als 450: prognostication in hypothermia · claudio sandroni: first author of two systematic reviews...
TRANSCRIPT

Dallas 2015
TFQO: Clifton Callaway
EVREVs: Claudio Sandroni (COI #134); Eyal Golan (COI #61)
Taskforce: ALS
ALS 450: Prognostication in Hypothermia

Dallas 2015 COI Disclosure (specific to this systematic review)
Commercial/industry
Claudio Sandroni: none
Eyal Golan: none
Potential intellectual conflicts Claudio Sandroni: first author of two systematic reviews on prognostication after cardiac arrest and of the ERC-ESICM Advisory Statement on prognostication in comatose survivors of cardiac arrest
Eyal Golan: first author of a systematic review on prognostication after cardiac arrest in patients receiving targeted temperature management and author of the Canadian Guidelines on the use of targeted temperature management after cardiac arrest

Dallas 2015
2010 CoSTR
No reviews in 2010
Dallas 2015
C2015 PICO
Population: Adults with ROSC who are treated with targeted temperature management (TTM)
Intervention: any clinical variable when normal (e.g. 1. Clinical Exam, 2. EEG or SSEP, 4. Imaging, 5. Other)
Comparison: any clinical variable when abnormal
Outcomes Survival with Favorable neurological or functional outcome at discharge, 30 days, 60 days, 180 days AND/OR 1 year, Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year

Dallas 2015 Inclusion/Exclusion & Articles Found
Inclusion: adult (≥16 years) pts, comatose (unconscious, unresponsive, or GCS≤8)
Exclusion: Studies including pts. in hypoxic coma from causes other than CA (e.g., respiratory arrest, CO poisoning) except when a subpopulation of cardiac arrest patients could be evaluated separately.
Included: 44 articles were included in final analysis

Dallas 2015
Grading: risk of bias
Serious = treating team aware of the results of the index test
Very serious = index test used for WLST
Other variables
Sedation, paralysis (when applicable)
Best CPC reported
Length of follow-up
Interobserver agreement

Dallas 2015
Imprecision
Serious = upper limit of the 95%CIs of the estimate of the false positive rate (FPR) was greater than 5%
Very serious = upper 95%CI limit was greater than 10%

Dallas 2015
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Al Thenayan, 2008
PLR, CR, MR no No No no no No 90 days Not reported Very serious
Bisschops 2011 PLR+CR+MR, myoclonus, EEG
no No Yes no no No 90 days Yes (BR) Very serious
Bisschops 2011 SSEP no No N/A no no No 90 days Yes Very serious
Bouwes 2009 SSEP (TH) limited Yes N/A no yes No 30 days No Serious
Bouwes 2012 PLR, CR, M1-2, myoclonus
no No uncertain no yes No 180 days Uncertain Serious
Bouwes 2012 SSEP (TH) limited No N/A no no No 180 days No Serious
Bouwes 2012 SSEP (after RW) no No N/A no no No 180 days Yes Very serious
Bouwes, 2012 NSE yes No N/A no no N/A 180 days Uncertain Serious
Choi 2012 SSSEP, CT, MRI no No N/A no no No Discharge Not reported Very serious
Choi, 2012 PLR no No No no no No Discharge Not reported Very serious
Cloostermans 2012
cEEG no Yes No no yes No 180 days No Serious
Cloostermans 2012
SSEP no No N/A no yes No 180 days Yes Very serious
Crepeau 2013 cEEG, myoclonus no Yes No no no No Discharge Yes Very serious
Cronberg 2011 SSEP no No N/A yes no Yes 180 days Yes Very serious
Cronberg 2011 EEG no Yes Yes yes no No 180 days No Serious
Cronberg, 2011 PLR, CR, MR, myoclonus
no No Yes yes no No 180 days Yes (PLR,
MR) Very serious
Cronberg, 2011 NSE no No N/A yes no N/A 180 days No Serious
Cronberg, 2011 MRI DWI no Yes N/A yes no No 180 days No Serious

