agenda part 1 chair: dr hilary byrne governing... · gwyneth wilson registered nurse governing body...
TRANSCRIPT

Meeting of NHS South Norfolk Clinical Commissioning Group Governing Body
13.30 – 15.30
Tuesday, 26th January 2016
Colin Chapman Room, Hethel Engineering Centre, Chapman Way, Hethel, Norwich, NR14 8FB
AGENDA
AGENDA – Part 1 Chair: Dr Hilary Byrne
ITEM TIME SUBJECT
1. 13.30 Chair’s opening comments and housekeeping notes
2. Apologies for Absence
3. Declarations of Interest
4. Minutes from Previous Meeting 24 November 2015 Part 1
5. Decision Log
6. 13.40 Decision
6.1 Finance & Performance Report David Gilburt Paper
6.2 QIPP 15/16 & 16/17 Margaret Blackett Paper
6.3 Audiology Eligibility Threshold Proposal Dr Dustyn Saint & Jocelyn Pike
Paper
7. 14.40 Discussion
7.1 Summary of Planning Guidance 16/17 Jocelyn Pike Paper
7.2 Commissioning and Contracting Update Jocelyn Pike Paper
7.3 Mazars Report & Recommendation – Independent review of deaths LD & MH Patients
Alison Leather Paper
7.4 Governing Body Assurance Framework Amanda Brown Paper
8. 15.15 Information
8.1 Communications and Engagement Report Oliver Cruickshank Paper
8.2 Transforming Care Alison Leather Paper
8.3 Audit Committee Report Anna Bennett Verbal
8.4 Corporate Affairs Report Amanda Brown Paper
9. 15.30 Any Other Business
Date and time of next meeting
The next meeting of NHS South Norfolk Clinical Commissioning Group Board will be held on Tuesday 22nd March 2016, Colin Chapman Room, Hethel Engineering Centre, Chapman Way, Hethel,
Norwich, NR14 8FB
In accordance with the Public Bodies (Admission to Meetings) Act 1960, the public and members of the Press
will be excluded from the remainder of the meeting where there is business of a confidential nature to be transacted, publicity concerning which could be prejudicial to the public interest

(A) CSU (Anglia) Commissioning Support Unit LAT Local Area Team (of the National Commissioning Board)
2ww Two Week Wait LMC Local Medical Committee
A&E Accident and Emergency LTC Long Term Conditions
AQP Any Qualified Provider MFE Medicine for the Elderly
ASCU NHS Anglia Commissioning Support Unit MIU Minor Injuries Unit
AT Area Team MONITOR NHS Foundation Trust Regulator
BDC Broadland District Council MRSA Methicillin Resistant Staphylococcus Aureus
BMA British Medical Association MSOA Middle Layer Super Output Area
BMI Body Mass Index N&W CSU Norfolk and Waveney Commissioning Support Unit
C2C Consultant to Consultant NCB National Commissioning Board (Now NHS England)
C&B Choose and Book NCC Norfolk County Council
CCG Clinical Commissioning Group NCHC Norfolk Community Health and Care services provider organisation
CFT Community Foundation Trust NHS National Health Service
CHC Continuing Healthcare NHS NCB NHS National Commissioning Board
CHD Coronary Heart Disease NHSM&E NHS Midlands and East
CIC Community Interest Company NICE National Institute for Health and Clinical Excellence
COF Commissioning Outcomes Framework NNUHFT Norfolk and Norwich University Hospitals Foundation Trust
COPD Chronic Obstructive Pulmonary Disease NQB NHS National Quality Board
CPA Care Programme Approach NSFT Norfolk and Suffolk NHS Foundation Trust
CQC Care Quality Commission OOH Out of Hours
CQRM Contractual Quality Review Meeting PALs Patient Advice and Liaison Service
CQUIN Contracting for Quality and Innovation PbR Payment by Results
DES Directly Enhanced Service PCT Primary Care Trust
DIST Dementia Intensive Support Team PMS Primary Medical Services
DoH Department of Health PPE Patient and Public Engagement
DSR Directly Standardised Rates PPG Patient Participation Group
ECG Electrocardiogram PPI Patient and Public Involvement
EEAST East Anglian Ambulance Services NHS Trust PROMS Patient Reported Outcome Measures
EIT Early Intervention teams QALY Quality Adjusted Life Year
EMIS Egton Medical Information Systems (GP Information System) QEHKLFT Queen Elizabeth Hospital Kings Lynn NHS Foundation Trust
EoE East of England QIPP Quality, Innovation, Productivity and Prevention
ERPHO East of England Public Health Observatory QIR Quality Issue Report
FOI Freedom of Information QOF Quality and Outcomes Framework
FRR Financial Risk Rating R&D Research & Development
FT Foundation Trust RCA Root Cause Analysis
GBAF Governing Body Assurance Framework RCGP Royal College of General Practitioners
GP General Practitioner RMC Referrals Management Centre
H&WB Health & Wellbeing Board RTT Referral to Treatment
HCAI Healthcare Acquired Infection SCN Strategic Clinical Network
HDU High Dependency Unit SI Serious Incidents
HES Hospital Episode Statistics SLA Service Level Agreement
HOSC Health Overview and Scrutiny SNCCG South Norfolk Clinical Commissioning Group
IAPT Improving Access to Psychological Therapies SNDC South Norfolk District Council
ICAS Independent Complaints Advocacy Service SPA Single Point of Access
ICO Integrated Care Organisation SPOT Spend and Outcome relative to other CCGs
IFR Individual Funding Request SUS Secondary Uses Service
IG Information Governance TAG Therapeutic Advisory Group
IM&T Information Management and Technology TIA Transient Ischaemic Attack
IMD Index of Multiple Deprivations TOP Termination of Pregnancy
JHWS Joint Health and Wellbeing Strategy VTE Venous thrombo-embolism
JPUHFT James Paget University Hospital Foundation Trust WSH West Suffolk Hospital
KPI Key Performance Indicator Y&HPHO Yorkshire & Humber Public Health Observatory
LA Local Authority
Card Key
Elected Governing Body Member LAY Governing Body Member
Officers of SNCCG on Governing Body Officer SNCCG, not Governing Body

