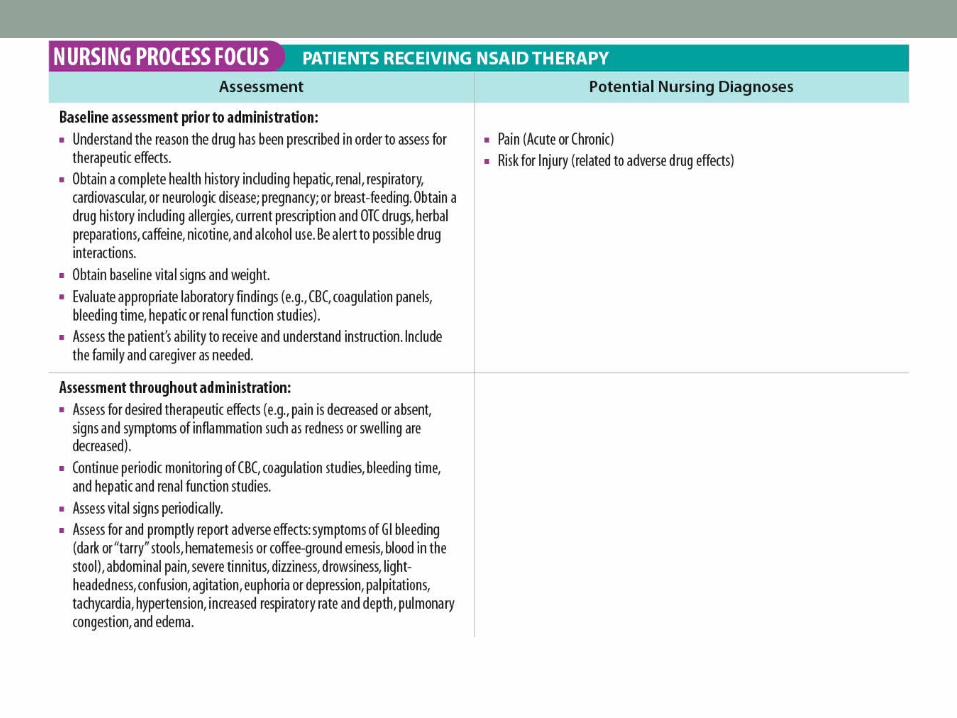
• Thorough assessment for hypersensitivity, bleeding disorders
• Through assessment for gastric ulcers, severe renal/hepatic disease, pregnancy
Nonopioid Analgesics (continued)
• Obtain laboratory tests on renal and liver function
• Pain assessment• Monitor for side effects
Opioid (Narcotic) Analgesic
• Prototype drug: Opioid agonists (morphine)• Mechanism of action: interacts with mu and kappa receptor sites
• Primary use: for analgesia and anesthesia• Adverse effects: respiratory depression, sedation, nausea, and vomiting

