an analysis of migration health in kenya - … analysis of migration health in kenya. ......
TRANSCRIPT
IN KENYA AN ANALYSIS OF MIGRATION HEALTH
2 3
© International Organization for Migration
Regional Mission for East & Central AfricaChurch Road – off Rhapta Road, WestlandsPO Box 55040 – 00200, Nairobi, Kenya
Tel: +254 20 444 4174 Email: [email protected]
www.nairobi.iom.int
The opinions expressed in the report are those of the author and do not necessarily reflect the views of the International Organization for Migration.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form, or by any means including, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the publisher.
2 3
HEALTHY MIGRANTS IN HEALTHY COMMUNITIES
CONTENTS
04 BACKGROUND
05 OVERVIEW
08 MIGRATIONASASOCIALDETERMINANTOFHEALTH
09 MIGRATIONHEALTHCONCERNSINKENYA
TuberculosisandMigration HIVandMobility ReproductiveHealthandMigration Additionalhealthconcerns
15 POLICYANALYSIS
16 THEWAYFORWARD
Recommendations
19 REFERENCES
COVER:Ayoungpastoralistgirltravelslong,arduousdistancesinsearchofwater©SilverscreenPictures

4 5
OVERVIEW
Migration Health in Kenya
Migrationisnowaglobalphenomenon,with3percentoftheworld’spopulation living temporarilyorpermanentlyoutside theircountryoforigin(WorldBank,2009).Climatechange,urbanization,andexpandedtrade are likewise driving increased population mobility within andbetweencountries.
Likemost countries, Kenya is host to diverse typologies ofmigrants.Within Kenya, poverty is pushing people tomove in search ofwork.Ethnicconflictandviolentcattleraidshaveforcedwholecommunitiesinto displacement camps. Climate change is slowly tightening its gripon arable land, pressuring families to find livelihoods elsewhere. Agooddegreeofrural–ruralmigrationtakesplacetosugar,flower,andteaplantations.Kenyaalsoabsorbsavarietyofmigrantsandrefugeesfrom its neighbours, namely Sudan, Somalia, Ethiopia, Tanzania, andUganda.Mobile populations include sexworkers, pastoralists, fishingcommunities,transportworkers,andcivilservants.
Aspopulationmobility isoneof thedefiningcomponentsof the21stCentury,migrationmustalsoberecognizedasasocialdeterminantofhealth;mobilitynotonlyimpactsuponanindividual’svulnerabilityandsocialwelfare,butalsotheirmentalandphysicalwell-being.
However,notallmigrantsandmobilepopulationsareequallyatrisktoadversehealth. It is notpeoplemoving,per se, that aggravatespoorhealth,butthewayinwhichtheymoveandthecontextwithinwhichmovementtakesplace.Forexample,incomedisparities,separationfromfamily,alcoholuse,andalackofeffectivepreventionprogrammingaredrivingriskysexualbehaviour,andthusHIVtransmission,alongtransportcorridors. Cramped urban settlements are prone to tuberculosistransmission, and highly-mobile pastoralists need to be reachedwithservicesatthoselocationswheretheysettleatparticulartimesofyear.
A number of social factors, such as immigration status, stigma, andlanguagebarriersarepreventingmigrantsfromaccessingqualityhealthcare.InreducinghealthinequityinKenya,aconcertedeffortisrequiredin making health systems more “migrant friendly”. As some healthissuesrelatedtotrans-bordermobilitycannotbesolvedbyKenyaalone,internationalcollaborationisrequired.
BACKGROUNDObjective
An Analysis of Migration Health in Kenya was commissioned by theMinistryofPublicHealthandSanitation(MoPHS)andtheInternationalOrganizationforMigration(IOM)toprovideanoverviewoftheissueofmigrationhealthinKenya.Informationwasderivedfromanextensiveliterature review and interviews with key informants, includingthe Government, United Nations agencies and non-governmentalorganizations.
ThetwingoalsofKenya’sSecondNationalHealthSectorStrategicPlanaretoreduceinequalitiesinhealthcareandreversethedownwardtrendin health related impact and outcome indicators (Republic of Kenya,2005a).ByprovidingananalysisofmigrationhealthinKenya,thisreportaimstostimulatediscussionwhichwillleadtodecisiveactionfromtheGovernmentandpartnerstoensuremigrantsmaybegintoenjoymoreequitableaccesstohealthservices.Asmigrantsdonotliveinisolation,butratherindiversecommunities,theirhealthstatushasanimpactonthecommunityat-large.Itisthereforetheresponsibilityof–andinthebestinterestof–Kenyatocaterfortheirbasichealthneeds.
BACKGROUND OVERVIEW
Migrationcanbedefinedas“aprocessofmoving,eitheracrossaninternationalborder,orwithinaState.Itisapopulationmovement,encompassinganykindofmovementofpeople,whateveritslength,compositionandcauses;itincludesthemigrationofrefugees,displacedpersons,uprootedpeopleandeconomicmigrants”(IOM,2004).
GovernmentchildgrowthmonitoringandimmunizationcampaignatanIOMEastleighCommunityWellnessCentreinNairobi©A.Corio
6 7
Typologies of migrants
Often inappropriately clumped together under the term “refugee”,migrantsandmobilepopulationshavelargelybeenoverlookedwithinKenya’shealthcaresystem,includingpoliciesandstrategies,financing,research and surveillance, human resources, health promotion, andservicedelivery.
