an integrated system based approach to workforce
TRANSCRIPT
NORTHUMBRIA UNIVERSITY
An integrated system based approach to
workforce development for Enhanced Care for
Older People with Complex Needs
Dr Juliana Thompson, Sue Tiplady, Dr Anne McNall, Professor Glenda Cook, Lindsay Courtney
February 2018
Commissioned and funded by NHS Newcastle Gateshead Clinical
Commissioning Group
1
Contents Page
1 Background 3
2 Aims and objectives of ‘assessing the 9 state of workforce competency’
3 Methodology and methods 10
3.1 Phase 1, strand 1: competency gap Analysis 11
3.2 Phase 1, strand 2: stakeholder perspectives of cross system assessment of competency and proficiency 15
3.3 Phase 2: stakeholder perspectives of developing a workforce development strategy 17
4 Findings 19
4.1 Phase 1, strand 1 19 4.2 Phase 1, strand 2 36 4.3 Phase 2 52
5 Discussion 59
6 Recommendations 69
7 Appendices 74
7.1 Web links to phase 1, strand 1 surveys 74 7.2 Phase 1, strand 1 observation tool 75 7.3 Information sources concerning 83
apprenticeships and funding
8 References 84
2
Acknowledgements
We the Research Team wish to express our appreciation of the participants who provided
generous input into this study. We also wish to acknowledge the priority given to the topic of
workforce development by NHS Newcastle Gateshead Clinical Commissioning Group
Gateshead Care Home Programme Team, and for commissioning this study.

3
1: Background The national Vanguard initiative was set up to identify and test new care models with the
purpose of developing blueprints for the transformation of National Health Service (NHS)
community and primary services in England (NHS England, 2017a). One of the five types of
Vanguard is Enhanced Health in Care Homes. These programmes recognise that care
homes are caring for older people with increasing levels of frailty, disability and multi-
morbidities; and who are highly dependent, have complex conditions including dementia,
have limited functional reserve, and require end-of-life care (Salisbury et al, 2011; Barnett et
al, 2012; Cornwell, 2012; European Commission, 2015). The Enhanced Health in Care
Homes programmes aim to make health services for care home residents more accessible,
cost effective, and tailored to their needs, so that quality of life and quality of care is
improved and unnecessary hospital admissions are avoided.
In recent years, the Gateshead Care Home programme has provided enhanced healthcare
in care homes through integrated multi-sector working. This involves aligning general
practitioner (GP) practices and older people nurse specialists (OPSNs) to care homes. This
allows these care homes to access multi-disciplinary community virtual wards, and wider
health and social care services. Locally, this multi-disciplinary approach is leading to
improved quality of care, and reductions in avoidable hospital admissions. These positive
outcomes led to the Gateshead Care Home programme becoming a Vanguard Enhanced
Health in Care Homes site, enabling it to build and develop this model of care (NHS
England, 2017b).
The Gateshead model cuts across traditional health and social care boundaries and focuses
on transforming the whole system. This involves developing new care pathways and
systems/services for care delivery, so that high quality care for residents can be provided.
This transformation requires a workforce that is highly competent, and appropriately skilled.
An initial research study was commissioned by Newcastle Gateshead Clinical
Commissioning Group (CCG) in early 2016 (Cook et al, 2016). The aim of this study was to
explore the experiences and competencies of the current Gateshead Care Home workforce
team to inform workforce development for the delivery of the Gateshead service model. The
findings of this study suggested a need for a workforce competency framework that is
standardised and integrated, specific to the needs of residents, and covers the whole
workforce from those providing essential care to specialist and advanced practice levels. As
a consequence, Newcastle Gateshead CCG commissioned the development of a workforce

4
competency framework for Enhanced Care for Older people with Complex Needs (EnCOP)
(Thompson et al, 2017).
Development of the EnCOP workforce competency framework
The emphasis on competency rather than on role allows the framework to be both
standardised and flexible, enabling it to encompass and support the development of all
health and social care personnel who provide services for residents, regardless of role, or
employing organisation. The purpose of competency frameworks is to provide a system-wide
coherent approach to: determining what competencies are required within the workforce;
identifying ‘competency gaps’; identifying, commissioning, and providing learning
opportunities, education programmes and assessment processes to support competency
development; developing clear career progression opportunities and pathways within and
across organisations; facilitate the adoption of high quality practices; pursue innovative
service strategies, and informing service users what competencies they should expect staff
to have (Staron, 2008; Roche, 2009; McNall, 2012).
The most effective competency frameworks are co-produced by practitioners and
educationalists/academics (Anema and McCoy, 2010). The ENCOP framework was
developed via a collaborative process involving academic staff from Northumbria University
with expertise in the care of older people and workforce development, and practitioner
stakeholders with expertise and experience in providing care for older people and care home
residents with complex needs.
The study design consisted of two interrelated stages. Stage one involved the development
of a draft workforce competency framework by a team of researchers from Northumbria
University. This involved:
• review of existing workforce competency research literature relevant to the care of
older people
• analysis of existing competency frameworks that have relevance to the care of older
people
• discussions with the multi-disciplinary, multi-sector Care Home Vanguard ‘Pathways
of Care’ (PoC) team from Gateshead and Newcastle localities to identify
competencies required at each practice level (essential, specialist and advanced).
The PoC team consists of representatives from a wide range of health and social
care professionals and organisations. The aim of the team is to improve healthcare
services for local care home residents and their families by identifying practice areas
5
requiring improvement, then designing, implementing and evaluating new care
delivery models to address these improvement needs.
Stage two involved a stakeholder workshop to discuss the draft framework, and to provide
an opportunity for attendees to contribute their views on its further development. Attendees
numbered 65 and represented a broad range of professions and service-users, and
stakeholder groups from the NHS, private and voluntary care sectors.
The involvement of individuals from a range of groups ensured that many perspectives were
brought to the discussions. This was important, as care homes are located at the
intersection of health and social care, and public, private and voluntary sector care services
– locations where cross-organisational working and the enabling of seamless transitions
across services is essential.
Structure of the EnCOP workforce competency framework
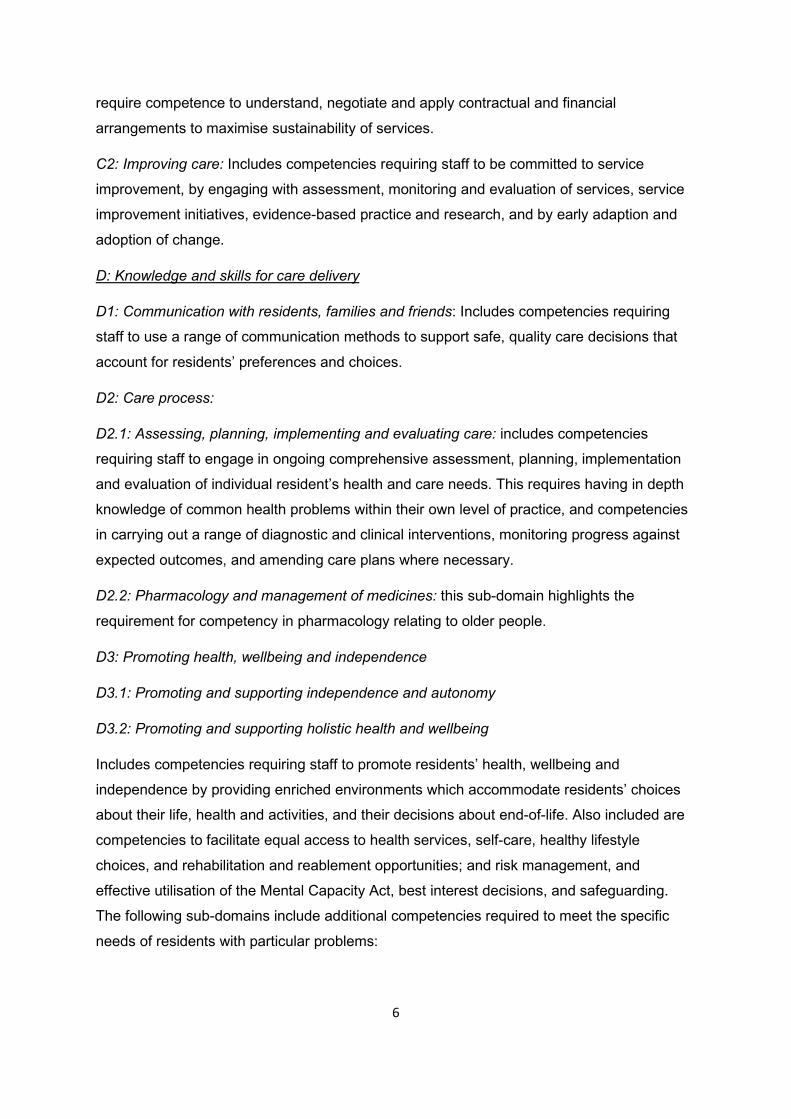
The framework consists of four inter-related domains, and each domain is comprised of sets
and subsets of competencies:
A: Values and attitudes: Includes values and attitudes competencies; and also includes
competencies requiring staff to be aware of their own values and attitudes, and acknowledge
that residents and their families and friends will have their own sets of values and beliefs that
influence their choices and decisions.
B: Workforce collaboration, co-operation and support
B1: Inter-professional and inter-organisational working and communication: Includes
competencies requiring staff to engage in inter-professional and inter-organisational working
and communication, and develop collaborative, co-operative working relationships with all
members of the care team.
B2: Teaching, learning, and supporting competence development: Includes competencies
requiring staff to acquire and maintain evidence-based knowledge and skills, and support
others in the development of knowledge and skills on an ongoing basis in order to increase
scope of practice and ensure a highly competent workforce.
C: Leading, organising, managing and improving care
C1: Leading, organising and managing care: Includes competencies requiring staff to use
principles of leadership, organisation and management in order to facilitate provision of safe,
effective and efficient practice. This involves engaging with care systems and clinical
governance, and managing services and resources including staffing and skill mix. Staff also
6
require competence to understand, negotiate and apply contractual and financial
arrangements to maximise sustainability of services.
C2: Improving care: Includes competencies requiring staff to be committed to service
improvement, by engaging with assessment, monitoring and evaluation of services, service
improvement initiatives, evidence-based practice and research, and by early adaption and
adoption of change.
D: Knowledge and skills for care delivery
D1: Communication with residents, families and friends: Includes competencies requiring
staff to use a range of communication methods to support safe, quality care decisions that
account for residents’ preferences and choices.
D2: Care process:
D2.1: Assessing, planning, implementing and evaluating care: includes competencies
requiring staff to engage in ongoing comprehensive assessment, planning, implementation
and evaluation of individual resident’s health and care needs. This requires having in depth
knowledge of common health problems within their own level of practice, and competencies
in carrying out a range of diagnostic and clinical interventions, monitoring progress against
expected outcomes, and amending care plans where necessary.
D2.2: Pharmacology and management of medicines: this sub-domain highlights the
requirement for competency in pharmacology relating to older people.
D3: Promoting health, wellbeing and independence
D3.1: Promoting and supporting independence and autonomy
D3.2: Promoting and supporting holistic health and wellbeing
Includes competencies requiring staff to promote residents’ health, wellbeing and
independence by providing enriched environments which accommodate residents’ choices
about their life, health and activities, and their decisions about end-of-life. Also included are
competencies to facilitate equal access to health services, self-care, healthy lifestyle
choices, and rehabilitation and reablement opportunities; and risk management, and
effective utilisation of the Mental Capacity Act, best interest decisions, and safeguarding.
The following sub-domains include additional competencies required to meet the specific
needs of residents with particular problems:
7
D4: Management of dementia (these competencies are in addition to D1,2 and 3)
D5: Management of mental health (these competencies are in addition to D1,2 and 3)
D6: Management of frailty (these competencies are in addition to D1,2 and 3)
D7: End of Life care (these competencies are in addition to D1,2 and 3).
Although all domains and competencies are inter-related, findings from the literature review
and analysis of the discussions from the PoC meetings highlighted that the ability of staff to
deliver quality care very much depend upon a whole workforce ability to:
• Establish and maintain a culture of compassionate, relationship-centred values and
attitudes.
• Work collaboratively, co-operatively and supportively.
• Lead, manage, organise and continuously improve systems of care, and sustain
these improvements.
When developing the framework, the decision was made to emphasise these core workforce
requirements by creating domains that comprise of competencies that specifically address
these (domains A, B and C). These domains precede domain D because the study findings
suggest they are prerequisites for the development of knowledge and skills for care delivery,
and quality, seamless care delivery practice. In other words, having knowledge and skills in
care delivery is not enough on its own. Practitioners need to have the right values, be able to
work together, and lead and improve care if the care delivered is going to be effective.
Figure 1: Competency domains for a care home workforce

8
Levels of practice
The framework includes three competency levels: essential practice, specialist practice and
advanced practice. The competency levels are progressive and cumulative i.e. as levels
advance, they integrate and expand upon competencies from the preceding level. Some
individuals may have competencies from more than one level. For example, a registered
nurse working in a care home may have all essential practice competencies and some
specialist practice competencies; a care home manager, an OPSN or a GP may have most
specialist practice competencies and some advanced practice competencies. By comparing
existing competencies and competency levels with the framework, areas for development
can be identified. On an individual basis, this knowledge can support personal development
and career progression.
On a whole workforce basis, this knowledge can support understanding of workforce
education and development needs and workforce planning.
Figure 2: Example of a page from the EnCOP framework
9
2: Aims and objectives of ‘assessing the state of workforce competency’ The knowledge, skills and competencies required across the whole workforce have been
agreed, culminating in the collaborative development of the EnCOP competency framework
(Thompson, et al 2017). The current project, aimed to understand the current state of
workforce competency in the Newcastle Gateshead area to inform future strategic workforce
development within the regional Sustainability and Transformation Plan (STP). This was
achieved by addressing the following objectives:
1. Develop understanding of the existing competencies of care home staff and NHS
professionals working in 2 pilot care homes by mapping staff against the relevant
level of the EnCOP competency framework (gap analysis) to understand
workforce development need and priority areas for development.
2. Develop understanding of capacity, capability and agreement for cross system
practice based learning and assessment through; the identification and
development of staff from different organisations within the pilot sites as
mentors/practice based supervisors/ assessors of competence, and collaborative
exploration of the agreements/policies needed to enable cross system learning
and assessment.
3. Engage employers in the sector (including care homes, foundation trusts,
community teams, local authority, social care provider organisations) in
collaborative exploration of the findings, identified priorities, proposed workforce
competency development solutions and sustainable funding options including the
apprenticeship levy, HEE Continuing Workforce Development (CWD) monies and
the European Social Fund (ESF).
10
3: Methodology and methods To address the above aim and objectives a mixed method study informed by collaborative
action research was undertaken. The primary purpose of action research is to bring about
change in specific situations, in local systems and real world environments, with the aim of
solving real problems, which was the intention of this project. A core principle of collaborative
action research is that researchers collaborate with practitioners and other stakeholders, and
research with, rather than on the researched, and embed the perspectives of key
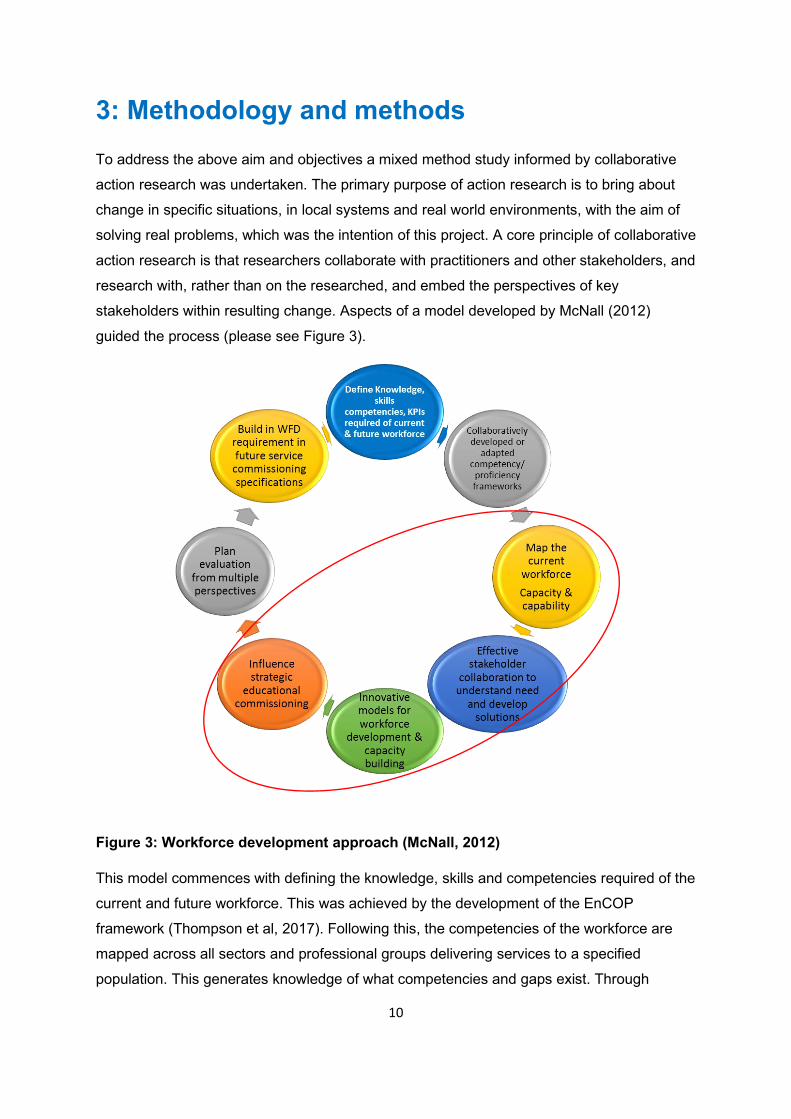
stakeholders within resulting change. Aspects of a model developed by McNall (2012)
guided the process (please see Figure 3).
Figure 3: Workforce development approach (McNall, 2012)
This model commences with defining the knowledge, skills and competencies required of the
current and future workforce. This was achieved by the development of the EnCOP
framework (Thompson et al, 2017). Following this, the competencies of the workforce are
mapped across all sectors and professional groups delivering services to a specified
population. This generates knowledge of what competencies and gaps exist. Through

