animal growth and development – 1...
TRANSCRIPT
4/6/2009
1
Animal growth and development – 1st review
Animal Science 123Animal Growth & Development
R. D. SainzLecture 09
Growth curves Growth curves
300
400
500
wt,
kg
0
100
200
0 5 10 15 20 25 30 35
Age, months
Bod
y w
Allometric growthAllometric growth
60
80
100
, kg
Muscle
Fat
0
20
40
0 50 100 150 200 250 300
Carcass wt, kg
Wt,
Bone

4/6/2009
2
SummarySummary
• Growth cannot be simply an increase in size, but must instead be accompanied by development
• Development includes increasing complexity, d h i f d f tiand changes in form and function
• Allometric growth means that different body components grow at different rates and times
SizeSize
• Weight*
• Length
• Height
CompositionCompositionThe main chemical components of the body
are water, fat, protein and ash:
Lean animal5%
Fat animal3%
60%15%
20%
45%
37%
15%
Water
Fat
Protein
Ash

4/6/2009
3
Measuring body compositionMeasuring body composition
• Direct– Kill, grind, sub-sample and analyze
• Indirect methods (in vivo)– Non-invasive (varying degrees)– Non-destructive
External measurements:– Weight– Height
Measuring body compositionMeasuring body composition
– Body mass index = W/H2 (kg/m2)– Subcutaneous fat» Skinfold thickness» Ultrasound» CAT scans
• Example: assume lean and fat animals, both weighing 100 kg;– Inject 10 mL of D2O– Allow to equilibrate– Sample body fluid
• Body water (L) = Dose (mL) / Concentration (mL/L)
• Body water % = 100 x body water (L) / body wt (kg)y y ( ) y ( g)
• Then: use previously determined ratios of water:protein:ash, e.g. 12:4:1, so that
• Body protein % = body water % ÷ 3
• Body fat % = 100 – [body water % * (12+4+1)/12]

4/6/2009
4
More methodologiesMore methodologies• Cellular
– Cell culture– Primary vs cell lines
• Hormonal– Bioassays– Radioimmunoassays (RIA)– Enzyme-linked immunosorbent assays
(ELISA)– Ligand binding studies (receptors)
General principles• Endocrine: hormone is produced in a specific gland,
secreted into circulation, and exerts specific actions on remote target cells;SOURCE REMOTE FROM TARGET
• Paracrine: hormone is produced by some tissue cells, a ac e o o e s p oduced by so e ssue ce s,and diffuse through the extracellular space to exert specific actions on nearby target cells;SOURCE NEAR TARGET
• Autocrine: hormone is produced by cells and exerts its actions on the same cells;SOURCE = TARGET
From: LeRoith et al., 2001

4/6/2009
5
• Indirect effects of GH are mediated by IGF-I
• Most of the IGF-I in circulation is produced by the liver, in response to GH stimulation
Growth hormone & IGF-I
y , p• Responsiveness to GH is regulated by
nutrition (insulin) and also by sex steroids• Whole-body growth is sensitive to GH and
IGF-I, therefore to GH and responsiveness (receptor number, affinities) to GH
3% of BW
3% of BW
3% of BW
3% of BW
1.8% of BW
3% of BW
3% of BW
1% of BW
3% of BW3% of BW(10 days)
From: Breier, BH, Bass, JJ, Butler, JH and Gluckman, PD. 1986. The somatotrophic axis in young steers: influence of nutritional status on pulsatilerelease of growth hormone and circulating concentrations of insulin-like growth factor 1. J. Endocr. 111, 209-215.
Hormone action involves several steps1. hormone binds to specific receptors,2. binding alters the conformation of the receptor,3. post-receptor signaling events
a) membrane receptors – for non-permeable hormones; peptides, catecholamines • 2nd messengers (including cAMP, Ca2+, Tyr-PO4, etc.)
mediate actions• receptor cycling (membrane ↔ cytosol)
b) cytosolic receptors – for membrane-permeable hormones; lipid-soluble, steroids internalization of the hormone-receptor complex• transfer into nucleus, produce direct effects on gene
expression

4/6/2009
6
Insulin receptor: Tyrosine Insulin receptor: Tyrosine kinase activationkinase activation
From: Saltiel, 2003 NEJM 349:26
Insulin receptor: Tyrosine Insulin receptor: Tyrosine kinase activationkinase activation
From: Saltiel, 2003 NEJM 349:26
From: Herrington & Carter-Su, 2001. TIEM 12:252.

