altered maternal micronutrients (folic acid, vitamin b 12 ) and omega 3 fatty acids through...
TRANSCRIPT
REVIEW
Altered maternal micronutrients (folic acid, vitamin B12) and omega 3 fattyacids through oxidative stress may reduce neurotrophic factors in pretermpregnancy
MADHAVI DHOBALE & SADHANA JOSHI
Department of Nutritional Medicine, Interactive Research School for Health Affairs, Bharati Vidyapeeth University, Pune 411043,
Maharashtra, India
AbstractPreterm pregnancies account for approximately 10% of the total pregnancies and are associated with low birth weight (LBW)babies. Recent studies have shown that LBW babies are at an increased risk of developing brain disorders such as cognitivedysfunction and psychiatric disorders. Maternal nutrition, particularly, micronutrients involved in one-carbon metabolism (folicacid, vitamin B12, and docosahexaenoic acid (DHA)) have a major role during pregnancy for developing fetus and are importantdeterminants of epigenesis. A series of our studies in pregnancy complications have well established the importance of omega 3fatty acids especially DHA. DHA regulates levels of neurotrophins like brain-derived neurotrophic factor and nerve growth factor,which are required for normal neurological development. We have recently described that in one carbon metabolic pathway,membrane phospholipids are major methyl group acceptors and reduced DHA levels may result in diversion of methyl groupstoward deoxyribonucleic acid (DNA) ultimately resulting in DNA methylation. In this review, we propose that altered maternalmicronutrients (folic acid, vitamin B12), increased homocysteine, and oxidative stress levels that cause epigenetic modificationsmay be one of the mechanisms that contribute to preterm birth and poor fetal outcome, increasing risk for behavioural disorders inchildren.
Keywords: Epigenetics, docosahexaenoic acid, neurotrophins, behavioural disorders, pregnancy complications
Introduction
Pregnancy outcome is known to be influenced by duration of
gestation and rate of fetal growth. Preterm birth complicates
about 5–10% of all births resulting in low birth weight (LBW)
and increased infant morbidity and mortality [1]. LBW is
defined by WHO as birth weight less than 2500 g. The rate of
preterm birth has increased in many locations, predominantly
because of increasing indicated preterm births and preterm
delivery of artificially conceived multiple pregnancies. A
recent report suggests that 30% of total neonatal deaths in
India are due to preterm births [2].
Maternal nutrition
Pregnancy is a period of increased metabolic demands, with
changes in the woman’s physiology and the requirements of a
growing fetus [3]. Maternal nutrition that plays a critical role
in fetal growth is one of the important intrauterine environ-
mental factors that alters the expression of the fetal genome
and may have lifelong consequences. Micronutrients like folic
acid and vitamin B12 have major role in one-carbon
metabolism, since they are required for the transfer of methyl
groups for methylation of deoxyribonucleic acid (DNA),
RNA, proteins, and membrane phospholipids. Alteration in
the levels of these micronutrients can have adverse effects on
the mother, resulting in pregnancy complications and birth
defects [4].
Long-chain polyunsaturated fatty acids (LCPUFA), parti-
cularly docosahexaenoic acid (DHA), are important consti-
tuents of all cell membrane phospholipids and precursors of
eicosanoids and are critical nutritional sources for the
developing fetus. Our earlier studies have shown reduced
DHA levels in women with pregnancy complications like
preeclampsia [5] or in women delivering preterm [6]. Our
studies indicate that increased oxidative stress may be one of
the causative factors for degrading LCPUFA in women
delivering preterm [6,7]. Since DHA accretion to the fetus
takes place mainly in the last trimester of pregnancy, children
born preterm miss out on this opportunity and may have
reduced levels of DHA.
Thus, maternal micronutrients (folic acid, vitamin B12)
and omega 3 fatty acids are important intrauterine environ-
mental factors affecting placental and fetal growth and
development (Figure 1). It has been proposed that environ-
mental factors, particularly maternal undernutrition, act in
early life to programme the risks for adverse health outcomes,
such as cardiovascular disease, obesity, and the metabolic
syndrome in adult life.
