american cancer society guidelines on nutrition and ... · pdf fileacs guidelines on nutrition...
TRANSCRIPT
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
92 CA A Cancer Journal for Clinicians
ABSTRACT The American Cancer Society (ACS) has set aggressive challenge goals for the
nation to decrease cancer incidence and mortality—and to improve the quality of life of cancer
survivors—by the year 2015.
To address these critical goals, the ACS publishes the Nutrition and Physical ActivityGuidelines to serve as a foundation for its communication, policy, and community strategies
and ultimately, to affect dietary and physical activity patterns among Americans.
These guidelines, published every five years, are developed by a national panel of experts
in cancer research, prevention, epidemiology, public health, and policy, and as such, they
represent the most current scientific evidence related to dietary and activity patterns and
cancer risk.
The American Cancer Society guidelines include recommendations for individual choices
regarding diet and physical activity patterns, but those choices occur within a community
context that either facilitates or interferes with healthy behaviors. Therefore, this committee
presents one key recommendation for community action to accompany the four
recommendations for individual choices for nutrition and physical activity to reduce cancer
risk. This recommendation for community action underscores just how important community
measures are to the support of healthy behaviors by means of increasing access to healthful
food choices and opportunities to be physically active.
The ACS guidelines are consistent with guidelines from the American Heart Association for
the prevention of coronary heart disease as well as for general health promotion, as defined
by the Department of Health and Human Services’ 2000 Dietary Guidelines for Americans.1,2
(CA Cancer J Clin 2002;52:92-119.)
Dr. Byers is Professor, PreventiveMedicine, University of ColoradoHealth Science Center, Denver, CO.
Dr. Nestle is Professor and Chair,Department of Nutrition and FoodStudies, New York University, NewYork, NY.
Dr. McTiernan is AssociateMember, Fred Hutchinson CancerResearch Center, Seattle, WA.
Ms. Doyle is Director, Nutrition andPhysical Activity, American CancerSociety, Atlanta, GA.
Ms. Currie-Williams is Manager,Nutrition and Physical Activity,American Cancer Society, Atlanta,GA.
Dr. Gansler is Director of MedicalStrategies, American CancerSociety, Atlanta, GA, and Editor of CA.
Dr. Thun is Vice President,Epidemiology and SurveillanceResearch, American Cancer Society,Atlanta, GA.
The following report was approvedby the American Cancer SocietyNational Board of Directors onNovember 1, 2001.
This article is also available online atwww.cancer.org.
American Cancer Society Guidelineson Nutrition and Physical Activity forCancer Prevention: Reducing the Risk of Cancer with Healthy FoodChoices and Physical Activity
Tim Byers, MD, MPH; Marion Nestle, PhD, MPH;Anne McTiernan, MD, PhD;Colleen Doyle, MS, RD;Alexis Currie-Williams, MPH, CHES;Ted Gansler, MD;Michael Thun, MD; and the American Cancer Society 2001 Nutrition and Physical ActivityGuidelines Advisory Committee*
*See pages 104 and 105.

INTRODUCTION
The Importance of Diet and Physical Activity in
Cancer Prevention
For the great majority of Americans who donot smoke cigarettes, dietary choices andphysical activity are the most importantmodifiable determinants of cancer risk.3
Evidence suggests that one third of the morethan 500,000 cancer deaths that occur in theUnited States each year can be attributed todiet and physical activity habits, with anotherthird due to cigarette smoking. Althoughgenetic inheritance influences the risk ofcancer, and cancer arises from geneticmutations in cells, most of the variation incancer risk across populations and amongindividuals is due to factors that are notinherited. Behavioral factors such as smokingcigarettes, consuming foods along certainpatterns of diet, and staying active across thelifespan can substantially affect one’s risk ofdeveloping cancer.4,5,6 Because healthfulindividual behaviors are most effectivelyenabled by social and environmental supportwithin communities, these 2001 guidelinesinclude, for the first time, an explicitrecommendation for community action.
OVERVIEW OF THE GUIDELINES
The American Cancer Society publishesnutrition and physical activity guidelines toadvise health care professionals and the generalpublic about dietary and other lifestylepractices that reduce cancer risk.7 Theseguidelines, updated in 2001 by the AmericanCancer Society Nutrition and Physical ActivityGuidelines Advisory Committee, are based onexisting scientific evidence that relates diet andphysical activity to cancer risk in humanpopulation studies as well as in laboratoryexperiments.
These guidelines reflect the current state ofthe scientific evidence. For many issues, theevidence is not definitive either because studiesare not yet available, or current findings areinconsistent. Although the randomized,controlled trial is often considered the goldstandard for scientific conclusions, suchevidence is not presently available—and maynever become available—for many dietaryfactors associated with cancer risk. Inferencesabout the many complex interrelationshipsamong diet, physical activity, and cancer riskare based, for the most part, on observationalstudies coupled with advancing understandingof the biology of cancer.The relative strengthof current scientific evidence linking majorcomponents of diet to common cancer sites issummarized later in Table 5. In considering thetotality of evidence from a variety of sources,these guidelines take into consideration boththe benefits to cancer risk reduction andoverall health benefits. Although no diet canguarantee full protection against any disease,these guidelines offer the best informationcurrently available about how diet and physicalactivity can reduce the risk of cancer.The ACSguidelines are consistent with guidelines fromthe American Heart Association for theprevention of coronary heart disease as well asfor general health promotion, as defined by theDepartment of Health and Human Services’2000 Dietary Guidelines for Americans.1,2
The American Cancer Society guidelinesinclude recommendations for individualchoices regarding diet and physical activitypatterns, but those choices occur within acommunity context that either facilitates orinterferes with healthy behaviors. Therefore,this committee presents one keyrecommendation for community action toaccompany the four recommendations forindividual choices for nutrition and physicalactivity to reduce cancer risk (Table 1). Thisrecommendation for community actionunderscores the importance of community
Volume 52 • Number 2 • March/April 2002 93
CA Cancer J Clin 2002;52:92-119

measures to support healthy behaviors byincreasing access to healthful food choices andopportunities to be physically active.
AMERICAN CANCER SOCIETY GUIDELINES FOR
NUTRITION AND PHYSICAL ACTIVITY
Recommendation for Community Action
Social, economic, and cultural factorsstrongly influence individual choices aboutdiet and physical activity. While mostAmericans would like to adopt a healthfullifestyle, many encounter substantial barriers
that make it difficult to follow diet and activityguidelines. Indeed, current trends towardincreasing consumption of high-calorieconvenience foods and restaurant meals, anddeclining levels of physical activity arecontributing to an alarming epidemic ofobesity among Americans of all ages and acrossall population segments.2 Longer workdays andmore households with multiple wage earnersreduce the amount of time available forpreparation of meals, with a resulting shifttoward increased consumption of food outsidethe home—often processed foods, fast foods,and snack foods. Reduced leisure time,increased reliance on automobiles for
94 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
American Cancer Society (ACS) Guidelines on Nutrition and Physical Activity for Cancer PreventionACS Recommendations for Individual Choices
1. Eat a variety of healthful foods, with an emphasis on plant sources.
• Eat five or more servings of a variety of vegetables and fruits each day.• Choose whole grains in preference to processed (refined) grains and sugars.• Limit consumption of red meats, especially those high in fat and processed.• Choose foods that help maintain a healthful weight.
2. Adopt a physically active lifestyle.
• Adults: engage in at least moderate activity for 30 minutes or more on five or more days of the week; 45 minutes or moreof moderate-to-vigorous activity on five or more days per week may further enhance reductions in the risk of breast andcolon cancer.
• Children and adolescents: engage in at least 60 minutes per day of moderate-to-vigorous physical activity at least five days per week.
3. Maintain a healthful weight throughout life.
• Balance caloric intake with physical activity.• Lose weight if currently overweight or obese.
4. If you drink alcoholic beverages, limit consumption.
ACS Recommendation for Community Action
Public, private, and community organizations should work to create social and physical environments that support the adoptionand maintenance of healthful nutrition and physical activity behaviors.
• Increase access to healthful foods in schools, worksites, and communities.• Provide safe, enjoyable, and accessible environments for physical activity in schools, and for transportation and recreation
in communities.
TABLE 1

transportation, and increased availability ofelectronic entertainment and communicationsmedia all contribute to a less active andincreasingly sedentary lifestyle.These trends areof particular concern, especially with regard tothe adverse effects they have on the long-termhealth of children, who are establishing lifetimepatterns of diet and physical activity, as well ason the poor, who live in communities with lessaccess to safe and healthful lifestyle options.
Facilitating improved diet and increasedphysical activity patterns will require multiplestrategies, ranging from the implementation ofcommunity and work-site health promotionprograms to policies that affect communityplanning, transportation, school-based physicaleducation, and food services. Particular effortswill be needed to ensure that all populationgroups have access to healthful food choicesand opportunities for physical activity. Bothpublic and private organizations at the local,state, and national levels will have to developnew policies and will need to raise or reallocateresources to facilitate needed changes. Healthcare professionals, who can be especiallypersuasive on matters of lifestyle change, canprovide leadership in promoting policychanges in their communities.
The decline in cigarette use by adultsprovides a useful analogy for the power of socialcontext in changing health behaviors. Adult-per-capita cigarette consumption began asustained decline after the 1964 SurgeonGeneral’s Report, which publicized the healthhazards of smoking.6 From that time on, othercommunity-wide social and political factorshave become increasingly important in reducingsmoking. These include public policy changesregulating cigarette advertising, restrictingminors’ access to tobacco products, increasingtaxation of tobacco products, and addressingconcerns about rights of nonsmokers, andexposure to second-hand smoke. Establishinghealthful patterns of diet and physical activitywill require similar purposeful changes in
individual lifestyle choices and in public policy.Public, private, and community organizationsshould strive to create social and physicalenvironments that support the adoption andmaintenance of healthful dietary and physicalactivity behavior patterns.
Recommendations for Individual Choices
There is strong scientific evidence thathealthful dietary patterns, in combination withregular physical activity, can reduce cancerrisk.4,5 Approximately 35 percent of cancerdeaths in the United States may be avoidablethrough dietary modification.8,9,10,11 Thescientific study of nutrition and cancer ishighly complex, and many important questionsremain unanswered. It is not presently clear how single nutrients, combinations ofnutrients, overnutrition and energy imbalance,or the amount and distribution of body fat at particular stages of life affect one’s risk ofspecific cancers. However, epidemiologicalstudies have shown that populations whosediets are high in vegetables and fruits and lowin animal fat, meat, and/or calories have areduced risk of some of the most commontypes of cancer. Until more is known about thespecific components of diet that influencecancer risk, the best advice is to emphasizewhole foods and certain broad dietary patterns,as described within these guidelines.
1. Eat a variety of healthful foods, with anemphasis on plant sources.
Eat five or more servings of a variety ofvegetables and fruits each day.
• Include vegetables and fruits at everymeal and for snacks.
• Eat a variety of vegetables and fruits.• Limit French fries, snack chips, and other
fried vegetable products.• Choose 100% juice if you drink fruit or
vegetable juices.
Volume 52 • Number 2 • March/April 2002 95
CA Cancer J Clin 2002;52:92-119

