als 713: prognostication in normothermia · dallas 2015 tfqo: clifton callaway (coi #214) evrevs:...
TRANSCRIPT

Dallas 2015
TFQO: Clifton Callaway (COI #214)
EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35)
Taskforce: ALS
ALS 713: Prognostication in Normothermia
Dallas 2015 COI Disclosure (specific to this systematic review)
Commercial/industry
Claudio Sandroni: none
Tobias Cronberg: none
Potential intellectual conflicts Claudio Sandroni: first author of two systematic reviews on prognostication after cardiac arrest and of the ERC-ESICM Advisory Statement on prognostication in comatose survivors of cardiac arrest
Tobias Cronberg: author of the ERC-ESICM Advisory Statement on
prognostication in comatose survivors of cardiac arrest
Dallas 2015
2010 CoSTR
ALS-PA-041A (Clinical Examination)
ALS-PA-051A (Electrophysiology)
ALS-PA-052A-B (Biomarkers)
ALS-PA-059 (Imaging)
Dallas 2015
2010 Clinical Examination
The following parameters predicted poor outcome (CPC 3 or 4, or death) with a false-positive rate (FPR) of 0%:
absent vestibulo-ocular reflexes at 24 h [(95%CI 0%-14%)] (LOE P1)
absence of pupillary light and corneal reflex at 72 h (95% CI 0% to 9%) (LOE P1)
GCS <5 at 48 h (95% CI 0% - 13%) (LOE P1) and on day 3 (95% CI 0% - 6%) (LOE P2)
a clinical examination score<15 on day 4 [(95%CI 0% -18%) (LOE P1)
However, in 1 study an absent motor response (GCS motor =1) at 72 h after cardiac arrest predicted poor outcome with a FPR of 5% [(95%CI 2% to 9%] (LOE P1)
The presence of myoclonus status in adults was strongly associated with poor outcome (LOE P1; LOE P3; LOE P4), but rare cases of good neurological recovery have been described and accurate diagnosis was problematic.
Dallas 2015
2010 Clinical Examination
Treatment Recommendations There are no clinical neurologic signs that reliably predict poor outcome <24 hours after cardiac arrest.
In adult patients who are comatose after cardiac arrest, have not been treated with hypothermia and have no confounding factors (e.g., hypotension, sedatives or neuromuscular blockers), the absence of both pupillary light and corneal reflex at 72 hours reliably predicts poor outcome.
Absence of vestibulo-ocular reflexes at 24 hours and a GCS motor score of 2 or less at 72 hours are less reliable.
Other clinical signs, including myoclonus, are not recommended for predicting poor outcome

Dallas 2015
2010 Clinical Examination
Knowledge Gaps
The reevaluation of prognostic indicators during therapeutic hypothermia and in the presence of other confounders needs to be completed to guide current post–cardiac arrest care.
Dallas 2015
2010 Electrophysiology
SEP measured between 4 h and 2 weeks after cardiac arrest were associated with poor outcome in 14 studies (LOE P1, P2, P3)
The absence of cortical N20 response to median nerve stimulation at 24 to 72 hours after cardiac arrest predicted poor outcome (CPC 3 or 4, or death) with a FPR of 0.7% (95% CI 0.1 -3.7) (LOE P1)
Electroencephalography predicted poor outcome in comatose survivors of cardiac arrest within 1 week after cardiac arrest in 12 studies (LOE P1, P3, P4, P5).
In a meta-analysis, EEG showing generalized suppression to less than 20 µV, burst-suppression pattern associated with generalized epileptic activity, or diffuse periodic complexes on a flat background 12 to 72 hours after sustained ROSC predicted a poor outcome (FPR of 3%, 95% CI 0.9% to 11%).
Dallas 2015
2010 Electrophysiology
Treatment Recommendations No electrophysiological study reliably predicts outcome of comatose patient after cardiac arrest in the first 24 hours.
After 24 hours, bilateral absence of the N20 cortical response to median nerve stimulation predicts poor outcome in comatose cardiac arrest survivors not treated with therapeutic hypothermia.
In the absence of confounding circumstances, such as sedatives, hypotension, hypothermia, or hypoxemia, it is reasonable to use unprocessed EEG interpretation (specifically identifying generalized suppression to less than 20 µV, burst suppression pattern with generalized epileptic activity, or diffuse periodic complexes on a flat background) observed between 24 and 72 hours after sustained ROSC to assist the prediction of a poor outcome in comatose survivors of cardiac arrest not treated with hypothermia.

Dallas 2015
2010 Electrophysiology
Knowledge Gaps More data are needed about the performance and timing of somatosensory evoked potentials and electroencephalography criteria for aiding prognostication in patients treated with induced hypothermia.
Dallas 2015
2010 Biomarkers
Serum neuronal-specific enolase (NSE) elevations are associated with poor outcome for comatose patients after cardiac arrest (LOE P1; LOE P2; LOE P3).
Although specific cutoff values with a FPR of 0% have been reported, clinical application is limited due to variability in the 0% FPR cutoff values reported among various studies.
Serum S100 elevations are associated with poor outcome for comatose patients after cardiac arrest (LOE P1; LOE P2; LOE P3)
Worse outcomes for comatose survivors of cardiac arrest are also associated with increased levels of cerebrospinal fluid (CSF)-CK (LOE P2), CKBB (LOE P1; LOE P2; LOE P3). However, 1 study found no relationship between cerebrospinal fluid-CKBB and prognosis (LOE P2).
Outcomes are also associated with increased cerebrospinal fluid levels of other markers including NSE (LOE P1; LOE P2; S100 (LOE P2); LDH, GOT (LOE P2); neurofilament (LOE P3); and acid phosphatase and lactate (LOE P2).
Dallas 2015
2010 Biomarkers
Treatment Recommendations Evidence does not support the use of serum or cerebrospinal fluid biomarkers alone as predictors of poor outcomes in comatose patients after cardiac arrest with or without treatment with therapeutic hypothermia.
Limitations included small numbers of patients and/or inconsistency in cutoff values for predicting poor outcome.
Dallas 2015
2010 Biomarkers
Knowledge Gaps Future studies should identify and resolve the heterogeneity of cutoff values used to predict poor outcome with a FPR of zero.
Studies also must account for confounders that may alter levels or predictive performance of various markers (eg, hypothermia, underlying disease, pregnancy, intra-aortic balloon pump, brain instrumentation, hemodialyisis, or other organ failure).
Studies examining whether biomarkers can be used to monitor ongoing injury and response to therapy may be useful.
Dallas 2015
2010 Imaging
MRI There are no LOE P1-P2-studies that support the use of MRI.
In 32 studies (P3-P5) the timing of MRI ranged from 1 day to 10 months after ROSC.
Overall these studies were limited by small sample sizes, variable time of imaging (many very late in the course of the event), lack of comparison with a standardized method of prognostication, often nonmodern MRI techniques, and early withdrawal of care.
Dallas 2015
2010 Imaging
CT There are no LOE P1-P2-studies that support the use of CT.
In 22 studies (P3-P5) the timing of MRI ranged from 1 h to 20 days after ROSC.
Overall these studies were limited by small sample sizes, variable time of imaging (many very late in the course of the event), lack of comparison with a standardized method of prognostication, and early withdrawal of care.
Dallas 2015
2010 Imaging
Treatment Recommendations There is insufficient evidence to recommend for or against the routine use of neuroimaging to predict outcome of adult cardiac arrest survivors.