4/6/2009
7
From: Herrington & Carter-Su, 2001. TIEM 12:252.
From: Herrington & Carter-Su, 2001. TIEM 12:252.
From: LeRoith & Nissley, 2005. J. Clin. Invest. 115:233.
4/6/2009
8
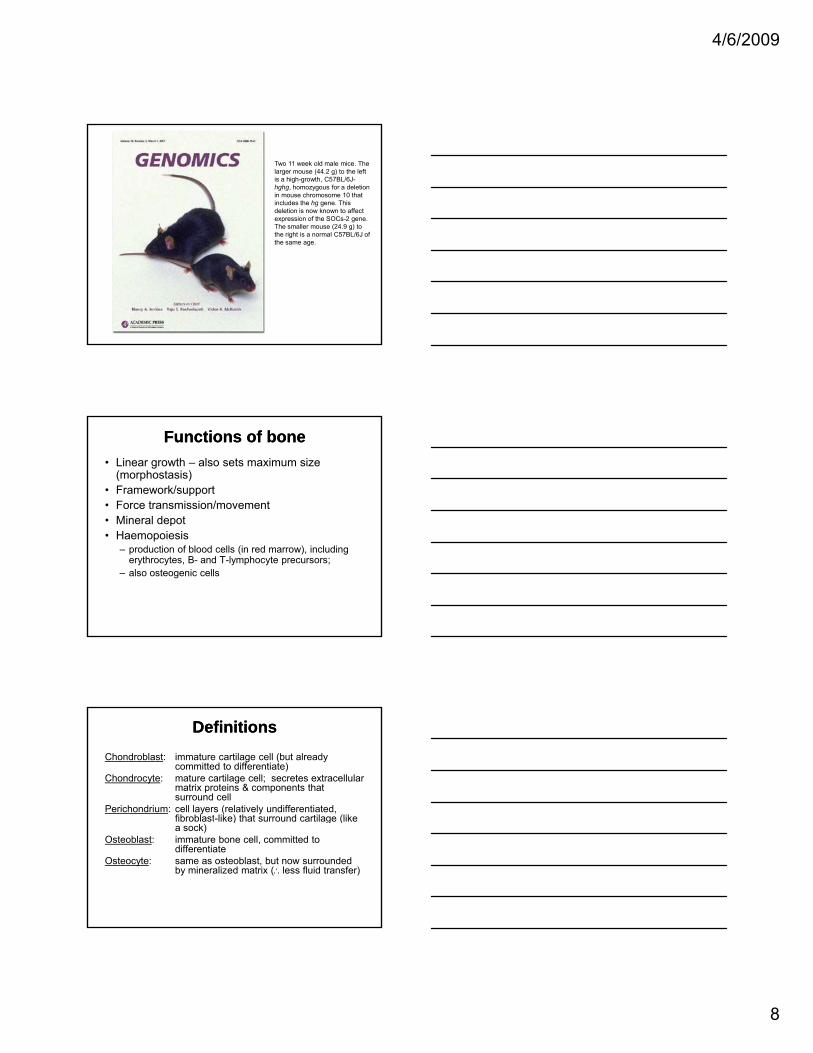
Two 11 week old male mice. The larger mouse (44.2 g) to the left is a high-growth, C57BL/6J-hghg, homozygous for a deletion in mouse chromosome 10 that includes the hg gene. This deletion is now known to affect expression of the SOCs-2 gene. The smaller mouse (24.9 g) to the right is a normal C57BL/6J ofthe right is a normal C57BL/6J of the same age.
Functions of boneFunctions of bone• Linear growth – also sets maximum size
(morphostasis)• Framework/support• Force transmission/movement• Mineral depotp• Haemopoiesis
– production of blood cells (in red marrow), including erythrocytes, B- and T-lymphocyte precursors;
– also osteogenic cells
DefinitionsDefinitionsChondroblast: immature cartilage cell (but already
committed to differentiate)Chondrocyte: mature cartilage cell; secretes extracellular
matrix proteins & components that surround cell
Perichondrium: cell layers (relatively undifferentiated, fibroblast like) that surround cartilage (likefibroblast-like) that surround cartilage (like a sock)
Osteoblast: immature bone cell, committed to differentiate
Osteocyte: same as osteoblast, but now surrounded by mineralized matrix (∴less fluid transfer)

4/6/2009
9
DefinitionsDefinitions
Osteoid: bone matrix, same as cartilage but type I collagen instead of type II; framework that can be impregnated by mineral crystals
Periosteum: relatively undifferentiated (fibroblast-like) cell layers that surround bone
DefinitionsDefinitionsPhysis: growth plate; also known as the
epiphyseal growth plate; region in which longitudinal growth of long bones occurs
Epiphysis: ends of long bonesDiaphysis: portion of long bone in between proximal
and distal metaphysesM t h i f t f ti f til i tMetaphysis: zone of transformation of cartilage into
bone, between the physis and diaphysis; area of bone resorption, ossification and calcification
From: Frandson, R. D. 1986. Anatomy and Physiology of Farm Animals. Lea & Febiger, Philadephia.

