antibody-drug conjugates for solid tumours: current
TRANSCRIPT

Antibody-drug conjugates for solid tumours: Current understanding and future directions
touchEXPERT OPINIONS
Disclaimer
∙ Unapproved products or unapproved uses of approved products may be discussed by the faculty; these situations may reflect the approval status in one or more jurisdictions.
∙ The presenting faculty have been advised by touchIME to ensure that they disclose any such references made to unlabelled or unapproved use.
∙ No endorsement by touchIME of any unapproved products or unapproved uses is either made or implied by mention of these products or uses in touchIME activities.
∙ touchIME accepts no responsibility for errors or omissions.

What is the current status of ADCs for solid tumours?
Prof. Giuseppe Curigliano
Associate Professor of Medical OncologyUniversity of Milan, Milan, Italy

How do antibody-drug conjugates differ from other
treatments for solid tumours?
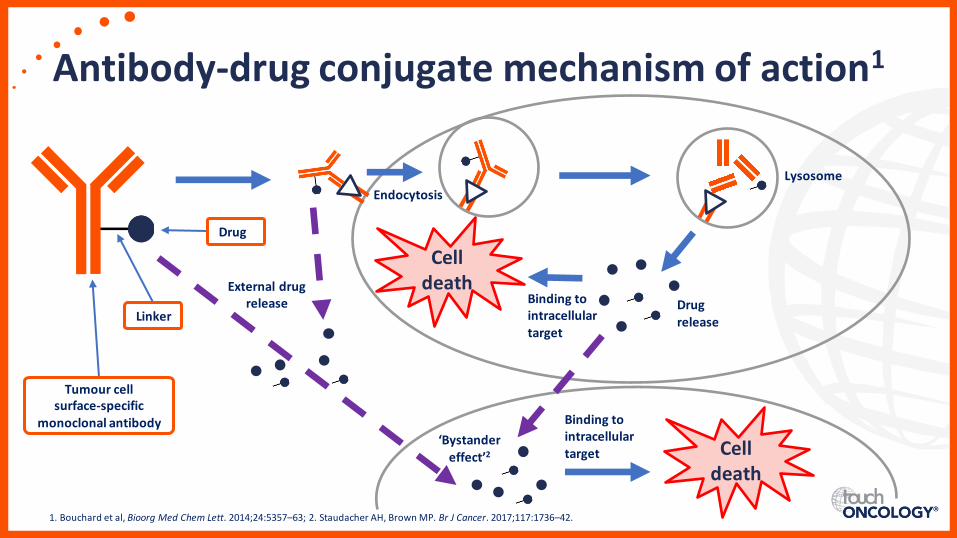
Antibody-drug conjugate mechanism of action1
1. Bouchard et al, Bioorg Med Chem Lett. 2014;24:5357–63; 2. Staudacher AH, Brown MP. Br J Cancer. 2017;117:1736–42.
Drug
Linker
Tumour cell surface-specific
monoclonal antibody
Endocytosis
Lysosome
Drug release
Binding to intracellular target
Celldeath
Binding to intracellular target Cell
death
External drug release
‘Bystander effect’2

What were the key efficacy findings in solid tumours for
emerging antibody-drug conjugates in 2020?

Summary of key efficacy data
CI, confidence interval; HER2, human epidermal growth factor receptor 2; NSCLC, non-small cell lung cancer; PFS, progression-free survival.1. Nakagawa K et al. Presented at World Conference on Lung Cancer Annual Meeting: 28–31 January 2021 2. Shitara K, et al. N Engl J Med. 2020;382:2419–30.
DESTINY-Lung01, phase II study of trastuzumab deruxtecan in HER2 overexpressing NSCLC1
(N=49)Median PFS: 5.4 months
(95% CI, 2.8–7.0)
DESTINY-Gastric01, phase II study of trastuzumab deruxtecan in HER2+ gastric cancer2
(N=125)Median PFS: 5.6 months
(95% CI, 4.3–6.9)100
0
40
60
80
20
Pro
bab
ility
of
PFS
(%
)
Time (months)0 1 132 3 4 10 11 125 6 7 8 9
Indicates upper andlower 95% CICensored cases
49 45 029 26 23 2 2 217 10 7 5 3No. of patients at risk
Trastuzumab deruxtecanPhysician’s choice of chemotherapy
100
0
40
60
80
20
10
20
20
20
90
Time (months)0 3 246 18 219 12 15
Trastuzumab deruxtecanPhysician’s choice of chemotherapy
No. of patients at risk
Pe
rce
nta
ge o
f p
atie
nts
(%
)
66
80
29
52
125 115 088 7 354 33 14
62 54 037 2 019 10 2

