antibiotics & infections -...
TRANSCRIPT

Approach to
Antibiotics & Infections
by Sam Gharbi, MD

i
Antibiotics & Infections
2
Antibiotics & Infections
DisclaimerExtensive effort has been exerted in order to make this book as accurate as possible. However, the accuracy and completeness of the information provided cannot be guaranteed. This book is to be used as an educational guide only, and healthcare professionals should use sound clinical judge-ment and individualize therapy to each specific patient care situation.
The author makes no claims whatsoever, expressed or implied, about the authenticity, accuracy, reliability, completeness, or timeliness of the mate-rial presented in this book. In no event shall the author be liable to any party for indirect, direct, special, incidental, or consequential damages, including but not limited to lost profits arising out of the use of this book, even if the author has been advised of such damage.
By having read the above, or by use of this book, be it partially or in its entirety, you have explicitly consented your agreement to the above dis-claimer.
I often found that the approach to understanding antibiotics was one of the more poorly taught subjects during medical training. This e-book in fact first started as a collection of notes that I made for myself during medical school, and that I kept adding to during resi-dency and fellowship as I pieced together knowledge and experience that accrued on the topic over the years.
This e-book is meant to be an educational resource to help build a framework towards un-derstanding antibiotics and building a better approach. It is important to note that this e-book is not designed for clinical decision making. In such situations, I would recommend referring to your Sanford guide, or other center-specific resource.
A sincere thank you to all the physicians, residents, students, and pharmacists who have reviewed this text over the years and given constructive feedback in working to make it as accurate and user friendly as possible. In particular, a very big thanks to Dr. Iain Mackie for his years of support and mentorship, without whom this work would likely not have come to fruition.
To you the reader, I hope that you find this guide a useful learning resource, and I wish you the best of luck in your ongoing medical education.
Sincerely,
Sam Gharbi
FOREWORD
3
Antibiotics & Infections
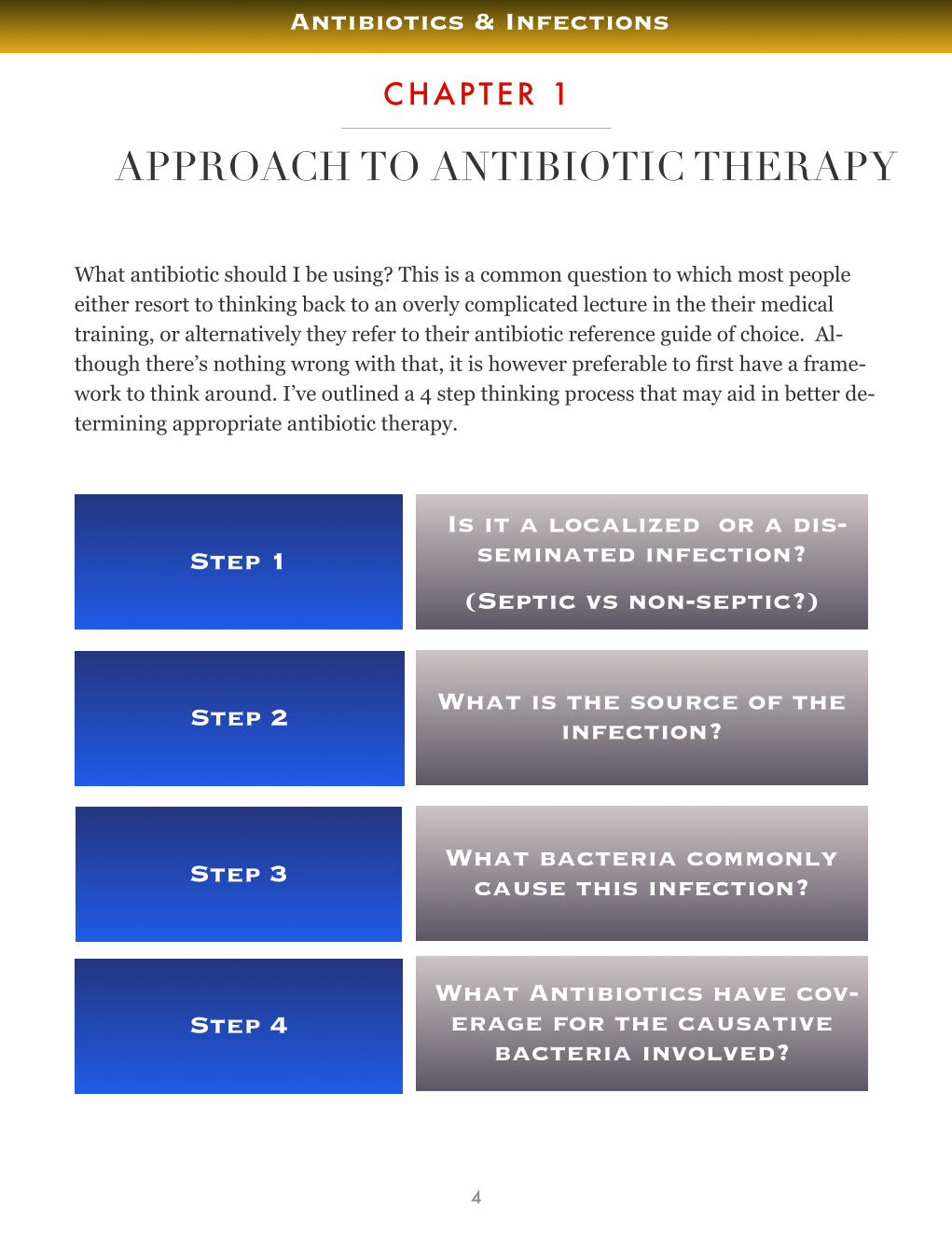
What antibiotic should I be using? This is a common question to which most people either resort to thinking back to an overly complicated lecture in the their medical training, or alternatively they refer to their antibiotic reference guide of choice. Al-though there’s nothing wrong with that, it is however preferable to first have a frame-work to think around. I’ve outlined a 4 step thinking process that may aid in better de-termining appropriate antibiotic therapy.
APPROACH TO ANTIBIOTIC THERAPY
CHAPTER 1
4
Antibiotics & Infections
Step 3
Step 4
Step 2
Step 1Is it a localized or a dis-
seminated infection?
(Septic vs non-septic?)
What is the source of the infection?
What bacteria commonly cause this infection?
What Antibiotics have cov-erage for the causative
bacteria involved?

Step 1: Is it a localized or a disseminated infection (sepsis)?
The first question you need to ask yourself whenever a patient presents with a poten-tial infection is whether it is a localized infection, or a disseminated infection? In other words, is the patient septic or not.
If it is sepsis, then this will mean that the patient will need immediate broad spectrum antibiotic coverage as the initial step, while you investigate the underlying source. It is imperative to note that you should never delay antibiotic therapy in a septic patient.
If possible, you should get cultures before antibiotic therapy is initiated, but do not de-lay antibiotic therapy if cultures are not readily available. A classic example is in men-ingitis patients, where you may want to get an LP, or even a CT head prior to perform-ing an LP, and then starting antibiotics so that you do not affect the yield of your LP culture results. However, in such situations the delay can potentially be in the magni-tude of hours, and may result in adverse outcomes for your patient. Hence, the take home message is do not delay antibiotic therapy.
Evidence Based Medicine
• In septic patients, evidence has shown that antibiotic delay results in an 8% increase in mortality per hour of delay. Early goal directed therapy (antibiotics) has shown im-proved mortality of 30% versus 46% (Rivers trial, 2001)
STEP 1
SECTION 1
5
Antibiotics & Infections

Step 2: What is the source of infection?
Sometimes the source of the infection can be quite obvious, and in other circum-stances, it can be quite challenging.
If it is a localized infection, then you must determine the diagnosis or at least a differ-ential for what localized infections you may be dealing with. Your choice of initial anti-biotics will need to include coverage for the spectrum of possible infections in your dif-ferential diagnosis.
In the situation where you have a septic patient, ideally the appropriate cultures are drawn and antibiotics are started without delay, after which you must determine the source of infection. Often determining the source involves a thorough history & physi-cal examination, as well as clues from your investigations.
Remember to note whether your patient is immunosuppressed or not, since this will determine if you need to expand your differential diagnosis for the source of infection. For example, in an HIV positive patient with a low CD4 count, the differential diagno-sis for the source of infection would be more extensive than in a patient who is not im-munosuppressed.
STEP 2
SECTION 2
6
Antibiotics & Infections