Knowledge Gaps Adequately powered prospective studies are required to evaluate the accuracy of CT, MRI, or both in prognosticating outcome of comatose cardiac arrest survivors.
Outcome prediction should include a comparison with more conventional methods.
All studies should allow for sufficient time to realize patient recovery, avoiding the bias of self-fulfilling prophecy and premature withdrawal of care.
Dallas 2015
C2015 PICO
Population: Adults with ROSC who are not treated with targeted temperature management (TTM)
Intervention: any clinical variable when normal (e.g. 1. Clinical Exam, 2. EEG, 3. SSEP, 4. Imaging, 5. Other)
Comparison: any clinical variable when abnormal
Outcomes Survival with Favorable neurological or functional outcome at discharge, 30 days, 60 days, 180 days AND/OR 1 year, Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year
Dallas 2015 Inclusion/Exclusion & Articles Found
Inclusion: adult (≥16 years) pts, comatose (unconscious, unresponsive, or GCS≤8)
Exclusion: Studies including pts. in hypoxic coma from causes other than CA (e.g., respiratory arrest, CO poisoning) except when a subpopulation of cardiac arrest patients could be evaluated separately.
Included: 46 articles
Dallas 2015 2015 Proposed Treatment Recommendations
Clinical Examination - 1
We recommend using the absence of pupillary reflex to light (or the combined absence of both pupillary and corneal reflexes) at ≥72h from ROSC to predict poor outcome.
We suggest against using an absent or extensor motor response to pain (M≤2) alone to predict poor outcome, given its high false positive rate. However, due to its high sensitivity, this sign may be used to identify the population with poor neurological status needing prognostication or to predict poor outcome in combination with other more robust predictors.
Dallas 2015 2015 Proposed Treatment Recommendations
Clinical Examination - 2
We suggest using the presence of a status myoclonus within 72 h from ROSC in combination with other predictors for prognosticating a poor neurological outcome.
We suggest prolonging the observation of clinical signs when interference from residual sedation or paralysis is suspected, so that the possibility of obtaining false positive results is minimized.
Dallas 2015 2015 Proposed Treatment Recommendations
Electrophysiology
We recommend using bilateral absence of N20 SSEP wave at ≥24h after ROSC to predict poor outcome.
We suggest using the presence of burst-suppression on EEG at 72h from ROSC in combination with other predictors for prognosticating a poor neurological outcome.
We suggest against using EEG grades due to the inconsistencies in their definitions.
We also do not suggest using low-voltage EEG given the potential interferences of technical factors on EEG amplitude.
Dallas 2015 2015 Proposed Treatment Recommendations
Biomarkers
We suggest using high serum values of NSE at 24-72 h from ROSC in combination with other predictors for prognosticating a poor neurological outcome. However, no threshold enabling prediction with zero FPR can be recommended.
We suggest using utmost care and preferably sampling at multiple time-points when assessing NSE, to avoid false positive results due to hemolysis.
Dallas 2015 2015 Proposed Treatment Recommendations
Imaging
We suggest using the presence of a marked reduction of the GM/WM ratio on brain CT within 48 h after ROSC or the presence of extensive reduction in diffusion on brain MRI at 2-6 days after ROSC in combination with other predictors for prognosticating a poor neurological outcome.
We suggest using brain imaging studies for prognostication only in centers where specific experience is available.
Dallas 2015
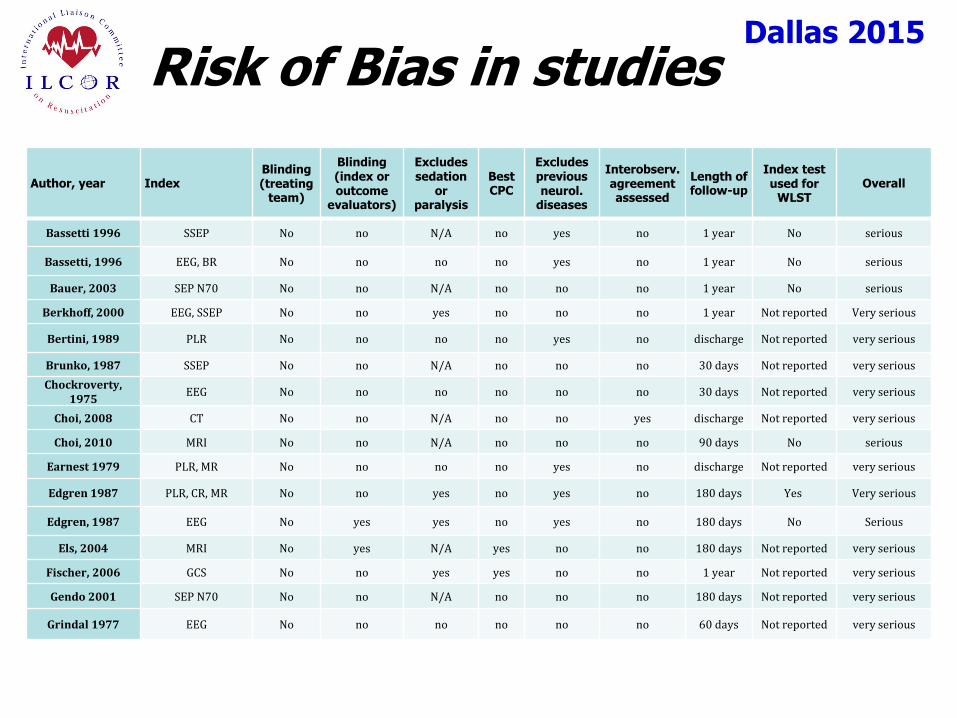
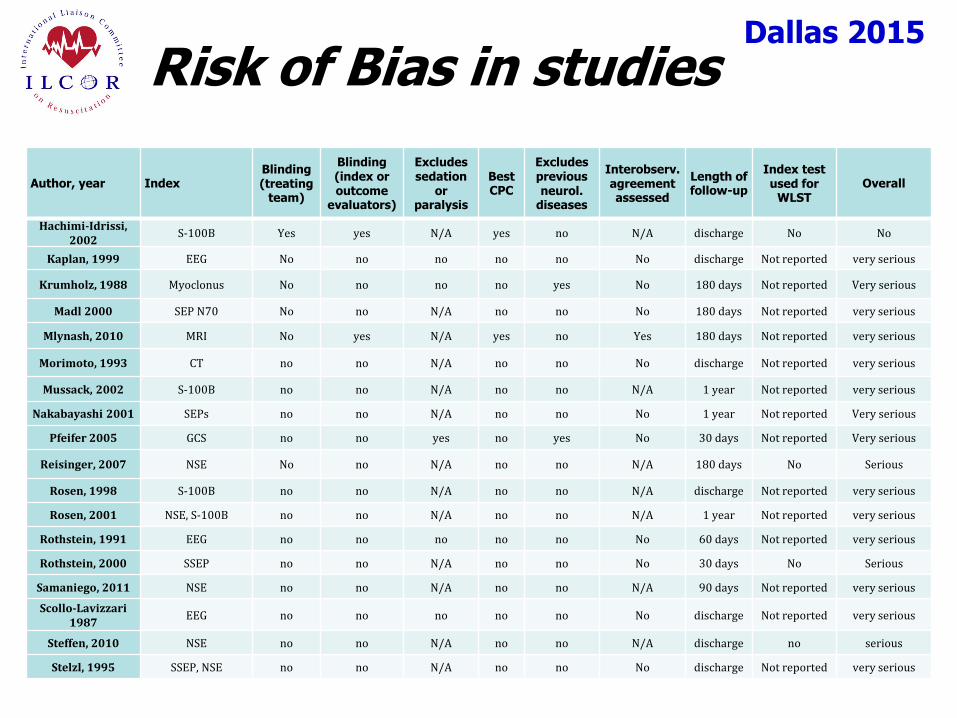
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Bassetti 1996 SSEP No no N/A no yes no 1 year No serious
Bassetti, 1996 EEG, BR No no no no yes no 1 year No serious