Dallas 2015
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Fugate 2010 PLR, CR, MR, myoclonus
no No No no no No Discharge Yes Very serious
Fugate 2010 NSE, CT no No N/A no no No Discharge No Serious
Huntgeburth 2014
NSE no No N/A no no No 60 days Not reported Very serious
Inamasu 2010 CT no Yes N/A no no Yes 180 days Not reported Very serious
Kawai 2011 EEG no No No no no No 180 days Not reported Very serious
Kim, 2012 NSE, MRI no No N/A no no no (MRI) N/A (NSE)
180 days Not reported Very serious
Kim 2013 MRI no No N/A no no No 180 days Uncertain Serious
Kim S 2013 CT no Yes N/A no no No Discharge Not reported Very serious
Leary 2010 BIS no No No no no N/A Discharge Not reported Very serious
Lee 2013 NSE, CT no Yes N/A No No No Discharge No
withdrawal Serious
Legriel 2009 EEG no Yes No no no No Discharge Not reported Very serious
Legriel 2013 Myoclonus no No No no no No 1 year Uncertain Serious
Legriel 2013 EEG no No No no no No 1 year No Serious
Leithner 2010 SSEP no No N/A no no No Discharge Not reported Very serious
Mani 2012 EEG no Yes No no no Yes Discharge Uncertain Serious
Mlynash, 2010 MRI no Yes N/A yes no Yes 180 days Not reported Very serious
Mortberg, 2011 NSE, S-100B no No N/A no no N/A 180 days Not reported Very serious
Oddo 2014 BR, Myoclonus no No Yes no no No 90 days Yes Very serious

Dallas 2015
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Okada 2012 PLR, MR no No No no yes No Discharge Not reported Very serious
Oksanen, 2009 NSE no No No no no N/A 180 days No Serious
Rittenberger 2012
EEG, myoclonus no No No no no No Discharge Not reported Very serious
Rossetti 2010 BR, MR, myoclonus, EEG
no No Yes no no No 180 days Yes (BR, EEG) Very serious
Rossetti 2010 SSEP no No N/A no no No 180 days Yes Very serious
Rossetti 2012 BR, MR, myoclonus, EEG
no No Yes no no No 90 days Yes (BR,
myoclonus, EEG)
Very serious
Rossetti, 2012 SSEP, NSE yes No N/A no no no (SSEP); N/A (NSE)
90 days Yes (SSEP) Very serious
Rundgren 2010 EEG no Yes No no no No 180 days No Serious
Rundgren, 2009 NSE, S-100B no No N/A yes yes N/A 180 days No Serious
Sakurai 2006 BAEP wave V absent
no No N/A no yes No 60 days Not reported Very serious
Samaniego 2011 BR, MR, myoclonus no No No no no No 90 days Yes Very serious
Samaniego, 2011 SSEP no No N/A no no N/A 90 days Yes Very serious
Samaniego, 2011 NSE no No N/A no no N/A 90 days No Serious
Schefold 2009 GCS ≤ 4 no No No no no No Discharge Yes Very serious
Seder 2010 BIS no No N/A no no N/A Discharge Not reported Very serious
Stammet 2009 BIS limited Yes N/A yes no N/A 180 days No Serious
Stammet 2013 BIS no No Yes no no N/A 180 days Not reported Very serious
Stammet 2013 S-100B no No N/A no no N/A 180 days Not reported Very serious

Dallas 2015
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Tiainen 2005 SSEP limited No N/A no yes No 180 days No Serious
Tiainen, 2003 NSE, S-100B no Yes N/A no no N/A 180 days Not reported Very serious
Wennervirta 2009
EEG no Yes No no yes No 180 days Not reported Very serious
Wennervirta, 2009
NSE, S-100B no No N/A no yes N/A 180 days Not reported Very serious
Wijman, 2009 MRI (ADC) limited Yes N/A yes no No 180 days No Serious
Zanatta 2012 SSEP, MLCEP no No N/A no no No 90 days Not reported Very serious
Zellner 2013 NSE, S-100B No No No No No No 180 days Not reported Very serious

Dallas 2015
Clinical examination
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified four studies on corneal reflex, pupillary reflex, motor response, Glasgow Coma Score, or myoclonus (295 patients, very low quality of evidence).
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified five studies on corneal reflex, pupillary reflex, motor response, brainstem reflexes, or myoclonus (388 patients, very low quality of evidence).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified four studies on corneal reflex, pupillary reflex, motor response, brainstem reflexes, or myoclonus (642 patients, low or very low quality of evidence).

Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Corneal
reflex (4) At 72-120h
Very
serious No Serious Serious Very low 43 3 132 123 25 [18-32] 2 [0-7] 5 [2-16]
Pupillary
reflex (5) at 72-108h
Very
serious No No No Low 42 1 180 160 19 [14-26] 1 [0-3] 7 [2-22]
GCS Motor
1-2 (6) At 36-108h
Very
serious No No
very
serious very low 257 28 111 239 70 [65-74] 10 [7-15] 6 [4-9]
Myoclonus
(5) At 24-72h
Very
serious No Serious serious very low 182 16 249 274 41 [36-46] 6[3-9] 6 [4-10]
Status
myoclonus
(3)
≤72h Very
serious No No No Low 25 0 137 78 16 [11-22] 0 [0-4] 4 [2-10]

Dallas 2015 Draft Treatment Recommendations
Clinical Examination - 1
We recommend using bilaterally absent pupillary light reflexes or the combined absence of both pupillary and corneal reflexes at ≥72 h from ROSC to predict poor outcome (Strong recommendation, low QOE)
We suggest against using an absent or extensor motor response to pain (M≤2) alone to predict poor outcome, given its high false positive rate (weak recommendation, very low QOE). However, due to its high sensitivity, this sign may be used to identify the population with poor neurological status needing prognostication or to predict poor outcome in combination with other more robust predictors.
We suggest using the presence of a status myoclonus within 72 h from ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, low QOE).

Dallas 2015 Draft Treatment Recommendations
Clinical Examination - 2
We suggest prolonging the observation of clinical signs when interference from residual sedation or paralysis is suspected, so that the possibility of obtaining false positive results is minimized (weak recommendation, very low QOE).
We recommend that the earliest time to prognosticate a poor neurological outcome using clinical examination is 72hrs after ROSC, and should be extended longer if the residual effect of sedation and/or paralysis confounds the clinical examination.

Dallas 2015
Myoclonus
Is a clinical sign
Sudden, brief, shock-like, involuntary movements caused by muscular contractions or inhibitions
Focal = involving only a few adjacent muscles
Generalized = involving most of the muscles in the body, often not synchronously

Dallas 2015
Status myoclonus
A prolonged period of frequent myoclonic jerks
There is no universal consensus on the duration or frequency of the myoclonic jerks necessary to qualify them as a status myoclonus
Proposed definition = generalised continuous myoclonus persisting for ≥30 minutes
Dallas 2015
Myoclonus and epilepsy
Myoclonus is only inconsistently associated with EEG epileptiform activity
Most frequent EEG correlate of post-anoxic myoclonus is burst-suppression
Status epilepticus = continuous and prolonged epileptiform activity on EEG
It may or may not be associated with clinical manifestations, including myoclonus

Dallas 2015
Status epilepticus
Status myoclonus MSE
Dallas 2015
Knowledge Gaps
In comatose resuscitated patients who have been treated with TTM, prospective studies are needed to investigate:
the pharmacokinetics of sedative and NMB drugs
the reproducibility of clinical signs used to predict
outcome.
There is no universally accepted definition of status myoclonus
Recently proposed definition = generalised myoclonus persisting for ≥30 minutes.

Dallas 2015
Electrophysiology
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 8 studies on SSEP, EEG or BIS (571 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 30 days, we identified one study on SSEP (77 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 60 days we identified one study on BAEPs (26 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified five studies on SSEP or EEG (362 patients, low or very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified ten studies on SSEP, EEG or BIS (921 patients, moderate, low, or very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 1 year, we identified one study on EEG (106 patients very low QOE).

Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Absent N20
SSEP (4) During TTM Serious No No No Moderate 60 3 164 194 28 [22-34] 2 [1-4] 12 [5-32]
Absent N20
SSEP (10) After RW
Very
serious No Serious No Very low 42 1 180 160 45 [41-50] 1 [0-3] 14 [6-32]
Unreactive
EEG (3) During TTM
Very
serious No No Serious Very low 80 3 46 120 63 [54-72] 2 [1-7] 18 [5-61]
Unreactive
EEG (3) After RW
Very
serious no no No Low 85 0 52 86 62 [53-70] 0 [0-3] 33 [7-163]
Burst-
suppression
EEG (4)
During TTM Very
serious no serious Serious Very low 55 3 57 111 49 [40-58] 3 [1-7] 11 [4-30]
Burst-
suppression
EEG (1)
After RW Serious no very
serious Very low 7 0 31 57 18 [8-34] 0 [0-5] 22 [1-379]

Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
EEG
seizures,
nonreactive
During TTM Very
serious No -
Very
serious Very low 10 0 23 28 30 [16-49] 0 [0-10] 18 [1-293]
EEG
seizures After RW
Very
serious No -
Very
serious Very low 9 0 17 12 35 [17-56] 0 [0-22] 9 [1-145]
EEG
seizures
During TTM
and RW
Very
serious No - Serious Very low 5 0 16 33 24 [8-47] 0 [0-9] 17 [1-292]
Status
epilepticus During TTM
Very
serious no - no Low 5 0 34 12 13 [4-27] 0 [0-22] 4 [0,2-60]
Status
epilepticus After RW
Very
serious no - serious Very low 4 0 5 21 44 [14-79] 0 [0-13] 20 [1-334]
Status
epilepticus
(2)
≤72h Very
serious No serious
Very
serious Very low 43 2 131 31 25[18-32] 6 [1-20] 3 [0-23]

Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Flat During
TTM Serious No -
Very
serious Very low 10 21 26 17 31 55 [38-71] 46 [32-59]
Flat or low-
voltage
During
TTM Serious No -
Very
serious Very low 9 8 0 12 26 40 [19-64] 0 [0-11]
Flat After RW Serious No - Serious Very low 5 6 3 32 54 16 [6-31] 5 [1-15]
BIS=0 During
TTM
Very
serious no -
Very
serious Very low 14 0 14 17 50 [31-69] 0 [0-16] 18 [1-284]
Lowest mean
BIS≤ 5,5
During
TTM
Very
serious no -
Very
serious Very low 29 7 5 34 85 [69-95] 17 [7-32] 5 [3-10]
Lowest
BIS=0
During
TTM
Very
serious No -
Very
serious Very low 26 4 8 37 76 [59-89] 10 [3-23] 8 [3-30]

Dallas 2015 Draft Treatment Recommendations
Electrophysiology
We recommend using bilateral absence of N20 SSEP wave at ≥72h after ROSC to predict poor outcome (strong recommendation, low QOE).
We suggest using EEG-based predictors such as absence of EEG reactivity (weak recommendation, low QOE), presence of burst-suppression (weak recommendation, very low QOE) or status epilepticus (weak recommendation, very low QOE) at ≥72h after ROSC in combination with other predictors for prognosticating a poor neurological outcome.
We suggest against using BIS to predict poor outcome (weak recommendation, very low QOE).

Dallas 2015
Knowledge Gaps
In most prognostication studies on TTM-treated patients, SSEPs have been used as a criterion for WLST
Blinded studies on SSEPs are needed to assess the relevance of self-fulfilling prophecy for SSEP.
Definitions of EEG-based predictors are inconsistent among prognostication studies.
Future studies should comply with recently recommended definitions (Hirsch and coll., 2013).
The stimulation modalities for eliciting EEG reactivity have not been standardised.

