anatomical variants of ct pns
DESCRIPTION
ANATOMICAL VARIANTS OF CT PNSTRANSCRIPT

ANATOMIC VARIANTS CT-
PNS-To highlight the clinically relevant
sinonasal anatomy and variants
Susritha.kDpt of ENTASRAMS.
The significance of anatomic variants is determined by its relationship with the osteomeatal channels and nasal air passages.
The ability of the variation to obstruct the air passages implies a role in recurrence of sinusitis.

The nasal turbinates are embryologically derived from a series of outgrowths from the foetal lateral nasal wall.
The outgrowths form a series of ridges, referred to as “ethmoturbinals” which are separated by furrows.
Each ridge has an anterior ascending portion and a posterior descending portion.
The uncinate process develops from the descending portion of the first ridge, which is also known as the “nasoturbinal”
The agger nasi develop from its ascending portion.
The second ridge forms the bulla lamella, or the bulla ethmoidalis when pneumatized.
The middle turbinate develops from the third ridge, which is the first permanent ethmoturbinal.
The fourth ridge, the second permanent ethmoturbinal, forms the superior turbinate.
Based upon this, variations in development and pneumatization of the ethmoturbinals may lead to anatomical variations within the bony structures of the ethmoidal complex.

The Agger Nasi Air Cell :
Its an ethmoturbinal remnant present in nearly all patients.
The ANC is the most constant and anterior of the ethmoidal air cells.
Located anterior to the vertical attachment of the middle turbinate to the skull base.


The degree of ANC pneumatization varies and has a significant effect on both the size of the frontal sinus ostium and the shape of the recess.
If the ANC is small, then the “beak” of the frontal process of the maxilla, lying anteriorly and superiorly, will be prominent and extend posteriorly into the frontal recess, resulting in a narrow ostium.
If the ANC is large, the beak will be small, resulting in a wider ostium but potentially causing obstruction more inferiorly.

Fronto-ethmoid/kunh cells/bulla frontalis
Are the anterior ethmoid cells which invade the frontal bone, bulging its floor
They are more easily demonstrated at saggital view, where they appear as ethmoid air cells located above the ethmoid bulla and as an extension towards the frontal sinus.
Depending on their size and pneumatization extent, such cells may affect the frontal sinus drainage.
These air cells, are categorized into four types depending on their number and degree of extension into the frontal sinus.
They are all located superior to the ANC.

Type 1 (most common): Single cell superior to the ANC that does not extend into the frontal sinus
Type 2: Two or more cells superior to the ANC that may or may not extend into the frontal sinus.
Type 3: Single frontal cell superior to the ANC that extends into the frontal sinus.
Type 4: Completely contained in the frontal sinus. This configuration is rare.


Sphenoethmoid cell (Onodi cell) :
This is formed by lateral and posterior pneumatization of the most posterior ethmoid cells over the sphenoid sinus.
The presence of Onodi cells increases the chance that the optic nerve and / or carotid artery would be exposed in the pneumatized cell.
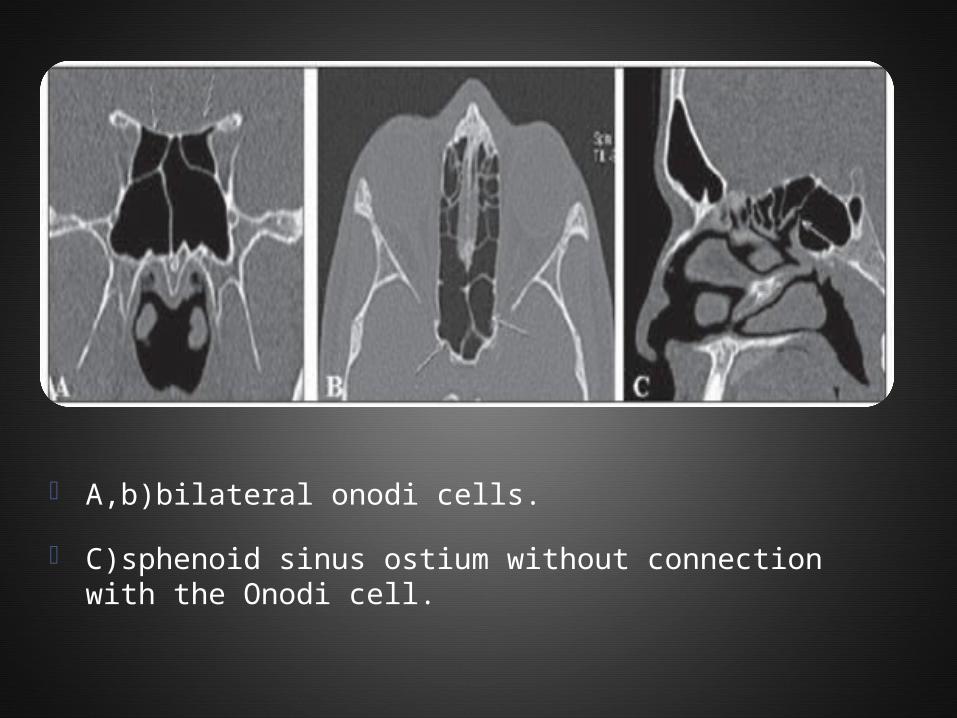
A,b)bilateral onodi cells.
C)sphenoid sinus ostium without connection with the Onodi cell.