Choose whole grains in preference toprocessed (refined) grains and sugars.
• Choose whole grain rice, bread, pasta,and cereals.
• Limit consumption of refinedcarbohydrates, including pastries,sweetened cereals, soft drinks, and sugars.
Limit consumption of red meats, especiallythose high in fat and processed.
• Choose fish, poultry, or beans as analternative to beef, pork, and lamb.
• When you eat meat, select lean cuts andhave smaller portions.
• Prepare meat by baking, broiling, orpoaching rather than by frying orcharbroiling.
Choose foods that help you maintain ahealthful weight.
• When you eat away from home, choosefoods that are low in fat, calories, andsugar, and avoid large portion sizes.
• Eat smaller portions of high-caloriefoods. Be aware that “low-fat” or“nonfat” does not mean “low-calorie,”and that low-fat cakes, cookies, andsimilar foods are often high in calories.
• Substitute vegetables, fruits, and otherlow-calorie foods for calorie-dense foodssuch as French fries, cheeseburgers, pizza,ice cream, doughnuts, and other sweets.
Beneficial Effects of Vegetables and Fruits
Greater consumption of vegetables, fruits, orboth together has been associated in themajority of epidemiological studies with alower risk of lung, oral, esophageal, stomach,and colon cancer. Evidence is less strong forcancers considered hormonal, such as breastand prostate. Diet can be an important factoreven in cancers caused, in large part, by otherfactors. For instance, many studies have found a
lower risk of lung cancer among those who eatmore vegetables and/or fruits in theirdiet.12,13,14,15 Although the major factor thatcauses lung cancer is tobacco smoking, diet alsomodifies risk, both in smokers and in lifelongnonsmokers.
Evidence that vegetable and fruitconsumption reduces cancer risk has led toattempts to isolate specific nutrients and toadminister these in pharmacological doses tohigh-risk populations. Most of these attemptshave been unsuccessful in preventing cancer orits precursor lesions, and in some cases, havehad adverse effects. Notable examples are thethree randomized trials of beta-carotene forthe prevention of lung cancer, initiated becauseof many observational epidemiological studiesindicating lower risk of lung cancer in personseating foods high in beta-carotene.Two of theclinical trials showed that smokers taking high-dose beta-carotene supplements developedlung cancer at higher rates than those taking aplacebo,14,15 while a third study showed noeffect.16 These findings support the idea thatbeta-carotene may be only a proxy for othersingle nutrients or combinations of nutrientsfound in whole foods, and that taking a singlenutrient in large amounts may be harmful.
It is presently unclear which components ofvegtetables and fruits are most protectiveagainst cancer.17 Vegetables and fruits arecomplex foods, each containing more than 100potentially beneficial vitamins, minerals, fiber,and other substances that may help to preventcancer. Vegetables and fruits also containspecific phytochemicals, such as carotenoids,flavonoids, terpenes, sterols, indoles, andphenols that show benefit against certaincancers in experimental studies. There isongoing research, for example, on the potentialbenefits of green and dark yellow vegetables,plants related to the cabbage family, soyproducts, legumes, allium (onion and garlic),and tomato products. Until more is known
96 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

about specific food components, the bestadvice is to eat five or more servings of avariety of vegetables and fruits in their variousforms: fresh, frozen, canned, dried, and juiced.
Despite recommendations from numeroushealth agencies to eat at least five servings ofvegetables and fruits each day, intake of thesefoods remains low among adults andchildren.18,19 Concern about low-intake levelshas led to a nationwide initiative—the National5 A Day for Better Health program—to helpinsure that vegetables and fruits are availableand accessible to all population groups, and toincrease vegetable and fruit consumption tofive or more servings per day.20
Whole Grains
Grains such as wheat, rice, oats, and barley,and the foods made from them, constitute thebasis of a healthful diet. Whole grains are animportant source of many vitamins andminerals that have been associated with lowerrisk of colon cancer, such as folate, vitamin E,and selenium.21 Whole grains are higher infiber, certain vitamins, and minerals thanprocessed (refined) flour products. Althoughthe association between fiber and cancer risk isinconclusive,22,23 consumption of high-fiberfoods is still recommended. Since the benefitsgrain foods impart may derive from their othernutrients as well as from fiber, it is best toobtain fiber from whole grains—andvegetables and fruits—rather than from fibersupplements. As shown in Table 2, standardportion sizes are quite small.
Beans are excellent sources of manyvitamins and minerals, protein, and fiber. Beansare legumes, the technical term for the familyof plants that includes dried beans, pinto beans,lentils, and soybeans, among many others.Beans are especially rich in nutrients that mayprotect against cancer24 and can be a usefullow-fat, high-protein, alternative to meat.
Dietary Fat and Consumption of Red Meat
High-fat diets have been associated with anincrease in the risk of cancers of the colon andrectum, prostate, and endometrium. Theassociation between high-fat diets and breastcancer is much weaker. Research continues toexamine whether the association betweenhigh-fat diets and various cancers in someepidemiological studies is due to the totalamount of fat, the particular type of fat
Volume 52 • Number 2 • March/April 2002 97
CA Cancer J Clin 2002;52:92-119
What Counts as a Serving?
Fruits• 1 medium apple, banana, or orange• 1/2 cup of chopped, cooked, or canned fruit• 3/4 cup of 100% fruit juice
Vegetables• 1 cup of raw, leafy vegetables• 1/2 cup of other cooked or raw vegetables, chopped• 3/4 cup of 100% vegetable juice
Grains• 1 slice of bread• 1 ounce of ready-to-eat cereal• 1/2 cup of cooked cereal, rice, or pasta
Beans and nuts• 1/2 cup of cooked dry beans• 2 tablespoons of peanut butter• 1/3 cup nuts
Dairy foods and eggs• 1 cup of milk or yogurt• 11/2 ounces of natural cheese• 2 ounces of processed cheese• 1 egg
Meats• 2-3 ounces of cooked, lean meat, poultry, or fish
TABLE 2
Source: US Department of Agriculture and US Departmentof Health and Human Services. Nutrition and Your Health:Dietary Guidelines for Americans, 4th ed. Home and GardenBull 232. Washington, DC: Government Printing Office,1995.

(saturated, monounsaturated, or polyun-saturated), the calories contributed by fat, orsome other factor associated with high-fatfoods. Fats such as the saturated fat in redmeats, omega-3 fatty acids in fish oils, ormonounsaturated fats in olive oil, for example,likely differ in their effects on cancer risk.Therelationship between specific types of fat andcertain cancers is an important area of currentresearch.25
Because a gram of fat contains more thantwice the calories of a gram of protein orcarbohydrates (9 versus 4 kcal/gram), studiescannot easily distinguish the effects of fat itselffrom the effects of the calories it contains. Inaddition, dietary fat consumption is alsocorrelated with greater consumption of meatand calories; lower consumption of vegetables,fruits, and grains; and higher body weight, sothat it may be difficult to disentangle theseparate contribution of fats to cancer risk.
Foods from animal sources remain majorcontributors of total fat, saturated fat, andcholesterol in the American diet.26 Althoughmeats are good sources of high-quality proteinand can supply many important vitamins andminerals, consumption of meat—especially redmeats (beef, pork, lamb)—has been associatedwith cancers in many studies, most notablythose of the colon and prostate.27 How muchof this association is due to specific constituentswithin meat (such as saturated fats) or tocorrelated dietary factors is presentlyunclear.28,29,30 For example, mutageniccompounds, such as heterocyclic amines, areproduced when protein is cooked at a hightemperature, and may contribute to theassociation between meat and colon cancer.
Much evidence indicates that saturated fatmay be particularly important in increasingrisk of cancer as well as for heart disease.Thebest way to reduce saturated fat intake is tomake wise choices in the selection andpreparation of animal-based foods. Choose
lean meats and lower-fat dairy products, andsubstitute vegetable oils for butter or lard. Foodlabels can be a useful guide to choosingpackaged foods lower in saturated fat. Choosesmaller portions and use meat as a side dishrather than as the focus of a meal. Emphasizebeans, grains, and vegetables in meals to helpshift dietary patterns to include more foodsfrom plant rather than animal sources.Preparation methods are also important.Baking and broiling meat, rather than frying,reduces its overall fat content. Meat should becooked thoroughly to destroy harmful bacteriaand parasites, but should not be charred.
Choosing Foods that Help Maintain aHealthful Body Weight
Most people cannot maintain a healthfulbody weight without limiting caloric intakewhile maintaining regular physical activity.Current trends indicate that the largestpercentage of calories in the American dietcomes from foods high in fat, sugar, and refinedcarbohydrates. Consuming a varied diet thatemphasizes plant-based foods may help todisplace these calorie-dense foods. Limitingportion sizes, especially of these types of foods,is another important strategy to reduce totalcaloric intake.
Replacing dietary fat with foods that arehigh in calories from sugar and other refinedcarbohydrates does not protect against obesity.The decrease in fat intake and increase inconsumption of refined carbohydrates thatoccurred in the United States between 1977and 1995 coincided with an 8% increase in theprevalence of obesity.31,32 Excessive intake ofsugar and other highly-refined carbohydratesmay contribute to insulin insensitivity,alterations in the amount and distribution ofbody fat, and increased concentrations ofgrowth factors that may promote the growth ofcancers.
98 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

2. Adopt a physically active lifestyle.• Adults: engage in at least moderate
activity for 30 minutes or more on fiveor more days of the week; 45 minutes ormore of moderate-to-vigorous activityon five or more days per week mayfurther enhance reductions in the risk of breast and colon cancer.
• Children and adolescents: engage in atleast 60 minutes per day of moderate-to-vigorous physical activity for at least fivedays per week.
Benefits of Physical Activity
Scientific evidence indicates that physicalactivity may reduce the risk of several types ofcancer, including cancers of the breast andcolon, and can provide other important healthbenefits.33,34 Physical activity acts in a varietyof ways to impact cancer risk. Regularphysical activity helps maintain a healthfulbody weight by balancing caloric intake withenergy expenditure.35 Other mechanisms bywhich physical activity may help to preventcertain cancers may involve both direct andindirect effects. For colon cancer, physicalactivity accelerates the movement of foodthrough the intestine, thereby reducing thelength of time that the bowel lining isexposed to mutagens.36 For breast cancer,vigorous physical activity may decrease theexposure of breast tissue to circulatingestrogen.36 Physical activity may also affectcancers of the colon, breast, and other sites byimproving energy metabolism and reducingcirculating concentrations of insulin andrelated growth factors. Physical activity helpsto prevent adult-onset diabetes, which hasbeen associated with increased risk of cancersof the colon, pancreas, and possibly othersites.37,38,39,40 The benefits of physical activity gofar beyond reducing the risk of cancer,
however, and include reducing the risk ofother chronic diseases, such as heart disease,diabetes, osteoporosis, and hypertension.
Recommended Amount of Activity
There are many unanswered questionsabout the optimal intensity, duration, andfrequency of physical activity needed to reducecancer risk. However, current evidencesuggests that there is substantial risk reductionfor colon cancer from simply not beingsedentary. And by participating in moderate-to-vigorous physical activity at least 45 minuteson five or more days of the week, individualsmay achieve optimal activity levels needed toreduce the risk of developing both breast andcolon cancers, as well as several other types ofcancer, including kidney, endometrial, andesophageal cancer.30,41,42,43,44 Moderate-to-vigorous physical activity is needed tometabolize stored body fat and to modifyphysiological functions that affect insulin,estrogen, androgen, prostaglandins, andimmune function.5,45,46 This recommendationto include physical activity in one’s lifestyle toreduce cancer risk is supported by a recent
Volume 52 • Number 2 • March/April 2002 99
CA Cancer J Clin 2002;52:92-119
Examples of Moderate and Vigorous Intensity Physical Activities
Moderate Intensity Activities Vigorous Intensity Activities
Exercise Walking, dancing, leisurely bicycling, Jogging or running, fast bicycling,and Leisure ice skating, roller skating, horseback circuit weight training, aerobic
riding, canoeing, yoga dance, martial arts, jumping rope,swimming
Sports Volleyball, golfing, softball, baseball, Soccer, field or ice hockey,badminton, doubles tennis, lacrosse, singles tennis,downhill skiing racquetball, basketball,
cross-country skiing
Home Mowing the lawn, general lawn Digging, carrying and hauling,Activities and garden maintenance masonry, carpentry
Occupational Walking and lifting as part of the job Heavy manual labor (forestry,Activities (custodial work, farming, auto or construction work, fire fighting)
machine repair)
TABLE 3