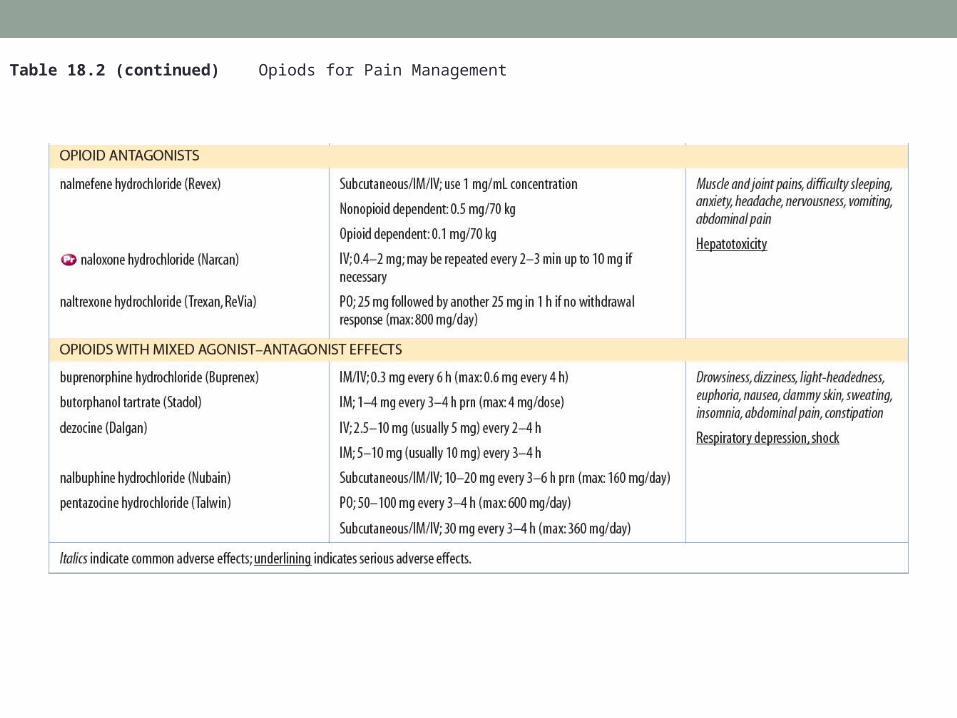
Table 18.2 (continued) Opiods for Pain Management


Morphine Animation
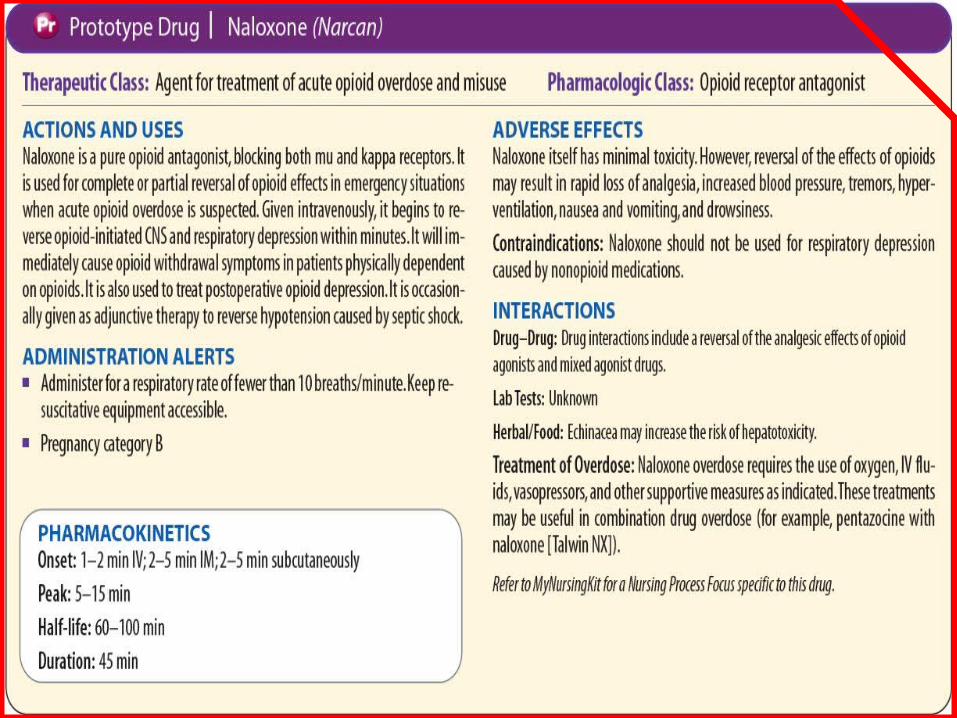
Opioid Antagonists
• Prototype drug: naloxone (Narcan)• Mechanism of action: interact with receptors
• Primary use: to reverse respiratory depression and other acute symptoms of opioid addiction, toxicity, overdose
Opioids with Mixed Agonist-Antagonist Activity
• Example: Talwin• Stimulate opioid receptor, thus causing analgesia• Withdrawal symptoms and side effects not as
intense as those of opioid agonists

