alteration in esophageal motility after laryngectomy
TRANSCRIPT

Alteration in Esophageal Motility after Laryngectomy
Andre Duranceau, MD,’ Durham, North Carolina
Glyn Jamieson, MUD,7 Durham, North Carolina
Alfred L. Hurwltz, MD,* Durham, North Carolina
R. Scott Jones, MD, Durham, North Carolina
Raymond W. Postlethwait, MD, Durham, North Carolina
Laryngectomy is an accepted procedure in the treatment of laryngeal cancer [I]. This operation completely interrupts the continuity of the proxi- mal digestive tube and may lead to derangements in esophageal motility. Although dysphagia after laryngectomy has been reported [2], careful motil- ity analyses of the entire esophagus have not been performed in patients with laryngectomy. The purpose of the present investigation was to ob- serve the effect of laryngectomy on the motility of the esophagus and its sphincters.
Material and Methods
Patients. Manometric studies were performed on a consecutive group of twelve patients with laryngectomy selected from the ambulatory and inpatient otolaryngol- ogy service. Although half of the patients complained of some dysphagia, the only criterion for selection was prior laryngectomy. One patient underwent supraglottic laryngectomy whereas all the others had total laryngec- tomy. In two patients the esophageal motility studies were considered technically inadequate, and these pa- tients were eliminated from the study. All the laryngec- tomy patients were male with a mean age of fifty-nine years. Their demographic and clinical features are shown in Tables I and II.
Six patients without esophageal disease or symptoms were used as controls. Three of the six patients were
From the Department of Surgery and Division of Gastroenterology. Duke University Medical Center, and the Durham Veterans Administrations Hospital, Durham, North Carolina.
Reprint requests shoukf be addressed to R. Scott Jones, MD, Depart- ment of Surgery, Duke University Medical Center, Durham, North Caro- lina 27710.
Presented at the 16th Annual Meeting of the Society for Surgery of the Alimentary Tract, San Antonio, Texas, May 20-21. 1975.
l Present address: Department of Surgery, Hotel Dieu De Montreal, 3640 Rue St. Urbain, Montreal, Quebec H2W IT6. Canada.
t Present address: Department of Surgery, University of Adelaide. A& efatde 500 1, Australia.
* Present address: Eastroenterology Section, Veterans Administration Hospital, 4150 Clement Street, San Francisco, California 94121.
undergoing radiation therapy for laryngeal carcinoma prior to definitive surgery. All of the patients in the con- trol group were male with a mean age of fifty-seven years.
Apparatus. Manometric studies were performed with a triple lumen polyethylene tube, each lumen having an internal diameter of 0.8 mm and an orifice diameter of 1.2 mm. The lumen openings were 5 cm apart, oriented at approximately 120° to each other. Each lumen was perfused continuously with water at 1.91 cc/min, utiliz- ing a Harvard Syringe Infusion pump. The pressures from the columns of water were transmitted to external Statham P-23 strain gauges and transcribed by a San- born 350 recorder.
Calibration. The water-filled apparatus was calibrat- ed with a mercury manometer, the entire system being open to air. Pressures were recorded in mm Hg, the zero reference point being atmospheric pressure. The appa- ratus was calibrated at the beginning and conclusion of each study.
Procedure. The manometry tube was passed into the stomach via the nares. It was then removed by 0.5 cm increments in the region of the two esophageal sphinc- ters and by 1.0 cm increments in the body of the esopha- gus. Constant recording of all swallows was monitored by a belt pneumograph placed around the patient’s neck. The patient sipped 2 cc of water with each swallow (“wet swallows”). The patient was in the supine position with the pressure transducers positioned at head level. Paper speed was 1 mm/set for recordings of the lower esophageal sphincter (LES) and esophageal body and 5 mm/set for recordings of the upper esophageal sphincter (UES).
Manometric Interpretation. All swallows recorded in the UES and LES were analyzed for pressure, degree of relaxation, and degree of coordination. Measurements of esophageal body wave pressure and peristalsis were made over a 3 cm midsegment on either side of an arbi- trary line halfway between the two sphincters. This line separated “proximal” from “distal” esophagus.