extensive review by the World HealthOrganization.47
For people who are largely inactive or justbeginning a physical activity program, agradual increase to 30 minutes per day ofmoderate-to-vigorous physical activity on atleast five days per week will provide substantialcardiovascular benefits and aid in weightcontrol.48,49 Those who are already active at least30 minutes on most days of the week shouldstrive toward accumulating 45 minutes ofmoderate-to-vigorous activity on most days ofthe week. Selected examples of moderate andvigorous activities are provided in Table 3.
Moderate activities are those that requireeffort equivalent to a brisk walk. Vigorousactivities generally engage large muscle groupsand cause an increase in heart rate, breathingdepth and frequency, and sweating. Theseactivities can be performed in a variety ofsettings: occupational, recreational, in the homeor garden, and with friends or family.50,51 Whilethere is limited evidence regarding whether
physical activity is most protective if done in asingle session or incrementally throughout theday, it is reasonable to assume that benefit canbe accumulated in separate sessions of 20 to 30minutes each.
Adopting a physically active lifestyleinvolves making deliberate decisions andchanging lifestyle behaviors in order to selectactive rather than sedentary behavior. Toenhance the ability of individuals to adopt amore active lifestyle, communities as well asindividuals need to implement changes. Ideasto reduce sedentary behavior are suggested inTable 4.
People who are less active thanrecommended by these guidelines shouldgradually increase the intensity, duration, andfrequency of physical activity. Most childrenand young adults can safely engage inmoderate physical activity without consultingtheir physicians. However, men over 40,women over 50, and people with chronicillnesses and/or established cardiovascular riskfactors should consult their physicians beforebeginning a vigorous physical activityprogram. Stretching and warm-up periodsshould be part of each exercise session toreduce risk of musculoskeletal injuries. Moredetailed information on exercise safety can befound in the Surgeon General’s Report onPhysical Activity and Health.52
Because one of the best predictors of adultphysical activity is activity levels duringchildhood and adolescence, and because of thecritical role physical activity plays in weightmaintenance, children and adolescents shouldbe encouraged to be physically active atmoderate-to-vigorous intensities for at least 60minutes per day on five or more days perweek.53,53a Such activities should include sportsand fitness activities at school and at home.Tohelp achieve activity goals, daily physicaleducation programs and activity breaks shouldbe provided for children at school, and
100 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
Suggested Ways to Reduce Sedentary Behavior
Use stairs rather than an elevator.
If you can, walk or bike to your destination.
Exercise at lunch with your co-workers, family, or friends.
Take a 10-minute exercise break at work to stretch or take a quick walk.
Walk to visit co-workers instead of sending an e-mailmessage.
Go dancing with your spouse or friends.
Plan active vacations rather than only driving trips.
Wear a pedometer every day and watch your daily stepsincrease.
Join a sports team.
Use a stationary bicycle while watching TV.
Plan your exercise routine to gradually increase the days per week and minutes per session.
TABLE 4

television viewing and computer game timeshould be minimized at home.
The health benefits of physical activity inpreventing cancer and other chronic diseasesare thought to accumulate over the course of alifetime5 and are facilitated by the developmentof healthy activity patterns in childhood.However, increasing the level of physicalactivity at any age can provide importanthealth benefits. Although it is uncertain at thepresent time whether increasing physicalactivity among the elderly will reduce cancerrisk, many other health benefits can beachieved by an appropriate exercise regimen,even among the elderly.54
3. Maintain a healthful weight throughout life.• Balance caloric intake with physical
activity.• Lose weight if currently overweight
or obese.
Balancing Energy Intake and Expenditure
Overweight and obesity are associatedwith increased risk for cancers at several sites:breast (among postmenopausal women),colon, endometrium, adenocarcinoma of theesophagus, gallbladder, pancreas, and kidney.These findings are supported both by animal studies and by epidemiologicalstudies.30,40,41,55,56,57,58,59,60
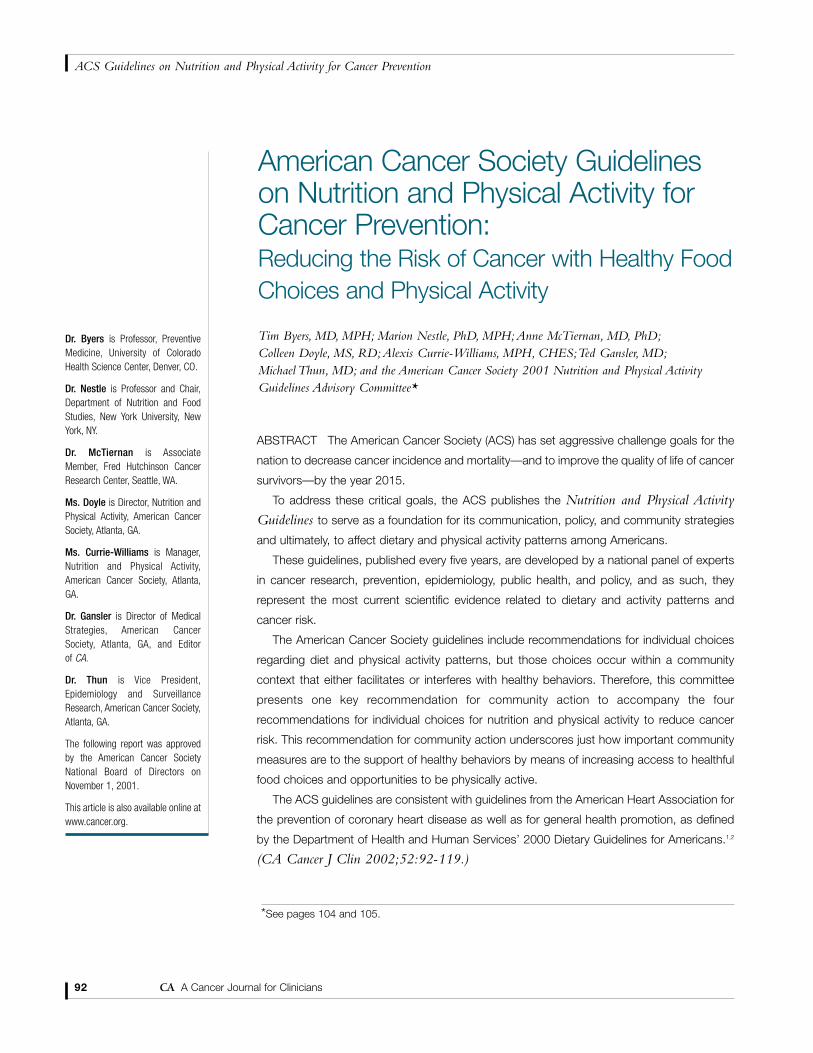
The Body Mass Index (BMI) is anexpression of weight-for-height calculated asbody weight in kilograms divided by height inmeters, squared.61 Exact cut-offs for BMI levelsat elevated risk are difficult to define, sinceepidemiological studies have used differentcutpoints in calculating cancer risks associatedwith body weight. However, experts considera BMI within the range of 18.5 to 25.0 kg/m2
to be healthful, a BMI between 25.0 and 29.9to be overweight, and a BMI of 30.0 and overto be obese (Figure 1). Individuals should
strive to maintain a BMI between 18.5 and25.0 kg/m2.
The best way to achieve a healthful bodyweight is to balance energy intake (foodintake) with energy expenditure (physicalactivity). Excess body fat can be reduced byrestricting caloric intake and increasingphysical activity. Caloric intake can be reducedby decreasing the size of food portions andlimiting the intake of calorie-dense foods highin fat and refined sugars (e.g., fried foods,cookies, cakes, candy, ice cream, and softdrinks). Such foods should be replaced withfoods like vegetables and fruits, whole grains,and beans. People should be aware that mealsserved in restaurants typically exceed theportion sizes needed to meet recommendeddaily caloric intake. Physical activity as well asdiet is essential for maintenance of a healthfulweight (see Recommendations for IndividualChoices, recommendation number two,page 99).
As yet, no studies have convincinglydemonstrated that losing weight reduces therisk of cancer, although there are biologicallyplausible mechanisms to suggest that weightloss might be beneficial. Overweight or obeseindividuals who intentionally lose weight havereduced levels of circulating glucose, insulin,and bioavailable estrogens and androgens. Thehealth effects of intentional weight loss aredifficult to evaluate, because people whomanage to lose weight may do so because ofunrecognized illness. Weight loss that resultsfrom an underlying illness or from smokingdoes not benefit one’s health. Even though ourknowledge about the relationship betweenweight loss and cancer risk is incomplete,individuals who are overweight and obeseshould be encouraged and supported in theirefforts to reduce weight. Obesity is a major riskfactor not only for cancer, but also for diabetes,stroke, and coronary heart disease.
Because overweight in youth tends to
Volume 52 • Number 2 • March/April 2002 101
CA Cancer J Clin 2002;52:92-119

102 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
6'6"
6'5"
6'4"
6'3"
6'2"
6'1"
6'0"
5'11"
5'10"
5'9"
5'8"
5'7"
5'6"
5'5"
5'4"
5'3"
5'2"
5'1"
5'0"
4'11"
4'10"
Healthy Weight BMI from 18.5 up to 25 refers to healthy weight.
Height*
Pounds†
BMI (Body Mass Index)
18.5
25 30
Overweight BMI from 25 up to 30 refers to overweight.
Obese BMI 30 or higher refers to obesity. Obese persons are also overweight.
*Without shoes. †Without clothes.
50 75 100 125 150 175 200 225 250 275
BMI measures weight in relation to height. The BMI ranges shown above are for adults. They are not exact ranges of healthy and unhealthy weights. However, they show that health risk increases at higher levels of overweight and obesity. Even within the healthy BMI range, weight gains can carry health risks for adults.
Directions: Find your weight on the bottom of the graph. Go straight up from that point until you come to the line that matches your height. Then look to find your weight group.
FIGURE 1
Are You at a Healthy Body Weight?
Source: Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2000, page 3.The higher weights apply mainly to men who have more muscle and bone. To use this chart, find your height in feet and inches (without shoes) along the left side of the graph. Trace the line corresponding to your height across the figure until it intersects with the vertical line corresponding to your weight in pounds (without clothes). The point of intersection lies within aband that indicates whether your weight is healthy or is moderately or severely overweight.