Summary of key efficacy data
ChT, chemotherapy; CI, confidence interval; EV, enfortumab vedotin; HR, hazard ratio; OS, overall survival.1. Powles T, et al. N Engl J Med. 2021; doi: 10.1056/NEJMoa2035807.
EV-301, phase III study of enfortumab vedotin in bladder cancer
EV (n=301) ChT (n=307)
Number of deaths 134 167
Median OS, months (95% CI)
12.88(10.58–15.21)
8.97 (8.05–10.74)
HR (95% CI), p-value 0.70 (0.56–0.89), p=0.001
100
0
40
50
80
10
20
30
60
70
90
Pe
rce
nta
ge o
f p
atie
nts
aliv
e
Time (months)No. of patients at riskEnfortumab
vedotinChemotherapy
0 3 246 9 12 15 18 211 2 4 5 7 0 11 13 14 16 17 19 20 22 238
301 257 0222 130 63 33 7 2286 272 246 234 190 105 85 52 42 23 15 4 3 1 1158
307 250 0198 101 51 29 6 2288 274 238 219 163 84 66 44 32 16 11 4 2 1 0131
Enfortumab vedotinChemotherapyCensored

Summary of key efficacy data
CI, confidence interval; HER2, human epidermal growth factor receptor 2; HR, hazard ratio; ORR, objective response rate; PFS, progression-free survival; SG, sacituzumabgovitecan; TNBC, triple-negative breast cancer; TPC, treatment of physician’s choice.1. Bardia A, et al. LBA17, presented at ESMO 2020.
ASCENT, phase III study of sacitzuzmab govitecan in metastatic TNBC
SG (n=235) TPC (n=233)
Number of events 166 150
Median PFS, months (95% CI)
5.6(4.3–6.3)
1.7 (1.5–2.6)
HR (95% CI), p-value 0.41 (0.32–0.52), p<0.0001
ORR, % 35 5
p-value p<0.0001
100
0
40
60
80
20Pro
bab
ility
of
PFS
(%
)
Time (months)No. of patients at risk
SG
TPC
0 3 246 9 12 15 18 21
SGTPCCensored
235 134 81 37 22 13 8 1222 166 127 104 63 54 33 24 05 316 15 89
233 35 12 6 2 1 0 0179 78 32 19 9 7 4 2 00 02 2 00

What are the key adverse events associated with
antibody-drug conjugates?

Common AEs in approved ADCs
ADC, antibody-drug conjugate; AE, adverse event.1. RxList. 2020. Available at: www.rxlist.com/padcev-side-effects-drug-center.htm (accessed 12 February 2021); 2. RxList. 2020. Available at: www.rxlist.com/enhertu-side-effects-drug-center.htm (accessed 12 February 2021); 3. Banerji U, et al. Lancet Oncol. 2019;20:1124–35; 4. RxList. 2020. Available at: www.rxlist.com/trodelvy-side-effects-drug-center.htm (accessed 12 February 2021).
Neutropenia
Enfortumab vedotin: 4%Trastuzumab duocarmazine: 6%Trastuzumab deruxtecan: 16%Sacituzumab govitecan: 43%
Anaemia
Trastuzumab deruxtecan 7%Sacituzumab govitecan: 12%
Vomiting
Enfortumab vedotin: 2%Trastuzumab deruxtecan: 3.8%
Sacituzumab govitecan: 6%
Fatigue
Enfortumab vedotin: 6%Trastuzumab duocarmazine: 4%
Trastuzumab deruxtecan: 6%Sacituzumab govitecan: 8%
Grade ≥31–4Nausea
Enfortumab vedotin: 3%Trastuzumab deruxtecan: 7%Sacituzumab govitecan: 6%
Conjunctivitis
Trastuzumab duocarmazine: 3%
Diarrhoea
Enfortumab vedotin: 6%Trastuzumab deruxtecan: 1.7%
Sacituzumab govitecan: 9%
Rash
Enfortumab vedotin: 13%Sacituzumab govitecan: 3%

What are the benefits of antibody-drug conjugates over other available treatments for
solid tumours in clinical practice?

