alveolar bone necrosis and spontaneous tooth exfoliation ... · alveolar bone necrosis and...
TRANSCRIPT

177
Alveolar bone necrosis and spontaneous tooth exfoliation associated with trigeminal herpes zoster: a report of three cases
Nam-Kyoo Kim1, Bong Chul Kim2, Jung-woo Nam1, Hyung Jun Kim1
1Department of Oral and Maxillofacial Surgery, College of Dentistry, Yonsei University, Seoul, 2Department of Oral and Maxillofacial Surgery, Daejeon Dental Hospital, College of Dentistry, Wonkwang University, Daejeon, Korea
Abstract (J Korean Assoc Oral Maxillofac Surg 2012;38:177-83)
Herpes zoster is a viral infection caused by the reactivation of the varicella zoster virus, an infection most commonly affecting the thoracolumbar trunk. Herpes Zoster Infection (HZI) may affect the cranial nerves, most frequently the trigeminal. HZI of the trigeminal nerve distribution network manifests as multiple, painful vesicular eruptions of the skin and mucosa which are innervated by the infected nerves. Oral vesicles usually appear after the skin manifestations. The vesicles rupture and coalesce, leaving mucosal erosions without subsequent scarring in most cases. The worst complication of HZI is post-herpetic neuralgia; other complications include facial scarring, motor nerve palsy and optic neuropathy. Osteonecrosis with spontaneous exfoliation of the teeth is an uncommon complication associated with HZI of the trigeminal nerve. We report several cases of osteomyelitis appearing on the mandible, caused by HZI, and triggering osteonecrosis or spontaneous tooth exfoliation.
Key words: Human herpesvirus 3, Herpes zoster, Osteonecrosis, Tooth exfoliation[paper submitted 2011. 8. 30 / revised 1st 2011. 10. 13, 2nd 2012. 1. 9 / accepted 2012. 1. 11]
festationcanbeobservedwhenthemaxillaryandmandibular
branchesareaffected4.
Oralvesiclesappearmainlyafteraskinmanifestation3,5.
Sometimes,however, theremaybemucosal involvement
withoutskinlesion5.Thevesicleseruptandleavemucosal
erosionsbutnoscar inmostcases3.Themostsignificant
complicationofHZI is post-herpetic neuralgia5; other
complicationsmayincludefacialscarring,motornervepalsy,
opticneuropathy,blindness,encephalitis,andcalcinosiscutis6.
ThebonychangeinassociationwithHZIwasfirstreported
byRose in19087.AccordingtoDechaumeetal. (1955)8,
Gonnet’spresentationin1922wasthefirstreporttoestablish
interestinosteonecrosisandtoothexfoliationassociatedwith
HZI2.Complicationsuchasosteonecrosiswithspontaneous
toothexfoliationisveryrare.Thus,wereportsomecasesof
osteomyelitis inthemandiblecausedbyHZIaffectingthe
trigeminalnerve.
II. Cases Report
1. Case 1
A78-year-oldmalepatientvisitedourhospitalonFebruary
12,2010withchiefcomplaintofosteonecrosisofmandible
I. Introduction
Thevaricellazostervirus(VZV)produces twoclinical
results:varicellaorchickenpoxandherpeszosterinfection
(HZI)1.VaricellacausedbytheprimaryinfectionofVZVis
abenignchildhooddiseaseproducingeruptivevesicles.Asa
resultofprimaryinfectioninthevaricella,askinvirusmoves
toasensorynerveandremainsinlatentstateinaganglion1,2.
WhenVZVinlatentstateisreactivated,itdevelopsintoHZI,
whichcausesseverepainandpainfulvesiclesintheskinand
mucosaaroundtheaffectedsensorynervedistribution3,4.