continue throughout life, the increasingprevalence of overweight and obesity in pre-adolescents and adolescents may increase theincidence of cancer in the future. For thesereasons, efforts to establish healthful weight,physical activity habits, and patterns of weightgain should begin in childhood.
4. If you drink alcoholic beverages, limitconsumption.
People who drink alcohol should limit theirintake to no more than two drinks per day formen and one drink a day for women.2 Therecommended limit is lower for womenbecause of their smaller body size and slowermetabolism of alcohol. A drink of alcohol isdefined as 12 ounces of beer, five ounces ofwine, or 1.5 ounces of 80-proof distilled spirits.Alcohol consumption is an established cause ofcancers of the mouth, pharynx, larynx,esophagus, liver, and breast.62,63 Alcoholconsumption may also be related to increasedrisk of colon cancer. For each of these cancers,risk increases substantially with intake of morethan two drinks per day.Alcohol consumptioncombined with tobacco increases the risk ofcancers of the mouth, larynx, and esophagus farmore than the independent effect of eitherdrinking or smoking. Furthermore, regularconsumption of even a few drinks per weekhas been associated with an increased risk ofbreast cancer in women. The mechanism bywhich alcohol is related to breast cancer is notknown with certainty, but may be due toalcohol-induced increases in circulatingestrogens or other hormones in the blood,reduction of folic acid levels, or to a directeffect of alcohol or its metabolites on breasttissue.64 Reducing alcohol consumption maybe an important way for many women toreduce their risk of breast cancer. Some studiessuggest that consuming the recommendedamount of the vitamin folic acid can minimizethe increased risk of breast cancer from
alcohol, but this relationship has not beenfirmly established.4
Complicating the recommendation foralcohol and cancer risk reduction is theevidence that even moderate intake ofalcoholic beverages appears to decrease the riskof coronary heart disease in both men andwomen.65,66 Even though alcohol can reducethe risk of coronary heart disease in women,those women who are at high risk of breastcancer might reasonably consider abstainingfrom alcohol. Public health officials advisepeople who already drink alcoholic beveragesto limit their intake to two drinks a day formen and one drink per day for women.Thereis no compelling reason for adults whocurrently do not consume alcoholic beveragesto start consuming alcohol to reduce their riskfor heart disease, as cardiovascular risk can bereduced by not smoking, consuming a low-saturated fat diet, avoiding obesity, stayingphysically active on a regular basis, andcontrolling blood pressure.
Some groups of people should not drinkalcoholic beverages at all. These includechildren and adolescents; individuals of anyage who cannot restrict their drinking tomoderate levels; women who are or maybecome pregnant; individuals who plan todrive or operate machinery or who take partin other activities that require attention, skill,or coordination; and individuals takingprescriptions or over-the-counter medicationsthat can interact with alcohol.
DIET AND PHYSICAL ACTIVITY FACTORS
THAT AFFECT RISKS FOR THE MOST
COMMON CANCERS
While the diet and activity factors presentedwithin the guidelines are intended to reduceoverall cancer risk, certain dietary and physicalactivity habits affect specific cancer sites. Thissection summarizes the relation of diet and
Volume 52 • Number 2 • March/April 2002 103
CA Cancer J Clin 2002;52:92-119

physical activity factors toparticular common cancersin the United States.
Bladder Cancer
The major risk factors forbladder cancer are tobaccosmoking and exposure tocertain industrial chemicals.Limited evidence suggeststhat drinking more fluidsmay lower the risk ofbladder cancer, as may eatingmore vegetables.67
Brain Cancer
There are no knownnutritional risk factors forbrain cancer.
Breast Cancer
Breast cancer is the mostcommon cancer diagnosedamong American womenand is second only to lungcancer as a cause of cancerdeaths in women.The risk ofbreast cancer is increased byseveral reproductive andother factors that presently
cannot be easily modified: menarche beforeage 12, nulliparity or first birth at age greaterthan 30, late age at menopause, and a familyhistory of breast cancer. Risk, however, can bereduced by changes in behavior, includinglimiting the use of hormone replacementtherapy, avoiding obesity, staying physicallyactive, and breast feeding.
Some studies also suggest that diets high invegetables and fruits decrease the risk for breastcancer, although this evidence is much weaker
than for other cancer sites. Alcohol increasesrisk modestly, however, and increasingevidence suggests that longer duration andgreater intensity of physical activity areassociated with reduced risk of breast cancer.At the present time, the best nutritional adviceto reduce the risk of breast cancer is to engagein vigorous physical activity at least four hoursa week, avoid or limit intake of alcoholicbeverages to no more than one drink per day,and minimize lifetime weight gain through thecombination of caloric restriction and regularphysical activity.5,34,55,60,64
Colorectal Cancer
Colorectal cancer is the second leading causeof cancer death among American men andwomen combined. Risk of colorectal cancer isincreased in those with a family history ofcolorectal cancer. In addition to diet andphysical activity, several other modifiable riskfactors influence the etiology of this cancer.Risk is increased by tobacco use and possiblyexcessive alcohol consumption. Risk may bedecreased by use of aspirin or other non-steroidal anti-inflammatory drugs and, possibly,by hormone replacement therapy. Currently,however, neither aspirin-like drugs norpostmenopausal hormones are recommendedto prevent colorectal cancer because of theirpotential side effects. Studies demonstrate alower risk of colon cancer among those whoare moderately active on a regular basis, andincreasing evidence suggests that more vigorousactivity may have an even greater benefit inreducing the risk of colon cancer.33,42 Physicalinactivity is more consistently associated withincreased risk of cancer of the colon thancancer of the rectum. Diets high in vegetablesand fruits have been associated with decreasedrisk, and diets high in red meat have beenassociated with increased risk of coloncancer.25,27,28 There is some evidence that folic
104 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
*AMERICAN CANCER SOCIETY 2001NUTRITION AND PHYSICAL ACTIVITYGUIDELINES ADVISORY COMMITTEE
American Cancer Society VolunteerParticipants:Tim Byers, MD, MPH,† Professor,Preventive Medicine, University ofColorado Health Science Center, Denver,CO and Marion Nestle, PhD MPH,†
Professor and Chair, Department ofNutrition and Food Studies, New YorkUniversity, New York, NY (Co-Chairs);Barbara Ainsworth, PhD, MPH, AssociateProfessor of Epidemiology, Department ofEpidemiology and Biostatistics, Norman J.Arnold School of Public Health, Universityof South Carolina, Columbia, SC; Dileep G.Bal, MD, Chief, Cancer Control Branch,California Department of Health Services,Sacramento, CA; Abby Bloch, PhD, RD,FADA, Nutrition Consultant, New York, NY;Ralph J. Coates, PhD, Associate Directorfor Science, Division of Cancer Preventionand Control, CDC, Atlanta, GA; WendyDemark-Wahnefried, PhD, RD, AssociateResearch Professor of Surgery, DukeUniversity Medical Center, Durham, NC;Patricia J. Elmer, PhD, Center for HealthResearch, Portland, OR, representing theAmerican Heart Association; Susan B.Foerster, MPH, RD, California Departmentof Health Services, Sacramento, CA; PeterGann, MD, ScD, Associate Professor,Preventive Medicine, NorthwesternUniversity, Chicago, IL; Edward L.Giovannucci, MD, ScD, AssociateProfessor of Medicine, Harvard School ofPublic Health, Boston, MA; E. J.Hawrylewicz, PhD, Director of Research,Senior Attending, Emeritus, Mercy Hospitaland Medical Center, Chicago, IL; Jerianne Heimendinger, ScD, MPH, RD,Research Scientist and Lifestyles ResearchCenter Acting Director, Center forBehavioral and Community Studies, AMCCancer Research Center, Denver, CO;

acid supplements may reduce the risk of coloncancer. The best nutritional advice to reducethe risk of colon cancer is to increase theintensity and duration of physical activity; eatmore vegetables and fruits; limit intake of redmeat; avoid obesity; and avoid excess alcoholconsumption.33,40,42,43 In addition, it is veryimportant to follow the ACS guidelines forregular colorectal screening, as identifying andremoving polyps in the colon can preventcolorectal cancer (see Smith R, Cokkinides V, vonEschenbach A, et al. American Cancer SocietyGuidelines for the Early Detection of Cancer. CACancer J Clin 2002;52:8-22).
Endometrial Cancer
Studies of endometrial cancer consistentlyfind that obesity and use of hormonereplacement therapy after menopause increasecancer risk.The association with overweight isthought to result from the increase in estrogenlevels that occurs among postmenopausalwomen who are overweight. Consumption ofvegetables and fruits may decrease risk ofendometrial cancer. At the present time, thebest advice to reduce the risk of endometrialcancer is to maintain a healthful weightthrough diet and regular physical activity, andeat at least five servings of vegetables and fruitseach day.30
Kidney Cancer
Kidney cancer risk is increased among thosewho are overweight. The reason for this isunknown.The best nutritional advice to lowerrisk for kidney cancer is to avoid becomingoverweight.58
Leukemias and Lymphomas
There are no known nutritional risk factorsfor leukemias or lymphomas.
Lung Cancer
Lung cancer is the leadingcause of cancer death amongAmericans. More than 85percent of lung cancersoccur because of tobaccosmoking. Many studies havedemonstrated that the risk oflung cancer is lower amongsmokers and nonsmokerswho consume at least fiveservings of vegetables andfruits a day. Althoughhealthful eating may reducethe risk of lung cancer, therisks posed by tobaccoremain substantial. Nutri-tional supplementation withhigh doses of beta-caroteneand/or vitamin A hasincreased (not decreased)lung cancer risk amongsmokers (see Beta-carotene,page 107). At the presenttime, the best advice toreduce the risk of lungcancer is to avoid tobaccouse or exposure, and to eat at least five servings of vegetables and fruits every day.6,13,14,15
Oral and Esophageal Cancers
Tobacco (including cigarettes, chewingtobacco, and snuff) and alcohol, alone, butespecially when used together, increase therisk for cancers of the mouth and esophagus.Obesity increases the risk for adenocarcinomaoccurring in the lower esophagus and at thejunction of the esophagus and stomach, likelydue to the increased acid reflux fromabdominal obesity. Eating recommended
Volume 52 • Number 2 • March/April 2002 105
CA Cancer J Clin 2002;52:92-119
Laurence Kolonel, MD, PhD, DeputyDirector, Cancer Research Center,University of Hawaii, Honolulu, HI; LarryKushi, PhD, Associate Director forEpidemiology, Division of Research, KaiserPermanente of Northern California,Oakland, CA; Bonnie Liebman, MS,Director of Nutrition, Center for Science inthe Public Interest, Washington, DC; M.Elena Martinez, PhD, RD, AssociateProfessor of Public Health, Arizona CancerCenter, and College of Public Health,University of Arizona, Tucson, AZ; AnneMcTiernan, MD, PhD,† Associate Member,Fred Hutchinson Cancer Research Center,Seattle, WA; Esther F. Myers, PhD, RD,FADA, Director, Scientific Affairs andResearch, American Dietetic Association,Chicago, IL; Arthur Schatzkin, MD, DrPH,Chief, Nutrition Epidemiology Branch,National Cancer Institute, Bethesda, MD;Marty Slattery, PhD, MPH, Professor,Family and Preventive Medicine, School ofMedicine University of Utah, Salt Lake City,UT
American Cancer Society StaffParticipants:Rick Alteri, MD, Associate Medical Editor;Colleen Doyle, MS, RD,† Director, Nutritionand Physical Activity; Vilma Cokkinides,PhD, Program Director Risk FactorSurveillance; Alexis Currie-Williams,MPH, CHES,† Manager, Nutrition andPhysical Activity; Ted Gansler, MD,†
Director of Medical Strategies; WendiKlevan, Director, Cancer ControlCommunications; Marji McCullough,ScD, RD, Senior Epidemiologist; DavidRinger, PhD, MPH, Scientific ProgramDirector; Robert A. Smith, PhD, Director,Cancer Screening; Hugh Stallworth, MD,MPH, National Vice President, Cancer Riskand Sites; Michael Thun, MD,† VicePresident, Epidemiology and SurveillanceResearch; Shalini Vallabhan, PhD,Director, Policy Research, NationalGovernment Relations Department
† Member, Executive Editorial Subcommittee.