11
stakeholder collaboration, solutions to address gaps are developed. The findings provide an
evidence base that underpins future workforce planning which is integral to the Sustainability
and Transformation Plan (STP) following completion of the Vanguard programme.
The study had 2 phases. Phase 1 had 2 parallel strands – strand 1 sought to develop
knowledge of competencies of care home and NHS staff working in 2 pilot care home sites,
and strand two explored with key stakeholders the issues that need to be addressed and
agreed to achieve cross system agreement for mentors/assessors to operate across
organisational boundaries (addressing objectives 1 and 2). In phase two recommendations
for a workforce strategy and delivery plan were developed with health and social care
employers and commissioners (addressing objective 3).
Research ethics approval to undertake the study was secured from the Faculty of Health and
Life Sciences, Northumbria University on 14 December 2017.
3.1 Phase 1, strand 1: competency gap analysis
A competency gap analysis was undertaken to identify existing workforce competency, and
identify workforce development need and priority areas for development. This was achieved
by using data collection methods to map participants' competency against the relevant level
of the EnCOP competency framework. Data was collected via 2 methods:
Method 1: competency survey
Method 1 data collection: 3 online survey tools were developed reflecting the three
competency levels included in the EnCOP workforce competency framework (i.e essential,
specialist and advanced levels). Participants were required to complete the survey they felt
was relevant to their competency level. The surveys were 2-part. The first part was common
to all 3 surveys and collected quantitative data including: demographic information;
consideration of role, experience, personal and professional development; access to
education, training, statutory and mandatory updating; support, appraisal and supervision;
perceived workforce competency need; preferred learning approach; existing and required
infrastructure to enable practice based learning and assessment of competence. The second
part of the surveys were specific to the 3 competency levels and required participants to
record their perceived competence and confidence against the relevant competencies within
the EnCOP framework on a scale of 1 to 5 – 1=not sure what this means; 2=not at all
competent; 3=not very competent, 4=somewhat competent; 5=very competent (web links to
the surveys are provided in appendix 7.1).

12
Method 1 sample: The study was located within the geographical area served by Newcastle
Gateshead CCG. In total, there are 81 care homes within this area. Inclusion criteria for the
study care homes were:
• Mixed registration status (residential, nursing, and/or EMI).
• Offer services to older people with complex physical, cognitive and mental health
problems.
• Offer student nurse placements (in order to explore the potential requirements for
sustainable future workforce).
After applying the inclusion criteria, the sample population was 22. Members of the
Newcastle Gateshead Vanguard Pathway of Care team who work with these 22 care homes
identified homes in which staff were likely to be in a position to make the significant
commitment that will be required for participation. A sampling matrix using a purposive
sampling approach was applied to the responding care homes. The criteria for the sampling
matrix included homes in different localities, variety of health and social care professions
working in the homes, and variety of competency levels of staff (i.e. essential, specialist and
advanced levels). From the sampling matrix, 2 care home pilot sites were identified. In total,
122 health and care staff work in and into the pilot care homes.
The surveys were circulated as both online and pdf hardcopy surveymonkey questionnaires
to care home managers and Older Person Specialist Nurse team leaders. Managers and
team leaders were asked to distribute the surveys to staff, and participating staff chose the
survey which they felt was most relevant to their competency level. To enhance the
response rate, members of the research team visited the care homes to raise awareness of
the questionnaires. This resulted in a total of 36 responses – a 30% response rate: 10 health
care assistants, 4 nursing assistants, 3 care home management team (2 registered nurses,
1 non-nurse), 9 OPSN Band 6, 5 OPSN Band 7, 3 registered nurses, 1 GP, 1 allied
healthcare professional. All health care assistants and nursing assistants, and the non-nurse
management team member completed the essential level questionnaire (n=15). All RNs, 8
OPSN Band 6, 4 OPSN Band 7 and the OT completed the specialist questionnaire (n=16).
Both management team nurses, the GP, 1 OPSN Band 6 and 1 OPSN Band 7 completed
the advanced questionnaire (n=5). Although the response rate was low, this rate is not
unusual for external surveys (Gray et al, 2017).
Method 2: observation of practice
Method 2 data collection: Members of the research team who have in depth knowledge of
the EnCOP framework observed participants’ practice using an observation survey tool. This

13
tool was used to collect quantitative data to identify and record observed levels of
competence and confidence against the relevant EnCOP framework for each participant.
The tool was supplemented with observers’ notes used to record examples of observed
practice that illustrated competency levels. In order to check interrater reliability, all research
team members involved in the observations used the tool to assess a simulated ward round
prior to using the tool during the study (a copy of the observation tool is provided in appendix
7.2).
Method 2 sample
All health and care staff working in and into the pilot care homes were informed about the
observation study and invited to take part. Staff that agreed to participate were requested to
sign a consent form. During the observation periods, individuals who were not participants
were sometimes present (for example, staff who did not wish to be participants in the study,
and residents/families). The researchers asked these individuals’ permission to observe
participants’ practice in their presence, and made it clear that only observations of
participants would be recorded. 21 episodes of observation of practice involving 71
individual health and care workers took place. These included 26 health care assistants, 3
nursing assistants, 4 OPSN Band 6, 10 OPSN Band 7, 11 registered nurses, 2 allied
healthcare professionals, 5 GPs, 6 consultants, and 4 care home management team (all
RNs). In line with questionnaire participants’ self-reported competency category, health care
assistants and nursing assistants were mapped against essential level competencies, and
GPs and care home nurse management team members were mapped against advanced
level competencies. In line with all RNs, allied healthcare professionals and the majority of
OPSN questionnaire participants, RNs, AHPs and OPSNs were mapped against specialist
level competencies. Consultants did not complete questionnaires so the research team
decided to map consultants against the advanced level.
Strand 1 data analysis
Data from the questionnaires completed online were imported into SPSS, and data from the
hardcopy questionnaires and observation tools were entered manually into SPSS in
preparation for inferential and descriptive statistical analysis. For consistency, part 2 of the
advanced level questionnaires completed by the 2 OPSNs were removed from the data set,
and part 1 was transferred to the specialist level data set.
Descriptive frequency analysis was used to analyse part 1 of the questionnaires. Part 2 of
the questionnaires was analysed as follows:

14
• The questionnaires required participants to self-rate their competence against each
individual competency of the EnCOP framework. Competencies ratings within each
domain/sub-domain were calculated via mode. This method was chosen as it was
considered to be consistent with the method of rating observations i.e researchers
rated practice according to most common competency levels observed within each
domain/sub-domain.
• A Mann-Whitney U test was used to compare differences between self-reported and
observed domain/sub-domain competency ratings. Consultants were not included in
this comparison of difference as they did not self-report. Likewise, the non-nurse
management team member was not included as no observations were undertaken of
this participant. There were no statistical significant differences between the self-
reported and observed data sets, except essential level ‘improving care’ whereby
self-reported competency (mean rank = 18.64) was found to score statistically
significantly higher (U = 54, p = 0.018) than observed competency; and specialist
level ‘teaching, learning and support’ whereby self-reported competency (mean rank
= 23.63) was found to score statistically significantly higher (U = 54, p = 0.000) than
observed competency. The data sets were therefore combined, but the significantly
higher self-reported data for essential level ‘improving care’ and specialist level
‘teaching, learning and support’ were removed.
• Mann Whitney U tests were used to compare differences in pilot site competency,
and differences in NHS/non-NHS competency.
• Spearman rho correlation calculations were used to determine possible relationships
between highest academic level and competence, and to determine possible
relationships between competence in interprofessional working and clinical
competence; teaching, learning and support and clinical competence; and
leadership, organization and management and clinical competence.
• Domain/sub-domain ratings 2-5 were assigned nominal numbers, and means and
standard deviations were calculated (rating 1 ‘not sure what this means’ was not
included in these calculations). This facilitated descriptive analysis of the workforce
and identification of priority areas for competency development for competency level
(essential, specialist and advanced) and role.
15
3.2 Phase 1, strand 2: stakeholder perspectives of cross system assessment of competency and proficiency
An area of specific relevance to this current project is the development of capacity within
Newcastle and Gateshead care homes for the supervision and mentoring of staff, and
capability to assess competence. This is an emerging and ongoing area of development
which includes consideration of the use of accreditation of prior learning (APEL) to recognize
prior learning and meet the mentor standards (NMC 2008) to become registered mentors. In
acknowledgement of this ongoing workforce development, the following methods were
applied to develop knowledge of the existing situation and explore barriers and facilitators to
progress:
Method 1
The identification and development of staff from different organisations within the pilot sites
as potential or actual mentors/practice based supervisors/assessors of competence.
Method 2: stakeholder interviews
Method 2 data collection: The original plan was to complete uni-organisation focus group
interviews with professionals from care home, NHS and social care services who have
responsibility for staff learning and assessment. While individuals were keen to participate,
however existing commitments limited availability to take part in group interviews. The
research methods were therefore adapted to include dyad and individual interviews as well
as uni-organisational group interviews. Focus group interviews are conducive to promoting
rich discussion and sharing of experiences between participants. The uni-organisation group
interviews enabled staff from each organisation to articulate their own perspectives. In
contrast, and complementary to the group discussions, individual interviews facilitated in-
depth discussions of particular situations that occurred with regard to competency
development and assessment. During the interviews, issues that need to be addressed to
achieve cross system agreement for mentors/assessors to operate across organisational
boundaries were explored. Also options for preparation of supervisors and practice-based
assessors were discussed.
Method 2 sample
Professionals from a wide range of care home, NHS and social care organisations across
the North East region who have responsibility for staff learning and assessment were
identified and invited to attend an interview. In order to optimise participation in the study,
these interviews were held within participants’ work places. Staff that agreed to participate
16
were requested to sign a consent form. In total 29 individuals agreed to participate in the
study and all were interviewed. Interview methods were 2 focus group interviews (n=9 and
n=10), 2 dyads and 6 individual interviews. Individuals from 6 care home organisations, the
NHS, and a local authority took part:
Care home organisations:
• 2 x operational managers
• 12 x care home managers
• 1 x clinical lead nurse
• 2 x practice development nurses
Local authority:
• 1 x social worker
NHS:
• 2 x GPs
• 1 x consultant geropsychiatrist
• 1 x nurse consultant for older people
• 3 x OPSNs
• 2 x clinical educators
• 1 x lead nurse (quality)
• 1 x nurse lead (Vanguard)
In order to maximise confidentiality, when reporting data in the form of participants’ verbatim
quotes, their employing organisations only are given.
Strand 1, method 2 data analysis
Audio recordings were made of the focus group interviews. The audio recorded data was
transcribed verbatim, and was then open coded by individual members of the research team.
This allowed elucidation and description of the participants’ experiences of competency
assessment, while creating meaningful themes. Thematic analysis was chosen as it is ‘a
method for organising, analysing and reporting patterns (themes) within data. It minimally
organises and describes your data set in (rich) detail’ (Braun and Clarke, 2006, p.79). The
approach taken was inductive, in other words the analysis was data driven, rather than
theory driven. The 6 phase guide to conducting thematic analysis, as outlined by Braun and
Clarke (2006) was used. This process has the following phases: familiarisation with the data;
generating initial codes; organisation of the initial codes into patterns to generate themes;

17
reviewing themes; defining and naming themes; interpretation. During this process, all
transcripts were then independently coded by another team member, and the outcomes
were compared with the original coding to validate themes. A further level of rigour was
inbuilt into the data analysis process through discussing preliminary themes emerging from
data analysis with workshop participants in phase 2 of the study.
3.3 Phase 2: stakeholder perspectives of developing a workforce development strategy
Data collection
Two stakeholder workshops were attended by employers and commissioners in services
providing care for older people. These were held on 9 February 2018 and 12 February 2018.
Two workshops were held to maximize opportunities for participation. The workshops
provided a forum to explore the findings from phase 1, and exploration of issues regarding
the existing and required infrastructure for practice based learning and competency
assessment. The workshops also provided opportunity for participants to make
recommendations for a workforce development strategy, workforce development solutions,
and options for sustainable funding options of identified solutions. All participants were also
encouraged to record their views on post-it notes as the discussions progressed. This
provided a further opportunity to capture individual views. Summary points from the group
discussions were recorded on flip charts by members of the research team.
Sample
Invitations to take part in the workshops were distributed by the Gateshead Vanguard team
and the research team. Invitations were distributed to the following categories of potential
participants across Tyne and Wear, North Tyneside and Durham:
• Workforce leads in Newcastle Gateshead CCG
• Community team managers
• Community teams linked with the Pathways of Care of the Newcastle Gateshead
Vanguard programme
• Commissioners of services for older people
• Integration lead in Local Authorities
• Care home managers in Gateshead and Newcastle
• Regional managers from care home companies
• Health Education England (education commissioners)
• NHS England North, Director of nursing/independent sector, regional lead

18
Individuals that agreed to participate were requested to sign a consent form. In total 23
individuals agreed to participate in the study representing 16 organisations (including care
home companies, CCG’s, commissioning, NHS services, Local Authorities). The
involvement of employers from different organisations ensured that diverse perspectives
were brought to the discussions.
Data analysis
Data collected via post-it notes and flip charts was transcribed in preparation for analysis.
Content analysis was used to systematically categorise the data and capture the themes and
main ideas expressed during the group activities (Mayring, 2000).

19
4: Findings 4.1 Phase 1, strand 1
Learning
Participants were asked about their actual and preferred methods of learning. The following
figures illustrate these methods at each competency level:
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%
Specificcourse
providedexternally
In house Shadowing E learning Work-basedlearning
Blendedlearning
Personalstudy
Figure 4: Essential: Methods of learning: actual and preferred
Actual courses Preferred courses
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%
Specificcourse
providedexternally
In house Shadowing E learning Work-basedlearning
Blendedlearning
Personalstudy
Figure 5: Specialist: Methods of learning: actual and preferred
Actual courses Preferred courses
20
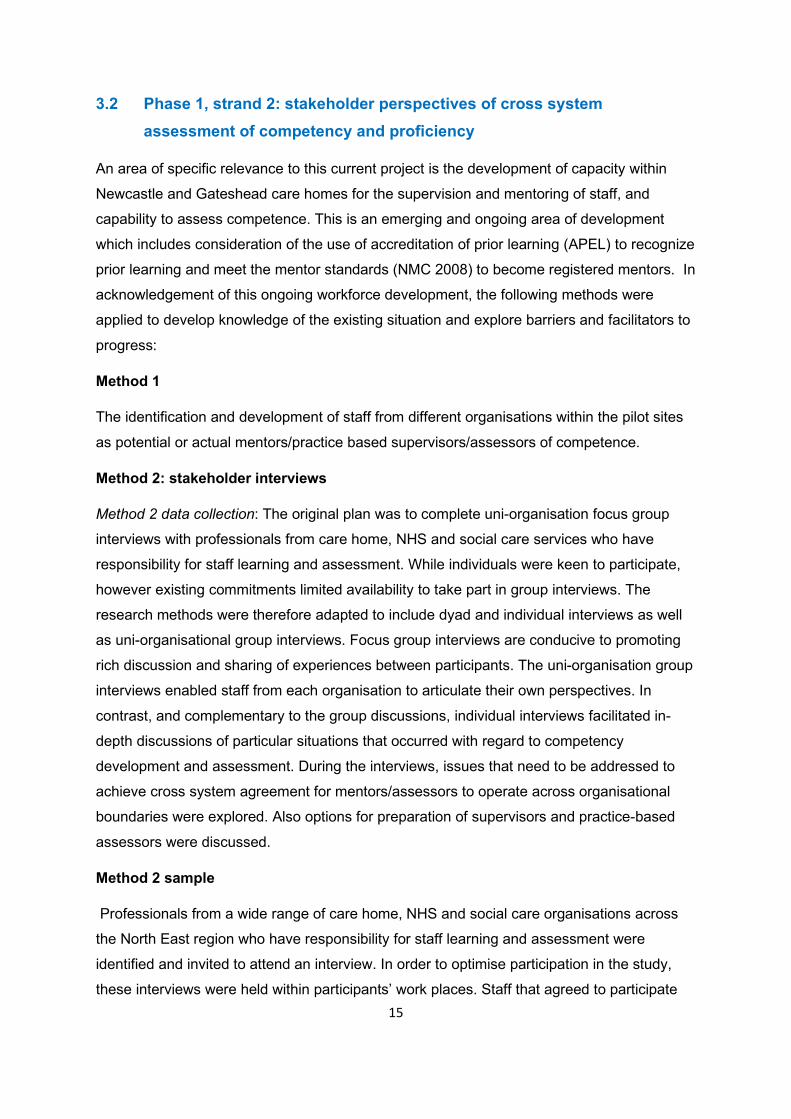
The findings show that:
• External and in-house learning rates were between 50% and 65%, but preferred
rates were between 30% and 50%.
• Shadowing rates were between 0% and 50% but preferred rates were between 50%
and 100%.
• E-learning rates were between 80% and 100% but preferred rates were between 0%
and 30%.
• Personal study rates were between 0% and 100% but were not preferred by any
group.
• Worked based learning rates were between 0% and 10% but this was a highly
popular learning method with preferred rates between 95% and 100%.
• Blended learning was reported by participants not to occur, but all participants said
this would be a preferred learning method.
The results suggest that preferred methods of learning and professional development are
not reflected in available programmes of learning or support. However, during observations
of practice, it was apparent that work-based learning does occur during the virtual ward
rounds (discussed below). It may be that participants did not recognize this as a learning
experience.
Participants were asked about engaging with learning and professional development. The
following figures illustrate these concerns at each competency level.
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
100.00%
Specificcourse
providedexternally
In house Shadowing E learning Work-basedlearning
Blendedlearning
Personalstudy
Figure 6: Advanced: Methods of learning: actual and preferred
Actual courses Preferred courses