The interpretation of the manometric recordings was made according to the following criteria. The UES was
30 The American Journal of Surgery

Esophageal MotMty after Laryngectomy
TABLE I Demographic and Surgical Features of the Laryngectomy Patients ~_____~~
Previous Age Radio- Gastrointestinal
Patient and Sex Diagnosis Operation therapy Surgery -_ ..~..__.._. .~_________
1 62.M Carcinoma of larynx with Total laryngectomy and left Yes Vagotomy and left neck metastases radical neck dissection pyloroplasty
2 54,M Carcinoma of larynx Total laryngectomy No NO
3 56,M Carcinoma of tongue Total laryngectomy and right Yes No radical neck dissection
4 64,M Supraglottic carcinoma Total laryngectomy and left No Hemigastrectomy radical neck dissection
5 50,M Bilateral vocal cord carcinoma Total laryngectomy and right No No with right neck metastases radical neck dissection
6 73,M Carcinoma of left pyriform Total laryngectomy and left NO No sinus radical neck dissection
7 51,M Carcinoma of larynx with Total laryngectomy and left No No left neck metastases radical neck dissection
a 63,M Carcinoma of larynx Total laryngectomy No No 9 59,M Carcinoma of larynx Total laryngectomy and right No No
radical neck dissection 10 61,M Carcinoma of epiglottis Supraglottic laryngectomy and Yes No
left radical neck dissection -.--- -_-----.-..--._~ ~
“coordinated” with pharyngeal contraction when the peak of pharyngeal contraction corresponded to the nadir of UES relaxation; in addition, the phase of UES relaxation entirely encompassed the phase of pharyn- geal contraction. When the UES relaxed within 5 mm Hg of baseline cervical esophageal pressure, UES relaxa- tion was “complete.”
Peristalsis in the body of the esophagus was “normal” when the wave peaks were separated by more than 1.25 seconds. This corresponds to a maximum wave speed of
4 cm/set. The LES was “coordinated” when the phase of LES
relaxation entirely encompassed the oncoming petistal- tic wave. When the LES relaxed to within 5 mm Hg of intragastric pressure, LES relaxation was “complete.”
The statistical method employed was the t test for un- paired values, and p < 0.05 was considered statistically
significant.
Results
Upper Esophageal Sphincter (Figure 1). There
was a statistically significant difference between
the control group and the laryngectomy group for the resting and contraction pressures as well as for the coordination and relaxation of the UES. The
control group showed a resting pressure of 34.3 f
6.8 mm Hg (mean value f SEM); the peak postde- glutition pressure was 46.4 f 8.4 mm Hg. The UES coordination with the pharynx was normal in 98.9 f 1.1 per cent of swallows, and its relaxation was complete in 97 f 2.3 per cent of swallows. In the
Laryngectomy patients the resting UES pressure was 12.9 f 3.0 mm Hg; the peak postdeglutition pressure was 24.5 f 3.5 mm Hg. The coordination
TABLE I I Symptoms of the Laryngectomy Patients ---~ -_-
Pa- Dys- Regurgi- Py- Odyno- tient phagia tation rosis phagia Aspiration
--.-- --- 1 No No No No Not Applicable* 2 Yes No No No Not Applicable* 3 Yes No No No Not Applicable* 4 No No No No Not Applicable* 5 Yes Yes No No Not Applicable* 6 No Yes No No Not Applicable* 7 Yes No No No Not Applicable* a No Yes Yes No Not Applicable* 9 No No No No Not Applicable*
10 Yes No No No Yes+ -...- ..-.--- --
* Permanent tracheostomy. + Supraglottic laryngectomy.
P < 0.025 PixSSURE P<OO5
PcOO25 P<O.OI
Flpure1.Upperesoph8fwlsphhctefhconttiandpa-
thts. si&ukult Mbr8f~~es af8 fmtd h&zathg h- pabd tuncth 8tt.r taryqpctomy.
Volunu 131, Januaw 1976 31

Dwanceau et al
mmHg
- CONTRACTION PRESSURE
P <to5
-COOROINAllON
PCO.025
Figure 2. Proximal esophagus. lmpairmenf of wave con- trection and reductbn in coordinated perktakk k noted in ttte /aryngectomees.