Bauer, 2003 SEP N70 No no N/A no no no 1 year No serious
Berkhoff, 2000 EEG, SSEP No no yes no no no 1 year Not reported Very serious
Bertini, 1989 PLR No no no no yes no discharge Not reported very serious
Brunko, 1987 SSEP No no N/A no no no 30 days Not reported very serious
Chockroverty, 1975
EEG No no no no no no 30 days Not reported very serious
Choi, 2008 CT No no N/A no no yes discharge Not reported very serious
Choi, 2010 MRI No no N/A no no no 90 days No serious
Earnest 1979 PLR, MR No no no no yes no discharge Not reported very serious
Edgren 1987 PLR, CR, MR No no yes no yes no 180 days Yes Very serious
Edgren, 1987 EEG No yes yes no yes no 180 days No Serious
Els, 2004 MRI No yes N/A yes no no 180 days Not reported very serious
Fischer, 2006 GCS No no yes yes no no 1 year Not reported very serious
Gendo 2001 SEP N70 No no N/A no no no 180 days Not reported very serious
Grindal 1977 EEG No no no no no no 60 days Not reported very serious
Dallas 2015
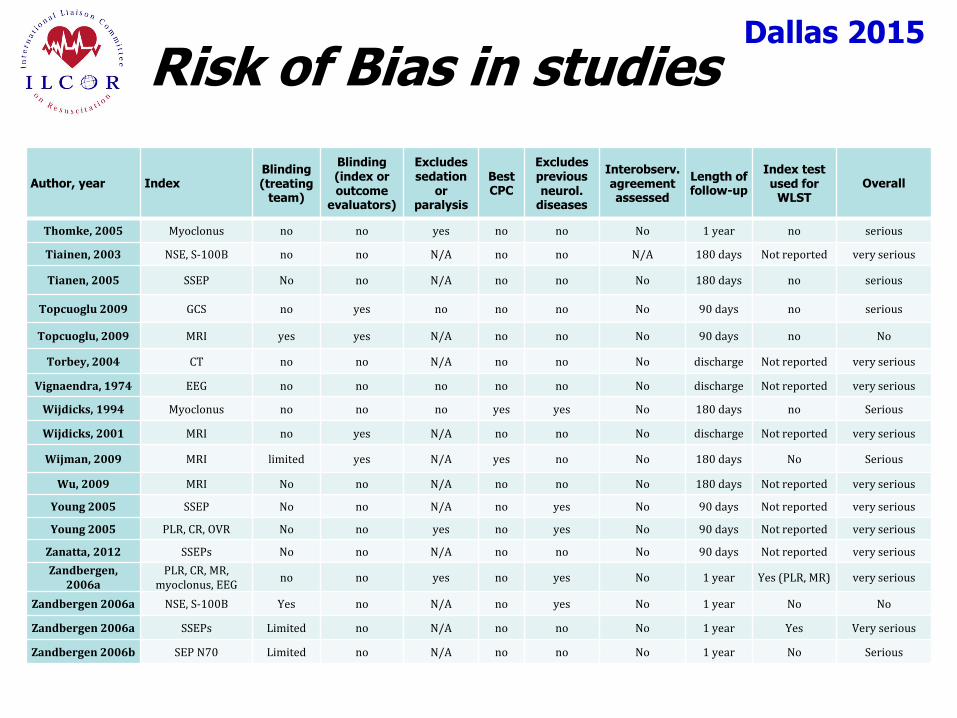
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Hachimi-Idrissi, 2002
S-100B Yes yes N/A yes no N/A discharge No No
Kaplan, 1999 EEG No no no no no No discharge Not reported very serious
Krumholz, 1988 Myoclonus No no no no yes No 180 days Not reported Very serious
Madl 2000 SEP N70 No no N/A no no No 180 days Not reported very serious
Mlynash, 2010 MRI No yes N/A yes no Yes 180 days Not reported very serious
Morimoto, 1993 CT no no N/A no no No discharge Not reported very serious
Mussack, 2002 S-100B no no N/A no no N/A 1 year Not reported very serious
Nakabayashi 2001 SEPs no no N/A no no No 1 year Not reported Very serious
Pfeifer 2005 GCS no no yes no yes No 30 days Not reported Very serious
Reisinger, 2007 NSE No no N/A no no N/A 180 days No Serious
Rosen, 1998 S-100B no no N/A no no N/A discharge Not reported very serious
Rosen, 2001 NSE, S-100B no no N/A no no N/A 1 year Not reported very serious
Rothstein, 1991 EEG no no no no no No 60 days Not reported very serious
Rothstein, 2000 SSEP no no N/A no no No 30 days No Serious
Samaniego, 2011 NSE no no N/A no no N/A 90 days Not reported very serious
Scollo-Lavizzari 1987
EEG no no no no no No discharge Not reported very serious
Steffen, 2010 NSE no no N/A no no N/A discharge no serious
Stelzl, 1995 SSEP, NSE no no N/A no no No discharge Not reported very serious
Dallas 2015
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Thomke, 2005 Myoclonus no no yes no no No 1 year no serious
Tiainen, 2003 NSE, S-100B no no N/A no no N/A 180 days Not reported very serious
Tianen, 2005 SSEP No no N/A no no No 180 days no serious
Topcuoglu 2009 GCS no yes no no no No 90 days no serious
Topcuoglu, 2009 MRI yes yes N/A no no No 90 days no No
Torbey, 2004 CT no no N/A no no No discharge Not reported very serious
Vignaendra, 1974 EEG no no no no no No discharge Not reported very serious
Wijdicks, 1994 Myoclonus no no no yes yes No 180 days no Serious
Wijdicks, 2001 MRI no yes N/A no no No discharge Not reported very serious
Wijman, 2009 MRI limited yes N/A yes no No 180 days No Serious
Wu, 2009 MRI No no N/A no no No 180 days Not reported very serious
Young 2005 SSEP No no N/A no yes No 90 days Not reported very serious
Young 2005 PLR, CR, OVR No no yes no yes No 90 days Not reported very serious
Zanatta, 2012 SSEPs No no N/A no no No 90 days Not reported very serious
Zandbergen, 2006a
PLR, CR, MR, myoclonus, EEG
no no yes no yes No 1 year Yes (PLR, MR) very serious
Zandbergen 2006a NSE, S-100B Yes no N/A no yes No 1 year No No
Zandbergen 2006a SSEPs Limited no N/A no no No 1 year Yes Very serious
Zandbergen 2006b SEP N70 Limited no N/A no no No 1 year No Serious
Dallas 2015
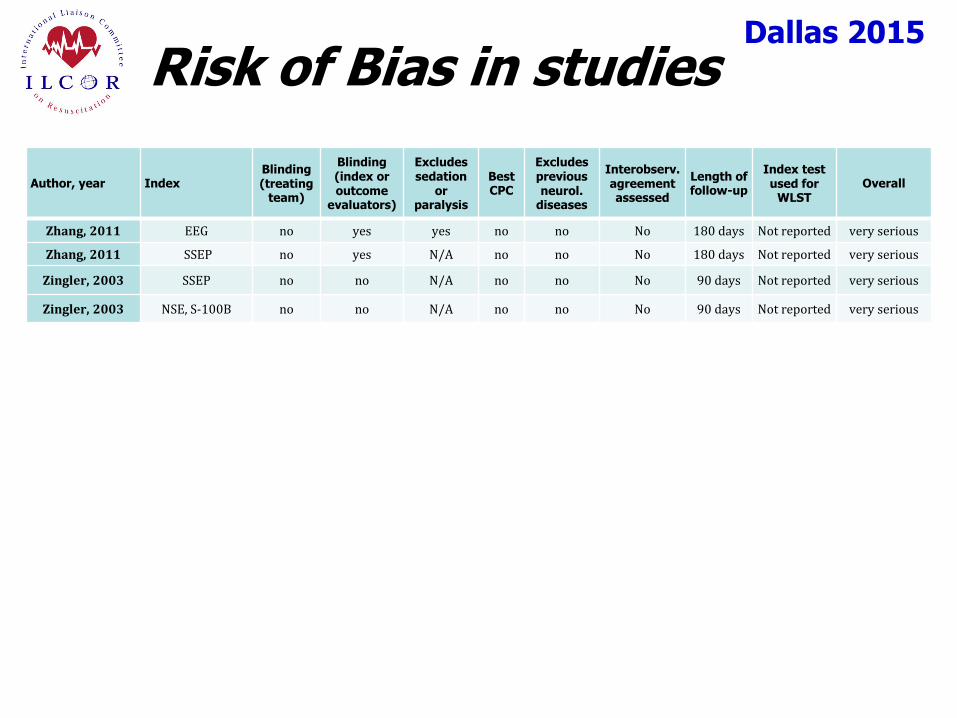
Risk of Bias in studies
Author, year Index Blinding (treating
team)
Blinding (index or outcome
evaluators)
Excludes sedation
or paralysis
Best CPC
Excludes previous neurol.