TypesofmigrantsinKenyacommonlyincludeirregularmigrants,asylumseekers,labourmigrants,economicmigrants,traffickedpersons,urbanmigrants, commercial farmworkers, internally displaced persons andrefugees.Migrantsalsoincludemobilepopulationssuchassexworkers,pastoralists, fishing communities, transporters, civil servants, anduniformedpersonnel.
Irregularmigrantsarethosewhohaveenteredahostcountrywithoutlegalauthorizationand/orwhohaveoverstayedtheirauthorizedentry,andassuch,faceuniquevulnerabilities,notablythoserelatedtohealth.Oftendesperatetoavoidaccessingpublicservicesduetodistrustorforfearofbeingdeportedordiscriminatedagainst,irregularmigrantsoftenonlyseekmedicalassistancewhenthere isnootheralternatecourseandtendtomissoutonimportantpromotivehealthmeasuressuchasimmunizations,pregnancycare,andsafechildbirth(IOM,2009).Non-migrant friendly services also discouragepatients by not catering fortheirculturalandlanguageneeds.
Push and pull factors: determinants and consequences of migration
Theclassictheorytoexplainwhypeoplemigratefromonecountrytoanother is the“pushandpull” factor: peoplemigrate inresponsetopushfactorsintheircountryoforiginand/orpullfactorsinthecountryofdestination.Thepushfactorsaregenerallynegative,whilstthepullfactorsarelargelypositive(Potocky-Tripodi,2002).
OVERVIEW OVERVIEW
From the literary review and discussions with key informants, thefollowingpushandpullfactorswereuncovered:
Economic:
• Wideningfinancialdisparityandthegrowingneedforyoungand relativelycheaplabourdrivespeopleawayinsearchofemployment• Inequitabledistributionofresourcesencouragespeopletosearch forequalityandwealthelsewhere• Workrequirementsoftennecessitatetravelformilitaryofficials, tradesmen,andtransportworkers• Kenyaisatransitcountryforgoodsflowingtoitslandlocked neighbours,thuslargenumbersofmobilepopulationssaturateits roadandwatertransportcorridors.
Socio-cultural:
• Poorschooling,socialservices,healthcare,familyreunification andprotectionpushespeopletomoveinsearchofnewlocales withimprovedfacilities• Insufficientfamilysupportstructuresencourageindividuals tomigrate.
Natural, environmental and seasonality:
• Climatepushespastoralistsandcattlerustlerstomoveseasonally• Ruraltourbanmigrationcan,inpart,beattributedtothescarcity ofnaturalresources;collapsingandcontractingindustriesforce peopletomoveinsearchofanewtrade• Naturaldisasterspushthoseunabletocopeorsurviveintosafer localesordisplacementcamps• Outbreaksofdiseasecompelpeopletomoveinto non-susceptibleregions.
Socio-political environment:
• OngoingconflictinSomaliaandSudanandeconomicdisparityin EthiopiahasresultedinalargenumberofmigrantscrossingKenya’s porousborders.

8 9
MIGRATION AS A SOCIAL DETERMINANT OF HEALTH
The definition of health
The1946constitutionoftheWorldHealthOrganizationdefineshealthasa“stateofcompletephysical,mentalandsocialwell-beingandnotmerelytheabsenceofdiseaseor infirmity.”“Migrationhealth”refersto thewell-beingofmigrants,mobilepopulations, their families,andcommunitiesaffectedbymigration.
Migration as a social determinant of health
Althoughmobility is not of itself detrimental to health, it is a socialdeterminant of health. The circumstance in which migration takesplace, together with individual factors such as gender, language,immigration status, and culture, have a significant impact on health-related vulnerabilities and access to services (IOM, 2010a). Thechallenge for the KenyanGovernment and partners is to understandthesesocialdeterminantsinordertoimprovethewelfareofmigrantsandcommunitiesasawhole.
Amultitudeofsourcesindicatethatamajorchallengefacingthehealthofmigrantsisaccesstoappropriateservices.Geographicalaccessibility,availability,affordability,andacceptabilityarethefourmajorchallengesto access, all of whichmust be addressed when reassessing Kenyanhealthpolicy.
So, why is it imperative thatmigrants gain access to health servicesinKenya?Addressingthehealthneedsofmigrantsnotonly improvestheir well-being, but it also safeguards the health of Kenyan hostcommunities. In addition acceptance and integration of migrantscontributes towards social andeconomicdevelopment. Furthermore,well-beingisafundamentalhumanrightwhichisrecognizedinthenewConstitution.
With data captured from the literature review and interviews withkey informants, the following were cited as major health-relatedvulnerabilitiesformigrants:
MIGRATION HEALTH CONCERNS IN KENYA
Tuberculosis and migration in Kenya
Kenya is among the world’s top 22 high tuberculosis (TB) burdencountries (WHO, 2010). Amajor reason for increased TB in Kenya inthepastdecade is the concurrentHIVepidemic,with44percent co-infectionin2009.