(Received 2 February 2011; revised 5 March 2011; accepted 1 April 2011)
Correspondence: Dr. Sadhana Ramchandra Joshi, Interactive Research School for Health Affairs, Bharati Vidyapeeth University, Pune-Satara Road, Pune
411043, India. Tel: 91-20-24366929, 91-20-24366931. Fax: 91-20-24366929. E-mail: [email protected]
The Journal of Maternal-Fetal and Neonatal Medicine, 2012; 25(4): 317–323
� 2012 Informa UK, Ltd.
ISSN 1476-7058 print/ISSN 1476-4954 online
DOI: 10.3109/14767058.2011.579209
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.

Folate. Pregnancy is a period of high folate demand, estimated
to be increased 5- to 10-fold, driven by the critical importance
of folate for DNA synthesis, cellular division and proliferation,
the growth and development of the placenta and fetus, and
uterine enlargement [8]. Folate, a water-soluble vitamin, plays
an essential role as a cofactor in one-carbon metabolism,
during which it promotes the re-methylation of homocysteine
– a cytotoxic sulphur containing amino acid that can induce
the DNA strand breakage, oxidative stress, and apoptosis.
Folate provides the methyl group for the conversion of
methionine to S-adenosylmethionine (SAM), the major
methyl donor for most methyltransferases reactions for the
methylation of lipid (PC-DHA to PE-DHA), DNA, and
proteins (histones).When folate levels are low, SAM is
depleted, resulting in a reduction in the methylation of
DNA and thereby enhancing gene transcription and DNA
strand breakage and can impair DNA repair resulting in
genetic mutations or triggering apoptosis [9]. Low maternal
folate, acting to increase homocysteine levels, may provide a
functional link between many of the identified prenatal risk
factors and the hypothesized mechanisms whereby neurode-
velopmental patterning deviates toward a schizophrenic
potential [10].
Vitamin B12. Vitamin B12, also called cobalamin, is a water-
soluble vitamin with a key role in the normal functioning of
the brain and nervous system. It is normally involved in the
metabolism of every cell of the body, especially affecting DNA
synthesis and regulation, but also fatty acid synthesis and
energy production [11]. Vitamin B12 plays a crucial role in
methionine and homocysteine metabolism in most of the cell
types.
Vitamin B12 deficiency during pregnancy is known to result
in elevated levels of homocysteine in the fetus and increases
the incidence of developmental defects in its nervous system.
Vitamin B12 occurs in extensive amounts in animal-derived
foods and is essential for one-carbon metabolism. Indians
primarily consume a vegetarian diet that is Vitamin B12
deficient, which may lead to hyperhomocysteinemia. Altered
one-carbon metabolism, in addition to increasing the levels of
homocysteine, is known to alter the levels of methylation of
catecholamines, phospholipids, and chromatin (histone and
DNA), leading to epigenetic regulation of vital developmental
genes in schizophrenia [12]. Our earlier studies in animals
have shown that maternal folate levels alter brain DHA
concentrations in the offspring [13].