21
0
2
4
6
8
10
12
IT skills Using thelibrary
Being in aclassroom
Writtenwork
Presenting IT facilitiesat home
IT facilitiesat work
Time tostudy
Figure 7: Essential: Concerns about learning
0
2
4
6
8
10
12
14
IT skills Using thelibrary
Being in aclassroom
Writtenwork
Presenting IT facilitiesat home
IT facilitiesat work
Time tostudy
Figure 8: Specialist: Concerns about learning

22
Time to study was a major concern for all groups with between 83% and 100% of
participants expressing concern. Although the advanced group were not concerned about IT
skills or facilities, between 25% and 35% of essential and specialist groups were, and for 7%
to 33% of essential and specialist participants, accessing IT facilities at home was a
problem. 17% of essential level participants expressed concern about being in a classroom;
between 25% and 43% of all groups were concerned about written work, and between 21%
and 42% of all groups were concerned about presenting.
These results suggest that concerns about using IT/accessing IT at home (essential;
specialist) may contribute to why e-learning is unpopular. Also, concerns about time to study
and written work/presenting even at specialist and advanced levels may contribute to why
work-based and blended learning are popular options (ie practical learning/assessment,
aspects of which could be integrated within the working day).
Participants were asked whether a recognised qualification in the care of older people with
complex needs was important. The following figures show the responses at each
competency level:
0
0.5
1
1.5
2
2.5
3
3.5
IT skills Using thelibrary
Being in aclassroom
Writtenwork
Presenting IT facilitiesat home
IT facilitiesat work
Time tostudy
Figure 9: Advanced: Concerns about learning
23
0
2
4
6
8
10
12
14
16
Recognisedqualification
Recognitionprior skills
Newknowledge
Careerprogression
Improving care Improvedconfidence
Influencechange
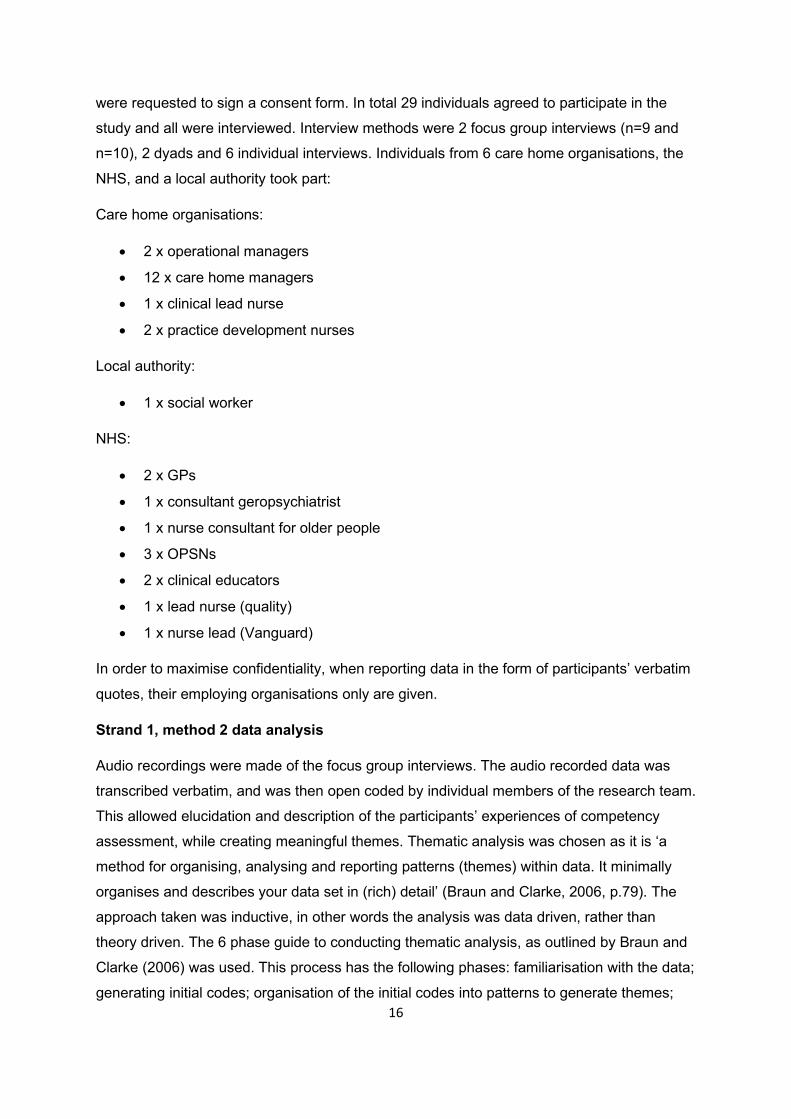
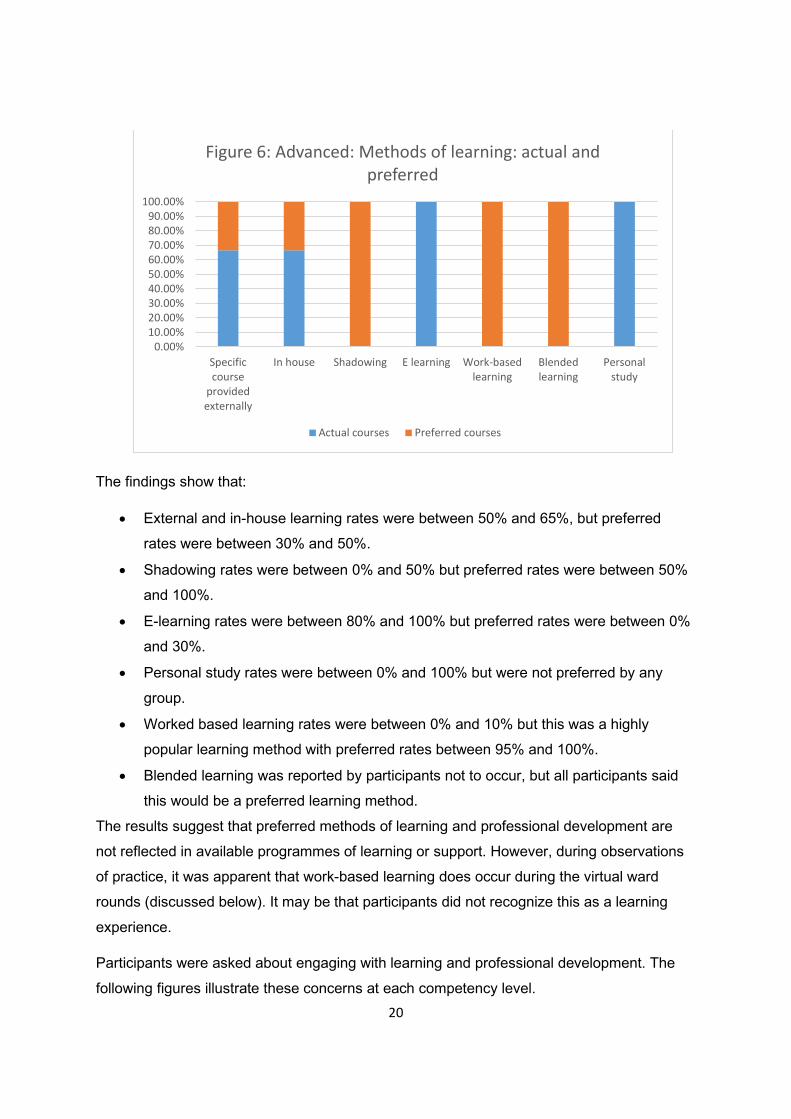
Figure 10: Essential: Importance of a recognised qualification in care of older people with complex needs
Important Not important
02468
101214161820
Recognisedqualification
Recognitionprior skills
Newknowledge
Careerprogression
Improving care Improvedconfidence
Influencechange
Figure 11: Specialist: Importance of a recognised qualification in care of older people with complex needs
Important Not important

24
87% essential level participants, 78% specialist level participants and 100% advanced level
participants said having a recognised qualification in the care of older people with complex
needs was important as a means of developing new knowledge, improving care, improving
confidence, recognising prior skills, influencing change, and career progression.
Competency
Location and competency
Comparisons of location and competency domains/sub-domains showed that at the
essential level, ‘teaching, learning and support’ (mean rank = 21.17) was found to score
statistically significantly higher in location A (U = 43.5, p = 0.01) than location B, as did
location A’s ‘leading, organizing and managing care’ (mean rank 24.5, U = 80, p = 0.03).
This may be due to the inclusion of nursing assistants in the location A sample only. The
care home in location B did not employ nursing assistants.
Comparisons of location and competency domains/sub-domains showed that at the
specialist level, ‘collaborative working and communication’ (mean rank = 23) was found to
score statistically significantly higher in location A (U = 90, p = 0.005) than location B, as did
location A’s ‘assessing, planning, implementing and evaluating care’ (mean rank 22.1, U =
103, p = 0.027), and location A’s ‘management of mental health’ (mean rank 17.09, U =
49.5, p = 0.025). This may be due to the influence of location A’s virtual ward model, which
promotes interprofessional working and facilitates the upskilling of OPSNs via maximizing
0
0.5
1
1.5
2
2.5
3
3.5
Recognisedqualification
Recognitionprior skills
Newknowledge
Careerprogression
Improving care Improvedconfidence
Influencechange
Figure 12: Advanced: Importance of a recognised qualification in care of older people with complex needs
Important Not important
25
learning opportunities between consultants and nurses; the availability of OPSNs working at
a higher competency level; and because RN staff working in the care home in location A
includes some RNs with mental health expertise.
Comparisons of location and competency domains/sub-domains showed that at the
advanced level (NB small sample), ‘improving’ (mean rank = 10.17) was found to score
statistically significantly higher in location A (U = 4, p = 0.01) than location B, as did location
A’s ‘communicating with patients and families’ (mean rank 10.17, U = 4, p = 0.006), location
A’s ‘pharmacology’ (mean rank 8.4, U = 1, p = 0.009), and location A’s ‘promoting
independence and autonomy’ (mean rank 6.83, U = 1.5, p = 0.047).This may be due to the
inclusion of consultants within the workforce model for location A.
Organisation and competency
All participants working at essential level were non-NHS employees.
Comparisons of organisation and competency domains/sub-domains showed that at the
specialist level, NHS staff were found to score statistically significantly higher than non-NHS
staff:
• Teaching learning and support – mean rank 19.23, U = 65.5, p = 0.025
• Improving care - mean rank 21.79, U = 42, p = 0.000
• Communication with patients/families - mean rank 20.48, U = 95, p = 0.032
• Assessing, planning, implementing and evaluating care - mean rank 22.11, U = 89.5,
p = 0.013
• Promoting holistic health and well-being - mean rank 17.12, U = 66, p = 0.049
• Dementia – mean rank 16.94, U = 52, p = 0.029
• Frailty - mean rank 17.63, U = 26, p = 0.001
This may be due to NHS staff having access to a range of education and professional
opportunities and having an infrastructure more able to support workforce competency
development.
At advanced level, there was no significant differences between organisation and
competency domains/sub-domains (NB small sample). Although results show NHS
consultants work at a higher level than other staff, NHS GPs work at a lower level so that
organisational differences in general are not apparent.

26
Highest academic level and competency
Although some essential level participants had ‘A’ levels, and some specialist level
participants had Master/Bachelor level qualifications, there was no statistical significance
between highest academic level and competency for essential and specialist level
participants. There was a negative relationship between highest academic level and some
competency domains/sub-domains at advanced level (NB small sample):
• Communication with patients/families - negative relationship (rho(3)=-1) and is
statistically significant (p=0)
• Assessing, planning, implementing, evaluating care - negative relationship (rho(3)=-
1) and is statistically significant (p=0)
• Promoting independence and autonomy - negative relationship (rho(3)=-1) and is
statistically significant (p=0)
• Promoting holistic health and well negative relationship (rho(3)=-1) and is statistically
significant (p=0)
• Mental health - negative relationship (rho(3)=-1) and is statistically significant (p=0)
In this case, staff with level 5 qualifications that focused on care home management had
higher competency levels than staff with Masters’ degree qualifications in subjects not
specifically related to care homes or care of older people.
These results suggest that programmes of learning and development need to be relevant if
they are to enhance competency in the care of older people.
Collaborative working and clinical competencies
Correlational comparisons between competency in collaborative working and clinical
competencies showed positive relationships in all areas and these were statistically
significant positive relationships as follows:
For essential level participants:
• Assessing, planning, implementing, evaluating care - rho(35)=0.696, p=0.000
• Pharmacology - rho(35)=0.533, p=0.023
• Promoting independence and autonomy - rho(35)=0.525, p=0.01
• Promoting holistic health and well being - rho(35)=0.552, p=0.001
• Dementia rho(35)=0.672 p=0.000
• Mental health rho(35)=0.652 p=0.005
• Frailty rho(35)=0.808 p=0.000

27
• End of life care rho(35)=0.721 p=0.001
For specialist level participants:
• Assessing, planning, implementing, evaluating care - rho(35)=0.718, p=0.000
• Promoting holistic health and well being - rho(35)=0.606, p=0.001
• End of life care rho(35)=0.477 p=0.021
• For advanced level participants:
• Assessing, planning, implementing, evaluating care - rho(16)=0.546, p=0.035
Teaching, learning and support and clinical competencies
Correlational comparisons between competency in teaching, learning and support and
clinical competencies showed positive relationships in all areas and these were statistically
significant positive relationships as follows:
For essential level participants:
• Assessing, planning, implementing, evaluating care - rho(28)=0.717, p=0.000
• Pharmacology - rho(28)=0.773, p=0.000
• Promoting independence and autonomy - rho(28)=0.513, p=0.004
• Promoting holistic health and well being - rho(28)=0.757, p=0.000
• Dementia rho(28)=0.745 p=0.000
• Mental health rho(28)=0.689 p=0.002
• Frailty rho(28)=0.756 p=0.001
• End of life care rho(28)=0.771 p=0.000
For specialist level participants:
• Assessing, planning, implementing, evaluating care - rho(28)=0.464, p=0.009
• Frailty rho(28)=0.606 p=0.001
For advanced level participants no domain is statistically significant.
Leadership, organisation and management and clinical competencies
Correlational comparisons between competency in Leadership, organisation and
management and clinical competencies showed positive relationships in all areas and these
were statistically significant positive relationships as follows:
For essential level participants:
• Assessing, planning, implementing, evaluating care - rho(35)=0.659, p=0.000

28
• Pharmacology - rho(35)=0.610, p=0.006
• Promoting independence and autonomy - rho(35)=0.449, p=0.007
• Promoting holistic health and well being - rho(35)=0.625, p=0.000
• Dementia rho(35)=0.593 p=0.002
• Mental health rho(35)=0.8 p=0.000
• Frailty rho(35)=0.668 p=0.003
• End of life care rho(35)=0.8591 p=0.000
For specialist level participants:
• Assessing, planning, implementing, evaluating care - rho(35)=0.431, p=0.011
• Pharmacology - rho(35)=0.369, p=0.049
• Promoting independence and autonomy - rho(35)=0.431, p=0.018
• Dementia rho(35)=0.535 p=0.003
• Mental health rho(35)=0.505 p=0.008
• Frailty rho(35)=0.586 p=0.002
For advanced level participants no domain is statistically significant.
These results suggest that higher levels of competency in collaborative working, teaching,
learning and support and leading, organising and managing is associated with higher
competency in clinical practice. This is particularly significant at essential and specialist
levels.
Competency gap analysis and priority areas for development
Essential: The mean combined self-reported and observed competency scores for all
essential level participants are illustrated in figure 13:

29
Strong areas were: values and attitudes; communication with patients and families;
promoting and supporting independence and autonomy. Weak areas were: teaching,
learning and support; improving care; assessing, planning, implementing and evaluating
care; pharmacology; dementia; mental health; frailty; end of life care.
A review of the trends for occupational roles included in the essential level group reflected
the combined group trend in that results for health care assistants and nursing assistants
showed similar areas of strength and weakness.
2
2.5
3
3.5
4
4.5
5
Figure 13: Essential: Self reported and observed competency
Mean
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas
30
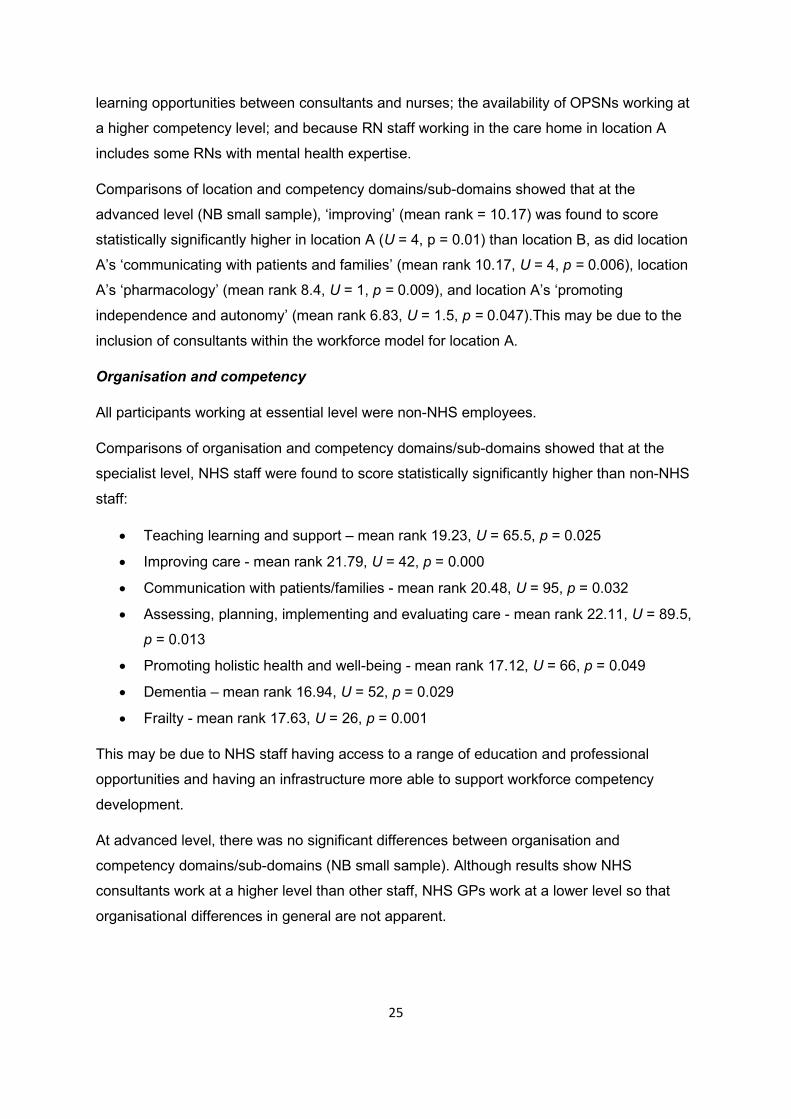
However, results for nursing assistants consistently showed higher levels of competence in
all areas. Only location A employs nursing assistants. These staff are recruited internally for
this role from the health care assistant workforce. Candidates have to apply for, and are
interviewed for, the role and once accepted, undertake an in house professional
development programme, which includes some work-based learning and shadowing the
management team and RNs (some RNMHs -mental health). The aim of the programme is to
develop management skills, clinical skills and skills specific to the care of older people
including dementia, mental health, frailty and end-of-life care. The non-nurse deputy
manager has undertaken professional development via informal shadowing and working with
2
2.5
3
3.5
4
4.5
5
Figure 14: Essential by role: Mean self reported and observed competency
HCA NA D Man (non nurse)
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas

31
experienced RN managers. This staff member has a number of years’ experience as a
senior carer.
Specialist: The mean combined self-reported and observed competency scores for all
specialist level participants are illustrated in figure 15:
Strong areas were: values and attitudes; inter-professional and inter-organisational working
and communication; communication with patients and families; pharmacology; promoting
and supporting independence and autonomy; promoting holistic health and well being; end
of life care. A particularly weak area was teaching, learning and support.
2
2.5
3
3.5
4
4.5
5
Figure 15: Specialist: Mean self-reported and observed competency
Mean
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas
32
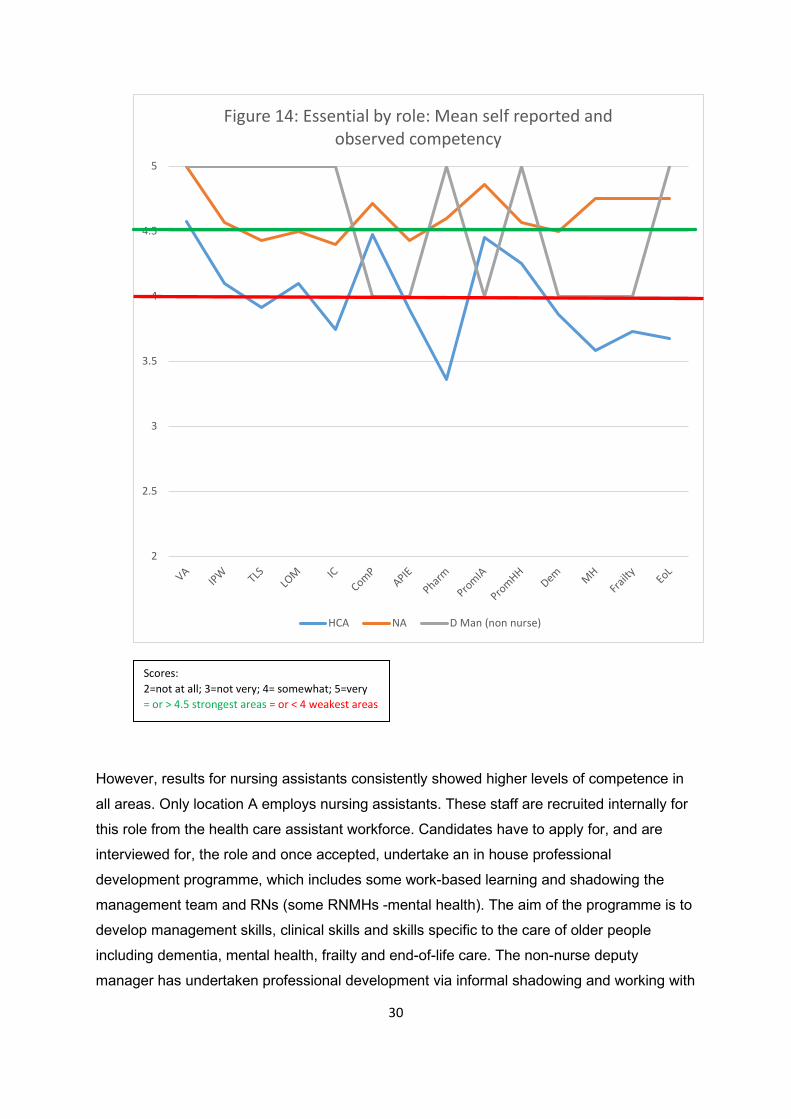
A review of the trends for occupational roles included in the specialist level group reflected
the combined group trend to an extent, although OPSN Band 6 nurses were also weak at
pharmacology, assessment, and mental health management, and consistently practiced at a
lower competency level than OPSN Band 7 nurses across all domain/sub-domains.
Observations of OPSN Band 6 nurses highlighted that while they managed ward rounds and
records GP assessment and plans, their input into assessment was limited. The group often
practiced in isolation rather than using their rounds as opportunities to teach, support and
assess learning for care home staff. There was a recognition of complex co-morbidities and
frailty, but limited recognition of the implications for medicine management or for the resident
in general. This group were strong collaborative workers in that they were effective brokers
of information between care homes and the NHS. They also had good levels of competency
in promoting independence and health and well-being, and managing dementia care.
Care home RNs required competency development in a number of areas, in particular
teaching, learning and support, leading and managing care, improving care, assessment and
2
2.5
3
3.5
4
4.5
5
Figure 16: Specialist by role: mean self reported and observed competency
OPNS6 (mean) OPNS7 (mean) RN (mean) Allied (mean)
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas

33
implementation of care, and frailty. Teaching and support was problematic for participants as
most were not registered mentors. Previous work undertaken at a local level suggests being
able to mentor student nurses contributes to practice development in care homes, as
students introduce and reinforce current evidence-based practice, and act as catalysts for
promoting closer working relationships and learning opportunities between sectors and
organisations (Tiplady, Thompson and Proud, 2018). Also, a lack of opportunities for the RN
participants’ own competency development limited how they could support other staff. Care
home RNs managed care on a day-to-day basis, but tended to rely on management teams,
GPs and OPSNs to lead care. On occasions, RNs attempted to lead care processes and
decisions but were ‘overruled’ by OPSN Band 7 nurses. In terms of improving care, some
RNs reported that they did not really see this as part of their role. Rather this was seen as
the remit of management teams and OPSNs. Care home RN participants were not generally
familiar with the process of comprehensive geriatric assessment or their contribution to this.
While they recognised and identified problems, care was at times reactive. Due to limited
access to competency development, competency assessment, clinical skills updates, and
some equipment and resources, these RNs were unable to undertake some interventions.
With regard to frailty, the RNs recognised it on an informal, intuitive basis but were not
familiar with frailty assessment or how frailty impacts on health. The care home RN
participants demonstrated a good level of competency in pharmacology. For example, they
questioned current medication regimes and initiated medication reviews, and identified
changes in residents that could be attributed to medication.
Allied health care professional participants were very strong in promoting independence and
autonomy and health and well-being, and management of frailty. Weaker areas were
pharmacology, mental health and end of life care. Development in teaching and support
competency may contribute to developing rehab skills within the healthcare assistant
workforce and the wider MDT.
OPSN Band 7 nurse participants scored means of >4.5 in most domains/sub-domains,
suggesting that they are working towards advanced level practice. This may be because
they are working at a senior nurse level and because many have undertaken development
programmes in prescribing and advanced clinical skills. This group of staff have regular
access to learning sessions during/after the ‘virtual ward rounds’. During these rounds, the
OPSN Band 7 nurse team meet with consultant geriatricians and consultant psychiatrists to
discuss patients on the round case-by-case and in detail. This not only enables collaborative
care that meets the individual needs of patients, but it is also a forum for teaching and
learning. In addition, during discussions barriers and challenges with regard to system
34
processes are identified and strategies implemented to address these. Evaluations of
services and research studies are also initiated. After the rounds, presentations and learning
sessions are provided that address issues suggested by, and therefore relevant to,
attendees. As findings suggest that this experience is a valuable method of developing a
range of competencies, it should perhaps be open to care home staff as well as NHS staff.
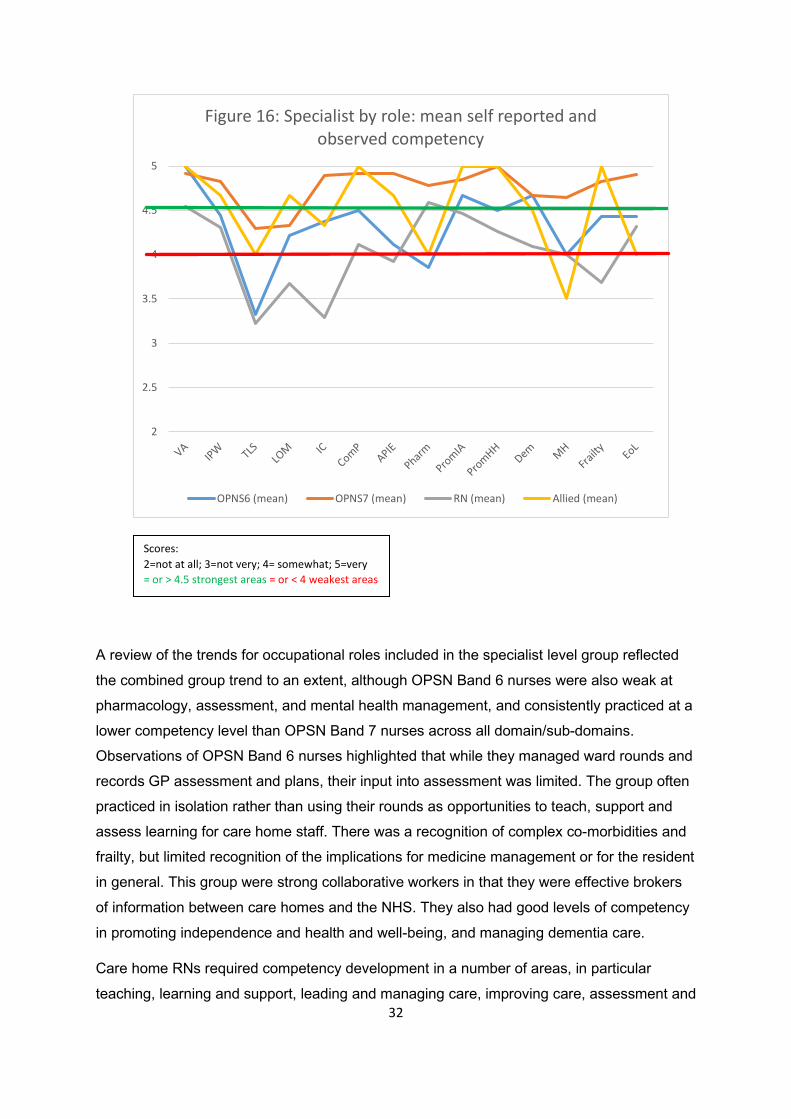
Advanced: The mean combined self-reported and observed competency scores for all
specialist level participants are illustrated in figure 17:
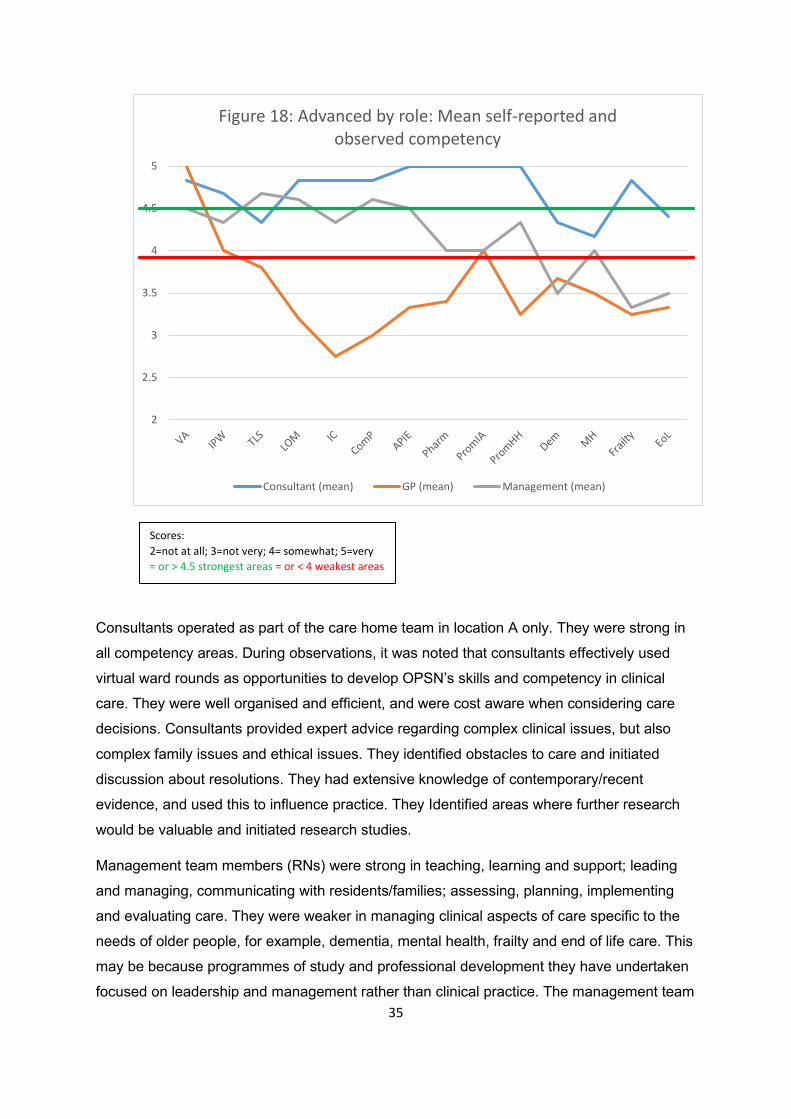
Strong areas were: values and attitudes, and promoting and supporting independence and autonomy. Weak areas were: management of dementia, management of mental health, management of frailty, and end of life care.
A review of the mean competencies for roles within the advanced level, however, showed a wide disparity in competence.
2
2.5
3
3.5
4
4.5
5
Figure 17: Advanced: Mean self-reported and observed competency
Mean
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas
35
Consultants operated as part of the care home team in location A only. They were strong in
all competency areas. During observations, it was noted that consultants effectively used
virtual ward rounds as opportunities to develop OPSN’s skills and competency in clinical
care. They were well organised and efficient, and were cost aware when considering care
decisions. Consultants provided expert advice regarding complex clinical issues, but also
complex family issues and ethical issues. They identified obstacles to care and initiated
discussion about resolutions. They had extensive knowledge of contemporary/recent
evidence, and used this to influence practice. They Identified areas where further research
would be valuable and initiated research studies.
Management team members (RNs) were strong in teaching, learning and support; leading
and managing, communicating with residents/families; assessing, planning, implementing
and evaluating care. They were weaker in managing clinical aspects of care specific to the
needs of older people, for example, dementia, mental health, frailty and end of life care. This
may be because programmes of study and professional development they have undertaken
focused on leadership and management rather than clinical practice. The management team
2
2.5
3
3.5
4
4.5
5
Figure 18: Advanced by role: Mean self-reported and observed competency
Consultant (mean) GP (mean) Management (mean)
Scores: 2=not at all; 3=not very; 4= somewhat; 5=very = or > 4.5 strongest areas = or < 4 weakest areas
36
members were innovative in supporting learning. For example, in one instance, the
management team facilitated all care staff, domestic staff and kitchen staff to complete NVQ
3 health and social care with the aims of developing a flexible workforce, allowing ancillary
staff to understand how their roles can contribute to care, and supporting career
development. Management teams also proactively engaged with education providers and
university research teams to develop ways of improving and assessing competency. One
care home management team also developed an in-house competency assessment system,
a method of cascading training, and an in house professional development programme for
nursing assistants.
A caveat regarding the findings about GP competency is that the sample size was small.
This limited sample showed that GP participants were not working at advanced level. This
may be because GPs are generalist rather than specialist practitioners, and within the care
home team, the GP role is the only role that does not specifically relate to the care of older
people with complex needs. Although these participants demonstrated leadership,
collaborative working with OPSNs and care home staff, this did not meet the advanced level
criteria. Ward rounds and encounters with OPSNs, RNs and HCAs provided opportunities for
learning and collaborative work, but these opportunities were sometimes missed. In some
instances, GP participants demonstrated limited knowledge of polypharmacy and the
implications of polypharmacy and changes in medication for frail older people. In some
instances, there appeared to be limited understanding of the care management of people
with multi-morbidity. Some interventions were ‘trial and error’ based, and some participants
strongly relied upon OPSNs to guide care decisions.
4.2 Phase 1, strand 2
This strand of the study aimed to gain insight into stakeholder perspectives of capacity,
capability and agreement for cross system practice based learning and assessment through
focus group, individual and dyad interviews; and identify and develop staff from different
organisations within the pilot sites as mentors/practice based supervisors/ assessors of
competence. A number of themes emerged from the data collected during this strand of the
study. These were: the need for a workforce competent in the care of older people with
complex needs; standardisation of competency levels across the care of older people’s
workforce; competence development; assessment of competence to practice; mentorship
and supervision.
37
The need for a workforce competent in the care of older people with complex needs
Participants’ responses suggested that having competent staff improves the quality of care
and reduces variation in the standard of care delivered, but also that having competent staff
is important in achieving resident focused outcomes.
Well obviously the benefits for the residents -it improves the quality of the
service. It also standardises the service, and the fact you’re not dependent
on somebody being on shift to what approach you get (NHS)
We need to be able to meet their needs and improve their outcomes.
Because they’re not here to die, they’re here to live… So people have to be
competent to care for residents from the day the residents comes into the
home (Care home)
Participants proposed that caring for older people requires a broad knowledge–base and a
range of competencies because of the complexity of caring for people with multi-morbidity
and frailty:
They are looking after people, who are living longer. They’re frailer. They’ve got
multiple, you know, co-morbidities. Complex care needs. And they’re looking after,
you know, a unit of 25 beds Whereas, you can have a 20-bedded orthopaedic unit,
and the 20-bedded orthopaedic unit are all hips and knees and you know what that
protocol is. The diversity of care needs within… Within the care homes is… Is
enormous (NHS).
Participants identified that having a competent workforce had benefits for the wider health
and social care system in that competent staff could assist in reducing pressure on other
parts of the system, including the prevention of avoidable hospital attendances and
admissions:
If people are getting good, person-centred, holistic care from people with the
right skills, they won’t hit the rest of the system so much, inappropriately
(NHS)
I’ve done the PEG training. Why would you let somebody wait in A&E
because their PEG has come out?... so I think the more competent we are
the better. If we can change a PEG then it prevents a hospital admission
(Care home).
38
It was also suggested that a competent workforce benefits service provider organisations by
providing evidence for Care Quality Commission (CQC) inspections, which in turn improved
CQC reports. Good CQC reports were associated with increasing resident occupancy and
associated financial benefits.
The company, at the end of the day, they are a business. And the better that
they train their staff up, the better, you know, a business, lead... You know,
at the end of the day, it’s all finance. So, it gets their grades up better, so
they’re benefitting financially. And the homes fill up. Because, as we know,
in this day and age, there is a lot of occupancy problems. And it’s usually the
homes with poor occupancies, because they haven’t got a steady stream of
nurses who are competent and carers who are competent (Care Home).
Achieving competence was also felt to be important to staff, in that this increased their self-
esteem and pride in their work:
Plus the staff, because they feel proud in themselves that they’ve learnt to
upgrade their skills (Care home).
Standardisation of competency levels across the care of older people’s workforce
Frail older people with complex health problems require care from a workforce that is
proficient in personal care, enablement, management of complex multimorbidities, acute
deterioration and interventions in emergency situations. No-one individual or individual
service can manage this alone, hence input from multiple professionals occur. A number of
participants indicated that in order to achieve quality multi-professional working,
standardisation of competency across the whole workforce needs to occur:
The benefits for the residents was that it improves the quality of the service.
And then everybody gets a good quality service. It also standardises the
service, and the fact you’re not dependent on somebody being on shift to
what approach you get. Because one of the things I thought I found is a lot
of people have, like, a training programme. Not everybody had the same
training. So, that knowledge was lost if you weren’t on shift. So, that’s why I
try to standardise it across everybody. And for the person themselves, is,
like, obviously, that they… They bring up that they’re quality nurses. But
also their self-worth as well. And they see the difference it can make with
people in their care (Care home).
39
The participants suggested that effective multiprofessional working relies on an assumed
understanding of the competence of professionals involved in patient care. This in turn relies
on an inherent expectation that there is standardisation of competencies within professional
groups. However, in the following example, it is clear that there is variation in what
individuals within a profession are proficient to do:
There should be some standards in the home as well…in terms of bloods,
some nurses can’t take bloods…I have been on a ward round and three
patients have needed bloods. It’s an agency staff member on duty who
hasn’t had ……blood taking training ticked off….so then you’ve got to get the
district nurses in to do that. And then the district nurses will say – “Oh, well,
that’s a nursing patient, the home should be providing the service to take
bloods”. It is a minefield (NHS).
Another participant highlighted that core competencies are required by different care home
resident populations:
Different competencies are required in different services caring for different
patient groups. In the unit upstairs they’ll take ECG readings, which you
wouldn’t do downstairs. They do… They’re like a hospital ward – so the
girls up there have upgraded their skills, and they use their skills downstairs
for us. But, you know, in an elderly setting – in a nursing home – you
wouldn’t be doing an ECG. But because the upstairs unit is an NHS unit that
provides services for older people who are less stable, they do. So, yeah,
they’re able to keep their skills updated, more than the staff downstairs. But
that’s the difference (NHS).
Here there is the suggestion that there could be different sets of core competencies: a)
generic across professional groups who are working at different levels of practice; and b)
specific competencies within services. This, together with the fact that many different
organisations are involved in the provision of care for older people with complex needs, has
led to different facilities and different organisations taking different approaches to developing
competency. In the following example, a care home with a rehabilitation unit focused on
competencies that promote independence:
Now, we ended up on 19 competencies. The biggest one, and it threaded
through all the other ones, was communication. Because it’s pertinent to all
of them. There was also mobility. With or without aids. Assisted and
unassisted transfers. Bed mobility. Exercise. Kitchen practice. Stair