Figure 3. ._
C~NTRACTIOII PRESSURE
P < 0.025
COORDlNAIlON
P < 0.05
Dktai esophagus. impaimwnt of wave contrac- tfon and of coordinated perktakis k noted in the iaryn- gectomy patknts.
PRESSURE lls
PfAK x POST M6lulllloN COORDINAIION
PRESSURE Y.S N.5 NS
Figure 4. Lower esophageal sphincter. No difference in functh k noted between controls and iaryngectomees.
32
was normal in 73.9 per cent of swallows, whereas
relaxation was complete in 65.3 f 9.4 per cent of
swallows. Proximal Esophagus (Figure 2). There was a
statistically significant difference between the proximal esophageal waves studied in patients
with laryngectomy and those studied in controls.
In both groups the resting intraesophageal pres-
sure was normal (-4.0 mm Hg in the control group
and -5.2 mm Hg in the laryngectomees. Wave
pressure in controls showed a mean peak pressure
of 24.1 f 3.2 mm Hg, with normal peristalsis in 99
per cent of the waves. The patients with laryngec-
tomy showed markedly diminished peak contrac- tion pressures with a mean of 13.7 f 2.6 mm Hg;
only 76 f 11.3 per cent of the waves showed a nor-
mal peristaltic pattern.
Distal Esophagus (Figure 3). Esophageal peri-
stalsis was also significantly affected in the distal
half of the esophagus. In both groups, the resting
pressures corresponded to normal intraesophageal
pressures (-3.5 mm Hg in controls, -5.4 mm Hg
in patients with laryngectomy). The peak wave
pressures were significantly different, with mean
pressures of 58.7 f 13.7 mm Hg in the control
group and 20.4 f 2.8 mm Hg in the laryngectomy
group. All the waves (100 per cent) were well coor- dinated in the control patients, but only 85.0 f 8.5 per cent were coordinated in the patients with lar-
yngectomy. Lower Esophageal Sphincter (Figure 4). No sig-
nificant difference between controls and laryngec-
tomees were noted in the resting and postdegluti-
tion LES pressures, nor in the degree of LES coor-
dination and relaxation. In the control group the
resting pressure was 14.6 f 1.9 mm Hg, and the
peak postdeglutition pressure was 23.4 f 2.2 mm
Hg. The coordination of the sphincter with the on- coming wave was normal in 90.2 f 3.6 per cent of the swallows, and complete relaxation occurred in
92.8 f 3.4 per cent of swallows. The laryngectomy patients had a slightly lower resting pressure of
10.0 f 2.2 mm Hg, with a postdeglutition pressure
of 18.6 f 3.1 mm Hg. The LES coordination was normal in 94.8 f 2.8 per cent of the swallows and its relaxation complete in 97.5 f 1.2 per cent of the swallows.
Comments
Dysphagia may occur after total or partial laryn- gectomy [2,3]. Although this complication is not commonly reported, its occurrence may produce much disability. Marked postoperative difficulties
The American Journal of Sugery

Esophageal MotMty after Laryngectomy
40 Ucm 22 cm
PROX. ESOPH. 20
0 t _ //__>
T
F&we 5. Mttttty trachgs of two f.iatk?nts (A and 6) showkg kmwn#ete relaxatkn of the upper esophageal spnkrcrer. WS = wet swallow.
may develop in some patients as a consequence of dysphagia, whereas pulmonary soilage may devel- op in those without permanent tracheostomy.
The clinical basis for dysphagia in this setting is threefold: (1) interruption of the upper digestive tube, (2) interruption of the pharyngeal branches of the vagus nerve, and (3) anterior fixation of tra- cheal structures due to suigical or tracheostomy- induced cicatrix [3,5].
Interruption of the upper digestive tube after laryngectomy may interfere with swallowing func- tion in two ways. First, it may completely sever the connection of the laryngeal constrictors, the most important of which is the cricopharyngeus. This will tend to obliterate the major pressure compo- nent of the upper “high pressure zone” as mea- sured manometrically. Second, loss of the pharyn- geal constrictors may impair UES relaxation (Fig- ure 5), since such relaxation requires an adequate pharyngeal pressure stimulus [6]. The effects of pharyngoesophageal transection on esophageal peristalsis and LES function are unknown.
The pharyngeal branches of the vagus nerve are probably responsible for maintaining the resting tone, relaxation, and contraction of the UES [7]. Interruption of these branches and of the superior laryngeal nerves may interfere with the motor function of this structure as well as impair the sen- sation in the larynx and epiglottis. Since radical laryngectomy leads to sacrifice of local vagal branches bilaterally, impairment of UES function might occur [6]. Furthermore, experimental cervi- cal vagotomy in the dog may produce a manomet- ric picture suggestive of achalasia [8]. Therefore, vagal interruption after laryngectomy may not
-
25sec- Ftgure 6. MottMy tractngs of two path& (A ami 6) showtng lack of coordtnated pet&tats& h the body of the esophagus. WS = wet swattow.
only produce local derangements in UES function but may also produce abnormalities in esophageal peristalsis and LES function.
Finally, anterior fixation of peritrachael struc- tures may occur with laryngectomy and preclude forceful pharyngeal contraction [5]. As stated above, an adequate pharyngeal stimulus is re- quired for normal UES relaxation. Diminution of this stimulus, therefore may produce dysphagia.
The present study shows marked derangement in UES relaxation and coordination in laryngec- tomees when these patients are compared to con- trols. These findings confirm the clinical and ex- perimental data stated previously [6-101.
A unique finding in this study was the signifi- cant reduction in esophageal body wave pressures and in percentage of normal esophageal peristaltic waves. (Figure 6.) This finding occurred in both proximal and distal esophagus, and suggests that disruption of the pharyngoesophageal junction af- fects wave pressure and propagation in the skeletal and smooth-muscled esophagus. The exact neuro-
Volume 131, January 1976 33
Duranceau et al
STOMACH 20
49cm 55 cm
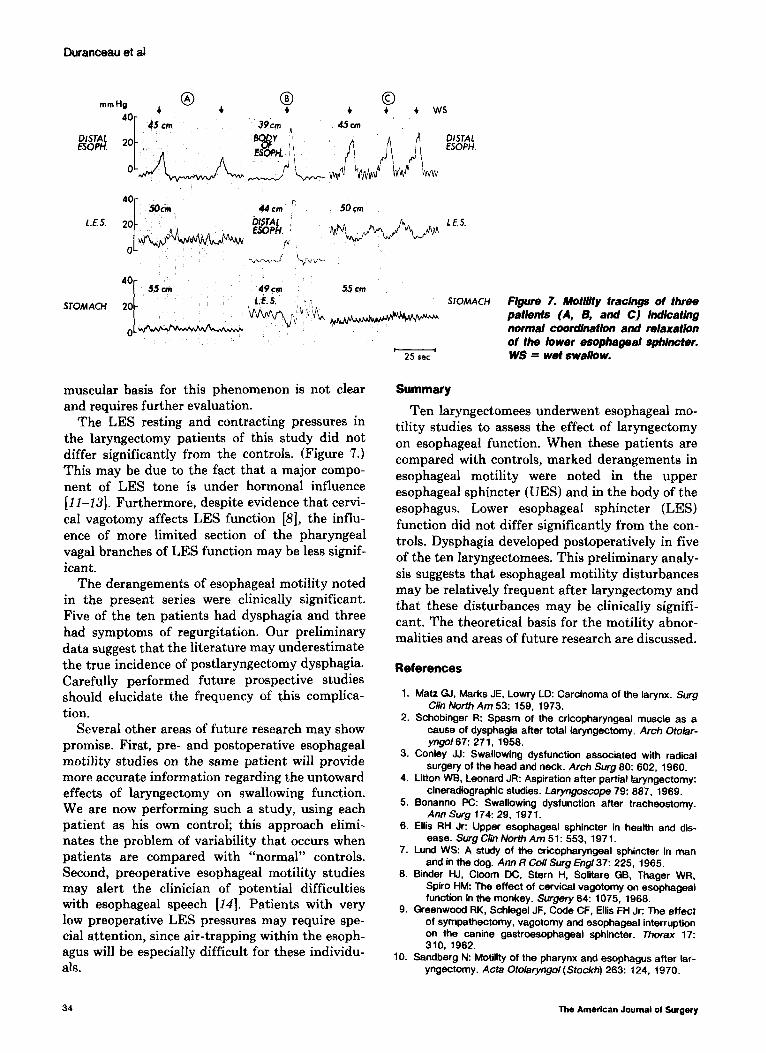
1. E. s. . ; STOMACH Figure 7. Motility tracings of three patientS (A, B, and C) indicating
muscular basis for this phenomenon is not clear and requires further evaluation.
Summary
The LES resting and contracting pressures in the laryngectomy patients of this study did not differ significantly from the controls. (Figure 7.) This may be due to the fact that a major compo- nent of LES tone is under hormonal influence [II-131. Furthermore, despite evidence that cervi- cal vagotomy affects LES function [8], the influ- ence of more limited section of the pharyngeal vagal branches of LES function may be less signif- icant.
The derangements of esophageal motility noted in the present series were clinically significant. Five of the ten patients had clysphagia and three had symptoms of regurgitation. Our preliminary data suggest that the literature may underestimate the true incidence of postlaryngectomy dysphagia. Carefully performed future prospective studies should elucidate the frequency of this complica- tion.
Ten laryngectomees underwent esophageal mo- tility studies to assess the effect of laryngectomy on esophageal function. When these patients are compared with controls, marked derangements in esophageal motility were noted in the upper esophageal sphincter (UES) and in the body of the esophagus. Lower esophageal sphincter (LES)
function did not differ significantly from the con- trols. Dysphagia developed postoperatively in five of the ten laryngectomees. This preliminary analy- sis suggests that esophageal motility disturbances may be relatively frequent after laryngectomy and that these disturbances may be cIinicaIly signifi- cant. The theoretical basis for the motility abnor- malities and areas of future research are discussed.
References
1. Matz 61, Marks JE, Lowry LD: Carcinoma of the larynx. Surg C/in North Am 53: 159, 1973.
Several other areas of future research may show promise. First, pre- and postoperative esophageal motility studies on the same patient will provide more accurate information regarding the untoward effects of laryngectomy on swallowing function. We are now performing such a study, using each patient as his own control; this approach elimi- nates the problem of variability that occurs when patients are compared with “normal” controls. Second, preoperative esophageal motility studies may alert the clinician of potential difficulties with esophageal speech [14]. Patients with very low preoperative LES pressures may require spe- cial attention, since air-trapping within the esoph- agus will be especially difficult for these individu- als.
2. Schobinger R: Spasm of the cricopharyngeal muscle as a cause of dysphagia after total laryngectomy. Arch Otobr- yngo167: 271, 1958.
3. Coniey JJ: Swallowing dysfunction associated with radical surgery of the head and neck. Arch Surg 80: 602, 1960.
4. Litton Wi3. Leonard JR: Aspiration after partial laryngectomy: cineradiographic studies. Laryngoscope 79: 887, 1969.
5. Eonanno PC: Swallowing dysfunction after tracheostomy. Ann Surg 174: 29, 1971.
6. Ellis RH Jr: Upper esophageal sphincter in health and dis- ease. Surg C/in North Am 51: 553. 1971.
7. Lund WS: A study of the cricopharyngeal sphincter in man and in the dog. Ann R Co/l Surg Engl37: 225. 1965.
8. Binder HJ, Cloom DC, Stern H, Soliiare GB, Thager WR, Spiro HM: The effect of cervical vagotomy on esophageal function in the monkey. Surgery 64: 1075. 1968.
9. Greenwood RK, Schlegel JF, Code CF, Ellis FH Jr: The effect of sympathectomy, vagotomy and esophageal interruption on the canine gastroesophageal sphincter. Thorax 17: 310, 1962.
10. Sandberg N: Motility of the pharynx and esophagus after lar- yngectomy. Acta Otokiryngol (Stockh) 263: 124. 1970.
34 The American Journal of Surgery
normal coordination and relaxation of the lower esophageal sphincter. WS = wet swallow.

Esophageal Motility after Laryngectomy
Il. Cohen S, Harris LD: The tower esophageal sphincter. Gas- froenferohqy 63: 1066, 1972.
12. Cohen S, Lipshutz W: Hormonal regulation of human lower esophageal sphincter completence: interaction of gastrin and secretin. J C/in hvest 50: 449, 197 1.
13. Jaffer SS, Maklout GM, Schorr BA, Zfass AM: Nature and ki- netics of fnhibltion of lower esophageal sphincter pressure by glucagon. Gastroenterobgy 67: 42, 1974.
14. Wolfe RD, Olson JE, Goldenberg DB: Rehabilitation of the laryngectomee: the role of the distal esophageal sphinc- ter. Laryngoscope 81: 1971, 1971.
Gilbert Hermann (Denver, CO): Is there a relation- ship between these studies and clinical symptoms? Fol- lowing the lead of Doctor Ellis, who has done much of this work, we attempted to correlate pressure studies with clinical symptoms. We found that some patients with a great deal of motility abnormalities had few symptoms and other patients that have had few abnor- malities had many symptoms. We have not been able to predict on the basis of motility studies alone which pa- tients are going to have trouble with swallowing and which are not. Was there correlation between the abnor- malities that were seen here and the clinical symptoms in individual patients?
Thomas Taylor Smith (Seattle, WA): We have had several patients who have had a soft tube inserted into the trachea after some pulmonary difficulty from vomit- ing with aspiration. The tube was left in for several days, after which the patients had severe difficulty swallow- ing. After tracheostomy, the patients had to learn to swallow again. The respiratory and head and neck sur- geons in Seattle tell me that this is extremely common and I wonder whether this is not a problem both post laryngectomy and a post assisted breathing.
David B. Skinner (Chicago, IL): Recently, Doctor Charles Winans and colleagues from our Gastroenterol- ogy Group studied laryngectomy patients to see if it could be predicted which ones would be able to master esophageal speech. As I recall that study, there was a correlation between the patient’s ability to master the art of esophageal speech after laryngectomy and a di- minished cricopharyngeal sphincter pressure. I would like to ask the authors if they could correlate their manometric findings to the patient’s ability to master esophageal speech.
Robert E. Condon (Milwaukee, WI): The problem of patients who have had laryngectomy, or tracheostomy, is that there is fixation of the tissues in the neck, partic- ularly anteriorly. Most patients who have difficulty swallowing post laryngectomy learn to handle this by extending their neck to produce a cone in the pharynx. It is like a pelican swallowing a fish. From the diagram of the authors’ studies, it looked as though their patients were having wet swallows in the horizontal position. I am curious if the authors studied any patients in the vertical position and particularly during pharyngeal coning produced by vertical extension.
Harlan Root (San Antonio, TX): Would the authors discuss the possible influence of vagal injury in this se- ries? I think the proximal esophageal disruption has been addressed by Doctor Condon, but whether or not vagal injury has occurred should be studied and evalu- ated for motility abnormality.
Andre Duranceau (closing): In answer to Doctor Hermann’s question, for the correlation of clinical symptoms, two out of ten patients had severe dysphagia; three had a very moderate to slight dysphagia, qualified as sticking of food after swallowing; and five patients were completely asymptomatic.
As for Doctor Smith’s remarks, we think that a differ- ent mechanism was involved in this study. These studies were all made many months after laryngectomy and we think a different etiologic feature may he involved.
Regarding esophageal speech therapy, the correlation was attempted in both since this was mainly a retrospec- tive study compared with a similar control group. It was a difficult correlation to make and we think that only with a well planned prospective study would such a cor- relation be made. We could not actually show a correla- tion in our group.
In response to Doctor Condon, no vertical studies were performed in any of our patients, and in the whole of our study, we used wet swallows only in the horizontal position.
In answer to Doctor Root, we think that the vagal in- fluence is probably an important one. We did not evalu- ate formally the vagal function after laryngectomy, but the interruption of vagal branches might play an impor- tant role in the abnormalities that we have seen in our work.
volume 131, January 1979 35