ana iif automation: moving towards harmonization? results...
TRANSCRIPT

Research ArticleANA IIF Automation Moving towards HarmonizationResults of a Multicenter Study
Stefanie Van den Bremt1 Sofie Schouwers2 Marjan Van Blerk3 and Lieve Van Hoovels1
1Department of Laboratory Medicine OLV Hospital Aalst Belgium2Department of Laboratory Medicine GZA Hospitals Antwerp Belgium3Scientific Institute of Public Health (WIV-ISP) Brussels Belgium
Correspondence should be addressed to Lieve Van Hoovels lievevanhoovelsolvz-aalstbe
Received 1 November 2016 Revised 24 January 2017 Accepted 1 February 2017 Published 21 February 2017
Academic Editor Senthami R Selvan
Copyright copy 2017 Stefanie Van den Bremt et alThis is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Background Our study aimed to investigate whether the introduction of automated anti-nuclear antibody (ANA) indirectimmunofluorescence (IIF) analysis decreases the interlaboratory variability of ANA titer results Method Three serum sampleswere sent to 10 laboratories using the QUANTA-Lyser in combination with the NOVA View Each laboratory performed theANA IIF analysis 10x in 1 run and 1x in 10 different runs and determined the endpoint titer by dilution One of the three sampleshad been sent in 2012 before the era of ANA IIF automation by the Belgian National External Quality Assessment (EQA) SchemeHarmonization was evaluated in terms of variability in fluorescence intensity (LIU) and ANA IIF titer Results The evaluation ofthe intra- and interrun LIU variability revealed a larger variability for 2 laboratories due to preanalytical and analytical problemsReanalysis of the EQAsample resulted in a lower titer variabilityDiluted endpoint titerswere similar to the estimated singlewell titerand the overall median titer as reported by the EQA in 2012ConclusionThe introduction of automatedmicroscopic analysis allowsmore harmonized ANA IIF reporting provided that this totally automated process is controlled by a thorough quality assuranceprogram covering the total ANA IIF process
1 Introduction
Autoantibodies to nuclear antigens (anti-nuclear antibodiesANAs) are useful as diagnostic biomarkers for a variety ofautoimmune diseases [1ndash6]
According to the recent recommendations of the Amer-ican College of Rheumatology ANA Task Force the indi-rect immunofluorescence (IIF) assay on human epidermoidlaryngeal carcinoma cells (HEp-2 cells) remains the goldstandard for ANA testing [3] Displaying a multitude ofhuman autoantigens this substrate enables highly sensitivepreidentification of ANAs and the determination of theirtiters The rather large variability in ANA titers betweenlaboratories running HEp-2 ANA IIF has been documentedin (inter)national proficiency testing programs [7 8] and isnot at all surprising given the intermanufacturer variationsin the HEp-2 substrate and the fixation process differences
in conjugate and microscope optics and most importantlythe subjective reading of the slides [6]
As an attempt to overcome this lack of standardizationmanufacturers have developed several computer-aided diag-nosis (CAD) systems which acquire analyze and displaydigital images of stained IIF slides [9 10] Currently availableautomated ANA IIF image analyzing systems (NOVA View(Inova Diagnostics San Diego USA) AKLIDES (Medi-pan Berlin Germany) Zenit G-Sight (Menarini FlorenceItaly) EUROPattern (Euroimmun LubeckGermany) ImageNavigator (Immuno Concepts Sacramento USA) andHELIOS (Aesku Wendelsheim Germany)) have alreadybeen reviewed extensively [9 10] These systems differ interms of DNA counterstain software algorithms for IIFdetection and pattern recognition run-time types of recog-nized ANA IIF patterns and their ability to analyze different
HindawiJournal of Immunology ResearchVolume 2017 Article ID 6038137 7 pageshttpsdoiorg10115520176038137
2 Journal of Immunology Research
Table 1 Summary of the main sample characteristics of the samples included in the study
Sample 1 Sample 2 Sample 3
Disease Crohnrsquos disease(Remicade therapy) Unknown Sjogrenrsquos syndrome
Diagnosisfollow-up Follow-up Diagnosis Unknown
Origin Diluted native OLVpatient sample
Diluted native GZAand OLV patient
sample
Native patient sampleused by WIV (EQA
SN11641)Identifiedautoantibodiessect None CENP-B SSARo60 + SSBLa
Indirectimmunofluorescencepattern on HEp-2
Homogeneous Centromere Speckled
DiagnosisFollow-up = at time of diagnosis versus follow-up of known diagnosis OLV = Onze Lieve Vrouw Hospital Aalst GZA = GasthuisZusters HospitalAntwerp WIV = Scientific Institute of Public Health Brussels EQA = extern quality control SN = sample number sectTested for dsDNA nRNPSm SmSSARo60 Ro52 SSBLa Scl-70 Jo-1 PCNA PM-Scl Rib-P and CENP-B IgG
substrates Despite these differences scientific literature sug-gests that because they are all able to overcome some of thedrawbacks of manual ANA IIF analysis these systems maycontribute to the harmonization of the HEp-2 IIF analysis[6] However until now none of the published studies haveinvestigated the degree of harmonization resulting fromANAIIF automation in actual routine clinical practice
Our study aimed to investigate if the use of automatedANA IIF image analyzing systems contributes to the com-parability of quantitative results in ANA testing by sending3 serum samples to 10 clinical laboratories using the NOVAView Harmonization was evaluated in terms of variabilityin fluorescence intensity on the one hand and ANA IIF titervariability on the other hand
2 Materials and Methods
21 Sample Preparation and Distribution Table 1 lists the 3samples under study and tabulates the clinical diagnosis theANA staining pattern and the presence of antibodies toDNAand extractable nuclear antigens (ENAs) Samples 1 and 2were prepared by the clinical laboratories of OLV HospitalAalst and GZA Hospitals Antwerp Both samples originatedfrom patients with high titer of ANA and were diluted withANA negative serum targeting a 1320 ANA IIF reactivity
Sample 3 originated from a patient with Sjogrenrsquos syn-drome In 2012 before the era of ANA IIF automation itwas sent by the BelgianNational ExternalQualityAssessment(EQA) Scheme to all Belgian laboratories performing ANAtesting The overall median titer was 11280 [11]
The 3 samples were stored at minus20∘C packaged in accor-dance with postal regulations and distributed by overnightmail All samples tested negative for hepatitis B surfaceantigen and antibodies to hepatitis C virus and humanimmunodeficiency viruses 1 and 2 During the period of themulticenter study all samples were stored at 2ndash8∘C in theparticipating laboratories
Ethical committee approval was obtained in bothorganizing hospitals (Belgian registration numbers AalstB126201525864 and Antwerp 150908ACADEM)