ThenationalTBstrategyspecificallyhighlightstheneedforstrengtheningprogramming to reach migrants in crowded urban centres, nomadiccommunities, migrant workers, and transport workers. Thesepopulationsoftenfacebarrierstoaccessing informationandservices,includingappropriatediagnosis.Treatmentiscomplicatedbytheneedtoadheretotheregimeforsixmonths,andtrans-bordercollaborationisthereforenecessary.Surveillanceneedstobestrengthenedinborderareas(RepublicofKenya,2010c).
MIGRATION AS A SOCIAL DETERMINANT OF HEALTH MIGRATION HEALTH CONCERNS IN KENYA

10 11
MIGRATION HEALTH CONCERNS IN KENYA MIGRATION HEALTH CONCERNS IN KENYA
IN FOCUS: Tuberculosis among urban migrants
Eastleigh, a large trading district inNairobi, is home to thousands ofmigrantslargelyfleeingprolongedpovertyandconflictinEthiopiaandSomalia.Eastleighisalsoamajortransitpointbetweenrefugeecamps,Somalia,andthirdcountriestowhichmigrantstravelthroughlegalandirregularchannels.
A largeproportionof thepopulation lives in overcrowded, dark, andpoorlyventilatedapartmentblocks,whichareconducivetothespreadoftuberculosis(TB).
The vast majority of migrants residing in Eastleigh are residing withirregular immigration status, and are hence deprived of basic healthservices due to fear or distrust of the authorities. Stigma, languagebarriers,andlackofhealthliteracyaresomeofthesocialfactorswhichdiscouragemigrantsfromseekingappropriatediagnosisandtreatment.Forthesereasons,privatehealthfacilitiesarepreferred,andmanyarenotlicensedbytheGovernment.
Duetotheirmobilenature,manymigrantswhostartonTBtreatmentin Eastleigh do not complete their course of medication and oftenleave the district without adequate follow-up. This leads to furtherTBtransmissionandcanresultindrugresistancewhichcarrieshighermortalityratesandburdentothehealthsystem.
AkeyissueinaddressingthisissueistounderstandthatmigrantsarenotspreadingTB,butrather,thattheyareunabletoaccesstheappropriateservicesfordiagnosisandtreatment.
HIV and mobility in Kenya
ThenationalHIVprevalenceinKenyawasestimatedat7.4percentin2007(RepublicofKenya,2008)and6.3percentin2009(KNBSandICFMacro,2010).MobilityhasoftenbeenfalselyhighlightedasariskfactorforHIVinfectionandithasoccasionallybeenmisconstruedthatmobilepopulationscarryHIVfromhigherto lowerprevalencecountries.Thereality is that inorder tospreadthevirus,an individualmustfirstbeinfectedwithdetectablelevelsofvirusintheirbodies,andthenengagein riskbehaviour, suchasunprotectedsexor injectingdrugs.Aswithotherhealthissues,itisthecontextofmigrationandhowoneismobilethatdifferentiallyimpactsvulnerability.
Others have assumed that “vulnerable” populations must also havehigherHIVprevalence.Asynthesisofsevensub-SaharanAfricancountriesfoundrefugeesinallbutonecampsettingtohaveaprevalencewhichwascomparativelymuchlowerthaninsurroundinghostcommunities.Agradualriseinprevalenceincampswasattributedtorefugeesengagingin risk behaviour with members of host communities (Spiegel et al,2007).IOMhaslikewisefoundthatHIVprevalenceamongrefugeesandmigrantsundergoingmigrationhealthassessmentsinNairobi is justasmallfractionoftheprevalenceofNairobi,andmoreorlessonparwiththeprevalenceincountriesoforigin.Thepost-conflictsetting,however,may see a precipitous rise in HIV prevalence asmay be the case innorthernUganda,Somaliland,andpartsofsouthernSudan.
While data is not sufficient to identify a link between populationdisplacementintheemergencycontextandincreasedHIVtransmission,Kenyaexperiencedmajor breakdowns in theprovisionofHIV-relatedservicesinthe2008electionaftermath.Guidelinesandcapacitiesarerequiredatalllevelstopreventsimilarsystemicbreakdownsinfutureemergencies.
IN FOCUS: Risky sexual behaviour along transport corridors in East Africa
Most-at-riskpopulations,suchasfemalesexworkersandtheirclients,account for an estimated 14 per cent of all new infections. This is asubstantialdecreasefromtheearlyyearsoftheepidemicwhenfemalesex worker and truck drivers were seen as core population groups;however,vulnerablegroupsalongtransportcorridorsremainsubstantialcontributorsofnewinfectionsandremainamongthemostimportantpopulationsnotadequatelycoveredby thepreventionefforts (NACC,2009a). A 2005 study estimated that along theMombasa - Kampalahighway3,200to4,148newHIVinfectionsoccureveryyear(Morris&Ferguson,2006).
In ports, cities, border crossings, and truck stops, income disparitiesbetween “mobilemenwithmoney” andwomen of lower economicstatus fuels amarket for sex (IOM& UAC, 2008). Asmany of theserelationshipsevolveintolong-termpartnerships,condomuseremainslow. Becausemanymen andwomen in these locations have severaldifferentsexualpartners,thereishighpotentialofspreadingthevirus,especially among thosewhoarenewly infectedand thushavemuchhigherlevelsofvirusintheirbodies(Halperin&Epstein,2007).