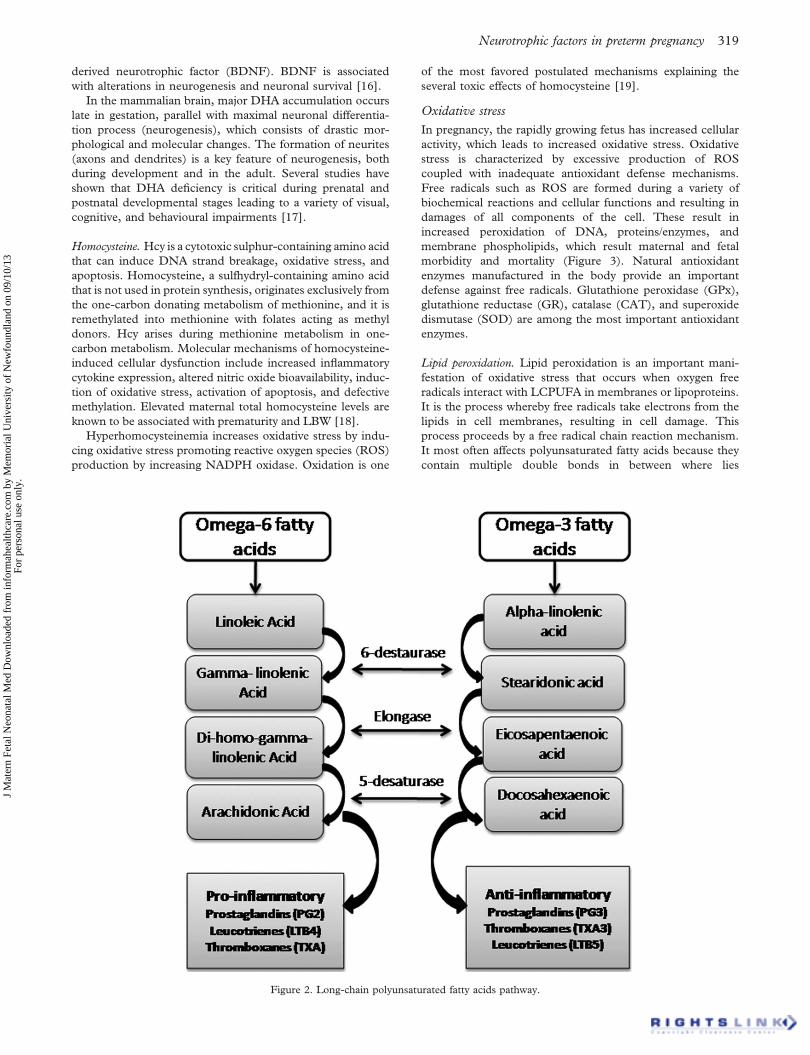
Omega 3-fatty acids. There are two types of PUFAs, n76
and n73 essential fatty acids. Linoleic acid (LA) is the
major n76 fatty acid, and alpha-linolenic acid (ALA) is the
major n73 fatty acid. In the body, LA is metabolized to
arachidonic acid (AA), and ALA is metabolized to
eicosapentaenoic acid (EPA) and DHA by D-5 desaturase
and D-6 desaturase enzymes (Figure 2). Nutritionally,
important essential n73 fatty acids are ALA, EPA, and
DHA. The human body cannot synthesize n73 fatty acids
de novo, but it can synthesize from ALA. These conversions
occur competitively with n76 fatty acids, which are
essential closely related chemical analogues that are derived
from LA. Both the n73 ALA and n76 LA are essential
nutrients that must be obtained from food. Synthesis of the
longer n73 fatty acids from ALA within the body is
competitively slowed by the n76 analogues. Thus, accu-
mulation of long-chain n73 fatty acids in tissues is more
effective when they are obtained directly from food [14].
In olden days, the ratio of n76 to n73 essential fatty acids
was 1 to 2:1. Today, this ratio is about 10 to 20 to 25:1,
indicating that modern day diets are deficient in n73 fatty
acids compared with the diet on which humans evolved and
their genetic patterns were established [14]. The n73 and
n76 fatty acids are not interconvertible in the human body
and are important components of all cell membranes and it
influence eicosanoid metabolism, gene expression, and inter-
cellular cell-to-cell communication.
During early life, there is limited metabolic capability to
convert ALA to DHA. Therefore, the fetus is completely
dependant on maternal source of DHA. Placental uptake of
maternal fatty acids is essential for growth and development of
the feto-placental unit. DHA and AA are critical nutritional
source for the developing fetus and infant. Throughout the
fetal life, placenta selectively and subsequently transports AA
and DHA from mother to the fetus [15].
Omega-3 fatty acids especially have shown to be essential
for normal neurological development, maintenance of learn-
ing and memory, and neuronal plasticity. DHA are also
known to influence levels of neurotrophins especially brain-
Figure 1. Role of maternal micronutrients and omega-3 fatty acids in placental and fetal growth and development.
318 M. Dhobale & S. Joshi
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.
derived neurotrophic factor (BDNF). BDNF is associated
with alterations in neurogenesis and neuronal survival [16].
In the mammalian brain, major DHA accumulation occurs
late in gestation, parallel with maximal neuronal differentia-
tion process (neurogenesis), which consists of drastic mor-
phological and molecular changes. The formation of neurites
(axons and dendrites) is a key feature of neurogenesis, both
during development and in the adult. Several studies have
shown that DHA deficiency is critical during prenatal and
postnatal developmental stages leading to a variety of visual,
cognitive, and behavioural impairments [17].