Dallas 2015
Biomarkers
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 4 studies on NSE (354 patients, moderate, low or very low quality of evidence).
For the critical outcome of survival with unfavorable neurological status or death at 60 days, we identified one study on NSE (73 patients, very low quality of evidence)
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified 3 studies on NSE (248 patients, very low quality of evidence)
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 8 studies on NSE or S-100B (810 patients, moderate, low, or very low quality of evidence).

Dallas 2015
Evidence profile table
Predictor,
timing,
studies
Th
resh
old
(mcg
L-1)
Risk of bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
NSE
24 h
(6)
31.2 Very serious no - very
serious very low 2 1 8 24 20 [3-56] 4 [0-20] 5 [1-49]
41 Serious no - very
serious very low 7 2 32 48 18 [8-34] 4 [0-14] 4 [1-20]
49.6 Very serious no - very
serious very low 20 0 5 9 80 [59-93] 0 [0-29] 15 [1-229]
52.4 Very serious no very
serious very low 1 0 9 20 10 [0-45] 0 [0-14]
6 [0,3-
129]
80.8 Serious no No Moderate 22 0 60 60 27 [18-37] 0 0-4][ 33 [2-535]
151.4 Very serious No Very
serious Very low 8 0 54 41 13 [6-24] 0 [0-7] 11 [1-191]

Dallas 2015
Evidence profile table
Predictor,
timing,
studies
Th
resh
old
(mcg
L-1)
Risk of bias
In
dire
ctn
ess
In
co
nsis
ten
cy Imprecision
Quality of
evidence TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
NSE
48 h
(13)
4.97 Very serious no - Very serious very low 2 1 8 24 20 [3-56] 4 [0-20] 5 [1-49]
25 Very serious no very serious very low 2 0 7 24 22 [3-60] 0 [0-12] 13 [1-238]
33 Serious No S Serious Very low 122 11 107 191 53 47-60] 5 [3-10] 9 [5-16]
44.3 Very serious no - Very serious Very low 19 0 3 7 86 [64-97] 0 [0-34] 14 [1-209]
52.7 Very serious no - No Low 49 0 33 60 60 [48-70] 0 [0-5] 73 [5-1157]
54.5 Very serious no Very serious Very low 14 0 10 9 10]0-45] 0 [0-28] 12 [1-176]
58.3 Serious no Very serious Very low 43 11 116 140 27 [10-35] 7 4-13][ 4 [2-7]
59.25 Very serious No Very serious Very low 1 0 9 20 10 [0-45] 0 [0-14] 6 [0-129]
81.8 Serious No Np Moderate 29 0 130 151 18 [13-25] 0 [0-2] 56 [3-909]
112.4 Very Serious No Serious Very low 9 0 21 33 30 [15-49] 0 [0-9] 21 [1-343]
151.5 Very Serious No Serious Very low 14 0 48 41 23 [13-35] 0 [0-7] 19 [1-343]

Dallas 2015
Evidence profile table
Predictor,
timing
Th
resh
old
(mcg
L-1)
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
NSE 72h
(4)
33 Serious No - Very
serious Very low 18 4 6 14 75 [53-90] 22 [6-48] 3 [1-8]
57.2 Very
serious No -
Very
serious Very low 11 0 13 9 46 [26-67] 0 [0-28] 9 [1-142]
65.4 Very
serious No - Serious Very low 23 0 7 33 77 [58-90] 0 [0-9] 52 [3-813]
78.9 Very
serious no Serious Very low 21 0 23 53 48 [32-63] 0 [0-5] 52 [3-828]

Dallas 2015
Huntgeburth et al., Neurocrit Care 2014; 20: 358-66

Dallas 2015
Oksanen T et al Resuscitation 2009; 80: 165-70

Dallas 2015
Lee BK et al Resuscitation 2013; 84: 1387-92

Dallas 2015 Draft Treatment Recommendations
Biomarkers
We suggest using high serum values of NSE at 48h-72h from ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, from moderate to very low QOE). However, no threshold enabling prediction with zero FPR can be recommended.
We suggest using utmost care and preferably sampling at multiple time-points when assessing NSE, to avoid false positive results due to hemolysis (weak recommendation, very low QOE).