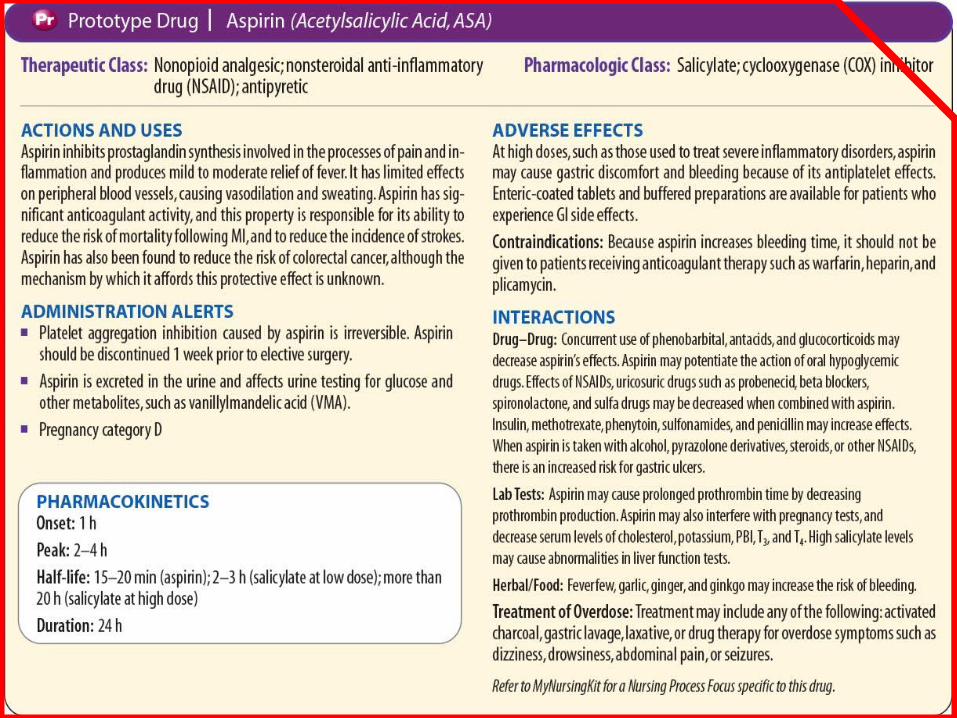
Salicylates
• Prototype drug: aspirin (ASA)• Mechanism of action: as anticoagulant, antipyretic, anti-inflammatory, and analgesic
• Adverse effects: with high doses may cause GI distress and bleeding
• May increase action of oral hypoglycemic agents
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
• Prototype drug: ibuprofen (Motrin)• Mechanism of action: to inhibit cyclooxygenase
and prevent formation of prostaglandins • Primary use: for mild or moderate pain and to
reduce inflammation • Adverse effects: GI upset, acute renal failure
Selective Cox-2 Inhibitors
• Prototype drug: celecoxib (Celebrex)• Mechanism of action: is similar to the NSAIDs• Primary use: to relieve pain, fever, inflammation• Adverse effects: mild and related to GI system