22 ANA IIF Methodology Ten Belgian clinical laboratories(3 university hospitals 5 nonuniversity hospitals and 2private laboratories) using the automated IIF NOVA Viewinstrument voluntarily participated in the multicenter studyAll used the NOVA Lite HEp-2 ANA kit (Inova DiagnosticsInc San Diego USA) which is mandatory for NOVA Viewand results in dyeing of the slides with two conjugates FITC(fluorescein isothiocyanate) and DAPI (410158406-diamidino-2-phenylindole) Sample dilution (1 80) and slide processingwere carried out automatically on a QUANTA-Lyser (InovaDiagnostics SanDiegoUSA) in all laboratories An overviewof the different types of NOVA View software version andQUANTA-Lyser and lot numbers of HEp-2 slides and DAPI-conjugate is available online in ldquoSupplementary Materialrdquoat httpsdoiorg10115520176038137 The presented resultshave been anonymized None of the mentioned upgrades(softwaremodel) of NOVAView andQUANTA-Lyser resultsin methodological changes leading to differences in ANA IIFresults
TheNOVAView instrument consists of an automated andfully motorized Olympus 1x81 inverted IIF microscope with4x 10x and 40x objectives and dual band DAPIFITC filtersa LED light source and a Kappa DX4 digital camera TheLED UV light source is a CoolLed PreciseExcite with exci-tation wavelengths of 400 nm (DAPI) and 490 nm (FITC)DAPI fluorescence is used by the NOVA View softwarefor localizing the HEp-2 cells and focusing Thereafter theimage analysis is performed based on the FITC signal Foreach well in a slide three to five images are acquired withboth the DAPI and the FITC filter Using FITC images thesystem measures the average intensity in units named aslight intensity units (LIU) discriminating between positiveand negative samples The cut-off set by Inova for ANA IIFpositivity is 48 LIU The NOVA View is able to identify andpropose five basic fluorescent ANA patterns (homogeneousspeckled centromere nucleolar and nuclear dots) based onsoftware algorithms Using pattern-specific dilution curvesthe measured LIU can be converted in an estimated endpointtiter (single well titer (SWT))
Journal of Immunology Research 3
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
1200160020002400280032003600400044004800
LIU
0200400600800
10001200140016001800
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0200400600800
10001200140016001800200022002400
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
1000120014001600180020002200
LIU
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
(a1) (a2) (a3)
(b1) (b2) (b3)
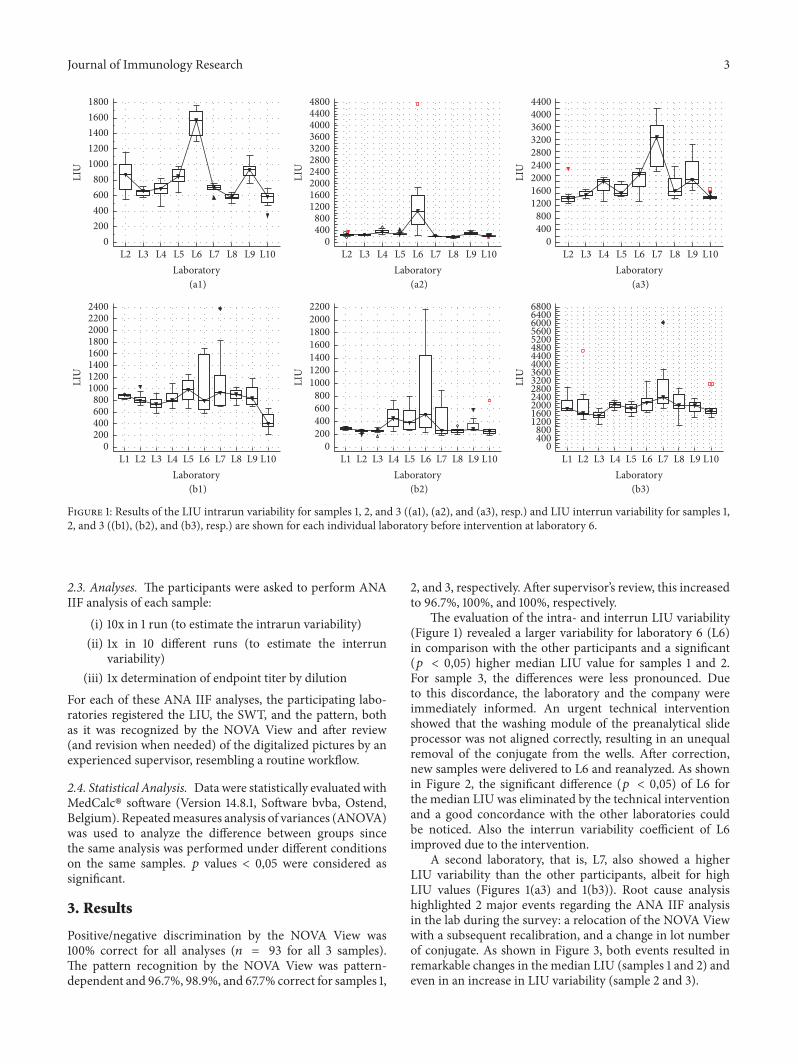
Figure 1 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory before intervention at laboratory 6
23 Analyses The participants were asked to perform ANAIIF analysis of each sample
(i) 10x in 1 run (to estimate the intrarun variability)(ii) 1x in 10 different runs (to estimate the interrun
variability)(iii) 1x determination of endpoint titer by dilution
For each of these ANA IIF analyses the participating labo-ratories registered the LIU the SWT and the pattern bothas it was recognized by the NOVA View and after review(and revision when needed) of the digitalized pictures by anexperienced supervisor resembling a routine workflow
24 Statistical Analysis Data were statistically evaluated withMedCalc software (Version 1481 Software bvba OstendBelgium) Repeatedmeasures analysis of variances (ANOVA)was used to analyze the difference between groups sincethe same analysis was performed under different conditionson the same samples 119901 values lt 005 were considered assignificant
3 Results
Positivenegative discrimination by the NOVA View was100 correct for all analyses (119899 = 93 for all 3 samples)The pattern recognition by the NOVA View was pattern-dependent and 967 989 and 677 correct for samples 1
2 and 3 respectively After supervisorrsquos review this increasedto 967 100 and 100 respectively
The evaluation of the intra- and interrun LIU variability(Figure 1) revealed a larger variability for laboratory 6 (L6)in comparison with the other participants and a significant(119901 lt 005) higher median LIU value for samples 1 and 2For sample 3 the differences were less pronounced Dueto this discordance the laboratory and the company wereimmediately informed An urgent technical interventionshowed that the washing module of the preanalytical slideprocessor was not aligned correctly resulting in an unequalremoval of the conjugate from the wells After correctionnew samples were delivered to L6 and reanalyzed As shownin Figure 2 the significant difference (119901 lt 005) of L6 forthe median LIU was eliminated by the technical interventionand a good concordance with the other laboratories couldbe noticed Also the interrun variability coefficient of L6improved due to the intervention
A second laboratory that is L7 also showed a higherLIU variability than the other participants albeit for highLIU values (Figures 1(a3) and 1(b3)) Root cause analysishighlighted 2 major events regarding the ANA IIF analysisin the lab during the survey a relocation of the NOVA Viewwith a subsequent recalibration and a change in lot numberof conjugate As shown in Figure 3 both events resulted inremarkable changes in the median LIU (samples 1 and 2) andeven in an increase in LIU variability (sample 2 and 3)
4 Journal of Immunology Research
(a1) (a2) (a3)
(b1) (b2) (b3)
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0
200
400
600
800
1000LI
U
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
10001200140016001800200022002400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
800
1000
1200
LIU
Figure 2 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory after intervention at laboratory 6
0200400600800
10001200140016001800200022002400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(a)
0
200
400
600
800
1000
LIU
and recalibrationAfter moving New conjugateInitial
23449
(b)
0400800
12001600200024002800320036004000440048005200560060006400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(c)
Figure 3 Results of LIU initial interrun variability interrun variability after relocation and subsequent calibration and interrun variabilityafter changing to another conjugate lot number for laboratory 7 for samples 1 2 and 3 ((a) (b) and (c) resp)
While the impact of the relocation and recalibration ofthe NOVA View was specific for L7 the increase in LIUvariability caused by the change of conjugate lot numberwas consistent with a more general observation All labora-tories using the same lot number conjugate that is 20337showed a higher LIU variability than laboratories using the3 other conjugate lot numbers but the difference was notsignificant (Figure 4 for pooled data) The laboratories usingthis 20337 conjugate lot that is L4 L5 L6 L7 and L8