Step 3: What bacteria commonly cause this infection?
Once you’ve determined the likely source (or the likely sources), then the next step is to determine what bacteria are commonly involved in causing such infections.
The method I would recommend is to go through the 4 broad bacterial classifications of potential causative agents for each infection:
Gram Positives
Gram Negatives
Anaerobes
Atypicals
For example, if you determine that you have a patient presenting with urosepsis (or in other words, with a urinary tract infection (UTI) as the source for the sepsis), then you must think to yourself, what gram positives,what gram negatives, what anaerobes, and what atypicals are involved in this infection? You should always ask this question whenever addressing the bacterial causes of an infection. In this case, gram negative bacteria are the predominant underlying agents for a UTI, while the gram positive En-terococcus is also causative agent. Anaerobes and atypicals are not causative agents.
STEP 3
SECTION 3
7
Antibiotics & Infections
1
2
3
4
Once you’ve determined the source of infection and the potential bacterial causative agents, then the next step is to ask yourself what potential antibiotics have coverage for these bacteria. You must ask yourself whether the antibiotic has gram positive, gram negative, anaerobic, and atypical coverage, and then use an antibiotic agent that has coverage for the spectrum of potential bacterial causes.
Furthermore, you should take antibiotic penetrance into consideration. For example, if you have a patient with suspected meningitis, then CNS penetrance of your antibi-otic choices should be taken into account.
Other questions you should ask yourself in choosing an antibiotic is to take into ac-count your local community or hospital’s antibiotic resistance profile. For example, there is significant resistance to ciprofloxacin in certain communities, hence making this a less ideal initial antibiotic choice for certain common infections such as UTIs.
Remember that once you have chosen an initial antibiotic, you should always follow up on the bacterial culture sensitivities (if and when available), and adjust your antibi-otic choice as necessary.
In the previous example for urosepsis, the predominant causative agents for a UTI are gram negatives & gram positives. Therefore, you determine that you will need good gram negative coverage, however you will also require decent gram positive coverage. You decide to initially treat your urosepsis patient with piperacillin-tazobactam. Within 24 hours the urine culture returns showing gram negative rods as the etiology, and within 48 hours you have speciation of the urine culture specimen showing E. coli that is broadly sensitive to most antibiotics. The patient is no longer clinically septic, and you can safely step down the patient to an antibiotic agent with good gram nega-tive coverage such as ceftriaxone or ciprofloxacin.
STEP 4
SECTION 4
8
Antibiotics & Infections
Step 4: What antibiotics have coverage for the causative bacteria?

Step 4: Summary - Choosing an Antibiotic
Does it cover the necessary gram positives, gram negatives, atypicals, & anaerobes involved in the infection in question?
Does it have good tissue penetrance for the infection in question?
Is there resistance to this antibiotic commonly encountered in my community/hospital? (in other words, what is my center’s antibiotic resistance profile?)
9
Antibiotics & Infections
2
1
3

In order to know how to properly use antibiotics as per the 4 step process outlined in Chapter 1, you must first understand the bacteria that commonly cause most infections and how they are classified, into either gram positive, gram negative, atypicals, or anaerobes. These topics will be covered in the following chapter, as well as a brief overview of viruses, protozoa, and helminths.
MICROBIOLOGY BASICSCHAPTER 2
10
Antibiotics & Infections
Bacteria
Viruses
Protozoa
Helminths

SECTION 1
11
Antibiotics & Infections
Gram Positive Bacteria

SECTION 2
12
Antibiotics & Infections
Gram Negative Bacteria
SECTION 3
13
Antibiotics & Infections
Resistant Bacteria
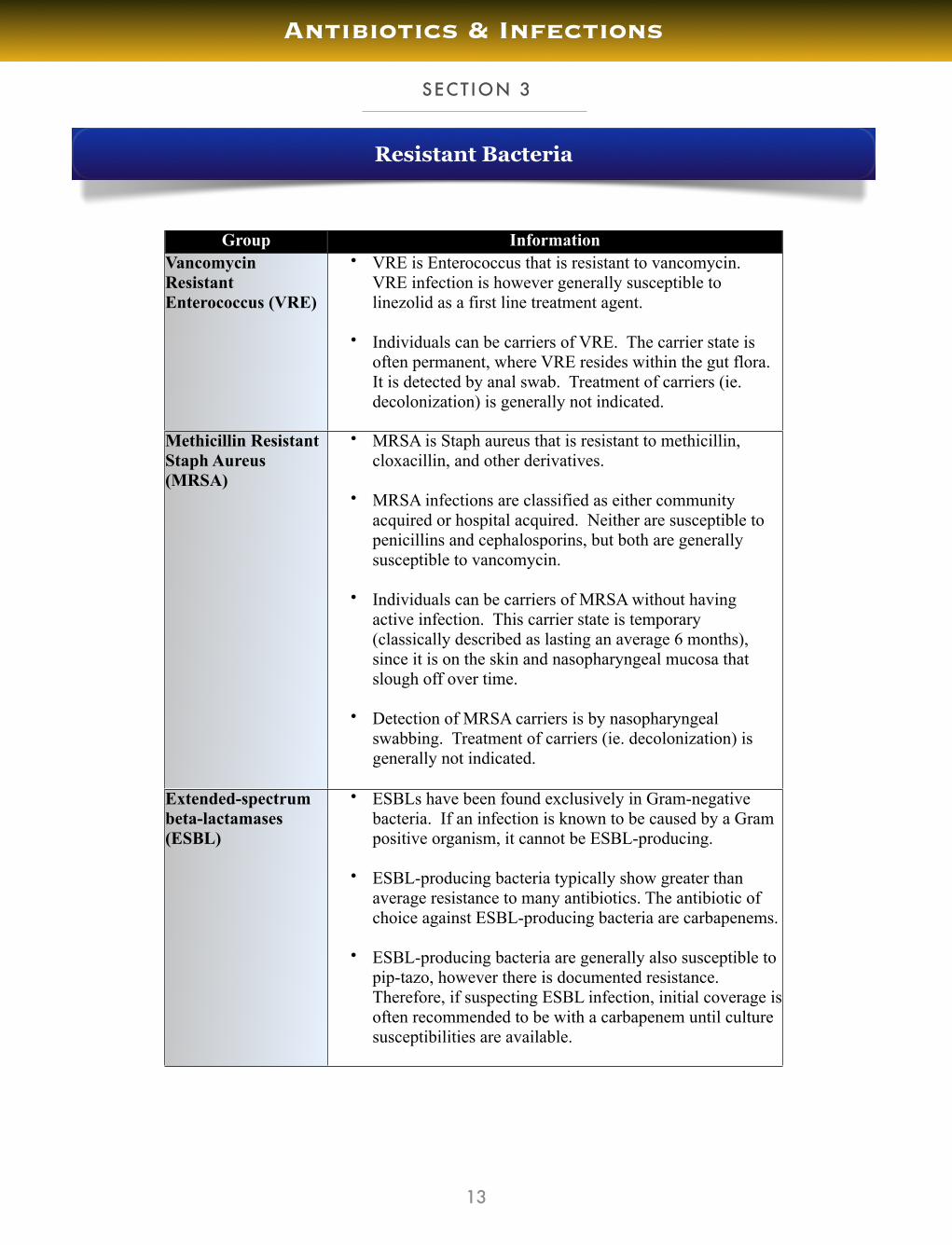
Group InformationVancomycin Resistant Enterococcus (VRE)
• VRE is Enterococcus that is resistant to vancomycin. VRE infection is however generally susceptible to linezolid as a first line treatment agent.
• Individuals can be carriers of VRE. The carrier state is often permanent, where VRE resides within the gut flora. It is detected by anal swab. Treatment of carriers (ie. decolonization) is generally not indicated.
Methicillin Resistant Staph Aureus (MRSA)
• MRSA is Staph aureus that is resistant to methicillin, cloxacillin, and other derivatives.
• MRSA infections are classified as either community acquired or hospital acquired. Neither are susceptible to penicillins and cephalosporins, but both are generally susceptible to vancomycin.
• Individuals can be carriers of MRSA without having active infection. This carrier state is temporary (classically described as lasting an average 6 months), since it is on the skin and nasopharyngeal mucosa that slough off over time.
• Detection of MRSA carriers is by nasopharyngeal swabbing. Treatment of carriers (ie. decolonization) is generally not indicated.
Extended-spectrum beta-lactamases(ESBL)
• ESBLs have been found exclusively in Gram-negative bacteria. If an infection is known to be caused by a Gram positive organism, it cannot be ESBL-producing.
• ESBL-producing bacteria typically show greater than average resistance to many antibiotics. The antibiotic of choice against ESBL-producing bacteria are carbapenems.
• ESBL-producing bacteria are generally also susceptible to pip-tazo, however there is documented resistance. Therefore, if suspecting ESBL infection, initial coverage is often recommended to be with a carbapenem until culture susceptibilities are available.