NHS South Norfolk Clinical Commissioning Group
This Register of Interests (Register) includes all interests declared by governing body members and members of committees or sub-committees, (including committees and sub-committees of the governing body) of NHS South Norfolk Clinical Commissioning Group (the CCG).
In accordance with the CCG’s constitution and section 14O of The National Health Service Act 2006, the CCG’s accountable officer must be informed of any interest which may lead to a conflict with the interests of the CCG and the public for whom they commission servicesin relation to a decision to be made by the CCG, that needs to be included in the Register within 28 days of the individual becoming aware of the potential for a conflict. The Register will be updated regularly (at no more than 3-monthly intervals). Interests that must be declared (whether such interests are those of the individual themselves or of a family member, close friend or other acquaintance of the individual) include:
roles and responsibilities held within member practices;
directorships, including non-executive directorships, held in private companies or PLCs;
ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG;
shareholdings (more than 5%) of companies in the field of health and social care;
a position of authority in an organisation (e.g. charity or voluntary organisation) in the field of health and social care;
any connection with a voluntary or other organisation contracting for NHS services;
research funding/grants that may be received by the individual or any organisation in which they have an interest or role;
any other role or relationship which the public could perceive would impair or otherwise influence the individual’s judgement or actions in their role within the CCG.

NHS South Norfolk Clinical Commissioning Group
Register of Interests
Declared interests as at January 2016 of the Governing Body are in the table below.
Name Position Interest Declared
Dr Hilary Byrne Chair GP Partner at Attleborough Surgeries which is part of Iceni Healthcare Limited, Director of Tonian Ltd, spouse employee of Suffolk CCG – declared 21 April 2015
Margaret Blackett Interim Chief Officer Director of Blackett Sharp Ltd, Director of Britannia Sailing Ltd, Shareholder in Blackett Sharp Ltd – declared 19 January 2016
Alison Leather Director of Quality Assurance None – declared 30 December 2015
David Gilburt Interim Chief Finance Officer Director and part owner of a private company – Bonduca Solutions Limited, Associate Lay Member and Chair of the Audit Committee of West Cheshire CCG, Non-Executive Director of The Robert Jones and Agnes Hunt Orthopedic Hospital NHS Foundation Trust (RJAH), actively involved in activities which support the Neuromuscular Centre in Winsford, Cheshire which provides a range of services and specialist advice for people with muscular dystrophy, occasional paid ad-hoc specialist advice to the Gerson Lehrman Group which provides access to research for a wide range of financial and investments institutions and life sciences companies – declared 4 January 2016
Gwyneth Wilson Registered Nurse Governing Body Family members are employees of Queen Elizabeth Hospital, Kings Lynn and Cambridge & Peterborough NHS Foundation Trust – declared 10 February 2015
Kevan Baker Governing Body Member Practice Manager at Wymondham Medical Partnership, Postmill Close Wymondham which is a shareholder in South Norfolk Healthcare C.I.C and Iceni Healthcare Limited, Wymondham Medical Partnership has an RSI contract with the PCRN team – declared 10 April 2015
Cathal Daly Governing Body Member Employee of Elmham Surgery and work at Mattishall Surgery on a self-employed basis, both practices are part of Iceni Healthcare Limited.
In 2013/14 Paid to speak for Pfizer, Ferring, Abbott, Napp and Sanofi. Attended advisory boards for Pierre Fabre, Abbott, Dallas Ashbourne, Novartis, Eisai, Almirall, Nutricia, Astra Zeneca, MSD, Napp, Proteus, Novo Nordisk, Actavis, Lifescan. Paid for written work by Amgen.