diseases
Interobserv. agreement assessed
Length of follow-up
Index test used for
WLST Overall
Zhang, 2011 EEG no yes yes no no No 180 days Not reported very serious
Zhang, 2011 SSEP no yes N/A no no No 180 days Not reported very serious
Zingler, 2003 SSEP no no N/A no no No 90 days Not reported very serious
Zingler, 2003 NSE, S-100B no no N/A no no No 90 days Not reported very serious
Dallas 2015
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 4 studies on brainstem reflexes, motor response, or myoclonus (650 patients, low or very low QOE)
For the critical outcome of survival with unfavorable neurological status or death at one year, we identified 2 studies on brainstem reflexes, motor response, GCS, or myoclonus (172 patients, very low QOE)
Clinical Examination - 1
Dallas 2015
Clinical Examination - 2
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified two studies on pupillary reflex and motor response or oculocephalic reflex (151 patients, very low QOE)
For the critical outcome of survival with unfavorable neurological status or death at 30 days, we identified one study on GCS (97 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified two studies on corneal reflex, pupillary reflex, motor response, oculovestibular reflex, GCS, or myoclonus (97 patients, very low QOE).
Dallas 2015
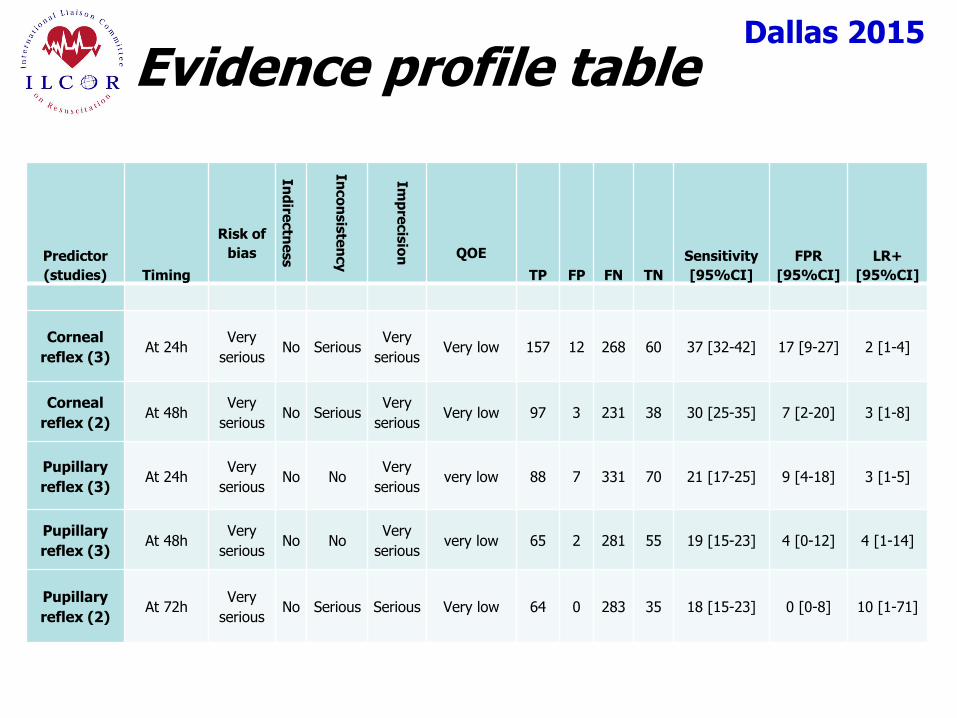
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Corneal
reflex (3) At 24h
Very
serious No Serious
Very
serious Very low 157 12 268 60 37 [32-42] 17 [9-27] 2 [1-4]
Corneal
reflex (2) At 48h
Very
serious No Serious
Very
serious Very low 97 3 231 38 30 [25-35] 7 [2-20] 3 [1-8]
Pupillary
reflex (3) At 24h
Very
serious No No
Very
serious very low 88 7 331 70 21 [17-25] 9 [4-18] 3 [1-5]
Pupillary
reflex (3) At 48h
Very
serious No No
Very
serious very low 65 2 281 55 19 [15-23] 4 [0-12] 4 [1-14]
Pupillary
reflex (2) At 72h
Very
serious No Serious Serious Very low 64 0 283 35 18 [15-23] 0 [0-8] 10 [1-71]
Dallas 2015
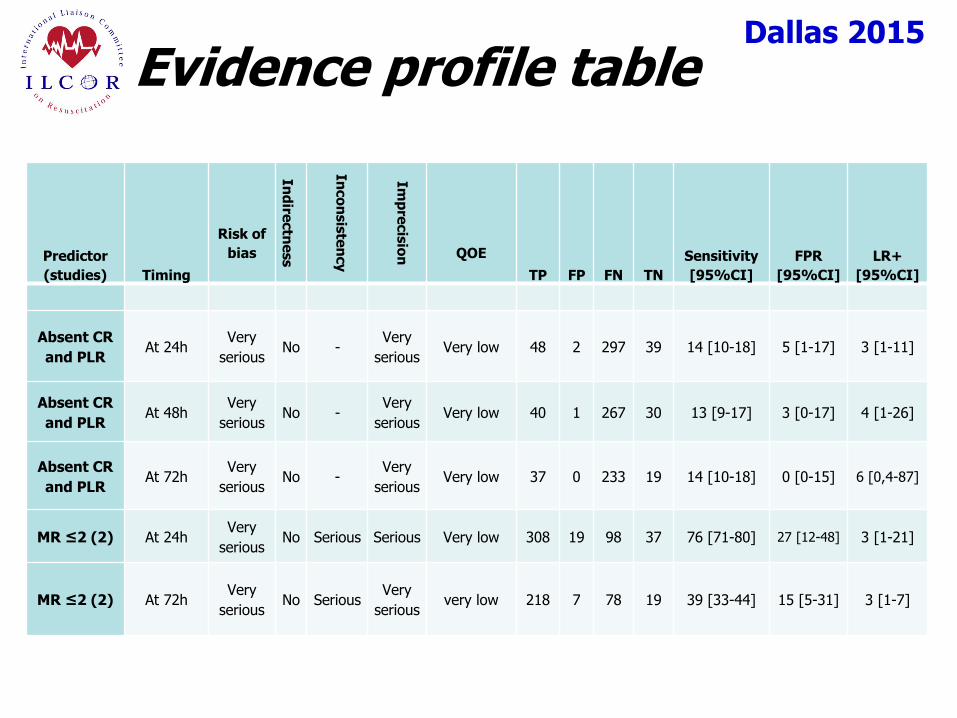
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Absent CR
and PLR At 24h
Very
serious No -
Very
serious Very low 48 2 297 39 14 [10-18] 5 [1-17] 3 [1-11]
Absent CR
and PLR At 48h
Very
serious No -
Very
serious Very low 40 1 267 30 13 [9-17] 3 [0-17] 4 [1-26]
Absent CR
and PLR At 72h
Very
serious No -
Very
serious Very low 37 0 233 19 14 [10-18] 0 [0-15] 6 [0,4-87]
MR ≤2 (2) At 24h Very
serious No Serious Serious Very low 308 19 98 37 76 [71-80] 27 [12-48] 3 [1-21]
MR ≤2 (2) At 72h Very
serious No Serious
Very
serious very low 218 7 78 19 39 [33-44] 15 [5-31] 3 [1-7]
Dallas 2015 2015 Proposed Treatment Recommendations