“Inmyhouse,therearemany,manypeople.Thehouserentsareveryhigh.Thesearehardshipsthatcausethespreadofvariousdiseases.Wealsodonothavemoneytoaccessqualitymedicalhealthcare.”
AnurbanmigrantresidinginEastleigh,IOM2011a

12 13
MIGRATION HEALTH CONCERNS IN KENYA MIGRATION HEALTH CONCERNS IN KENYA
TheepidemiologyofHIValongtransportcorridors isnotrestrictedtotruckdriversandsexworkers.Ashighlighted inFigureOne,a femalesexworker engageswith a diverse clientele, ofwhich only about 30percentaretruckerdrivers(RepublicofKenya,2005b).Asimilar2008InternationalOrganizationforMigrationstudyontheKampala–Jubacorridorshowedsimilarfindings.
The lack of effective HIV prevention interventions in spaces ofvulnerabilityalongKenya’smajortransportcorridorsiscauseforalarm.A 2010 response analysis of fivemajor sites along the corridor fromMombasatoBusiawitnessednoinstanceofbehaviouralinterventionsthoughnearly30agenciesclaimedtorunsuchprogrammes.Over60percentof600truckersandfemalesexworkersinterviewedreportedhavingnever received information onHIV/AIDS. In spite ofworking in closeproximity,noinstanceofcollaborationbetweenagencieswasreported(IOM&NACC, 2010). Clinical services, includingHIV Counselling andTesting(HCT),arenotsufficientlyaccessible.Thescenarioisakintothatofatug-of-warwitheachagencypullingtheropeinadifferentdirectionand the responsemovingnowhere.Anational strategyhasyet tobedevelopedtoguideimplementingpartnersonacommonapproachthatcanbebroughttoscale.
Reproductive health and migration in Kenya
Thereproductivehealthneedsofrefugees living incampsettlementsarewelldocumented;however,significantgapsremaininunderstandingthe reproductive health needs of othermobile populations,whetherirregular migrants, pastoralists, or others (Hynes, Sheik, Wilson, &Spiegel, 2002). Irregular migrants and female sex workers are oftenoverlookedinregardstohealthpromotionactivities,includingaccesstofamilyplanning,prenatal,delivery,andearlychildhoodhealthcare.Thisleadstosuchissuesasmaternalmortalityandchronicmeaslesoutbreaksinurbanslumsduetolackofcoveragebyvaccinationcampaigns.
Apilot study found substantial differences in access tomaternal andchild health services between migrant and Kenyan women in thecommunityofEastleigh.Mostnotablewerethedifferencesinantenatalcare, labouranddelivery, contraceptionandbreastfeeding. Followinguponthefindingsusinginformaldiscussions,itwasfoundthatdespitea general consensus on the importance of accessing maternal-childhealth care,migrantwomen cited numerous barriers, including cost,languagebarriersandreligiousbeliefs,anda lackoftrust inavailableservices due to health care worker attitudes and quality of serviceswithinthefacilities(IOM&McGill,2011).
Additionally, appropriate service delivery is vital, especially with thecurrentpushamongtheGovernmentanddonorcommunityonutilizingmaternalchildhealthservicesasaconduittoaccessfemalesexworkersandvulnerablewomenwithHIVpreventionprogramming,whichisanapproach that the International Organization for Migration has longadvocatedfor.
IN FOCUS: reproductive health among pastoralists in Northern Kenya
NorthernKenyahasoneofthehighestmaternalmortalityratesinthecountry, estimated at 1,000 – 1,300 deaths per 100,000 live births,compared to 530 per 100,000 live births nationally. As one of thepoorest,remotestregionsinKenya,malnutritionisrampantandaccesstosafedrinkingwaterandimprovedtoiletfacilitiesisnon-existentforthemajorityofpastoralists(RepublicofKenya,2008;IOM/IGAD,2009).
The 2009 drought pushed malnutrition levels to 12 per cent in theGarissadistrict,and15percent in theBaringodistrict.Withdroughthitting Kenya hard in 2011, food instability, child undernutrition andmaternal mortality is currently a looming national disaster. Remotepastoralist communities will invariably be affected; maternal health
“Therewasnomeanstotakehertoahealth
centreandshehadbeeninlabourforfourdays.Thebleedingdidnot
stopafterdeliveringsowejustwatchedasshe
continuouslybledtodeath.”
Pastoralistmother,Turkana,IOM2011a
“SometimesyoufindthatthosewhoarenotHIVpositivearegivensupportandyouwhoispositivedonotbenefit.ThisiswhyifherhusbandtriestoseducemeIwillnotrefusebecausetheybenefitfromthesupportwhichIamsupposedtoget,andIwillsay‘tohellletthemdiewithme.’”HIVpositivefemalesexworker,Salgaa(IOM&NACC,2010)
FigureOne:ClienteleoffemalesexworkersalongtheMombasa–Kampalacorridor,datagatheredusing28-dayFSWdiaries(RepublicofKenya,2005b)

14 15
MIGRATION HEALTH CONCERNS IN KENYA POLICY ANALYSIS
facilities are severely lacking and pastoralists regularly have to travellongdistancestoreachthenearesthealthfacility.