40
practice. And then, like, some chronic conditions. Like Parkinson’s disease,
mental health... Also arthritis is another common one (NHS).
My competencies, that we’ve created, might be totally different to the care
home down the road (Care home).
It was clear that different organisations are working to identify the required competencies of
their workforce. This can lead to variation within the workforce, and when staff move from
one organisation to another often their competency is reassessed because there is lack of a
recognised standard or acceptance of previously assessed competence in another
organisation.
Some participants proposed that professional, regulatory, or commissioning bodies could
potentially have a role in determining competency standards:
And different governing bodies want things different. So, until the NMC, kind
of… Either steps up, or the commissioners step up, and this is their policies
and procedures around PEG feeding, oral medication… Every other
company is going to have completely different competencies. There’s no
baseline. There’s no set standard (NHS).
Other participants, however, identified that regulatory and commissioning bodies do have
requirements regarding workforce competency, but their requirements vary causing a
problem in itself:
In some places, the CQC don’t require anything…then the CCG in
partnership with the local authority who actually ask now, for those additional
training sessions. For example, they’ve now put... In [place name], they’ve
now asked for training on osteo and rheumatoid arthritis. That’s very new.
So, it tends to be external people who dictate what the skill should be (Care
home).
Tensions exist in agreeing the requirements of the workforce that is caring for complex older
people, particularly those living in long term care. The issue of lack of standardisation of
workforce competencies surface in many of the above extracts. Yet there is also a consistent
message that standardisation of competencies across the workforce would improve
interprofessional working and importantly care of frail older people with complex health
problems:
41
It’s about maintaining and improving the standards - that’s to benefit the
residents’ care (Care home).
Competence development
Although there is no standardisation of competency levels across the workforce, the
participants reported that their employing organisations have their own approaches to
competence development across all levels of practice. These include:
• Introductory standard education
• Role specific induction programmes
• Role modelling and shadowing
• Formal education and training (often this was non-accredited)
• Personal development plans
• Refresher sessions and up-dates
• Ongoing experiential learning
• Skill development to meet a specific resident need
• Virtual ward – case management
• Ward rounds in care homes where learning focused on individual problems and
management of complex conditions.
This range of learning opportunities could be broadly categorised as:
Initial development of competence to practice: This included introductory standard
education; role specific induction programmes, role modelling and shadowing; formal
education and training (often this was non-accredited).
An example of development of competence to practice was the introduction of nursing
assistant posts. Some organisations provided opportunities for care staff to undertake further
learning and development providing career progression to roles such as nursing assistants,
care home assistant practitioners (CHAPs), or nurse assistant practitioner (NAPs). These
roles have been developed within individual care home provider organisations, and are
generally non-accredited. Participants suggested that this initiative enhances competency
levels for the staff involved, and also has a positive effect on staff’s self-esteem and self-
worth:
Seniors felt valued that they were having some dedicated development that
would enhance their skills (Care home).
42
The difficultly with non- accredited learning is that it is often not standardised to support
achievement of a given level of knowledge or competence. Whilst it may provide career
progression within a specific organisation, the lack of transferability means it may not be
recognised in other organisations, leading to repeated learning and assessment and lack of
progression.
Ongoing personal development: This included: personal development plans; refresher
sessions and up-dates; ongoing experiential learning. An example of ongoing personal
development was the use of appraisal as a personal development tool. While there was
variation across care home organisations in the learning and development opportunities that
staff could access, in some cases, the use of staff appraisal was identified as an opportunity
to assist staff development.
And what we do - it’s in two parts. The member of staff fills their own bit in,
and then the appraiser fills the second bit in. And then you get together and
you joint agree. And then, from the joint agreement, you sign up for the
personal development plan for that forthcoming year (Care home).
Bespoke learning in response to resident/patient need: This included: skill development to meet a specific resident need; virtual ward – case management; ward rounds in care homes where learning focused on individual problems and management of complex conditions.
An example of bespoke learning in response to need was the learning and skills
development that a particular care home team completed in preparation for a resident being
discharged from hospital:
We had a gentleman who was coming in with a trachy and we hadn’t done
one for a while so we requested the ward if we could go in and do a
refresher session. So we all went up and did a refresher session (Care
home).
Whilst the existence of this range of learning opportunities suggests that there is some
infrastructure to support continual workforce development, there are problems. The majority
of participants spoke of the difficulties that they experienced in accessing learning
opportunities that would enable them to fulfil their role effectively. One of the major problems
reported relates to difficulties accessing learning opportunities and competency development
provided by the NHS. Some participants suggested this was a barrier to integrated care:
I was told who to contact for some training at the hospital. I’ve emailed and
had no response. So it’s very sad that we are meant to be integrating, yet
there is no integrated training for care home staff (Care home).

43
Another barrier reported by participants was the cost and funding of specialist courses:
There is a lot of training that stipulate NHS only. A lot of university courses-
the CPD ones you’ve got to fund yourself (Care home).
So we’ve got three sets of clinical training coming up venepuncture,
tracheostomy and catheterisation that we have to fund (Care home).
Accessing relevant learning opportunities was particularly problematic for agency and night
staff. The shift patterns of these workers often prevents engagement with learning that is
delivered during the day. Also, lack of cover for those wanting to attend training and updates
was a barrier in many instances.
There were issues raised about the differences within and across organisations including the
variation in the financial recognition that staff received. One participant noted that lack of
financial recognition in their employment could pose a barrier to engaging staff in learning
and competency development:
We’ve just said that these people need really good skills, because these are
the most complex, but we actually pay them the worst wages in the country.
But now we’re expecting them to sign up to a competency framework with
equal skills. So, that could be a huge barrier (NHS).
A further financial difficulty arose for care workers who were paid for the extra hours worked
to attend learning sessions. Some of these staff found that this could impact on their benefit
and welfare payments, which discouraged engagement with competency development
opportunities.
Assessment of competence to practice
Participants proposed that one of the most significant problems concerning the development
of a competent workforce is demonstrating proficiency in specific competencies. A number of
factors contribute to this problem. For example, some participants identified the requirement
for assessors of clinical competencies to be occupationally competent as clinicians
themselves. As many care homes employ non-nurse managers or do not have a stable RN
staff base, access to competence assessment in house can be limited:
In this home, yes. But across the company, it’s not always easy. Because a
lot of the managers are non-nurse managers. So, they’re not able to sign
them off. And a lot of the homes don’t have a cohort of nurses, so they’re
relying on agency staff. So, there is an issue as to who’s deemed them as
44
competent. No. What’s happened in the past is I’ve had phone calls,
because I’m one of the very few nurse managers, being asked can I go along
and assess their competency? Or, can my clinical leads that I have here go
across and assess their competencies for them? (Care home).
Within this company this manager or her staff often assessed the competency of staff in
other homes, which led to depletion of service in their own care home.
An alternative approach to assessment of competencies in the care home sector could be
other professionals working in sectors such as the Local Authority or NHS fulfilling this
function. One participant explained how this was working successfully in a local care home:
The other thing you’ve got to think about is, like, who signs off the
competency when you’re talking about the sign off from a different
organisation. We overcome that by involving the workforce development
officer from the local authority. To be fair, he approached me first and then
kind of was very willing and very helpful in the whole process. To try and
standardise the observations, we had, like, standardised questions. So, it
would be, like, a case of, like, what you would expect to see. And if you
didn’t see that, what questions you might ask to, like, reinforce it. So, you
might see somebody walking along and prompting somebody to use the
walking frame properly. But you wouldn’t particularly... Like, see them
checking the safety features in it. So, you would, like, ask, you know, what
are the safety features? And it probably has been done, but you mightn’t
have observed it in that time. So, it’s just, like, trying to standardise what you
want to see to be signed by somebody as competent (NHS).
In this example, rather than relying solely on observations of practice, assessors built a
series of questions into the assessment process to improve the validity of assessment and
so their assessment could extend beyond the ‘here and now’ care episode. However, in
most cases, participants said that cross-organisational competency assessment was
problematic because assessors were concerned about implications concerning
accountability arising from assessing staff from another organisation:
Because they’re employed from a different company to us. So, I have asked
them to assist, but because they’re employed by another company in the
private sector, they don’t assist, and can’t assist (Care home).