In 2014/15 Attended a meeting sponsoured by Astra Zeneca. Paid to speak for Napp and Teva. Attended advisory boards for Warner Chilcott, Astellas, Leo, Nutricia, Sterling Anglian, MSD, Astra Zeneca, Biogen, Actavis and Boehringer Ingelheim. Paid to provide training by Astellas.
In 2015/16 Paid to speak for Napp and Teva. Attended advisory boards run for scope, Mead Johnson, Coloplast, Roche, Rosemont, Astra Zeneca, Nutricia, Bayer, Teva, HFA Healthcare, Shield Therapeutics and Philips. Paid for written work by Teva – declared 9 December 2015
Dr Keeva Rogers Governing Body Member GP Partner at Roundwell Medical Practice which is a part of Iceni Healthcare Limited, Class A shareholder in South Norfolk Healthcare C.I.C, Spouse employee Consultant of Norfolk and Norwich University Hospitals NHS Foundation Trust – declared 8 April 2015
Dr Graham Clark Governing Body Member GP Partner at Chet Valley Medical Practice, Loddon, which is part of Iceni Healthcare Limited, Class A shareholder in South Norfolk Healthcare Limited C.I.C, employed by Norfolk and Norwich University Hospitals NHS Foundation Trust as an Associate Specialist in the Accident and Emergency department, Partner works for Harleston Medical Practice – declared 25 April 2015
Dr Dustyn Saint Governing Body Member GP Partner at Long Stratton Medical Partnership which is part of Iceni Healthcare Limited, Director of Primary Care IT, Practice is part of South Norfolk Healthcare C.I.C, Partner of Clinical Opinions LLP; an organisation which provides the NHS, independent companies and overseas organisations with the opinions of experienced Clinicians working within the NHS – declared 19 January 2016
Dr Tony Palframan Governing Body Member GP Partner at Heathgate Medical Practice which is part of Iceni Healthcare Limited, Practice is part of South Norfolk Healthcare C.I.C, GP Tutor Health Education East of England, GP Education Lead East Anglia Faculty RCGP, Spouse is Brigade Manager, Norfolk Fire and Rescue. Registered patient of South Norfolk GP Practice – declared 28 July 2015
Susan Ringwood Lay Member, Patient & Public Involvement
Chief Executive of Age UK Norwich, Spouse is Manager of NCH&C charitable trust – declared 12 May 2015
Anna Bennett Lay Member, Governance Managing Director and Shareholder of AMB Business Management Ltd, Management Consultancy with NHS organisations (will not seek business with Norfolk NHS), Spouse is Director of AMB Business Management Ltd. Currently Interim Head of Contracting City and Hackney CCG (April 2014 to May 2015) – declared 9 September 2015
Dr Nicky Trepte Secondary Care Specialist Seckford Foundation Governor, Woodbridge Suffolk (Volunteer) and employee of Ipswich

Hospital NHS Trust – declared 21 April 2015

1
NHS South Norfolk Clinical Commissioning Group
DRAFT Minutes of NHS South Norfolk Clinical Commissioning Group Governing Body Part 1
1.30pm – 3.30pm Tuesday 24th November 2015
Colin Chapman Room, Hethel Engineering Centre, Chapman Way, Hethel, Norwich, Norfolk,
NR14 8FB _______________________________________________________________________________
Present: Dr Hilary Byrne (Chair) (HB) Governing Body Member Jim Hayburn (JH) Acting Chief Officer Anna Bennett (ABe) Lay Member (Audit and Governance) Cathal Daly (CD) Governing Body Member Kevan Baker (KB) Governing Body Member Dr Nicola Trepte (NT) Lay Member (Secondary Care Clinician) Dr Dustyn Saint (DS) Governing Body Member Susan Ringwood (SR) Lay Member (Patient and Public Engagement) Gwyneth Wilson (GW) Lay Member (Registered Nurse) David Gilburt (DG) Interim Chief Finance Officer Andrew Spring (AS) Interim Chief Finance Officer In attendance: Alan Kent (AK) Chair, Finance and Performance Committee Jocelyn Pike (JP) Chief Operating Officer Margaret Blackett (MB) Programme Director Amanda Brown (ABr) Acting Head of Corporate Affairs Samantha Cox (SC) Business Support (Minutes) Tim Curtis (TC) Communications Manager Alison Leather (AL) Director of Quality Assurance
1. Chair’s Opening Comments and Housekeeping Notes Action
HB welcomed all attendees to part 1 of the Governing Body meeting of NHS South Norfolk Clinical Commissioning Group (SNCCG). Introductions were made. HB requested questions from the members of the public be made at the end of the meeting and are directed to Heidi Davey. HB introduced DG, SNCCG’s new Interim Chief Finance Officer as Andrew Spring’s replacement. HB thanked AS for his work. HB also introduced Alison Leather as the new Director of Quality Assurance.
2. Apologies for Absence
Apologies were received from Dr Keeva Rogers (KR) Governing Body Member Dr Graham Clark (GC) Governing Body Member Dr Tony Palframan (TP) Governing Body Member
Agenda Item 4