can immediately be identified in Figure 2(b2) (laboratoryspecific data) characterized by the higher LIU variabilityRemarkable is that this variability is less pronounced forsamples 1 and 3 (higher LIU) Note that L10 was not includedin the conjugate analysis as they do not register the usedconjugate lot number
The goal of the study was to investigate if automationcontributes to the comparability of quantitative results inANA testing To this end sample 3 was included in the
Journal of Immunology Research 5
Other conjugatesConjugate 203370
200400600800
100012001400160018002000220024002600
LIU
(a)
Other conjugatesConjugate 203370
200
400
600
800
1000
LIU
(b)
Other conjugatesConjugate 203370
400800
12001600200024002800320036004000440048005200560060006400
LIU
(c)
Figure 4 Results of LIU variability for laboratories using conjugate lot number 20337 and laboratories using other conjugate lot numbers forsamples 1 2 and 3 ((a) (b) and (c) resp)
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
Endp
oint
tite
r
Sample 1 Sample 2 Sample 3
Multicenter comparison study 2016 Results WIV2012
(n = 24)
(n = 10)
160320640
12802560ge5120
01020304050607080
o
f the
labs
Figure 5 Overview of the reported ANA IIF titers for samples 1 2 and 3
study In 2012 24 laboratories using the InovaHEp2 substrateperformed manual ANA IIF analysis and reported titersranging within 1 160ndash1 2560 with a median ANA IIF titerof 1 640 which was comparable with the overall mediantiter of 1 1280 (cfr Figure 5) Only 25 of all laboratoriesreported themedianANA IIF titer of 1 640Analysis of a newaliquot of the original EQA sample in the present multicentercomparison study revealed a lower endpoint titer variabilitywith 70 of the laboratories reporting the median titer of1 1280 In addition diluted determined endpoint titers on theautomated system were similar (+minus1 titer) to the estimatedsingle well titer on the system and the overall median titer of1 1280 as reported by the Belgian EQA in 2012 [11] The samesmall variability in endpoint titer reporting was seen for theother samples (Figure 5)
4 Discussion
Due to the key position of ANA screening in the serologicaldiagnosis of systemic rheumatic diseases consistent repro-ducibility and high quality of HEp-2 cell-based IIF assaysare required [4] However the visual and therefore subjectiveevaluation of these assays complicates their standardizationFurthermore the analysis is labor intensive Consequentlyit does not meet the economic and quality requirementsgoverning current clinical laboratory practice Contempo-rary laboratories have to be efficient and highly automatedenvironments Therefore in an attempt to overcome thedrawbacks of manual ANA IIF analysis CAD systems wererecently developed [12 13] Besides the newer CAD systemalso the well-established automated slide processing is animportant part of ANA IIF analysis
6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Journal of Immunology Research
Table 1 Summary of the main sample characteristics of the samples included in the study
Sample 1 Sample 2 Sample 3
Disease Crohnrsquos disease(Remicade therapy) Unknown Sjogrenrsquos syndrome
Diagnosisfollow-up Follow-up Diagnosis Unknown
Origin Diluted native OLVpatient sample
Diluted native GZAand OLV patient
sample
Native patient sampleused by WIV (EQA
SN11641)Identifiedautoantibodiessect None CENP-B SSARo60 + SSBLa
Indirectimmunofluorescencepattern on HEp-2
Homogeneous Centromere Speckled
DiagnosisFollow-up = at time of diagnosis versus follow-up of known diagnosis OLV = Onze Lieve Vrouw Hospital Aalst GZA = GasthuisZusters HospitalAntwerp WIV = Scientific Institute of Public Health Brussels EQA = extern quality control SN = sample number sectTested for dsDNA nRNPSm SmSSARo60 Ro52 SSBLa Scl-70 Jo-1 PCNA PM-Scl Rib-P and CENP-B IgG
substrates Despite these differences scientific literature sug-gests that because they are all able to overcome some of thedrawbacks of manual ANA IIF analysis these systems maycontribute to the harmonization of the HEp-2 IIF analysis[6] However until now none of the published studies haveinvestigated the degree of harmonization resulting fromANAIIF automation in actual routine clinical practice
Our study aimed to investigate if the use of automatedANA IIF image analyzing systems contributes to the com-parability of quantitative results in ANA testing by sending3 serum samples to 10 clinical laboratories using the NOVAView Harmonization was evaluated in terms of variabilityin fluorescence intensity on the one hand and ANA IIF titervariability on the other hand
2 Materials and Methods
21 Sample Preparation and Distribution Table 1 lists the 3samples under study and tabulates the clinical diagnosis theANA staining pattern and the presence of antibodies toDNAand extractable nuclear antigens (ENAs) Samples 1 and 2were prepared by the clinical laboratories of OLV HospitalAalst and GZA Hospitals Antwerp Both samples originatedfrom patients with high titer of ANA and were diluted withANA negative serum targeting a 1320 ANA IIF reactivity
Sample 3 originated from a patient with Sjogrenrsquos syn-drome In 2012 before the era of ANA IIF automation itwas sent by the BelgianNational ExternalQualityAssessment(EQA) Scheme to all Belgian laboratories performing ANAtesting The overall median titer was 11280 [11]
The 3 samples were stored at minus20∘C packaged in accor-dance with postal regulations and distributed by overnightmail All samples tested negative for hepatitis B surfaceantigen and antibodies to hepatitis C virus and humanimmunodeficiency viruses 1 and 2 During the period of themulticenter study all samples were stored at 2ndash8∘C in theparticipating laboratories
Ethical committee approval was obtained in bothorganizing hospitals (Belgian registration numbers AalstB126201525864 and Antwerp 150908ACADEM)
22 ANA IIF Methodology Ten Belgian clinical laboratories(3 university hospitals 5 nonuniversity hospitals and 2private laboratories) using the automated IIF NOVA Viewinstrument voluntarily participated in the multicenter studyAll used the NOVA Lite HEp-2 ANA kit (Inova DiagnosticsInc San Diego USA) which is mandatory for NOVA Viewand results in dyeing of the slides with two conjugates FITC(fluorescein isothiocyanate) and DAPI (410158406-diamidino-2-phenylindole) Sample dilution (1 80) and slide processingwere carried out automatically on a QUANTA-Lyser (InovaDiagnostics SanDiegoUSA) in all laboratories An overviewof the different types of NOVA View software version andQUANTA-Lyser and lot numbers of HEp-2 slides and DAPI-conjugate is available online in ldquoSupplementary Materialrdquoat httpsdoiorg10115520176038137 The presented resultshave been anonymized None of the mentioned upgrades(softwaremodel) of NOVAView andQUANTA-Lyser resultsin methodological changes leading to differences in ANA IIFresults