Thoracolumbardermatomes(T3-L3)aremostcommonly
affectedbyHZI1,4.HZImayalsoaffectthecranialnerves,
with the trigeminalnervemostfrequentlyaffected(18.5-
22%)1.Herpes zoster affecting the trigeminal nerve is
generallyunilateral; itaffectsasinglebranchamongthree
branches,mainlythefirstbranchoropticnerve.Oralmani-
Hyung Jun KimDepartment of Oral and Maxillofacial Surgery, College of Dentistry, Yonsei University, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, KoreaTEL: +82-2-2228-3132 FAX: +82-2-2227-8022E-mail: [email protected]
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
CC
CASE REPORThttp://dx.doi.org/10.5125/jkaoms.2012.38.3.177
pISSN 2234-7550·eISSN 2234-5930
J Korean Assoc Oral Maxillofac Surg 2012;38:177-83
178
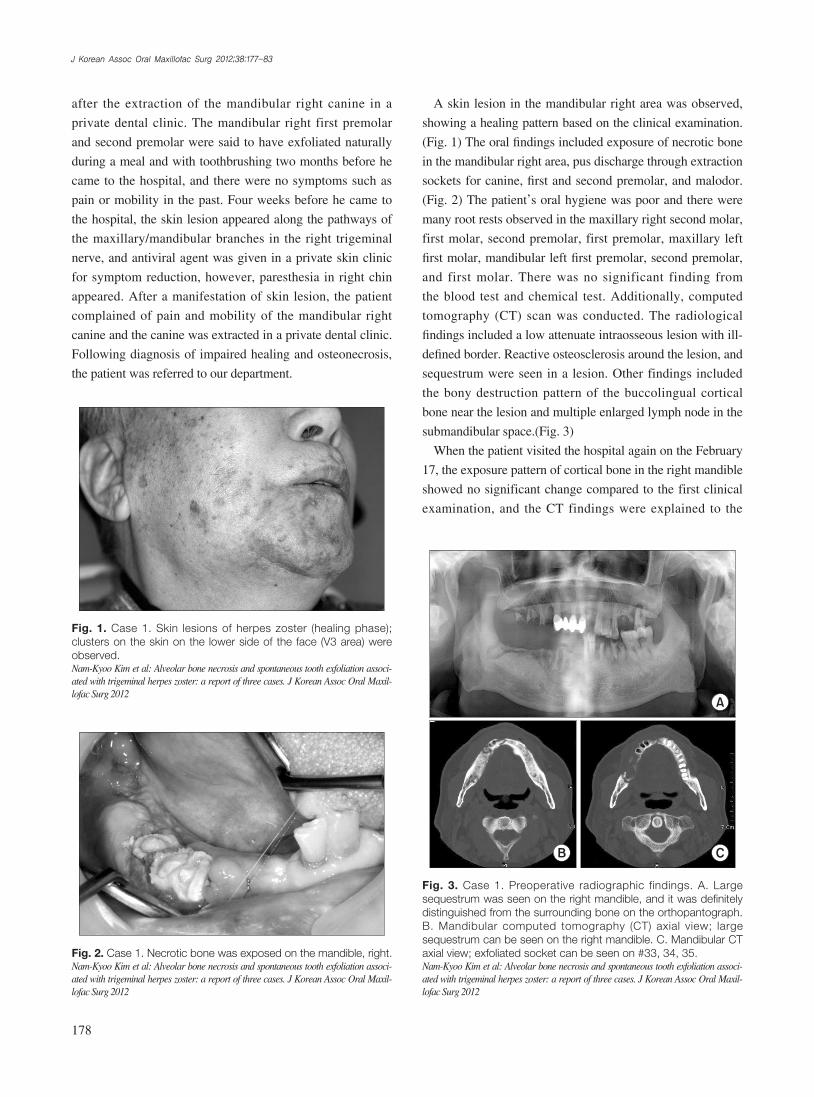
Askinlesioninthemandibularrightareawasobserved,
showingahealingpatternbasedontheclinicalexamination.
(Fig.1)Theoralfindingsincludedexposureofnecroticbone
inthemandibularrightarea,pusdischargethroughextraction
socketsforcanine,firstandsecondpremolar,andmalodor.