2
NHS South Norfolk Clinical Commissioning Group
3. Declarations of Interest
No new Declarations of Interest were identified at this time. HB reminded all to ensure their Declarations of Interest are up to date. HB reminded members to update their conflicts of interest in line with national guidelines.
4. Minutes from Previous Meeting & Actions Arising
Following amendments to be made to the minutes from 8th September 2015: Venue to be updated to Keystone Innovation Centre Andrew Spring to be added onto the attendee list Agenda Item 7.5, Page 5 - £400k goes towards a risk share on out of trust placements (Not OTP) JP to supply wording. Page 3, agenda item 6 to read £3.356k. Actions Arising Regular monthly messages in OC update. Once the above amendments have been made the minutes from the NHS South Norfolk Clinical Commissioning Governing Body meeting held on 8th September 2015 were approved as a true and accurate record of the meeting.
SC
JP
JH
5. Decision
5.1 Finance Report
AS presented the paper taking it as read highlighting that SNCCG are still forecasting to meet the financial plan However month 7 is showing a £4.93 million deficit and are therefore £1.3 million off plan. AS advised that SNCCG are borrowing money from the future which will need to be paid back in due course. NHS England have been pleased with the progress that the CCG has made over the past few months, particularly in Continuing Health Care (CHC) and Prescribing QIPP. AS advised that there are 2 long stay patients at West Suffolk Hospital Trust which have a substantial cost increase of £170k in month from a £12k average. NNUHFT moved back to plan where SNCCG was reporting as being underspent, the CCG are looking to review patients in terms of costs and charges. The Finance & Performance committee have been through the following reports in detail:
YTD position
FOT position
Underlying position
Finance report
Performance report
Non ISFE report AK advised that they have highlighted the issues and are assured actions are being taken. AB queried the reserves item in the Finance Report, AB stressed the 2 uncommitted commissioning reserves as there is a considerable amount of back ended financials and advised 2 risks; activity increase of which assumptions have been made and delivery of the QIPP programme. The risk is not just reputational as it also affects next year’s plan. JH supported AB’s concerns. AS advised regarding the potential risks in terms of delivering, the only risk which could have some effect is that activity has increased over the past few months. AS advised that challenges are occurring on a routine monthly basis. Practice code making progress and performance is improving. After discussion member of NHS South Norfolk Clinical Commissioning Group Governing Body noted the month seven reported year-to-date position and forecast year end position, along with the risks to delivery of the CCG’s 2015/16 financial plan.

3
NHS South Norfolk Clinical Commissioning Group
5.2 15/16 QIPP Report
AS presented the paper taking it as read advising that NHS SNCCG are reporting a delivery of £2,317k to the end of month 7 (October) against a budgeted plan of £2,846k, which is £529k behind plan. AS advised that the CCG is reporting that they will not deliver against the full value of the original plan, however they are committed to finding other mitigations and schemes in year. CHC AS advised that CHC has had a good month of QIPP delivery, they are making sure assessments are done correctly and work is ongoing. They are looking at 300 individual cases which could amount to a substantial sum per person. Prescribing AS advised that Prescribing progress is being made. £403k with £198 in month from M5. This is not in line with the original plan as work did not commence until 01/04/2015. Counting & Coding AS advised re Coding and Counting. Neil Wilson Associates work has come to a conclusion in terms of PBR elements, AS is waiting on the local price part. This hasn’t delivered at the level originally anticipated and the outcome was less than we predicted it would be. Neil Wilson Associates attended the Finance & Performance Committee. AK advised that there was no quantification of work at that point, however he did express disappointment and concern that they still hadn’t had any hard figures. AS gave an update on 3 challenge areas; paediatric short stay, day cases no procedure and ophthalmology procedures. AS had a list of 17 in total which turned out to be low value. HB asked that a ‘Dashboard’ is to be bought to the next Governing Body as per agreed in previous minutes, MB to action. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the contents of the 15/16 QIPP Report, the progress to month 7 (October) with delivering SNCCGs challenging programme of savings, and the risks associated with the significant increase in required monthly savings to the end of the year to achieve the planned financial position.
MB
5.3 16/17 QIPP Plan
AS presented the paper advising that progress to date is as follows:
£15,710k total value of opportunity
42 projects in the ‘Gateway Process’
12 (29%) already achieved ‘approval to implement’, valued at £5,826k
13 (31%) at Project Initiation Document stage, valued at £7,255k AS advised that last month 6 schemes were in gateway 0, 5 of these are now on plan. AS advised that the proposals as part of the QIPP programme for 16/17 are £13 million, this is 2.5 times bigger than this year’s QIPP programme. However the CCG are ahead of planning with draft programmes. SR thanked AS and colleagues for the commendable work they have done on this. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the progress with developing the plan at this stage and supports the delivery of the process outlined in the paper.

