alter obstructive lung disease 2.ppt - c.ymcdn.comc.ymcdn.com/sites/€¦ · therapeutic options:...
TRANSCRIPT

Obstructive Lung DiseaseMichael Alter, MD FCCP, FAASM
Department of Pulmonary/Critical Care/SleepHealthPartners Medical GroupAssistant Professor of Medicine
University of Minnesota Medical School
COPD
•Natural history•Pathophysiology•Diagnosis •Out‐patient management• In‐patient management
COPD
•Natural history•Pathophysiology•Diagnosis •Out‐patient management•In‐patient management

Case 1
•78 y.o. male•COPD•Current smoker•On no therapy•FEV1 70%•Can walk without any limitation, no respiratory symptoms
•SpO2 94% on RA
•Advair 250/50•Oxygen therapy•Albuterol prn•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab
Case 2
•82 y.o. female•COPD•Former smoker•Daily cough and wheezing
•On Albuterol•FEV1 30%• Limited to ADLs•SpO2 87% on RA
•Advair 250/50•Prn Albuterol•Oxygen therapy•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab

Case 3
•68 y.o. male•COPD•Former smoker•Daily cough and wheezing
•On Spiriva•FEV1 60%•Worsening SOB over last year
•SpO2 90% on RA
•Advair 250/50•Prn Albuterol•Oxygen therapy•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab

Burden of COPD
• Increasing Global Prevalence4th-leading cause of death worldwide12th-leading cause of disabilityBy 2020: 3rd-leading cause of death, 5th-leading cause of disabilityAnnual cost: $40 billion
Murray CJL, Lopez AD, Harvard University Press, 1996
COPD is a major public health problem in the US• 5% of adult population (1 in 20 adults)
• 16 to 20 million cases
• 4th leading cause of death: 112,000 deaths annually
• 2nd leading cause of disability
• In 2002 more women in US died of COPD then men
Burden of COPD
Michaud CM, et al. JAMA. 2002

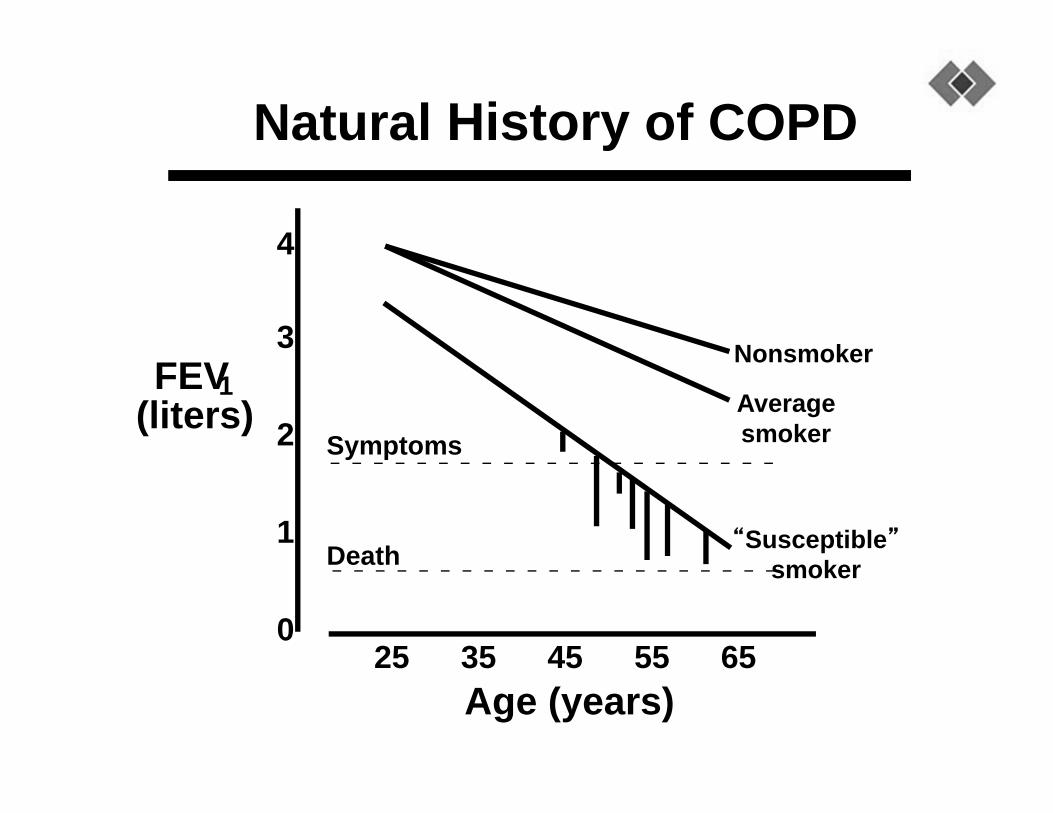
Natural History of COPD
25 35 45 55 65Age (years)
4
3
2
1
0
Symptoms
Death
Nonsmoker
Averagesmoker
“Susceptible”smoker
FEV1(liters)
Natural History of COPD
25 35 45 55 65Age (years)
4
3
2
1
0
Symptoms
Death
Nonsmoker
Averagesmoker
“Susceptible”smoker
FEV1(liters)

Global Initiative for Chronic Obstructive Lung Disease (GOLD)
•Launched in 1997 • in collaboration with the NHLBI, NIH and the WHO
•committees of experts around the world

Global Initiative for Chronic Obstructive Lung Disease (GOLD)
•Guidelines updated January 2015•Global strategy for the diagnosis, management, and prevention of COPD
•GOLD Website: www.goldcopd.org

GOLD Definition of COPD
2015 goldcopd.orgCOPD.com
“A common preventable and treatable disease, is characterized by airflow limitation that is usually
progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to
noxious particles or gases.”