Homocysteine. Hcy is a cytotoxic sulphur-containing amino acid
that can induce DNA strand breakage, oxidative stress, and
apoptosis. Homocysteine, a sulfhydryl-containing amino acid
that is not used in protein synthesis, originates exclusively from
the one-carbon donating metabolism of methionine, and it is
remethylated into methionine with folates acting as methyl
donors. Hcy arises during methionine metabolism in one-
carbon metabolism. Molecular mechanisms of homocysteine-
induced cellular dysfunction include increased inflammatory
cytokine expression, altered nitric oxide bioavailability, induc-
tion of oxidative stress, activation of apoptosis, and defective
methylation. Elevated maternal total homocysteine levels are
known to be associated with prematurity and LBW [18].
Hyperhomocysteinemia increases oxidative stress by indu-
cing oxidative stress promoting reactive oxygen species (ROS)
production by increasing NADPH oxidase. Oxidation is one
of the most favored postulated mechanisms explaining the
several toxic effects of homocysteine [19].
Oxidative stress
In pregnancy, the rapidly growing fetus has increased cellular
activity, which leads to increased oxidative stress. Oxidative
stress is characterized by excessive production of ROS
coupled with inadequate antioxidant defense mechanisms.
Free radicals such as ROS are formed during a variety of
biochemical reactions and cellular functions and resulting in
damages of all components of the cell. These result in
increased peroxidation of DNA, proteins/enzymes, and
membrane phospholipids, which result maternal and fetal
morbidity and mortality (Figure 3). Natural antioxidant
enzymes manufactured in the body provide an important
defense against free radicals. Glutathione peroxidase (GPx),
glutathione reductase (GR), catalase (CAT), and superoxide
dismutase (SOD) are among the most important antioxidant
enzymes.
Lipid peroxidation. Lipid peroxidation is an important mani-
festation of oxidative stress that occurs when oxygen free
radicals interact with LCPUFA in membranes or lipoproteins.
It is the process whereby free radicals take electrons from the
lipids in cell membranes, resulting in cell damage. This
process proceeds by a free radical chain reaction mechanism.
It most often affects polyunsaturated fatty acids because they
contain multiple double bonds in between where lies
Figure 2. Long-chain polyunsaturated fatty acids pathway.
Neurotrophic factors in preterm pregnancy 319
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.

methylene (-CH2-) groups that possess especially reactive
hydrogens. As with any radical reaction, the reaction
consists of three major steps: initiation, propagation, and
termination. In the initiation of lipid peroxidation, ROS
abstracts a hydrogen atom from an available lipid and
generates a second radical within the lipid bilayer, which
can react with another adjacent lipid. The chain reaction
spreads rapidly and can disrupt double bonds and fragment
lipids, leading to a loss of cell membrane integrity.
LCPUFA are more susceptible to lipid peroxidation
because of their high degree of unsaturation. Our earlier
studies in women delivering preterm indicate that maternal
plasma MDA levels were increased in preterm mothers as
well as in cord plasma samples [20]. Increased lipid
peroxidation and protein oxidation in both maternal and
fetal erythrocytes could be used as markers of oxygen
radical activity during intrauterine growth retardation.
Our recent studies in animals have shown that oxidative
stress is most likely triggered due to imbalance in maternal
micronutrients like folic acid and vitamin B12 during fetal
growth [21]. This may have implications for several neurode-
velopmental disorders since micronutrients and DHA are
important modulators for neural functioning. Increase in
oxidative stress can lead to reduced levels of neurotrophins
(Figure 4). Increased oxidative stress has been reported to be
associated with lower BDNF levels and neurodegenerative
disorders [22].
Neurotrophins
Neurotrophins are a unique family of polypeptide growth
factors that influence the proliferation, differentiation, survival
and death of neuronal and non-neuronal cells. There are four
family members of neurotrophins i.e. nerve growth factor
(NGF), brain-derived nerve growth factor (BDNF), neuro-
trophin-3 (NT-3), and neurotrophin-4 (NT-4). Neurotro-
phins play an important role for developing fetus during
pregnancy [23].
BDNF is abundant in peripheral nerves, affects normal
development, growth and survival and NGF promotes the
survival and functioning of cholinergic neurons in the basal
forebrain of the central nervous system. NGF and BDNF are
known to promote neuronal growth, differentiation in the
central and peripheral nervous system during fetal develop-
ment [24]. Each of these neurotrophic factors exerts its
biological activities through a family of tyrosine protein
kinases receptors (Trkases) and is responsible for mediating
neurotrophin signalling [25]. Two types of tyrosine kinase-
mediated neurotrophin receptors mediate biological activity:
high-affinity (Trk type A, B, and C) and low-affinity p75
receptor, a member of the tumor necrosis factor receptor
super-family. NGF selectively binds TrkA while, BDNF binds
Trk B, although some nonselective binding also occurs.