4
NHS South Norfolk Clinical Commissioning Group
5.4 Specialist Fertility Services – IVF
DS presented the paper advising that he sympathises that these decisions are difficult but financial situations have caused this to be the case. DS advised that the CCG Governing Body agreed that a period of online engagement would be held in order to understand the spectrum of opinions before making a decision to restrict the Specialist Fertility Services policy from 1st January 2016. This paper outlines the engagement activity that took place, and provides key themes from the 57 written responses received. These include:
Feedback on the proposed criteria
Impact on the wider economy
NICE Guidance
Affordability
Alternatives to the restriction Details of which are on the CCG website. DS advised that the CCG has to be aware that this could potentially have a knock on effect to Mental Health Services and a general impact on the wider economy. GW queried what the NICE guidelines advised. ABe confirmed that this was 3 cycles under the age of 40 or 2 cycles under the age of 42. HB’s understanding is that other CCG’s are looking to follow suit with Specialist Fertility Services. AB raised concerns that this feels like a small sum to be taking out, which could potentially have such a large backlash. JP advised ABe that unfortunately the CCG has to look at all options. JH agrees with JP need to review this going forward as well due to the size of financial challenges. After further discussions all were in agreement that the CCG should go ahead with the proposal, apart from AB who was in disagreement. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body supported the Specialist Fertility Services, with a 6 monthly review on a periodic basis.
5.5 Adult Safeguarding Policy
GW presented the paper and advised that all CCG’s have been asked to accept, the paper has also been to the Quality Committee who have agreed. GW also advised that this policy applies to all CCG Staff. GW to insert a link into the policy re whistleblowing. After further discussions, the board was in agreement to accept the paper once amendments have been made. After discussion member of NHS South Norfolk Clinical Commissioning Group Governing Body formally approved the Adult Safeguarding Policy.
GW
6. Discussion
6.1 Governing Body Assurance Framework
AB presented the paper and advised that no changes had been made to the GBAF since the last Governing Body meeting in September. AB advised that finance risk 1, delivery and achieving a balance position had previously been rated as a risk this has now been reduced to 15. AB also advised that commissioning risk 26 has come off because the NSFT contract has now been signed.

5
NHS South Norfolk Clinical Commissioning Group
AB explained that the GBAF and Risk Register are reviewed at each Audit Committee meeting, together with a team risk register which are reviewed on a rotational basis. JH explained the review process and figures to the room. AS needs to be kept on constant review. JH believes this should be reviewed each month at the Finance and Performance committee so that they can make a decision around the finance rating to give assurance to the Governing Body. JP advised that the CCG has concerns of IC24’s delivery of OOH111 in terms of delivering. This is currently being captured on the Commissioning team risk register. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted Governing Body Assurance Framework.
6.2 Commissioning and Contracting Update
JP presented the paper advising the below: The CCG are looking to hold the action plan for A&E and have applied sanctions till month 6 regarding the ambulance handover. An audit has taken place, SNCCG are waiting on the outcome. JP advised that SNCCG didn’t feel that the latest draft action plan was acceptable. The NNUHFT plans to complete pathways have been rejected by SNCCG. Still unassured on cancer and diagnostics. JP advised that mental health is a big issue as we believe that the figures aren’t correct. NSFT have a new reporting system called Lorenzo which has had some problems, they are having to manually report on all targets, however they are suggesting that they will produce clean data for month 7. Performance and Information subgroup is querying an activity contract query notice. Regarding AAT SNCCG have issued a CQN and are withholding 1% per month from October per month. As of 19th November the trust had still not responded, SNCCG are looking to retain funds. JP advised that they are assured regarding Community, Q2 will be on track. 1 service breaching, out to procurement. OOH/111 are being monitored weekly. CCG’s collectively felt it was too early to issue a CQN. They have and our providing us with an improvement plan. JP would suggest if we do not see an improvement within the next month, then to push for an improvement plan. JP to bring figures re staff next month. HB advised that there is an agenda item at the Contract and Performance Meeting to discuss clinical agency staff this week. HB advised CD that tendering has its place however careful consideration must happen and SNCCG should ensure it tenders appropriately. JP acknowledged this. KB advised that a rep from IC24 are attending the practice managers meeting tomorrow. JP advised that OOH111 are aware they have issues and acknowledge that they have a long way to go, they now attend the System Resilience Group and the Capacity Planning meetings. JP advised that Commissioning intentions have commenced and. A joint plan was agreed at the Joint Commissioning Executive, which have been submitted to NHS England which includes 27 separate work streams. ALL Senior Officers have to complete and take back to the Joint Commissioning Committee. These will then go back of NHS England and the Joint Commissioning Committee for sign off, JP to bring to December’s Governing Body.

6
NHS South Norfolk Clinical Commissioning Group
JP advised that SNCCG has launched a consultation to restrict hearing aids for which and event for stakeholders and the public will be held at Bawburgh, details are on SNCCG’s website. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the contents of the report and agreed that the procurement commences in November.
6.3 Quality & Safety Update
GW gave a verbal update advising that NSFT have a planned visit in June which is supported by NELCSU. The NNUH had a visit on the 19th November, GW is waiting on the report on this visit. No new infections with patients reported, no noro virus within the local area. 10 Serious Incidents (SI’s) have been reported, all Pressure Ulcers (PU’s) No SI’s have been reported at NSFT. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the update.
7. Information
7.1 Communications and Engagement Report
OC presented the paper advising that SNCCG have been working with NHS North Norfolk CCG and NHS Norwich CCG in the run up to winter, leading into national messaging to stay well this winter. SR thanked OC for his work on sensitive topics. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the contents of the report.
7.2 Audit Committee Report
ABe presented the paper advising that internal audit had taken place which reviewed progress on the 15/16 plan. The final report will need to be taken to a Conflicts of Interest Committee. Financial control return to NHSE needs to be signed off. Next meeting is on the 11th December to which they will report back to the Governing Body on the 22nd December. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the contents of the report.
7.3 Corporate Affairs Report
ABr presented the paper advising that South Norfolk CCG’s public Governing Body meetings for next year have been aligned with North Norfolk CCG and Norwich CCG, to assist in decision making around Joint Commissioning Committee and Joint Contracting Executives to ensure decisions are made together. After discussion members of NHS South Norfolk Clinical Commissioning Group Governing Body formally noted the contents of the report.
8. Any Other Business
None.