SECTION 4
14
Antibiotics & Infections
Special Classifications of Bacteria
Summary of OrganismsSummary of OrganismsAtypicals • Chlamydia pneumoniae
(also called Chlamydophila pneumoniae)• Mycoplasma • Legionella
Atypical organisms characteristically cause pneumonia.Atypical pneumonias due to mycoplasma and chlamydophila bacteria usually cause milder forms of pneumonia & often seen in younger patients, unlike other types of pneumonia that present more rapidly and with more severe early symptoms.
Atypical organisms characteristically cause pneumonia.Atypical pneumonias due to mycoplasma and chlamydophila bacteria usually cause milder forms of pneumonia & often seen in younger patients, unlike other types of pneumonia that present more rapidly and with more severe early symptoms.
Anaerobes Above Diaphragm:• Actinomyces• Peptococcus• Peptostreptococcus
Below Diaphragm:• Clostridium • Bacteroides
SPICE organisms(or SPACE)
• Serratia• Pseudomonas• Indole positive proteae
(Morganella, Proteus, & Providencia)• Citrobacter• Enterobacter
For SPICE organisms, resistance during therapy with the agent may occur and lead to clinical failure (classically with cephalosporin therapy). It is therefore recommended that combination antimicrobial therapy (i.e. beta-lactam/beta-lactamase inhibitor plus an aminoglycoside or fluoroquinolone) or a carbapenem alone be used when treating infections with these organisms.
For SPICE organisms, resistance during therapy with the agent may occur and lead to clinical failure (classically with cephalosporin therapy). It is therefore recommended that combination antimicrobial therapy (i.e. beta-lactam/beta-lactamase inhibitor plus an aminoglycoside or fluoroquinolone) or a carbapenem alone be used when treating infections with these organisms.
Encapsulated organisms
• Strep pneumoniae• H. influenzae• Neisseria meningitidis• Klebsiella pneumoniae
An increased risk of infection with encapsulated bacteria is seen in patients with asplenia (ie. splenectomy patients), and therefore need to consider vaccination in such patients to prevent serious infection. Note however that there is no available vaccination for Klebsiella.
An increased risk of infection with encapsulated bacteria is seen in patients with asplenia (ie. splenectomy patients), and therefore need to consider vaccination in such patients to prevent serious infection. Note however that there is no available vaccination for Klebsiella.

SECTION 5
15
Antibiotics & Infections
Viruses – DNA viridae
Viral Family Clinical InformationHepadnavirus • Hepatitis B
Herpesviruses • HSV1 & 2 – oral & genital lesions, encephalitis• VZV – chickenpox, shingles• EBV – mononucleosis, Burkitt’s lymphoma• CMV – infections in immunosuppressed (transplant & HIV)• HHV6 – Roseola• HHV8 – Kaposi’s sarcoma
Adenovirus • Conjunctivitis• Pharyngitis• Pneumonia• Diarrhea
Parvovirus • B19 virus o Arthritiso Aplastic anemiao Fifth disease (erythema infectiosum)o Hydrops fetalis
Polyomavirus(previously called Papovavirus)
• HPV – genital warts, cervical cancer• BK virus - hemorrhagic cystitis and nephropathy in renal
transplant recipients• JC virus – progressive multifocal leukoencephalopathy (PML)
in HIV patients
Poxvirus • Smallpox• Molluscum contagiosum

16
Antibiotics & Infections
Viruses – RNA viridae
Viral Family Clinical InformationRetroviruses • HIV
• HTLV – T cell leukemia
Picornaviruses • Hepatitis A• Coxsakie – myocarditis, meningitis, hand foot
mouth disease, pharyngitis• Polio• Echovirus – meningitis• Rhinovirus – common cold
Flaviviruses • Hepatitis C• Yellow Fever• Dengue• West Nile Virus
Deltaviruses • Hepatitis D
Caliciviruses • Hepatitis E• Norwalk – diarrhea
Reoviruses • Rotavirus - diarrhea• Reovirus – Colorado tick fever
Togaviruses • Rubella• Equine encephalitis
Paramyxoviruses • Measles• Mumps• RSV• Parainfluenza
Orthomyxoviruses • Infleunza (types A and B)
Rhabdoviruses • Rabies
Filoviruses • Ebola
Coronaviruses • Common cold• SARS

SECTION 6
17
Antibiotics & Infections
Protozoa
Organism SymptomsSymptoms Transmission DiagnosisGIGIGIGIGI
Entamoeba histolytica Bloody diarrheaLiver abscess
Cysts in waterCysts in water Serology orStool culture
Giardia lamblia Non-bloody diarrhea Cysts in waterCysts in water Stool culture
Cryptosporidum Non-bloody diarrhea in immunosuppressed
Cysts in waterCysts in water Acid Fast Stain
FEVERFEVERFEVERFEVERFEVERPlasmodium (Malaria):P. vivaxP. ovaleP. malariaeP. falciparum
Fever Female Anopheles Mosquito
Female Anopheles Mosquito
Blood smear (thick and thin smears)
Babesia(Babesiosis)
Fever Ixodes tickIxodes tick Blood smear
Leishmania(Leishmaniasis)
FeverSkin Lesions
Hepatosplenomegaly
SandflySandfly Blood smear
OTHEROTHEROTHEROTHEROTHEROTHERToxoplasma Brain abscess with ring
enhancing lesions in HIVCysts in meat and cat fecesCysts in meat and cat feces
Serology orBiopsy
Trypanosoma cruzi(Chaga’s disease)
Dilated cardiomyopathyDilated esophagus
Megacolon
Reduviid bugReduviid bug Blood smear
Trypanosoma:T. gambienseT. rhodesiense
African sleeping sickness:-Chancre
-Lymphadenitis
Tsetse flyTsetse fly Blood smear
SECTION 7
18
Antibiotics & Infections
Helminths
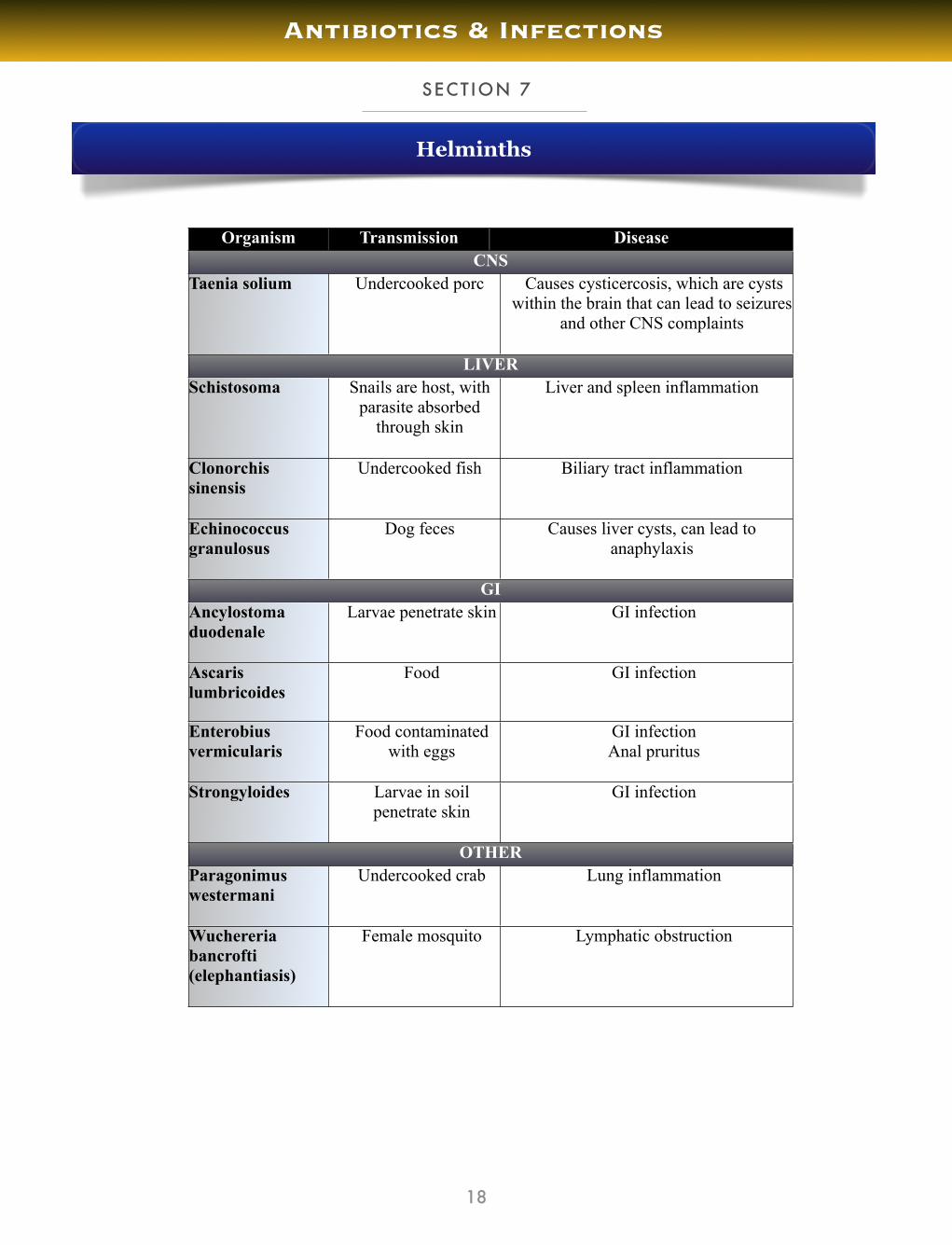
Organism Transmission DiseaseDiseaseCNSCNSCNSCNS
Taenia solium Undercooked porcUndercooked porc Causes cysticercosis, which are cysts within the brain that can lead to seizures
and other CNS complaints
LIVERLIVERLIVERLIVERSchistosoma Snails are host, with
parasite absorbed through skin
Snails are host, with parasite absorbed
through skin
Liver and spleen inflammation
Clonorchis sinensis
Undercooked fishUndercooked fish Biliary tract inflammation
Echinococcus granulosus
Dog feces Dog feces Causes liver cysts, can lead to anaphylaxis
GIGIGIGIAncylostoma duodenale
Larvae penetrate skinLarvae penetrate skin GI infection
Ascaris lumbricoides
FoodFood GI infection
Enterobius vermicularis
Food contaminated with eggs
Food contaminated with eggs
GI infectionAnal pruritus
Strongyloides Larvae in soil penetrate skinLarvae in soil penetrate skin
GI infection
OTHEROTHEROTHEROTHERParagonimus westermani
Undercooked crabUndercooked crab Lung inflammation
Wuchereria bancrofti(elephantiasis)
Female mosquitoFemale mosquito Lymphatic obstruction