Nonopioid Analgesics
• Prototype drug: acetaminophen (Tylenol)• Mechanism of action: to treat fever: at the level
of the hypothalamus and causes dilation of peripheral blood vessels enabling sweating and dissipation of heat
• Primary use: treatment of fever and to relieve pain
• Adverse effects: uncommon with therapeutic doses
Acetaminophen Animation
Click here to view an animation on the topic of acetaminophen.
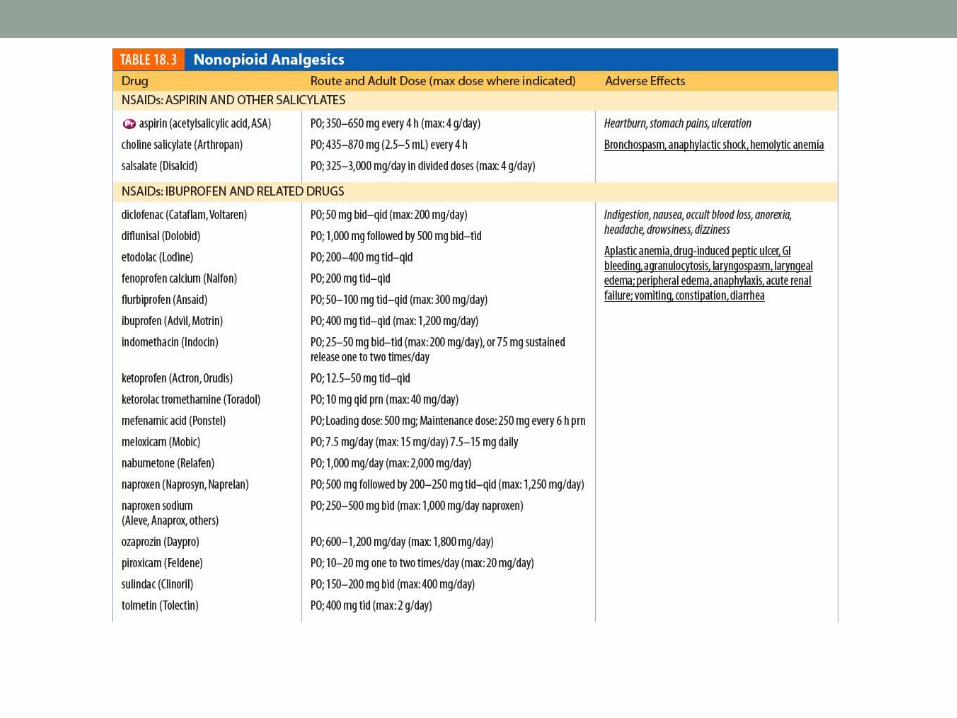

Table 18.3 (continued) Nonopioid Analgesics

Centrally Acting Agents
• Prototype drug: tramadol (Ultram)• Mechanism of action: has weak opioid activity• Primary use: as centrally acting analgesic• Adverse effects can include: CNS, GI, CV and
dermatologic effects

