alk t-lymphoproliferative diseases alk23/10/2017 1 escca 2017, thessaloniki, sep 24-27, 2017 paula...
TRANSCRIPT

23/10/2017
1
ESCCA 2017, Thessaloniki, Sep 24-27, 2017Paula C. Fernandez, MD/PhDInstitute for Laboratory Medicine, Kantonsspital Aarau, Switzerland
T-Lymphoproliferative Diseases
Mature T-cell Leukemias (leukemic/disseminated)
• T-cell prolymphocytic leukemia (T-PLL)• T-cell LGL leukemia (T-LGL)• Chronic LPD of NK cells*• Aggressive NK-cell leukemia• # Systemic EBV+ T-cell lymphoma of childhood• Adult T-cell lymphoma/leukemia (HTLV1+) (ATLL)
• Peripheral T-cell lymphoma, NOS (PTCL-NOS)• # Nodal peripheral T-cell lymphoma w. TFH phenotype *• Angioimmunoblastic T-cell lymphoma (AITL)• # Follicular T-cell lymphoma*• Anaplastic large cell lymphoma, ALK+ (ALK+ALCL)• # Anaplastic large cell lymphoma, ALK- (ALK-ACLCL)
Nodal T-cell Lymphomas
*Provisional entities# change from 2008
• Sézary syndrome (SS)• Mycosis fungoides (MF)• Primary cutaneous CD30+ T-LPD
• Lymphomatoid papulosis• Primary cuteanous ALCL
• Primary cutaneous gd T-cell lymphoma• # Primary cutaneous aggressive epidermotropic
cytotoxic T-cell lymphoma*• # Primary cutaneous acral CD8+ T-cell lymphoma*• # Primary cutaneous CD4+ small/medium LPD*• # Hydroa-vacciniforme-like LPD
Cutaneous T-cell Lymphomas (extranodal)
Mature T- and NK-cell NeoplasmsWHO classification 2016
LPD: lymphoproliferative disorder; TFH: T follicular helper
Extranodal T-cell Lymphomas
• Extranodal NK/T-cell lymphoma, nasal type• Enteropathy-associated T-cell lymphoma (former
EATL type I)• # Monomorphic epitheliotropic intestinal
lymphoma (former EATL type II, now MEITL)• # Indolent LPD of GI-tract*• Hepatosplenic T-cell lymphoma (HSTL)• # Breast-implant-associated anaplastic large cell
lymphoma*• Subcutaneous panniculitis-like T-cell lymphoma
(SPTCL)
• Pediatric-type FL
• Duodenal-type FL
• In situ follicular/mantle cell neoplasia
• EBV+ mucocutaneous ulcer
• *Indolent T/NK‐cell proliferations (GIT, Skin)
• *Breast implant-associated ALCL
• Primary cutaneous CD4+ small/medium T-cell LPD
• * Primary cutaneous acral CD8+ T-cell lymphoma
WHO 2016 update: recognition of indolent “Lymphoma/LPD“
*provisional entities
Indolent T/NK-cell proliferations
Early lymphoid lesions: conceptual, diagnostic and clinical challenges, Haematologica 2014;99(9)
• Interface between benign and malignant
• Include clonal proliferations, cells may carry molecular hallmarks of malignant counterpart
• No autonomous proliferation, limited potential for progression -> conservative treatment
Disease Genetic/molecular alteration
Frequency Effect
T-PLL TRA/D-TCL1 fusionTRA/D-MTCP1 fusion
JAK1/JAK3/STAT5Bmut.ATM deletion/mutation
75%1
75%70%
Aberrant TCL1 expression and activation of AKT pathwayAberrant MTCP1 expression and activation of AKT pathwayConstitutive activationImpaired DNA damage response