amounts of vegetables and fruits probablyreduces the risk of oral and esophagealcancers.At the present time, the best advice toreduce the risk of oral and esophageal cancersis to avoid all forms of tobacco, restrictalcohol consumption, avoid obesity, and eat at least five servings of vegetables and fruitseach day.68,69,70
Ovarian Cancer
There are no firmly established nutritionalrisk factors for ovarian cancer, though vegetableand fruit consumption may lower risk.
Pancreatic Cancer
Pancreatic cancer is the fifth leading cause ofcancer death in the United States, accountingfor nearly 30,000 deaths annually. Substantialevidence indicates that tobacco smoking,adult-onset diabetes, and impaired glucosetolerance increase the risk for pancreaticcancer.39 Some studies have also shown thatobesity and physical inactivity (both factorsstrongly linked to abnormal glucosemetabolism) are associated with elevatedpancreatic cancer risk, and that fruit andvegetable intake is associated with reducedrisk.59 At the present time, the best advice toreduce the risk of pancreatic cancer is to avoidtobacco use, maintain a healthful weight,remain physically active, and eat five or moreservings of vegetables and fruits each day.
Prostate Cancer
Prostate cancer is the most common canceramong American men.While prostate cancer isclearly related to male sex hormones, just hownutritional factors might increase risk remainsuncertain. Several studies have found highconsumption of red meat and dairy products tobe associated with increased risk of prostate
cancer.29,71 There is also evidence that a highcalcium intake, primarily through supplements,is associated with increased risk for moreaggressive types of prostate cancer.72 Otherstudies suggest that diets high in certainvegetables (including tomatoes, beans, andother legumes) are associated with decreasedrisk. Current evidence for these associations islimited, however. The possibility that specificnutrients in foods, notably vitamin E, selenium,and lycopene, may protect against prostatecancer is under active investigation. At thepresent time, the best advice to reduce the riskof prostate cancer is to limit intake of animal-based products, especially red meats and high-fat dairy products; and eat five or more servingsof vegetables and fruits each day.
Stomach Cancer
The incidence of stomach cancer continuesto decrease worldwide, especially in the UnitedStates.Year-round consumption of fresh foodsmade possible by refrigeration, and otherimprovements in food preservation methodshave likely helped to reduce the rate ofstomach cancer, as has concomitant reductionin the prevalence of chronic stomach infectionsby the bacterium Helicobacter pylori. At thepresent time, the best advice to reduce the riskof stomach cancer is to eat at least five servingsof vegetables and fruits daily.73
COMMON QUESTIONS ABOUT DIET AND CANCER
Because people are interested in therelationship specific foods or nutrients have tospecific cancers, research on dietary factors andcancer risk is often widely publicized. Healthprofessionals who counsel patients shouldemphasize that no one study provides the lastword on any subject, and that individual newsreports may overemphasize what appear to be
106 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

contradictory or conflicting results. In briefnews stories, reporters cannot always put newresearch findings in their proper context. Thebest advice about diet and physical activity isthat it is rarely, if ever, advisable to change dietor activity levels based on a single study ornews report, especially if the data are reportedas “preliminary findings.” The followingquestions and answers address commonconcerns about diet and physical activity inrelation to cancer.
Alcohol
Does alcohol increase cancer risk? Alcoholincreases the risk of cancers of the mouth,pharynx, larynx, esophagus, liver, and breast.People who drink alcohol should limit theirintake to no more than two drinks per day formen and one drink per day for women.A drinkis defined as 12 ounces of beer, 5 ounces ofwine, or 1.5 ounces of 80-proof distilled spirits.The combination of alcohol and tobaccoincreases the risk of cancer far more than theindependent effects of either drinking orsmoking. Regular consumption of even a fewdrinks per week is associated with an increasedrisk of breast cancer in women.Women at highrisk of breast cancer may consider abstainingfrom alcohol (see Recommendations for IndividualChoices, recommendation number four, page103).2,62,63,64
Antioxidants
What are antioxidants and what do they have todo with cancer? Certain nutrients in vegetablesand fruits appear to protect the body against thedamage to tissues that occurs constantly as aresult of normal metabolism. Because suchdamage is associated with increased cancer risk,the so-called “antioxidant nutrients” are thoughtto protect against cancer.8 Antioxidants includevitamin C, vitamin E, selenium, carotenoids, and
many other phytochemicals. Studies suggest thatpeople who eat more vegetables and fruits,which are rich sources of antioxidants, have alower risk for some types of cancer. Clinicalstudies of antioxidant supplements are currentlyunderway, but studies have not yet demonstrateda reduction in cancer risk from vitaminsupplements (see also Beta-carotene below;Lycopene, page 110; Selenium, page 111; VitaminE, page 114; Supplements, page 112). To reducecancer risk, the best advice presently is toconsume antioxidants through food sourcesrather than supplements.
Aspartame
Does aspartame cause cancer? Aspartame is alow-calorie artificial sweetener that is about200 times sweeter than sugar. Current evidencedoes not demonstrate any link betweenaspartame ingestion and increased cancer risk. People with the genetic disorderphenylketonuria should avoid aspartame intheir diets.
Beta-carotene
Does beta-carotene reduce cancer risk? Becausebeta-carotene, an antioxidant chemicallyrelated to Vitamin A, is found in vegetables andfruits, and because eating vegetables and fruitsis associated with a reduced risk of cancer, itseemed plausible that taking high doses ofbeta-carotene supplements might reducecancer risk. In three major clinical trials, peoplewere given high doses of synthetic beta-carotene in an attempt to prevent lung cancerand other cancers. Two studies found beta-carotene supplements to be associated with ahigher risk of lung cancer in cigarette smokers,and a third found neither benefit nor harmfrom beta-carotene supplements. Therefore,consuming vegetables and fruits that containbeta-carotene may be helpful, but high-dose
Volume 52 • Number 2 • March/April 2002 107
CA Cancer J Clin 2002;52:92-119

beta-carotene supplements may be harmful,especially for cigarette smokers.14,15,16
Bioengineered Foods
What are bioengineered foods, and are they safe?Bioengineered foods are made by adding genesfrom other plants or organisms to increase aplant’s resistance to insect pests, retard spoilage,or improve transportability, flavor, nutrientcomposition, or other desired qualities. Intheory, these added genes might createsubstances that could cause adverse reactionsamong sensitized or allergic individuals.However, there is currently no evidence thatthe substances found in bioengineered foodsnow on the market are harmful or that theywould either increase or decrease cancer riskbecause of the added genes.
Calcium
Is calcium related to cancer? Several studieshave suggested that foods high in calciummight help reduce the risk for colorectalcancer,74 and calcium supplementationmodestly reduces the formation of colorectaladenomas.There is also evidence, however, thata high calcium intake, primarily throughsupplements, is associated with increased riskfor prostate cancer, especially for prostatecancers that are more aggressive.72 In light ofthis, both men and women should strive toconsume recommended levels of calciumintake, primarily through food sources.Recommended intake levels of calcium are1000 mg/day for people aged 19 to 50 and1200 mg/day for people over 50 years old.Dairy products are excellent sources ofcalcium, as are some leafy vegetables andgreens. People who obtain much of theircalcium from dairy products should select lowor nonfat choices to reduce intake of saturatedfat.Those wishing to take calcium supplements
should consult with their health care provider.
Cholesterol
Does cholesterol in the diet increase cancer risk?Cholesterol in the diet comes only from foodsderived from animal sources—meat, dairyfoods, eggs, and animal fats.At present, there islittle evidence that cholesterol itself causes theincreased risk of certain cancers associated witheating foods from animal sources. Loweringblood cholesterol lowers cardiovascular diseaserisk, but there is no evidence that loweringblood cholesterol has an effect on cancer risk.
Coffee
Does drinking coffee cause cancer? Caffeine mayheighten symptoms of fibrocystic breast lumps(a type of benign breast disease) in somewomen, but there is no evidence that itincreases the risk of breast cancer or othertypes of cancer.The association between coffeeand pancreatic cancer, widely publicized in thepast, has not been confirmed by other studies.
Fat
Will eating less fat lower cancer risk? Diets highin fat are also high in calories and contribute toobesity, which in turn is associated withincreased risk of cancers at several sites.Although all types of fats have similar numbersof calories, there is some evidence that certaintypes, such as saturated fats, may have a greatereffect on increasing cancer risk, and that fatscontaining omega-3 fatty acids may reducecancer risk (see Recommendations for IndividualChoices, recommendation number one,page 95).
Fiber
What is dietary fiber and can it prevent cancer?Dietary fiber includes a wide variety of plant
108 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

carbohydrates that are not digestible byhumans. Specific categories of fiber are“soluble” (like oat bran) or “insoluble” (likewheat bran and cellulose). Soluble fiber helpsto reduce blood cholesterol and therefore,helps lower the risk of coronary heart disease.Good sources of fiber are beans, vegetables,whole grains, and fruits. Associations betweenfiber and cancer risk are inconclusive, butconsumption of these foods is stillrecommended because they contain othersubstances that can help prevent cancer andbecause of their other health benefits.
Fish Oils
Does eating fish protect against cancer? Fish is arich source of omega-3 fatty acids. Studies inanimals have found that these fatty acidssuppress cancer formation, and there is limitedsuggestive evidence of a possible benefit inhumans. Research has not yet demonstratedwhether the possible benefits of fishconsumption may be reproducible by takingomega-3 or fish oil supplements.
Fluorides
Do fluorides cause cancer? Extensive researchhas examined the effects of fluorides given asdental treatments, or added to toothpaste,public water supplies, or foods. Fluorides donot increase cancer risk.
Folic Acid
What is folic acid and can it prevent cancer?Folic acid (closely related to folate or folacin)is a B vitamin found in many vegetables,beans, fruits, whole grains, and fortifiedbreakfast cereals. Since 1998, all grainproducts have been fortified with folic acid.75
Folic acid deficiency may increase the risk ofcancers of the colorectum and breast.
Current evidence suggests that to reducecancer risk, folic acid is best obtained throughconsumption of vegetables, fruits, andenriched grain products.
Food Additives
Do food additives cause cancer? Manysubstances are added to foods to preserve themand to enhance color, flavor, and texture.Additives are usually present in very smallquantities in food, and no convincing evidenceexists that any additive consumed at these levelscauses human cancers.
Garlic
Can garlic prevent cancer? The health benefitsof the allium compounds contained in garlicand other vegetables in the onion family havebeen publicized widely, mostly because garlichas very small effects on blood cholesterollevels. Garlic is currently under study for itsability to reduce cancer risk. Insufficientevidence exists at this point to support aspecific role for this vegetable in cancerprevention.
Genetics
If our genes determine cancer risk, how can diethelp prevent cancer? Damage to the genes thatcontrol cell growth and maturation can eitherbe inherited or acquired during one’s lifetime.Certain types of mutations or genetic damagecan increase the risk of cancer. Nutrients in thediet can protect DNA from being damaged.Physical activity, weight control, and diet mightdelay or prevent the development of cancer inpeople with an increased genetic risk forcancer. The many interactions between dietand genetic factors are an important andcomplex topic of widespread current researchinterest.
Volume 52 • Number 2 • March/April 2002 109
CA Cancer J Clin 2002;52:92-119