ONODI CELL

Delano,fun zinreich classification
Relation b/w posterior group of sinuses with optic nerve
Type1: optic nerve adjacent to sphenoid sinus.
Type2: optic nerve indentation on sphenoid sinus.
Type3: optic nerve traversing through sphenoid sinus.
Type4: optic nerve adjacent to sphenoid & post. Eth. Sinus.
Uncinate process
The uncinate process is a superior extension of the lateral nasal wall that is anatomically relevant for draining the frontal recess.
Variations such as hypertrophy, deviation and pneumatization may affect the drainage, generating abnormalities in the osteomeatal complex.

A)horizontal uncinate
b)hypertrophy of lt uncinate.
C)pneumatisation of lt uncinate.
D)vertical lt uncinate.

Table showing types of OMC abnormalities

Variations in the superior insertion of the uncinate process are classified according to criteria developed by Landsber & Friedman
A: Type 1 (insertion into the lamina papyracea).
B: Type 2 (insertion into the posterior wall of agger nasi cell).
C: Type 3 (insertion into the lamina papyracea and junction of the middle turbinate with the cribriform plate).
D: Type 4 (insertion in to junction of the middle turbinate with the cribriform plate).
E: Type 5 (insertion into the skull base).
F: Type 6 (insertion into the middle turbinate)
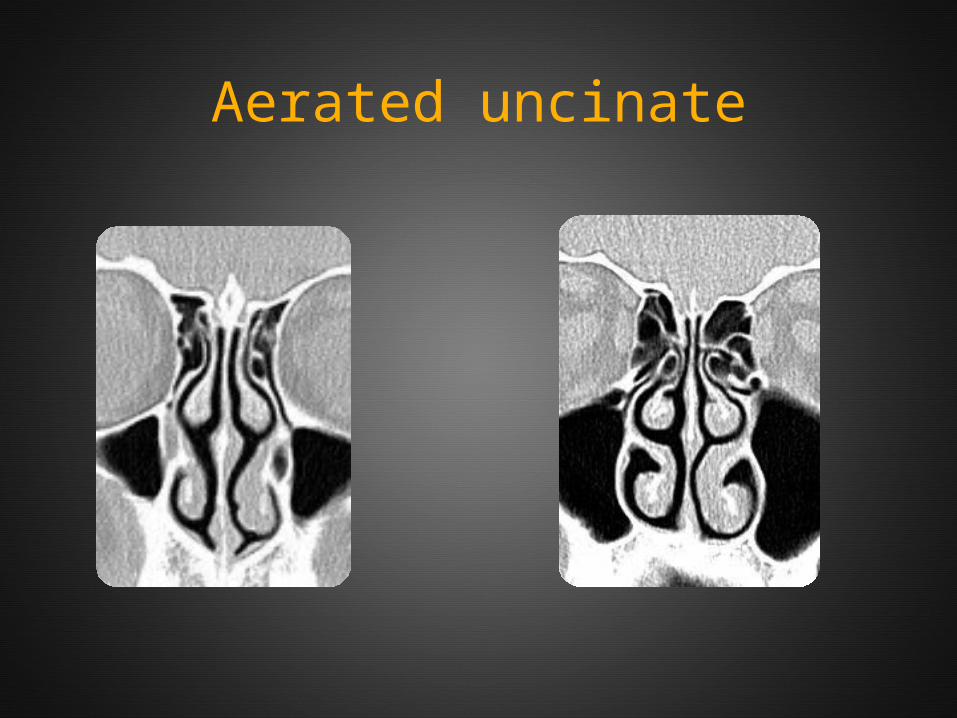
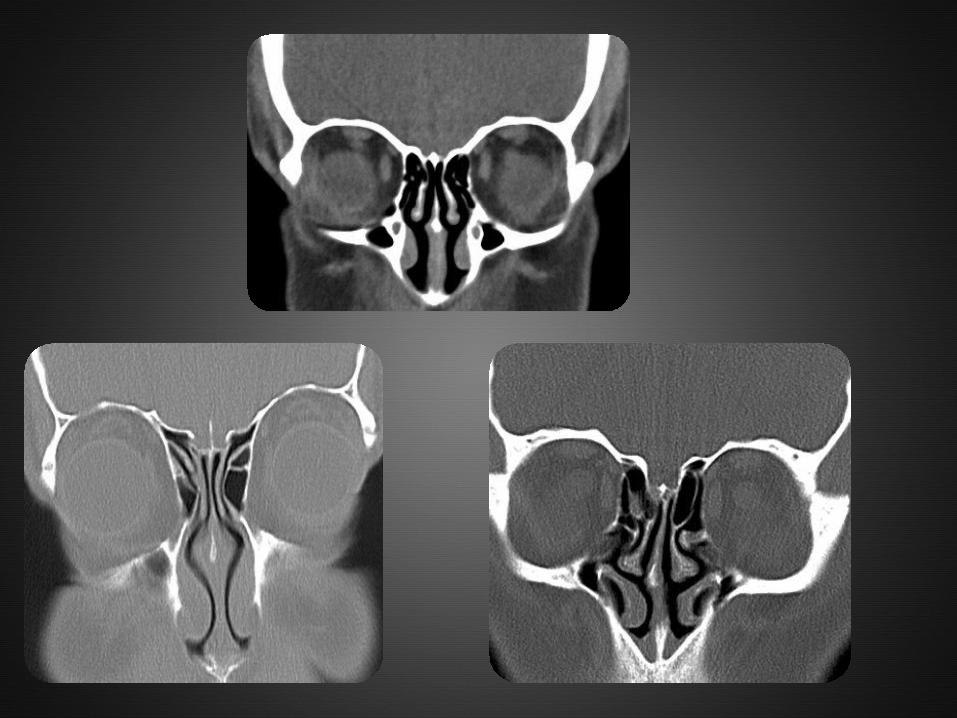
Aerated uncinate