Ergot Alkaloids
• Mechanism of action: to promote vasoconstriction• Primary use: to terminate ongoing migraines• Adverse effects: GI upset, weakness in the legs,
myalgia, numbness and tingling in fingers and toes, angina-like pain, tachycardia
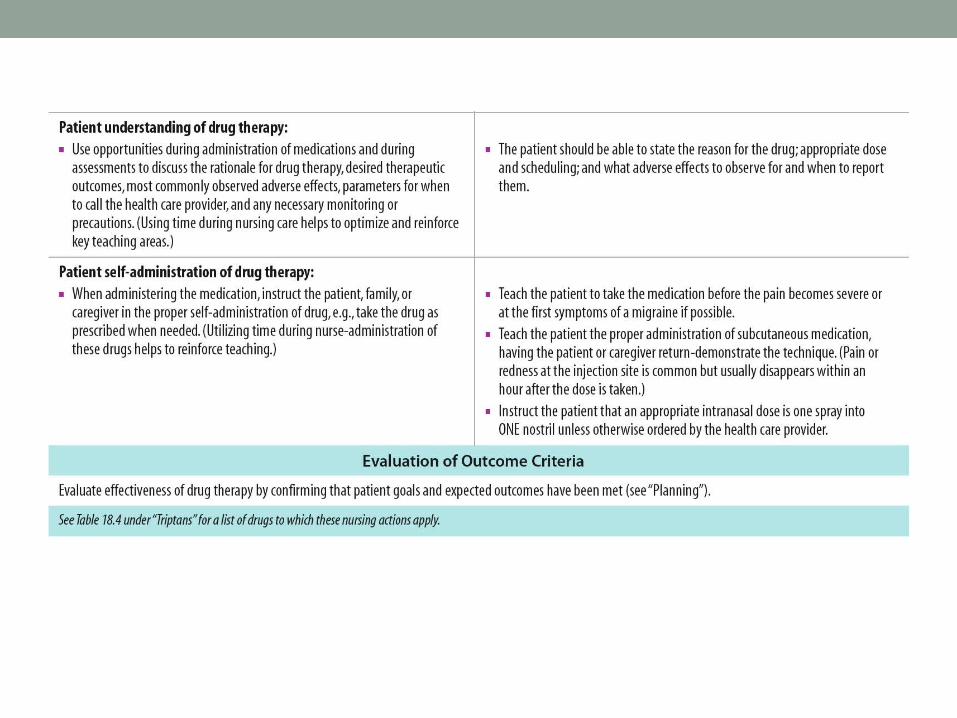
Triptans
• Prototype drug: sumatriptan (Imitrex)• Mechanism of action: to act as serotonin
agonists, constricting certain intracranial vessels • Primary use: to abort migraines with or without
auras • Adverse effects: GI upset
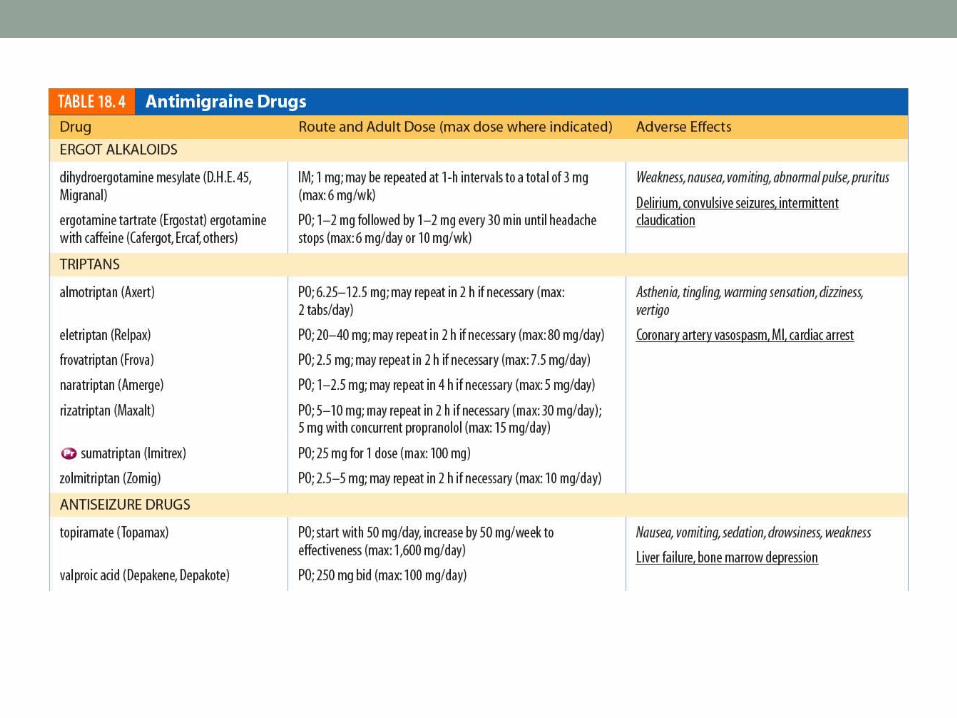

Table 18.4 (continued) Antimigraine Drugs

Opioid Agonists
• Mechanism of action: to interact with specific receptors
• Primary use: to relieve moderate to severe pain; some used for anesthesia
• Examples: OxyContin, Percocet
Opiod Antangonists
• Blockers of opioid activity• Used to reverse symptoms of opioid addiction, toxicity,
overdose
• Examples: Revex, Narcan, Trexan

Nonopioid Analgesics
• Used for fever, inflammation, and analgesia• Used for mild or moderate pain associated
with inflammation• Examples: Celebrex, Cataflam, Dolobid,
Lodine, Nalfon