Clinical Examination - 1
We recommend using the absence of pupillary reflex to light (or the combined absence of both pupillary and corneal reflexes) at ≥72h from ROSC to predict poor outcome (strong recommendation, QOE very low).
We suggest against using an absent or extensor motor response to pain (M≤2) alone to predict poor outcome, given its high false positive rate (weak recommendation, QOE very low). However, due to its high sensitivity, this sign may be used to identify the population with poor neurological status needing prognostication or to predict poor outcome in combination with other more robust predictors.
Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
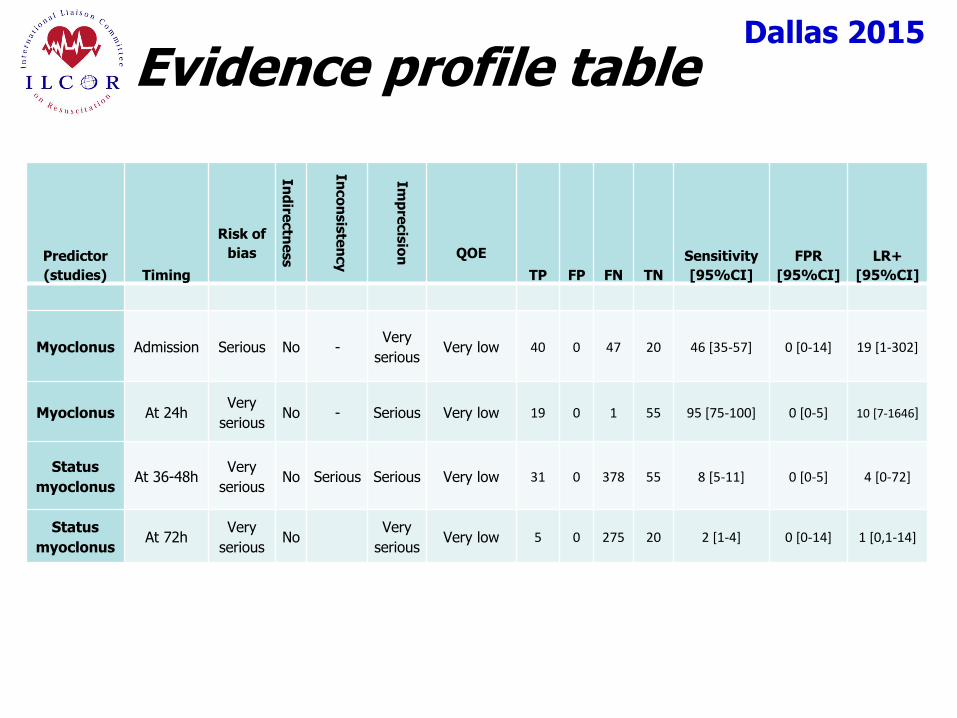
Myoclonus Admission Serious No - Very
serious Very low 40 0 47 20 46 [35-57] 0 [0-14] 19 [1-302]
Myoclonus At 24h Very
serious No - Serious Very low 19 0 1 55 95 [75-100] 0 [0-5] 10 [7-1646]
Status
myoclonus At 36-48h
Very
serious No Serious Serious Very low 31 0 378 55 8 [5-11] 0 [0-5] 4 [0-72]
Status
myoclonus At 72h
Very
serious No
Very
serious Very low 5 0 275 20 2 [1-4] 0 [0-14] 1 [0,1-14]
Dallas 2015 2015 Proposed Treatment Recommendations
Clinical Examination - 2
We suggest using the presence of a status myoclonus within 72 h from ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, QOE very low).
We suggest prolonging the observation of clinical signs when interference from residual sedation or paralysis is suspected, so that the possibility of obtaining false positive results is minimized.
Dallas 2015
Knowledge Gaps
Prospective studies are needed to investigate:
the pharmacokinetics of sedative and NMB drugs
the reproducibility of clinical signs used to predict
outcome.
There is no universally accepted definition of status myoclonus
Recently proposed definition = generalised myoclonus persisting for ≥30 minutes.
Dallas 2015
Electrophysiology - 1
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 2 studies on short-latency somatosensory evoked potentials (SSEP) (63 patients, very low QOE) and 3 studies on EEG (46 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 30 days, we identified 2 studies on SSEP (80 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 60 days we identified 2 studies on EEG (54 patients, very low QOE).
Dallas 2015
Electrophysiology - 2
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified 2 studies on SSEP or EEG (102 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 6 studies on SSEP, SEP or EEG (733 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 1 year, we identified 6 studies on SSEP or EEG (829 patients, low or very low QOE).

Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Absent N20
SSEP (4) At 24h
very
serious no serious no very low 156 0 206 92 43 [38-48] 0 [0-3] 24 [6-93]
Absent N20
SSEP (4) At 48h
very
serious no serious serious very low 125 0 145 58 46 [40-52] 0 [0-5] 11 [3-43]
Absent N20
SSEP (2) At 72h serious no serious serious very low 120 0 140 33 46 [40-52] 0 [0-9] 18 [3-122]
Absent N20
SSEP (3) At 12-72h
very
serious no serious serious very low 138 1 170 99 45 [39-51] 1 [0-5] 17 [4-65]
Dallas 2015
Evidence profile table
Predictor
(studies) Timing
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
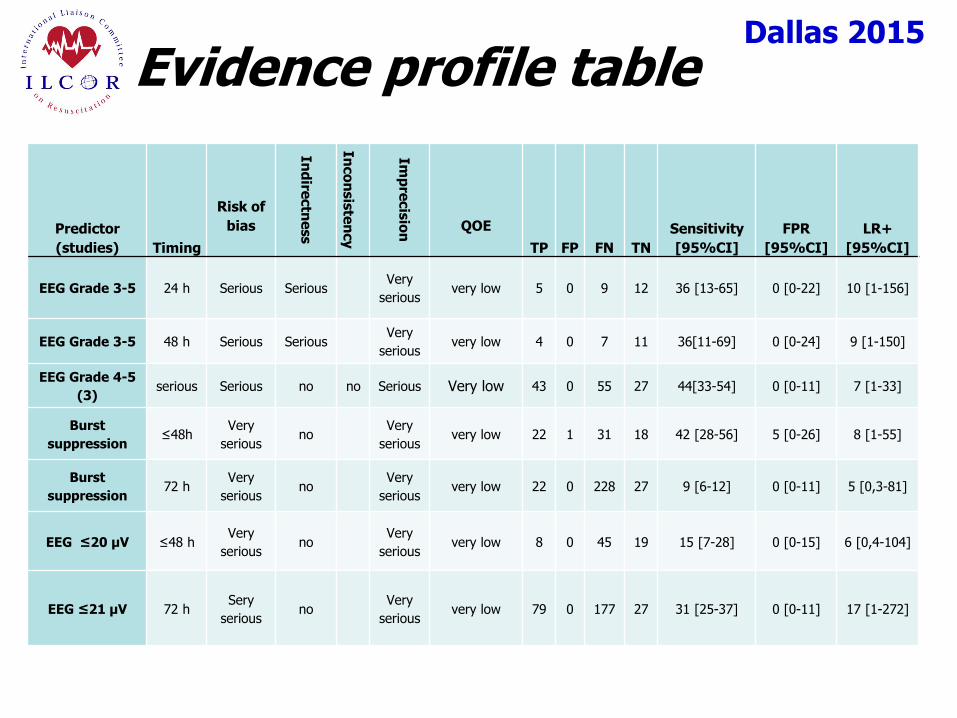
EEG Grade 3-5 24 h Serious Serious Very
serious very low 5 0 9 12 36 [13-65] 0 [0-22] 10 [1-156]
EEG Grade 3-5 48 h Serious Serious Very
serious very low 4 0 7 11 36[11-69] 0 [0-24] 9 [1-150]
EEG Grade 4-5
(3) serious Serious no no Serious Very low 43 0 55 27 44[33-54] 0 [0-11] 7 [1-33]
Burst
suppression ≤48h
Very
serious no
Very
serious very low 22 1 31 18 42 [28-56] 5 [0-26] 8 [1-55]
Burst
suppression 72 h
Very
serious no
Very
serious very low 22 0 228 27 9 [6-12] 0 [0-11] 5 [0,3-81]
EEG ≤20 µV ≤48 h Very
serious no
Very
serious very low 8 0 45 19 15 [7-28] 0 [0-15] 6 [0,4-104]
EEG ≤21 µV 72 h Sery
serious no
Very
serious very low 79 0 177 27 31 [25-37] 0 [0-11] 17 [1-272]
Dallas 2015 2015 Proposed Treatment Recommendations
Electrophysiology
We recommend using bilateral absence of N20 SSEP wave at ≥24h after ROSC to predict poor outcome (strong recommendation, QOE very low).
We suggest using the presence of burst-suppression on EEG at 72h from ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, QOE very low).
We suggest against using EEG grades due to the inconsistencies in their definitions (weak recommendation, QOE very low).
We also do not suggest using low-voltage EEG, given the potential interferences of technical factors on EEG amplitude (weak recommendation, QOE very low).

Dallas 2015
Knowledge Gaps
In most prognostication studies on TTM-treated patients, SSEPs have been used as a criterion for WLST
Blinded studies are needed to assess the relevance of self-fulfilling prophecy for SSEPs.
Definitions of EEG-based predictors are inconsistent among prognostication studies.
Future studies should comply with recently recommended definitions (e.g. Hirsch and coll., 2013).
Dallas 2015
Biomarkers
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 2 studies on S-100B (99 patients, low or very low QOE) and 1 study on NSE (73 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified 1 study on NSE (32 patients, very low QOE) and 1 study on S-100B (27 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 3 studies on NSE or S-100B (618 patients; moderate, low or very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at one year, we identified 2 studies on NSE or S-100B (86 patients, very low QOE)