TheNOVAView instrument consists of an automated andfully motorized Olympus 1x81 inverted IIF microscope with4x 10x and 40x objectives and dual band DAPIFITC filtersa LED light source and a Kappa DX4 digital camera TheLED UV light source is a CoolLed PreciseExcite with exci-tation wavelengths of 400 nm (DAPI) and 490 nm (FITC)DAPI fluorescence is used by the NOVA View softwarefor localizing the HEp-2 cells and focusing Thereafter theimage analysis is performed based on the FITC signal Foreach well in a slide three to five images are acquired withboth the DAPI and the FITC filter Using FITC images thesystem measures the average intensity in units named aslight intensity units (LIU) discriminating between positiveand negative samples The cut-off set by Inova for ANA IIFpositivity is 48 LIU The NOVA View is able to identify andpropose five basic fluorescent ANA patterns (homogeneousspeckled centromere nucleolar and nuclear dots) based onsoftware algorithms Using pattern-specific dilution curvesthe measured LIU can be converted in an estimated endpointtiter (single well titer (SWT))
Journal of Immunology Research 3
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
1200160020002400280032003600400044004800
LIU
0200400600800
10001200140016001800
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0200400600800
10001200140016001800200022002400
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
1000120014001600180020002200
LIU
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
(a1) (a2) (a3)
(b1) (b2) (b3)
Figure 1 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory before intervention at laboratory 6
23 Analyses The participants were asked to perform ANAIIF analysis of each sample
(i) 10x in 1 run (to estimate the intrarun variability)(ii) 1x in 10 different runs (to estimate the interrun
variability)(iii) 1x determination of endpoint titer by dilution
For each of these ANA IIF analyses the participating labo-ratories registered the LIU the SWT and the pattern bothas it was recognized by the NOVA View and after review(and revision when needed) of the digitalized pictures by anexperienced supervisor resembling a routine workflow
24 Statistical Analysis Data were statistically evaluated withMedCalc software (Version 1481 Software bvba OstendBelgium) Repeatedmeasures analysis of variances (ANOVA)was used to analyze the difference between groups sincethe same analysis was performed under different conditionson the same samples 119901 values lt 005 were considered assignificant
3 Results
Positivenegative discrimination by the NOVA View was100 correct for all analyses (119899 = 93 for all 3 samples)The pattern recognition by the NOVA View was pattern-dependent and 967 989 and 677 correct for samples 1
2 and 3 respectively After supervisorrsquos review this increasedto 967 100 and 100 respectively
The evaluation of the intra- and interrun LIU variability(Figure 1) revealed a larger variability for laboratory 6 (L6)in comparison with the other participants and a significant(119901 lt 005) higher median LIU value for samples 1 and 2For sample 3 the differences were less pronounced Dueto this discordance the laboratory and the company wereimmediately informed An urgent technical interventionshowed that the washing module of the preanalytical slideprocessor was not aligned correctly resulting in an unequalremoval of the conjugate from the wells After correctionnew samples were delivered to L6 and reanalyzed As shownin Figure 2 the significant difference (119901 lt 005) of L6 forthe median LIU was eliminated by the technical interventionand a good concordance with the other laboratories couldbe noticed Also the interrun variability coefficient of L6improved due to the intervention
A second laboratory that is L7 also showed a higherLIU variability than the other participants albeit for highLIU values (Figures 1(a3) and 1(b3)) Root cause analysishighlighted 2 major events regarding the ANA IIF analysisin the lab during the survey a relocation of the NOVA Viewwith a subsequent recalibration and a change in lot numberof conjugate As shown in Figure 3 both events resulted inremarkable changes in the median LIU (samples 1 and 2) andeven in an increase in LIU variability (sample 2 and 3)
4 Journal of Immunology Research
(a1) (a2) (a3)
(b1) (b2) (b3)
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0
200
400
600
800
1000LI
U
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
10001200140016001800200022002400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
800
1000
1200
LIU
Figure 2 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory after intervention at laboratory 6
0200400600800
10001200140016001800200022002400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(a)
0
200
400
600
800
1000
LIU
and recalibrationAfter moving New conjugateInitial
23449
(b)
0400800
12001600200024002800320036004000440048005200560060006400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(c)
Figure 3 Results of LIU initial interrun variability interrun variability after relocation and subsequent calibration and interrun variabilityafter changing to another conjugate lot number for laboratory 7 for samples 1 2 and 3 ((a) (b) and (c) resp)
While the impact of the relocation and recalibration ofthe NOVA View was specific for L7 the increase in LIUvariability caused by the change of conjugate lot numberwas consistent with a more general observation All labora-tories using the same lot number conjugate that is 20337showed a higher LIU variability than laboratories using the3 other conjugate lot numbers but the difference was notsignificant (Figure 4 for pooled data) The laboratories usingthis 20337 conjugate lot that is L4 L5 L6 L7 and L8
can immediately be identified in Figure 2(b2) (laboratoryspecific data) characterized by the higher LIU variabilityRemarkable is that this variability is less pronounced forsamples 1 and 3 (higher LIU) Note that L10 was not includedin the conjugate analysis as they do not register the usedconjugate lot number
The goal of the study was to investigate if automationcontributes to the comparability of quantitative results inANA testing To this end sample 3 was included in the
Journal of Immunology Research 5
Other conjugatesConjugate 203370
200400600800
100012001400160018002000220024002600
LIU
(a)
Other conjugatesConjugate 203370
200
400
600
800
1000
LIU
(b)
Other conjugatesConjugate 203370
400800
12001600200024002800320036004000440048005200560060006400
LIU
(c)
Figure 4 Results of LIU variability for laboratories using conjugate lot number 20337 and laboratories using other conjugate lot numbers forsamples 1 2 and 3 ((a) (b) and (c) resp)