Antimigraine Agents
• Triptans• Serotonin agonists• Act by constricting certain intracranial vessels
• Ergot alkaloids• Serotonin agonists• Act as vasoconstrictors• Terminate ongoing migraines
• Migranal, Axert, Relpax, Frova

NCLEX-RN ReviewQuestion 1
The nurse teaches the patient relaxation techniques and guided imagery as an adjunct to medication for treatment of pain. The nurse explains that the major benefit of these techniques is that they:
1. Are less costly 2. Allow lower doses of drugs
with fewer side effects3. Can be used at home 4. Do not require self-injection

NCLEX-RN ReviewQuestion 1 – Answer
1. Are less costly
2. Allow lower doses of drugs with fewer side effects
3. Can be used at home
4. Do not require self-injection

NCLEX-RN ReviewQuestion 1 – Rationale
Rationale: When used concurrently with medication, nonpharmacologic techniques may allow for lower doses and possibly fewer drug-related adverse effects. Relaxation techniques and imagery may also be used in the acute care setting.
NCLEX-RN ReviewQuestion 2
The nurse recognizes that opioid analgesics exert their action by interacting with a variety of opioid receptors. Drugs such as morphine act by:
1. Activating kappa and blocking mu receptors2. Inhibiting mu and kappa receptors 3. Activating mu and kappa receptors4. Blocking sigma and delta receptors

NCLEX-RN ReviewQuestion 2 – Answer
1. Activating kappa and blocking mu receptors
2. Inhibiting mu and kappa receptors
3. Activating mu and kappa receptors
4. Blocking sigma and delta receptors

NCLEX-RN ReviewQuestion 2 – Rationale
Rationale: Some opioid agonists, such as morphine, activate both mu and kappa receptors.

NCLEX-RN ReviewQuestion 3
A patient admitted with hepatitis B is prescribed Vicodin 2 tablets for pain. The appropriate nursing action is to:
1. Administer the drug as ordered2. Administer 1 tablet only3. Recheck the order with the health care
provider4. Hold the drug until the health care provider
arrives

NCLEX-RN ReviewQuestion 3 – Answer
1. Administer the drug as ordered
2. Administer 1 tablet only
3. Recheck the order with the health care provider
4. Hold the drug until the health care provider arrives

NCLEX-RN ReviewQuestion 3 – Rationale
Rationale: Vicodin is a combination drug of hydrocodone and acetaminophen. Acetaminophen can be hepatotoxic, and this patient has hepatitis B, a chronic liver disorder.
NCLEX-RN ReviewQuestion 5
Nursing interventions for a patient receiving opioid analgesics over an extended period should include:
1. Referring the patient to a drug treatment center
2. Encouraging increased fluids and fiber in the diet
3. Monitoring for GI bleeding4. Teaching the patient to self-assess blood
pressure
NCLEX-RN ReviewQuestion 5 – Answer
1. Referring the patient to a drug treatment center
2. Encouraging increased fluids and fiber in the diet
3. Monitoring for GI bleeding
4. Teaching the patient to self-assess blood pressure
NCLEX-RN ReviewQuestion 5 – Rationale
Rationale: Opioids suppress intestinal contractility, increase anal sphincter tone, and inhibit fluids into the intestines, which can lead to constipation.