Causes of COPD not caused by tobacco smoke•Not all patient’s with COPD smoke ~ 15%•Need to entertain COPD in non‐smokers if the shoe fits‐ cough, wheeze, SOB, dyspnea, hyperinflation on CXR

Risk Factors for COPD
GenesExposure to particlesTobacco smokeOccupational dusts, organic and
inorganic Indoor air pollution from heating
and cooking with biomass in poorly ventilated dwellings
Outdoor air pollution
Tager et al. Am Rev Resp Dis. 1988;

Causes of COPD not caused by tobacco smoke
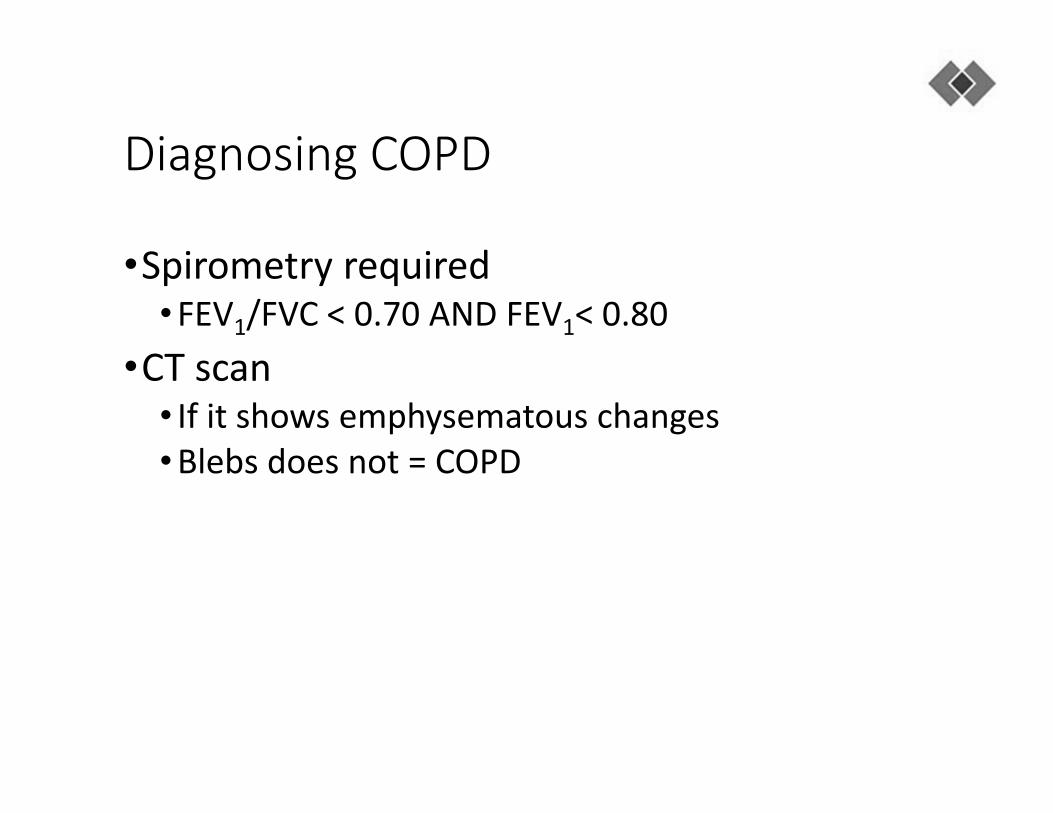
Diagnosing COPD
•Spirometry required•FEV1/FVC < 0.70 AND FEV1< 0.80
•CT scan• If it shows emphysematous changes•Blebs does not = COPD