Our earlier studies, in first-episode schizophrenia, showed
significantly reduced levels of DHA [26] and BDNF, and
NGF levels in first-episode schizophrenia patients were also
significantly lower [27,28] in plasma as well as in cerebrosp-
inal fluid of schizophrenia patients compared to control
subjects suggesting that reduced levels of membrane DHA
may affect the neuronal plasticity as indicated by the reduced
levels of neurotrophins in schizophrenia.
Therefore, based on our earlier studies and reported data,
we propose that in mothers delivering preterm, changes in the
levels of micronutrients and omega 3 fatty acids especially
DHA during pregnancy leads to altered levels of homocys-
teine, which may result in methylation of neurotrophic factor
genes especially BDNF. These changes in levels of neuro-
trophins may be responsible for risk for neurodevelopmental
disorders in infants born preterm.
Very few studies have examined the levels of neurotrophins
in mother and cord samples during pregnancy complications.
There are limited studies that have examined levels of BDNF
during pregnancy [29,30]. Most of these studies are on a small
sample size and also could be confounded by the use of
antenatal steroids, which are known to alter the levels of
BDNF.
More systemic studies need to examine levels of neuro-
trophins from cord blood and maternal blood in women
delivering preterm pregnancy. This work will be useful in
predicting the risk for psychiatric disorders in childhood and
later life.
Consequences of the hypothesis: implications forneurodevelopment
Recent studies have shown that children born preterm are
associated with increased risk for developing attention deficit
hyperactivity disorder in childhood [31] and schizophrenia
later life [32].
Figure 3. Role of oxidative stress in pregnancy.
Figure 4. Increased oxidative stress and reduced levels of neuro-
trophins.
320 M. Dhobale & S. Joshi
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.
It is well established that 50% of the brain is made up of
DHA and AA, which play major role in brain development.
Studies also suggest that DHA regulate the levels of
neurotrophic factors. Neurotrophic factors like BDNF are
proteins abundant in brain and peripheral nerves, which affect
development, growth, survival, and differentiation of neural
cells. It has also been reported that maternal plasma vitamin
B12 status during pregnancy is a major determinant of the
child’s cognitive function at 9 years of age [33].
Influences of maternal nutrition on epigenetic programming
are most important during prenatal and early postnatal develop-
ment, when epigenetic mechanisms undergo establishment and
maturation. Disruption of normal gene-specific methylation
patterns by perturbations in maternal nutrition may affect the
pregnancy outcome having long-term implications in the
offspring. Recent attention has also focused on the potential role
of the amino acid homocysteine, in adverse pregnancy outcomes
[18]. Recently, homocysteine has also been shown to impair
short- and long-term memories and reduce BDNF levels in the
rat hippocampus. Recent reports also suggest important auto-
crine/paracrine roles of the BDNF/TrkB signalling system