Moreover, there is a reluctance to seek services in health facilities.Pastoralists in Kenya tend to prefer traditional health care providersovermodernmedical practices (IOM/IGAD, 2009), as health facilitiesareperceivedaslesssufficientbecausetheyaretoofaraway,lackthenecessaryservicesandequipmentandservicesofferedarenotadaptedto a mobile lifestyle. An unfavourable attitude adopted by healthworkersandnomoneytopayfortreatmentwerealsocitedasreasonstoshunexistinghealthservices(IOM/IGAD,2009).
Improvedaccessforpastoralistcommunitiesmustbescaled-upthroughoutreachprogrammesthatareavailabletoremotepopulationsinawaythatistailoredtoseasonalmobilitypatterns.
Additional health concerns facing migrants in Kenya
Malaria: Malaria is the leading cause of morbidity and mortality inKenya (Republic of Kenya, 2008). Migrants and mobile populationsare particularly vulnerable as treated mosquito nets remain elusiveandhealthservicesarelacking.AreportbyMosca,Wagacha,Aketch,Stuckey and Gushulak (2000) indicates that a bulk of migrants whoresettle to third countries originate from rural refugee campswheremalariatransmissionmaybehyper-endemic.Severalstudieshavealsohighlightedthatmalariaisthetophealthconcernofmobilepopulationssuchastruckers,whosleepinorundertheirvehicleswithoutaccesstomosquitonets(IOM&GLIA,2006).
Theinformalprivatesectorhasproliferatedsinceitsliberalizationduringthe late1980s.Much like themajorityofKenyans, irregularmigrantsrelyontheprivatesectorand itcanbeassumedthattheymightnotreceiveappropriatediagnosisortreatmentastheyself-medicatewithshop-boughtanti-pyreticsandanti-malarialsthatmaynotmeetnationalstandardsforqualityandeffectiveness(RepublicofKenya,2001).
Measles and other vaccine-preventable infections: Kenya hasexperiencedmultipleoutbreaksofmeaslesoverthelastdecadedespitetheexistenceofaneffectiveandaffordablevaccine.In2005,2007,and2009outbreaksbeganwithunvaccinatedmigrants,manyofwhomcomefromnationswithhistoricallylowimmunizationcoverageandminimalhealth care delivery infrastructure. Migrants frequently distrust andhavemisconceptionssurroundingvaccinations;theseneedtobebetterunderstoodandmessagingdevelopedtobetterpromoteimmunization
uptakeinmigrantcommunities.Thepotentialre-emergenceofpolioisanotherparticularconcerninmigrantcommunities.
Occupational health:Longhours,lonelinessandharsh,dirtylivingandworking environments often expose labourmigrants to risks such asoccupational injury,gastrointestinal issues, tuberculosis,andHIV risk-behaviour.
Psychosocial health: Those who migrate clandestinely, or fall intothe hands of traffickers and end up in exploitive situations, aredisproportionately affected by psychosocial health. Conflict anddisplacementalsoinciteahugeemotionalburdenforthoseaffected.
POLICY ANALYSIS
TheBillofRightswhichisanchoredinthenew2010ConstitutionofKenyarecognizesthatitisafundamentaldutyoftheStatetoobserve,respect,protect,promote,andfulfiltherightsandfundamentalfreedomsofallpeopleinKenya.ItalsoassertsthateverypersoninKenyahastherighttothehighestattainablestandardofhealth.
However,Kenyastillhasalongwaytogobeforethisisrealized.Logisticalchallengestoreachmigrantsandmobilepopulations,top-downhealthsystemsthatfailtocontextualizeservicesforvulnerablepopulationsareallchallengesthatcan,andmust,beaddressed.
Interviewswith key informants highlight a growing concern that theKenyanGovernment’smandateforsecuringahealthypopulationdoesnotcommensuratewithitslackofinitiativeinreducinghealthdisparitiesin communities affected by migration and population mobility. Theprioritization of migrant health should be embedded within allKenyanMinistries. In Kenya, assistance provided to internalmigrantsis implemented by the Ministry of State for Special Programmes,whichinmostcasesrespondstodisasters,withminimalpreventiveorhealthpromotionprogrammesinplace.Theseprogrammesprotectingmigrantscannotbesidelined,and insteadshouldbe ingrainedwithinnationalactionplansandstrategies.

16 17
THE WAY FORWARD RECOMMENDATIONS
HowcanweprioritizemigrantswithastretchedhealthcaresystemthatevenKenyansarenotaccessing?Thisisacommonquestionarguedinmanypolicyforums;however,communicablediseasesdonotrespectborders and migrants live in communities with Kenyans. It is onlythrough partnership, led by the Government of Kenya, that we canprovidehealthcareforallwhoresidewithinitsborders.
THE WAY FORWARD
AsKenyaprogressestowardsVision2030,itwillcontinuetobeaprimedestinationforitsEastAfricanneighboursasaregionaleconomichub.MigrantswillcontinuetocometoKenyathroughoutthisforthcomingeconomicexpansion,andasaresultof increasedmovementoftradegoodsandpeoplewithinspacesofvulnerability,therewillinevitablybeanimpactonthehealthofcommunitiesthroughoutKenya.
Migrantandmobilepopulationsaccesstoessentialhealthinformationand services is often problematic. With the potential for increasednumbersofmigrants,itisessentialthatpolicymakersandprogrammemanagers gain a better understanding of the various typologies ofmigrantsandtheirunderlyinghealthdrivers,sothatthenationalhealthpackagecanbetailoredtotheirspecificneeds.