Dallas 2015
Knowledge Gaps
There is a need for standardisation of the measuring techniques for NSE and S-100 in cardiac arrest patients.
Little information is available on the kinetics of the blood concentrations of biomarkers in the first few days after cardiac arrest.

Dallas 2015
Imaging
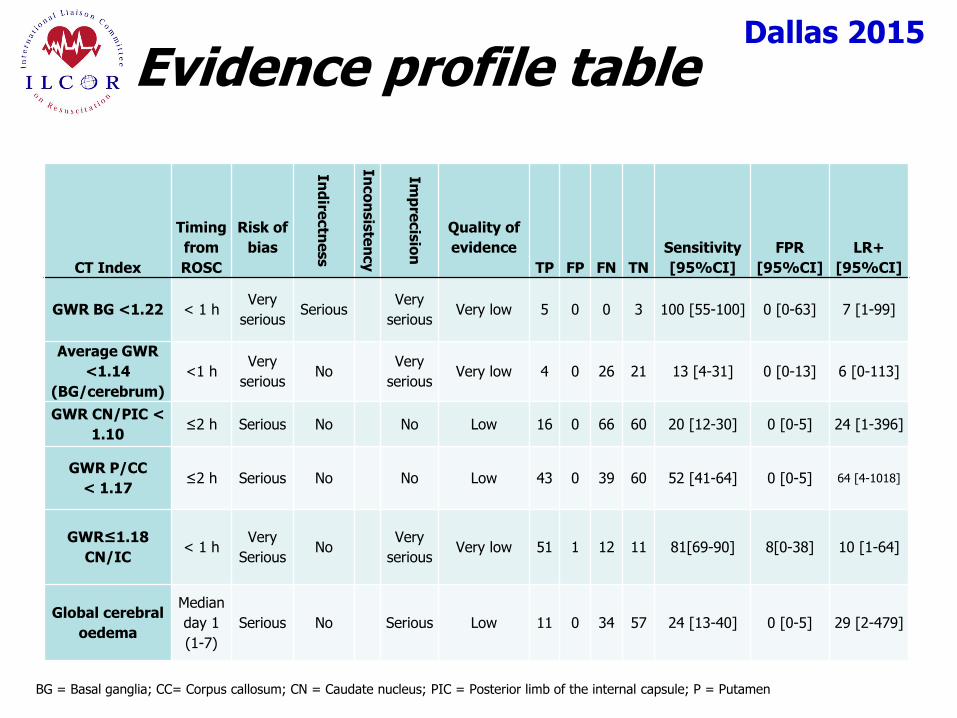
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 3 studies on CT (273 patients, low or very low quality of evidence).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 6 studies on CT or MRI (246 patients, very low quality of evidence).
Dallas 2015
Evidence profile table
CT Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
GWR BG <1.22 < 1 h Very
serious Serious
Very
serious Very low 5 0 0 3 100 [55-100] 0 [0-63] 7 [1-99]
Average GWR
<1.14
(BG/cerebrum)
<1 h Very
serious No
Very
serious Very low 4 0 26 21 13 [4-31] 0 [0-13] 6 [0-113]
GWR CN/PIC <
1.10 ≤2 h Serious No No Low 16 0 66 60 20 [12-30] 0 [0-5] 24 [1-396]
GWR P/CC
< 1.17 ≤2 h Serious No No Low 43 0 39 60 52 [41-64] 0 [0-5] 64 [4-1018]
GWR≤1.18
CN/IC < 1 h
Very
Serious No
Very
serious Very low 51 1 12 11 81[69-90] 8[0-38] 10 [1-64]
Global cerebral
oedema
Median
day 1
(1-7)
Serious No Serious Low 11 0 34 57 24 [13-40] 0 [0-5] 29 [2-479]
BG = Basal ganglia; CC= Corpus callosum; CN = Caudate nucleus; PIC = Posterior limb of the internal capsule; P = Putamen