Antibody-drug conjugate pros and cons1,2
mAb, monoclonal antibody; MDRP, multi-drug resistance pump.1. Nagayama A, et al. Target Oncol. 2017;12:719–39; 2. Tarcsa E, et al. Drug Discov Today Technol. 2020;doi:10.1016/j.ddtec.2020.07.002
Efficient targeting agent
Tumour cell specificity
Nanoscale drug carrier
Higher therapeutic index
Bystander effect
Off-target toxicity
Target antigen must be on all tumour cells
MDRPs can remove released drug from target cell
mAb size makes solid tumour penetration difficult

What’s next for ADCs in 2021 and beyond?
Prof. Giuseppe Curigliano
Associate Professor of Medical OncologyUniversity of Milan, Milan, Italy

When and how would emerging antibody-drug conjugates be
incorporated into the treatment paradigm?

Sequence of treatment
ADC, antibody-drug conjugate; ChT, chemotherapy; DFI, disease-free interval; ER, oestrogen receptor; HER2, human epidermal growth factor receptor 2; ET, endocrine treatment.1. Cardoso F, et al. Ann Oncol. 2020;31:1623–49.
Treatment of HER2+ advanced breast cancer
Trastuzumab deruxtecan
Other option not previously used to block HER2
Progression
T-DM1 (if available)
Previous treatment with (neo) adjuvant pertuzumab + trastuzumab
with a DFI <6–12 months
Unsuitable for ChT or with long DFI, minimal disease burden, and ER+
Anti-HER2 + ET
Trastuzumab + lapatinib
Trastuzumab + unused ChT
Trastuzumab + unused ET
if ER+
Tucatinib + trastuzumab + capecitabine
Second line
Third line
Fourth lineand beyond
First line

How do you manage adverse events and monitor patients
receiving ADCs?

Trastuzumab deruxtecan3
Interrupt dose until grade ≤2
Dose reduction 5.4 mg/kg→4.4 mg/kg →
3.2 mg/kg
Discontinue treatment if further dose
reduction required
How to manage common adverse eventsGrade ≥3 haematological toxicities, such as neutropenia
Sacituzumab govitecan4
Reduce dose by 25% at first occurrence
Reduce dose by 50% at second occurrence
Discontinue treatment at third occurrence
Trastuzumab duocarmazine2
Dose reduction 1.2 mg/kg Q3W→
0.9 mg/kg Q3W or
1.2 mg/kg Q6W
Enfortumab vedotin1
Interrupt dose until grade ≤1
Resume at same dose or consider dose
reduction by one level1.25 mg/kg →1.0 mg/kg→
0.75 mg/kg →0.5 mg/kg
Q3W, every 3 weeks; Q6W, every 6 weeks.1. US Food and Drug Administration. 2020. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2019/761137s000lbl.pdf (accessed 12 February 2021); 2. Banerji U, et al. Lancet Oncol. 2019;20:1124–35; 3. US Food and Drug Administration. 2020. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761139s000lbl.pdf (accessed 12 February 2021); 4. US Food and Drug Administration. 2020. Available at: www.accessdata.fda.gov/drugsatfda_docs/label/2020/761115s000lbl.pdf (accessed 12 February 2021).

Which ongoing clinical trials of emerging
antibody-drug conjugates are of most interest?

Ongoing trialsEstimated study completion date
Clinical trials listed by their identifiers at: ClinicalTrials.gov
2021 2022 2023 2024
Trastuzumab deruxtecanDESTINY-Breast 02NCT03523585
Trastuzumab deruxtecanDESTINY-Breast 03NCT03529110
Trastuzumab deruxtecan
DESTINY-Breast 04 NCT03734029
Trastuzumab deruxtecanDESTINY-Lung 02
NCT04644237
Trastuzumab deruxtecanDESTINY-Lung 03
NCT04686305
DatopotamabderuxtecanTROPION-LUNG01
NCT04656652
DatopotamabderuxtecanTROPION-PanTumorNCT03401385
ARX788ACE-Pan
Tumor-01 NCT03255070
Patritumabderuxtecan
HERTHENA-Lung01 NCT04619004
BAT8001 NCT04185649
Tisotumabvedotin
ENGOT-cx6 NCT03438396
EnfortumabvedotinEV-301
NCT03474107
Trastuzumab duocarmazine
TULIPNCT03262935

What are the future directions for
antibody-drug conjugates?

Future directions
New targets1 Drug-antibody ratio improvement2
Next-generation sequencing4
Antibody fragment-drug
conjugates3
1. Yamaguchi K, et al. Ann Oncol. 2020;31:S899–900; 2. Coats S, et al. Clin Cancer Res. 2019;25:5441–8; 3. Tarcsa E, et al. Drug Discov Today Technol. 2020; doi:10.1016/j.ddtec.2020.07.002; 4. Garczyk, S, et al. Am J Pathol 2020;190:323–32.