7
NHS South Norfolk Clinical Commissioning Group
Name Signature Date Signed on behalf of NHS South Norfolk Clinical Commissioning Group
Subject:
Finance Report at end of December 2015 (Month 9)
Presented by:
David Gilburt, Interim Chief Finance Officer
Submitted to:
SNCCG Governing Body
Date: 26th January 2016
Purpose of paper:
For information and discussion
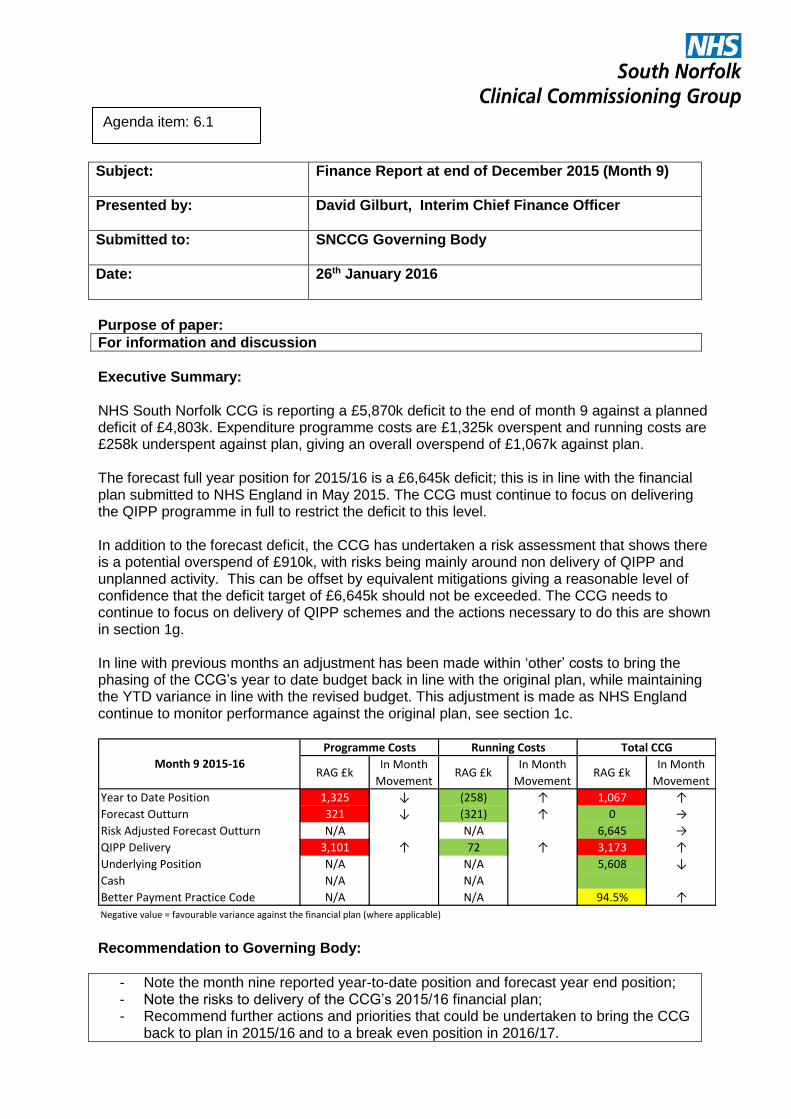
Executive Summary: NHS South Norfolk CCG is reporting a £5,870k deficit to the end of month 9 against a planned deficit of £4,803k. Expenditure programme costs are £1,325k overspent and running costs are £258k underspent against plan, giving an overall overspend of £1,067k against plan. The forecast full year position for 2015/16 is a £6,645k deficit; this is in line with the financial plan submitted to NHS England in May 2015. The CCG must continue to focus on delivering the QIPP programme in full to restrict the deficit to this level. In addition to the forecast deficit, the CCG has undertaken a risk assessment that shows there is a potential overspend of £910k, with risks being mainly around non delivery of QIPP and unplanned activity. This can be offset by equivalent mitigations giving a reasonable level of confidence that the deficit target of £6,645k should not be exceeded. The CCG needs to continue to focus on delivery of QIPP schemes and the actions necessary to do this are shown in section 1g. In line with previous months an adjustment has been made within ‘other’ costs to bring the phasing of the CCG’s year to date budget back in line with the original plan, while maintaining the YTD variance in line with the revised budget. This adjustment is made as NHS England continue to monitor performance against the original plan, see section 1c.
RAG £kIn Month
MovementRAG £k
In Month
MovementRAG £k
In Month
Movement
Year to Date Position 1,325 ↓ (258) ↑ 1,067 ↑
Forecast Outturn 321 ↓ (321) ↑ 0 →
Risk Adjusted Forecast Outturn N/A N/A 6,645 →
QIPP Delivery 3,101 ↑ 72 ↑ 3,173 ↑
Underlying Position N/A N/A 5,608 ↓
Cash N/A N/A
Better Payment Practice Code N/A N/A 94.5% ↑
Negative value = favourable variance against the financial plan (where applicable)
Programme Costs Running Costs Total CCG
Month 9 2015-16
Recommendation to Governing Body:
- Note the month nine reported year-to-date position and forecast year end position; - Note the risks to delivery of the CCG’s 2015/16 financial plan; - Recommend further actions and priorities that could be undertaken to bring the CCG
back to plan in 2015/16 and to a break even position in 2016/17.
Agenda item: 6.1