(Fig.2)Thepatient’soralhygienewaspoorandtherewere
manyrootrestsobservedinthemaxillaryrightsecondmolar,
firstmolar,secondpremolar,firstpremolar,maxillaryleft
firstmolar,mandibularleftfirstpremolar,secondpremolar,
and firstmolar.Therewasno significant finding from
theblood testandchemical test.Additionally,computed
tomography (CT)scanwasconducted.The radiological
findingsincludedalowattenuateintraosseouslesionwithill-
definedborder.Reactiveosteosclerosisaroundthelesion,and
sequestrumwereseeninalesion.Otherfindingsincluded
thebonydestructionpatternof thebuccolingualcortical
bonenearthelesionandmultipleenlargedlymphnodeinthe
submandibularspace.(Fig.3)
WhenthepatientvisitedthehospitalagainontheFebruary
17,theexposurepatternofcorticalboneintherightmandible
showednosignificantchangecomparedtothefirstclinical
examination,and theCTfindingswereexplained to the
after theextractionof themandibular right canine ina
privatedentalclinic.Themandibular right firstpremolar
andsecondpremolarweresaidtohaveexfoliatednaturally
duringamealandwithtoothbrushingtwomonthsbeforehe
cametothehospital,andtherewerenosymptomssuchas
painormobilityinthepast.Fourweeksbeforehecameto
thehospital,theskinlesionappearedalongthepathwaysof
themaxillary/mandibularbranches in theright trigeminal
nerve,andantiviralagentwasgiveninaprivateskinclinic
forsymptomreduction,however,paresthesiainrightchin
appeared.Afteramanifestationofskinlesion, thepatient
complainedofpainandmobilityof themandibular right
canineandthecaninewasextractedinaprivatedentalclinic.
Followingdiagnosisofimpairedhealingandosteonecrosis,
thepatientwasreferredtoourdepartment.
Fig. 1. Case 1. Skin lesions of herpes zoster (healing phase); clusters on the skin on the lower side of the face (V3 area) were observed. Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 2. Case 1. Necrotic bone was exposed on the mandible, right. Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 3. Case 1. Preoperative radiographic findings. A. Large sequestrum was seen on the right mandible, and it was definitely distinguished from the surrounding bone on the orthopantograph. B. Mandibular computed tomography (CT) axial view; large sequestrum can be seen on the right mandible. C. Mandibular CT axial view; exfoliated socket can be seen on #33, 34, 35. Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012

Alveolar bone necrosis and spontaneous tooth exfoliation associated with trigeminal herpes zoster: a report of three cases
179
gingivaandexposureofcorticalbonebeneath thegum.
Hehadusedmaxillarycompletedentureandmandibular
removablepartialdentureforseveralyears.
Theclinicalexaminationrevealedfindingsoferythematous
edemain therightchinandulcerandpost-inflammatory
hyperpigmentationintherightchinandpreauriculararea.
(Fig.5)Theoral findings included theextractionsocket
(consideredtohavebeendroppedrecently)ofthemandibular
rightcanine, firstandsecondpremolarusedasabutment
oftheremovablepartialdentures,exposureofneighboring
necroticbones,andinflammationofneighboringgingiva.
(Fig.6)Thepatientdidnot remember theexact timeof
patient andhis caregiver.We temporarilydiagnosed it
asmandibularosteomyelitiscausedbyHZI,hospitalized
thepatienton the18thof thesamemonthandyear,and
plannedantibiotherapy,consultationwithdermatologist,and
sequestrectomy.