Irradiated Foods
Why are foods irradiated, and do irradiated foodscause cancer? Radiation is increasingly used tokill harmful organisms on foods in order toextend their “shelf life.” Radiation does notremain in the foods after treatment, however,and there is no evidence that consumingirradiated foods increases cancer risk.
Lycopene
Will lycopene reduce cancer risk? Lycopene isthe red-orange carotenoid antioxidant found athigh levels in tomatoes and tomato-basedfoods. Several studies have reported thatconsumption of tomato products reduces therisk of some cancers. It is uncertain, however,whether lycopene is the micronutrientresponsible for this association. Absorption oflycopene is increased when lycopene-richvegetables are cooked and are consumedtogether with fat, although only very smallamounts of fat are needed for absorption. Evenif lycopene in foods is associated with lowerrisk for cancer, it does not follow that highdoses taken as supplements would be eithermore effective or safe.12
Meat: Cooking and Preserving
Should I avoid processed meats? Someepidemiological studies have linked highconsumption of processed meats withincreased risk of colorectal and stomachcancers. This association may or may not bedue to nitrites, which are added to manyluncheon meats, hams, and hot dogs tomaintain color and to prevent contaminationwith bacteria. Nitrites can be converted withinthe stomach into carcinogenic nitrosamines,which may increase the risk of gastric cancer.Diets high in vegetables and fruits containingvitamin C and phytochemicals retard theconversion of nitrites into nitrosamines.
Consumption of meats preserved by methodsinvolving smoke or salt increases exposure topotentially carcinogenic chemicals, and soshould be minimized.76
How does cooking meat affect cancer risk?Adequate cooking is necessary to kill harmfulmicroorganisms within meat. However, someresearch suggests that frying, broiling, orgrilling meats at very high temperatures createschemicals that might increase cancer risk.Although studies show these chemicals causecancer in animals, it is uncertain whether theyactually cause cancer in humans. Techniquessuch as braising, steaming, poaching, stewing,and microwaving meats minimize theproduction of these chemicals.
Obesity
Does being overweight increase cancer risk? Yes.Overweight and obesity are associated withincreased risk for cancers of the breast (among postmenopausal women), colon,endometrium, gallbladder, adenocarcinoma ofthe esophagus, pancreas, renal cell (kidney)carcinoma, and possibly other sites as well (see Recommendations for Individual Choices,recommendation number three, page101).55,56,57,58,59,60
Olive Oil
Does olive oil affect cancer risk? Consumptionof olive oil is not associated with any increasedrisk of cancer, and is most likely neutral withrespect to cancer risk.77 Olive oil is a significantsource of calories and should be used inmoderation.
Organic Foods
Are foods labeled “organic” more effective inlowering cancer risk? The term “organic” ispopularly used to designate plant foods grown
110 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

without pesticides and genetic modifications.At present, no research exists to demonstratewhether such foods are more effective inreducing cancer risk than are similar foodsproduced by other farming methods.
Pesticides and Herbicides
Do pesticides in foods cause cancer? Pesticidesand herbicides can be toxic when usedimproperly in industrial, agricultural, or otheroccupational settings. Although vegetables andfruits sometimes contain low levels of thesechemicals, overwhelming scientific evidencesupports the overall health benefits and cancer-protective effects of eating vegetables andfruits. At present there is no evidence thatresidues of pesticides and herbicides at the lowdoses found in foods increase the risk ofcancer.78
Physical Activity
Will increasing physical activity lower cancer risk?Yes. People who engage in moderate-to-vigorous levels of physical activity are at lowerrisk of developing colon and breast cancer thanthose who do not.5,33,34,35,36 This risk reduction isindependent of the impact of activity onweight. Data for a direct effect on the risk ofdeveloping other cancers are more limited.Nonetheless, overweight and obesity have beenassociated with many types of cancer, andphysical activity is a key component ofmaintaining or achieving a healthful bodyweight. In addition, physical activity has abeneficial impact on cardiovascular disease anddiabetes (see Recommendations for IndividualChoices, recommendation number two, page99).
Phytochemicals
What are phytochemicals, and do they reducecancer risk? The term “phytochemicals” refers
to a wide variety of compounds produced byplants. Some of these compounds protectplants against insects or have other biologicallyimportant functions. Some have eitherantioxidant or hormone-like actions both inplants and in people who eat them. Becauseconsumption of vegetables and fruits reducescancer risk, researchers are searching forspecific components that might account for thebeneficial effects. There is no evidence thatphytochemicals taken as supplements are asbeneficial as the vegetables, fruits, beans, andgrains from which they are extracted.
Saccharin
Does saccharin cause cancer? High doses of theartificial sweetener saccharin cause theformation of bladder stones that can lead tobladder cancer in rats. Saccharin consumptiondoes not cause the formation of bladder stonesin humans. If saccharin would increase cancerrisk in humans, it would do so at doses manytimes greater than amounts typically consumedby people.4 Large epidemiological studies havenot reported increases in bladder cancersamong people using saccharin, and saccharinhas been removed from the list of establishedhuman carcinogens by the US NationalToxicology Program.78
Salt
Do high levels of salt in the diet increase cancerrisk? Studies in other countries link dietscontaining large amounts of foods preserved bysalting and pickling with an increased risk ofstomach, nasopharyngeal, and throat cancer.No evidence suggests that salt used in cookingor in flavoring foods affects cancer risk.
Selenium
What is selenium and can it reduce cancer risk?Selenium is a mineral needed by the body as
Volume 52 • Number 2 • March/April 2002 111
CA Cancer J Clin 2002;52:92-119

part of antioxidant defense mechanisms.Animal studies suggest that selenium protectsagainst cancer, and one experimental trial hasshown selenium supplements might reduce therisk of cancers of the lung, colon, and prostate.However, repeated and well-controlled studiesare needed to confirm whether selenium ishelpful in preventing these cancers.79 High-dose selenium supplements are notrecommended, as there is only a narrowmargin between safe and toxic dosages. Themaximum dose in a supplement should notexceed 200 micrograms per day. Seafood,meats, and grain products are good sources ofselenium.
Soy Products
Can soybeans reduce cancer risk? Soy-derivedfoods are an excellent source of protein and agood alternative to meat. Soy contains severalphytochemicals, some of which have weakestrogenic activity and appear to protect againsthormone-dependent cancers in animalstudies.24,80 Most of the human studies compareAsian and Western populations, whosedifferences in cancer risk, however, may be dueto factors other than soy consumption.Consumption of soy milk and soy powder hasbeen shown to decrease concentrations ofcirculating estrogens. However, thephytoestrogens in soy are themselves weaklyestrogenic, and the effects of dietary soy or ofspecific doses of soy-containing foods oncancer risk are unknown. Presently noconvincing data exist to support the theorythat soy supplements are beneficial in reducingcancer risk. There is a theoretical possibilitythat high doses of soy might increase the riskof estrogen-responsive cancers, such as breastor endometrial cancer, in certain individuals.Breast cancer survivors should consume onlymoderate amounts of soy foods as part of ahealthy plant-based diet, and should notintentionally ingest very high levels of soy
products in their diet or more concentratedsources of soy, such as soy-containing pills,powders, or supplements containing isolated orconcentrated isoflavones (see Brown J, Byers T,Thompson K, et al. Nutrition During and AfterCancer Treatment: A Guide for Informed Choices by Cancer Survivors. CA Cancer J Clin 2001;51:153-187).
Sugar
Does sugar increase cancer risk? Sugar increasescaloric intake without providing any of thenutrients that reduce cancer risk. Bypromoting obesity and elevating insulin levels,high sugar intake may increase cancer risk.White (refined) sugar is no different frombrown (unrefined) sugar or honey with regardto these effects on body weight or insulin.
Supplements
Can nutritional supplements lower cancer risk?There is strong evidence that a diet rich invegetables, fruits, and other plant-based foodsmay reduce the risk of cancer, but there is noevidence at this time that supplements canreduce cancer risk. The few intervention/clinical trials done in human populationsdesigned to test whether supplements canreduce cancer risk have yielded disappointingresults.Vitamin and mineral supplements havebeen shown to reduce the risk of stomachcancer in intervention studies of malnourishedpersons in China and South America,81 butother studies using high doses of singlenutrients have shown no benefit and have evenshown harm (see Beta-carotene, page 107). Foodis the best source of vitamins and minerals.Supplements, however, may be beneficial forsome people, such as pregnant women, womenof childbearing age, and people with restricteddietary intakes. If a supplement is taken, thebest choice is a balanced multivitamin/mineralsupplement containing no more than 100
112 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

percent of the “Daily Value” (formerly listed onsupplement labels as ‘RDA’) of most nutrients,since high doses of some nutrients can haveadverse effects.
Can I get the nutritional equivalent of vegetablesand fruits in a pill? No. Many healthfulcompounds are found in vegetables and fruits,and it is likely that these compounds worksynergistically to exert their beneficial effect. Inmany cases, it is not known which compoundsor combination of compounds are mostbeneficial in reducing cancer risk. There arelikely to be important, but as yet unidentified,components of whole food that are notincluded in supplements.Additionally, the smallamount of dried powder in the pills that arerepresented as being equivalent to vegetablesand fruits frequently contains only a smallfraction of the levels contained in the wholefoods.
Tea
Can drinking tea reduce cancer risk? Someresearchers have proposed that tea mightprotect against cancer because of its antioxidantcontent (see Antioxidants, page 107). In animalstudies, some teas (including green tea) havebeen shown to reduce cancer risk, butepidemiological studies have had mixedfindings. Presently, tea has not been proven toreduce cancer risk in humans.82
Trans-fats
Do trans-saturated fats increase cancer risk?Trans-saturated fats are produced during themanufacture of hydrogenated oils such asmargarine or shortening to make them solid at room temperature. Recent evidencedemonstrates that trans-fats have adversecardiovascular effects, such as raising bloodcholesterol levels.83 Their relationship to cancerrisk, however, has not been determined.84
Vegetables and Fruits
Will eating vegetables and fruits lower cancerrisk? Greater consumption of vegetables, fruits,or both together has been associated in themajority of epidemiological studies with alower risk of lung, oral, esophageal, stomach,and colon cancer. Because it is not knownwhich of the many compounds in vegetablesand fruits are most protective, the best advice isto consume five or more servings of a varietyof vegetables and fruits each day (seeRecommendations for Individual Choices,recommendation number one, page 95).9,10
What are cruciferous vegetables and are theyimportant in cancer prevention? Cruciferousvegetables belong to the cabbage family, andinclude broccoli, cauliflower, Brussels sprouts,and kale. These vegetables contain certainchemicals thought to reduce the risk forcolorectal cancer. The best evidence suggeststhat a wide variety of vegetables, includingcruciferous and other vegetables, reducescancer risk (also see Phytochemicals, page 111).
Is there a difference in the nutritional value offresh, frozen, and canned vegetables and fruits? Yes,but they can all be good choices. Fresh foodsare usually considered to have the mostnutritional value. However, frozen foods can bemore nutritious than fresh foods because theyare often picked ripe and quickly frozen.Canning is more likely to reduce the heatsensitive and water-soluble nutrients becauseof the high heat temperatures necessary in thecanning process. Be aware that some fruits arepacked in heavy syrup, and some cannedvegetables are high in sodium. Choosevegetables and fruits in a variety of forms.
Does cooking affect the nutritional value ofvegetables? Boiling vegetables, especially forlong periods, can leach out their content ofwater-soluble vitamins. Microwaving and
Volume 52 • Number 2 • March/April 2002 113
CA Cancer J Clin 2002;52:92-119