during implantation, subsequent placental development, and
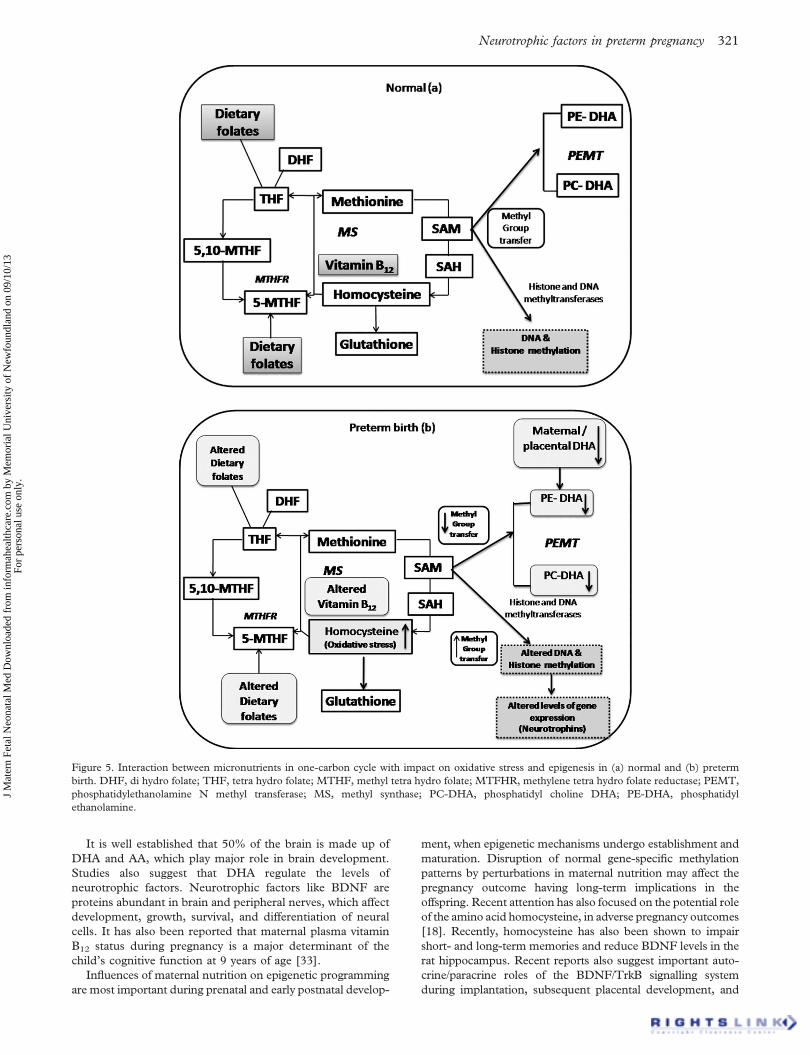
Figure 5. Interaction between micronutrients in one-carbon cycle with impact on oxidative stress and epigenesis in (a) normal and (b) preterm
birth. DHF, di hydro folate; THF, tetra hydro folate; MTHF, methyl tetra hydro folate; MTFHR, methylene tetra hydro folate reductase; PEMT,
phosphatidylethanolamine N methyl transferase; MS, methyl synthase; PC-DHA, phosphatidyl choline DHA; PE-DHA, phosphatidyl
ethanolamine.
Neurotrophic factors in preterm pregnancy 321
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.

fetal growth by increasing trophoblast cell growth and survival
[34]. However, the possible relationship between IUGR and
BDNF function remains unclear. In developing countries like
India, micronutrient deficiencies such as folic acid, vitamin B12,
and DHA are common and associated with poor pregnancy
outcomes such as LBW.
Our group has shown decreased DHA levels in pregnancy
complications like preterm and preeclampsia, which may result
in LBW babies [5,6]. It is known that low DHA levels are
associated with decreased levels of BDNF, which is crucial for
maintaining neuronal plasticity. Further, high levels of homo-
cysteine are associated with reduced DNA methylation
potential, whereas folate and vitamin B12 increase this potential.
Further, we have also reported in the one carbon cycle that when
DHA levels are low, influx of methyl groups may divert toward
histone and DNA [27]. It is possible that increased homo-
cysteine and reduced DHA status epigenetically alter the
BDNF gene resulting in altered expression at birth that persists
in later years. Influences of maternal nutrition on epigenetic
programming are most important during prenatal and early
postnatal development, when epigenetic mechanisms undergo
establishment and maturation. Disruption of normal gene-
specific methylation patterns by perturbations in maternal
nutrition may affect the pregnancy outcome having long-term
implications in the offspring.
Our recent several studies have shown that reduced
antioxidants and increased oxidative stress leads to impaired
essential polyunsaturated fatty acid levels that may be the key
factors involved in the development of preeclampsia [5,7].
Recent studies have shown that children born preterm are
associated with increased risk for neurodevelopmental beha-
vioural and cognitive disorders in childhood and continue in
adult life [31]. In our study, on drug-naıve patients with early
onset of psychosis and confirmed as schizophrenics showed
reduced levels of DHA, BDNF, and NGF in blood as well as
CSF at the onset of psychosis. Schizophrenia is well established
as the neurodevelopmental disorder. Thus, our data on
pregnancy complications and schizophrenia strongly support
the hypothesis that altered micronutrients like folic acid,
vitamin B12, and DHA, through the one-carbon cycle, may
cause epigenetic modifications of neurotrophins. This may
further contribute to risk for neurodevelopmental disorders in
children born preterm (Figure 5). Understanding the role of
neurotrophins like BDNF is timely and may provide important
clues to prevent such risk for neurodevelopmental disorders.