4/6/2009
10
Bone FormationBone Formation
• All bones form from a cartilage model, which first becomes ossified, and finally calcified.
• Ossification: production of osteoid (bone p (matrix) by osteoblasts and osteocytes
• Calcification: mineralization of the osteoid by deposition of hydroxyapatite crystals
Two types of developmentTwo types of development
• Endochondral: most common, occurring in long bones; osteogenesis takes place within a cartilage model (anlage) that forms in the developing limb budforms in the developing limb bud
• Intramembranous: osteogenesis occurs within a membrane, no cartilage model; flat bones (e.g., skull, pelvis, scapula)
Big picture of developmentBig picture of development
1. During embryonic development, shortly after the appearance of the notochord, clusters of differentiated cells appear in pairs along the dorsal streak; these clumps are called somites;
2. Within each somite, cells begin differentiating into distinct types, destined to become myogenic (muscle-forming) or chondrogenic (bone-forming)

4/6/2009
11
From: Gerrard, DE & Grant, AL 2003. Principles of Animal Growth & Development. Kendall/Hunt Pub. Co., Dubuque, IA
From: Frandson, RD. 1986. Anatomy and Physiology of Farm Animals. Lea & Febiger, Philadelphia.

4/6/2009
12
Three zones are present in the growth Three zones are present in the growth plateplate
• The resting zone contains inactive chondroblasts that can be recruited to divide;
• The proliferating zone contains actively dividing chondroblasts, forming columns of cells by clonal expansion;
• The hypertrophic (maturing) zone contains live chondrocytes that secrete matrix which is being calcified.
• Interval between closure of 1st and last growth plates– ≈ 5-6 years (human)– 3 years (rat)– >3.5 years (sheep)
• Generation time for GP cell division2 3 d ( t) 20 d (h )– ≈ 2.3 d (rat) vs. 20 d (human)
• SO:– no general rules about proximal vs. distal;– no single event causes GP closure (local regulation +
systemic factors)
From: Ham, AW & Cormack, DH. 1987. Ham’s Histology. Lippincott, Philadelphia.