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
Endp
oint
tite
r
Sample 1 Sample 2 Sample 3
Multicenter comparison study 2016 Results WIV2012
(n = 24)
(n = 10)
160320640
12802560ge5120
01020304050607080
o
f the
labs
Figure 5 Overview of the reported ANA IIF titers for samples 1 2 and 3
study In 2012 24 laboratories using the InovaHEp2 substrateperformed manual ANA IIF analysis and reported titersranging within 1 160ndash1 2560 with a median ANA IIF titerof 1 640 which was comparable with the overall mediantiter of 1 1280 (cfr Figure 5) Only 25 of all laboratoriesreported themedianANA IIF titer of 1 640Analysis of a newaliquot of the original EQA sample in the present multicentercomparison study revealed a lower endpoint titer variabilitywith 70 of the laboratories reporting the median titer of1 1280 In addition diluted determined endpoint titers on theautomated system were similar (+minus1 titer) to the estimatedsingle well titer on the system and the overall median titer of1 1280 as reported by the Belgian EQA in 2012 [11] The samesmall variability in endpoint titer reporting was seen for theother samples (Figure 5)
4 Discussion
Due to the key position of ANA screening in the serologicaldiagnosis of systemic rheumatic diseases consistent repro-ducibility and high quality of HEp-2 cell-based IIF assaysare required [4] However the visual and therefore subjectiveevaluation of these assays complicates their standardizationFurthermore the analysis is labor intensive Consequentlyit does not meet the economic and quality requirementsgoverning current clinical laboratory practice Contempo-rary laboratories have to be efficient and highly automatedenvironments Therefore in an attempt to overcome thedrawbacks of manual ANA IIF analysis CAD systems wererecently developed [12 13] Besides the newer CAD systemalso the well-established automated slide processing is animportant part of ANA IIF analysis
6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Journal of Immunology Research 3
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
1200160020002400280032003600400044004800
LIU
0200400600800
10001200140016001800
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0200400600800
10001200140016001800200022002400
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
1000120014001600180020002200
LIU
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
(a1) (a2) (a3)
(b1) (b2) (b3)
Figure 1 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory before intervention at laboratory 6
23 Analyses The participants were asked to perform ANAIIF analysis of each sample
(i) 10x in 1 run (to estimate the intrarun variability)(ii) 1x in 10 different runs (to estimate the interrun
variability)(iii) 1x determination of endpoint titer by dilution
For each of these ANA IIF analyses the participating labo-ratories registered the LIU the SWT and the pattern bothas it was recognized by the NOVA View and after review(and revision when needed) of the digitalized pictures by anexperienced supervisor resembling a routine workflow
24 Statistical Analysis Data were statistically evaluated withMedCalc software (Version 1481 Software bvba OstendBelgium) Repeatedmeasures analysis of variances (ANOVA)was used to analyze the difference between groups sincethe same analysis was performed under different conditionson the same samples 119901 values lt 005 were considered assignificant
3 Results
Positivenegative discrimination by the NOVA View was100 correct for all analyses (119899 = 93 for all 3 samples)The pattern recognition by the NOVA View was pattern-dependent and 967 989 and 677 correct for samples 1
2 and 3 respectively After supervisorrsquos review this increasedto 967 100 and 100 respectively
The evaluation of the intra- and interrun LIU variability(Figure 1) revealed a larger variability for laboratory 6 (L6)in comparison with the other participants and a significant(119901 lt 005) higher median LIU value for samples 1 and 2For sample 3 the differences were less pronounced Dueto this discordance the laboratory and the company wereimmediately informed An urgent technical interventionshowed that the washing module of the preanalytical slideprocessor was not aligned correctly resulting in an unequalremoval of the conjugate from the wells After correctionnew samples were delivered to L6 and reanalyzed As shownin Figure 2 the significant difference (119901 lt 005) of L6 forthe median LIU was eliminated by the technical interventionand a good concordance with the other laboratories couldbe noticed Also the interrun variability coefficient of L6improved due to the intervention
A second laboratory that is L7 also showed a higherLIU variability than the other participants albeit for highLIU values (Figures 1(a3) and 1(b3)) Root cause analysishighlighted 2 major events regarding the ANA IIF analysisin the lab during the survey a relocation of the NOVA Viewwith a subsequent recalibration and a change in lot numberof conjugate As shown in Figure 3 both events resulted inremarkable changes in the median LIU (samples 1 and 2) andeven in an increase in LIU variability (sample 2 and 3)
4 Journal of Immunology Research
(a1) (a2) (a3)
(b1) (b2) (b3)
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0
200
400
600
800
1000LI
U
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
10001200140016001800200022002400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
800
1000
1200
LIU
Figure 2 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory after intervention at laboratory 6
0200400600800
10001200140016001800200022002400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(a)
0
200
400
600
800
1000
LIU
and recalibrationAfter moving New conjugateInitial
23449
(b)
0400800
12001600200024002800320036004000440048005200560060006400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(c)
Figure 3 Results of LIU initial interrun variability interrun variability after relocation and subsequent calibration and interrun variabilityafter changing to another conjugate lot number for laboratory 7 for samples 1 2 and 3 ((a) (b) and (c) resp)
While the impact of the relocation and recalibration ofthe NOVA View was specific for L7 the increase in LIUvariability caused by the change of conjugate lot numberwas consistent with a more general observation All labora-tories using the same lot number conjugate that is 20337showed a higher LIU variability than laboratories using the3 other conjugate lot numbers but the difference was notsignificant (Figure 4 for pooled data) The laboratories usingthis 20337 conjugate lot that is L4 L5 L6 L7 and L8