Conclusion
Therefore, based on this review, we conclude that in mothers
delivering preterm, altered levels of micronutrients (folate and
vitamin B12) and omega 3 fatty acids especially DHA during
pregnancy leads to altered one-carbon metabolism and
increased oxidative stress, affecting expression of neurotrophic
factors. These changes may be responsible for risk for the
metabolic and neurodevelopmental disorders in infants born
preterm. Further, we hypothesize that altered one-carbon
metabolism and oxidative stress may lead to altered epigenetic
regulation of neurotrophic factors in preterm pregnancy.
Acknowledgment
The authors acknowledge Indian Council of Medical Re-
search for giving the senior fellowship to one of the authors
(MD).
Declaration of interest: The author reports no conflicts of
interest. The authors alone are responsible for the content and
writing of the paper.
References
1. McCormick MC. The contribution of low birth weight to infant
mortality and childhood morbidity. N Engl J Med 1985;312:82–
90.
2. World Health Organization Report: World Health Statistics.
Geneva: World Health Organization; 2006.
3. King JC. Physiology of pregnancy and nutrient metabolism. Am J
Clin Nutr 2000;71:1218S–1225S.
4. Ramakrishnan U, Manjrekar R, Rivera J, Gonzales-Cossio T,
Martorell R. Micronutrients and pregnancy outcome: a review of
the literature. Nutr Res 1999;19:103–159.
5. Mehendale S, Kilari A, Dangat K, Taralekar V, Mahadik S, Joshi
S. Fatty acids, antioxidants and oxidative stress in pre-eclampsia.
Int J Gynaecol Obstet 2008;100:234–238.
6. Kilari A, Mehendale S, Dangat K, Yadav HR, Gupta A, Taralekar
VS, Joshi SR. Long chain polyunsaturated fatty acids in mothers
of preterm babies. J Perinat Med 2010;38:659–664.
7. Joshi SR, Mehendale SS, Dangat KD, Kilari AS, Yadav HR,
Taralekar VS. High maternal plasma antioxidant concentrations
associated with preterm delivery. Ann Nutr Metab 2008;53:276–
282.
8. Antony AC. In utero physiology: role of folic acid in nutrient
delivery and fetal development. Am J Clin Nutr 2007;85:598S–
603S.
9. McKay JA, Williams EA, Mathers JC. Folate and DNA
methylation during in utero development and aging. Biochem
Soc Trans 2004;32:1006–1007.
10. Picker JD, Coyle JT. Do maternal folate and homocysteine levels
play a role in neurodevelopmental processes that increase risk for
schizophrenia? Harv Rev Psychiatry 2005;13:197–205.
11. Stover PJ. Physiology of folate and vitamin B12 in health and
disease. Nutr Rev 2004;62:S3–S12.
12. Roth TL, Lubin FD, Sodhi M, Kleinman JE. Epigenetic
mechanisms in schizophrenia. Biochim Biophys Acta 2009;
1790:869–877.
13. Rao S, Joshi S, Kale A, Hegde M, Mahadik S. Maternal folic acid
supplementation to dams on marginal protein level alters brain
fatty acid levels of their adult offspring. Metabolism 2006;55:628–
634.
14. Harris WS, Mozaffarian D, Lefevre M, Toner CD, Colombo J,
Cunnane SC, Holden JM, Klurfeld DM, Morris MC, Whelan
J. Towards establishing dietary reference intakes for eicosapen-
taenoic and docosahexaenoic acids. J Nutr 2009;139:804S–
819S.
15. Haggarty P. Fatty acid supply to the human fetus. Annu Rev Nutr
2010;30:237–255.
16. Su HM. Mechanisms of n-3 fatty acid-mediated development and
maintenance of learning memory performance. J Nutr Biochem
2010;21:364–373.
17. Nettleton JA. Are n - 3 fatty acids essential nutrients for fetal and
infant development? J Am Diet Assoc 1993;93:58–64.
18. Selhub J. Public health significance of elevated homocysteine.
Food Nutr Bull 2008;29:S116–S125.