NCLEX-RN ReviewQuestion 6
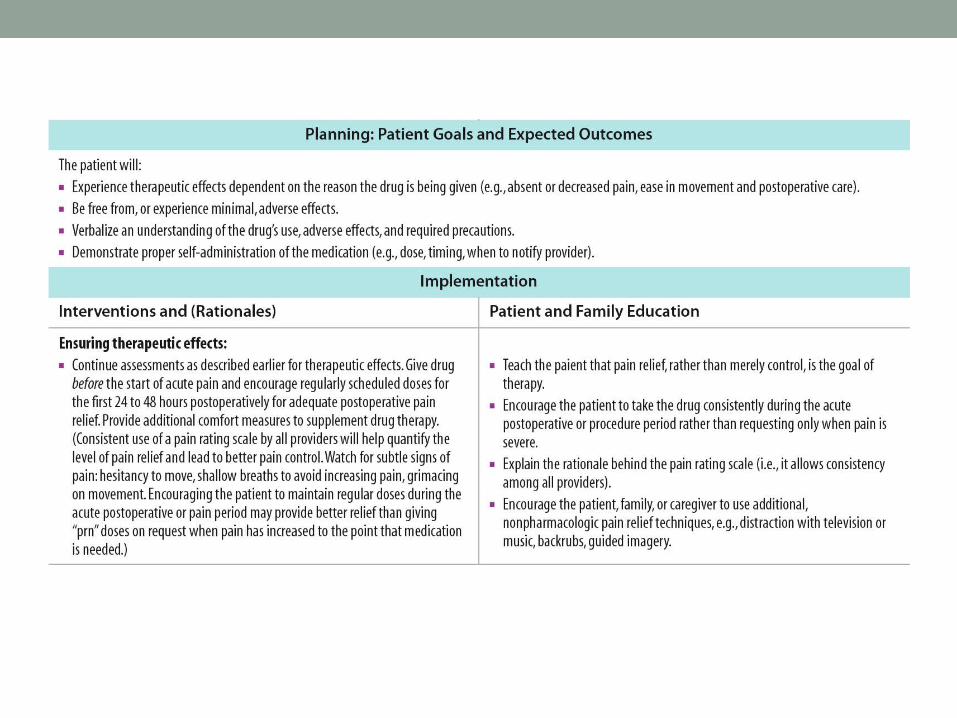
The most appropriate method to ensure adequate pain relief in the immediate postoperative period from an opioid drug would be to:
1. Give the drug only when the family members report that the patient is complaining of pain.
2. Give the drug every time the patient complains of acute pain.
3. Give the drug as consistently as possible for the first 24 to 48 hours.
4. Give the drug only when the nurse observes signs and symptoms of pain.

NCLEX-RN ReviewQuestion 6 – Answer
1. Give the drug only when the family members report that the patient is complaining of pain.
2. Give the drug every time the patient complains of acute pain.
3. Give the drug as consistently as possible for the first 24 to 48 hours.
4. Give the drug only when the nurse observes signs and symptoms of pain.

NCLEX-RN ReviewQuestion 6 – Rationale
Rationale: Opioid pain relievers should be given as consistently as possible, and before the onset of acute pain, in the immediate postoperative period unless the patient’s condition does not allow the consistent dosing (e.g., vital signs do not support regular doses).
Giving the drug only when the family members report that the patient is complaining of pain, every time the patient complains of acute pain, or only when the nurse observes signs and symptoms of pain. These methods of drug administration would potentially allow pain to become severe before being adequately treated. Patients or family members may not always report pain or may downplay the severity.
Cultural norms may also influence the patient’s way of exhibiting pain.


Drugs for Control of Pain
• Assessment• Carefully monitor client’s condition • Assess vital signs, especially respiratory status• Assess client’s pain level: character, duration, location, intensity of
pain • Obtain history of medications, alcohol use

Drugs for Control of Pain (continued)
• Assessment• Obtain medical history and history of migraine headaches• Assess client’s stress levels and coping mechanisms• Monitor for side effects and potential for dependency

Drugs for Control of Pain (continued)
• Nursing diagnosis• Knowledge deficit—condition, therapeutic regimen, side effects • Risk for dependency related to opioid therapy

Drugs for Control of Pain (continued)
• Planning• Goal is to explain proper use of medication• Client to be free of pain without dependency

Drugs for Control of Pain (continued)
• Implementation• Encourage compliance with medication regimen• Provide additional education

Drugs for Control of Pain (continued)
• Evaluation• Client should have pain control with limited side effects, no
dependency.
• Client verbalizes importance of taking prescribed medications.