can immediately be identified in Figure 2(b2) (laboratoryspecific data) characterized by the higher LIU variabilityRemarkable is that this variability is less pronounced forsamples 1 and 3 (higher LIU) Note that L10 was not includedin the conjugate analysis as they do not register the usedconjugate lot number
The goal of the study was to investigate if automationcontributes to the comparability of quantitative results inANA testing To this end sample 3 was included in the
Journal of Immunology Research 5
Other conjugatesConjugate 203370
200400600800
100012001400160018002000220024002600
LIU
(a)
Other conjugatesConjugate 203370
200
400
600
800
1000
LIU
(b)
Other conjugatesConjugate 203370
400800
12001600200024002800320036004000440048005200560060006400
LIU
(c)
Figure 4 Results of LIU variability for laboratories using conjugate lot number 20337 and laboratories using other conjugate lot numbers forsamples 1 2 and 3 ((a) (b) and (c) resp)
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
Endp
oint
tite
r
Sample 1 Sample 2 Sample 3
Multicenter comparison study 2016 Results WIV2012
(n = 24)
(n = 10)
160320640
12802560ge5120
01020304050607080
o
f the
labs
Figure 5 Overview of the reported ANA IIF titers for samples 1 2 and 3
study In 2012 24 laboratories using the InovaHEp2 substrateperformed manual ANA IIF analysis and reported titersranging within 1 160ndash1 2560 with a median ANA IIF titerof 1 640 which was comparable with the overall mediantiter of 1 1280 (cfr Figure 5) Only 25 of all laboratoriesreported themedianANA IIF titer of 1 640Analysis of a newaliquot of the original EQA sample in the present multicentercomparison study revealed a lower endpoint titer variabilitywith 70 of the laboratories reporting the median titer of1 1280 In addition diluted determined endpoint titers on theautomated system were similar (+minus1 titer) to the estimatedsingle well titer on the system and the overall median titer of1 1280 as reported by the Belgian EQA in 2012 [11] The samesmall variability in endpoint titer reporting was seen for theother samples (Figure 5)
4 Discussion
Due to the key position of ANA screening in the serologicaldiagnosis of systemic rheumatic diseases consistent repro-ducibility and high quality of HEp-2 cell-based IIF assaysare required [4] However the visual and therefore subjectiveevaluation of these assays complicates their standardizationFurthermore the analysis is labor intensive Consequentlyit does not meet the economic and quality requirementsgoverning current clinical laboratory practice Contempo-rary laboratories have to be efficient and highly automatedenvironments Therefore in an attempt to overcome thedrawbacks of manual ANA IIF analysis CAD systems wererecently developed [12 13] Besides the newer CAD systemalso the well-established automated slide processing is animportant part of ANA IIF analysis
6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Journal of Immunology Research
(a1) (a2) (a3)
(b1) (b2) (b3)
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0400800
120016002000240028003200360040004400480052005600600064006800
LIU
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0
200
400
600
800
1000LI
U
L2 L3 L4 L5 L6 L7 L8 L9 L10L1Laboratory
0200400600800
10001200140016001800200022002400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0400800
120016002000240028003200360040004400
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
LIU
L3 L4 L5 L6 L7 L8 L9 L10L2Laboratory
0
200
400
600
800
1000
1200
LIU
Figure 2 Results of the LIU intrarun variability for samples 1 2 and 3 ((a1) (a2) and (a3) resp) and LIU interrun variability for samples 12 and 3 ((b1) (b2) and (b3) resp) are shown for each individual laboratory after intervention at laboratory 6
0200400600800
10001200140016001800200022002400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(a)
0
200
400
600
800
1000
LIU
and recalibrationAfter moving New conjugateInitial
23449
(b)
0400800
12001600200024002800320036004000440048005200560060006400
LIU
and recalibrationAfter moving New conjugateInitial
23449
(c)
Figure 3 Results of LIU initial interrun variability interrun variability after relocation and subsequent calibration and interrun variabilityafter changing to another conjugate lot number for laboratory 7 for samples 1 2 and 3 ((a) (b) and (c) resp)
While the impact of the relocation and recalibration ofthe NOVA View was specific for L7 the increase in LIUvariability caused by the change of conjugate lot numberwas consistent with a more general observation All labora-tories using the same lot number conjugate that is 20337showed a higher LIU variability than laboratories using the3 other conjugate lot numbers but the difference was notsignificant (Figure 4 for pooled data) The laboratories usingthis 20337 conjugate lot that is L4 L5 L6 L7 and L8
can immediately be identified in Figure 2(b2) (laboratoryspecific data) characterized by the higher LIU variabilityRemarkable is that this variability is less pronounced forsamples 1 and 3 (higher LIU) Note that L10 was not includedin the conjugate analysis as they do not register the usedconjugate lot number
The goal of the study was to investigate if automationcontributes to the comparability of quantitative results inANA testing To this end sample 3 was included in the
Journal of Immunology Research 5
Other conjugatesConjugate 203370
200400600800
100012001400160018002000220024002600
LIU
(a)
Other conjugatesConjugate 203370
200
400
600
800
1000
LIU
(b)
Other conjugatesConjugate 203370
400800
12001600200024002800320036004000440048005200560060006400
LIU
(c)
Figure 4 Results of LIU variability for laboratories using conjugate lot number 20337 and laboratories using other conjugate lot numbers forsamples 1 2 and 3 ((a) (b) and (c) resp)
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
Endp
oint
tite
r
Sample 1 Sample 2 Sample 3
Multicenter comparison study 2016 Results WIV2012
(n = 24)
(n = 10)
160320640
12802560ge5120
01020304050607080
o
f the
labs
Figure 5 Overview of the reported ANA IIF titers for samples 1 2 and 3
study In 2012 24 laboratories using the InovaHEp2 substrateperformed manual ANA IIF analysis and reported titersranging within 1 160ndash1 2560 with a median ANA IIF titerof 1 640 which was comparable with the overall mediantiter of 1 1280 (cfr Figure 5) Only 25 of all laboratoriesreported themedianANA IIF titer of 1 640Analysis of a newaliquot of the original EQA sample in the present multicentercomparison study revealed a lower endpoint titer variabilitywith 70 of the laboratories reporting the median titer of1 1280 In addition diluted determined endpoint titers on theautomated system were similar (+minus1 titer) to the estimatedsingle well titer on the system and the overall median titer of1 1280 as reported by the Belgian EQA in 2012 [11] The samesmall variability in endpoint titer reporting was seen for theother samples (Figure 5)