Key Risks
Clinical:
Programme budgets may need to be revised if funds are unavailable.
Finance and Performance:
Not achieving the planned deficit will increase the 2016/17 QIPP requirement.
Impact Assessment (environmental and equalities):
N/A
Reputation: Reputational risk if the CCG fails to meet its 2015/16 financial targets.
Legal: N/A
Resource Required:
N/A
Reference document(s):
Documents referred to in report.
NHS Constitution:
N/A
Conflicts of Interest:
N/A
GOVERNANCE
Note Activity information is available up to the 30 November and unless otherwise stated all activity and performance measures are reported for the eight months ending November 2015. These activity numbers are used to forecast expenditure to the end of December in this month 9 finance report.
Process/Committee approval with date(s) (as appropriate)
Performance for month 9 was reviewed and discussed at the Finance and Performance Committee on 19th January 2016.

1. Summary of Financial Position 1a. Financial Position The table below summaries NHS South Norfolk CCG’s (SNCCG) year to date financial position at the end of month 9 and our full year forecast outturn by programme cost area. More detail is found in appendix 1.
SNCCG Financial Position at M9M9
budgetM9 actual
M9
variance
M9 YTD
budget
M9 YTD
actual
M9 YTD
variance
Full Year
budget
Full Year
forecast
Full Year
variance
INCOME -22,173 -22,173 0 -197,951 -197,951 0 -263,691 -263,691 0
ACUTE Total 11,335 11,529 194 102,814 104,109 1,294 137,724 138,306 582
COMMUNITY HEALTH SERVICES Total 2,389 2,310 -79 21,469 21,132 -338 28,512 27,875 -637
CONTINUING CARE Total 1,657 1,804 147 15,573 16,325 752 20,437 21,398 961
MENTAL HEALTH Total 1,879 1,837 -43 16,621 16,208 -413 22,161 21,517 -644
PRIMARY CARE Total 3,600 3,601 1 32,008 32,612 603 42,456 43,248 791
OTHER Total 2,003 1,869 -134 10,222 9,648 -574 13,651 12,917 -733
CORPORATE Total 676 415 -261 4,046 3,788 -258 5,395 5,074 -321
(SURPLUS)/DEFICIT 1,367 1,192 -175 4,803 5,870 1,067 6,645 6,645 0
Note - negative variance = underspend and positive variance = overspend
YTD Position £'000s Full Year Position £'000sIn Month Position £'000s
1b. Year to Date SNCCG is reporting a £5,870k deficit to the end of month 9 against a planned deficit of £4,803k. There are some significant year to date variances against the budget, the key ones are described below. The £1,067k year to date (YTD) deficit means that the CCG has exceeded the planned deficit for this stage of the financial year and needs to spend £1,067k less than it planned to do in the final three months of 2015/16. This represents 1.6% reduction in planned expenditure over the final three months of the year. Acute – overspend £1,294k Acute services are overspent by £1,294k (1.2%) YTD to December which represents an adverse movement of £194k in month. Norfolk and Norwich University Hospital Foundation Trust (NNUH) The table below presents the contract monitoring summary position for activity and finance at November (month 8) which shows over performance of £353k.