Thedermatologistdecidednottorequireadditionalantiviral
treatmentbecause theskin lesionhadalreadyenteredthe
healingstage,and just recommend theadministrationof
non-steroidalanti-inflammatorydrug (NSAID)andpre-
gabalintoproviderelieffrompost-herpeticneuralgia.With
antibiotherapy,squestrectomyandextractionofrootrests
wereperformedunderlocalanesthesiaonFebruary,26.The
bonydefectsweredressedwithVaselinegauze,whichwas
replacedonadailybasis.Thepostoperativeradiological
findingsshowednormalhealingpatternoftheareawherethe
bonewasremoved.(Fig.4)Thelesionwasoverlappedwith
softtissueingoodconditionninedaysaftertheoperation,
andthepatientdischargedthehospitalonthe16thdayafter
theoperation.Asaresultofmonitoringuntileightmonths
afterthesurgery,thepatientdidnotcomplainofpost-herpatic
neuralgia,andtherewerenofindingsofrecurrence.
2. Case 2
A77-year-oldmalepatientwasreferredtoourhospital
withchiefcomplaintofsoregingivaandmandibularpainon
December17,2010.Amonthbeforevisitingourhospital,
thepatientcomplainedofpainintherighteararea,vesicles
andswellingswithpainalongthepathwayofthetrigeminal
mandibularbranchontherightsideoftheface,andconsulted
anotolaryngologist,takingantiviralagentmedication.Two
weeksbeforehevisitedourhospital,hefeltpainfromsore
Fig. 4. Case 1. Post-operative radiographic findings post-operative day 8; the necrotic bone and multiple hopeless teeth were removed, and normal healing was noted.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 5. Case 2. Skin lesions of herpes zoster; erythematous swelling and ulcer with post-inflammatory hyperpigmentation. A. Skin lesion can be seen on the chin, right. B. Skin lesion can be seen on the preauricular area, right.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 6. Case 2. Necrotic bone was exposed, spontaneous teeth exfoliation on #43, 44, 45.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012

J Korean Assoc Oral Maxillofac Surg 2012;38:177-83
180
med;sincepost-herpaticneuralgiapersisted,gabapentin600
mg,tramadol37.5mg,acetaminophen325mg,andamino-
triptyline10mgwereadministeredtothepatient.
OnJune8,2011,aftercontinuousfollow-upforsixmonths,
post-herpaticneuralgiasubsided,andsequestrumformed
andnaturallyexfoliated.Biopsyoftheexfoliatedsequestrum
wasperformed,withtheresultreportedasnecroticbone.On
June29,theareawasoverlappedwithsofttissuearoundthe
lesion,healingwell.(Fig.8)
3. Case 3
OnJuly22,2010,a74-year-oldmalepatientvisitedour
hospitalwithchiefcomplaintofswellingoftheleftsideof
thefaceandpain.Hecomplainedofpainintheupperanterior
teeth for threedaysbeforehevisitedourhospital, and
vesiclesandedemawereformedalongthepathwayofthe
lefttrigeminalmaxillarybranchtwodaysbeforehevisited
ourhospital.OnJuly22,hewenttoaprivatedentalclinic;he
wasthenreferredtoourhospital.Hetookprescriptionpills
forhighbloodpressure,whichwasrelativelywell-regulated.
Heworemaxillaryandmandibularpartialdenturesforfive
years.Theclinicalexaminationshowedthattheleftsideof
thefacehaddiffuseerythematousplaquesandvesicleswith
tenderness.(Fig.9.A); theoralfindingsincludedmultiple
mucosalvesiclesandulcer formationon the leftpalate
togetherwithmobilityoftheremainingteethandalveolar
boneresorptioninedentulousstateexceptthemaxillaryright
andleftcentral incisor, lateral incisor,andcanine.(Fig.9.
B)HZIwasconsideredtobeinactivephase,consultation
wereadministeredwithadermatologistandaperiodontistto
preventosteonecrosisandlossofremainingteeth.Afterthe
toothexfoliation,butitwasestimatedtobeaboutoneweek
earlieraccording to theopinionsofhiscaregiverand the
peoplearoundhim.Assumingmandibularosteomyelitis
in associationwithHZI, antibioticswereprescribed to
preventsecondaryinfection,andCTscanwasconducted.