Dallas 2015
Evidence profile table
MRI Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Extensive cortical
lesion pattern
80H (IQR
55-117)
Very
serious No
Very
serious Very low 9 1 1 10 90 [55-100] 9 [0-41] 10 [2-65]
DWI changes in BG 80H (IQR
55-117)
Very
serious No
Very
serious Very low 8 1 2 10 80 [44-97] 9 [0-41] 9 [1-58]
DWI changes in BS 80H (IQR
55-117)
Very
serious No
Very
serious Very low 3 0 7 11 30 [7-65] 0 [0-24] 8 [0-132]
Changes in cortex +
BG
74h (IQR
61-86) Serious Serious
Very
serious Very low 11 0 8 3 58 [33-80] 0 [0-63] 5 [0-63]
Changes in cortex +
BG < 5 days
Very
serious No
Very
serious Very low 5 0 0 3 100 [55-100] 0 [0-63] 7 [1-99]

Dallas 2015
Evidence profile table
MRI Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
Quality of
evidence
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
ADC < 650 ▪ 10-6
mm2/sec in >10%
of brain volume
49-108 h Serious No Very
serious Very low 10 0 3 9 77 [46-95] 0 [0-28] 15 [1-227]
Occipital cortex
ADC < 616 ▪ 10-6
mm2/sec
45.8
(IQR
36,8-
52,4))
Very
serious No
Very
serious Very low 29 0 3 11 91 [75-98] 0 [0-24] 21 [1-324]
Putamen ADC < 590
▪ 10-6 mm2/sec
Very
serious No
Very
serious Very low 25 0 7 11 78 [60-91] 0 [0-24] 19 [1-281]
Thalamus ADC <
660 ▪ 10-6 mm2/sec
Very
serious No
Very
serious Very low 20 0 12 11 63 [44-79] 0 [0 24] 15 [1-228]

Dallas 2015 Draft Treatment Recommendations
Imaging
We suggest using the presence of a marked reduction of the GM/WM ratio on brain CT within 2 h after ROSC or the presence of extensive reduction in diffusion on brain MRI at 2-6 days after ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, very low QOE).
We suggest using brain imaging studies for prognostication only in centers where specific experience is available (weak recommendation, very low QOE).

Dallas 2015
Knowledge Gaps
Prospective studies in unselected patient populations and including inter-rater agreement are needed for evaluating the prognostic accuracy of imaging studies in comatose patients resuscitated from cardiac arrest.

Dallas 2015
Final comments
Bilaterally absent PLR or SSEP are the most robust predictors (FPR <5%, narrow Cis)
No index predicts poor outcome with absolute certainty
Multimodality is the most reasonable approach

(1) At ≥24h after ROSC in patients not treated with targeted temperature
(2) See text for details.
Poor outcome very likely
(FPR <5%, narrow 95%CIs)
Two or more of the following: - Status myoclonus ≤48h after ROSC - High NSE levels (2) - Unreactive burst-suppression or status epilepticus on EEG - Diffuse anoxic injury on brain CT/MRI (2)
One or both of the following: - No pupillary and corneal reflexes - Bilaterally absent N20 SSEP wave (1)
Yes
No
Indeterminate outcome Observe and re-evaluate
No
Exclude confounders, particularly residual sedation
Unconscious patient, M=1-2 at ≥72h after ROSC
Rewarming
Days 1-2
Days 3-5
EEG
- N
SE
Poor outcome likely
Yes
Controlled temperature
Cardiac arrest
SSEP
Stat
us
Myo
clo
nu
s
Use multimodal prognostication whenever possible
CT
Wait at least 24h
Mag
net
ic R
eso
nan
ce Im
agin
g (M
RI)

Dallas 2015
Next Steps
Consideration of interim statement
Person responsible
Due date