Achieving the healthMillennium Development Goals, the challengesfacedbytheGovernmentofKenyaanditspartnersistoensureequitableaccess to health and social services within the context of increasingdiversityanddisparities.Atthesametime,long-standingprogramminggaps related to migrants and mobile populations have yet to beadequatelyaddressed.Inordertomeetthesedemands,strengthenedpartnershipsarerequiredamongstakeholderswithinKenya,with thedonorcommunity,aswellaswithneighbouringcountries.
National policy in regards tomigrant healthmust be as bold as theConstitutionandBillofRights,wheretherightsofmigrantsareprotected.Utilizing such a lens it is easily understood that Kenya can adopt anapproachwherehealthymigrantsliveinhealthycommunities.Toachievesuchagoal,itisimperativethatwecometoacommonconsensusontheinclusionofmigrationhealthingeneralhealthpromotionandverticalhealthstrategiesinKenya.SpecificallythiscouldincludetheformationofaNationalForumforMigrationHealthchairedbytheGovernmentofKenya, tostrengthencoordinationamongstakeholdersandtodrawaCommonActionPlan(CAP)formigrationhealth.
RECOMMENDATIONS
TheGovernment,withsupportfrompartners,shouldtakeleadershipon:
1. Establishinganinstitutionalreferencepointforhealthissues relatingtomigrantsandmobilepopulations,forexample, adedicatedunitwithintheMinistryofHealth;
2. Reviewingnationalstrategiesandguidelinesandensuringthat mechanismsareinplacetoreducehealthdisparitiesfaced bymigrantsandmobilepopulations;
3. Facilitating,providing,andpromotingequitableaccessto comprehensiveavailable,affordableandnon-discriminatoryhealth services.Thisshouldincludehealthpromotion,diseaseprevention, andcareformigrants;
4. Offeringhealthservicesintargetareaswheremigrantsarepresent andwheretheycanbeaccessed,forexample,cross-border communities,hotspotsalongtransportcorridors,fishingvillages, plantations,andurbansettlements;
5. Providingbasichealthservicestomigrants,regardlessof immigrationstatus,asapublichealthpriority;
6. Makingservicesmoremigrant-friendlythroughsuchmeansas engagingmigrantcommunityleadersandemployingstaffwho speakmigrantlanguages;
7. Developingnationalstrategiestoaddressspecificissues,for instance,onscaling-uponenationalframeworkonpreventingHIV alongtransportcorridors;
8. Sensitizingandbuildingcapacityofpolice,healthcareproviders, andgatekeepers(includingsecurityguardsatclinics)tothe importanceofensuring“healthforall”andformeetingthespecific needsofmigrants;
9. Strengthenthedocumentationofhealthissuesfacingmigrants andmobilepopulations,includingqualitativeresearchonaccess andacceptability,disaggregatingsurveillancedatatoidentify migration-relateddata,andincludingmigration-relatedindicators inDemographicandHealthSurveysandrelatedactivities;
18 19
RECOMMENDATIONS REFERENCES
10. Expandingfundingandresearchcapacityforthoseinvestigating topicswithinthefieldofmigrationhealth;
11. Addressingtheenvironmentalandstructuralfactorsimpactingthe healthofmigrants,inadditiontoindividualriskfactors;
12. Strengtheningthecoordinationofhealthissuesthatfacemigrants amongstakeholderswithincommunities,countries,andbetween countries;
13. Asfeasible,strengtheningcollaborationonhealthprogramming betweenplacesoforigin,transit,anddestination;
14. Harmonizingtreatmentprotocolsbetweencountriesandestablish trans-borderreferralmechanismsforissuesincludingtuberculosis, HIV/AIDS,andmaternal-childhealth;
15. DevelopingaRegionalDisasterManagementPlantodealwith pandemics,breakdowninHIV/AIDSprogramming,andother disastersthataffectmigrantsanddisplacedpopulations.
REFERENCES
Halperin, D. and H. Epstein 2007 WhyisHIVPrevalencesoSevereinSouthernAfrica?Therole ofmultipleconcurrentpartnershipsandlackofmalecircumcision: ImplicationsforAIDSprevention.TheSouthernAfricanJournal ofHIVMedicine,March2007,pages19-25.
Hynes, M., Sheik, M., Wilson, H. G., & Spiegel, P. 2002 Reproductivehealthindicatorsandoutcomesamongrefugee andinternallydisplacedpersonsinpostemergencyphase camps.JournaloftheAmericanMedicalAssociation, 2002Aug7;288(5):595-603.
2002 Reproductivehealthindicatorsandoutcomesamongrefugee andinternallydisplacedpersonsinpostemergencyphase camps.JournaloftheAmericanMedicalAssociation.
Intergovernmental Authority on Development (IGAD), National AIDS Control Council (NACC), and International Organization for Migration (IOM)2009 PastoralismandHIV/AIDSinIGADCountries:Programme mapping,datasynthesis,andrecommendationsforpolicyand furtherresearch–KENYAREPORT,IOM,Nairobi.