Consultationwiththedermatologistandotolaryngologistwas
administeredfortheskinlesionandotalgia.Theradiological
findingshoweda lowattenuate intraosseous lesionwith
relatively ill-definedborderin themandibular rightarea
butnodestructionofcorticalboneorsequestrum.Someof
theenlargedlymphnodein thesubmandibularspacewas
observed.(Fig.7)Dermatologically,sinceonemonthhad
passedafterHZI,antiviraltreatmentwasnotrequired.For
post-herpaticneuralgia,pregabalinandacetaminophenwere
administered.
Whenhevisitedthehospitalagain,theexposurepatternof
therightmandibularcorticalbonehadnosignificantchange
comparedtothefirstclinicalexamination.Sincetherewas
neithersequestrumnoracute inflammation,weonlyuse
antibioticsandantimicrobials (ChlorhexidineGluconate
Solution)forpreventsecondaryinfection.Surgicalsques-
trectomywasplannedincaseofsequestrumdevelopsinthe
future.Continuousfollow-upanddisinfectionwereperfor-
Fig. 7. Case 2. Radiographic findings; diffuse radiolucent lesion and extraction sockets area seen on the mandible, right. A. Orthopantograph. B. Mandibular computed tomography (CT) view: coronal. C. Mandibular CT view: axial.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 8. Case 2. Soft tissue covering previous lesion.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012

Alveolar bone necrosis and spontaneous tooth exfoliation associated with trigeminal herpes zoster: a report of three cases
181
riskelementsmayincludeexternaldamageoftheaffected
dermatomes,psychologicalstress,andrace9.
The thoracicdermatome ismost commonlyaffected,
accountingfor50%of the totalcases9.Thecranialnerve
mayalsobeaffected,withthetrigeminalnervemostcom-
monlyaffected(18.5-22%of the totalcases)followedby
glossopharyngealnerveandhypoglossalnerve.Incaseof
trigeminalnerveinvolvement, it isunilaterallylimitedtoa
singlebranch,mainlyaffectingtheopticnerve2.
Oralsymptomisobservedwhenthetrigeminalmaxillary
andmandibularbranchesareaffectedandskin lesion is
mainlypreceded,butacasestartingwithparesthesiaof
mentalnervewasalsoreported11.Theerythematousvesicle
isdevelopedintheoralcavity;itruptures,formsanulcer,
andgetscoveredbywhitepseudomembrane2,5,11.Lympha-
denopathymay appear in the submandibular area5. In
addition,patientsmaycomplainofsymptomsimilartoacute
pulpitsoftheaffectedtoothandtoothache12;rootresorption
andperiapical lesionmayalsooccur13.Sincehistological
findings that are not significantly different from the
osteomyelitispatternshownecroticboneandinflammatory
cellinfiltration,thediagnosisoftherelationshipwithherpes
zostercanhardlybeconfirmedonlybysuchhistological
findings;thediagnosisshouldtakeintoaccounttheclinical
findings3,4,14.Amongthefindings,osteonecrosisofthejaw
andnaturaltoothexfoliationareveryrarecomplications4,5,15.
Jainetal.4conductedareviewofliteratureon41casesof
osteonecrosisofthejawcausedbyHZI.Theonsetagerange
wasfrom6to85,with8casesofpatientsundertheageof40,
treatmentbyadermatologist,antiviralagent(famciclovir750
mg),tramadol37.5mg,acetaminophen325mg,levocetirizine
HCl5mg,andmupirocin0.2%ointmentwereprescribed;
forperiodontal treatment, scalingandmonitoringwere
performed.OnJuly29,theskinlesionshowednormalhealing
patternbytheformationofcrust(Fig.10.A);theoralvesicles
alsohealednormallywithnosignificantscar.(Fig.10.B)On
August26ofthesameyear,monitoringrevealednomajor
abnormalityexceptmoderatemobilityof the remaining
maxillaryteeth,andthatpost-herpaticneuralgiasubsided.