4 Discussion
Due to the key position of ANA screening in the serologicaldiagnosis of systemic rheumatic diseases consistent repro-ducibility and high quality of HEp-2 cell-based IIF assaysare required [4] However the visual and therefore subjectiveevaluation of these assays complicates their standardizationFurthermore the analysis is labor intensive Consequentlyit does not meet the economic and quality requirementsgoverning current clinical laboratory practice Contempo-rary laboratories have to be efficient and highly automatedenvironments Therefore in an attempt to overcome thedrawbacks of manual ANA IIF analysis CAD systems wererecently developed [12 13] Besides the newer CAD systemalso the well-established automated slide processing is animportant part of ANA IIF analysis
6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
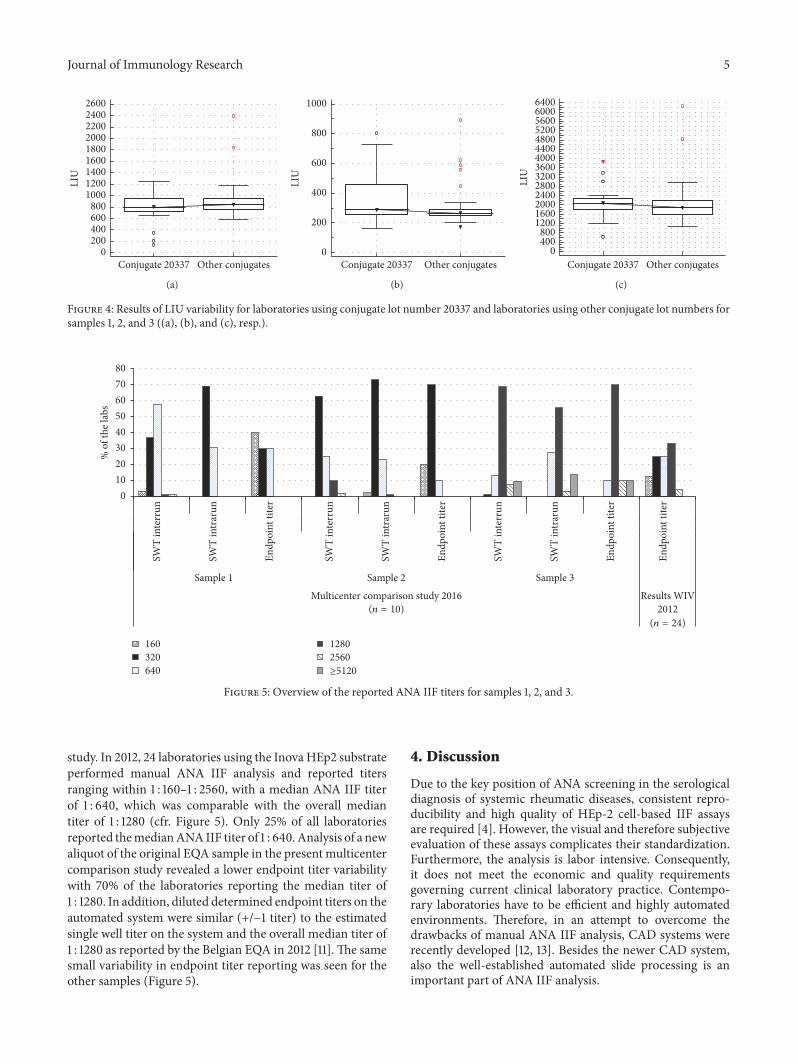
Journal of Immunology Research 5
Other conjugatesConjugate 203370
200400600800
100012001400160018002000220024002600
LIU
(a)
Other conjugatesConjugate 203370
200
400
600
800
1000
LIU
(b)
Other conjugatesConjugate 203370
400800
12001600200024002800320036004000440048005200560060006400
LIU
(c)
Figure 4 Results of LIU variability for laboratories using conjugate lot number 20337 and laboratories using other conjugate lot numbers forsamples 1 2 and 3 ((a) (b) and (c) resp)
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
SWT
inte
rrun
SWT
intr
arun
Endp
oint
tite
r
Endp
oint
tite
r
Sample 1 Sample 2 Sample 3
Multicenter comparison study 2016 Results WIV2012
(n = 24)
(n = 10)
160320640
12802560ge5120
01020304050607080
o
f the
labs
Figure 5 Overview of the reported ANA IIF titers for samples 1 2 and 3
study In 2012 24 laboratories using the InovaHEp2 substrateperformed manual ANA IIF analysis and reported titersranging within 1 160ndash1 2560 with a median ANA IIF titerof 1 640 which was comparable with the overall mediantiter of 1 1280 (cfr Figure 5) Only 25 of all laboratoriesreported themedianANA IIF titer of 1 640Analysis of a newaliquot of the original EQA sample in the present multicentercomparison study revealed a lower endpoint titer variabilitywith 70 of the laboratories reporting the median titer of1 1280 In addition diluted determined endpoint titers on theautomated system were similar (+minus1 titer) to the estimatedsingle well titer on the system and the overall median titer of1 1280 as reported by the Belgian EQA in 2012 [11] The samesmall variability in endpoint titer reporting was seen for theother samples (Figure 5)
4 Discussion
Due to the key position of ANA screening in the serologicaldiagnosis of systemic rheumatic diseases consistent repro-ducibility and high quality of HEp-2 cell-based IIF assaysare required [4] However the visual and therefore subjectiveevaluation of these assays complicates their standardizationFurthermore the analysis is labor intensive Consequentlyit does not meet the economic and quality requirementsgoverning current clinical laboratory practice Contempo-rary laboratories have to be efficient and highly automatedenvironments Therefore in an attempt to overcome thedrawbacks of manual ANA IIF analysis CAD systems wererecently developed [12 13] Besides the newer CAD systemalso the well-established automated slide processing is animportant part of ANA IIF analysis
6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Journal of Immunology Research
It is the responsibility of the laboratory to evaluate andcontrol all variables having a potential impact on the ldquototaltesting processrdquo This implicates preanalytical variables likepathology grade variation associated with sample originwashing or pipetting errors and analytical errors (eg reagentlot numbers and calibration errors) but also postanalyticalvariables (eg laboratory information system modification)Our study results reveal a reduction in ANA IIF titervariability between laboratories using the NOVA View butalso highlight the importance of quality assurance of the totalprocess by different problems encountered during the studyClinically important variability in ANA IIF LIU was shownfor L6 due to slide processor washing problems resulting inextended conjugate incubation times and significant higherLIU values Calibration error and conjugate lot changes alsorevealed clinical significant LIU shifts for L7
The implementation of CAD systems enables the intro-duction of objective internal control material (iQC) pro-cedures to monitor the total ANA IIF process Qualityassurance can rely on the daily follow-up of LIU valuesof positive and negative iQC measurements based on thetraditionally used Westgard multirules [14 15] Regardingthose iQC materials it is important to emphasize that theyshould assure the whole ANA IIF analysis process fromdilution up to result interpretation which is not always thecase when only company iQC materials are used Secondlythe effect of major variables (eg conjugate changes) is notshown at iQC samples with higher LIU values Positive iQCsamples around the cut-off of positivity reveal the mostinformation Our study shows already a considerable LIUvariability with one type of conjugate Not only the LIU targetvalue will be affected by a new lot number of conjugate butalso the LIU variation seems to be affected We anticipatethat besides a paired statistical analysis of the LIU valuesof a set of routine samples with current and new conjugatelot number also an intrarun imprecision analysis has to beperformed by the autoimmune laboratory before acceptancein routine ANA IIF practice Both analyses are of additionalvalue besides the current recommendation of at least 85numerical equivalent results [15] However there is a needfor universally accepted guidelines on how to perform lotswitch evaluations and consensus criteria for acceptability[16] Finally it is worthwhile to include a quality marker forthe whole ANA IIF testing process in the daily routine iQCanalysis for example median LIU for every routine run [17]This marker is independent on the sample position used andis of added value in the quality management of automatedANA IIF when initial lot-to-lot comparison protocols fail todetect a change [16]
As the evaluations of neither standardized positiveneg-ative discrimination neither pattern recognition were goalsof our current study the samples used were strongly ANAIIF positive with clearly defined and monospecific patternsThe interlaboratory positivenegative discrimination shouldbe a goal for a new study Enlarging the study scope withother CAD systems on the daily market will even give a morerealistic view on the ANA IIF variability burden introducedby the availability of different HEp-2 kits