VARIATIONS OF THE CRIBRIFORM PLATE
The cribriform plate may present at variable levels and, it is classified according to the criteria developed by Keros.
It is based on the height of the olfactory fossa in relation to the roof of the ethmoid sinus as compared with the length of the lateral lamella of cribriform plate.
The higher the Keros grade, the greater the chance of injury of the cribriform plate and olfactory fossa.

A: Type 1 (lateral cribriform lamella of 1–3 mm, the cribriform plate and the ethmoid cell roof are practically parallel to each other).
B: Type 2 (lateral lamella of 4-7 mm, cribriform plate is much below the nasal cavity as compared with the ethmoid roof).
C: Type 3 (lateral lamella of cribriform plate of 8–16 mm, ethmoid cell roof is located much above the plate

Haller cell
Infraorbital ethmoid cells or Haller cellsare ethmoid air cells located anteriorly to the ethmoid bulla, along the orbital floor, adjacent to the natural ostium of the maxillary sinus, which may cause mucociliary drainage obstruction, predisposing to the development of sinusitis.

VARIATIONS IN MIDDLE TURBINATE
Concha bullosa is a variation originated from pneumatization of the bone plate by extension of ethmoid sinus cells.
Such variation may be either uni- or bilateral.
Varied degrees of pneumatization of the concha may be observed, possibly causing middle meatus or infundibulum obstruction.



PARADOXICAL TURBINATES
Paradoxical turbinates occur as the convexity of the middle turbinate is directed towards the medial wall of the maxillary sinus.
Depending on the degree of curvature of the paradoxical turbinate compression of the infundibulum and sinusal obstruction may be observed.


ACCESSORY MAXILLARY OSTIA
Accessory maxillary ostia are generally solitary, but occasionally may be multiple.
Such variation may be congenital or secondary to sinusal diseases.
Possible mechanisms involved in the development of such variation include:
main ostium obstruction, maxillary sinusitis or anatomical/pathological factors in the middle meatus, resulting in rupture of membranous areas.