III. Discussion
TheprevalencerateofHZIinallagesisreportedtobe
1.2-4.8per1,000peopleeveryyear,with7.2-11.8people
over theageof609.Theprevalencerateandseriousness
increasewithage.40-50%ofthepatientswithHZIareover
theageof60everyyear,with50%ofpersonsover85years
oldrecordingprevalencerateofat leastonce10.Asto the
reasonforsuchprevalencerateincrease,naturalimmunity
declineaccordingtoage increasemaybeconsidered; the
declineinVZV-specificcellularimmunityaccordingtoage
increaseissupported1,10.Theprevalenceratealsoincreases
among immunocompromisedpatients such as patients
infectedwithhumanimmunodeficiencyvirus,hematologic
malignantdisease,andimmune-mediateddisorderandorgan
transplantpatients,andtheriskofHZIforsuchimmune-
suppressedpatientsalsoincreasesaccordingtoage1,9,10.Other
Fig. 9. Case 3. Lesions of herpes zoster (active phase). A. Extraoral view; diffuse erythematous plaques and vesicles were seen on the upper side of the face (V2 area) with tenderness. B. Intraoral view; multiple mucosal vesicles and ulcer formation observed on the maxilla, left.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012
Fig. 10. Case 3. Lesions of herpes zoster (healing phase). A. Extraoral view; clusters on the skin on the upper side of the face (V2 area) were seen. B. Intraoral view; normal healing state on mucosal lesion. No visible scar formation.Nam-Kyoo Kim et al: Alveolar bone necrosis and spontaneous tooth exfoliation associ-ated with trigeminal herpes zoster: a report of three cases. J Korean Assoc Oral Maxil-lofac Surg 2012

J Korean Assoc Oral Maxillofac Surg 2012;38:177-83
182
the intervalcloselyassociatedwith themanifestationof
herpeszosteraffectingthetrigeminalnerveandtheprogress
ofosteonecrosisandosteomyelitisaccompaniedby tooth
exfoliationintherelatedquadrantonly,weconfirmedthe
diagnosisofosteonecrosisofthejawtobeassociatedwith
HZI.SincethepatientinCase2hadonlymandibularright
firstandsecondpremolarsandcanineastheremainingteeth,
andtherewasnotopicalfactorintheotherquadrants,itmay
bemoredifficulttodistinguishfromgeneralosteomyelitis.
Nevertheless,consideringtheclinicalhistoryandpatterns,
wecannotruleouttherelationshipwithherpeszoster.
Thepathophysiologicalmechanismofosteomyelitisof
thejawcausedbytrigeminalherpeszosteriscontroversial,
and several hypotheses areunderdiscussion.The first
hypothesis is that localvasculitis causedby thedirect
extensionofneural inflammatoryresponsetotheadjacent
bloodvessels.Thiseventuallymaycauseaninfarctionof
thetrigeminalvesselsthataccompanythetrigemicalnerves
supplyingthe jawsandcausebonenecrosisbytriggering
ischemia16.Thesecondhypothesis is that thegeneralized
infectionof terminalnervessupplyingtheperiosteumand
periodontiumisbelievedtocausevasculitisoftheperiosteum
andperiodontiumand avascular necrosis over a large
area5,15,17.AccordingtoGildenetal.18,sinceVZVcanalsobe
invaginatedtothevascularendothelialcellintheperipheral
nervoussysteminsteadofbeinglimitedtothebrainorspinal
cord, itcausessmall ischemiclesion,possiblydeveloping
intonecrosisanddemyelination.Thereportcanserveas
groundsforthetwohypothesesabove18.Thethirdhypothesis
canbeadenervationofbone,butdenervationonlycan
hardlybethoughttocauseseriousbonedamageinashort
time15.Thefourthhypothesisisthatsystemicviralinfection
rendersdamagetoanodontoblastandbringsabout tissue
denaturation,causingpulpalnecrosis.Thefinalhypothesisis
thattheexistingpulpits,periodontitis,orsurgicalprocedure
around theHZI area can cause seriousnecrosisof the
alveolarbone3. IncomparingCase1,Case2,andCase3
above,theregulationofinitialresponseandtopicalfactorsis
meaningfulinpreventingcomplicationssuchasosteomyelitis
andosteonecrosisof the jaw,and the local factorcanbe
consideredacauseofthemechanisminthedevelopmentof
osteomyelitisassociatedwithtrigeminalherpeszoster.