Recognizing mixed or ldquonovelrdquo fluorescence patternsremains a challenge for every CAD system necessitatingexpert review [9] This difficulty is even more accentuatedby differences in fixative used for different HEp-2 cellpreparations causing a high variability in cell and nuclearmorphologywhich results in significant variability of stainingpatterns on the ANA HEp-2 IIF substrates obtained withslides from different manufacturers [7 18]This challenge hasled to a proposed consensus nomenclature for IIF patternsavailable on the international consensus of anti-nuclear anti-body pattern (ICAP) website (httpwwwANApatternsorg)The ultimate goal with the establishment of the ICAP is topromote harmonization of ANA test nomenclature as well asinterpretation guidelines forANA testing thereby optimizingusage in patient care [19] CAD systems offer the opportunityto easily apply this standardized nomenclature in routineautoimmune laboratories
5 Conclusion
Through the introduction of automatedmicroscopic analysismore harmonized ANA IIF reporting becomes feasibleprovided that this totally automated process is controlled bya thorough quality assurance programThis program impliesthe necessity of validation after recalibration and lot numberchanging of the most critical reagents (substrate and conju-gate) and a continuous internal quality control that coversthe total ANA IIF process from pre- to postanalytical phaseExtending the multicenter comparison to all automated IIFmicroscopes available nowadays is necessary to address theuniformity of the global ANA IIF analysis
Competing Interests
The authors declare that they have no competing interests
Acknowledgments
The authors gratefully acknowledge Juul Boes (AZ Turn-hout) Sylvie Goletti and Jean-Paul Tomasi (UCL Louvain)Leen Slaets and Sara Vijgen (Jessa Ziekenhuis Hasselt)Bjorn Gehesquiere and Ignace Van Hecke (CRI Zwijnaarde)Annemie Van Ruymbeke (AZ Alma Sijsele) Tine Geens andEddy Lens (CMAHasselt) Xavier Bossuyt LauraHendrickxand SilkeWillebrords (UZ Leuven) and Francis Corazza andCarole Nagant (CHU Brugmann Brussel) for participatingin the survey Christel Van Campenhout (WIV Brussels) forproviding sample 3 Ismaıl Nakach and Nathalie Vandeputte(Werfen NVSA Benelux) for their practical support
References
[1] A Doria M Zen M Canova et al ldquoSLE diagnosis andtreatment when early is earlyrdquo Autoimmunity Reviews vol 10no 1 pp 55ndash60 2010
[2] J Damoiseaux C A von Muhlen I Garcia-De La Torre etal ldquoInternational consensus on ANA patterns (ICAP) thebumpy road towards a consensus on reporting ANA resultsrdquoAutoimmunity Highlights vol 7 no 1 article no 1 pp 1ndash8 2016
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Journal of Immunology Research 7
[3] P L Meroni and P H Schur ldquoANA screening an old test withnew recommendationsrdquo Annals of the Rheumatic Diseases vol69 no 8 pp 1420ndash1422 2010
[4] R Tozzoli C Bonaguri A Melegari A Antico D Bassettiand N Bizzaro ldquoCurrent state of diagnostic technologies in theautoimmunology laboratoryrdquo Clinical Chemistry and Labora-tory Medicine vol 51 no 1 pp 129ndash138 2013
[5] MVanBlerk X Bossuyt RHumbel et al ldquoBelgian recommen-dations on ANA anti-dsDNA and anti-ENA antibody testingrdquoActa Clinica Belgica vol 69 no 2 pp 83ndash86 2014
[6] M Infantino F Meacci V Grossi et al ldquoThe burden of thevariability introduced by the HEp-2 assay kit and the CAD sys-tem in ANA indirect immunofluorescence testrdquo ImmunologicResearch pp 1ndash10 2016
[7] S S Copple S R Giles T D Jaskowski A E Gardiner AM Wilson and H R Hill ldquoScreening for IgG antinuclearautoantibodies by HEp-2 indirect fluorescent antibody assaysand the need for standardizationrdquo American Journal of ClinicalPathology vol 137 no 5 pp 825ndash830 2012
[8] M Van Blerk C Van Campenhout X Bossuyt et al ldquoCurrentpractices in antinuclear antibody testing results from thebelgian external quality assessment schemerdquoClinical Chemistryand Laboratory Medicine vol 47 no 1 pp 102ndash108 2009
[9] N Bizzaro A Antico S Platzgummer et al ldquoAutomated antin-uclear immunofluorescence antibody screening a comparativestudy of six computer-aided diagnostic systemsrdquoAutoimmunityReviews vol 13 no 3 pp 292ndash298 2014
[10] C Krause K Ens K Fechner et al ldquoEUROPattern Suite tech-nology for computer-aided immunofluorescencemicroscopy inautoantibody diagnosticsrdquo Lupus vol 24 no 4-5 pp 516ndash5292015
[11] WIV-ISP Rapport of eQC Sending 20121 ANA IIF 2012 httpswwwwiv-ispbeQMLactivitiesexternal qualityrapports downserologie non infectieuse20121 NIET INFEC SERO ANApdf
[12] K Egerer D Roggenbuck R Hiemann et al ldquoAutomatedevaluation of autoantibodies on human epithelial-2 cells as anapproach to standardize cell-based immunofluorescence testsrdquoArthritis Research andTherapy vol 12 no 2 article R40 2010
[13] D Roggenbuck R Hiemann D Bogdanos D Reinhold andK Conrad ldquoStandardization of automated interpretation ofimmunofluorescence testsrdquo Clinica Chimica Acta vol 421 pp168ndash169 2013
[14] T M Maenhouta C Bonroya C Verfaillie V Stove and KDevreese ldquoAutomated indirect immunofluorescencemicroscopyenables the implementation of a quantitative internal qualitycontrol system for anti-nuclear antibody (ANA) analysisrdquoClinical Chemistry and Laboratory Medicine vol 52 no 7 pp989ndash998 2014
[15] Clinical and Laboratory Standards Institute (CLSI) QualityAssurance of Laboratory Tests for Autoantibodies to NuclearAntigens (1) Indirect Fluorescent Assay for Microscopy and (2)Microtiter Enzyme Immunoassay Methods Approved GuidelineCLSI Document ILA2-A2 CLSIWayne Pa USA 2nd edition2006
[16] A Algeciras-Schimnich D E Bruns J C Boyd S C Bryant KA La Fortune and S K G Grebe ldquoFailure of current laboratoryprotocols to detect lot-to-lot reagent differences findings andpossible solutionsrdquo Clinical Chemistry vol 59 no 8 pp 1187ndash1194 2013
[17] S M N Mulliez T M Maenhout and C Bonroy ldquoImpact ofthe routine implementation of automated indirect immunoflu-orescence antinuclear antibody analysis 1 year of experiencerdquo
Clinical Chemistry and Laboratory Medicine vol 54 no 7 ppe183ndashe186 2016
[18] M Mahler P-L Meroni X Bossuyt and M J FritzlerldquoCurrent concepts and future directions for the assessment ofautoantibodies to cellular antigens referred to as anti-nuclearantibodiesrdquo Journal of Immunology Research vol 2014 ArticleID 315179 18 pages 2014
[19] E K L Chan J Damoiseaux O G Carballo et al ldquoReport ofthe first international consensus on standardized nomenclatureof antinuclear antibody HEp-2 cell patterns (ICAP) 2014-2015rdquoFrontiers in Immunology vol 6 article no 412 2015
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom