manual control of the upper esophageal · pdf filemanual control of the upper esophageal...
TRANSCRIPT

The LaryngoscopeVC 2010 The American Laryngological,Rhinological and Otological Society, Inc.
TRIOLOGICAL SOCIETYCANDIDATE THESIS
Manual Control of the Upper EsophagealSphincter
Peter C. Belafsky, MD, PhD
Objectives/Hypothesis: Oropharyngeal dyspha-gia (OPD) is common and costly. In order to improvequality of life for patients and costs to society, bettertreatments than currently available are needed. Theauthor hypothesized that manual control of the upperesophageal sphincter (UES) is possible by pulling thelarynx directly forward with anterior traction on thecricoid cartilage. The purpose of this investigationwas to evaluate the effectiveness of manual control ofthe UES as a possible therapy for OPD.
Study Design: Retrospective chart review, med-ical device development, prospective cadaver trial,and prospective animal experiment.
Methods: Charts were reviewed of all personswith OPD who had a traction suture placed by theauthor around the anterior rim of the cricoid carti-lage. The opening of the UES was assessed with andwithout traction on the suture. The ability of the cri-coid suture to improve UES opening was evaluatedunder fluoroscopy. The Swallow Expansion Device(SED) was designed to manually control the UES.The ability of the SED to manually open the UESwas evaluated. The SED was implanted in 10 cadav-ers, and 5,000 pulls of the device were performed oneach specimen to evaluate for gross damage to thecricoid cartilage. The ability of the SED to open theUES was evaluated under direct laryngoscopy. Thesafety and efficacy of the SED was evaluated in anovine model of OPD. The SED was implanted in eightsheep. Five thousand pulls of the device were per-formed on each animal weekly for 8 weeks. At theend of the study, damage to the cricoid cartilage was
evaluated histologically, and the ability of the SED toopen the UES and eliminate aspiration was assessedfluoroscopically.
Results: Six patients with OPD who had asuture placed around the anterior aspect of the cri-coid cartilage were identified. Anterior traction on thesuture improved UES opening by 0.36 cm (60.19 cm)(P < .01). A titanium-coated ferrous implant thatsecures to the cricoid cartilage was fabricated (SED).An external magnetic device that affixes to theimplant across intact skin was developed. Anteriortraction of the SED opened the UES in cadavers amean of 1.16 cm (60.22 cm) (P < .001). Anterior trac-tion on the SED opened the UES in sheep a mean of1.27 cm (60.36) (P < .001). Aspiration was eliminatedin 100% of the animals. The implant became infectedand had to be removed in one (12.5%) animal. Remod-eling of the cricoid cartilage was evident, but therewas no histologic evidence of cartilage damage.
Conclusions: Manual control of the upperesophageal sphincter is possible. Simple anterior trac-tion on the suture placed around the cricoid cartilageimproved UES opening by 0.36 cm (60.19) in a cohortof dysphagic patients. The Swallow Expansion Deviceopened the UES of cadavers and living sheep tosuperphysiologic proportions (P < .001). There was nohistologic evidence of cricoid damage from prolongeduse of the implant.
Key Words: Upper esophageal sphincter,swallow expansion device, oropharyngeal dysphagia,cricopharyngeus muscle, dysphagia, esophagus.
Laryngoscope, 120:S1–S16, 2010
INTRODUCTIONIn order of phylogenetic importance, the three pri-
mary functions of the larynx are airway protection,respiration, and phonation.1 If the larynx is unable toprovide adequate airway protection during deglutition,or the pharynx is unable to provide adequate bolustransit through the upper esophageal sphincter, oropha-ryngeal dysphagia (OPD) ensues. Causes of OPD includestroke, head and neck cancer, head injury, advancingage, cricopharyngeus muscle dysfunction, amyotrophiclateral sclerosis, pseudobulbar palsy, Alzheimer’s
From the Department of Otolaryngology/Head and Neck Surgery,University of California, Davis, Sacramento, California, U.S.A.
Editor’s Note: This Manuscript was accepted for publicationDecember 9, 2009.
This work was supported by a technology transfer award from theUniversity of California, Davis and partially supported by a developmentgrant from Medtronic, Inc. The University of California, Davis has fileda USPTO Patent Application (ID# 20090137859) based on this work.Dr. Belafsky is a consultant for Medtronic, Inc.
Send correspondence to Peter C. Belafsky, MD, Department ofOtolaryngology/HNS, University of California, Davis, 2521 StocktonBlvd., Suite 7200, Sacramento, CA 95817. E-mail: [email protected]
DOI: 10.1002/lary.20833
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S1

disease, Parkinson’s disease, multiple sclerosis, musculardystrophy, and myasthenia gravis. Estimates of theprevalence of OPD are staggering. Up to 16% of the gen-eral population may suffer from OPD.2 The prevalenceof dysphagia in the elderly may be as high as 50%.3 Con-current chemoradiation for head and neck cancer isassociated with a 45% incidence of prolonged feedingtube-dependent OPD and an incidence rate for aspira-tion of 59%.4,5 The incidence of dysphagia after stroke,the third leading cause of death in the United States,has been reported to be as high as 81%.6 Up to 60% ofnursing home residents suffer from OPD.7 The incidenceof swallowing difficulties in persons with Parkinson’sdisease is nearly 100%.8 By 2010, it is estimated that16.5 million people will need treatment for dysphagia.9
Despite the high prevalence of dysphagia, current treat-ment options provide only partial relief.
The impact of OPD on quality of life, morbidity, mor-tality, and healthcare expenditure is significant. In asurvey of nasopharyngeal cancer survivors, dysphagiawas the most important predictor of diminished quality oflife.10 Elevated anxiety and depression are associatedwith dysphagia in head and neck cancer patients.5 Dys-phagia in persons after total laryngectomy is associatedwith markedly increased social isolation, significantlyimpaired global functioning, depression, and anxiety, andin the general population, dysphagia is associated withdepression and reduced general health.11,12 Dysphagia isalso associated with the feeling of helplessness, and themajority of persons with OPD believe that their conditionis untreatable.13 Complications of dysphagia includeaspiration, dehydration, pneumonia, malnutrition, depres-sion, and death. The dysphagia-specific mortality rate inpersons treated with chemoradiation for head and neckcancer is 9%.5 Aspiration pneumonia is one of the mostcommon causes of death after stroke and is the most com-mon cause of death in persons with Parkinson’s disease.8,14
The incidence of aspiration pneumonia and death is nearly20% in poststroke dysphagic patients.14 Nursing homepatients with OPD have a 45% 12-month mortality rate.15
The yearly expenditure for an individual dependent ontube feeding is $30,000, and Medicare spends 6% of its an-nual durable medical equipment budget ($670 million) onenteral feeding supplies.16 Because of the high economiccost of OPD, the significant impact of OPD on quality oflife, and the associated morbidity and mortality, improvedrecognition and treatment of this disorder are warranted.
For persons with OPD, current treatment optionsinclude diet modification, swallowing therapy, intraoralprosthetics, nonoral feeding, and invasive surgery.17–29 Ifa comprehensive dysphagia assessment with videofluoro-scopy or nasoendoscopy reveals difficulty with certainfood consistencies, dietary restrictions may be recom-mended or food rheology may be manipulated.Depending on the individual needs and the cognitiveability of the patient, swallowing therapy may includeexercise, sensory enhancement, postural changes, trans-cutaneous electrical stimulation, and swallowingmaneuvers.17–19 Dental prosthetics may be employed torestore function to defects of the palate and tongue.20 Ifconservative management is unsuccessful in mitigating
OPD, surgery may be considered. Surgical proceduresshown to improve swallowing function in certain individ-uals with OPD include esophageal and upper esophagealsphincter dilation, cricopharyngeus muscle botulinumtoxin injection, cricopharyngeus muscle myotomy, medi-alization laryngoplasty, arytenoid adduction,laryngohyoid suspension, pharyngoplasty, epiglottopexy,lateral thyrolaminectomy, great auricular to superiorlaryngeal neurorrhaphy, diverticulectomy and diverticu-lotomy in patients with a hypopharyngeal diverticulum,vocal fold closure, laryngotracheal separation, and totallaryngectomy.21–29 The aim of these operations is toimprove laryngopharyngeal sensation, airway protection,and upper esophageal sphincter (UES) opening. Regard-less of our best efforts, these treatments fail in asignificant percentage of individuals.
Biomedical devices are accepted and used commonlyin medicine—artificial joints, cochlear implants, andpacemakers, to name a few. Cutting edge medical deviceresearch continues to move forward with, for example,clinical trials of retinal prostheses in blind persons andwireless telemetry of EMG signals being used to controlupper extremity prostheses.30,31 Although great progressin biomedical devices has been made for many other dis-orders, there is currently no device available to assistwith the act of deglutition.
The pharyngeal phase of deglutition requires intri-cate synchronization between lingual and pharyngealcontraction and relaxation of the UES. Opening of theUES requires elevation of the larynx off of the posteriorhypopharyngeal wall, muscular relaxation of the toni-cally active cricopharyngeus muscle, and distentioncaused by the passing bolus. The most important factorresponsible for UES opening is deglutitive laryngeal ele-vation.32 The most common cause of profound dysphagiais typically a combination of reduced lingual and pha-ryngeal contraction pressure and limited or absentlaryngohyoid elevation.29 Some of the disease statesassociated with diminished lingual and pharyngeal func-tion and diminished elevation include stroke, head andneck cancer, amyotrophic lateral sclerosis, head injury,skull base surgery, multiple sclerosis, and muscular dys-trophy. For individuals with profound OPD who failcurrently available methods of intervention, definitivetreatment options are limited. Most procedures involve apermanent separation of the airway and food passage,as occurs with total laryngectomy and laryngotrachealseparation. These surgeries are morbid and result inpermanent functional deficits. Oropharyngeal dysphagiais a mechanical problem in need of a biomechanical solu-tion. The author hypothesized that manual control ofthe UES was possible with a biomedical device.
The UES is a 2- to 5-cm long high-pressure zonelocated between the pharynx and esophagus. Because ofits location, this region has more appropriately beencalled the pharyngoesophageal segment or PES. TheUES refers specifically to the intraluminal high-pressurezone measured by manometry. The PES refers to theanatomic components that make up the high-pressurezone. The terms UES and PES are synonymous and maybe used interchangeably. The cricopharyngeus muscle
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S2

(CPM) makes up only one component of the PES. TheCPM is not synonymous with the UES and PES. TheUES can be modified with therapy and surgery. It is forthis reason that the UES has captured the interest ofnumerous dysphagia clinicians and surgeons.
The UES is made up of the inferior pharyngeal con-strictor, the CPM, and the most proximal portion of thecervical esophagus. All three muscles help maintain rest-ing tone. The functions of the UES are to preventaerophagia during respiration and phonation and toprotect against regurgitation of refluxed gastric and esoph-ageal contents into the pharynx and airway. The UESpossesses basal tone and remains in a contracted state atrest. It opens reflexively during deglutition, eructation,and emesis. Esophageal distension, pharyngeal stimula-tion, emotional stress, and acid instilled into the esophagusall contract the UES reflexively.33–36 Of the three compo-nents that make up the UES, only the CPM constricts andrelaxes during all reflex tasks. For this reason, many clini-cians regard the CPM as the only true sphincter.
The CPM is a C-shaped muscle attached to the lat-eral lamina of the cricoid cartilage. It consists of ahorizontal pars fundiformis and an oblique pars obliqua.A combination of slow type I and fast type II musclefibers allows the CPM to maintain a constant basal toneand to rapidly expand and contract when necessary.Intricate microdissections in 27 persons undergoing totallaryngectomy by Sasaki et al. suggest that the CPMreceives dual ipsilateral innervation from the pharyn-geal plexus (PP) and the recurrent laryngeal nerve(RLN).37 The PP projects to the posterior and the RLNprojects to the anterior motor units of the muscle. Sen-sory information from the CPM is provided by theglossopharyngeal nerve and cervical sympathetics.
The act of swallowing depends upon adequate andtimely UES opening. Opening of the UES depends upon
muscular relaxation, elevation of the larynx, and pha-ryngeal contraction. Jacob et al. described five phases ofUES opening.32 In phase I there is inhibition of tonicPES contraction. This is followed by elevation of thehyoid bone and larynx (phase II). In phase II, hyolaryng-eal excursion provides active opening of the UES. Theactive opening provided by elevation appears to be moreimportant than muscular inhibition. The UES can openby active distraction alone. Muscular relaxation withoutelevation will not open the UES. The larynx sits againstthe spine at rest (Fig. 1a). Without elevating the larynxaway from the spine, there is no outflow tract to allowpassage of a food bolus. If the larynx does not elevate toopen the UES, relaxation of the CPM is inconsequential.This has significant clinical implications as swallowingin individuals with good hyolaryngeal elevation butincomplete CPM relaxation is possible and frequentlyencountered (CPM bar, Fig. 1b). Swallowing in individu-als who can relax their CPM but cannot elevate theirlarynx and contract their pharynx to actively open theUES has not been observed. This accounts for thevariability in surgical outcomes reported with cricophar-yngeus muscle myotomy.38
Phase III of UES opening involves distention of theUES through bolus size and weight. This phase reliesupon pharyngeal and lingual peristalsis to propel thebolus past the spacious hypopharynx, through the nar-rowed but expanding UES, and into the cervicalesophagus. The elasticity of the UES allows it to beopened by the increasing pressure exerted by the pass-ing bolus. As the bolus passes, this elasticity causes acollapse of the UES (phase IV). Phase V involves UESclosure through active muscle contraction. For reasonsdiscussed subsequently, the author hypothesized thatpulling the cricoid cartilage anteriorly will bypass thesefive stages and directly open the UES.
Fig. 1. Region of the upper esophageal sphincter (UES). (a) At rest, the larynx is in juxtaposition to the anterior cervical spine and the UESis closed (red line). There is no passage to accept a food bolus. In order to open the UES, the larynx must elevate off of the spine in ananterior and cranial direction. (b) The larynx has elevated during deglutition and the UES is open. There is incomplete relaxation of thecricopharyngeus muscle (CPM) and a CPM bar is present (red arrow).
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S3

The first report of a surgeon manipulating the lar-ynx to open the UES was by Yrjo Meurman in 1957.39
He described a crico-hyoidopexia in two patients withtube-dependent OPD secondary to laryngeal trauma. Hisprocedure utilized fascia lata to elevate the cricoid carti-lage to the greater cornu of the hyoid bone bilaterally.By elevating the larynx, Dr. Meurman was able toimprove swallowing function in both of these individu-als. In 1959, Edgerton and McKee and DesPrez andKiehn both described the use of laryngeal suspension insurgical reconstruction of large oral cavity tumors.40,41
In 1968, Bocca et al. described suspension of the larynxto the hyoid remnant in persons undergoing supraglotticlaryngectomy.42 In 1969, Jabaley and Hoopes describedvarious techniques of laryngeal suspension to improveswallowing function in three individuals with dysphagiaafter surgical treatment of squamous cell carcinoma ofthe tongue and floor of mouth.43 They reported 3 differ-ent techniques of laryngeal suspension: 1) elevating thethyroid cartilage to the mandibular symphysis, 2) pull-ing the base of the tongue forward and securing it to amandibular bone graft, and 3) suspending the hyoidbone to the anterior mandible. They concluded that thetechnique of laryngeal suspension to the mandibularsymphysis is effective in primary or secondary recon-struction of surgical defects. In 1971, Calcaterradescribed the successful use of a modification of the la-ryngeal suspension technique described by DesPrez andKiehn in four patients after supraglottic laryngectomy.44
He noted that postoperatively ‘‘the larynx has enlargedthe hypopharyngeal funnel and facilitated alimentarytransit.’’ All patients were able to tolerate a regular dietby mouth.
In 1976, Dr. Richard Goode extended the indica-tions for laryngeal suspension beyond supraglotticlaryngectomy.45 He used a slight modification of Calca-terra’s technique combined with cricopharyngeus musclemyotomy in 19 patients who underwent major resectionof head and neck cancer. He was able to elevate the lar-ynx 1.5 to 3 cm, although he noted that postoperative‘‘dropping’’ of the larynx was likely to occur. A tracheot-omy was performed in all cases. Swallowing wasdetermined to be adequate in only 50% of cases treatedwith the operation. Dr. Goode concluded, ‘‘laryngeal sus-pension is not a panacea to provide swallowing in thisdifficult group of cases.’’
Seeking to improve on his initial results, Hillel andGoode described a lateral laryngeal suspension in1983.46 They reported that lateral suspension of the lar-ynx to the mandibular condyle provided a greater degreeof laryngeal suspension than midline elevation. Theyachieved satisfactory swallowing results in 13 of 14patients (93%). Complications were relatively commonand included wound infection, fistula, VIIth nerve palsy,and vocal fold paralysis. In 1992, Herrmann reportedthe use of fascia lata to achieve laryngeal suspension inpatients with severe neurogenic dysphagia, and in 2008,Aviv et al. described the use of laryngeal suspension asan adjunct to myotomy and greater auricular to superiorlaryngeal microneurorrhaphy in two patients.47,48 In2008, Kos et al. reported the most comprehensive experi-
ence with laryngeal suspension combined with UESmyotomy in 17 patients with severe OPD.29 The meanfollow-up for their cohort was approximately 4 years.The surgery was deemed a complete success in 53% (9/17) of the patients, a partial success in 18% (3/17), and afailure in 29% (5/17). Because the surgery permanentlyopens the esophageal inlet, the authors cautionedagainst performing the procedure in patients with gas-troesophageal reflux disease, and citing perioperativeairway concerns, have recommended tracheotomy at thetime of surgery. Limitations of the procedure include itspotential to cause airway compromise, its inability toproduce dynamic on-demand opening, the risk of aspira-tion associated with esophagopharyngeal reflux, variablesuccess, and the possibility of failure over time.Although the laryngeal suspension is appealing, the useof this procedure as a treatment of dysphagia has beenlimited primarily to the reconstruction of surgicaldefects.41–46
The author hypothesized that manual control of theUES is possible. In order to expand the anterior-poste-rior diameter of the UES, the body must pull the larynxcranially. Direct manipulation should permit anteriordisplacement, and anterior traction on the cricoid carti-lage should open the UES, perhaps more efficiently thanvertical elevation. The author placed a suture aroundthe cricoid cartilage of patients being evaluated for la-ryngeal suspension. Anterior traction on the suture insome patients opened the UES to superphysiologicdimensions (Fig. 2). Based on these initial observationsthe author designed a device to externally and manuallycontrol the upper esophageal sphincter.
The purpose of this investigation was to evaluatethe effectiveness of manual control of the UES. The spe-cific aims were 1) to evaluate UES opening onfluoroscopy with anterior traction on a suture placedaround the anterior rim of the cricoid cartilage in per-sons with OPD, 2) to design and fabricate a swallowexpansion device that mechanically opens the UES, 3) toevaluate the ability of the Swallow Expansion Device(SED) to open the UES in fresh cadavers, and 4) to eval-uate the safety and efficacy of the SED in an ovinemodel of OPD.
MATERIALS AND METHODS
Effectiveness of the Cricoid Traction SuturePermission to conduct this aspect of the study was
approved by the University of California, Davis, Human Sub-jects Institutional Review Board. The records of all personshaving had a cricoid suture placed by the author were retro-spectively reviewed. Data regarding patient age, gender, anddysphagia etiology were recorded into a clinical database. Eachpatient had 2-0 monofilament nylon suture on a C-14 cuttingneedle (SN-75 8; Syneture, Norwalk, CT) placed around the an-terior rim of the cricoid cartilage under local anesthesia in theoffice (Fig. 3). Great care was taken to maintain the needle tipsalong the internal aspect of the cricoid cartilage, keeping thestitches submucosal.
After suture placement, patients underwent a dynamicfluoroscopic swallow study with and without anterior tractionon the suture. All studies were conducted in accordance with
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S4

the routine radiographic protocols approved by our institution.Equipment used included a properly collimated OEC MedicalSystems (Salt Lake City, UT) 9800 Radiographic/Fluoroscopicunit that provided a 63-kV, 1.2-mA type output for the full fieldof view mode (12-inch input phosphor diameter). In accordancewith our protocol, subjects swallowed a 1 mL, 3 mL, and 20 mLliquid bolus (EZ-PAQUE Barium Sulfate Suspension, 60% wt/vol; 4 1 % wt/wt; E-Z-EM, Inc., Westbury, NY) from a spoon orcup. Bolus size was measured with a syringe or graduated med-icine cup.
The primary outcome variable for this experiment wasUES opening (cm). The quantitative assessment of UES openinghas been reported previously but will be described briefly.49 Flu-oroscopy trials were recorded digitally using a Sony MD-1000DVD recorder (Sony Corp. of America, New York, NY). Anterior
traction on the suture was performed under fluoroscopy by theauthor. The suture was pulled anteriorly until additional forceresulted in no further anterior UES displacement (UES max) oruntil the patient reported discomfort with the procedure. Theforce required to maximally displace the UES was measuredwith a digital force gauge (Imada, Inc., Northbrook, IL). A digi-tal still image at the point of maximum UES opening with andwithout anterior traction on the cricoid suture was capturedand imported into ImageJ 1.41 for the Macintosh (NationalInstitutes of Health, Bethesda, MD) for the largest bolus admin-istered. The software was calibrated to the known length of a 2-cm fluoroscopic marker placed directly beneath the chin. Thedistance between the anterior and posterior pharyngoesopha-geal segment at the point of maximum UES opening wascalculated using the analysis software with ImageJ. All
Fig. 2. Manual control of the upper esophageal sphincter (UES). (a) Lateral fluoroscopic view. The UES is closed at rest (small arrows). Amarker is placed on the anterior rim of the cricoid cartilage (large arrow). (b) Lateral fluoroscopic view. The suture is placed around the an-terior rim of the cricoid cartilage (large arrow). Anterior traction on the suture pulls the larynx directly forward and opens the UES to super-physiologic proportions (small arrows). (c) Flexible office endoscopic view. There is no anterior traction on the cricoid suture. The UES isclosed (arrowheads). (d) Flexible office endoscopic view. Anterior traction is applied to the cricoid suture. The UES is open to superphysio-logic proportions (arrowheads) exposing the posterior cricoid region. C ¼ posterior lamina of cricoid cartilage; cp ¼ cricopharyngeusmuscle.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S5

recordings were made from deidentified, prerecorded, randomlypresented digital video with and without anterior traction ofthe suture with no knowledge of the presence or absence of ten-sion on the suture. All data were coded and recorded into SPSS17.0 for the Macintosh (SPSS Inc., Chicago, IL). Maximum UESopening with and without anterior traction on the suture wascompared with the paired sample t test and the nonparametricMann-Whitney U test.
Design and Fabrication of the SEDThis aspect of the study was supported by a technology
transfer grant from the University of California, Davis. Devicedevelopment was structured through a series of five phasegates. These phase gates included orientation and project kick-off (phase 0), empiric cadaver testing (phase 1), conceptdevelopment (phase 2), final concept refinement (phase 3), andfunctional prototype development (phase 4). To achieve thesegoals, the author partnered with an International Organizationfor Standardization (ISO) 9001:2000 certified medical devicedesign company (Product Development Technologies, Inc., Chi-cago, IL). At the conclusion of this aspect of the study, a looks-like/works-like functional prototype was developed for use inthe cadaver and animal testing. The device included an implantthat was secured to the cricoid cartilage and an external mag-netic device that attached to the internal device across intactskin. Pulling the external device forward mechanically opensthe UES.
Effectiveness of the SED in Fresh CadaversPermission to conduct this aspect of the study was
approved by the University of California, Davis donated bodyprogram. The internal component of the SED was affixed to thecricoid cartilage in 10 fresh cadavers. A 3-cm curvilinear inci-sion was made in the cervical skin over the region of thecricothyroid membrane. The strap muscles were divided in themidline and the cricoid cartilage was identified (Fig. 4a). Five2-0 monofilament nylon sutures (SN-75 8; Syneture) or five 2-0Gore-Tex sutures (2N05; Gore Medical, Flagstaff, AZ) were uti-lized to secure the implant to the anterior aspect of the cricoidcartilage. A horizontal mattress was utilized for the centersuture (Fig. 4b). Care was taken to maintain the needle tipsalong the internal aspect of the cricoid cartilage, keeping the
stitches submucosal. The strap muscles were reapproximatedover the device and the skin was closed in two layers (Fig. 4c,Fig. 4d). The primary outcome variable for this experiment wasUES opening. A Dedo laryngoscope (Pilling Surgical, Horsham,PA) was utilized to expose the UES. Opening of the sphincterwith and without use of the SED was measured with an Aero-sizer airway sizing device (Alveolus, Inc., Charlotte, NC). Fivepulls of the SED were performed for each cadaver. All datawere coded and recorded into SPSS 17.0 for the Macintosh(SPSS Inc.). The mean UES opening with and without anteriortraction on the SED was evaluated with the paired sample ttest and the nonparametric Mann-Whitney U test.
To evaluate safety of the implant on the cricoid, the exter-nal magnet of the SED was affixed to the internal implantacross the skin, and 5,000 pulls were performed. At the end ofthe safety trial the implant was removed and the skin, subcuta-neous tissue, muscle, and cartilage were inspected for damage.
The Safety and Efficacy of the SED in an OvineModel of OPD
This aspect of the investigation was approved by the Uni-versity of California, Davis Institutional Animal Care and UseCommittee (IACUC). It was supported by a development grantfrom Medtronic, Inc. (Minneapolis, MN). To assess the safety ofthe SED, eight Dorper cross wethers (castrated male sheep)were anesthetized and placed under general anesthesia. Anes-thesia was induced with ketamine/valium (10 mg/kg and 0.25mg/kg). A 4-cm curvilinear incision was performed at the levelof the cricoid cartilage. The strap muscles were separated in themidline, and the cricoid cartilage was identified. The internalaspect of the SED was secured to the cricoid cartilage (Fig. 5)with five 2-0 monofilament nylon sutures (SN-75 8; Syneture).The strap muscles were reapproximated over the implant, andthe incision was closed in two layers and allowed to heal for 4weeks.
After the 4-week healing period, the animals were lightlyrestrained once a week for 8 weeks. The handheld magneticexternal component of the SED was affixed to the internal SEDacross intact skin, and 5,000 sequential pulls on the devicewere performed per session to open the UES. The author chose5,000 pulls because this number greatly exceeds what would beutilized during routine use (approximately 50 swallows per
Fig. 3. Cricoid suture. (a) The monofilament suture is placed around the anterior rim of the cricoid cartilage. Anterior traction on the sutureopens the upper esophageal sphincter. (b) Close-up of the cricoid suture. c ¼ outline of the anterior rim of the cricoid cartilage visiblebetween the suture limbs.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S6

meal), and this is a number that is tolerated by a lightlyrestrained animal and feasible to perform during the allocatedtest period.
Two weeks after the last session of SED pulls, the animalswere euthanized with an intravenous injection of sodium pento-barbital (10 mL/100 lb), and the SED implant was removed.The cricoid cartilage was examined and evaluated for signs ofinfection and irritation. The implant site was grossly evaluatedfor damage to the cricoid cartilage, strap muscles, subcutaneoustissue, and overlying skin. A biopsy of the cricoid cartilage wasobtained with a #11 scalpel blade (Canemco Inc., Quebec, Can-ada) perpendicular to the cricoid surface. This was comparedhistologically to a biopsy taken from the proximal thyroid carti-lage lamina at a location distant to where the implant waslocated. For histologic examination, the cartilage specimenswere fixed in 10% neutral buffered formalin, decalcified with10% Na2 ethylenediaminetetraacetate, buffered at pH 7.4, andembedded in paraffin. Sections were cut to 5 lm thickness on a
rotary microtome and stained with toluidine blue and basicfuchsin stain in Epon-Araldite plastic. The primary outcomevariable for this experiment was damage to the cricoid cartilagecaused by use of the SED. To quantify cartilage damage, thedegree of infiltration of inflammatory cells and cartilagedestruction was classified according to the cartilage damagescale (CDS) as developed by Magari et al. and adapted byothers.50 The CDS ranges from a low of 0 (no cartilage damage)to a high of 3 denoting severe cartilage inflammation and dam-age. To provide a less-biased assessment of cartilage damage,the histologic CDS was determined by an examiner blind to thesite of cartilage biopsy (cricoid vs. laryngeal control site).
To assess the efficacy of the SED, the device was evaluatedunder fluoroscopy in the same animals used in the above-out-lined safety trial. One week prior to implant removal andeuthanasia, the animals were placed under general anesthesia.A deep level of anesthesia was achieved with inhaled isofluraneto suppress all swallowing activity. The animals were secured
Fig. 4. Placement of the swallow expansion device in a human cadaver. (a) The cricoid cartilage is exposed through a small skin incision.(b) The implant is secured with five 2-0 nylon sutures (SN-75 8; Syneture, Norwalk, CT) around the anterior rim of the cricoid cartilage.(c) The strap muscles are closed over the implant. (d) The skin is closed in two layers.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S7

in a 60� upright position (Fig. 6). A properly collimated fluoros-copy unit with a 12-inch input phosphor (OEC MedicalSystems) was then centered on the cervical region. An 18-French red rubber catheter (Bard Medical Division, Covington,GA) was placed through the nasal cavity and advanced underfluoroscopic guidance until the tip of the catheter was posi-tioned in the pharynx just proximal to the tip of the epiglottis.A total of 20 mL of thin liquid barium sulfate (E-Z-EM Inc.,Lake Success, NY) was delivered through the catheter tubingdirectly into the pharynx. The barium administration was per-formed under real-time fluoroscopy and digitally recorded. Allstudies were performed in the lateral view. To provide a less bi-ased assessment, two 20-mL swallow trials were performedwithout the SED employed, and two 20-mL swallow trials were
performed with anterior traction on the SED. The four studytrials were randomly ordered. The ability of the SED to openthe UES and reduce aspiration was evaluated. The primary out-come variable for this experiment was UES opening (cm). Thisvariable was calculated by a blinded investigator using theidentical technique described at the beginning of the Materialsand Methods section on the effectiveness of the cricoid suture.The secondary outcome variable for this experiment was elimi-nation of aspiration. Aspiration was defined as any bariumtraversing the vocal folds on fluoroscopy. The mean UES open-ing with and without anterior traction on the SED wasevaluated with the paired sample t test and the nonparametricMann-Whitney U test. The presence of aspiration with andwithout anterior traction on the SED was evaluated with the v2
test.
RESULTS
Effectiveness of the Cricoid Traction SutureThe cricoid traction suture was placed in six indi-
viduals with feeding tube-dependent OPD (Table I). Themean age of the cohort was 67 years (611). The etiologyof dysphagia was chemoradiation for head and neck car-cinoma (4/6) and stroke (2/6). All patients were feedingtube-dependent for 100% of their nutritional require-ments. The mean (6 standard deviation) maximum UESopening improved from 0.16 cm (60.14) without tractionon the suture to 0.52 cm (60.07) with traction on thesuture (P < .01). The amount of improved UES openingranged from 0.02 to 0.59 cm. Anterior traction on thesuture eliminated aspiration in three out of four patientswho aspirated without traction on the suture (Fig. 7).Patients adapted easily to autonomous control of theirUES with the suture. The mean force required to maxi-mally open the UES was 4.18 pound-force (60.68).Improvement in swallowing function was so pronouncedthat three patients went home with the suture in placeso that they could eat. The suture caused local skin irri-tation in all patients and was removed (range, 2–9 days)without complication.
Design and Fabrication of the SEDThe final prototype of the SED was designed with
an internal and an external component. The internalcomponent is a titanium-coated ferrous implant that issecured to the cricoid cartilage through a small skin
Fig. 5. Placement of the swallow expansion device in a sheep.The implant is secured to the ovine cricoid cartilage with five 2-0nylon sutures (SN-75 8; Syneture, Norwalk, CT).
Fig. 6. Ovine model of oropharyngeal dysphagia. The sheep issecured in a 60� upright position. A properly collimated fluoros-copy unit is centered on the cervical region. An 18-French redrubber catheter is placed through the nasal cavity and advancedunder fluoroscopic guidance until the tip of the catheter is posi-tioned in the pharynx just proximal to the tip of the epiglottis. Bar-ium trials are administered under fluoroscopy and digitallyrecorder in real time.
TABLE I.Opening of the UES With the Cricoid Suture.
Patient Diagnosis GenderAge(yr)
UESo(cm),
No Suture
UESo(cm),
With Suture
1 CA oropharynx M 81 0.09 0.49
2 Unknown primary M 72 0.10 0.53
3 Stroke F 51 0.08 0.48
4 Laryngeal CA M 74 0.22 0.54
5 CA oropharynx M 56 0.05 0.64
6 Stroke F 68 0.41 0.43
UES ¼ upper esophageal sphincter; UESo ¼ upper esophagealsphincter opening; CA ¼ cancer; M ¼ male; F ¼ female.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S8
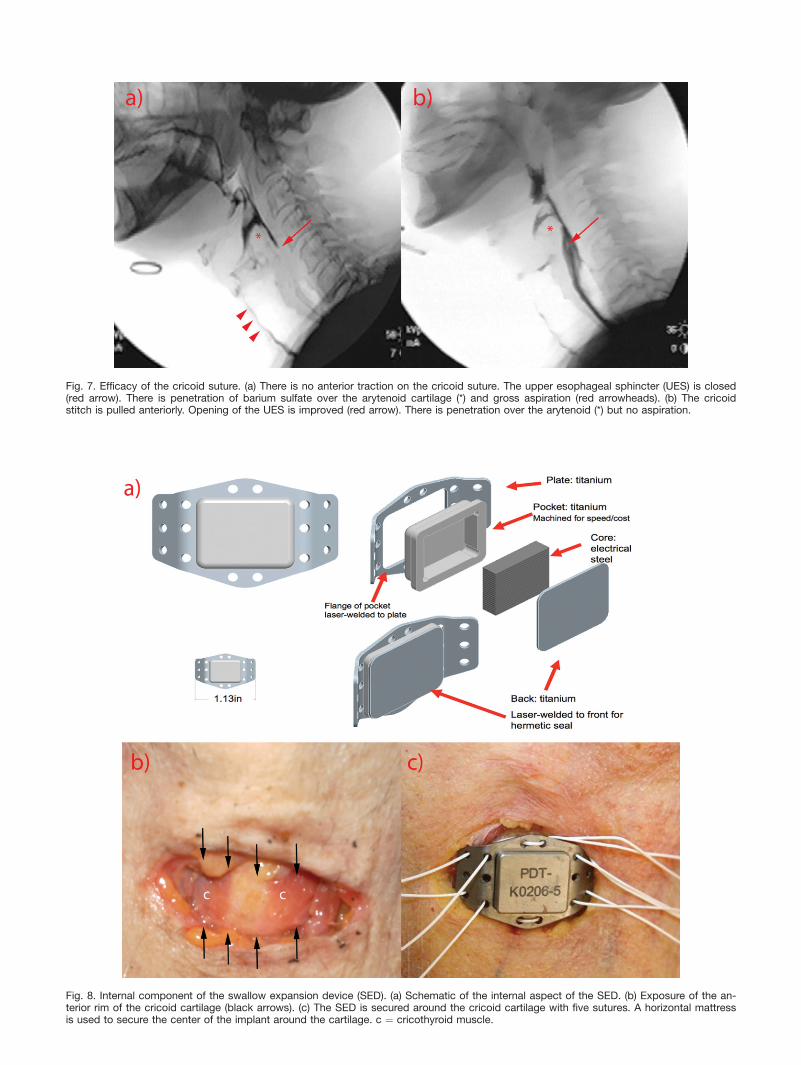
Fig. 7. Efficacy of the cricoid suture. (a) There is no anterior traction on the cricoid suture. The upper esophageal sphincter (UES) is closed(red arrow). There is penetration of barium sulfate over the arytenoid cartilage (*) and gross aspiration (red arrowheads). (b) The cricoidstitch is pulled anteriorly. Opening of the UES is improved (red arrow). There is penetration over the arytenoid (*) but no aspiration.
Fig. 8. Internal component of the swallow expansion device (SED). (a) Schematic of the internal aspect of the SED. (b) Exposure of the an-terior rim of the cricoid cartilage (black arrows). (c) The SED is secured around the cricoid cartilage with five sutures. A horizontal mattressis used to secure the center of the implant around the cartilage. c ¼ cricothyroid muscle.

incision (Fig. 8). Titanium implants have precedent inbiomedical devices and are used frequently in maxillo-facial, mandibular, and orbital reconstruction plates.Titanium is of a low density, strong, corrosion resistant,and highly biocompatible. It is an optimal material tohouse the iron core that is needed to provide magneticattraction to the external component of the device.Placement of the implant on the cricoid cartilage isminimally invasive and can be performed through asmall skin incision with local anesthesia (Fig. 8b, Fig.8c). The procedure is technically simple and theimplant can be removed without difficulty. The skinand strap muscles are closed over the implant andallowed to heal.
The external component of the SED houses a mag-net that can be attracted to the implant across intactskin (Fig. 9). The external device is utilized only duringswallowing. The patient places the external device onthe anterior cervical skin. Squeezing the handles of theexternal device delivers the magnet to the surfaceattracting it to the implant (Fig. 9b). The size of theexternal magnet and ferrous implant was based on theclinical dimensions of cadaveric cricoid cartilagesobtained from the author’s laboratory and from theresults of the force testing in the human suture experi-ments. Pulling the external device forward duringdeglutition mechanically opens the UES (Fig. 9c).Releasing the handles frees the magnet from the inter-nal implant (Fig. 9a). The distance of the magnet fromthe base of the housing can be adjusted to control attrac-tive force between the external device and implant (Fig.9a).
Experience with the cricoid suture suggests thatpatients readily adapt to autonomous control of theirUES. The device was designed so that it would be simi-lar in size to an electrolarynx (OptiVox; Smith Medical,
Fig. 9. External component of the swallow expansion device(SED). (a) The handles (h) are released and the magnet (m) isrecessed within the housing. When the device is placed on theskin with the handles released there is minimal magnetic attractiveforce with the internal SED implant. The device may be placed onor removed from the cervical skin. The screw (black arrow) can beadjusted to fine-tune the amount of magnetic force required. Thequantity of attractive force that is necessary will vary according toindividual patient skin thickness, amount of subcutaneous fat,muscle thickness, and tissue pliability. (b) The handles (h) aredepressed and the magnet (m) is delivered to the base of thehousing. This engages magnetic attractive force with the internalSED implant. (c) SED usage scenario. The external SED is placedon the anterior cervical skin and the handles are depressed. Theuser pulls the device forward and opens the upper esophagealsphincter. (d) Image of the functional external SED prototype.
Fig. 10. The effect of the swallow expansion device (SED) on the cricoid cartilage of a human cadaver. (a) The cricoid cartilage prior to SEDimplantation. (b) The cricoid cartilage after 5,000 pulls of the SED. There is no gross damage.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S10

Watford, UK). Patients in need of electronic speech haveadapted well to placing an electrolarynx on the neck,and preliminary experience suggests that a similardegree of manual dexterity is necessary to control theSED.
Effectiveness of the Swallow Expansion Devicein Fresh Cadavers
The SED was placed on the cricoid cartilage of 10fresh cadavers. The mean time required for device im-plantation was 12 minutes (64). Fifty thousand anteriorpulls of the device were performed for safety evaluation.There was no gross damage to the underlying cricoidcartilage or overlying skin upon device explantation(Fig. 10). The device opened the UES from a mean base-line of 0.00 mm (60.00) to a mean opening of 11.6 mm(62.18) (Table II, Fig. 11; P < .001). This is considerablygreater than normal gender and age-matched UES open-ing with a 3 mL bolus (5.2 mm, P < .001).
The Safety and Efficacy of the SED in an OvineModel of OPD
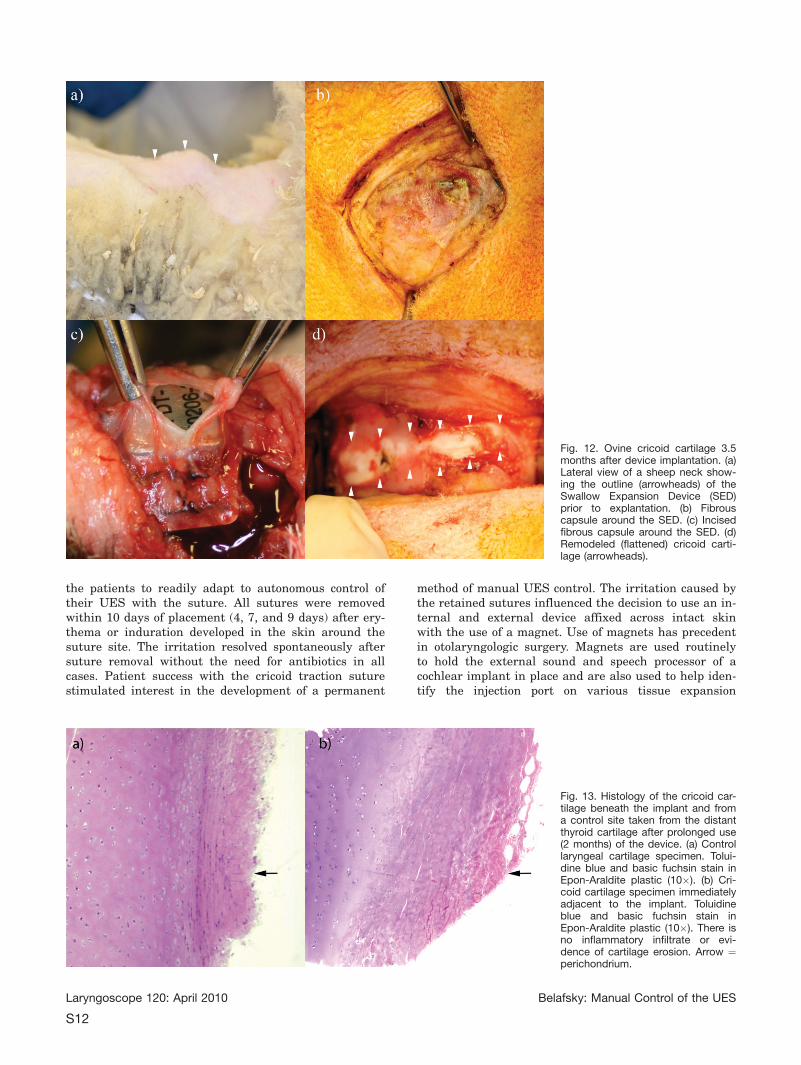
The SED was placed on the cricoid cartilage of eightsheep (Fig. 5). Five thousand pulls were performed oneach animal weekly for 4 weeks. At the time of explanta-tion, a thick fibrous capsule was evident around theimplant (Fig. 12a, Fig. 12b, Fig. 12c). There was grossremodeling of the cricoid cartilage with prolonged use ofthe SED. The angle of the anterior rim of the cricoid car-tilage flattened and adapted to the shape of the implant(Fig. 12d). There was no gross damage to the overlyingskin or strap muscles nor was there any cricoid cartilagefracture caused by prolonged use of the SED. One of theanimals developed cervical erythema and swelling. Anabscess was identified, and the grossly infected implantwas removed prematurely 3 weeks after implantation.The animal recovered completely without incident. Themean CDS was 0.0 (60.0) for the cricoid implant siteand 0.0 (60.0) for the control laryngeal cartilage site(Fig. 13; P >.05). Under fluoroscopy the device openedthe UES from a mean baseline of 0.15 cm (60.07) to amean maximum opening of 1.42 cm (60.41) (Table III;Fig. 14; P < .001). All of the animals (7/7) aspiratedwithout anterior traction on the SED. The device elimi-nated 100% of barium sulfate aspiration (Fig. 15).
DISCUSSIONThe data from this investigation suggest that man-
ual control of the UES is possible. Anterior tractionsuture on the cricoid cartilage in a cohort of individualswith tube-dependent OPD improved UES opening by0.36 cm (60.19) (P < .01). Aspiration was eliminated in75% (3/4). All of these patients had failed treatmentwith extensive swallowing therapy. Three patientsdesired to leave the suture in place so that they couldenjoy oral intake at home. The patients participated in abrief biofeedback session under real-time videofluoro-scopy by the speech language pathologist. Theimmediate feedback provided by the fluoroscopy allowed
TABLE II.Opening of the UES in Fresh Cadavers With the SED.
CadaverNumber Gender
Age(yr)
Cause ofDeath
UES OpeningWith SED (cm)
1 F 60 Unknown 1.00
2 F 86 Stroke 0.80
3 F 96 Unknown 1.11
4 M 91 Unknown 1.33
5 M 72 GI bleed 1.07
6 M 79 Unknown 1.07
7 F 58 Breast CA 1.27
8 M 79 Prostate CA 1.47
9 F 87 RF 1.00
10 M 75 Lung CA 1.47
UES ¼ upper esophageal sphincter; SED ¼ Swallow Expansion De-vice; F¼ female; M ¼ male; GI ¼ gastrointestinal; CA ¼ cancer; RF ¼ respi-ratory failure.
Fig. 11. Direct endoscopic view of the upper esophageal sphincter (UES) with and without anterior traction on the swallow expansion de-vice (SED). (a) No anterior traction on the SED. The UES is closed (white arrowheads). (b) The SED is pulled anteriorly. The UES is openedto superphysiologic proportions (white double arrow). VF ¼ vocal folds. CP ¼ cricopharyngeus muscle.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S11
the patients to readily adapt to autonomous control oftheir UES with the suture. All sutures were removedwithin 10 days of placement (4, 7, and 9 days) after ery-thema or induration developed in the skin around thesuture site. The irritation resolved spontaneously aftersuture removal without the need for antibiotics in allcases. Patient success with the cricoid traction suturestimulated interest in the development of a permanent
method of manual UES control. The irritation caused bythe retained sutures influenced the decision to use an in-ternal and external device affixed across intact skinwith the use of a magnet. Use of magnets has precedentin otolaryngologic surgery. Magnets are used routinelyto hold the external sound and speech processor of acochlear implant in place and are also used to help iden-tify the injection port on various tissue expansion
Fig. 12. Ovine cricoid cartilage 3.5months after device implantation. (a)Lateral view of a sheep neck show-ing the outline (arrowheads) of theSwallow Expansion Device (SED)prior to explantation. (b) Fibrouscapsule around the SED. (c) Incisedfibrous capsule around the SED. (d)Remodeled (flattened) cricoid carti-lage (arrowheads).
Fig. 13. Histology of the cricoid car-tilage beneath the implant and froma control site taken from the distantthyroid cartilage after prolonged use(2 months) of the device. (a) Controllaryngeal cartilage specimen. Tolui-dine blue and basic fuchsin stain inEpon-Araldite plastic (10�). (b) Cri-coid cartilage specimen immediatelyadjacent to the implant. Toluidineblue and basic fuchsin stain inEpon-Araldite plastic (10�). There isno inflammatory infiltrate or evi-dence of cartilage erosion. Arrow ¼perichondrium.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S12

devices. The magnet in the external aspect of the SEDwas effective at opening the UES. The mean UES open-ing with the SED was 1.16 cm in cadavers and 1.42 cmin sheep. This is more than twice the mean UES openingin normal individuals with a 3 mL bolus (0.51 cm).2
In order to open the UES, the body must elevatethe larynx. The hyoid bone serves as a fulcrum so thatthe suprahyoid musculature (geniohyoid, mylohyoid, thy-rohyoid, digastric, and stylohyoid) can elevate the larynxanteriorly and superiorly off of the spine. The elevationprovided by the body in normal individuals is notadequate in and of itself to open the UES. Opening doesnot occur until the elastic sphincter is distended by theadvancing food bolus.32 Opening of the UES with bolusdistention (phase III of UES opening) relies upon pha-ryngeal and lingual peristalsis to push the bolusthrough the narrowed sphincter. Patients with tube-de-pendent OPD secondary to lingual and pharyngealweakness do not possess the ability to open the UESbecause they lack the ability to propel a bolus and dis-
tend the sphincter. Based on the Pythagorean theorem,a surgeon would have to elevate the larynx 15.18 cm to-ward the mandibular symphysis and beyond in order toobtain the PES opening the author achieved with theSED by pulling the UES directly anteriorly (Fig. 16;UESo). This is analogous to elevating the larynx to theapproximate level of the nasal tip. This degree of perma-nent elevation is not possible. Laryngeal suspensionsurgery is capable of elevating the larynx 3 cm.45
There are several potential advantages to manualcontrol of the UES with the SED over traditional laryn-geal suspension surgery. Placement of the implant onthe cricoid is minimally invasive and can be performedthrough a small skin incision with local anesthesia inless than 15 minutes. The procedure is technically sim-ple and can be performed by a clinician with minimalinstruction and no subspecialty training. A perioperativetracheotomy is not necessary. If the device gets infectedor needs to be explanted to perform an imaging study itcan be removed easily. Manual control of the UES withthe SED is a dynamic process. The larynx does not needto be permanently secured to the mandible. The patientcan open the UES on demand. Airway protection fromesophagopharyngeal reflux is not compromised. Finally,the SED resulted in superphysiologic opening. Pullingthe cricoid anteriorly is more efficient at opening theUES than elevating the larynx anteriorly and superiorly.We anticipate that when human trials with the SEDcommence, patients will require a brief instruction ses-sion with the speech language pathologist under real-time fluoroscopy. This will assure swallowing safety withthe device and educate the patient on safe and properuse. Preliminary experience with the cricoid suture sug-gests that this may be a 10-minute addition to thetraditional videofluoroscopic swallowing study.
Potential limitations of the SED include the possi-bility of infection and damage to the cricoid cartilage.There was no gross damage to the cricoid cartilage in
TABLE III.Opening of the UES in Sheep with the SED.
SheepNo. Gender
Weight(lb)
UES Openingat Rest(cm)
UES OpeningWith SED
(cm)
1 M 76 0.09 1.44
2 M 77 0.08 N/A
3 M 74 0.24 2.17
4 M 75 0.14 1.22
5 M 75 0.13 1.03
6 M 81 0.11 1.39
7 M 77 0.24 1.73
8 M 104 0.08 0.99
UES ¼ upper esophageal sphincter, SED ¼ Swallow Expansion De-vice; M ¼ male; N/A ¼ not available; device got infected and was removedbefore testing.
Fig. 14. Fluoroscopic view of opening of the ovine upper esophageal sphincter (UES) with the swallow expansion device (SED). (a) TheUES is closed without use of the SED (arrow). (b) The external component of the SED is affixed to the implant across intact skin (arrow).Anterior traction on the SED opens the UES to superphysiologic proportions.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S13

our cadaver or animal experiments in over 350,000 pullsof the device. Remodeling of the cricoid cartilage didoccur with prolonged use in sheep (Fig. 12d). This didnot narrow the lumen of the subglottic airway nor did itcause any noticeable airway compromise. Infectionnecessitated early removal in one animal (12.5%). Cervi-cal erythema and swelling at the implant site wasnoticed in the second postoperative week. The animalwas treated with broad spectrum antibiotics for 7 daysand the signs of infection did not improve. A localizedabscess was identified and the implant was removed inthe third postoperative week. The animal recoveredwithout incident. There was no histologic evidence ofdamage or infection to the cricoid cartilage in this ani-mal. The majority of people who benefited from thecricoid suture and who would likely benefit from theSED are irradiated head and neck cancer patients. Infec-tion and cricoid damage are of even greater concern inthis population. Safety of the device in cadavers and innonirradiated sheep is not sufficient to conclude that thedevice is safe in irradiated, living individuals. Becauseof the iron core, the device would need to be removedprior to a magnetic resonance imaging study. This isanother concern, specifically in the cancer and strokepopulations.
Another limitation of this investigation is the mod-est sample size. The cricoid suture was studied in sixpatients. The initial excitement with the therapeutic ef-ficacy of the suture was tempered by the fact that allpatients sent home with the stitch in place developedlocal irritation and had to have the suture removedwithin 10 days time. This experience restricted forth-coming suture placement and focused attention ondevelopment of the SED. The sample size for thecadaver study was 10 subjects, and the animal trial waslimited to eight subjects. The primary analytic goal of
these investigations was to evaluate the ability of theSED to open the UES. Although the sample size of theseexperiments was limited, pretrial power calculationsrevealed that these studies had 85% power to detect a0.6 standard deviation improvement in UES opening.
Fig. 15. Elimination of aspiration with use of the swallow expansion device (SED) in the ovine model of oropharyngeal dysphagia. (a) A totalof 20 mL of barium is instilled through the catheter into the pharynx. The upper esophageal sphincter (UES) opening (white arrow) with noanterior traction of the SED (black arrow) is 0.09 cm. There is gross penetration and aspiration of the barium bolus (white arrowheads). (b)Manual control with anterior traction of the SED (black arrow) has increased the UES opening (white arrow) to 1.44 cm. The penetrationand aspiration is eliminated.
Fig. 16. Laryngeal elevation diagram. The Pythagorean theoremstates that, in a right triangle, the area of the square of the hypot-enuse (c2) is equal to the sum of the squares of the other two legsof the triangle (a2þ b2). Based on this theorem, a surgeon wouldhave to elevate the larynx 15.18 cm toward the mandibular sym-physis (c) in order to obtain the upper esophageal sphincter open-ing (UESo) we achieved with the SED by pulling the cricoiddirectly anterior with the swallow expansion device.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S14

The primary experimental goal was met in all threeexperiments. The data provide strong evidence that an-terior traction of the cricoid cartilage with suture orwith the assistance of the SED opens the UES. The sec-ondary goal of these studies was to evaluate the safetyof the device. The initial sample size calculation for thesheep study determined that the experiment had an88% chance of identifying at least one adverse event,such as infection that occurred in 10% or more of sheepwith the SED implant. One infection necessitating earlyimplant removal was experienced. Now that efficacy hasbeen established, future investigation is necessary todetermine the true cumulative incidence of implantinfection in a larger population of living animals.
CONCLUSIONManual control of the upper esophageal sphincter is
possible. A simple anterior traction suture placed aroundthe anterior aspect of the cricoid cartilage improvedUES opening by 0.36 cm (60.19) in a cohort of dysphagicpatients. An internal implant on the cricoid cartilageaffixed to an external magnet across intact skin openedthe UES of fresh cadavers and living sheep to superphy-siologic proportions.
AcknowledgmentsWith eternal gratitude for your unwavering support,
encouragement, friendship, and mentorship: Drs. Markand Robert Belafsky, Dr. Gregory Postma, Dr. Jamie Kouf-man, Dr. Robert Sataloff, Dr. Paul Donald, Dr. Hilary Bro-die, Dr. Gregory Farwell, Dr. Rebecca Leonard, Dr.Catherine Rees, Dr. Jacquie Allen, Jan Pryor, CherylWhite, Shannon Whitney, Rebecca Anson, Sonia Blue, TodStoltz, Joel Delman, and Dr. Sheri Belafsky.
BIBLIOGRAPHY
1. Tucker HM. The Larynx. New York: Thieme Medical Pub-lishers; 1987:21–32.
2. Bloem BR, Lagaay AM, van Beek W, et al. Prevalence ofsubjective dysphagia in community residents aged over87. BMJ 1990;300:721–722.
3. Schroeder PL, Richter JE. Swallowing disorders in the el-derly. Semin Gastrointest Dis 1994;5:154–165.
4. Nguyen NP, Moltz CC, Frank C, et al. Dysphagia followingchemoradiation for locally advanced head and neck can-cer. Ann Oncol 2004;15:383–388.
5. Nguyen NP, Frank C, Moltz CC, et al. Aspiration rate fol-lowing chemoradiation for head and neck cancer: anunderreported occurrence. Radiother Oncol 2006;80:302–306.
6. Meng NH, Wang TG, Lien IN. Dysphagia in patients withbrainstem stroke: incidence and outcome. Am J PhysMed Rehabil 2000;79:170–175.
7. Siebens H, Trupe E, Siebens A, et al. Correlates and conse-quences of eating dependency in institutionalized elderly.J Am Geriatr Soc 1986;34:192–198.
8. Rosenbek JC, Jones HN. Dysphagia in Movement Disorders.San Diego, CA: Plural Publishing; 2009:115–124.
9. Robbins J, Langmore S, Hind JA, et al. Dysphagia researchin the 21st century and beyond: proceedings from Dys-phagia Experts Meeting, August 21, 2001. J Rehabil ResDev 2002;39:543–548.
10. Lovell SJ, Wong HB, Loh KS, et al. Impact of dysphagia onquality of life in nasopharyngeal carcinoma. Head Neck2005;27:864–872.
11. Maclean J, Cotton S, Perry A. Dysphagia following a totallaryngectomy: the effect on quality of life, functioning,and psychological well-being. Dysphagia 2009;24:314–321.
12. Eslick GD, Talley NJ. Dysphagia: epidemiology, risk factorsand impact on quality of life—a population-based study.Aliment Pharmacol Ther 2008;27:971–979.
13. Ekberg O, Hamdy S, Woisard V, et al. Social and psycholog-ical burden of dysphagia: its impact on diagnosis andtreatment. Dysphagia 2002;17:139–146.
14. Schmidt J, Holas M, Halvorson K, Reding M. Videofluoro-scopic evidence of aspiration predicts pneumonia anddeath but not dehydration following stroke. Dysphagia1994;9:7–11.
15. Croghan JE, Burke EM, Caplan S, Denman S. Pilot study of12-month outcomes of nursing home patients with aspira-tion on videofluoroscopy. Dysphagia 1994;9:141–146.
16. Callahan CM, Buchanan NN, Stump TE. Healthcare costsassociated with percutaneous endoscopic gastrostomyamong older adults in a defined community. J Am GeriatrSoc 2001;49:1525–1529.
17. Blumenfeld L, Hahn Y, Lepage A, Leonard R, Belafsky PC.Transcutaneous electrical stimulation versus traditionaldysphagia therapy: a nonconcurrent cohort study. Otolar-yngol Head Neck Surg 2006;135:754–757.
18. Mepani R, Antonik S, Massey B, et al. Augmentation ofdeglutitive thyrohyoid muscle shortening by the ShakerExercise. Dysphagia 2009;24:26–31.
19. Logemann JA. Treatment of oral and pharyngeal dyspha-gia. Phys Med Rehabil Clin N Am 2008;19:803–816, ix.
20. Robbins KT, Bowman JB, Jacob RF. Postglossectomy deglu-titory and articulatory rehabilitation with palatal aug-mentation prostheses. Arch Otolaryngol Head Neck Surg1987;113:1214–1218.
21. Wang AY, Kadkade R, Kahrilas PJ, Hirano I. Effectivenessof esophageal dilation for symptomatic cricopharyngealbar. Gastrointest Endosc 2005;61:148–152.
22. Zaninotto G, Marchese Ragona R, Briani C, et al. The roleof botulinum toxin injection and upper esophagealsphincter myotomy in treating oropharyngeal dysphagia.J Gastrointest Surg 2004;8:997–1006.
23. Kelly JH. Management of upper esophageal sphincter disor-ders: indications and complications of myotomy. Am JMed 2000;108(suppl 4a):43S–46S.
24. Mok P, Woo P, Schaefer-Mojica J. Hypopharyngeal pharyn-goplasty in the management of pharyngeal paralysis: anew procedure. Ann Otol Rhinol Laryngol 2003;112:844–852.
25. Woodson G. Cricopharyngeal myotomy and arytenoidadduction in the management of combined laryngeal andpharyngeal paralysis. Otolaryngol Head Neck Surg 1997;116:339–343.
26. Flint PW, Purcell LL, Cummings CW. Pathophysiology andindications for medialization thyroplasty in patients withdysphagia and aspiration. Otolaryngol Head Neck Surg1997;116:349–354.
27. Fujimoto Y, Hasegawa Y, Yamada H, Ando A, Nakashima T.Swallowing function following extensive resection of oralor oropharyngeal cancer with laryngeal suspension andcricopharyngeal myotomy. Laryngoscope 2007;117:1343–1348.
28. Wirth D, Kern B, Guenin MO, et al. Outcome and qualityof life after open surgery versus endoscopic stapler-assisted esophagodiverticulostomy for Zenker’s diverticu-lum. Dis Esophagus 2006;19:294–298.
29. Kos MP, David EF, Aalders IJ, Smit CF, Mahieu HF. Long-term results of laryngeal suspension and upper esopha-geal sphincter myotomy as treatment for life-threateningaspiration. Ann Otol Rhinol Laryngol 2008;117:574–580.
30. Caspi A, Dorn JD, McClure KH, et al. Feasibility study of aretinal prosthesis: spatial vision with a 16-electrodeimplant. Arch Ophthalmol 2009;127:398–401.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S15

31. DeMichele GA, Troyk PR, Kerns DA, Weir R. An implant-able myoelectric sensor based prosthesis control system.Conf Proc IEEE Eng Med Biol Soc 2006;1:2970–2973.
32. Jacob P, Kahrilas PJ, Logemann JA, Shah V, Ha T. Upperesophageal sphincter opening and modulation duringswallowing. Gastroenterology 1989;97:1469–1478.
33. Lang IM, Layman F, Hogan WJ, Dodds WJ, Shaker R.Characterization and quantification of a pharyngo-UEScontractile reflex in cats. Am J Physiol 1994;267(6 pt 1):G972–G983.
34. Freiman JM, EI-Sharkawy TY, Diamant NE. Effect of bilat-eral vagosympathetic nerve blockade on response of thedog upper esophageal sphincter (UES) to intraesophagealdistention and acid. Gastroenterology 1981;81:78–84.
35. Shaker R, Ren J, Xie P, Lang IM, Bardan E, Sui Z. Charac-terization of the pharyngo-UES contractile reflex inhumans. Am J Physiol 1997;273(4 pt 1):G854–G858.
36. Cook IJ, Dent J, Shannon S, Collins SM. Measurement ofupper esophageal sphincter pressure. Effect of acute emo-tional stress. Gastroenterology 1987;93:526–532.
37. Sasaki CT, Kim YH, Sims HS, Czibulka A. Motor innerva-tion of the human cricopharyngeus muscle. Ann Otol Rhi-nol Laryngol 1999;108:1132–1139.
38. Buchholz DW. Cricopharyngeal myotomy may be effectivetreatment for selected patients with neurogenic oropha-ryngeal dysphagia. Dysphagia 1995;10:255–258.
39. Meurman Y. Suspension of the larynx with fascial strips onthe hyoid bone for removal of deglutition disorders aftertrauma [in German]. Arch Ohren Nasen Kehlkopfbeilkd1957;172:96–104.
40. Edgerton MT, McKee DM. Reconstruction with loss of thehyomandibular complex in excision of large cancers.AMA Arch Surg 1959;78:425–436.
41. DesPrez JD, Kiehn CL. Methods of reconstruction followingresection of anterior oral cavity and mandible for malig-nancy. Plast Reconstr Surg Transplant Bull 1959;24:238–249.
42. Bocca E, Pignataro O, Mosciaro O. Supraglottic surgery ofthe larynx. Ann Otol Rhinol Laryngol 1968;77:1005–1026.
43. Jabaley ME, Hoopes JE. A simple technique for laryngealsuspension after partial or complete resection of the hyo-mandibular complex. Am J Surg 1969;118:685–690.
44. Calcaterra TC. Laryngeal suspension after supraglottic lar-yngectomy. Arch Otolaryngol 1971;94:306–309.
45. Goode RL. Laryngeal suspension in head and neck surgery.Laryngoscope 1976;86:349–355.
46. Hillel AD, Goode RL. Lateral laryngeal suspension: a newprocedure to minimize swallowing disorders followingtongue base resection. Laryngoscope 1983;93:26–31.
47. Herrmann IF. Surgical solutions for aspiration problems.J Jpn Bronchoesophageal Soc 1992;43:72–79.
48. Aviv JE, Mohr JP, Blitzer A, Thomson JE, Close LG. Resto-ration of laryngopharyngeal sensation by neural anasto-mosis. Arch Otolaryngol Head Neck Surg 1997;123:154–160.
49. Leonard R, MackenzieS. Dynamic swallow studies: mea-surement techniques. In: Leonard R, Kendall K, eds. Dys-phagia Assessment and Treatment Planning: A TeamApproach. San Diego, CA: Plural Publishing; 2008:265–294.
50. Magari K, Nishigaki F, Sasakawa T, et al. Anti-arthriticproperties of FK506 on collagen-induced arthritis in rats.Inflamm Res 2003;52:524–529.
Laryngoscope 120: April 2010 Belafsky: Manual Control of the UES
S16