Few endoscopic pictures


Bulla ethmoidalis

Concha bullosa
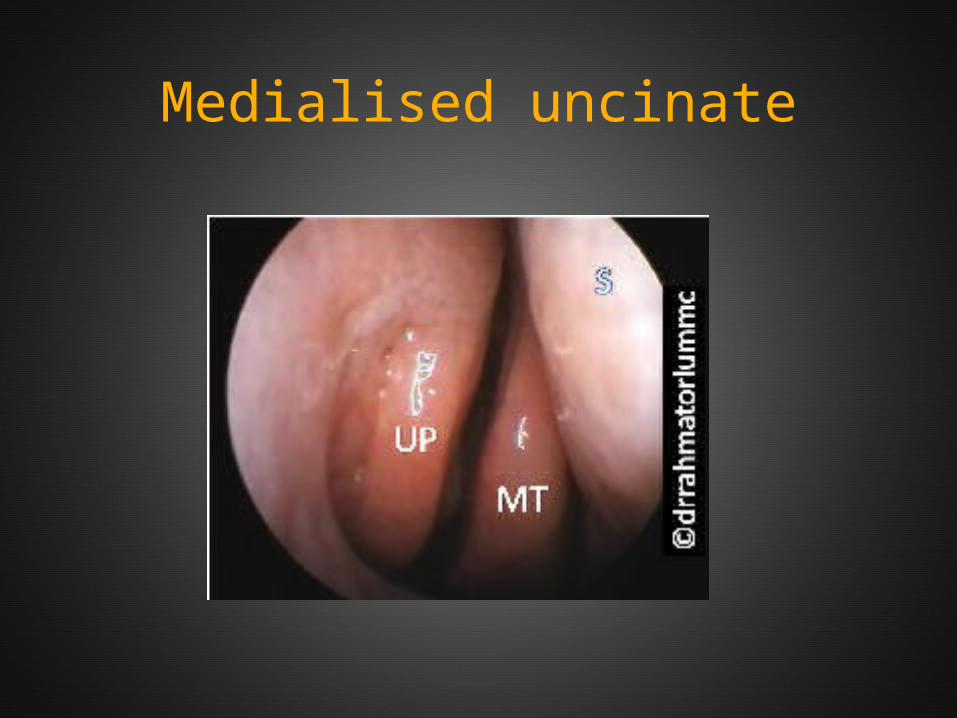
Medialised uncinate

Elevated uncinate
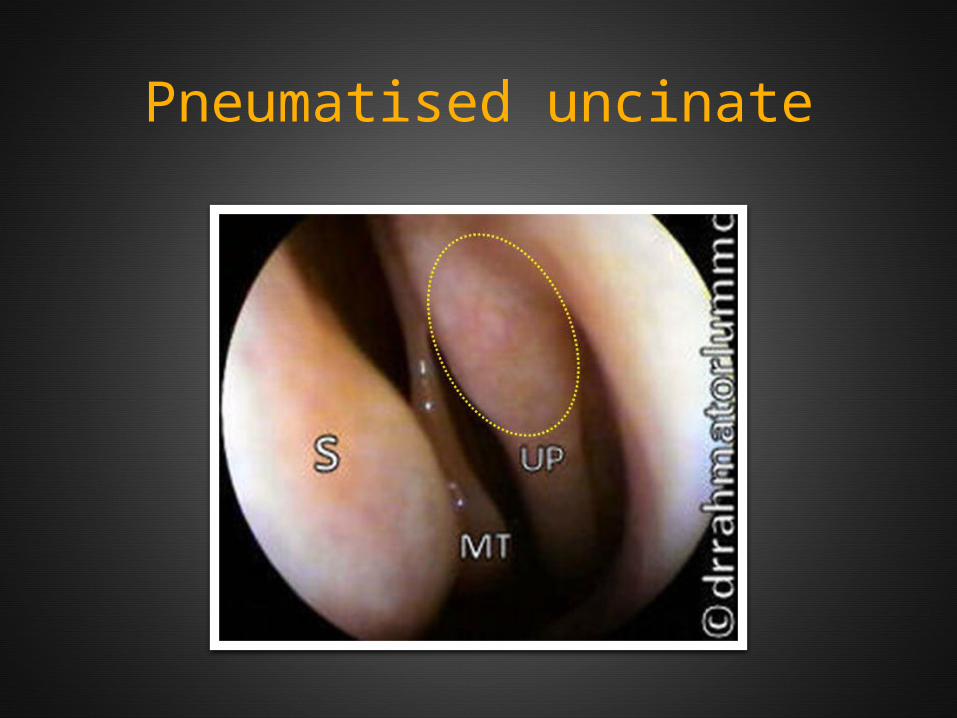
Pneumatised uncinate

Obstructive uncinate