Intergovernmental Panel on Climate Change (IPCC)2007 WorkingGroupIIContributiontotheIntergovernmentalPanel onClimateChangeFourthAssessmentReportClimateChange 2007:ClimateChangeImpacts,AdaptationandVulnerability, April2007.
International Maritime Organization (IMO) and Ports Management Authority of East & Southern Africa (PMAESA)2008 ImpactAssessmentStudyofHIV/AIDSinPMAESAPortof Mombasa,Kenya,IMO,Nairobi.
International Organization for Migration (IOM)2011a TheSocialDeterminantsofHealthinMigrant PopulationsinKenya2010a BackgroundPaperfor2010WorldMigrationReport:Future CapacityNeedsinManagingtheHealthAspectsof MigrationIOMGeneva2010b MigrationandHealthinSouthAfrica:Areviewofthecurrent situationandrecommendationsforachievingtheWorldHealth AssemblyResolutiononthehealthofMigrants,IOM,Pretoria.
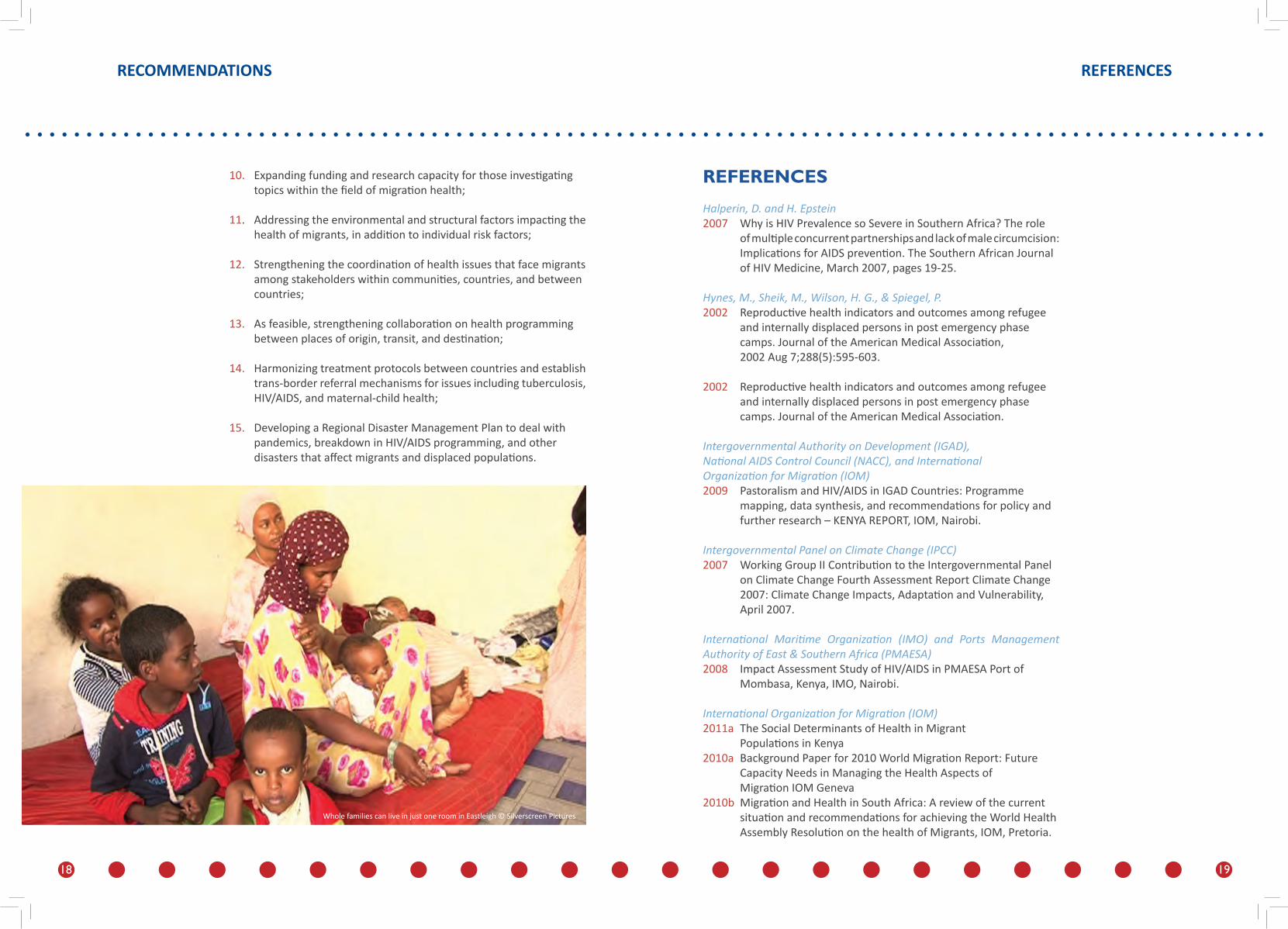
WholefamiliescanliveinjustoneroominEastleigh©SilverscreenPictures

20 21
REFERENCES REFERENCES
2010c NationalConsultationMigration&HIVinTanzania:Uniformed Personnel,MobilePopulations,andBorderCommunities,1-2 June2010,DarEsSalaam,Tanzania.IOM,DaresSalaam.2009 SessionSummaryReport:Sub-plenary5–HealthPromotion:An ApproachtoImprovingtheHealthofMigrants,IOM,Nairobi2004 InternationalMigrationLawNo.10,GlossaryonMigration, IOM,Geneva.2000 Malariareductioninmobilepopulations:TheIOMSupplementary MedicalProgrammeforSub-SaharanAfrica,IOM
International Organization for Migration and McGill University2011 AccesstoMaternal&EarlyChildhoodHealthCareforUrban MigrantsinEastleigh,Nairobi,Kenya.IOM,Nairobi
International Organization for Migration and National AIDS Control Council (NACC)2010 ResponseAnalysisofCombinationPreventionalongthe NorthernTransportCorridorinKenya(inpress).