The last step in your 4 step approach is choosing the appropriate antibiotic. The fol-lowing pages provide an overview of the major antibiotics and the spectrum of their coverage, which are generally organized under gram positives (GP), gram negatives (GN), anaerobes, and atypicals. There is no easy way around this last step other than simply memorizing the antibiotic coverage. However, I find that the format provided that involves the learning the 4 big categories and the notable exclusions for each cate-gory makes the memorization process somewhat less tedious.
Penicillins
Cephalosporins
Carbapenems
Vancomycin
Linezolid & Macrolides
Aminoglycosides
Fluoroquinolones
Other
ANTIBIOTIC COVERAGE
CHAPTER 3
19
Antibiotics & Infections
Note: In the following pages, the grey boxes incorporated within the various tables indicate important hints & tips for antibiotic coverage

SECTION 1
20
Antibiotics & Infections
PenicillinsPenicillinsPenicillin V (PO)Penicillin G (IV/IM)
• GP except: Staph aureus • Anaerobes except: Bacteroides• Treponema• Pasteurella
Amoxicillin (PO)Ampicillin (IV)
• GP except: Staph aureus• Anaerobes except: Bacteroides• Neisseria meningitides• Pasteurella
MethicillinCloxacillin/DicloxacillinNaficillin/Oxacillin
• GP except: Enterococcus & Listeria • Anaerobes except: Bacteroides
PiperacillinTicarcillin
• GP except: Staph aureus & Enterococcus• GN rods including: Pseudomonas• Anaerobes
Beta-Lactamase InhibitorsBeta-Lactamase InhibitorsClavulin (PO) = Amoxacillin + Clavulanate • GP except E. faecium & MRSA
• GN except Pseudomonas• All anaerobes• No atypical coverage
Timentin (IV) = Ticarcillin + ClavulanateTazocin (IV) = Piperacillin + Tazobactam
• GP except E. faecium & MRSA• GN including Pseudomonas• All anaerobes• Poor atypical coverage
Overall, the Beta-Lactamase inhibitors expand the spectrum of the respective penicillins to include beta-lactamase producing S. aureus, H. influenzae, Neisseria gonorrhoeae, some Enterobacteriaceae, and anaerobes.
Piperacillin-tazobactam, dosed at 3.375 g every six hours, may not be an adequate dose for the treatment of P. aeruginosa infections
Note that the above drugs do not have good coverage for ESBLs, where there has been up to 50% resistance noted in some studies. ESBLs have so far only been seen in Gram Negative bacteria.
Overall, the Beta-Lactamase inhibitors expand the spectrum of the respective penicillins to include beta-lactamase producing S. aureus, H. influenzae, Neisseria gonorrhoeae, some Enterobacteriaceae, and anaerobes.
Piperacillin-tazobactam, dosed at 3.375 g every six hours, may not be an adequate dose for the treatment of P. aeruginosa infections
Note that the above drugs do not have good coverage for ESBLs, where there has been up to 50% resistance noted in some studies. ESBLs have so far only been seen in Gram Negative bacteria.
Penicillins
SECTION 2
21
Antibiotics & Infections
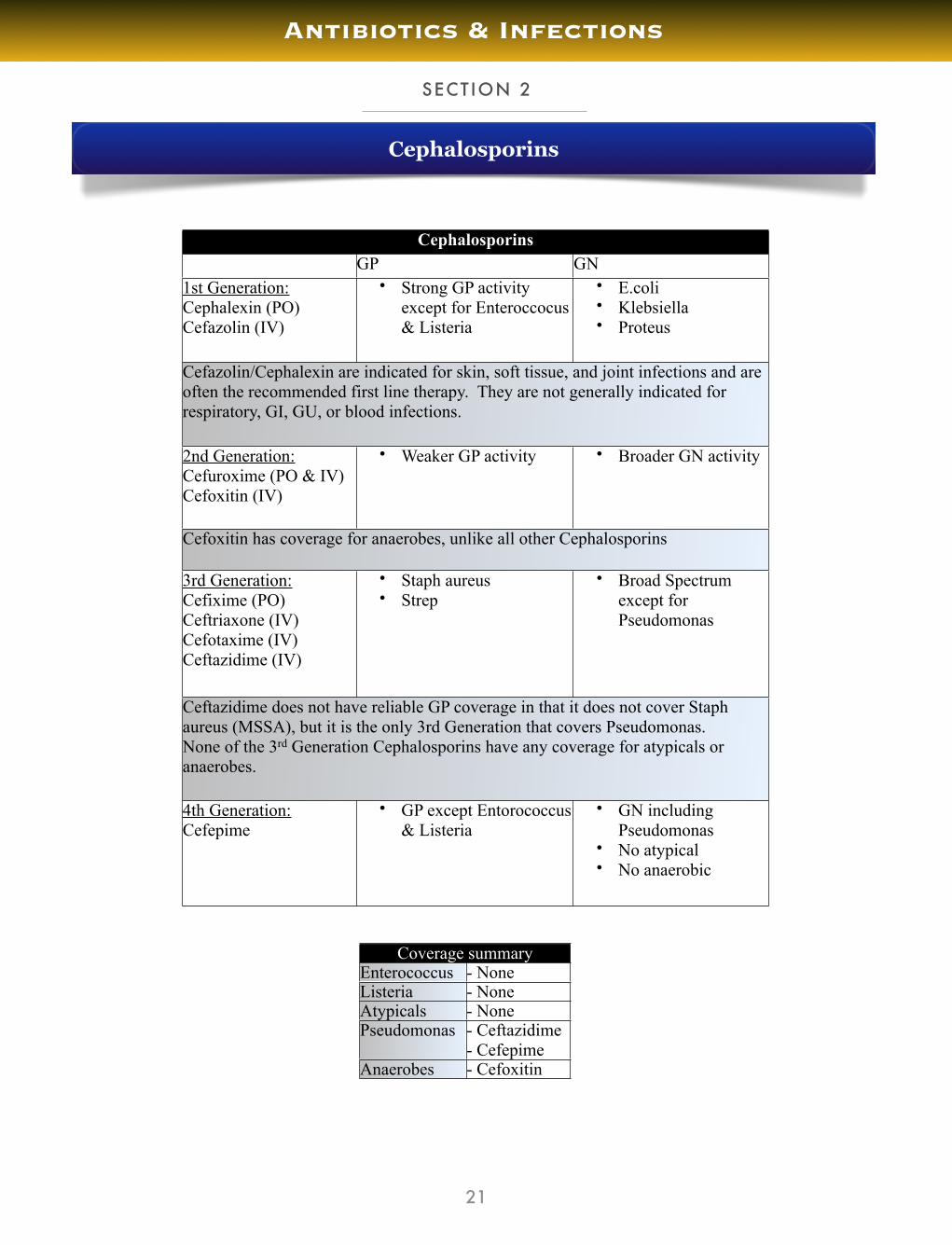
CephalosporinsCephalosporinsCephalosporinsGP GN
1st Generation:Cephalexin (PO)Cefazolin (IV)
• Strong GP activity except for Enteroccocus & Listeria
• E.coli• Klebsiella• Proteus
Cefazolin/Cephalexin are indicated for skin, soft tissue, and joint infections and are often the recommended first line therapy. They are not generally indicated for respiratory, GI, GU, or blood infections.
Cefazolin/Cephalexin are indicated for skin, soft tissue, and joint infections and are often the recommended first line therapy. They are not generally indicated for respiratory, GI, GU, or blood infections.
Cefazolin/Cephalexin are indicated for skin, soft tissue, and joint infections and are often the recommended first line therapy. They are not generally indicated for respiratory, GI, GU, or blood infections.
2nd Generation:Cefuroxime (PO & IV)Cefoxitin (IV)
• Weaker GP activity • Broader GN activity
Cefoxitin has coverage for anaerobes, unlike all other CephalosporinsCefoxitin has coverage for anaerobes, unlike all other CephalosporinsCefoxitin has coverage for anaerobes, unlike all other Cephalosporins
3rd Generation:Cefixime (PO)Ceftriaxone (IV)Cefotaxime (IV)Ceftazidime (IV)
• Staph aureus• Strep
• Broad Spectrum except for Pseudomonas
Ceftazidime does not have reliable GP coverage in that it does not cover Staph aureus (MSSA), but it is the only 3rd Generation that covers Pseudomonas.None of the 3rd Generation Cephalosporins have any coverage for atypicals or anaerobes.
Ceftazidime does not have reliable GP coverage in that it does not cover Staph aureus (MSSA), but it is the only 3rd Generation that covers Pseudomonas.None of the 3rd Generation Cephalosporins have any coverage for atypicals or anaerobes.
Ceftazidime does not have reliable GP coverage in that it does not cover Staph aureus (MSSA), but it is the only 3rd Generation that covers Pseudomonas.None of the 3rd Generation Cephalosporins have any coverage for atypicals or anaerobes.
4th Generation:Cefepime
• GP except Entorococcus & Listeria
• GN including Pseudomonas
• No atypical• No anaerobic
Coverage summaryCoverage summaryEnterococcus - NoneListeria - NoneAtypicals - NonePseudomonas - Ceftazidime
- CefepimeAnaerobes - Cefoxitin
Cephalosporins