Thecasesaboveandliteraturereviewrevealthat,incaseof
theoutbreakoftrigeminalherpeszoster,thepromptapplication
ofantiviralagents,activeuseofpainkillers,andeffective
regulationof topicalfactorswillbehelpful inpreventing
suchcomplications1,4,9,10.Ifosteomyelitisandosteonecrosis
10casesofthosebetween40and60,and12casesofthose
over60.Theprevalencerateincreasedaccordingtoage,with
nodifferencebygender4,16.Itmainlyappearedunilaterally
inthemaxillaormandibleoftheaffectedskin.13patients
haditinthemaxilla,and18patients,inthemandible.There
were31lostteethinthemaxillaand44teethinthemandible,
makingthemandibleapredilectionsite.Sincetheanterior
teethnumbered64andtheposteriorteethwere61,therewas
nosignificantdifferenceintheanteroposteriorposition.The
exfoliatedteethperpatientwere0-7; infivecases,all the
teethoftheaffectedquadrantwerelost4.
Withregardtothetimeintervalbetweentheoutbreakof
HZIandosteonecrosisaccompaniedby tooth loss,Mintz
andAnavi3presentedin1992areportontheintervalofan
averageof21.2daystogetherwiththeoccurrenceofnatural
toothexfoliationabout2-6weeksafterHZImanifestation
throughareviewof14studies.Severalauthors5,11reported
thatitoccurredbetweentwoweeksafterearlyinfectionwith
complicationofosteonecrosisandtoothexfoliation,butother
authors4reportedthatitoccurredbetween3-12weeksafter
HZImanifestationasa latecomplication.Inthefirstcase
reportedinthispaper,theextractionofthemandibularright
caninewasperformedabout4weeksafterHZImanifestation
eventhoughthemandibularfirstandsecondpremolarswere
ruledoutbecause thosepremolarswere lost fourweeks
beforetheoutbreakofskinlesion.Inthesecondcase,natural
toothexfoliationoccurredaboutthreeweeksafterHZImani-
festation.
Taking intoaccount thecomparisonofgeneralosteo-
myelitis, incaseof findings thatshowamedicalhistory
ofherpeszoster recentlyaffecting the trigeminalnerve
andvesicular lesionin therelatedfacialareawithproper
interval,andthatthelesionislimitedonlytoquadrantofjaw
withtheaffectednervedistributed,itmaybediagnosedas
osteomyelitisofthejawcausedbytrigeminalherpeszoster.
PatientsshowingosteomyelitisofthejawinCase1andCase
2wereold,takingprescriptionpillsforhighbloodpressure
andhavingmedicalhistoryofcoronaryarterybypasssurgery
toavoidanginapectoris andcerebral artery infarction,
respectively.Since theywereoldandweakpatientswith
blooddiseases, itmightbediagnosedasgeneralchronic
pyogenicosteomyelitiscausedbylocaldentalinfection.In
Case1,however,manyremainingteethwereaffectedby
dentalcariesorrootrests;sincetheradiopaquelesionsaround
therootapexweredistributedinthemaxillaandmandible,it
couldbejudgedthattherewaslocaldentalinfectioncausing
chronicosteomyelitis.Takingintoaccountthefindingsof

Alveolar bone necrosis and spontaneous tooth exfoliation associated with trigeminal herpes zoster: a report of three cases
183
maxilla:casereport.JOralMaxillofacSurg1999;57:1249-51.7. RoseF.Postherpeticneuralgia; trophic lesions inhand'sbones
similartorheumatoidarthritis.NouvelleIconogrdelaSalpêtrière,SocNeurol1908;9:64.[French]
8. DechaumeM,DescrozaillesC,GarlopeauF,RobertJ.Localizedmandibularnecrosisduring trigeminalherpes.RevueStomatol1955;56:516-21.[French]