T-LGL STAT3 mutationsSTAT5B mutations
30-40%Rare
Constitutive activationConstitutive activation
CLPD-NK STAT3 mutations 25-30% Constitutive activation
ATLL JAK3mutationCCR4 mutation
10%25%
Constitutive activationPI3K/AKT activation
SS TCF3 deletionTP53 deletion
ARID1A mutations
70%75%40%
Enhanced cell-cycle progressionImpaired DNA damage responseChromatin remodeling
Recurrent genetic alterations in mature T/NK-cell leukemias
Gaulard&Levald, SeminHematol, 2014Bailey &Elenitoba-Johnson, Curr. Hematol. Malig. Rep 2015
T-PLL: T-cell prolymphocytic leukemia; T-LGL: T-cell large granular lymphocyte leukemia; CLPD-NK: chroniclymphoproliferative disorders of NK cells; ATLL: Adult T-cell lymphoma / leukemia; SS Sèzary Syndrome
slide by J. Almeida, Salamanca,Spain
Disease Genetic/molecular alteration
ALK+ALCL t(2;5)(p23;q35) (NPM-ALK)t(1;2) (TPM3-ALK)t (2;3) (TFG-ALK)Inv2 (ATIC-ALK)
t(2;22) (CTLC-ALK)
ALK-ALCL DUSP22-IRF4 locus on 6p25.3* (30%)P63 on 3q28* (8%)
AITL(and TFH-like PTCL-NOS)
RHOA mutationsTET2, IDH2 and DNMT3A mutations
PTCL-NOS “GATA3” (↑GATA3, CCR4, IL18RA, CXCR7 and IK)
“TBX21” (↑TBX21, EOMES, CXCR3, IL2RB, CCL3 and IFNg)
HTCL Isochromosome 7q (majority of cases)
* 5y-OS of 90% for DUSP22+ALK-ALCL vs 85% for ALK+ALCL (vs. 17% for P63+ cases)
Gaulard&Levald, SeminHematol, 2014Hapgood&Savage, Hematol. Oncol. 2015slide by J. Almeida, Salamanca,Spain
Recurrent genetic alterations in mature T/NK-cell leukemias
23/10/2017
2
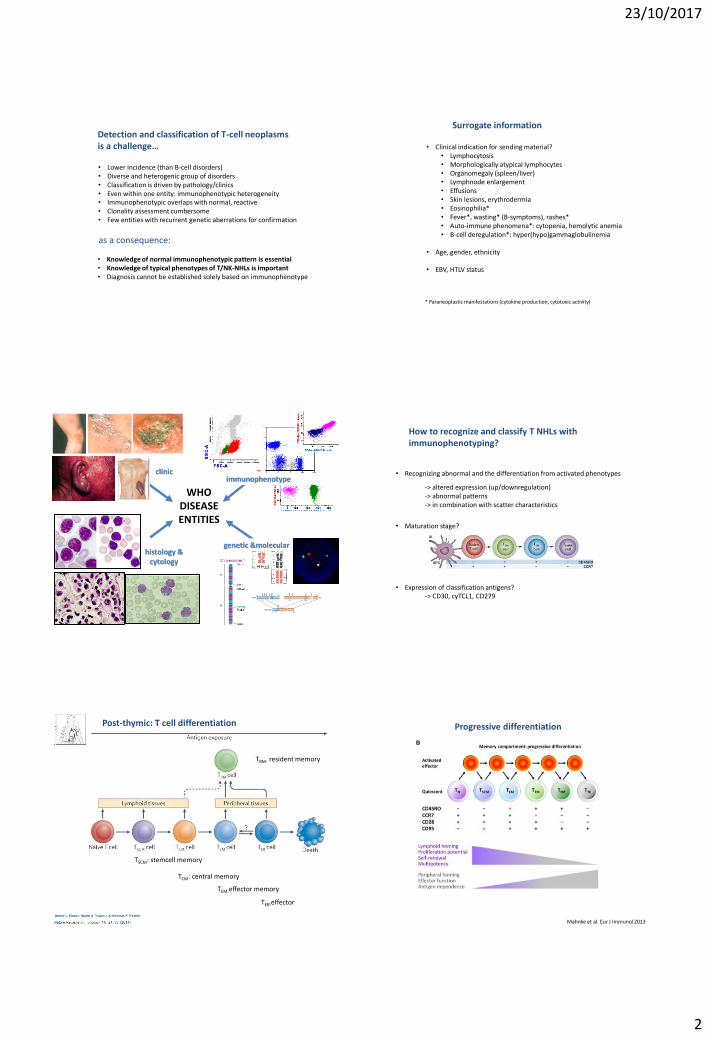
• Lower incidence (than B-cell disorders)• Diverse and heterogenic group of disorders• Classification is driven by pathology/clinics• Even within one entity: immunophenotypic heterogeneity• Immunophenotypic overlaps with normal, reactive• Clonality assessment cumbersome• Few entities with recurrent genetic aberrations for confirmation
Detection and classification of T-cell neoplasmsis a challenge…
as a consequence:
• Knowledge of normal immunophenotypic pattern is essential• Knowledge of typical phenotypes of T/NK-NHLs is important• Diagnosis cannot be established solely based on immunophenotype
Surrogate information
• Clinical indication for sending material?• Lymphocytosis• Morphologically atypical lymphocytes• Organomegaly (spleen/liver)• Lymphnode enlargement• Effusions• Skin lesions, erythrodermia• Eosinophilia*• Fever*, wasting* (B-symptoms), rashes*• Auto-immune phenomena*: cytopenia, hemolytic anemia• B-cell deregulation*: hyper(hypo)gammaglobulinemia
• Age, gender, ethnicity
• EBV, HTLV status
* Paraneoplastic manifestations (cytokine production, cytotoxic activity)
CD8 - FITC
CD
4 -
PEC
y5
WHO DISEASE ENTITIES
clinic
histology & cytology
genetic &molecular
immunophenotype
How to recognize and classify T NHLs with immunophenotyping?