steaming may be the best ways to preserve thenutritional content in vegetables.
Should I be juicing my vegetables and fruits?Juicing can add variety to the diet, and can be agood way to consume vegetables and fruits,especially for those who have difficulty chewingor swallowing. Juicing also improves the body’sabsorption of some of the nutrients in vegetablesand fruits. However, juices may be less fillingthan whole vegetables and fruits and contain lessfiber. Fruit juice, in particular, can contribute lotsof calories to one’s diet. Commercially juicedproducts should be 100% vegetable or fruit juicesand should be pasteurized to eliminate harmfulmicroorganisms.
Vegetarian Diets
Do vegetarian diets reduce cancer risk?Vegetarian diets include many health-promoting features; they tend to be low insaturated fat and high in fiber, vitamins, andphytochemicals (e.g., flavonoids, etc.). It is notpossible to conclude at this time, however, thata vegetarian diet has any special benefits for theprevention of cancer.Vegetarian diets differ incomposition, although all avoid consumptionof red meat. A vegetarian diet can be quitehealthful if it is carefully planned and providesadequate calories. Diets including lean meats insmall to moderate amounts can be just ashealthful. The greater the restriction of foodgroups in a particular diet, the more possibilitythere is of dietary deficiencies. Strict vegetariandiets that avoid all animal products, includingmilk and eggs, should be supplemented withvitamin B12, zinc, and iron (especially forchildren and premenopausal women).
Vitamin A
Does vitamin A lower cancer risk? Vitamin A(retinol) is obtained from foods in two ways:preformed from animal food sources, andderived from beta-carotene in plant-based
foods.Vitamin A is needed to maintain healthytissues.Vitamin A supplements, whether in theform of beta-carotene or retinol, have not beenshown to lower cancer risk, and high-dosesupplements may, in fact, increase the risk forlung cancer.14,15
Vitamin C
Does vitamin C lower cancer risk? Vitamin C isfound in many vegetables and fruits. Manystudies have linked consumption of vitamin C-rich foods with a reduced risk for cancer.Thefew studies in which vitamin C has been givenas a supplement, however, have not shown areduced risk for cancer.85,86
Vitamin E
Does vitamin E lower cancer risk? One clinicaltrial showed that men who took vitamin E (50mg/day) had a lower risk of prostate cancercompared with men who took a placebo,14 butthis observation has yet to be confirmed.
Water and Other Fluids
How much water and other fluids should I drink?Consumption of water and other liquids mayreduce the risk of bladder cancer, as waterdilutes the concentration of carcinogens andshortens the time in which they are in contactwith the bladder lining. Drinking at least eightcups of liquid a day is usually recommended,and some studies indicate that even more maybe beneficial.65
AMERICAN CANCER SOCIETY GRADES FOR
BENEFIT VERSUS HARM
To review the strength of the scientificevidence, a guidelines subcommittee used amethod of summarizing the evidence similar tothe methods used by other expert panels. Forexample, the US Preventive Services Task Force
114 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

judged the scientific evidence related to clinicalpreventive services using a system thatconsidered both the source and strength of theevidence: from at least one controlled clinicaltrial, from good uncontrolled trials, frommultiple good observation studies, expertopinion, and case reports. They thencharacterized those guidelines on a five-pointgrading scheme as to the strength of theguideline: “good for recommending, fair forrecommending, insufficient to recommend foror against, fair for not recommending, good fornot recommending.” The American Institutefor Cancer Research (AICR) World CancerResearch Fund project summarized the nature
of the scientific evidence for nutritional factorsin cancer prevention as being either“convincing, probable, possible, or insufficient.”
The American Cancer Society sub-committee employed a method similar to bothgroups. For each issue, the committee judgedthe likelihood of benefit to the general public as follows:
A1. Convincing evidence for a benefit.A2. Probable benefit.A3. Possible benefit.
B. Insufficient evidence to concludebenefit or risk.
C. Evidence of lack of benefit.D. Evidence of harm.
Volume 52 • Number 2 • March/April 2002 115
CA Cancer J Clin 2002;52:92-119
TABLE 5
*Note: Group met in 2001 and recommendations were adopted by the American Cancer Society Board of Directors in November, 2001.
American Cancer Society Grades for Benefit Versus Harm (2001)*
Nutritional Factor Colorectal Breast Prostate Lung Esophageal, Stomach Pancreatic Bladder EndometrialCancer Cancer Cancer Cancer Oral Cancer Cancer Cancer Cancer Cancer
Increasing vegetable A2 A3 A3 A2 A2 A2 A3 A3 A3and fruit intake
Limiting intake of A2 B A3 B B C A3 C Bred meat
Increasing physical A1 A1 B B B B B B A2activity
Avoiding overweight A1 A1 C B A2 C A3 C A1
Limiting alcohol intake A3 A2 C B A1 C A3 C B
Consuming soy foods B B B B B B B B B
Taking beta-carotene B B C D B B B B Bsupplements
Taking vitamin E B B A3 C B B B B Bsupplements
Taking vitamin C B B B B B B B B Bsupplements
Taking folic acid A3 A3 B B B B B B Bsupplements
Taking selenium A3 B A3 A3 B B B B Bsupplements

THE AMERICAN CANCER SOCIETY’S COMMIT-
MENT TO NUTRITION AND PHYSICAL ACTIVITY
FOR CANCER PREVENTION
The American Cancer Society is committedto improving the ability of Americans to eat ahealthful diet and to be active because of thepotential impact of diet and activity on cancerrisk.The ACS has set aggressive challenge goalsfor the nation to decrease cancer incidence andmortality—and to improve the quality of life ofcancer survivors—by the year 2015. As part ofits strategic plan for achieving these goals, theACS has established nationwide nutrition andphysical activity objectives: to increase theawareness of the relationship of nutrition andphysical activity to cancer risk and to motivateand enable all Americans to lead a healthful andactive lifestyle.
To address these critical goals, the ACSpublishes its Nutrition and Physical ActivityGuidelines to serve as a foundation for itscommunication, policy, and communitystrategies and ultimately, to affect dietary andphysical activity patterns among Americans.These guidelines, published every five years, aredeveloped by a national panel of experts incancer research, prevention, epidemiology,public health, and policy, and they represent themost current scientific evidence related todietary and activity patterns and cancer risk.Recognizing that the ability to make healthfulchoices is often affected by factors within theenvironment in which people live, work, andplay, the guidelines also attempt to identify keysocial and structural factors that influenceaccess to resources for a healthful, activelifestyle.The ACS makes use of these guidelinesto influence legislative and regulatory issuesthat support nutrition and physical activity; toinfluence environmental changes that increasepublic access to and availability of healthfulfoods and opportunities for physical activity; toadvise the public about issues related to
nutrition, physical activity, and cancer; and todevelop education programs and interventionsdesigned to improve the dietary and activityhabits of people of all ages.
The ACS also recognizes that manyimportant questions about nutrition, physicalactivity, and cancer risk remain unanswered.The ACS will continue to support an ongoingprogram of research that addresses biological,clinical, epidemiological, behavioral, and policystudies on the role diet and physical activityplay in cancer prevention. Greater efforts onthe part of individuals in public and privateagencies are also needed to translate theseguidelines into effective action that reduces theburden of cancer among Americans.
The ACS continues to support nutritionresearch in two ways: by conducting its ownresearch, and by funding outstanding researchprojects throughout the country. Staff scientistsof the ACS are conducting epidemiologicalresearch in which they analyze and interpretdata related to cancer mortality with regard to lifestyle among a population of more thanone million people. In addition, scientiststhroughout the United States apply forresearch grants for their own investigations.The ACS reviews these applications rigorously,and awards funding to only the mostmeritorious proposals. Studies supported bythe ACS on the role of diet and activity oncancer risk have been made possible by theefforts of nearly 100,000 volunteers and the financial contributions of millions ofAmericans.
To reverse current trends in diet and activityhabits and the resultant increases in overweightand obesity among many segments of thepopulation—including both youth andadults—increased attention and dedicatedresources are needed. Positive action on the part of communities, public and privateorganizations, and individuals working togetherto raise the awareness of this issue and to
116 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention

influence public policy and resource allocationwill be needed. By acting on what is knownnow, and by continuing to pursue acomprehensive research agenda that includespolicy and environmental change strategies, theACS believes it can stimulate effective action to reduce the burden of cancer amongAmericans. CA
Volume 52 • Number 2 • March/April 2002 117
CA Cancer J Clin 2002;52:92-119
REFERENCES
1. Krauss RM, Eckel RH, Howard B, et al.American Heart Association Dietary Guidelines:Revision 2000:A statement for healthcare profes-sionals from the Nutrition Committee of theAmerican Heart Association. Circulation 2000;102:2284-2299.
2. US Department of Health and HumanServices. USDA Dietary Guidelines forAmericans, 5th ed., 2000. Home and GardenBulletin No. 232:239.
3. McGinnis JM, Foege WH. Actual causes ofdeath in the United States. JAMA 1993;270:2207-2212.
4. World Cancer Research Fund in associationwith American Institute for Cancer Research.Food, Nutrition and the Prevention of Cancer:AGlobal Perspective. World Cancer ResearchFund,Washington DC, 1997.
5. Freidenreich, CM. Physical activity and cancerprevention: From observational to interventionresearch. Cancer Epidemiol Biomarkers Prev2001;10:287-301.
6. US Department of Health and HumanServices, Centers for Disease Control andPrevention, National Center for Chronic DiseasePrevention and Health Promotion, Office onSmoking and Health. Reducing Tobacco Use: AReport of the Surgeon General, 2000.
7.The Work Study Group on Diet,Nutrition, andCancer: ACS Guidelines on Diet, Nutrition, andCancer. Cancer 1991;41:334-338.
8. Willett WC. Micronutrients and cancer risk.Am J Clin Nutr 1994;59:1162-1165.
9. Steinmetz KA, Potter JD.Vegetables, fruit, andcancer. I. Epidemiology. Cancer Causes Control1991;2:325-357.
10. Steinmetz KA, Potter JD.Vegetables, fruit, andcancer. II. Mechanisms. Cancer Causes Control1991;2:427-442.
11. Ames BN, Gold LS, Willett WC. The causesand prevention of cancer. Proc Natl Acad Sci U SA 1995;2:5258-5265.
12. Giovannucci E. Tomatoes, tomato-basedproducts, lycopene and cancer: Review of the
epidemiologic literature. J Natl Cancer Inst1999;91:317-331.
13. Biesalski HK, de Mesquita BB, Chesson A, etal. European consensus statement on lung cancer:Risk factors and prevention. Cancer 1998;48:167-176.
14.The Alpha-Tocopherol, Beta Carotene CancerPrevention Study Group.The effect of vitamin Eand beta carotene on the incidence of lung can-cer and other cancers in male smokers. N Engl JMed 1994;330:1029-1035.
15. Omenn G, Goodman G,Thornquist M, et al.Effects of a combination of beta carotene andvitamin A on lung cancer and cardiovascular disease. N Engl J Med 1996;334:1150-1155.
16. Henneken SC, Buring J, Manson J, et al. Lackof effect of long term supplementation with beta-carotene on the incidence of malignant neo-plasms and cardiovascular disease. N Engl J Med1996;334:1145-1149.
17. Trichopoulos D, Willett WC. Introduction:Nutrition and cancer. Cancer Causes Control1996;7:3-4.
18. Life Sciences Research Office, Federation ofAmerican Societies for Experimental Biology.Third Report on Nutrition Monitoring in theUnited States.Washington, DC: US GovernmentPrinting Office, 1995.
19. Havas S, Heimendinger J, Damron D, et al.5 A Day for better health: Nine communityresearch projects to increase fruit and vegetableconsumption. Public Health Rep 1995;110:68-79.
20. Potter JD, Finnegan JR, Guinard J-X, et al.5 A Day for Better Health Program EvaluationReport. Bethesda, MD: National Institutes ofHealth, National Cancer Institute. November2000; NIH Publication No. 01-4904.
21. Slavin JL. Mechanisms for the impact ofwhole grain foods on cancer risk. J Am Coll Nutr2000;19:3002-3075.
22. Schatzkin A, Lanza E, Corle D, et al. Lack ofeffect of a low-fat, high-fiber diet on the recur-rence of colorectal adenomas. Polyp PreventionTrial Study Group. N Engl J Med 2000;342:1149-1155.
23.Alberts DS, Martinez, ME, Roe DJ, et al. Lackof effect of a high-fiber cereal supplement on therecurrence of colorectal adenomas. PhoenixColon Cancer Prevention Physicians’ Network.N Engl J Med 2000;342:1156-1162.
24. Messina M, Erdman JW, eds. Modern applica-tions for an ancient bean: Soybeans and the pre-vention and treatment of chronic disease. J Nutr1995;125:567-569.
25. Glade MJ. Dietary fat and cancer: Genetic andmolecular interaction. Annual ResearchConference, American Institute for CancerResearch. Nutrition 1997;13:75-77.
26. Gerrior S, Bente L. Nutrient content of theUS Food Supply, 1909-1994. US Department ofAgriculture, Center for Nutrition Policy andPromotion. Home Economics Research ReportNo. 53, 1997.
27. Kushi LH, Lenart EB, Willett WC. Healthimplications of Mediterranean diets in light ofcontemporary knowledge. 2. Meat, wine, fats, andoil.Am J Clin Nutr 1995;61:1465-1427.
28. Potter JD. Nutrition and colorectal cancer.Cancer Causes Control 1996;7:127-146.
29. Kolonel LN. Nutrition and prostate cancer.Cancer Causes Control 1996;7:83-94.
30. Hill HA,Austin H. Nutrition and endometri-al cancer. Cancer Causes Control 1996;7:19-32.
31. Enns CW, Goldman JD, Cook A. Trends infood and nutrient intakes by adults: NFCS 1977-1978, CSFII 1989-1991, and CSFII 1994-1995.Family Economics and Nutrition Review1997;10:2-15.
32. Flegal KM, Carroll MD, Kuczmarski RJ, et al.Overweight and obesity trends in the UnitedStates: Prevalence and trends, 1960-1994. Int JObes Relat Metab Disord 1998;22:39-47.
33. Slattery ML, Edwards SL, Ma KN, et al.Physical activity and colon cancer: A publichealth perspective. Ann Epidemiol 1997;7:137-145.
34. McTiernan A. Associations between energybalance and body mass index and risk of breastcarcinoma in women from diverse racial and eth-nic backgrounds in the US. Cancer 2000;88:1248-1255.