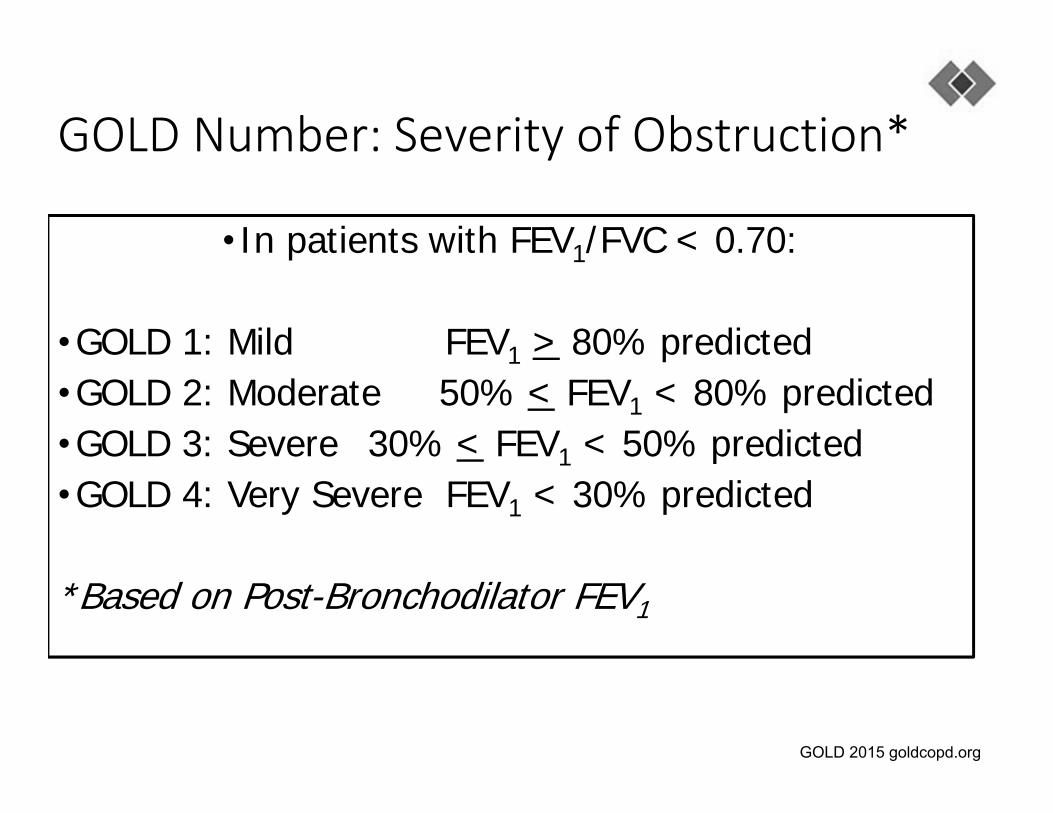
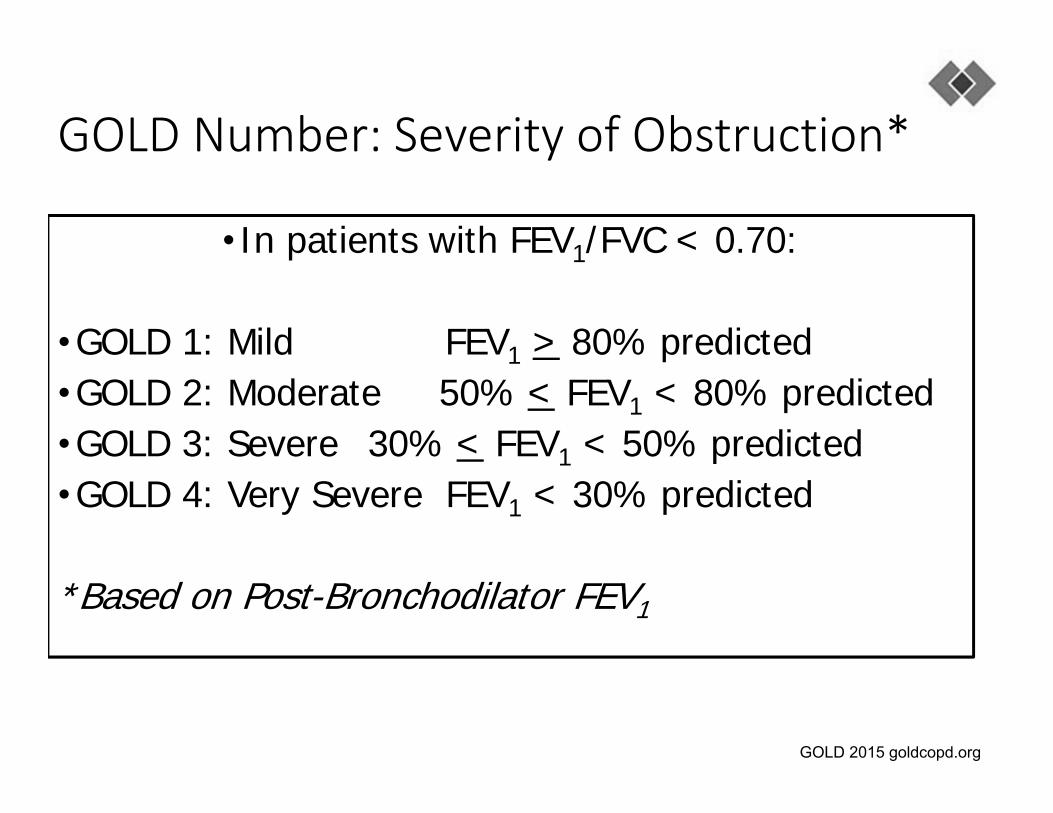
GOLD Number: Severity of Obstruction*
• In patients with FEV1/FVC < 0.70:
•GOLD 1: Mild FEV1 > 80% predicted •GOLD 2: Moderate 50% < FEV1 < 80% predicted•GOLD 3: Severe 30% < FEV1 < 50% predicted•GOLD 4: Very Severe FEV1 < 30% predicted
*Based on Post-Bronchodilator FEV1
GOLD 2015 goldcopd.org
GOLD Number: Severity of Obstruction*
• In patients with FEV1/FVC < 0.70:
•GOLD 1: Mild FEV1 > 80% predicted •GOLD 2: Moderate 50% < FEV1 < 80% predicted•GOLD 3: Severe 30% < FEV1 < 50% predicted•GOLD 4: Very Severe FEV1 < 30% predicted
*Based on Post-Bronchodilator FEV1
GOLD 2015 goldcopd.org

Spirometry

Mortality based on GOLD Severity
Hurst JR, et al. N Engl J Med 2010Decramer M, et al. (UPLIFT)Lancet 2009Jenkins CR, et al. Respir Res 2009Goldcopd.org

COPD
•Natural history•Pathophysiology•Diagnosis •Out‐patient management•In‐patient management
Therapeutic Options: Key Points
Smoking cessation has the greatest capacity to influence the natural history of COPD.
Pharmacotherapy and nicotine replacement reliably increase long-term smoking abstinence rates.
All COPD patients benefit from regular physical activity and should repeatedly be encouraged to remain active.
Therapeutic Options: Key Points
Smoking cessation has the greatest capacity to influence the natural history of COPD.
Pharmacotherapy and nicotine replacement reliably increase long-term smoking abstinence rates.
All COPD patients benefit from regular physical activity and should repeatedly be encouraged to remain active.

Prevention of COPD ProgressionSmoking Cessation
Years of follow-up
MeanFEV1 (L)
0 1 5432
2.9
2.8
2.7
2.6
2.5
2.4
Sustained quitters
Continuing smokers
Anthionsen, et al. JAMA 1994;272:1497
Prevention of COPD Progression:Smoking Cessation
•Only therapy proven to slow the decline in lung function
•Reduces all cause mortality by 27%
•Difficult to achieve• long-term abstinence rates can be as high as 25% in patients with
early COPD
Anthonisen NR, Ann Intern Med. 2005Anthonisen NR, Ann Intern Med. 2005

Natural History of COPD
25 35 45 55 65Age (years)
4
3
2
1
0
Symptoms
Death
Nonsmoker
Averagesmoker
“Susceptible”smoker
FEV1(liters)
Quitters

Natural History of COPD
25 35 45 55 65Age (years)
4
3
2
1
0
Symptoms
Death
Nonsmoker
Averagesmoker
“Susceptible”smoker
FEV1(liters)
Quitters

Smoking Cessation
•Nicotine replacement therapy & counseling• 25% sustained quit rate
• Bupropion (Zyban™) & counseling• 25 to 29% sustained quit rate
•Varenicline (Chantix) & counseling• 43% sustained quit rate
•When I ask all successful quitters how they quit• →Cold turkey
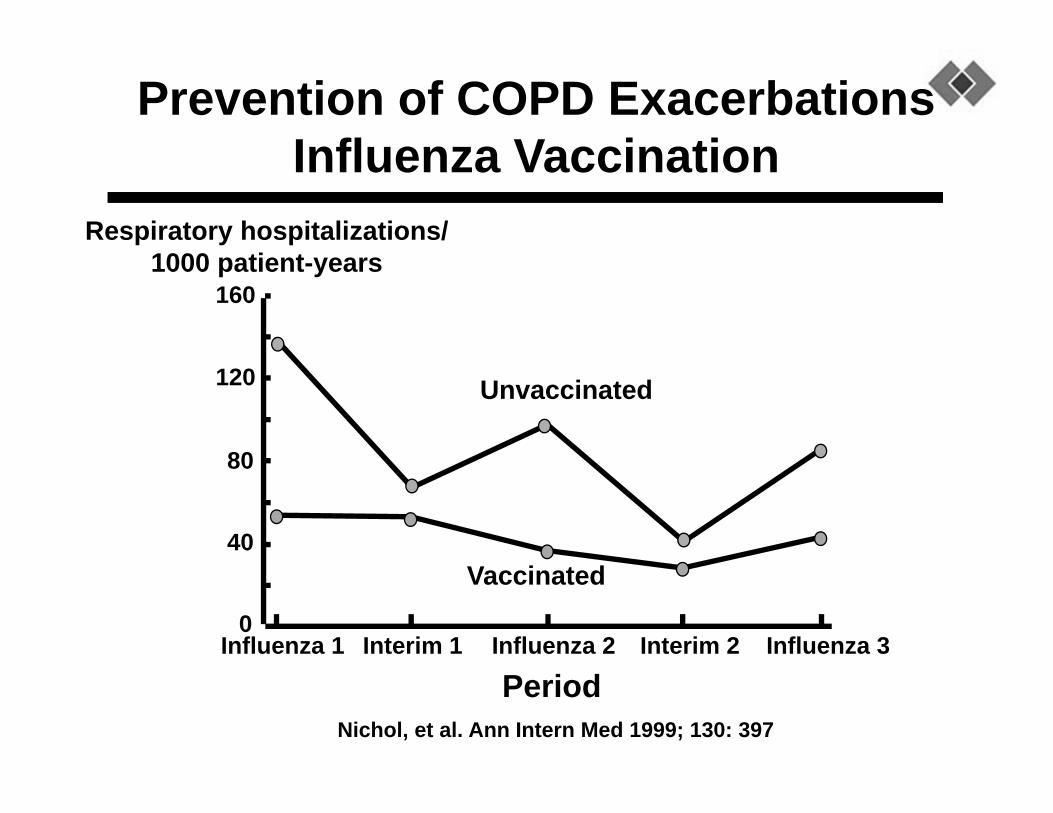
160
120
80
40
0Influenza 1 Influenza 3Influenza 2Interim 1 Interim 2
Period
Vaccinated
Unvaccinated
Nichol, et al. Ann Intern Med 1999; 130: 397
Prevention of COPD ExacerbationsInfluenza Vaccination
Respiratory hospitalizations/1000 patient-years
•Influenza vaccines can reduce serious illness
• Not 100% effective
• The odds are in their favor to vaccinate
•Pneumococcal vaccine recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV1 < 40% predicted
• No effect on morbidity, mortality, exacerbation rate
• Reduced pneumonia
Therapeutic Options: Other Pharmacologic Treatments

Therapeutic Options: COPD Medications
Beta2-agonists
Short-acting beta2-agonists- e.g Albuterol
Long-acting beta2-agonists – e.g. Salmeterol, Formoterol
Anticholinergics
Short-acting anticholinergics- e.g. Ipratropium
Long-acting anticholinergics – e.g. Tiotroprium
Combination short-acting beta2-agonists + anticholinergic in one inhaler – e.g. Combivent ™Methylxanthines
Inhaled corticosteroids – anything that ends in –sone, -lone, etc
Combination long-acting beta2-agonists + corticosteroids in one inhaler- .e.g Advair ™ (Serevent/Fluticasone), Symbicort ™Systemic corticosteroids
Phosphodiesterase-4 inhibitorsMacrolide antibiotics

Treatment options
•COPD is a disease of airflow obstruction•Obstruction stems from mucus production, airway narrowing, bronchospasm, smooth muscle contraction
•Treatment is aimed at ↓ mucus produc on, ↓inflamma on, ↓ bronchospasm,↓ smooth muscle contraction
•Steroids (↓inflamma on and mucus produc on) and Bronchodilators (↓smooth muscle contrac on, ↓airway narrowing)

Treatment options
•COPD is a disease of airflow obstruction• Obstruction stems from mucus production, airway narrowing, bronchospasm, smooth muscle contraction
• Treatment is aimed at ↓ mucus produc on, ↓inflamma on, ↓ bronchospasm,↓ smooth muscle contrac on
•Steroids (↓inflamma on and mucus produc on) and Bronchodilators (↓smooth muscle contrac on, ↓airway narrowing)

Treatment strategies
•Maintenance therapy•Generally long acting medications
•Rescue therapy•Generally short acting•Used for exacerbations or before activity
• Avoidance of risk factors
- smoking cessation
- reduction of indoor pollution
- reduction of occupational exposure
• Influenza vaccination
Manage Stable COPD: All COPD Patients
Bronchodilator central to symptomatic management
prescribed as-needed or regular basis to prevent or reduce symptoms
Principal bronchodilator: beta2-agonists and anticholinergics or combo therapy
Choice of treatment depends on availability of medications and each patient’s individual response in terms of symptom relief and side effects
Therapeutic Options: Bronchodilators

Long-acting inhaled bronchodilators (LABA)
convenient and more effective for symptom relief than short-acting bronchodilators
reduce exacerbations and related hospitalizations and improve symptoms and health status.
Cognitive function and ability to properly use inhaler therapy should be assessed regularly
Therapeutic Options: Bronchodilators
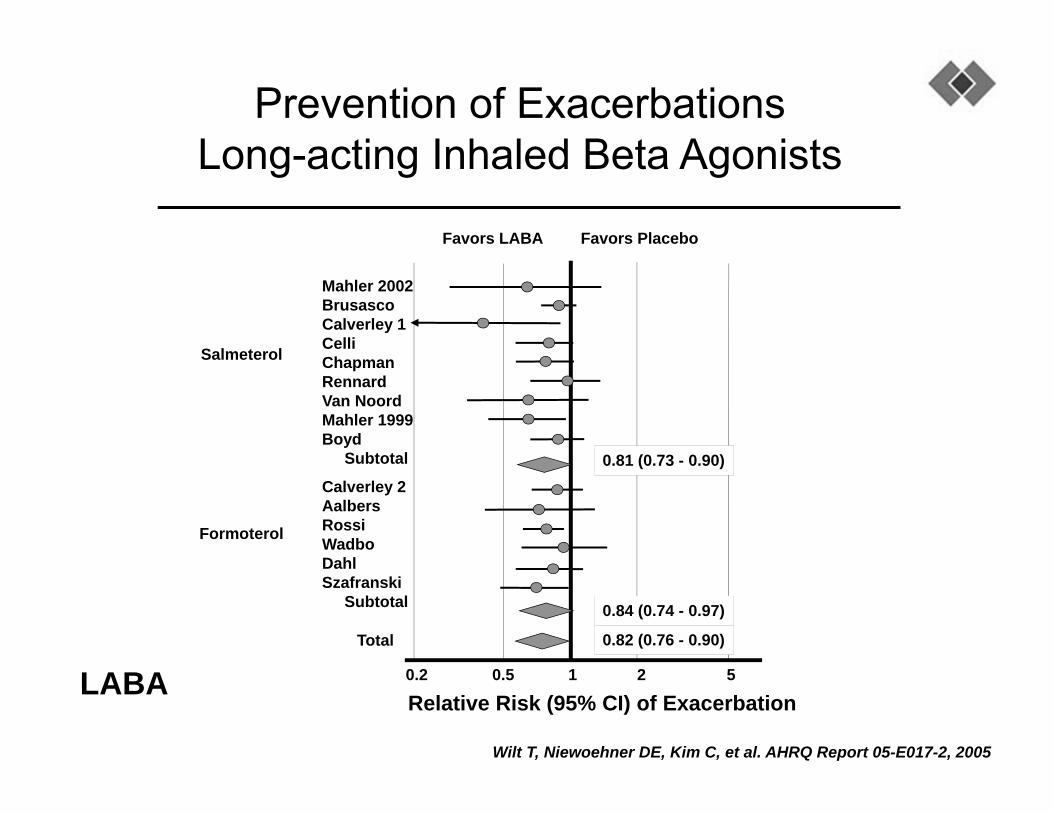
Wilt T, Niewoehner DE, Kim C, et al. AHRQ Report 05-E017-2, 2005
Prevention of ExacerbationsLong-acting Inhaled Beta Agonists
Relative Risk (95% CI) of Exacerbation
Favors LABA Favors Placebo
0.2 10.5 2 5
Mahler 2002BrusascoCalverley 1CelliChapmanRennardVan NoordMahler 1999Boyd
Subtotal
Calverley 2AalbersRossiWadboDahlSzafranski
Subtotal
Total 0.82 (0.76 - 0.90)
0.84 (0.74 - 0.97)
0.81 (0.73 - 0.90)
Salmeterol
Formoterol
LABA
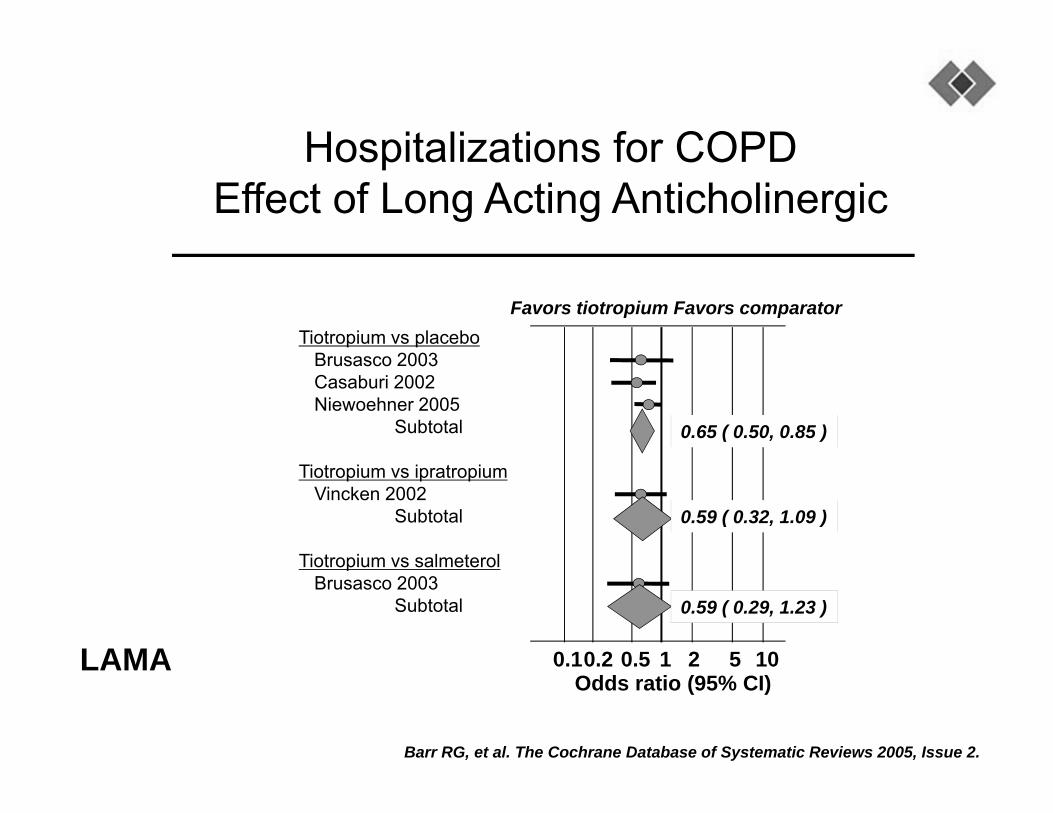
Hospitalizations for COPDEffect of Long Acting Anticholinergic
Barr RG, et al. The Cochrane Database of Systematic Reviews 2005, Issue 2.
Tiotropium vs placeboBrusasco 2003Casaburi 2002Niewoehner 2005
Subtotal
Tiotropium vs ipratropiumVincken 2002
Subtotal
Tiotropium vs salmeterolBrusasco 2003
Subtotal
0.1 1 2 5 100.50.2Odds ratio (95% CI)
Favors tiotropium Favors comparator
0.65 ( 0.50, 0.85 )
0.59 ( 0.32, 1.09 )
0.59 ( 0.29, 1.23 )
LAMA
Regular treatment with inhaled corticosteroids (ICS) improves symptoms, lung function and quality of life and reduces frequency of exacerbations for COPD patients with an FEV1< 60% predicted.
Associated with an increased risk of pneumonia
Withdrawal may lead to exacerbations in some patients
Therapeutic Options: Inhaled Corticosteroids

Wilt T, Niewoehner DE, Kim C, et al. AHRQ Report 05-E017-2, 2005
Prevention of ExacerbationsInhaled Corticosteroids
Relative Risk (95% CI) of Exacerbation0.2 10.5 2 5
BurgeCalverley 03Mahler 02van der ValkPaggiaro
Subtotal
BourbeauCalverly 04SzafranskiVestbo
Subtotal
Fluticasone
Budesonide
WeirSubtotal
Total
Beclomethasone0.64 (0.41 - 1.00)
0.78 (0.66 - 0.91)
0.81 (0.68 - 0.95)
0.78 (0.70 - 0.88)
Favors ICS Favors Placebo

Chronic treatment with systemic corticosteroids should be avoided because of an unfavorable benefit-to-risk ratio.
Therapeutic Options: Systemic Corticosteroids

inhaled corticosteroid + long-acting beta2-agonist
more effective than the individual components in improving lung function and health status and reducing exacerbations in moderate to very severe COPD.
Combination therapy is associated with an increased risk of pneumonia
Addition of a long-acting beta2-agonist/inhaled glucocorticosteroid combination to an anticholinergic (tiotropium) appears to provide additional benefits
Therapeutic Options: Combination Therapy
Severe and very severe COPD (GOLD 3 and 4) + history of exacerbations and chronic bronchitis
Phospodiesterase-4 inhibitor (PDE-4), roflumilast (Daliresp™)
Reduces exacerbations treated with oral glucocorticosteroids
I have no patients taking this
Therapeutic Options: Phosphodiesterase-4 Inhibitors

Relieve symptoms Improve exercise tolerance Improve health status
Prevent disease progression Prevent and treat exacerbations Reduce mortality
Reducesymptoms
Reducerisk
Manage Stable COPD: Goals of Therapy