45
I don’t see them on a regular basis, doing it. So, there is a bit of a… A
dodgy… You know, like there are issues of accountability. I’m signing
somebody off, but I’m not watching them in practice all the time. I’m just
seeing that one-off session. And I know have to do… If it’s venepuncture, I
would have to observe them six times. But, I’m only seeing a snapshot. I’m
not working with that physical person all the time to be monitoring their
progress (NHS).
While this participant said that clinical activities had to be observed 6 times prior to
competency sign-off, this was not consistent across all organisations. Some participants
reported that 3 observations were sufficient for sign-off, and others suggested up to 10
observations. Defining the number of repeated observations required is an attempt to
improve the validity of assessment to ensure the person is proficient in different contexts and
situations, however reliance on numbers of observations reflects the lack of confidence and
competence of assessors to make an accountable decision regarding proficiency.
Some participants suggested that education providers do not routinely offer competence
assessment as part of their education programme. There was a range learning opportunities
that could be accessed by care home staff, however much of this provision was
predominately offering training focused on knowledge and skills development without always
assessing that knowledge and skill development had occurred and could be applied in the
practice setting. Determination of competence to practice was then left as a responsibility for
the employing organisation:
So, the nurses can go on a ten-day clinical course over three months.
They’ll do the theory. They’ll do a practice session on that day. So, if it’s…
For example, doing a catheterisation, they’ll use a model where you… You
know, you insert the catheter and everything. They’ll monitor you doing that,
but then they give you a competency framework to take away, to be signed
off by staff that are in your home, and they’re competent enough to sign off
your competencies (Care home).
Cross organisational assessment is not just problematic from the perspective of the
assessor. Being assessed by individuals working for external agencies was also of concern
due to perceived tensions in relations between health and social care organisations, but also
because the assessed may have little knowledge about the assessors’ own competency
levels:
46
It is interesting. Because, historically, the relationship between health and
social care hasn’t been the best. There’s always been that hierarchical
attitude in my view, of NHS staff coming in to care homes. And that
Cinderella service - it’s still not brushed off. And so, I think there would be a
reluctance within the care homes to be assessed by those people. But,
actually, we don’t know what their competencies and skills are (Care home).
Other barriers to competency assessment reported by participants included the time
required to assess competence and the need for this to be inherent in practice rather than an
added extra in one-off pre-determined situations:
I think that’s the big thing about it. As I said before, it needs to be part of
their daily practice, and not additional to their daily practice. Because
nobody has got time to do anything extra (NHS).
Also, assessing competency for night shift staff was problematic due to reduced opportunity
for working with those with appropriate proficiency to assess their performance.
During interviews, participants were asked to identify approaches that could be implemented
as competency assessment methods. A number of suggestions were made including:
continual observation of staff performance; self-assessment; reflective practice; audit of
practice and practice outcomes; observation and sign off of competency requirements by
senior staff; 1:1 supervision. Participants highlighted that there is a need for integrated
assessment which encompasses knowledge, understanding and the values that underpin
proficiency, not just observation of clinical activities. In order to facilitate this, and overcome
the challenges and inconsistencies apparent in current competency assessment practices,
there is a need for an integrated approach across the system. However, to increase validity
and reliability of assessment this should be underpinned with; a standardised competency
framework to enable objective assessment against agreed criteria rather than subjective
decision making, and appropriate preparation of those assessing proficiency in the principles
and practice of valid and reliable assessment (Cassidy 2009, Cowan et al 2005) with annual
update (as required by the NMC 2008). To plan and manage this at scale requires the
development of infrastructure to develop and assess the achievement of proficiency against
the mentor standards. In addition, there is need for a cross organisational agreement to
address governance issues of signing off competencies across organisational boundaries.
47
Mentorship and supervision
During the study, the following categories of individuals who were responsible for
supervision and assessment of competence were identified within the pilot sites:
Location A:
• NHS RN mentors – 1 x OPSN
• Care home RN mentors – 0
• NHS assessors of competence – 0
• Individuals with responsibility to assess competence in care homes – 2 x
management team (using an in house competency assessment framework)
• NHS practice based supervisors - 0 (consultants, GPs and allied healthcare
professionals act as supervisors for NHS staff within their own professions, but not
specifically with regard to the formalized development of competency in the care of
older people with complex needs. These professionals do not act as supervisors for
care home staff).
• Care home practice based supervisors – 2 x management team and all RNs and
nursing assistants supervise staff.
Location B:
• NHS RN mentors – 1 x OPSN
• Care home RN mentors – 0
• NHS assessors of competence – 0
• Care home assessors of competence – 0
• NHS practice based supervisors - 0 (consultants, GPs and allied healthcare
professionals act as supervisors for NHS staff within their own professions, but not
specifically with regard to the formalized development of competency in the care of
older people with complex needs. These professionals do not act as supervisors for
care home staff).
• Care home practice based supervisors – 2 x management team and all RNs
supervise staff.
In order to attain a clearer picture of mentorship and supervision beyond the 2 pilot sites,
phase 1, strand 2 interview participants were asked about their experiences within the care
home setting of these activities. It was noted that during the interviews, participants holding a
nursing qualification used the term ‘mentorship’ when discussing the support of student
nurses, but ‘supervision’ when discussing the support of staff. Other groups used the term
48
‘supervision’ in relation to both students and staff. There was also awareness that to assess
the practice of student healthcare professionals, assessors usually have to be a registered
assessor (for example, an NMC registered mentor), although this is not the case with regard
to assessment of competency for staff.
All participants identified that mentorship/supervision was part of their role. However, there
were variances in how prepared participants were for this aspect of their role, particularly
with regard to care home staff. A few care home staff felt very well prepared:
I have completed my mentorship module with [university name] and also
completed an internal supervision training course with a previous employer.
Recently, the company has developed a mentorship induction program that I
have received training on. This includes both face-to-face sessions and an e
learning module. The training I have received regarding mentorship has
prepared me well to support colleagues and students (Care home).
For this participant, their current employing organisation provides a development programme
for mentorship/supervision. However, many care home provider organisations neither
provide such programmes, nor engage with education providers who do provide them.
Participants suggested that this may be because until recently, care homes did not host
student nurses in this region, so as NMC registered mentors were not much required in
these settings, formal mentorship/supervision development programmes have not been
deemed necessary. For care home staff, this has resulted in either there being no
opportunity for development in this area of practice, or in staff having to rely on
mentorship/supervision skills they developed in previous roles (without required annual
update), or via informal experiential learning which does not necessarily lead to achievement
of the NMC mentor/assessor standards (2008) :
I am a registered NMC teacher and mentor, but if I had not had all my
previous experience of working as a senior lecturer in university and practice
within clinical settings then the role would have been harder as I have had no
support to do this from the company (Care home).
With regards supervision, this is something I believe I had an awareness of,
due to personally receiving supervision over the years, however I think this is
something I have learnt and developed through experience rather than a
formal supportive structure (Care home).
49
Despite the lack of opportunities to develop mentorship/supervision skills within care home
settings, the participants were mindful that regulatory and professional bodies have
expectations that formal supervision takes place:
Supervision is a national… It’s through CQC guidelines as well that we have
to all have a supervision every eight weeks. That is six supervisions a year,
and an appraisal once a year as well. They’re CQC requirements under the’
well-led’ section (Care home).
However, although CQC have determined regulations regarding minimum numbers of
supervision sessions, different organisations and even different care homes within the same
organisation, had their own methods of carrying out supervision. Some participants stated
that supervision was little more than a ‘tick box’ exercise, others worked in care homes that
held more sessions than the CQC recommendations, others used formal appraisal-like
supervision sessions, while others used the sessions as a means of reflecting and
developing practice skills.
A number of participants did acknowledge the benefits of supervision, viewing it as a
valuable method of improving care practices. Some suggested that supervision provides an
opportunity to reflect on what is working well, and to explore areas where improvements
could be made. Supervision could provide a learning opportunity to discuss required
standards of practice:
We have just had a supervision between the two of us, about how best to
deal with comments from professionals that would improve the care on a
day-to-day basis. So following supervision that becomes the manager’s
responsibility, in terms of leadership within his home, my responsibility to
support him to do that. Informal supervisions don’t tend to happen for
negative things. These can be about improving the care (Care home).
The home manager actually chooses a policy a month and do that within
supervisions (Care home).
Some participants suggested that group supervision sessions provided opportunities to
review practice against national and professional standards with a view to ensuring best
evidence-based practice, and instilling professional values:
It’s about being able to set up professional supervision groups with the
nurses to look at trends that are happening in the home. To look at new
developments from either the NMC or the NICE guidelines. To make sure

50
that we’re actually doing best practice. It’s also about, importantly, talking to
carers. And when I’m in the homes, making a point of hopefully getting a
group of carers together to talk about those core professional values of the
need for respect, kindness, compassion when caring (care home).
Supervision was also highly valued by participants as a means of supporting individuals’
clinical skills practice. Participants proposed that if skills are not practiced regularly, staff can
lose confidence and proficiency. In these situations, participants said peer support and
clinical supervision are welcomed:
We kind of continuously assess each other and support one another. For
example, at the weekend, I had to erect a syringe driver. And, yes, it’s been
maybe a couple of months since I did one. You know, I still read it, but I had
the support of another colleague who supervised me initially. I was quite
confident - it was just that added backup. You know, support for each other
is important. So, I think we do continuously support each other with every
task that goes on in the home (Care home).
The interview findings clearly reinforced the need to develop mentors/supervisors/
assessors of competence who are readily available in organisations, work in a standardised
way to: eliminate variation in competency development; capitalise on good competency
develop practices already utilised; and ensure capacity for developing competence in the
care of older people with complex needs in both the current and future workforce. Within
the pilot sites, the research team aimed to achieve this via provision of appropriate
preparation (delivered in the practice setting, with backfill for care home staff) to enable
evidence based supervision, coaching and assessment of competence that is valid and
reliable using the EnCOP competency framework. For staff at specialist and advanced
practice level, this was to be via enrolling on a nationally recognised credit bearing module
(facilitating learning and assessment in practice offered at level 6 or 7), or accreditation of
prior learning (APEL) against the module learning outcomes. For senior support workers
this was to be a bespoke course (non-credit bearing) at the appropriate level to enable
evidence based supervision, coaching and assessment of competence that is valid and
reliable using the EnCOP competency framework. Undertaking these modules would
enable staff to be registered as an assessor on the Northumbria University mentor data
base (wherever they are employed) and offered annual updating. It would also enable staff
with professional registration to use this learning and development as evidence for
revalidation purposes.

51
Due to contractual delays, the study did not commence until mid December 2017. This
meant that in order to achieve the deadline, the study had to be completed within 2.5
months. Time was reduced further due to the Christmas and New Year period, during which
research staff were unavailable due to statutory leave, and commencing programmes of
study was not a priority for either NHS or care home staff. As a result, it was not possible to
deliver a bespoke course for senior carers before the submission deadline for the report.
However, the course is planned for delivery in the 2 pilot sites in March 2018.
With regard to modules for advanced and specialist practitioners, staff working in the pilot
sites who were not registered mentors were invited to enrol onto Northumbria University’s
mentorship course for professional practice with a view to either undertaking the mentorship
module, or obtaining accreditation for their prior experiential learning (APEL). However,
enrolment onto widely available modules was delayed due to difficulties in accessing funding
from Health Education England North East (HEENE). HEENE’s (2017) ‘widening access
policy’ for continuing workforce development states:
This policy requires individual organisations to register with HEE as
approved to access CWD provision. This will involve providing details of their
organisation, a key contact and to state they acknowledge and accept the
conditions of accessing continuing workforce development via the application
form for non-NHS staff to access the HEE funded post-registration education
provision. Once the application form has been returned and approved, this
will allow non-NHS employees to apply for HEE funded CWD provision.
Once organisations have registered, they will appear on an approved list of
widening access organisations. When universities receive applications from
non-NHS employees, universities will verify that applicants’ employers have
signed up to the policy before processing applications… Organisations that
choose not to register with HEE will not be able to access post-registration
education and training or any provision commissioned by HEE (HEENE,
2017).
The process required to register with HEE proved difficult to achieve for the pilot care home
sites. This was because managers were unsure who from their organisations was
responsible for registering and acting as the key contact. Regional and operational
managers of the pilot site organisations were not aware of this requirement, and requested
more information and time to consider how best to meet these requirements prior to
registering. The research team liaised with teaching and support staff from Northumbria
University’s ‘Mentor/Education Preparation’ programme and found that this situation was

52
not unique to the 2 pilot sites. A number of care home staff had recently attempted to enrol
onto the mentorship programme (since the recent introduction of student placements in
care homes), and had faced similar challenges in accessing HEENE funding.
Once the registration process was recognised as a barrier to enrolment on mentorship
programmes in the North East of England, HEENE rescinded this requirement. Hence, from
late January 2018, to gain access to funded mentor courses there is no requirement to
apply to HEENE for funding by non-NHS organisations or individuals. Individuals now
directly apply to a North East university of their choice, and once the application is received
by the university’s programme support team, it is checked to ensure that the individual’s
employing organisation offers placements on pre-registration health programmes. If this is
the case, the university can offer a place on the module under their HEENE contract. Since
the registration requirement was rescinded, staff from the pilot care home sites have
applied for mentorship modules, and will commence their study or APEL process in March
2018.
Preparation of care home staff to enable them to provide evidence based supervision,
coaching and assessment of competence was also facilitated by means of mentor updates.
The research team identified individuals who had been mentors in previous roles, but
whose mentor registration had lapsed once they were employed by care home provider
organisations. There were no such staff in the pilot site care homes, but a number of staff in
this situation were identified across the region. These staff were offered mentor update
sessions so that they could re-enter the mentor register. To-date, 8 staff have received
updates, and a further 14 are planned for March/April 2018.
In January 2018, Northumbria University employed 2 practice education facilitators who
work in private, independent and voluntary sector organisations (PIVO). These staff are
responsible for developing a register of mentors in the care home sector, contribute to
recruiting care home staff to the mentorship programme which can be completed by formal
study or APEL of prior experience against the module outcome and support academic staff
with module delivery or APEL for this sector. They also support staff to maintain mentor
registration by offering annual mentor updates required by the NMC, and for a range of staff
working in, and into, care homes.
4.3 Phase 2
The post-it note and flip chart data were initially transcribed and entered into an
internet application to create a Wordle. Wordles, or word clouds, produce a visual

53
representation of the text, giving greater prominence to the most frequently used
words in records of the discussion that took place during the workshops. This
provided a basic understanding of the data. ‘Need’ featured prominently in this
visual representation, reflecting the participants’ overwhelming view that the status
quo cannot be maintained; and that there is a pressing need for a strategy to
develop an integrated approach to workforce development for enhanced care for
older people. This included significant discussion of approaches to learning,
assessment of practice, and determination of competency and proficiency. These
issues were frequently discussed across all levels of practice including direct care,
specialist levels within the whole system (see figure 19, stakeholder workshop
Wordle).
Figure 19: Stakeholder workshop Wordle
The Wordle highlights the diversity of topics that were explored in the workshops. These
discussions were rich, with participants offering different perspectives on complex issues.
There was also learning within these discussions when participants shared current initiatives
for competence development of their staff, barriers to accessing accredited education, and
funding. These discussions are captured in the following sections – challenges, solutions
and funding options.