118 CA A Cancer Journal for Clinicians
ACS Guidelines on Nutrition and Physical Activity for Cancer Prevention
35. Health Implications of Obesity. NationalInstitutes of Health Consensus Statement 1985Feb 11-13;5:1-7.
36. McTiernan A, Ulrich C, Slate S, et al. Physicalactivity and cancer etiology: Associations andmechanisms. Cancer Causes Control 1998;9:487-509.
37. Wideroff L, Gridley G, Mellenkjaer L, et al.Cancer incidence in a population-based cohortof patients hospitalized with diabetes mellitus inDenmark. J Natl Cancer Inst 1997;89:1360-1365.
38. Lindblad P, Chow WH, Chan J, et al.The roleof diabetes mellitus in the aetiology of renal cellcancer. Diabetologia 1999;42:107-112.
39. Calle EE, Murphy TK, Rodriquez C, et al.Diabetes mellitus and pancreatic cancer mortalityin a prospective cohort of United States adults.Cancer Causes Control 1998;9:403-410.
40. Will JC, Galuska DA, Vinicor F, et al.Colorectal cancer: Another complication of dia-betes mellitus? Am J Epidemiol 1998;147:816-825.
41. Wolk A, Lindblad P, Adami H-O. Nutritionand renal cell cancer. Cancer Causes Control1996;7:5-18.
42. Martinez ME, Giovannucci E, Speigelman D,et al. Leisure-time physical activity, body size, andcolon cancer in women. Nurses’ Health StudyResearch Group. J Natl Cancer Inst 1997;89:948-955.
43. Slattery ML, Potter B, Caan et al. Energy bal-ance and colon cancer—beyond physical activity.Cancer Res 1997;57:75-80.
44. Carpenter CL, Ross RK, Paganini-Hill A, etal. Lifetime exercise activity and breast cancer riskamong post menopausal women. Br J Cancer1999;80:1852-1858.
45.Verloop J, Rookus MA, van der Kooy K, et al.Physical activity and breast cancer risk in womenaged 20-54 years. J Natl Cancer Inst 2000;92:128-135.
46. Freidenreich CM, Rohan TE. Physicial activ-ity and risk of breast cancer. Eur J of Cancer Prev1995;4:145-151.
47. International Agency for Research onCancer, World Health Organization. CancerPrevention Series. Physical Activity Body Weight,and Cancer. 2001. Lyon, France. In Press.
48. Hootman JM, Macera CA, Ainsworth BA, etal. Association among physical activity level, car-diorespiratory fitness and risk of musculoskeletalinjury.Am J Epidemiol 2001;154:251-258.
49. Blair SN, Kohl HW, Gordon NF, et al. Howmuch physical activity is good for health? AnnuRev Public Health 1992;13:99-126.
50. Shephard RJ, Futcher R. Physical activity andcancer: How may protection be maximized? Crit
Rev Oncog 1997;8:219-272.
51. Davey Smith G, Shipley MJ, Batty GD, et al.Physical activity and cause-specific mortality inthe Whitehall study. Public Health 2000;114:308-315.
52. US Department of Health and HumanServices, Centers for Disease Control andPrevention, National Center for Chronic DiseasePrevention and Health Promotion, ThePresident’s Council on Physical Fitness andSports, Surgeon General’s Report on PhysicalActivity and Health:243-250.
53. Pangrazi PP. Promoting physical activity foryouth. J Sci Med Sport 2000;3:280-286.
53a. Corbin CB and Pangrazi PP. Physical activi-ty for children:A statement of guidelines. Reston,VA, National Association for Sport and PhysicalEducation, 1998.
54. Curl, WW. Aging and exercise: Are they compatible in women? Clin Orthop 2000;372:151-158.
55. van den Brandt PA, Spiegelman D,Yaun, SS, etal. Pooled analysis of prospective cohort studieson height, weight, and breast cancer risk. Am JEpidemiol 2000;152:514-527.
56. Calle EE,Thun MJ, Petrelli JM, et al. Body-mass index and mortality in a prospective cohortof US adults. N Engl J Med 1999;341:1097-1105.
57. Freidenreich CM. Review of anthropometricfactors and breast cancer risk. Eur J Cancer Prev2001;10:15-32.
58. Chow WH, Gridley G, Fraumeni JF, et al.Obesity, hypertension and the risk of kidney can-cer in men. N Engl J Med 2000;343:1305-1311.
59. Michaud DS, Giovannucci E,Willett WC, etal. Physical activity, obesity, height, and the risk ofpancreatic cancer. JAMA 2001;286:921-929.
60. Cleary MP, Maihle NJ.The role of body massindex in the relative risk of developing pre-menopausal versus postmenopausal breast cancer.Proc Soc Exp Biol Med 1997;6:28-43.
61. Kuczmarski RJ, Flegal KM. Criteria for defi-nition of overweight in transition: Backgroundand recommendations for the United States. AmJ Clin Nutr. 2000;7:1074-1081.
62. World Health Organization, InternationalAgency for Research on Cancer. IARCMonographs on the Evaluation of CarcinogenicRisks to Humans: Alcohol Drinking. Vol 44.Lyon, France: IARC, 1988.
63. Report on Carcinogens, Ninth Edition; USDepartment of Health and Human Services,Public Health Service, National ToxicologyProgram; May, 2000.
64. Smith-Warner SA, Speigelman D, Yaun SS,et al. Alcohol and breast cancer in women:A pooled analysis of cohort studies. JAMA. 1998;
27:535-540.
65.Ashley MJ, Ferrence R, eds. Moderate drink-ing and health:The scientific evidence. ContempDrug Probl 1994;21:1-204.
66. Criqui MH. Alcohol consumption and car-diovascular disease. In: R Paoletti, AL Klatsky, APoli, S Zakhari, eds. Moderate AlcoholConsumption and Cardiovascular Disease.Dordrecht, NL: Kluwer Academic Publishers;2000:23-36.
67. Michaud DS, Spiegelman D, Clinton SK, et al.Fluid intake and the risk of bladder cancer inmen. N Engl J Med 1999;340:1390-1397.
68. Marshall JR, Boyle P. Nutrition and oral can-cer. Cancer Causes Control 1996;7:101-112.
69. Cheng KK, Day NE. Nutrition andesophageal cancer. Cancer Causes Control 1996;7:33-40.
70. Riboli E, Kaaks R, Esteve J. Nutrition andlaryngeal cancer. Cancer Causes Control 1996;7:147-156.
71. Kolonel LN. Nutrition and Prostate Cancer.In: Coulston AM, Rock CL, and Monsen ER.Nutrition in the Prevention and Treatment ofDisease. San Diego, CA:Academic Press;2001:373-386.
72. Giovannucci E, Rimm EB, Wolk A, et al.Calcium and fructose intake in relation to risk ofprostate cancer. Cancer Res 1998;58:442-447.
73. Kono S, Hirohata T. Nutrition and stomachcancer. Cancer Causes Control 1996;7:41-55.
74. Martinez ME,Willett WC. Calcium, vitaminD, and colorectal cancer: A review of the epi-demiological evidence. Cancer EpidemiolBiomarkers Prev 1998;7:163-168.
75. Honein, MA, Paulozzi LJ, Mathews TJ, et al.Impact of folic acid fortification of the US foodsupply on occurrence of neural tube defects.JAMA 2001;285:2981-2986.
76. Joossens JV, Hill MJ, Elliott P, et al. Dietarysalt, nitrate and stomach cancer mortality in 24countries. European Cancer Prevention (ECP)and the INTERSALT Cooperative ResearchGroup. Int J Epidemiol 1996;25:494-504.
77. Trichopoulou A, Katsouyanni K, Stuver S, etal. Consumption of olive oil and specific foodgroups in relation to breast cancer risk in Greece.J Natl Cancer Inst 1995;87:110-116.
78. National Research Council. Carcinogens andAnticarcinogens in the Human Diet.Washington,DC: National Academy Press, 1996.
79. Clark LC, Combs GF Jr,Turnbull BW, et al.Effects of selenium supplementation for cancerprevention in patients with carcinoma of theskin. A randomized controlled trial. NutritionalPrevention of Cancer Study Group. JAMA 1996;276:1957-1963.

80. Petrakis NL, Barnes S, King EB, et al. Stimulatory influenceof soy protein isolates on breast secretion in pre-and post-menopausal women. Cancer Epidemiol Biomarkers Prev1996;5:785-794.
81. Blot W, Li J, Taylor P, et al. Nutrition intervention trials inLinxian, China; supplementation with specific vitamin/mineralcombinations, cancer incidence and disease-specific mortality inthe general population. J Natl Cancer Inst 1993;85:1483-1492.
82. Katiyar SK, Mukhtar H.Tea in chemoprevention of cancer:Epidemiologic and experimental studies. Intl J Oncology1996;8:221-238.
83. Hu FB, Stampfer MJ, Manson JE, et al. Dietary fat intake andthe risk of coronary heart disease in women. N Engl J Med1997;337:1491-1499.
84. Willett WC. Specific Fatty acids and risks of breast andprostate cancer: Dietary intake. Am J Clin Nutr 1997;66:1557-1563.
85. Block G.Vitamin C and cancer prevention: The epidemio-logic evidence.Am J Clin Nutr 1991;53:270-282.
86. Byers T, Perry G. Dietary carotenes, vitamin C and vitamin Eas protective antioxidants in human cancers. Annu Rev Nutr1992;12:139-159.
Volume 52 • Number 2 • March/April 2002 119
CA Cancer J Clin 2002;52:92-119