• Recognizing abnormal and the differentiation from activated phenotypes
• Maturation stage?
• Expression of classification antigens? -> CD30, cyTCL1, CD279
-> altered expression (up/downregulation)-> abnormal patterns-> in combination with scatter characteristics
TSCM: stemcell memory
TCM: central memory
TEM:effector memory
TEff:effector
Post-thymic: T cell differentiation
TRM: resident memory
Progressive differentiation
Mahnke et al. Eur J Immunol 2013

23/10/2017
3
Cell Origin of T-cell Lymphoma
PLL
De Leval&Gaulard, ASH Educational Book, 2008
Antigens investigated in T-cell malignancies
• «pan T-cell»: CD3, CD4, CD8, CD7, CD2, CD5, TCRab, TCRgd and CD45
• co-stimulatory antigens: CD28, CD27, CD26
• maturation-related: CD45RA, CD45RO
• homing receptors: CCR7 (CD197)
• activation-related: CD38, HLA-DR, CD25, CD11b, CD11c
• NK-associated: CD16, CD94
• cytotoxicity-related: CD56, CD57, Granzyme, Perforin
• classification markers: CD30 (ALCL), CD10 (AITL), cyTCL1 (PLL), CD279/PD-1 (AITL)
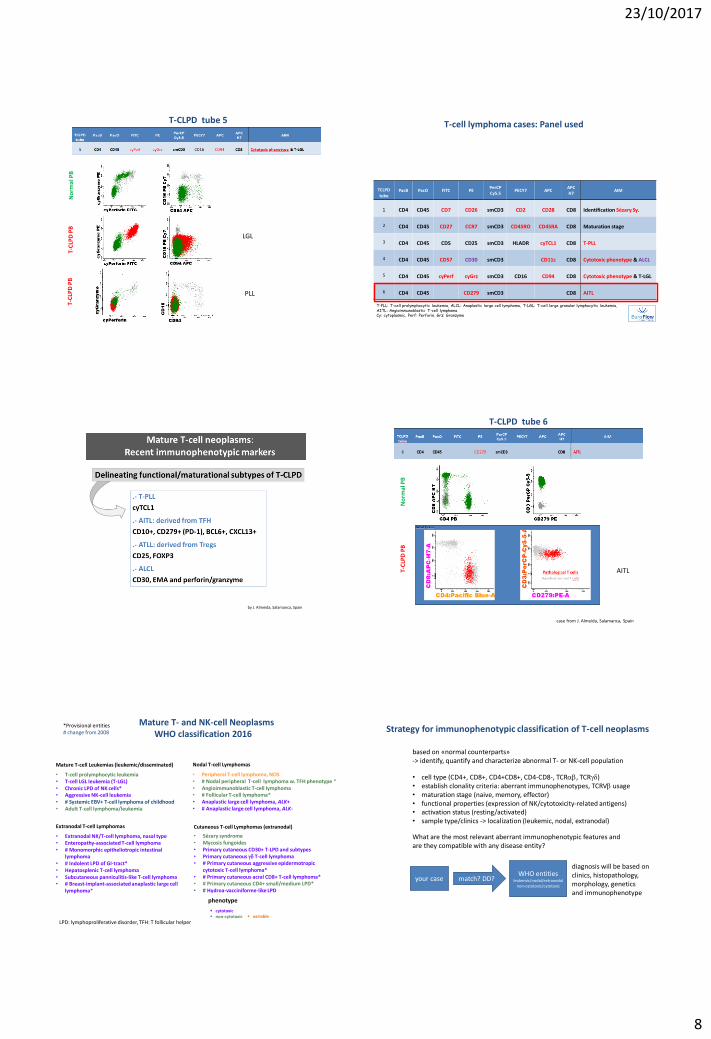
T-cell lymphoma cases: Panel used
Screening PacB PacO FITC PEPerCP-Cy5.5
PECY7 APC APCH7
LymphoidScreeningTube: LST
CD4CD20
CD45 CD8Anti-sIgl
CD56Anti-sIgk
CD5 Anti-TCRgd
CD19
smCD3 CD38
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Analysis and Gating (Software Infinicyt)
1) Exclusion of doublets and debris:
2) Select Lymphocytes:
-> double check in individual plots(e.g. SSC/CD3) that all events selected)
3) Lymphocytes: select B, T
B-cellsT-cells
NK-cells
Analysis and Gating (Software Infinicyt)
4) check B-cells
B-cells Plasma cells? B-progenitors?