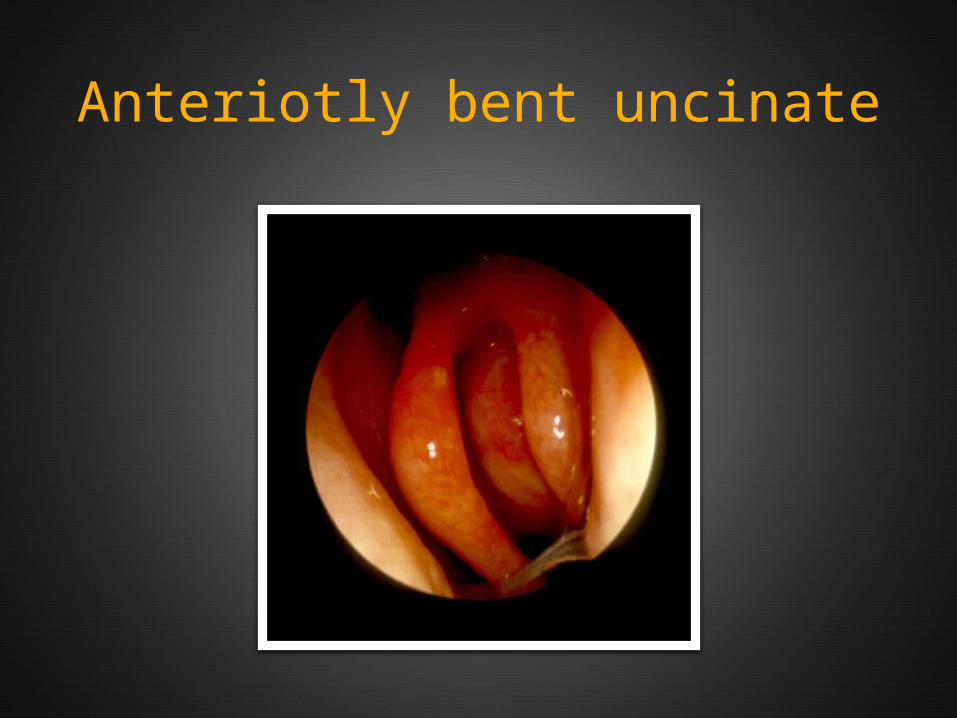
Anteriotly bent uncinate
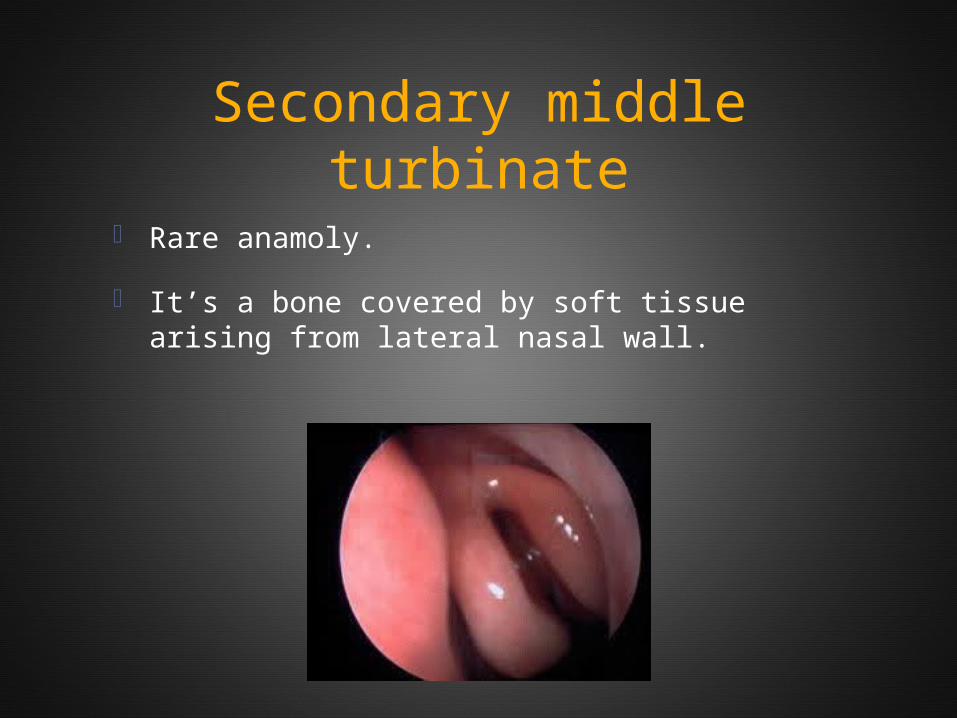
Secondary middle turbinate
Rare anamoly.
It’s a bone covered by soft tissue arising from lateral nasal wall.


THANK YOU…!