9. SchmaderKE,DworkinRH.Naturalhistoryand treatmentofherpeszoster.JPain2008;9(1Suppl1):S3-9.
10. WeaverBA.Herpeszosteroverview:naturalhistoryandincidence.JAmOsteopathAssoc2009;109(6Suppl2):S2-6.
11. SchwartzO,KvorningSA.Toothexfoliation,osteonecrosisofthejawandneuralgiafollowingherpeszosterofthetrigeminalnerve.IntJOralSurg1982;11:364-71.
12. SigurdssonA,JacowayJR.Herpeszoster infectionpresentingasanacutepulpitis.OralSurgOralMedOralPatholOralRadiolEndod1995;80:92-5.
13. RamchandaniPL,MellorTK.Herpeszosterassociatedwithtoothresorptionandperiapicallesions.BrJOralMaxillofacSurg2007;45:71-3.
14. ArikawaJ,MizushimaJ,HigakiY,HoshinoJ,KawashimaM.Mandibularalveolarbonenecrosisaftertrigeminalherpeszoster.IntJDermatol2004;43:136-7.
15. GartyBZ,DinariG, SarnatH,CohenS,NitzanM.Toothexfoliationandosteonecrosisofthemaxillaaftertrigeminalherpeszoster.JPediatr1985;106:71-3.
16. WrightWE,DavisML,GeffenDB,MartinSE,NelsonMJ,StrausSE.Alveolarbonenecrosisandtooth loss.ararecomplicationassociatedwithherpeszosterinfectionofthefifthcranialnerve.OralSurgOralMedOralPathol1983;56:39-46.
17. HallHD,JacobsJS,O'MalleyJP.Necrosisofmaxillainpatientwithherpeszoster.Reportofacase.OralSurgOralMedOralPathol1974;37:657-62.
18. GildenD,CohrsRJ,MahalingamR,NagelMA.aricellazostervirusvasculopathies:diverseclinicalmanifestations, laboratoryfeatures,pathogenesis,andtreatment.LancetNeurol2009;8:731-40.
ofthejawoccurascomplications,suchcomplicationscanbe
treatedthroughtheproperuseofantibioticstoavoidsecondary
infection,squestrectomy,removalofinflammatorytissue,and
regularfollowup2,4,13-15.Inthesecases,whenosteomyelitisof
thejawandosteonecrosisaccompaniedbytoothexfoliation
asrarecomplicationsaftertheoutbreakoftrigeminalherpes
zosteroccur,activeuseofpainkillers,regulationoftopical
factors,andproperextractionofdeadboneandaffectedteeth
bringaboutgoodresults.
References
1. GershonAA,GershonMD,BreuerJ,LevinMJ,OaklanderAL,GriffithsPD.Advancesintheunderstandingofthepathogenesisandepidemiologyofherpeszoster.JClinVirol2010;48Suppl1:S2-7.
2. MendietaC,MirandaJ,BrunetLI,GargalloJ,BeriniL.Alveolarbonenecrosis and tooth exfoliation followingherpes zosterinfection:areviewoftheliteratureandcasereport.JPeriodontol2005;76:148-53.
3. MintzSM,AnaviY.Maxillaryosteomyelitisandspontaneoustoothexfoliationafterherpeszoster.OralSurgOralMedOralPathol1992;73:664-6.
4. JainMK,ManjunathKS,JagadishSN.Unusualoralcomplicationsofherpeszosterinfection:reportofacaseandreviewofliterature.OralSurgOralMedOralPatholOralRadiolEndod2010;110:e37-41.
5. MutoT,TsuchiyaH,SatoK,KanazawaM.Toothexfoliationandnecrosisof themandible--a rarecomplication followingtrigeminalherpeszoster:reportofacase.JOralMaxillofacSurg1990;48:1000-3.
6. OwotadeFJ,UgbokoVI,KoludeB.Herpeszosterinfectionofthe