Kappa/lambda should overlapp for CD19 and CD20
Analysis and Gating (Software Infinicyt)
5) check NK-cells
Include: CD56+CD8-/+NK-cells Include only CD4-
NK are CD3-CD5-CD38+

23/10/2017
4
Analysis and Gating (Software Infinicyt)
6) check T-cellsTCRg/d pos cells All other T-cells:
Normal T-cellsubpopulations: CD4+CD8+(dim)CD4+(dim)CD8+CD4-CD8-
Normal Patterns of activation: CD5 and CD38
naive recently activated late activated/ terminally differentiated
Reactive T cells in a 10y oldwith EBV infection
reactive
CD
3
CD5
normal
CD4/CD8 ratio 0.2 scatter CD38+
Pictograms from M. Lima, Porto, Portugal
Screening: what to look for
No
rmal
PB
T-C
LPD
PB
Ratio: 0.9
Ratio: 0.2
large granularlymphocyte leukemia(LGL)
Example:
Green: normal T-cellsGrey: B- and NK-cellRed: abnormal T-cells
Screening: what to look for
No
rmal
PB
Ratio: 0.9
T-C
LPD
PB
Ratio: 930
Prolymphocytic leukemia (PLL)Example:
Green: normal T-cellsGrey: B- and NK-cellRed: abnormal T-cells
T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Normal Patterns of activation
naive Recently activated Late activated/ Terminally differentiated
Romero P, J Immunol 2007; 178
CD4
CD8
Pictograms from M. Lima, Porto, Portugal

23/10/2017
5
T-CLPD tube 1
No
rmal
PB
T-C
LPD
PB
Example: Sézary Syndrome, pathognomonic: CD7-, CD26-
Green: normal T-cellsRed: abnormal T-cellsGrey: B- and NK-cell
T-CLPD tube 1
No
rmal
PB
T-C
LPD
PB
PLLExample:
Green: normal T-cellsRed: abnormal T-cellsGrey: B- and NK-cell
T-CLPD tube 1
No
rmal
PB
T-C
LPD
PB
LGLExample:
Green: normal T-cellsRed: abnormal T-cellsGrey: B- and NK-cell T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Maturation stages
by J. Almeida, Salamanca, Spain
Different possible combinations: shown CCR7/CD27/CD45RA/CD45RO
Normal Patterns of activation
naive recently activated late activated/ terminally differentiated
Pictograms from M. Lima, Porto, Portugal

23/10/2017
6
No
rmal
PB
T-C
LPD
PB
LGLExample:
T-CLPD tube 2Green: normal T-cellsRed: abnormal T-cellsGrey: B- and NK-cell
T-CLPD tube 2
No
rmal
PB
T-C
LPD
PB
PLLExample:
T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Normal Patterns of activation
naive recently activated late activated/ terminally differentiated
Pictograms from M. Lima, Porto, Portugal
www.control-T.de
TCL1: T-cell lymphoma breakpoint 1
Over-expression of this oncogene is due to translocation in proximityof TCR-regulatory elements-> classification marker for PLL
T-CLPD tube 3
No
rmal
PB
T-C
LPD
PB
T-C
LPD
PB
PLL with inv14q(q11;q32)TCL1
PLL with t(X;14)(q28;q11)MTCP1 (homologue of TCL1)
CD25
HLA
DR
ATLL

23/10/2017
7
T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Normal Patterns of activation
naive recently activated late activated/ terminally differentiated
CD30 expression in T-NHL
www.scienceofCD30.com
T-CLPD tube 4
No
rmal
PB
T-C
LPD
PB
T-C
LPD
PBAnaplastic
Large CellLymphoma(ALCL)
LGL
T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
Normal Patterns
late activated/ terminally differentiated
recently activatednaive
Romero P, J Immunol 2007; 178Pictograms by M. Lima, Porto, Portugal
23/10/2017
8
T-CLPD tube 5
No
rmal
PB
T-C
LPD
PB
T-C
LPD
PB
PLL
LGL
T-PLL: T-cell prolymphocytic leukemia, ALCL: Anaplastic large cell lymphoma, T-LGL: T-cell large granular lymphocytic leukemia, AITL: Angioimmunoblastic T-cell lymphomaCy: cytoplasmic, Perf: Perforin, Grz: Granzyme