SECTION 3
22
Antibiotics & Infections
CarbapenemsCarbapenemsImipenemMeropenem
• GP except Enterococcus faecium & MRSA • GN including Pseudomonas & ESBL• Anaerobes• Poor atypical coverage
Imipenem is believed to have poor CNS penetrationMeropenem is believed to have good CNS penetration.Carbapenems are the drugs of choice if ESBL is suspected
Ertapenem is a Carbapenem that has a narrower spectrum of coverage than the other carbapenems, and in particular does not cover Pseudomonas.
Imipenem is believed to have poor CNS penetrationMeropenem is believed to have good CNS penetration.Carbapenems are the drugs of choice if ESBL is suspected
Ertapenem is a Carbapenem that has a narrower spectrum of coverage than the other carbapenems, and in particular does not cover Pseudomonas.
Carbapenems

SECTION 4
23
Antibiotics & Infections
Vancomycin Overview
Dosing:
• Vancomycin doses of 15 to 20 mg/kg should be administered every twelve hours in pa-tients with normal renal function.
• In patients with renal insufficiency, doses of 15 to 20 mg/kg should be administered less frequently (every 24 to 48 hrs, and not every twelve hours as in patients with nor-mal renal function)
• For rapid achievement of target concentrations in seriously ill patients, a loading dose of 25 to 30 mg/kg may be considered
Monitoring:
• Trough levels of vancomycin must be measured before the 3rd dose of vancomycin ini-tially, to ensure that there is an adequate serum concentration
• Vancomycin trough concentrations of at least 10 mcg/mL should be achieved.
• In the setting of severe or invasive infections (such as endocarditis, osteomyelitis, pros-thetic joint infections and infections involving the central nervous system), many fa-vour vancomycin trough concentrations of 15 to 20 mcg/mL.
Adverse Effect:
• Red Man Syndrome - a histamine-mediated flushing during or immediately following infusion of vancomycin. In the setting of red man syndrome, the rate of infusion may be reduced to 500 mg over 1 hour.
• Note: Vancomycin does NOT cause nephrotoxicity
VancomycinVancomycinVancomycin • GP including MRSA & Enterococcus
• C. difficile
Vancomycin is given IV in all situations except for treatment of C. difficile, in which case only PO vanco is effective.Vancomycin is given IV in all situations except for treatment of C. difficile, in which case only PO vanco is effective.
Vancomycin

SECTION 5
24
Antibiotics & Infections
Protein Synthesis Inhibitors: 50S ribosomeProtein Synthesis Inhibitors: 50S ribosomeMacrolides:ErythromycinClarithromycinAzithromycin
• GP except Enterococcus & MRSA • GN: H. influenzae, Legionella, B.pertussis• Atypicals• Bartonella
Clindamycin • GP except MRSA & Enterococcus• Anaerobes
Linezolid • GP including MRSA & VRE
Macrolides & Linezolid

SECTION 6
25
Antibiotics & Infections
Protein Synthesis Inhibitors: 30S ribosomeProtein Synthesis Inhibitors: 30S ribosomeAminoglycosides:GentamicinNeomycinStreptomycinAmikacinTobramycin
• GN except Neisseria
Tobramycin is the only aminoglycoside that has good coverage for Pseudomonas.Tobramycin is the only aminoglycoside that has good coverage for Pseudomonas.
Tetracyclines:TetracyclineMinocyclineDoxycycline
• GP• Anaerobes• Atypicals: Chlamydia, Mycoplasma, Borrelia, Rickettsia• Treponema
Doxycycline provides malaria prophylaxis.Doxycycline provides malaria prophylaxis.
Aminoglycosides & Tetracyclines
SECTION 7
26
Antibiotics & Infections
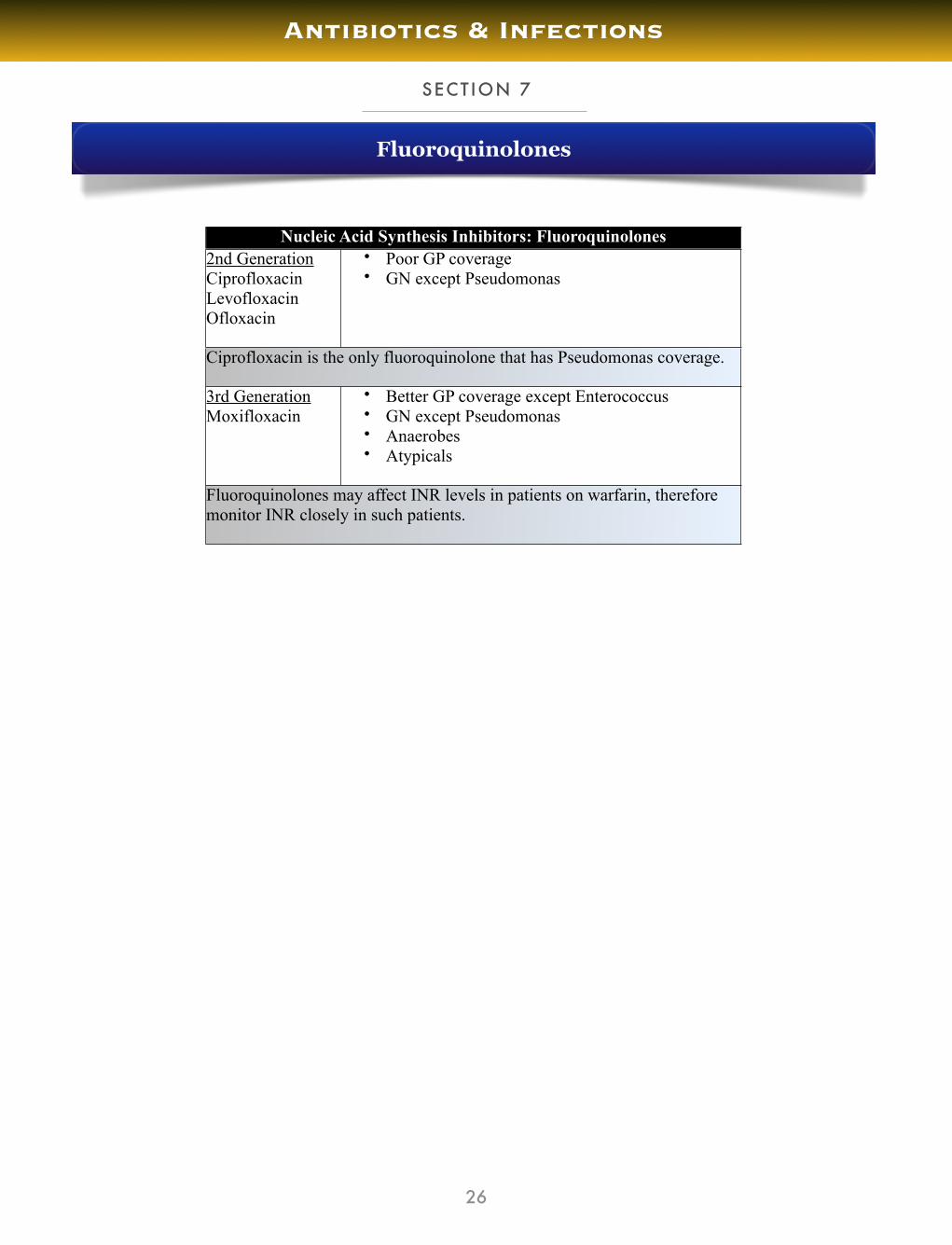
Nucleic Acid Synthesis Inhibitors: FluoroquinolonesNucleic Acid Synthesis Inhibitors: Fluoroquinolones2nd GenerationCiprofloxacinLevofloxacinOfloxacin
• Poor GP coverage• GN except Pseudomonas
Ciprofloxacin is the only fluoroquinolone that has Pseudomonas coverage. Ciprofloxacin is the only fluoroquinolone that has Pseudomonas coverage.
3rd GenerationMoxifloxacin
• Better GP coverage except Enterococcus• GN except Pseudomonas• Anaerobes• Atypicals
Fluoroquinolones may affect INR levels in patients on warfarin, therefore monitor INR closely in such patients. Fluoroquinolones may affect INR levels in patients on warfarin, therefore monitor INR closely in such patients.
Fluoroquinolones

SECTION 8
27
Antibiotics & Infections
Nucleic Acid Synthesis Inhibitors : OthersNucleic Acid Synthesis Inhibitors : OthersMetronidazole(Flagyl)
• Anaerobes• Protozoa
TMP-SMX(Trimethoprim-sulfamethoxizole/ Septra)
• GP• GN enterics• Nocardia• Other: Pneumocystis jiroveci (PCP), Toxoplasma gondii
Nitrofurantoin • GP including Enterococcus• GN coliforms
Rifampin • GP cocci including MRSA• Mycobacteria
Other
General Principles
Antibiotic Synergy
Broad Spectrum Coverage
Illness-Specific Coverage
Bacterial-Specific Coverage
Antibiotics & Infections
CNS Penetrance
IV to PO Conversions
Commonly Missed Sites of Infection
ANTIBIOTIC PRINCIPLES
CHAPTER 4
28
Antibiotics & Infections