Dallas 2015
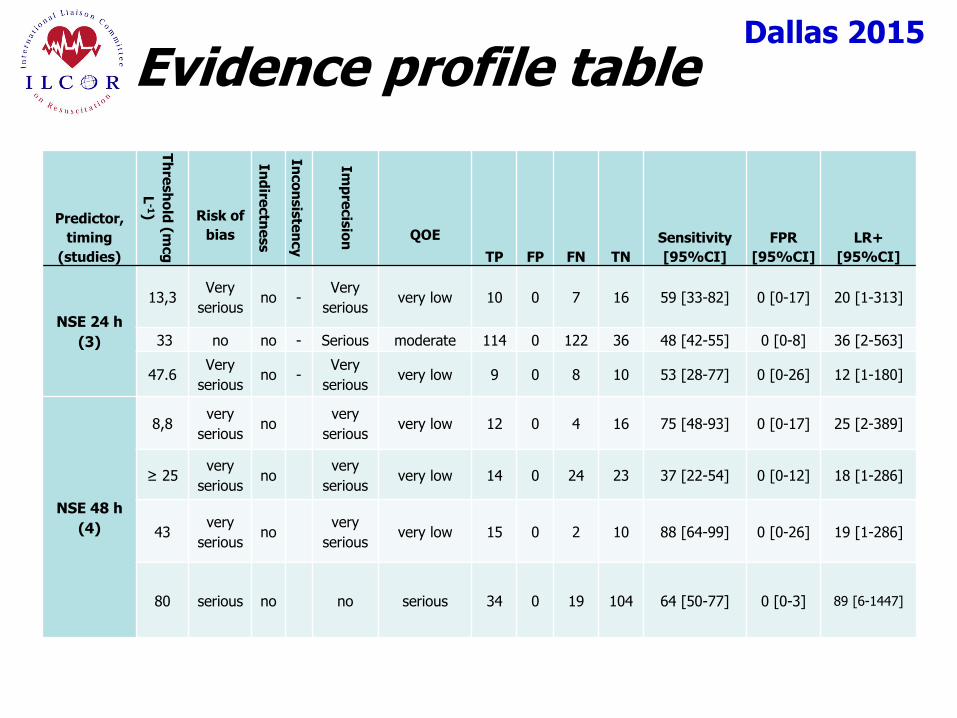
Evidence profile table
Predictor,
timing
(studies)
Th
resh
old
(mcg
L-1) Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
NSE 24 h
(3)
13,3 Very
serious no -
Very
serious very low 10 0 7 16 59 [33-82] 0 [0-17] 20 [1-313]
33 no no - Serious moderate 114 0 122 36 48 [42-55] 0 [0-8] 36 [2-563]
47.6 Very
serious no -
Very
serious very low 9 0 8 10 53 [28-77] 0 [0-26] 12 [1-180]
NSE 48 h
(4)
8,8 very
serious no
very
serious very low 12 0 4 16 75 [48-93] 0 [0-17] 25 [2-389]
≥ 25 very
serious no
very
serious very low 14 0 24 23 37 [22-54] 0 [0-12] 18 [1-286]
43 very
serious no
very
serious very low 15 0 2 10 88 [64-99] 0 [0-26] 19 [1-286]
80 serious no no serious 34 0 19 104 64 [50-77] 0 [0-3] 89 [6-1447]
Dallas 2015
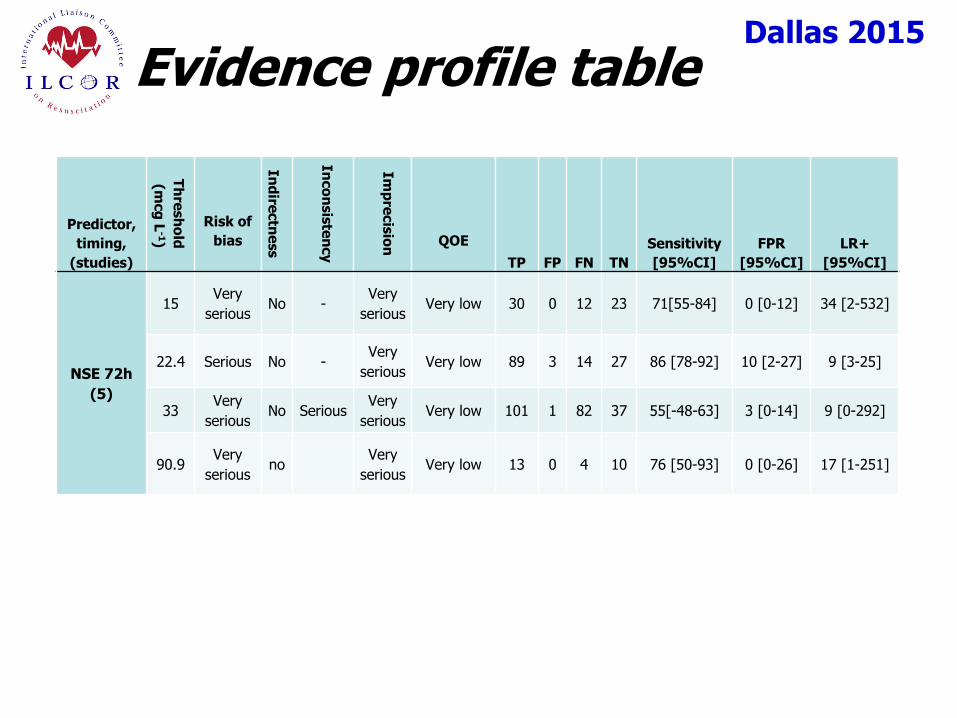
Evidence profile table
Predictor,
timing,
(studies)
Th
resh
old
(mcg
L-1)
Risk of
bias
In
dire
ctn
ess
In
co
nsis
ten
cy
Im
pre
cis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
NSE 72h
(5)
15 Very
serious No -
Very
serious Very low 30 0 12 23 71[55-84] 0 [0-12] 34 [2-532]
22.4 Serious No - Very
serious Very low 89 3 14 27 86 [78-92] 10 [2-27] 9 [3-25]
33 Very
serious No Serious
Very
serious Very low 101 1 82 37 55[-48-63] 3 [0-14] 9 [0-292]
90.9 Very
serious no
Very
serious Very low 13 0 4 10 76 [50-93] 0 [0-26] 17 [1-251]
Dallas 2015 2015 Proposed Treatment Recommendations
Biomarkers
We suggest using high serum values of NSE at 24-72 h from ROSC in combination with other predictors for prognosticating a poor neurological outcome. However, no threshold enabling prediction with zero FPR can be recommended (weak recommendation, QOE very low).
We suggest using utmost care and preferably sampling at multiple time-points when assessing NSE, to avoid false positive results due to hemolysis.

Dallas 2015
Knowledge Gaps
There is a need for standardisation of the measuring techniques for NSE and S-100 in cardiac arrest patients.
Little information is available on the kinetics of the blood concentrations of biomarkers in the first few days after cardiac arrest.
Dallas 2015
Imaging
For the critical outcome of survival with unfavorable neurological status or death at discharge, we identified 3 studies on CT (113 patients, very low QOE) and 2 studies on MRI (40 patients, very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 90 days, we identified 2 studies on MRI (61 patients, low or very low QOE).
For the critical outcome of survival with unfavorable neurological status or death at 180 days, we identified 3 studies on MRI (34 patients, very low QOE).
Dallas 2015
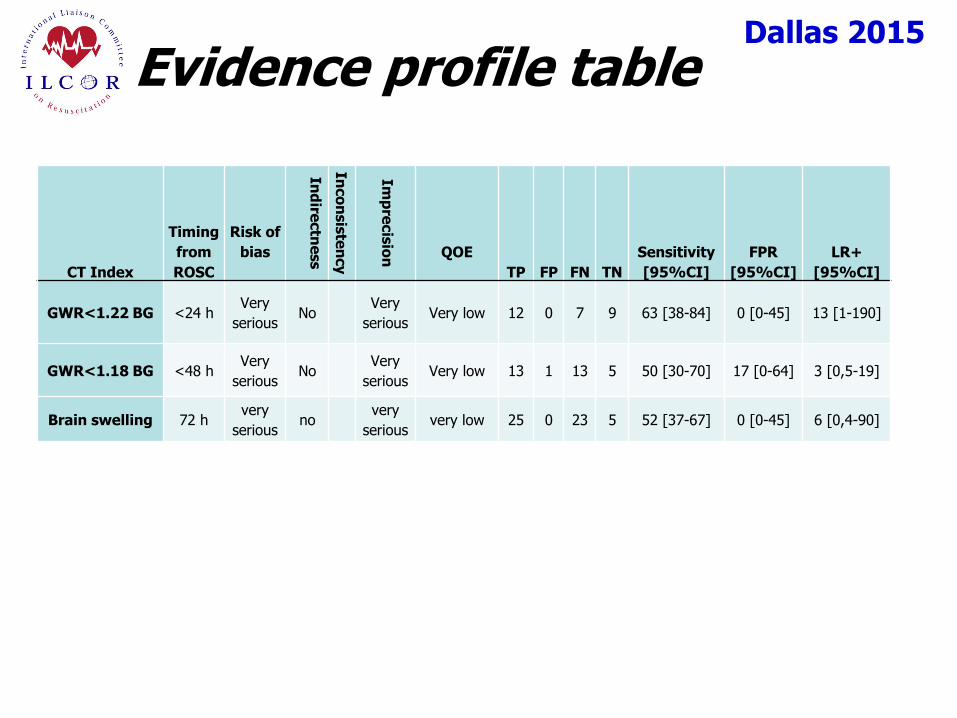
Evidence profile table