T-cell lymphoma cases: Panel used
TCLPDtube
PacB PacO FITC PEPerCPCy5.5
PECY7 APCAPCH7
AIM
1 CD4 CD45 CD7 CD26 smCD3 CD2 CD28 CD8 Identification Sézary Sy.
2 CD4 CD45 CD27 CCR7 smCD3 CD45RO CD45RA CD8 Maturation stage
3 CD4 CD45 CD5 CD25 smCD3 HLADR cyTCL1 CD8 T-PLL
4 CD4 CD45 CD57 CD30 smCD3 CD11c CD8 Cytotoxic phenotype & ALCL
5 CD4 CD45 cyPerf cyGrz smCD3 CD16 CD94 CD8 Cytotoxic phenotype & T-LGL
6 CD4 CD45 CD279 smCD3 CD8 AITL
by J. Almeida, Salamanca, Spain
T-CLPD tube 6
No
rmal
PB
T-C
LPD
PB
AITL
case from J. Almeida, Salamanca, Spain
Mature T-cell Leukemias (leukemic/disseminated)
• T-cell prolymphocytic leukemia• T-cell LGL leukemia (T-LGL)• Chronic LPD of NK cells*• Aggressive NK-cell leukemia• # Systemic EBV+ T-cell lymphoma of childhood• Adult T-cell lymphoma/leukemia
• Peripheral T-cell lymphoma, NOS • # Nodal peripheral T-cell lymphoma w. TFH phenotype *• Angioimmunoblastic T-cell lymphoma• # Follicular T-cell lymphoma*• Anaplastic large cell lymphoma, ALK+ • # Anaplastic large cell lymphoma, ALK-
Nodal T-cell Lymphomas
*Provisional entities# change from 2008
• Sézary syndrome • Mycosis fungoides• Primary cutaneous CD30+ T-LPD and subtypes• Primary cutaneous gd T-cell lymphoma• # Primary cutaneous aggressive epidermotropic
cytotoxic T-cell lymphoma*• # Primary cutaneous acral CD8+ T-cell lymphoma*• # Primary cutaneous CD4+ small/medium LPD*• # Hydroa-vacciniforme-like LPD
Cutaneous T-cell Lymphomas (extranodal)
Mature T- and NK-cell NeoplasmsWHO classification 2016
LPD: lymphoproliferative disorder, TFH: T follicular helper
Extranodal T-cell Lymphomas
• Extranodal NK/T-cell lymphoma, nasal type• Enteropathy-associated T-cell lymphoma • # Monomorphic epitheliotropic intestinal
lymphoma• # Indolent LPD of GI-tract*• Hepatosplenic T-cell lymphoma• Subcutaneous panniculitis-like T-cell lymphoma• # Breast-implant-associated anaplastic large cell
lymphoma*
cytotoxic non-cytotoxic variable
phenotype
Strategy for immunophenotypic classification of T-cell neoplasms
based on «normal counterparts» -> identify, quantify and characterize abnormal T- or NK-cell population
• cell type (CD4+, CD8+, CD4+CD8+, CD4-CD8-, TCRab, TCRgd)• establish clonality criteria: aberrant immunophenotypes, TCRVb usage• maturation stage (naive, memory, effector)• functional properties (expression of NK/cytotoxicity-related antigens)• activation status (resting/activated)• sample type/clinics -> localization (leukemic, nodal, extranodal)
What are the most relevant aberrant immunophenotypic features andare they compatible with any disease entity?
your case match? DD?WHO entities
leukemic/nodal/extranodalnon-cytotoxic/cytotoxic
diagnosis will be based on clinics, histopathology,morphology, geneticsand immunophenotype

23/10/2017
9
Thank you foryour attention
thanks to:Margarida Lima, Porto, PortugalJulia Almeida, Salamanca, Spain