54
Challenges
The workforce required to care for older people with complex health problems sit across
multiple statutory and independent sector organisations. This is a large and diverse
workforce that will increase with the ageing society. There is now an increase in the oldest
old, and there is a direct relationship between advanced older age, multimorbidity, frailty and
end-of-life. This population requires a workforce that is integrated across health and social
care and across sectors, yet there is a lack of a collaborative approach to workforce
development across all services caring for older people. Also, there are not enough people
who are proficient in in the delivery of essential, specialist and advanced levels of practice
within the EnCOP framework to provide care for older people with complex needs. There is
an urgent need to upskill across and within the workforce, with particular attention to care
home nurses, health care assistants and GPs to manage complex older people who are
living in care home settings and other types of supported housing. Whilst clinical supervision
provides good opportunities for learning, there is a short fall in supervision for care home
managers. This is a national problem that requires solutions that work within localities.
Workshop participants stressed their concern that the majority of resources for developing
professional competency are available to NHS professionals, but not to the non-NHS
workforce. While participants acknowledged that there is funding available for non-NHS staff
education (for example HEENE ring-fence 10% of their funding for non-NHS education),
there remains significant competition within the independent sector for access to
commissioned CWD. It was also highlighted that many organisations are unaware of this
funding, and those that are aware are unsure of how to access it, or they find the process of
applying for it complicated, and therefore a barrier to access.
There were many illustrations of care home staff not being able to access relevant
education. They acknowledged that learning opportunities do exist, but the challenge rests in
the limitation of learning options that are accredited, result in competency development and
proficiency and are provided in a way that is accessible, eg practice based. In the main,
education provider companies focus on knowledge development rather than competence
development. For an integrated approach to workforce development, there needs to be a
shift towards competence development.
The complexity of the care home sector adds to the challenge of adopting a whole system
integrated approach to workforce development. The size of care homes and diversity of care
home organisations impact on education provision – with some offering an extensive in-
house suite of learning opportunities and others accessing courses provided by a range of
55
external education providers. This diversity of education offered contributes to a lack of
standardisation, not only of the education provision but the quality of learning opportunities.
The following issues were highlighted by participants:
• Competence to practice is not agreed across the older people’s workforce
• Assessment of competency is not standardised, leading to concerns about validity of
the assessment where this does occur
• There is no standardised approach for agreeing when staff are proficient.
• There are no agreed processes to ensure the reliability of assessment of both
competence and proficiency.
• There is no standardised approach to ensure staff maintain their proficiency through
regular updating and supervision.
There are gaps in the current learning opportunities offered and there is an opportunity with
the availability of new funding streams to address gaps. Participants agreed that this should
be through a system based approach with an agreed method determining proficiency against
the EnCOP competency framework for the older people’s workforce. This is not easy and will
require new ways of working and cultural change across large complex sectors. There are
barriers, including different organisational priorities, varying governance arrangements, lack
of clarity of use of the available funding steams such as the apprenticeship levy and barriers
accessing CWD funding.
Solutions
When discussing the challenges that are currently faced regarding workforce development,
workshop participants readily identified solutions. Some of these would require system-wide
change to support integrated working across sectors. Other solutions concerned the learning
offered. There was general agreement that there should be a move away from the existing
model of training, to approaches that support competency development and proficiency
maintenance. These ideas were captured in the notes made by the facilitators. The following
present’s key points that were recorded during these discussions and these are explored in
the discussion and recommendation sections of this report.
Whole system approach to integrated workforce development • A standardised whole system approach to workforce development should be adopted
within localities and region-wide. • Make recommendations to regional commissioning groups and commissioners, STP
neighbourhoods and communities group, Closer to home and Frailty leads for an integrated whole-system workforce development approach.
• Services and organisations should work together across operational boundaries to
56
define workforce development requirements through assessment of community profiles.
• Establish a ‘community of practice’ to develop a joined up learning offer for all levels of practice.
• Appoint a designated body or workforce development lead with a remit of co-ordinating workforce development across providers.
• Explore options for a transactional approach to commissioning that is based on outcomes, adds value, and commissions for capacity (this may optimise the role of contracts in supporting the development of the workforce).
• A system-wide framework for workforce development for the care of older people with complex needs should be integrated into commissioning and regulatory processes.
• Build on successful models such as OPSN working in nursing homes to other sectors such as OPSN working in residential care homes.
Sign up to EnCOP across organisations and boundaries • Adoption of the EnCOP competency framework across health and social care
systems to support staff to develop competence at different levels of practice. • Transform job descriptions and align to the EnCOP framework. • Develop an infrastructure for delivery and competence development and proficiency
maintenance that is aligned with the requirements of regulatory and professional bodies.
• Benchmarking and standardise specialist practice across all localities. • Identify carer learning requirements, and provide opportunities to develop and
recognise their knowledge and skills. • Agree a policy for the assessment of proficiency and ‘sign-off’ of competencies that is
recognised across organisational boundaries. Provision of an enhanced learning offer that is accessible to the older people’s whole workforce
• Learning should be based within a locality to optimise the fit with local workforce requirements.
• An integrated learning portfolio should be established and available across a locality. • Reduce variance in current education provision and standardize to match the EnCOP
framework. • Adopt a strategic approach to apprenticeships at all levels of practice of the EnCOP
framework including: o Consideration of using or adapting the current Associate Nurse
apprenticeship in the care home sector o Development of a trailblazer group to explore potential for new apprenticeship
standard for Specialist Practitioner in the care of older people with complex needs.
o Explore potential of Advanced Clinical Practitioner apprenticeship o Shared learning across organisations that taps into existing expertise,
enhances understanding of everyone’s role and increases learning. • Enhance the interprofessional learning offered in all localities.
57
• Opportunities for regular updates to support proficiency maintenance that reflects and integrates new advances in practice.
• Specialist learning programmes to enhance competencies of care home nursing staff, managers and GPs for managing the care of complex older people.
• Certificates of attending training need to be backed up by assurance of competence.
Recognition of competence and proficiency across older people’s services • Explore the feasibility of adopting ‘Passports of competency,’ or ‘Passports to
practice’ within the workforce. • Investigate if these passports would be welcomed by employers. • A ‘Brief profile’ or ‘WFD one page profile’ could be used by health and social care
staff working into care homes to evidence their knowledge, skills and competencies.
Assessment of competence and clinical supervision • A system-wide framework for assessment of competence and proficiency should be
agreed • In-house education providers should assess competency and proficiency provided
consideration is given to addressing validity and reliability • Appointment of practice educators who work across sectors and services • NHS organisational staff could provide support to registered nurses across providers
for clinical supervision and vice versa • Build competence development into coaching and appraisal of roles • Standardise assessment of competence across professions for all competency levels
Approaches for the delivery of the learning offer
• Practice-based approaches to learning and competence development should be adopted.
• Practice-based learning should replace off-site education wherever possible unless the education would be enhanced (for example by access to simulation facilities) .
• Integrate routines practices as opportunities for learning: o Ward rounds in care homes are effective in the development of competence. o Making every contact count as a learning opportunity. o Virtual ward rounds as learning opportunities across all levels of practice.
• Blended learning should be considered to optimise the benefits of face-to-face and e-learning for those working in care homes.
• Practice based learning could be supported by teams of practice educators. enabled to work across organisational boundaries within the geographical locality
Access to the learning portfolio
• Ensure that care home staff understand what specialist care courses are provided by HEI.
• Information should be made available to care homes about processes for registration for access to funded education provided by HEIs.
58
Funding options: opportunity and issues
There was much discussion about the types of revenue streams to support workforce
development, what the funding could support and how to access funding. Hence there is
clearly a need for information to enable employers and commissioners to make decisions
about workforce requirements. Key issues that were highlighted were:
• There is a need to understand how employers are spending their apprenticeship levy, what success has been achieved regarding levy spending, and what competency gaps exist after spending the levy (some employers are spending their levy on practice levels 2 and 3; up-skilling deputy and care home managers; creating a skills academy).
• There is a need to explore other sources of funding to support workforce development including the European Social Fund; Better Care Fund (if it could be demonstrated that this would improve outcomes); HEE commissioned CWD provision under widening access policy
• Influencing the commissioning of CWD that is aligned with the development of a proficient workforce rather than the provision of training.
Reach and significance
The workshop participants argued that an integrated approach to development of the older
people’s workforce is urgently required. Local solutions can be developed, however there is
a real need to share what works within localities in order to impact on the quality of care for
older people nationally. A career framework that works across sectors and service provision
could be explored by both employers and professional bodies. Workshop participants
highlighted that workforce development is a national issue that requires effective locality
based solutions.
59
5: Discussion Competency gap analysis
Findings from the study in two care home sites identified areas for competency development
for all 3 competency levels:
Essential level: All competency domains/sub domains require development, although
participants did demonstrate strengths in values and attitudes, communication with
residents/families, and promoting independence, health and well-being. Priority areas for
development are:
• Teaching, learning and support
• Improving care
• Assessment, planning, implementation and evaluation of care
• Pharmacology
• Management of dementia
• Management of mental health
• Management of frailty
• End of life care.
Specialist level: The primary priority area for development is teaching, learning and support.
Specialist level practitioners need to develop and practice mentorship, teaching, and
assessment of competency skills if the competency of the workforce at large is to be
developed and maintained, not only for the present, but for the future.
OPSN Band 7 nurses demonstrate high levels of competency across most specialist level
domains/sub domains. To enhance competency to advanced level, an advanced
professional development programme is required.
OPSN Band 6 nurses and care home RNs require development in all areas to ensure their
skills and competencies address the needs of older population with complex co-morbidities
and frailty. Priority areas for OPSN Band 6 nurses are:
• Teaching, learning and support
• Assessment, planning, implementation and evaluation of care
• Pharmacology
• Management of mental health.
Priority areas for RNs are:
60
• Teaching, learning and support
• Leading, organizing and managing care
• Improving care
• Assessment, planning, implementation and evaluation of care
• Management of mental health
• Management of frailty.
Care home RNs require competency development in leadership and improving care to
enhance their ability to address issues around resourcing and equipment acquisition, and
improving care systems, as well as care management. However, NHS staff need to
recognize and value their input i.e. allow and enable care home RNs to lead care.
Advanced level: The sample size for advanced level competency was small, which
compromises validity of the findings. However, within the small sample, consultants
demonstrated advanced competency in most domains/sub domains. Partnership working
between consultant geriatricians and consultant psychiatrists maximized provision of a
comprehensive advanced service. During the virtual ward rounds, consultants were able to
support competency development of OPSN Band 7 nurses. GPs and care home staff were
not in attendance during these observations. Similar events attended by consultants, GPs
and care home staff may be useful.
Management team participants demonstrated competency in the care domains of values and
attitudes; collaborative working; teaching, learning and support; leading, organizing and
managing, and improving care. They demonstrated competency in assessment. Clinically
based skills required further development. This may be because current professional
development programmes for managers focus strongly on leadership and management. An
advanced practice programme, which includes clinical care specifically to address the needs
of older people may therefore be beneficial. Priority areas for management team members
are:
• Pharmacology
• Promoting independence and autonomy
• Management of dementia
• Management of mental health
• Management of frailty
• End of life care.

61
GPs who participated in this study were not working at advanced level practice in any
domain/sub domain. They require development in all areas. This may because they are
generalist practitioners rather than having specialist/advanced knowledge in caring for older
people with complex needs. The RCGPs and RPS have developed an accredited ‘GPs with
a Special Interest (GPwSI) framework for developing competency in the care of older
people, which could be used to enhance skills in this practice area (RCGP, 2018). This
programme was developed independently of EnCOP, and as workforce development
progresses in the future there is the potential to align GpwSI and EnCOP. Alternatively, new
professional development programmes could be developed based on the EnCOP framework
to standardise competency in the care of older people across roles and sectors irrespective
of role.
Learning
The findings suggest that preferred methods of learning and professional development were
not reflected in available programmes of learning or support. E-learning was used widely, but
was the least popular learning method. Externally provided and in house programmes of
study were often used, and fairly well received. However, the most preferred methods of
professional development were practice-based learning, blended learning and shadowing –
methods which participants said, are used infrequently. Observations, however, showed that
these methods are used, but are not necessarily recognized as learning experiences as they
occur informally. An important factor in the quality of learning when using practice based
learning or shadowing is the quality of the practice of the person/people modelling or
supporting the learning process. The practice based facilitators of learning must be both
occupationally competent /proficient and proficient in facilitating and assessing practice
proficiency in others. At present there is limited availability of such support.
The primary concern for participants regarding learning was finding time to study. This was a
particular problem for night shift staff, as this group struggled to access daytime education
sessions. There were also concerns about written work/presenting, even at specialist and
advanced levels, and essential level participants were concerned that paid hours for
education sessions outside their usual working hours would impact on employment benefits.
These concerns may contribute to why work-based and blended learning were popular
options i.e. they involve practical learning and assessment methods, aspects of which could
be integrated into work time, so that concerns about time, night shift working, written work
and benefit payments could be reduced. Essential and specialist level participants were also
concerned about using IT/accessing IT at home, which may contribute to why e-learning was
so unpopular.
62
The findings suggest that practice-based and blended learning methods are not just
preferred, but may enhance competency. The nursing assistants in location A consistently
worked at a higher competency level than health care assistants. Nursing assistants
undertake an in-house professional development programme, which includes some work-
based learning, and shadowing the management team and RNs. This may contribute to their
higher competency levels. OPSN Band 7 nurses consistently worked at higher competency
levels than other nurses. A number of factors may contribute to this, for example, their
seniority as nurses, and their advanced clinical and prescribing skills. However, their
exposure to, and participation in, virtual ward rounds facilitates their upskilling as these
events act as forums for teaching and learning between consultants and nurses. An
additional factor affecting these learning experiences is the relevance of learning to all
individuals irrespective of their role and level of practice. Many of the cases discussed during
virtual wards rounds are complex cases that require clinical management from the multi-
professional team. No single professional knowledge base is adequate on its own for
effective care, thus learning occurs across the multidisciplinary team when professionals
involved in the case share their understanding of the problem and potential interventions and
solutions. After the rounds, presentations and learning sessions addressing issues that are
relevant to attendees further enhance these learning experiences.
Accommodating the preferred learning methods identified in this study on a more formal
basis would require a shift in the way learning and professional development programmes
are commissioned, provided and delivered. There would need to be less emphasis on
training, e-learning and ‘classroom’ type teaching, and much more emphasis on learning,
and developing skills and competency using practice based, shadowing and blended
learning methods.
The vast majority of participants said having a recognised qualification in the care of older
people with complex needs was important as a means of developing new knowledge,
improving care, improving confidence, recognising prior skills, influencing change, and
career progression. Having a recognised qualification would also enable a more
standardised approach to competency development. This would reduce variation in
competency across sectors and organisations, and facilitate more effective multi-
professional working that can rely on an expectation that there is standardisation of
competencies within professional groups. A standardised and recognised qualification would
also be more acceptable to professional, regulatory and commissioning bodies. However,
findings suggest that achieving a knowledge based qualifications is not enough in itself to
develop competency/proficiency. Programmes of learning and development need to be

63
directly relevant to enable achievement of the specified competencies within the EnCOP
framework, through the development and assessment of BOTH knowledge and
understanding AND competency in practice, if they are to enhance competency in the care
of older people.
Competency
Findings demonstrated that nurse participants working in the NHS have higher competency
levels than nurses working in care homes. A contributory factor may be that NHS nurses can
access a range of learning opportunities not open to care home nurses. This includes
updates and assessments to maintain competency in a range of clinical skills and
interventions. This suggests a need to for an infrastructure that facilitates learning and
competency development across sectors, so that the workforce is able to respond to patient
need seamlessly and efficiently.
Location A employed nursing assistants who had undertaken an in-house programme of
professional development that develops management skills, clinical skills and skills specific
to the care of older people including dementia, mental health, frailty and end-of-life care. The
rationale behind developing nursing assistants is to enhance the competency of the non-
professional care workforce. This group works at a higher level of competency than health
care assistants. Location B did not employ nursing assistants but were keen to explore ways
of introducing this role into their organisation as they were aware that other companies were
successfully developing the role. The current nursing associate apprenticeship (Institute for
Apprenticeships, 2016) could be utilised and adapted to develop a role specific to care
homes.
Both pilot care homes were sited in locations that align OPSNs and GPs with care homes,
which allows care homes to access multi-disciplinary ward rounds, and wider health and
social care services. Comparisons of location and competency domains/sub-domains
showed that in many areas, specialist and advanced level competency scored significantly
higher in location A than in location B. This may be due to the influence of location A’s
virtual ward model, which: uses the input of consultants with specific expertise in the care of
older people with complex needs; promotes inter-professional working and facilitates the
upskilling of OPSNs via maximizing learning opportunities between consultants and nurses,
and the availability of senior OPSNs working at a higher competency level. Rolling out this
model may enhance competency in other localities.
The EnCOP framework is based on the premise that having knowledge and skills in care
delivery is not enough on its own. Practitioners need to have the right values, be able to

64
work together, and lead and improve care if the care delivered is going to be effective –
hence the A B C D structure of the framework. This premise was borne out in this study as
findings showed a positive relationship between collaborative working competency and
clinical skill competency; teaching, learning and support competency and clinical
competency; and leading, organising and managing competency and clinical competency.
Any professional development or learning programme should therefore embed within it these
competency development areas. A particular area requiring development within the
teaching, learning and support sub-domain was supervision processes and competency
assessment. In terms of supervision, standard, valid and robust practices are required that
meet the needs of professional, regulatory and commissioning bodies, and that aim to
improve and ensure safe practice. In terms of competency assessment, it was very clear in
the findings that the number of individuals proficient in competency assessment needs to
expand. These individuals need to be able to demonstrate competency in their own clinical
area, and strategies are required to facilitate these individuals to work across sectors. In
order to meet the competencies required for a standardised qualification, methods of
assessment need to be standardised, integrated with, and encompass the knowledge,
understanding and values of a standard competency framework such as EnCOP.
Throughout all stages of the study, it was found that difficulties in accessing funding to
support competency development was a significant barrier to upskilling and developing the
workforce caring for older people with complex needs. It is essential that current available
funding streams are identified, publicised and made easily accessible to all organisations
and sectors. Also, plans and solutions at a strategic level are required to ensure
maximisation of efficiency and effectiveness of funding streams.
Accreditation and recognised qualifications
The vast majority of participants said having a recognised qualification in the care of older
people with complex needs was important as a means of developing new knowledge,
improving care, improving confidence, recognising prior skills, influencing change, and
career progression. However, the findings suggest that achieving a knowledge based
qualifications is not enough in itself to develop competency/proficiency. Programmes of
learning and development need to be directly relevant to enable achievement of the
specified competencies within the EnCOP framework, through the development and
assessment of competence in practice underpinned by knowledge and understanding at the
appropriate level in the care of older people with complex needs. Some relevant national
frameworks exist for recognised qualifications with accreditation, however there are some
gaps which can be addressed by actions as identified below.
65
Advanced Clinical Practice (ACP)
Health Education England has recently published the Multi-professional framework for
advanced clinical practice in England (ACP). This framework, which builds upon
previous work, guides the preparation of the ACP workforce in a consistent way to ensure
safety, quality, and effectiveness. The framework has been developed for use across all
settings including primary care, community care, acute, mental health and learning
disabilities and is multidisciplinary in its approach. It sets out the required core capabilities
for health and care professionals if they are to be considered and recognised at working at
the level of advanced clinical practice. The framework sets out the educational requirements
and key principles and governance expectations to guide the planning and development of
the ACP workforce including the generic knowledge and competencies of advanced clinical
practice (around 80% of the curriculum), however there is recognition that the application of
advanced clinical practice requires specific knowledge and competencies relevant to the
client group. As such, ACP programmes, which are commissioned by HEE enable them to
be aligned to particular contexts of practice through specific content and competencies. For
example, in a local pilot, HEE have commissioned the development of an ACP programme
with defined pathways including one specific to the care of older people with complex needs.
This will result in an academically accredited qualification, a Post Graduate Diploma in
Advanced Clinical Practice, which is at the required level 7 and maps to all required
capabilities and pillars of Advanced Clinical practice and the EnCOP framework. Whilst there
are a limited number of HEE funded places in the pilot phase, there is potential to
commission further places, provided capacity is built to enable assessment of proficiency
specific to the context.
In recognition of the importance of the ACP role in many contexts of practice, an
apprenticeship standard is currently in development.
https://www.instituteforapprenticeships.org/apprenticeship-standards/advanced-clinical-
practitioner-degree/
Once finalised, employers can use their apprenticeship levy to fund new or existing
employees who meet the entry criteria (must be registered health professionals who are at
graduate level) to undertake the apprenticeship with 80% of time in practice based learning
and 20% in formal learning. The funding band has not yet been published, which will indicate
the maximum amount employers can draw down from the levy pot to enable them to
commission a local provider. Education providers who are on the apprenticeship provider
66
framework can provide such programmes, and can align their ACP provision with the
EnCOP framework.
Specialist Practice
The nature of specialist practice encompassed in the EnCOP framework is not reflective of
the knowledge and competencies of either the Registered Nurse Adult (Level 6 Degree in
Adult Nursing, although previously Advanced Diploma, Diploma or Certificate level) or
Registered Manager award (Level 5 Diploma in Leadership for Health and Social Care –
adult care, previously Level 4 Certificate). Both awards are of relevance and provide
background knowledge and competence, however, as indicated in the EnCOP competency
framework, Specialist Practice includes additional knowledge and competence relating to all
domains of the EnCOP framework, but specifically Domain D, knowledge and skills for
practice required when caring for older people with complex needs. An additional period of
learning, building on the initial qualification could enable achievement of the required
competencies at the level of specialist practice. Specialist practice is located at level 6
(degree level) on the regulated qualification framework.
A multi-disciplinary programme of learning and assessment could be developed and
provided at level 6 (degree level) to enable nurses, AHPs or care home managers to
develop proficiency at the specialist level of the EnCOP framework. HEE currently
commission continuing workforce development (CWD) and this study should inform future
commissioning decisions. Consideration would be needed of the current restrictions on
access to HEE funded CWD highlighted in this report to make this an accessible and
equitable provision for all relevant staff whether employed in independent or NHS sector.
In order to provide a longer term sustainable funding solution, there is the option of
developing a new apprenticeship standard via the trailblazer route. Apprenticeship standards
can be developed in relation to a defined job role (Specialist Practitioner in Care of Older
People with Complex Needs). It must be employer led to meet an identified workforce
development gap, and involve at least 10 employers. The trailblazer process is outlined via
the link but does take around 18 moths to develop and reach approval for delivery
https://www.gov.uk/government/publications/how-to-develop-an-apprenticeship-standard-
guide-for-trailblazers
67
Essential practice
Those providing the essential level of care described in the EnCOP framework are mainly
support workers/senor support workers employed in the independent sector adult social
care. Funding for adult social care WFD is from Skills for Care via their WFD fund (£12m)
now mainly provided via apprenticeships which develop occupational competence rather
than short training courses.
Apprenticeship standards approved for delivery include;
• Healthcare support worker (level 2)
• Adult care worker (level 2)
• Lead adult care worker (level 3)
• Nursing Associate (level 5)
• Healthcare assistant practitioner (level 5)
Other apprenticeship routes are in development
• Lead practitioner in adult care (level 4)
• Leader/manager in adult care (level 5)
The findings from the study support recent strategic intent to join up the system to
commission, provide more effective WFD and evaluate the impact.
“HEE currently spends over £350 million each year supporting workforce development.
Alongside this there is investment by other national bodies on specific service areas (such
as NHS England’s investment in IAPT training), the investment of employers, and of staff
members themselves on CPD. However, there is a growing recognition that we need to seek
to align all this investment from across the system to better develop the workforce to deliver
improvements in patient care.” HEE (2017: 46)
However, as identified by HEE
“There are no standard training requirements across large parts of the adult social care
sector with too many staff not receiving training or professional development, despite
providing direct care for vulnerable adults whose dignity and quality of life is dependent on
the quality of their work. The Care Certificate, developed by HEE, Skills for Care and Skills
68
for Health, provides a standard induction framework across social care and health. There is
no mandated …development across employers. “ (HEE 2017: 69)
Whilst the Green paper on adult social care is due to be published summer 2018, this report
provides evidence to inform the need for appropriate workforce development to support
integrated models of care:
https://www.gov.uk/government/news/government-to-set-out-proposals-to-reform-care-and-
support