4/6/2009
13
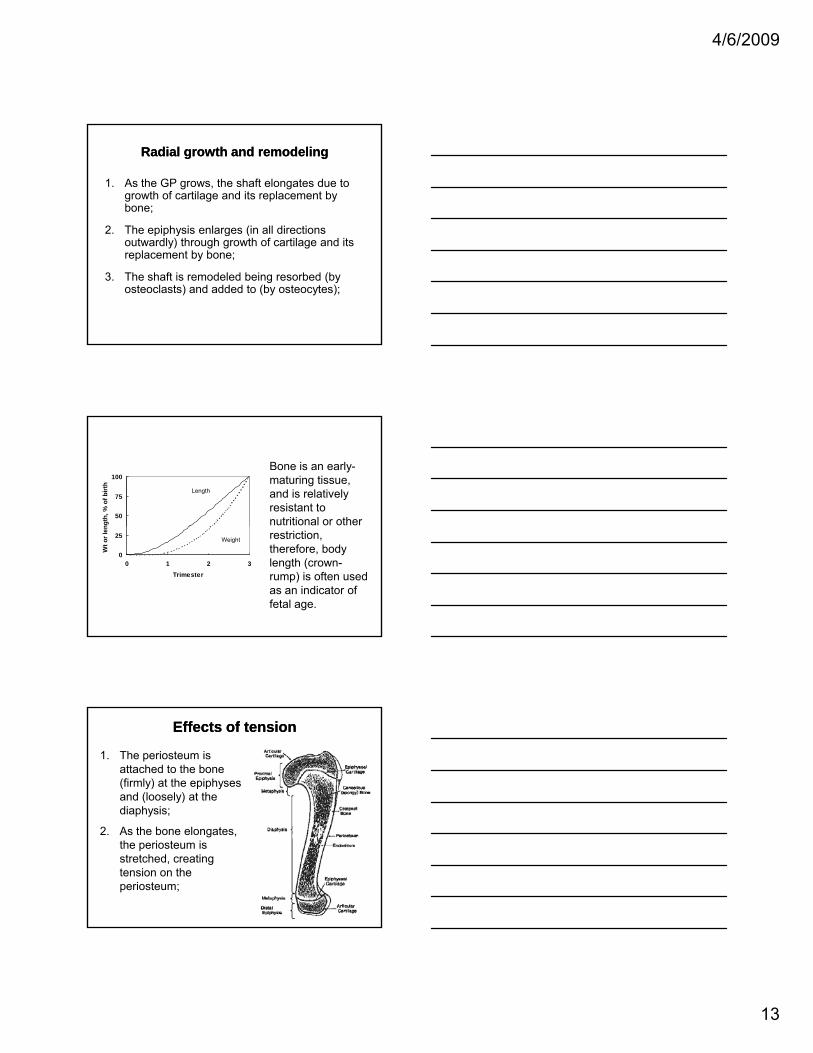
Radial growth and remodelingRadial growth and remodeling
1. As the GP grows, the shaft elongates due to growth of cartilage and its replacement by bone;
2. The epiphysis enlarges (in all directions p p y g (outwardly) through growth of cartilage and its replacement by bone;
3. The shaft is remodeled being resorbed (by osteoclasts) and added to (by osteocytes);
50
75
100
ngth
, % o
f birt
h
Length
Bone is an early-maturing tissue, and is relatively resistant to nutritional or other
0
25
0 1 2 3Trimester
Wt o
r len
Weight restriction, therefore, body length (crown-rump) is often used as an indicator of fetal age.
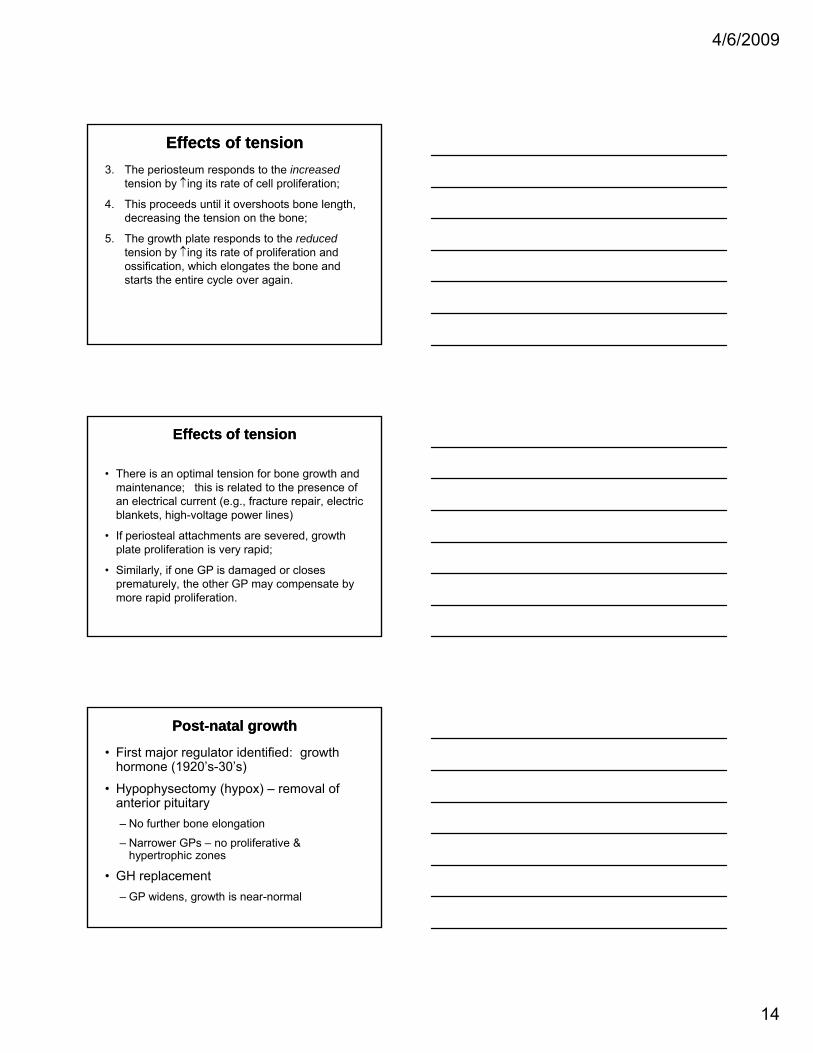
Effects of tensionEffects of tension
1. The periosteum is attached to the bone (firmly) at the epiphyses and (loosely) at the diaphysis;
2. As the bone elongates, the periosteum is stretched, creating tension on the periosteum;
4/6/2009
14
Effects of tensionEffects of tension3. The periosteum responds to the increased
tension by ↑ing its rate of cell proliferation;
4. This proceeds until it overshoots bone length, decreasing the tension on the bone;
5 Th th l t d t th d d5. The growth plate responds to the reducedtension by ↑ing its rate of proliferation and ossification, which elongates the bone and starts the entire cycle over again.
• There is an optimal tension for bone growth and maintenance; this is related to the presence of an electrical current (e.g., fracture repair, electric blankets, high-voltage power lines)
Effects of tensionEffects of tension
• If periosteal attachments are severed, growth plate proliferation is very rapid;
• Similarly, if one GP is damaged or closes prematurely, the other GP may compensate by more rapid proliferation.
• First major regulator identified: growth hormone (1920’s-30’s)
• Hypophysectomy (hypox) – removal of anterior pituitary
PostPost--natal growthnatal growth
– No further bone elongation
– Narrower GPs – no proliferative & hypertrophic zones
• GH replacement– GP widens, growth is near-normal