Manage Stable COPD: Pharmacologic Therapy(Medications in each box are mentioned in alphabetical order, and therefore not
necessarily in order of preference.)
Patient First choice Second choice Alternative Choices
ASAMA prn
orSABA prn
LAMA or
LABA or
SABA and SAMA
Theophylline
BLAMA
orLABA
LAMA and LABA SABA and/or SAMATheophylline
C
ICS + LABAor
LAMA LAMA and LABAPDE4-inh.
SABA and/or SAMATheophylline
D
ICS + LABAor
LAMA
ICS and LAMA orICS + LABA and LAMA or
ICS+LABA and PDE4-inh. orLAMA and LABA or
LAMA and PDE4-inh.
CarbocysteineSABA and/or SAMA
Theophyllineazithromycin

Treatment strategies
•Maintenance therapy•Think through what you are treating:•SOB just with ac vity: → prn Albuterol•Use Albuterol more than BID → LABA or LAMA (Fomoterol, Incruse™)
•Night me symptoms → LABA or LAMA•Chronic Cough → LACS•Moderate to Severe COPD → LABA/LACS and/or LAMA (Symbicort™)

Treatment strategies
•Maintenance therapy•Rescue therapy for exacerbations
•Continue maintenance therapy•Short acting beta agonists scheduled
• Nebulizer more beneficial then MDI
•Prednisone 40 mg p.o. for 5 days• I’d avoid medrol dose packs
Treatment strategies
•Anti‐biotics• moderate or severe exacerbation of COPD
• having at least two of these three symptoms • ↑ dyspnea, ↑ sputum volume, or ↑sputum purulence
• No anti‐biotics• Mild‐ having only one of these three symptoms and not requiring hospitalization
•Haemophilus influenzae,Moraxella catarrhalis, and Streptococcus pneumoniae
Treatment strategies
•Anti‐biotics• moderate or severe exacerbation of COPD
• having at least two of these three symptoms • ↑ dyspnea, ↑ sputum volume, or ↑sputum purulence
• No anti‐biotics• Mild‐ having only one of these three symptoms and not requiring hospitalization
•Haemophilus influenzae,Moraxella catarrhalis, and Streptococcus pneumoniae

COPD ExacerbationsAntibiotic Therapy
Ram FSF, et al. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD004403.
Alonso 1992
Anthonisen 1987
Elmes 1965
Jorgensen 1992
Pines 1968
Pines 1972
Total
Favors placeboFavors antibiotic
RR (95% CI) of Treatment Failure
0.67 (0.56 -0.80)
0.1 1 2 5 100.50.2

COPD
•Natural history•Pathophysiology•Diagnosis •Out‐patient management•In‐patient management
Inpatient treatment strategies
•When to hospitalize:•Acute or acute‐on‐chronic respiratory acidosis• Inadequate response to outpatient/ER management•↑ intensity of symptoms over baseline •Severe underlying COPD (eg, [FEV1] ≤50% of predicted)
•Older age• Insufficient home support•History of frequent exacerbations•Comorbidities

Inpatient treatment strategies
• Strategy focus similar to Outpatient management• Reduce inflammation: Steroids• Reduce bronchospasm: Nebulized Beta‐agonist• Oxygen therapy• Non‐invasive ventilation (Bi‐PAP) for respiratory acidosis• Mechanical ventilation for respiratory acidosis that does not respond to Bi‐PAP
• Target normal pH, not normal PaCO2
• Antibiotics

All COPD patients benefit from exercise training programs with improvements in exercise tolerance and symptoms of dyspnea and fatigue.
Although an effective pulmonary rehabilitation program is 6 weeks, the longer the program continues, the more effective the results.
If exercise training is maintained at home the patient's health status remains above pre-rehabilitation levels.
Therapeutic Options: Rehabilitation

Rehabilitation Therapy for COPDExercise Capacity
McGavin,1977Cockcroft, 1981Booker, 1984Jones, 1985Lake, 1990Simpson, 1992Weiner, 1992Goldstein, 1994Wijkstra, 1994Guell, 1995Strijbos, 1995
Overall effect
Favors control Favors treatment
Effect size (SD units)-2 -1 0 1 2 3 4
Lacasse, et al. Lancet 1996;348:1115

00
44
88
1212
1616
2020
PlaceboPlacebo RehabilitationRehabilitation0
4
8
12
16
20
Placebo Rehabilitation00
5050
100100
150150
200200
250250
ControlControl RehabilitationRehabilitation0
50
100
150
200
250
Control RehabilitationBaselineBaseline 6 weeks6 weeks 1 year1 year
Walking distance (m)Walking distance (m)Quality of life (CRQ score)Quality of life (CRQ score)
Efficacy of Pulmonary Rehabilitation in COPD
Griffiths et al. Lancet. 2000;355:362-368.

Oxygen Therapy: The long-term administration of oxygen (> 15 hours per day) to patients with chronic respiratory failure has been shown to increase survival in patients with severe, resting hypoxemia.
Ventilatory Support: Combination of noninvasive ventilation (NIV) with long-term oxygen therapy may be of some use in a selected subset of patients, particularly in those with pronounced daytime hypercapnia.
Therapeutic Options: Other Treatments
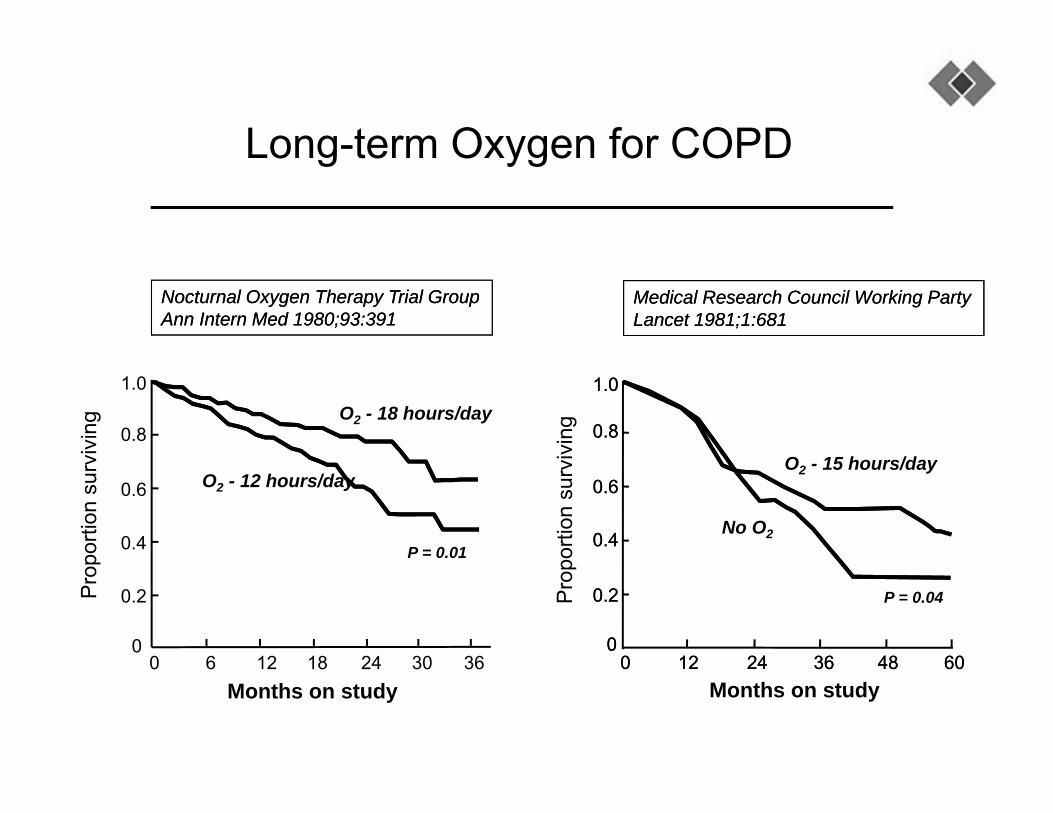
Long-term Oxygen for COPD
1.0
0
0.8
0.6
0.4
0.2
6 12 18 3630240Months on study
O2 - 18 hours/day
O2 - 12 hours/day
P = 0.01
Nocturnal Oxygen Therapy Trial GroupAnn Intern Med 1980;93:391Nocturnal Oxygen Therapy Trial GroupAnn Intern Med 1980;93:391
Pro
porti
on s
urvi
ving
P = 0.04
1.01.0
0.80.8
0.60.6
0.40.4
0.20.2
0000 1212 2424 3636 4848 6060
Months on study
O2 - 15 hours/day
No O2
Pro
porti
on s
urvi
ving
Medical Research Council Working PartyLancet 1981;1:681Medical Research Council Working PartyLancet 1981;1:681

Indications for Oxygen use
•SpO2 < 88% or PaO2 < 55 mmHg•SpO2 < 89% or PaO2 56‐59 mmHg
•Edema suggesting CHF•Pulmonary HTN or cor pulmonale•Hct > 56%
•If SpO2 > 88% → Exercise tes ng•Any other values will not be covered

•Mucoactive agents
•Methylxanthines
•Mechanical techniques to augment sputum clearance
•Have not been shown to confer benefit for patients with a COPD exacerbation
•It does not mean there is no place in their use
Therapeutic Options: Other Treatments without documented benefits

Case 1
• 78 y.o. male• COPD• Current smoker• On no therapy• FEV1 70%• Can walk without any limitation, no respiratory symptoms
• SpO2 94% on RA
• Advair 250/50• Oxygen therapy• Albuterol prn• Spiriva• Prednisone burst• Daily Prednisone• Smoking cessation• Pulmonary Rehab

Case 1
•78 y.o. male•COPD•Current smoker•On no therapy•FEV1 70%•Can walk without any limitation, no respiratory symptoms
•SpO2 94% on RA
•Advair 250/50•Oxygen therapy•Albuterol prn•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab
Case 2
• 82 y.o. female• COPD• Former smoker• Daily cough and wheezing• On Albuterol• FEV1 30%• Limited to ADLs• SpO2 87% on RA
• Advair 250/50• Prn Albuterol • Oxygen therapy• Spiriva• Prednisone burst• Daily Prednisone• Smoking cessation• Pulmonary Rehab

Case 2
•82 y.o. female•COPD•Former smoker•Daily cough and wheezing
•On Albuterol•FEV1 30%• Limited to ADLs•SpO2 87% on RA
•Advair 250/50•Prn Albuterol•Oxygen therapy•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab

Case 3
•68 y.o. male•COPD•Former smoker•Daily cough and wheezing
•On Spiriva•FEV1 60%•Worsening SOB over last year
•SpO2 90% on RA
•Advair 250/50•Prn Albuterol•Oxygen therapy•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab

Case 3
•68 y.o. male•COPD•Former smoker•Daily cough and wheezing
•On Spiriva•FEV1 60%•Worsening SOB over last year
•SpO2 90% on RA
•Advair 250/50•Prn Albuterol•Oxygen therapy•Spiriva•Prednisone burst•Daily Prednisone•Smoking cessation•Pulmonary Rehab
• 4th-leading cause of death worldwide• Not all patient’s with COPD smoke ~ 15%• Spirometry required: FEV1/FVC < 0.70 AND FEV1< 0.80• Patients with very Severe COPD FEV1 < 30% have 24% 3 year mortality• Smoking Cessation is key• Goal of treatment is to address the underlying cause
What you Have learned today