SECTION 1
29
Antibiotics & Infections
Broad Spectrum Coverage Patient Population of ChoicePiperacillin + Tazobactam (Pip-Tazo) orTicarcillin + Clavulanate (Timentin)
1st line choice in septic patients where you are not suspecting ESBL
Carbapenem (Imipenem or Meropenem) 1st line choice in septic patients where you are suspecting ESBL
Ciprofloxacin + Metronidazole Option in septic patients who have a penicillin allergy. There are several other potential options in such patients. I recommend consulting your local antibiotic guidelines for further information.
Note that you should add Vancomycin to any of the above regimens for broad spectrum coverage if you are suspecting MRSA infection or Enterococcus faecium.
Note that none of the above regimens provide adequate atypical coverage, therefore if you are suspecting an atypical organism as a cause of infection you should add a macrolide such as clarithromycin or azithromycin.
Note that there is minor cross reactivity between carbapenems and penicillins, hence why some physicians argue against using them in patients with penicillin allergy.
Note that you should add Vancomycin to any of the above regimens for broad spectrum coverage if you are suspecting MRSA infection or Enterococcus faecium.
Note that none of the above regimens provide adequate atypical coverage, therefore if you are suspecting an atypical organism as a cause of infection you should add a macrolide such as clarithromycin or azithromycin.
Note that there is minor cross reactivity between carbapenems and penicillins, hence why some physicians argue against using them in patients with penicillin allergy.
Broad-Spectrum Coverage
SECTION 2
30
Antibiotics & Infections
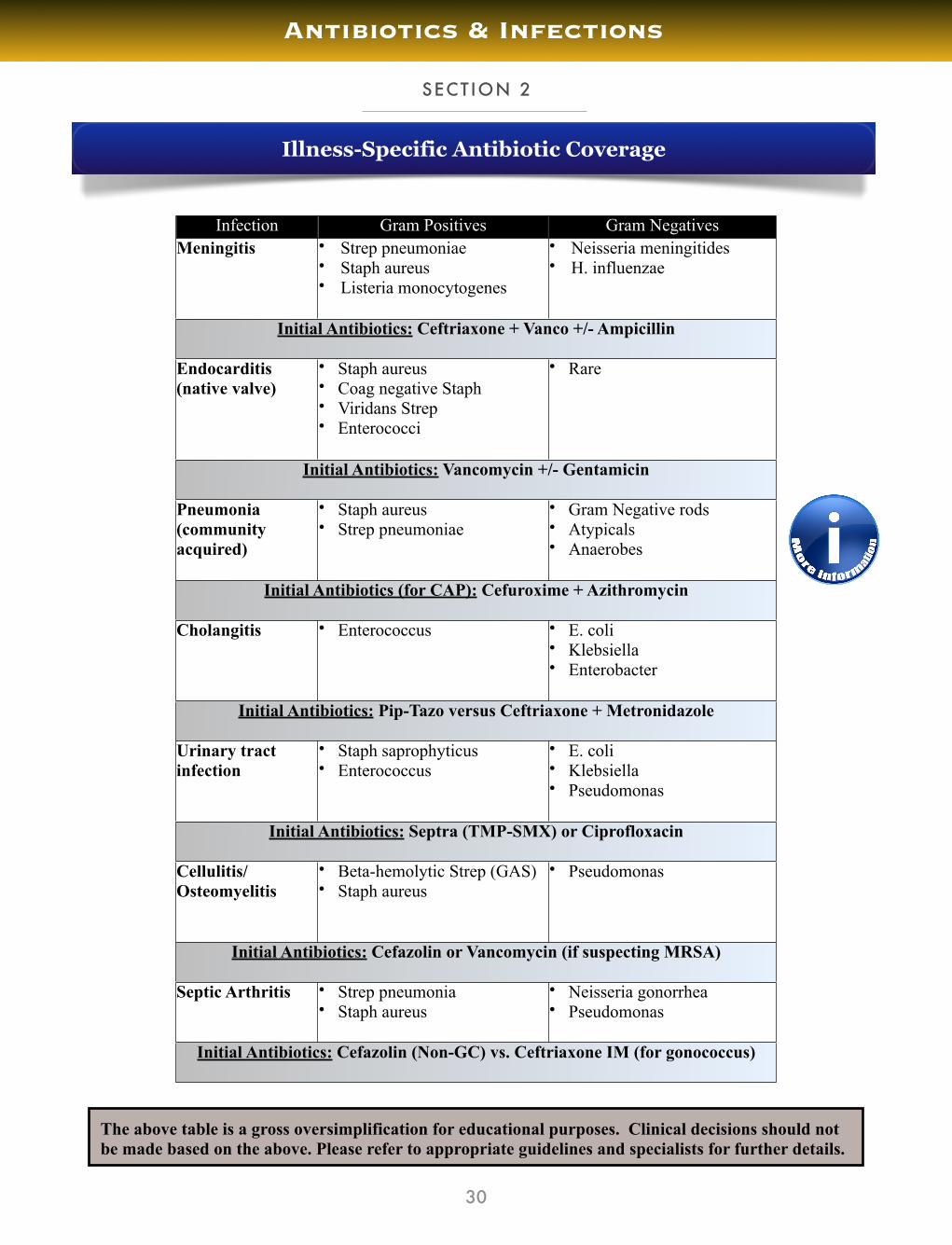
Infection Gram Positives Gram NegativesMeningitis • Strep pneumoniae
• Staph aureus• Listeria monocytogenes
• Neisseria meningitides• H. influenzae
Initial Antibiotics: Ceftriaxone + Vanco +/- AmpicillinInitial Antibiotics: Ceftriaxone + Vanco +/- AmpicillinInitial Antibiotics: Ceftriaxone + Vanco +/- Ampicillin
Endocarditis(native valve)
• Staph aureus• Coag negative Staph• Viridans Strep• Enterococci
• Rare
Initial Antibiotics: Vancomycin +/- GentamicinInitial Antibiotics: Vancomycin +/- GentamicinInitial Antibiotics: Vancomycin +/- Gentamicin
Pneumonia(community acquired)
• Staph aureus• Strep pneumoniae
• Gram Negative rods• Atypicals• Anaerobes
Initial Antibiotics (for CAP): Cefuroxime + AzithromycinInitial Antibiotics (for CAP): Cefuroxime + AzithromycinInitial Antibiotics (for CAP): Cefuroxime + Azithromycin
Cholangitis • Enterococcus • E. coli• Klebsiella• Enterobacter
Initial Antibiotics: Pip-Tazo versus Ceftriaxone + Metronidazole Initial Antibiotics: Pip-Tazo versus Ceftriaxone + Metronidazole Initial Antibiotics: Pip-Tazo versus Ceftriaxone + Metronidazole
Urinary tract infection
• Staph saprophyticus• Enterococcus
• E. coli• Klebsiella• Pseudomonas
Initial Antibiotics: Septra (TMP-SMX) or CiprofloxacinInitial Antibiotics: Septra (TMP-SMX) or CiprofloxacinInitial Antibiotics: Septra (TMP-SMX) or Ciprofloxacin
Cellulitis/Osteomyelitis
• Beta-hemolytic Strep (GAS)• Staph aureus
• Pseudomonas
Initial Antibiotics: Cefazolin or Vancomycin (if suspecting MRSA)Initial Antibiotics: Cefazolin or Vancomycin (if suspecting MRSA)Initial Antibiotics: Cefazolin or Vancomycin (if suspecting MRSA)
Septic Arthritis • Strep pneumonia• Staph aureus
• Neisseria gonorrhea• Pseudomonas
Initial Antibiotics: Cefazolin (Non-GC) vs. Ceftriaxone IM (for gonococcus)Initial Antibiotics: Cefazolin (Non-GC) vs. Ceftriaxone IM (for gonococcus)Initial Antibiotics: Cefazolin (Non-GC) vs. Ceftriaxone IM (for gonococcus)
Illness-Specific Antibiotic Coverage
The above table is a gross oversimplification for educational purposes. Clinical decisions should not be made based on the above. Please refer to appropriate guidelines and specialists for further details.
SECTION 3
31
Antibiotics & Infections
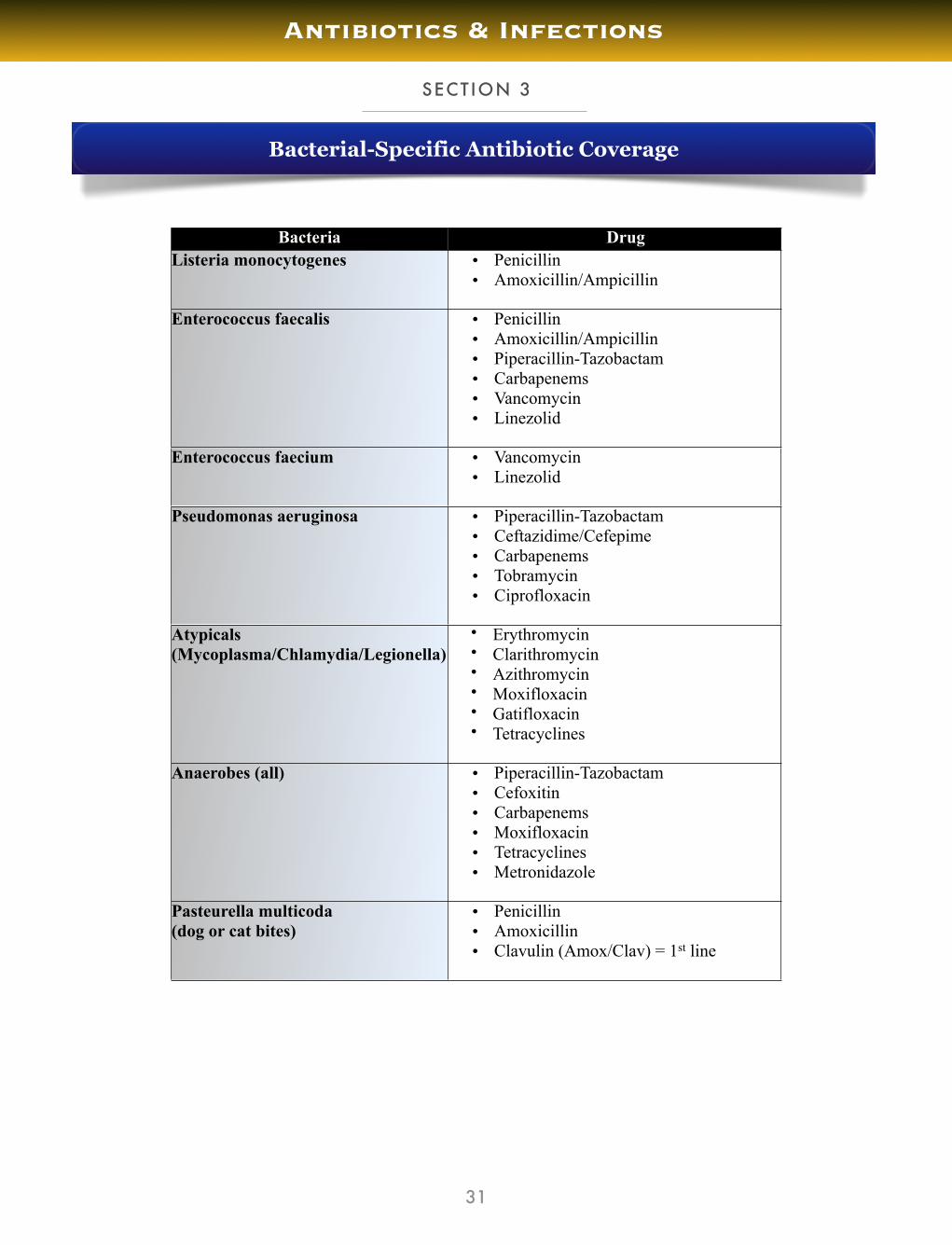
Bacteria DrugListeria monocytogenes � Penicillin
� Amoxicillin/Ampicillin
Enterococcus faecalis � Penicillin� Amoxicillin/Ampicillin � Piperacillin-Tazobactam� Carbapenems� Vancomycin� Linezolid
Enterococcus faecium � Vancomycin� Linezolid
Pseudomonas aeruginosa � Piperacillin-Tazobactam� Ceftazidime/Cefepime� Carbapenems� Tobramycin� Ciprofloxacin
Atypicals(Mycoplasma/Chlamydia/Legionella)
• Erythromycin• Clarithromycin• Azithromycin• Moxifloxacin• Gatifloxacin• Tetracyclines
Anaerobes (all) � Piperacillin-Tazobactam� Cefoxitin� Carbapenems� Moxifloxacin� Tetracyclines� Metronidazole
Pasteurella multicoda(dog or cat bites)
� Penicillin� Amoxicillin� Clavulin (Amox/Clav) = 1st line
Bacterial-Specific Antibiotic Coverage