International Organization for Migration and the Great Lakes Initiative on HIV/AIDS (GLIA)2006 Long-distanceTruckDrivers’PerceptionsandBehaviorsTowards STI/HIV/TBandExistingHealthServicesinSelectedTruckStops oftheGreatLakesRegion:aSituationalAssessment. IOM,Nairobi.
International Organization for Migration and Uganda AIDS Commission (UAC)2008 HIVHot-spotMappingandSituationalAnalysisalongthe Kampala–JubaTransportRoute,IOM,Kampala.
Kenya National Bureau of Statistics (KNBS) and ICF Macro2010 KenyaDemographicandHealthSurvey2008-9,Calverton, Maryland:KNBSandICFMacro
Morris C.N. and Ferguson A.G.2006 EstimationofthesexualtransmissionofHIVinKenyaandUganda ontheTrans-AfricaHighway:thecontinuingroleforprevention inhighriskgroups,Sex.Transm.Inf.,July2006,doi:10.1136/ sti.2006.020933.
Mosca D, Wagacha B, Aketch J, Stuckey J, Gushulak B. 2000 MalariaReductioninMobilePopulations.TheIOMsupplementary medicalprogrammeforSub-SaharanAfrica,International OrganizationforMigration,Nairobi,Kenyaand Geneva,Switzerland.
National AIDS Control Council (NACC), UNAIDS, and World Bank2009a KenyaHIVPreventionResponseandModesofTransmission Analysis–FinalReport,March2009.NACC,Nairobi.2009b KenyaNationalAIDSStrategicPlan2009/10–2012/13:Delivering onUniversalAccesstoServices.NACC,Nairobi.
Potocky-Tripodi. M2002 BestpractisesforSocialWorkwithrefugeesandimmigrants, ColumbiaUniversityPress,USA
Republic of Kenya2010a BudgetPolicyStatement,March2010.Ministryof Finance,Nairobi.2010b TheConstitutionofKenya–RevisedEdition2010,National CouncilforLawReporting,Nairobi.2010c DivisionofLeprosy,Tuberculosis,andLungDisease,Kenya: StrategicPlan2011-2015,MinistryofPublicHealthand Sanitation,Nairobi.2008 KenyaAIDSIndicatorSurvey2007:PreliminaryReport,National AIDS/STDControlProgrammeandMinistryofHealth,Nairobi.2008 MinistryofPublicHealthandSanitation:StrategicPlan2008- 2012,MOPHS,Nairobi.2005a ReversingtheTrends:theSecondNationalHealthSector StrategicPlanofKenya–NHSSPII2005-2010, MinistryofHealth,Nairobi.2005b HotSpotMappingoftheNorthernCorridorTransportRoute: Mombasa–Kampala,Finalreport,MinistryofTransport,Nairobi.2001 NationalMalariaStrategy2001–2010, MinistryofHealth,Nairobi.
Spiegel, P., Bennedsen, A., Claass, J., Bruns, L., Njogu, P., Yiweza, D., and Schilperoord, M.2007 PrevalenceofHIVinfectioninconlict-affectedanddisplaced peopleinsevensub-SaharanAfricancountries:asystematic review.TheLancet2007;369:2187–95.

22 23
United Nations Department of Economic and Social Affairs (DESA) / Population Division 2009 WorldUrbanizationProspects:The2009Revision,United NationsSecretariat,NewYork.
World Bank 2009 WorldDevelopmentIndicators,WorldBank,Washington,DC
World Health Organization 2008a GlobalTuberculosisControl–Surveillance,Planning,Financing.2008b Healthofmigrants:ResolutionoftheSixty-firstWorldHealth Assembly(WHA61.17),WorldHealthOrganization,Geneva.2007 EverybodyBusiness:Strengtheninghealthsystemstoimprove healthoutcomes-WHO’sFrameworkforAction,WHO,Geneva.
World Health Organization, IOM, Government of Spain2010 HealthofMigrants:TheWayForward–Reportofaglobal consultation,Madrid,Spain3-5March2010,WHO,Geneva.
REFERENCES CHAPTER ONE | xxxxxxx xxxxx xxxxx
JamillaNamatoustandswaitingforclientsinthebordertownofBusia©CHibbert“IfmenhaveHIV,thentheyseenoreasontowearacondom.Thisputsusatrisk”shesays

24
© 2011 International Organization for Migration
Regional Mission for East & Central AfricaChurch Road – off Rhapta Road, Westlands
PO Box 55040 – 00200, Nairobi, Kenya
Tel: +254 20 444 4174 Email: [email protected]
www.nairobi.iom.int
HEALTHY MIGRANTS IN HEALTHY COMMUNITIES