69
6: Recommendations Recommendations for workforce development
The research highlighted the lack of an integrated system based approach to workforce
development and the problems and barriers inherent in the use of a training approach. At the
stakeholder event, participants considered the options available, and indicated support for
the adoption of a workforce development approach, which focuses on both individual
learning and the system wide changes needed to enable the development and assessment
of proficiency across the workforce aligned to the EnCOP framework. The study identified a
lack of capacity and capability across the system to support practice based learning. It also
highlighted that we do not have a clear picture of the potential funding available via the
apprenticeship levy or other sources to support future workforce development in the older
person’s workforce.
Recommendation 1: Adopt a whole system approach to integrated older people’s workforce development
An ageing society, with an associated increase in people with complex health and social
care needs, requires a workforce, now and in the future, that is competent in the
management of complex care as well as capable of working in pathways within and across
organisations. Shunting service users across service boundaries and across sectors for
specialist care should be a thing of the past, and service delivery can be wrapped around the
older person and their family in integrated health and care systems. This transformation
requires a whole system approach to workforce development. Appointment of a designated
body or workforce development lead within the STP footprint, and localised practice
educators who are both occupationally competent to specialist / advanced level of the
EnCOP framework and proficient at facilitating learning and assessing proficiency in others
who have responsibility for, and agreement to work across organisational boundaries would
ensure that WFD strategy and solutions are based upon evidence and offer standardization
of approach and economy of scale. The appointed workforce development lead could work
with commissioners of services to develop service specifications providing leverage for the
recommendations to be embedded within employing organisations.

70
Recommendation 2: Gain agreement across all sectors for adoption of a competency framework for all levels of practice to deliver enhanced care for older people with complex needs
The older people’s workforce is diverse and for effective care and service delivery there is a
need for standardisation of competency across organisations and sectors. This can be
achieved through agreement of competency to practice rather than on role requirements.
The EnCOP framework offers elucidation of competencies required at essential, specialist
and advanced levels of practice across the whole workforce. Consideration should be given
to aligning job descriptions, professional and regulatory requirements against the EnCOP
framework within public and independent sector organisations across the region. At present
there is variation in the competence of professionals working at specialist and advanced
levels of practice, with a greater degree of standardisation in essential practice. The
evidence from this study suggests that the variation in specialist and advanced practice is
not widely acknowledged, and that there is potential to upskill groups within the older
people’s workforce in the management of complex healthcare. This situation contributes to
some of the challenges of inter-professional practice and working across organisational
boundaries. With the adoption of a competency framework, such as EnCOP it would be
possible to adopt a ‘Passport of competence’ or ‘Passport to practice’ by the workforce. This
would support working across organisational boundaries and enhance inter-professional
working through recognition of personal competence to practice.
Recommendation 3: Develop infrastructure for practice based learning and assessment
Develop necessary strategic infrastructure, via funded practice educator roles as described
above, covering a specific geographical location eg a CCG area, to lead, develop and
support a network of practice based mentor/assessors to facilitate practice based learning
and assessment. Practice educator roles provide an effective link between practice and
education and have been used effectively in a range of contexts to support a workforce
development approach. The roles should span organisational boundaries and have the
necessary strategic agreement in place to support workforce development across a sector,
and able to work across NHS, private, independent and voluntary sector providers. The
practice educator role requires the post holder to be proficient in the practice context (able to
demonstrate proficiency at advanced practice level of the EnCOP) and proficient at
facilitating learning and workforce development with responsibility for:

71
• Strategic leadership of WFD for the older people’s workforce across organisational
boundaries within a given geographical locality.
• Development of capacity for practice based learning and assessment through the
identification and facilitation of staff from care homes and community settings to
achieve the NMC mentor standards (or alternative, as the standards are currently
being reviewed) through access to the taught mentor/assessor module which is HEE
funded, or through the accreditation of prior experiential learning route for those with
experience but without a relevant qualification.
• Partnership working with education providers to develop and deliver accredited
programmes relevant to each level of the EnCOP framework which are delivered in
the practice setting using a blended learning approach. Such programmes may be
aligned to the appropriate apprenticeship standards (employer funded via the levy
payment) or specifically commissioned using HEE or other funding sources.
• Facilitate the development of necessary policies, procedures, and memoranda of
understandings as required to enable cross system acceptance and agreement of
practice based assessment of proficiency. Cross organisational competency sign off
is urgently needed to enable professionals to work across health and care sectors,
which is increasingly becoming common place as new models of care are being
embedded across older people’s services.
Recommendation 4: Equality of access to practice-based learning for development of proficiency at all levels of practice
Cross organisational and professional learning and development is important in increasing
the workforce’s ability to manage complex care and this has a positive impact on the
individual’s confidence and skills in fulfilling their role. Traditionally there has been a lack of
parity for all sections of the older people’s workforce to access learning opportunities and
this has contributed to variation in competency across the workforce. The move to an
integrated approach to workforce development requires all learning and development
opportunities for all member of the workforce irrespective of the employing organization.
Commission the development and delivery of accredited programmes of study which lead to
the development of proficiency at each level of the competency framework (essential,
specialist, advanced) which are:
• Practice based.
• Integrated with routine practices as opportunities for learning (ward rounds in care
homes; virtual ward).

72
• Interprofessional, and facilitate opportunities for shared learning with experts in a
locality.
• Provided via a blended learning model
• Where technology enhanced learning/e learning is used it should be of high quality
and underpinned by pedagogy of effective TEL (DH 2011)
• Academically accredited at the relevant level
• Enable ‘Recognition and Accreditation of Prior Learning’ (RPL).
• Assessed in theory and practice (enable achievement of proficiency)
• Provide a ‘learning passport’ which is recognized across the system.
Consideration should be given to developing, or further development of, accredited
programmes of learning where gaps exist in the workforce. These include:
• Development of a trailblazer in multiprofessional/multi-skilled specialist practice
for older people with complex needs.
• Using or adapting the current nursing associate apprenticeship (Institute for
Apprenticeships, 2016) in the care home sector.
• Having student nurses on placement in care homes increases the future
workforce competence in managing the complex needs of residents. This this
model should be encouraged and consideration given to rolling this out across
other professional groups.
Recommendation 5: Develop understanding of funding sources, options and related issues
There is a need for employers to explore sources of funding to support workforce
development including the apprenticeship levy; European Social Fund; Better Care Fund (if it
could be demonstrated that this would improve outcomes); and HEE commissioned CWD
provision under the widening access policy. Through collaborative working it is feasible that
employers will be able to access funding for workforce development that has not been
previously available.
Identify and engage employers in the sector to explore potential funding available to support
WFD via the apprenticeship levy. Employers with a pay bill of over £3 million per year have
been subject to the levy since April 2017, which means 0.5% of their pay bill is paid into the
apprenticeship fund via PAYE. Employers receive a 10% top up into their digital account.
They may draw down this funding to use for approved apprenticeships for their own staff.
Each apprenticeship standard has a maximum amount of funding that can be drawn down

73
(for example £3,000 for a support worker, £27,000 for a nursing apprenticeship) and used to
commission an education provider who is on the approved provider list of apprenticeships..
Apprenticeships are provided via a partnership model, where the education provider is
responsible for the learning and assessment of the apprentice, and the employer is involved
in the assessment of the apprentice in their work role. Employers who do not use the levy
money they have paid in, lose it. Smaller employers not subject to the levy can use the levy
fund to pay 90% of the cost of an approved apprenticeship for their staff, with the employer
responsible for the remaining 10% of the cost.
Exploration of the use of levy funding should involve key people within provider
organisations (NHS, private and independent providers) who have information and influence
on their organisational intent and use of the apprenticeship levy and the amount available to
them. Agreement for the strategic use of levy funding should be sought to benefit the whole
sector.
Recommendation 6: Commission an evaluation of outcomes which incorporates effectiveness of WFD
Given the investment in WFD, it is important that any strategic WFD programmes are
properly evaluated (HEE 2017). Evaluation should provide evidence of impact on the
participants and those they support (residents/patients). Kirkpatrick’s (1994) four stage
model of evaluation focuses on reaction, learning, behaviour, results.
• Reaction: Did individual learners enjoy and benefit from the learning experience?
• Learning: Was there an improvement in knowledge, skills and values?
• Behaviour: Have learners changed the way they practice as a result of learning?
• Results: What are the outcomes of WFD on patient/resident outcomes?

74
7: Appendices 7.1: Links to the phase 1, strand 1 surveys:
essential.html
specialist.html
advanced.html

75
Appendix 7.2
Observation Survey Tool – Phase 1, strand 1 Each attendee at the virtual ward round who is a study participant is to be observed. Oberved competence and confidence should be mapped against the following EHC framework domains and sub-domains (refer to the full EHC competency framework to assist with mapping if necessary).
Values, attitudes and behaviours
Participant Role EHC framework level Not at all Not very Somewhat Very N/A (essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
B: Workforce collaboration, co-operation, communication and support
B1: Inter-professional and inter-organisational working and communication
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
76
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
B2: Teaching, learning, and supporting competence development
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
C: Leading, organising, managing and improving care
C1: Leading, organising and managing care
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
77
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
C2: Improving care
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D: Knowledge and skills for care delivery
D1: Communication with older people, families and friends
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
78
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D2: Care process
D2.1: Assessing, planning, implementing and evaluating care
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D2.2: Pharmacology and management of medicines
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------

79
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D3: Promoting health, wellbeing and independence
D3.1: Promoting and supporting independence and autonomy
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D3.2: Promoting and supporting holistic health and wellbeing
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------

80
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D4: Management of dementia
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D5: Management of mental health
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------

81
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D6: Management of frailty
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
D7: End of life care
Participant Role EHC framework level Not at all Not very Somewhat Very N/A
(essential, specialist, advanced)
P1 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P2 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P3 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
P4 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------

82
P5 ------- ----------------------------------------- ------------- -------------- --------------- ------- --------
(add further participants if necessary)
83
Appendix 7.3: Information sources concerning apprenticeships and funding
Apprenticeship standards can be found here: https://www.gov.uk/guidance/search-for-apprenticeship-standards Standards in development here: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/641042/Copy_of_CURRENT_STANDARDS_IN_DEVELOPMENT.pdf If no standard exists that meets employer specific need employers can group together (needs at least ten employers) to form a trailblazer: https://www.gov.uk/government/publications/how-to-develop-an-apprenticeship-standard-guide-for-trailblazers Frameworks .gov.uk/government/publications/how-to-develop-an-apprenticeship-standard-guide-for-trailblazerstrailblazers" https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/601512/Apps_Framesworks_Standards_A_to_Z.pdf If you as an employer and know which apprenticeship standard you require for your employees you can find a provider here by doing a postcode search: https://findapprenticeshiptraining.sfa.bis.gov.uk/ You can keep up to date with new standards being approved and proposed nationally here and there is an opportunity to log and comment on proposals every month: https://consult.education.gov.uk/ Funding bands for standards and frameworks can be found here: https://www.gov.uk/government/publications/apprenticeship-funding-bands Funding guidance for levy payers can be found here: https://www.gov.uk/government/publications/apprenticeship-levy-how-it-will-work/apprenticeship-levy-how-it-will-work#non-levy-paying-employers Funding guidance for non-levy payers can be found here: https://www.gov.uk/government/publications/apprenticeship-levy-how-it-will-work/apprenticeship-levy-how-it-will-work#non-levy-paying-employers All training providers (including employers wishing to deliver training to their own staff) must be on the Register of Approved Training Providers. See here: https://roatp.apprenticeships.sfa.bis.gov.uk/download

84
8: References
Anema M, McCoy J (2010) Competency-Based Nursing Education: Guide to Achieving Outstanding Learner Outcomes. Springer, New York.
Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B (2012) Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 380(9836): 37-43.
Braun, V. and Clarke, V. (2006) Using thematic analysis in psychology. Qualitative Research in Psychology, 3 (2) pp77-101.
Cassidy, S (2009) Subjectivity and the valid assessment of pre-registration student nurse clinical learning outcomes: Implications for mentors. Nurse Education Today 29 p33-39
Cook G, McNall A, Thompson J, Hodgson P (2016) Gateshead Care Home Workforce Competencies. Northumbria University, Newcastle.
Cornwell J (2012) The Care of Frail Older People with Complex Needs: Time for a Revolution. The King’s Fund, London.
Cowan, DT, Norman,I, Coopamah, VP (2005) Competence in nursing practice: A controversial concept – A focused review of literature. Nurse Education Today 25 p355-362
European Commission (2015) The Ageing Report: Economic and Budgetary Projections for the 28 EU Member States (2013-2060). European Commission, Brussels.
Health Education England (2017) Widening access to post-registration education policy https://madeinheene.hee.nhs.uk/Portals/94/Widening%20Access%20Policy%20-%20June%202017.pdf
Health Education England (2017) Facing the Facts, shaping the future consultation.
https://www.hee.nhs.uk/our-work/workforce-strategy
Institute for Apprenticeships (2016) Nursing associate apprenticeship. https://www.instituteforapprenticeships.org/apprenticeship-standards/nursing-associate/
Mayring, P. (2000) Qualitative content analysis. Forum. Qualitative Social Research, 1 (2), 20-24.
McNall A (2012) An Emancipatory Practice Development Study: Using Critical Discourse Analysis to Develop the Theory and Practice of Sexual Health Workforce Development. Thesis submitted for the award of Professional Doctorate in Nursing, Northumbria University.
NHS England (2017a) New Care Models.https://www.england.nhs.uk/ourwork/futurenhs/new-care-models/
NHS England (2017b) Newcastle and Gateshead Clinical Commissioning Group: The Vanguard and the People it Serves. https://www.england.nhs.uk/ourwork/new-care-models/vanguards/care-models/care-homes-sites/gateshead/
Roche A. (2009) New horizons in AOD workforce development. Drugs, Education, Prevention and Policy 16(3): 193-204.

85
Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA (2011) Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. British Journal of General Practice 61(582): 12–e21.
Staron M (2008) Workforce Development: A Whole-of-System Model for Workforce Development. http://lrrpublic.cli.det.nsw.edu.au/lrrSecure/Sites/Web/13289/ezine/year_2008/sep/thinkpiece_whole_system_approach.htm
Thompson J, Tiplady S, McNall A, Murray J, Cook G, Hodgson P (2017) Workforce Competency Framework: Enhanced Health in Care Homes. Northumbria University, Newcastle.