32
Antibiotics & Infections
Drugs of Choice (if sensitivity)Drugs of Choice (if sensitivity)Bacteria Antibiotic
• Streptococcus • Penicillin
• MSSA • Cloxacillin
• MRSA • Vancomycin
• Enterococcus • Ampicillin
• Listeria • Ampicillin
• Pseudomonas • Ceftazidime or Ciprofloxacin
• Atypicals • Azithromycin or Clarithromycin
• Anaerobes • Metronidazole
Antibiotics of Choice

SECTION 4
33
Antibiotics & Infections
Class Antibiotic UsesPenicillins Penicillin • Meningitis
• Endocarditis• Skin/Soft Tissue
Penicillins
AmpicillinAmoxicillin
• Meningitis• Endocarditis• Intra-abdominal• UTI
Penicillins
Cloxacillin • Endocarditis• Cellulits• Osteomyelitis• Septic Arthritis
Penicillins
Piperacillin-TazobactamTicarcillin-Clavulanate
• Sepsis
Cephalosporins 1st Gen CefazolinCephalexin
• Skin/Soft Tissue• UTI
Cephalosporins
2nd Gen Cefuroxime
• Pneumonia
Cephalosporins
3rd Gen Ceftriaxone
• Meningitis• Pneumonia• UTI
Cephalosporins
4th Gen Cefepime
• Febrile Neutropenia• Severe Sepsis
Carbapenems ImipenemMeropenem
• Sepsis
Glycopeptides Vancomycin • MRSA infections
Antibiotics & Infections
34
Antibiotics & Infections
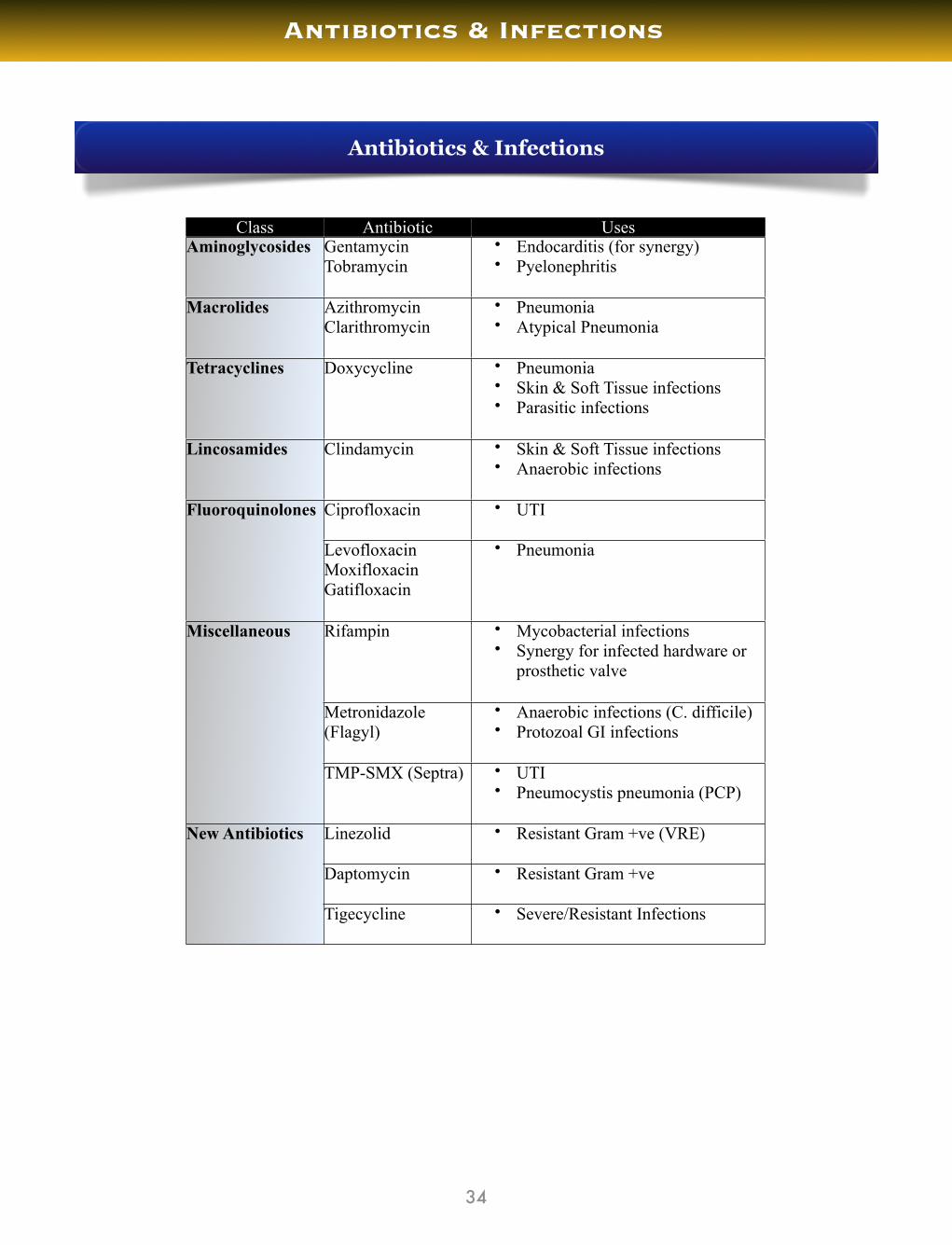
Class Antibiotic UsesAminoglycosides Gentamycin
Tobramycin• Endocarditis (for synergy)• Pyelonephritis
Macrolides AzithromycinClarithromycin
• Pneumonia• Atypical Pneumonia
Tetracyclines Doxycycline • Pneumonia• Skin & Soft Tissue infections• Parasitic infections
Lincosamides Clindamycin • Skin & Soft Tissue infections • Anaerobic infections
Fluoroquinolones Ciprofloxacin • UTIFluoroquinolones
LevofloxacinMoxifloxacinGatifloxacin
• Pneumonia
Miscellaneous Rifampin • Mycobacterial infections• Synergy for infected hardware or
prosthetic valve
Miscellaneous
Metronidazole (Flagyl)
• Anaerobic infections (C. difficile)• Protozoal GI infections
Miscellaneous
TMP-SMX (Septra) • UTI• Pneumocystis pneumonia (PCP)
New Antibiotics Linezolid • Resistant Gram +ve (VRE)New Antibiotics
Daptomycin • Resistant Gram +ve
New Antibiotics
Tigecycline • Severe/Resistant Infections
Antibiotics & Infections