CT Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
GWR<1.22 BG <24 h Very
serious No
Very
serious Very low 12 0 7 9 63 [38-84] 0 [0-45] 13 [1-190]
GWR<1.18 BG <48 h Very
serious No
Very
serious Very low 13 1 13 5 50 [30-70] 17 [0-64] 3 [0,5-19]
Brain swelling 72 h very
serious no
very
serious very low 25 0 23 5 52 [37-67] 0 [0-45] 6 [0,4-90]
Dallas 2015
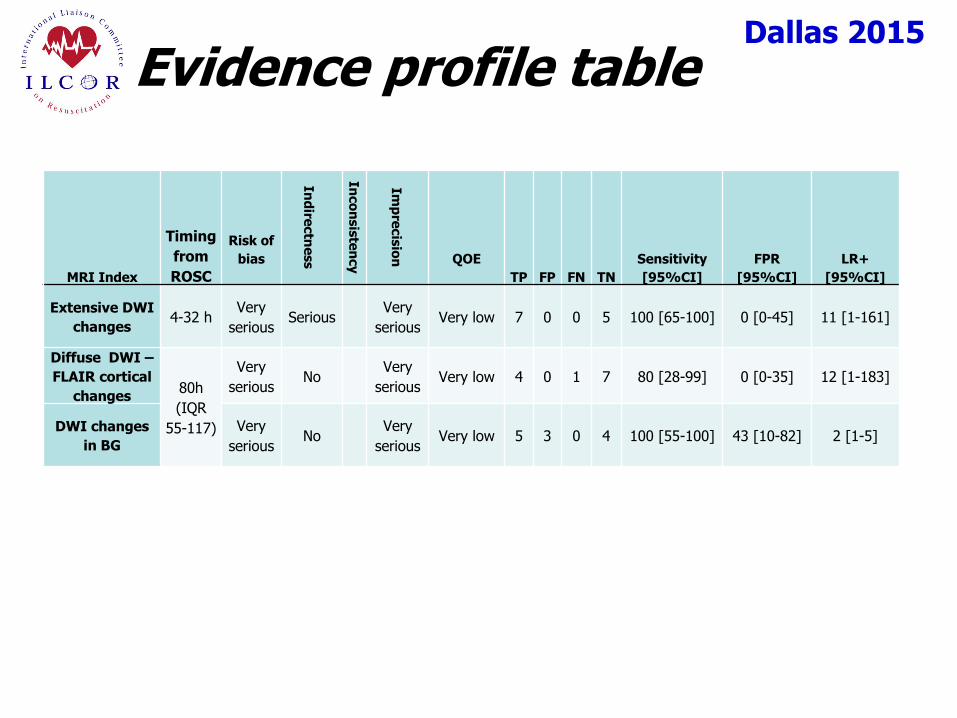
Evidence profile table
MRI Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Extensive DWI
changes 4-32 h
Very
serious Serious
Very
serious Very low 7 0 0 5 100 [65-100] 0 [0-45] 11 [1-161]
Diffuse DWI –
FLAIR cortical
changes 80h
(IQR
55-117)
Very
serious No
Very
serious Very low 4 0 1 7 80 [28-99] 0 [0-35] 12 [1-183]
DWI changes
in BG
Very
serious No
Very
serious Very low 5 3 0 4 100 [55-100] 43 [10-82] 2 [1-5]
Dallas 2015
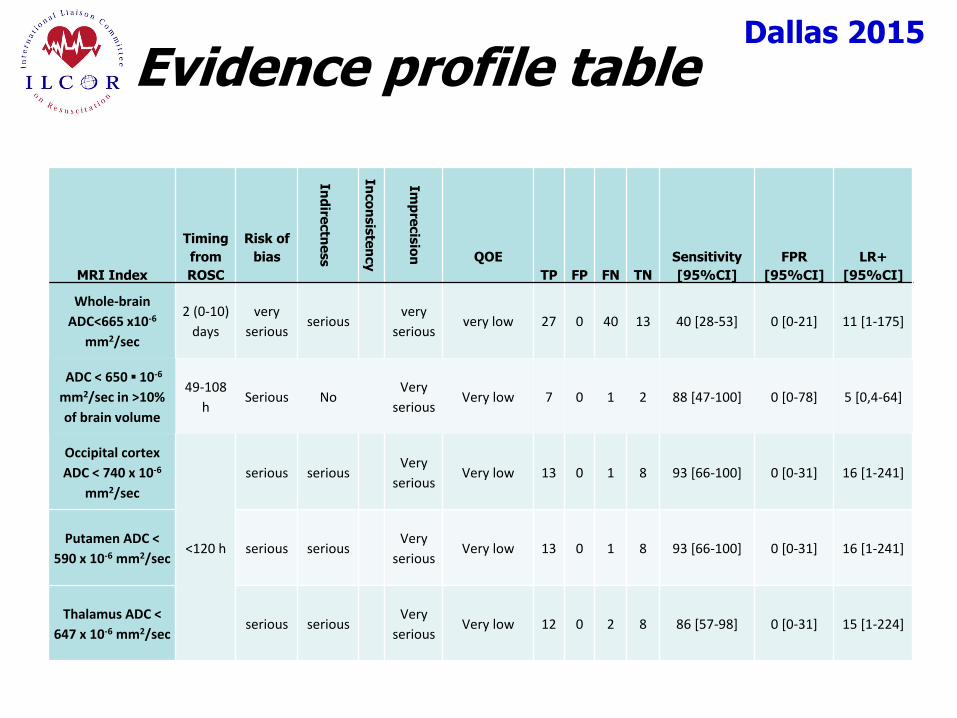
Evidence profile table
MRI Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Whole-brain
ADC<665 x10-6
mm2/sec
2 (0-10)
days
very
serious serious
very
serious very low 27 0 40 13 40 [28-53] 0 [0-21] 11 [1-175]
ADC < 650 ▪ 10-6
mm2/sec in >10%
of brain volume
49-108
h Serious No
Very
serious Very low 7 0 1 2 88 [47-100] 0 [0-78] 5 [0,4-64]
Occipital cortex
ADC < 740 x 10-6
mm2/sec
<120 h
serious serious Very
serious Very low 13 0 1 8 93 [66-100] 0 [0-31] 16 [1-241]
Putamen ADC <
590 x 10-6 mm2/sec serious serious
Very
serious Very low 13 0 1 8 93 [66-100] 0 [0-31] 16 [1-241]
Thalamus ADC <
647 x 10-6 mm2/sec serious serious
Very
serious Very low 12 0 2 8 86 [57-98] 0 [0-31] 15 [1-224]

Dallas 2015
Evidence profile table
MRI Index
Timing
from
ROSC
Risk of
bias
Ind
irectn
ess
Inco
nsis
ten
cy
Imp
recis
ion
QOE
TP FP FN TN
Sensitivity
[95%CI]
FPR
[95%CI]
LR+
[95%CI]
Extensive global
FLAIR changes ≤7d
very
serious no
very
serious very low 6 0 0 2 100 [61-100] 0 [0-78] 6 [0,4-71]
Extensive cortical
DWI and FLAIR
changes
≤7d no no very
serious low 13 0 1 2 93 [66-100] 0 [0-78] 5 [0,4-68]

Dallas 2015 2015 Proposed Treatment Recommendations
Imaging
We suggest using the presence of a marked reduction of the GM/WM ratio on brain CT within 48 h after ROSC or the presence of extensive reduction in diffusion on brain MRI at 2-6 days after ROSC in combination with other predictors for prognosticating a poor neurological outcome (weak recommendation, QOE very low).
We suggest using brain imaging studies for prognostication only in centers where specific experience is available.
Dallas 2015
Knowledge Gaps
Prospective studies in unselected patient populations and including inter-rater agreement are needed for evaluating the prognostic accuracy of imaging studies in comatose patients resuscitated from cardiac arrest.
Dallas 2015
Next Steps
Consideration of interim statement
Person responsible
Due date