19. Tyagi N, Sedoris KC, Steed M, Ovechkin AV, Moshal KS, Tyagi
SC. Mechanisms of homocysteine-induced oxidative stress. Am J
Physiol Heart Circ Physiol 2005;289:H2649–H2656.
20. Joshi SR, Mehendale SS, Dangat KD, Kilari AS, Yadav HR,
Taralekar VS. High maternal plasma antioxidant concentrations
associated with preterm delivery. Ann Nutr Metab 2008;53:276–
282.
21. Roy S, Kale A, Dangat K, Sable P, Kulkarni A, Joshi S. Maternal
micronutrients (folic acid and vitaminB12) and omega 3 fatty
acids: implication for neurodevelopment risk in the rat offspring.
Brain Dev, in press.
322 M. Dhobale & S. Joshi
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.

22. Berk M, Kapczinski F, Andreazza AC, Dean OM, Giorlando F,
Maes M, Yucel M, Gama CS, Dodd S, Dean B, et al. Pathways
underlying neuroprogression in bipolar disorder: focus on
inflammation, oxidative stress and neurotrophic factors. Neurosci
Biobehav Rev 2011;35:804–817.
23. Sizonenko SV, Bednarek N, Gressens P. Growth factors and
plasticity. Semin Fetal Neonatal Med 2007;12:241–249.
24. Allen SJ, Dawbarn D. Clinical relevance of the neurotrophins and
their receptors. Clin Sci (Lond) 2006;110:175–191.
25. Skaper SD. The biology of neurotrophins, signalling pathways,
and functional peptide mimetics of neurotrophins and their
receptors. CNS Neurol Disord Drug Targets 2008;7:46–62.
26. Kale A, Joshi S, Naphade N, Sapkale S, Raju MS, Pillai A,
Nasrallah H, Mahadik SP. Opposite changes in predominantly
docosahexaenoic acid (DHA) in cerebrospinal fluid and red
blood cells from never-medicated first-episode psychotic patients.
Schizophr Res 2008;98:295–301.
27. Kale A, Joshi S, Naphade N, Sapkale S, Raju MS, Pillai A,
Nasrallah H, Mahadik SP. Reduced folic acid, vitamin B12 and
docosahexaenoic acid and increased homocysteine and cortisol in
never-medicated schizophrenia patients: implications for altered
one-carbon metabolism. Schizophr Res 2008;98:295–301.
28. Kale A, Joshi S, Pillai A, Naphade N, Raju M, Nasrallah H,
Mahadik SP. Reduced cerebrospinal fluid and plasma nerve
growth factor in drug-naıve psychotic patients. Schizophr Res
2009;115:209–214.
29. Malamitsi-Puchner A, Economou E, Rigopoulou O, Boutsikou
T. Perinatal changes of brain-derived neurotrophic factor in pre-
and fullterm neonates. Early Hum Dev 2004;76:17–22.
30. Chouthai NS, Sampers J, Desai N, Smith GM. Changes in
neurotrophin levels in umbilical cord blood from infants with
different gestational ages and clinical conditions. Pediatr Res
2003;53:965–969.
31. Shum D, Neulinger K, O’Callaghan M, Mohay H. Attentional
problems in children born very preterm or with extremely low
birth weight at 7-9 years. Arch Clin Neuropsychol 2008;23:103–
112.
32. Doyle LW, Anderson PJ. Adult outcome of extremely preterm
infants. Paediatrics 2010;126:342–351.
33. Bhate V, Deshpande S, Bhat D, Joshi N, Ladkat R, Watve S, Fall
C, de Jager CA, Refsum H, Yajnik C. Vitamin B12 status of
pregnant Indian women and cognitive function in their 9-year-old
children. Food Nutr Bull 2008;29:249–254.
34. Kawamura K, Kawamura N, Sato W, Fukuda J, Kumagai J,
Tanaka T. Brain-derived neurotrophic factor promotes implanta-
tion and subsequent placental development by stimulating
trophoblast cell growth and survival. Endocrinology 2009;150:
3774–3782.
Neurotrophic factors in preterm pregnancy 323
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
emor
ial U
nive
rsity
of
New
foun
dlan
d on
09/
10/1
3Fo
r pe
rson
al u
se o
nly.