SECTION 5
35
Antibiotics & Infections
Antibiotic Synergy Overview
• This is a phenomenon where two antibiotics, when combined, work in a way that the total effect is greater than the predicted sum of the agents working together. In essence, think of 1+1= 3
• Clinically, synergy is applied for the treatment of Gram Positive infections, most notably for the treatment of infections caused by:
1. Staph aureus2. Viridans Strep3. Enterococcus
• The recipe for the combination of antibiotics in order to achieve synergy is the following:
Penicillins, Cephalosporins, or Vancomycin+
Aminoglycoside (usually Gentamicin)
• The Beta Lactams (Penicillin, Cephalosporin) or the Vancomycin are to be used to give Gram positive coverage for the infection, to which an Aminoglycoside is added for in-creased killing power.
• Now, this may seem counter-intuitive since aminoglycosides do not cover Gram Positive when used alone, but in conjunction with Penicillin, Cephalosporin, or Vancomycin (which work to inhibit cell wall synthesis), it is capable of gaining entry into the bacterial cell and hence has a Gram Positive bactericidal capacity.
• Clinically, synergy is most notably used in endocarditis, where Staph aureus, Viridans Strep, and Enterococcus are common etiologic agents.
Antibiotic Synergy

SECTION 6
36
Antibiotics & Infections
CNS penetranceCNS penetranceGood CNS Penetrance • Ampicillin
• Ceftriaxone• Meropenem• Vancomycin• Doxycycline• Metronidazole
Poor CNS Penetrance • Piperacillin-Tazobactam• Ticarcillin-Clavulanate• Clindamycin
CNS Penetrance

SECTION 7
37
Antibiotics & Infections
IV to PO conversionsIV to PO conversionsIV PO
Ø Pip-Tazo Ø Amox-Clav
Ø Vanco Ø Septra
Ø Cefazolin Ø Cephalexin
Ø Ceftriaxone or Cefotaxime
Ø Cefuroxime
Hints & Tips
• Note that the antibiotic dosages will change when transitioning from IV to PO• Note that Septra can only be used to treat community acquired MRSA, and not hospi-
tal acquired MRSA (due to resistance)
IV to PO Conversions

SECTION 8
38
Antibiotics & Infections
Commonly Missed Sites of Infections
Hints & Tips
• Whenever working up a febrile or septic patient for infection, remember to approach the situational diagnostically from a head to toe anatomic approach.
• If you have screened for common sites of infection without successfully identifying a source, ensure that you have examined for the abovementioned sites of infection.
Commonly Missed Sites of Infection• Sinusitis• Dental abscess• Retropharyngeal abscess• Sternoclavicular joint• Prostatitis• Liver/Abdominal abscess• Diverticular abscess

Csf Analysis
Sputum Culture
Blood Culture
Urine Culture
Ascitic Fluid Analysis
Joint Fluid Analysis
Skin/Wound Culture
Culture Contaminants
FLUID & CULTURE ANALYSIS
CHAPTER 5
39
Antibiotics & Infections

• CSF taken on lumbar puncture (LP) should routinely be sent for:
• Cell count• Culture• Glucose• Protein
• Also, fluid appearance and opening pressure should routinely be assessed on lumbar puncture. Cloudy appear-ance of the fluid suggests infection, as well as high opening pressures can suggest infection.
CSF profiles for the different CNS infections:CSF profiles for the different CNS infections:CSF profiles for the different CNS infections:CSF profiles for the different CNS infections:CSF profiles for the different CNS infections:
Normal Bacterial Viral/Syphilis TB/FungusAppearanceGlucoseProteinCell CountPredominant CellPressure
Clear2.8-4.40.20-0.45< 6Lymphocytes100-200
Normal/ cloudyDecreasedIncreasedIncreasedPMNsMay be high
Normal/cloudyNormalIncreasedIncreasedLymphocytesNormal
CloudyDecreasedIncreasedIncreasedLymphocytesIncreased
Hints & Tips
The take home message from the above table is that the glucose levels are often normal in viral CNS infections (ie. HSV encephalitis), whereas they are decreased in other causes for CNS infections.
SECTION 1
40
Antibiotics & Infections
CSF Analysis

• Sputum culture is routinely performed in patients with a productive cough where there is a query for an underlying pneumonia.
• It is important to note that the quality of the sam-ple needs to be assessed to ensure that it is a true sputum sample. This is done by reviewing the epithelial cell count on the sputum sample.
• Blood cultures, whenever ordered, should be drawn x 2 bottles. This is in the event of a contaminant in one bottle, to be able to compare with the other culture bottle. If one bottle grows an organism whereas the other doesn’t, this suggests a contaminant.
• The most common contaminant growing in a positive blood culture is coagulase negative Staph (Staph epi-dermis), since it grows on skin and hence indicates a likely skin contaminant.
• If there is no growth of bacteria on blood cultures within 48 hours, then it is generally considered safe to con-clude that it is a negative blood culture for most organisms.
• Urinalysis is a quick method to screen for possible un-derlying UTI. A positive leukocyte esterase and/or posi-tive nitrites on urinalysis (U/A) suggests UTI.
• Nitrites being positive on urinalysis suggests Enterobac-teriaceae as the causative organism for UTI, which are mainly one of the following oxidase negative gram negative bacilli: E Coli,Klebsiella, Proteus.
SECTION 2
41
Antibiotics & Infections
Sputum Cultures
Urinalysis & Urine Cultures
Blood Cultures
Is it a true sputum sample? < 25 epithelial cells = true sputum culture > 25 epithelial cells = saliva
Nitrites Positive on U/A means:
• E. coli• Klebsiella• Proteus

• In patients with a history of cirrhosis and ascites who present with abdominal pain, peritoneal fluid should be col-lected through paracentesis to assess for any underlying sponteanous bacterial peritonities (SBP).
• The appearance of the ascitic fluid should be noted:
• Clear = normal uncomplicated ascites• Cloudy = suggestive of SBP• Bloody = suggestive of malignancy vs traumatic tap
• Routine tests for ascitic fluid:
• Albumin - to calculate SAAG• Cell count - to look for SBP• Culture - to look for SBP
• Other tests for ascitic fluid (not routine):
• Glucose - often low in SBP• Protein - high risk of SBP if protein <1g/L • LDH - ascites to serum LDH ratio >1 suggest SBP
SECTION 3
42
Antibiotics & Infections
SBP Diagnosis
• Cloudy ascitic fluid appearance is suggestive of SBP
• PMN count > 250 cells/mm3 on paracentesis is diagnostic of SBP
Ascitic Fluid Analysis
SAAG
• SAAG = Serum albumin - Ascites albumin
• SAAG > 11 = ascites from portal hypertension
• SAAG < 11 = ascites not from portal hypertension

Send joint aspiration fluid for:
o Cell counto Gram stain & culture
Cell Count Interpretation
• A synovial fluid leukocyte count <2000/µL and neutrophils <50% is negative for infection
• A synovial fluid leukocyte count above 2000/µL indicates inflammation
• A synovial fluid leukocyte count > 50,000/µL with predominant neutrophils (>50%) suggests infec-tion
• If no polymorphs are present on a skin or wound culture despite a positive culture result, then the positive result is likely a contaminant. Polymorphs indicate the body’s immune response to an infection. If they are absent from a wound culture in particular, you should question whether the organisms growing on the culture are simply contaminants.
SECTION 4
43
Antibiotics & Infections
Joint Fluid Analysis
Skin & Wound Cultures
Septic Arthritis Workup
• Joint fluid WBC > 50,000/µL suggests infection
Note that gram stain can be negative in certain patients with septic arthritis. Therefore, in patients with clinical suspicion of infection, treat with antibiotics until synovial fluid culture results are available

SECTION 5
44
Antibiotics & Infections
Culture Contaminants
Consider Contaminant if...Consider Contaminant if...
Sputum Culture >25 epithelial cells
Blood CultureOnly 1 of 2 culture bottles positive, especially if
coagulase negative Staph
UrinalysisNegative Leukocyte Esterase
Negative Nitrites
Wound Culture Negative polymorphs (PMNs)