4/6/2009
15
Sex steroidsSex steroids
• Mainly estrogen and testosterone
• Can stimulate bone growth (e.g., puberty) or stop itstop it
• Lack of estrogen is involved in the post-menopausal onset of osteoporosis
Estrogen Estrogen • ERα and ERβ both present in GP• Inhibit cartilage growth and enhance maturation
of the GP;• Low levels stimulate osteoblasts indirectly (via ↑
IGF-I)
• High levels (e.g., at puberty) inhibit growth:↓ cartilage growth
↑maturation of the GP
• Inhibit bone resorption by osteoclasts
Growth factor Osteoblast OsteoclastDNA Collagen resorption
Insulin-like growth factor-I (IGF-I) + + -IGF-II + +Prostaglandins + + +Epidermal growth factor (EGF) + - +Transforming growth factor-α (TGFα) +TGF-β1 + - +Platelet-derived growth factor (PDGF) + + +Fibroblast growth factor (FGF α, β) ++ -Interleukin-1 (IL-1 α, β) + + +Tumor necrosis factor (TNF) -Interferon-γ - - -Bone morphogenetic protein (BMP) + +

4/6/2009
16
Regulation of calcium and phosphorusRegulation of calcium and phosphorus
• All tissues/cells require precise concentrations of Ca2+ for proper function
• Circulating Ca2+ exchanges with tissue pools and the storage pool in bone
• 99% of body calcium (ca. 1 kg) is in the mineralized bone
From: Murray, RK, Mayes, PA, Granner, DK, and Rodwell, VW. 1990. Harper’s Biochemistry. Appleton & Lange, San Mateo, CA.
Parathyroid hormone (PTH)Parathyroid hormone (PTH)• Principal role = maintenance of plasma calcium
concentration• Released by the parathyroid gland in response to low
plasma [Ca2+]; undergoes further processing in the liver• Raises plasma Ca2+ by stimulation of:
– bone resorption by osteoclastsy– renal tubule reabsorption of calcium– 1-25-(OH)2D3 production → increased intestinal Ca2+ absorption,
bone resorption
• Lowers plasma P by stimulation of renal excretion, thus preventing harmful CaPO4 precipitates in tissues
• PTH may be anabolic or catabolic, depending upon its interactions with other hormones and health/disease state

4/6/2009
17
Vitamin D (calcitriol)Vitamin D (calcitriol)• Nutrient and hormone• Maintains normal plasma calcium
↑ resorption of bone by osteoclasts↑ intestinal absorption of Ca and P↑ l t ti f PO↑ renal retention of PO4
• Direct effects on osteoblasts↑collagen synthesis↓ osteocalcin synthesis↑ IGF-I synthesis? osteoblast proliferation
CalcitoninCalcitonin
• Produced in the C cells of the thyroid gland
• Released in response to elevated plasma [Ca2+]
• Increases renal Ca excretionIncreases renal Ca excretion
• Decreases bone resorption (direct effects on osteoclasts)