SNCCG NNUH Finance Report to M08
Row LabelsActivity Plan Activity
Activity
Variance
Activity %
VarianceTariff Plan Tariff
Tariff
Variance
Tariff %
Variance
Elective 19,903 16,006 -3,897 -19.6% 15,022,731 14,524,309 -498,422 -3.3%
Daycase 17,175 13,493 -3,682 -21.4% 8,464,088 8,114,361 -349,727 -4.1%
Elective Ordinary 2,728 2,513 -215 -7.9% 6,558,643 6,409,948 -148,695 -2.3%
Non-Elective 12,711 12,957 246 1.9% 21,673,453 22,356,679 683,225 3.2%
Emergency 10,980 11,240 260 2.4% 20,482,629 21,130,919 648,290 3.2%
Other Non Elective 1,732 1,717 -15 -0.9% 3,063,023 3,041,028 -21,995 -0.7%
Credits & Readmissions 0 0 0 #VALUE! -1,872,199 -1,815,268 56,930 -3.0%
Outpatient 120,681 120,474 -207 -0.2% 12,889,596 13,074,503 184,907 1.4%
Attendances 96,110 95,530 -580 -0.6% 9,741,992 9,763,748 21,756 0.2%
Procedures 18,705 20,466 1,761 9.4% 3,010,668 3,206,194 195,526 6.5%
Telephone 5,866 4,478 -1,388 -23.7% 136,936 104,561 -32,375 -23.6%
Cost & Volume 47,347 43,152 -4,195 -8.9% 6,979,673 6,919,737 -59,937 -0.9%
Critical Care 1,121 911 -210 -18.8% 1,160,299 947,215 -213,084 -18.4%
Maternity Pathway 2,680 2,687 7 0.3% 2,222,998 2,265,008 42,010 1.9%
Direct Access Radiology 21,539 19,893 -1,646 -7.6% 1,072,936 934,337 -138,599 -12.9%
Outpatient Radiology 12,256 12,539 283 2.3% 1,173,370 1,264,340 90,970 7.8%
Other 9,751 7,122 -2,629 -27.0% 1,350,070 1,508,837 158,767 11.8%
Block #VALUE! 3,940,843 3,940,843 0 0.0%
Other #VALUE! 936,078 971,083 35,005 3.7%
CQUIN #VALUE! 1,536,059 1,544,679 8,619 0.6%
Grand Total 200,643 192,589 -8,054 -4.0% 62,978,434 63,331,832 353,398 0.6% The following two tables set out the top three over and under spent specialties at month 8 within Elective, Non Elective and Outpatient PODs. SNCCG NNUH Top Over Spent Areas
Row Labels Activity Plan ActivityActivity
Variance
Activity %
VarianceTariff Plan Tariff
Tariff
Variance
Tariff %
Variance
Elective 19,903 16,006 -3,897 -19.6% 15,022,731 14,523,648 -499,083 -3.3%
Trauma & Orthopaedics 909 889 -20 -2.2% 2,711,917 2,835,455 123,538 4.6%
Dermatology 683 826 143 20.9% 465,970 566,344 100,374 21.5%
Gastroenterology 3,458 3,696 238 6.9% 1,551,607 1,631,983 80,376 5.2%
Non-Elective 12,711 12,957 246 1.9% 23,209,028 23,750,660 541,632 2.3%
Paediatrics 1,022 1,329 307 30.0% 756,594 987,798 231,204 30.6%
Respiratory Medicine 500 565 65 13.0% 1,181,737 1,411,769 230,032 19.5%
Gastroenterology 439 512 73 16.5% 1,078,609 1,277,310 198,701 18.4%
Outpatient 120,681 120,474 -207 -0.2% 12,681,219 12,866,536 185,317 1.5%
Dermatology 7,482 8,714 1,232 16.5% 689,750 787,080 97,330 14.1%
Clinical Haematology 4,723 4,643 -80 -1.7% 543,339 609,734 66,395 12.2%
Gynaecology 5,115 5,331 216 4.2% 652,083 716,262 64,179 9.8%
SNCCG NNUH Top Under Spent Areas
Row LabelsActivity Plan Activity
Activity
Variance
Activity %
VarianceTariff Plan Tariff
Tariff
Variance
Tariff %
Variance
Elective 19,903 16,006 -3,897 -19.6% 15,022,731 14,523,648 -499,083 -3.3%
General Surgery 1,176 945 -231 -19.6% 2,243,908 1,831,923 -411,985 -18.4%
Ophthalmology 3,176 2,585 -591 -18.6% 1,752,093 1,434,035 -318,058 -18.2%
Gynaecology 546 483 -63 -11.5% 874,260 755,240 -119,020 -13.6%
Non-Elective 12,711 12,957 246 1.9% 23,209,028 23,750,660 541,632 2.3%
Trauma & Orthopaedics 721 640 -81 -11.3% 2,259,571 2,046,520 -213,051 -9.4%
Endocrinology 338 299 -39 -11.5% 795,161 673,963 -121,198 -15.2%
General Medicine 1,308 1,154 -154 -11.8% 876,449 789,991 -86,458 -9.9%
Outpatient 120,681 120,474 -207 -0.2% 12,681,219 12,866,536 185,317 1.5%
Respiratory Medicine 4,040 3,443 -597 -14.8% 418,361 355,325 -63,036 -15.1%
Urology 6,796 6,301 -495 -7.3% 1,048,239 995,951 -52,288 -5.0%
Hepatology 1,388 1,139 -249 -17.9% 175,793 142,317 -33,476 -19.0% Detailed activity is received one month in arrears therefore the month 9 financial position includes a cost estimate for December activity. Furthermore the financial variance includes an adjustment for contractual fines and penalties for failure to deliver the constitutional standards set out in the NHS contract. Fines are calculated using actual performance to month 7 and estimates for months 8 & 9. A total £716k of fines have been reinvested in improving services at NNUH with the balance of £749k being used towards funding additional elective activity with independent providers.

West Suffolk NHS Foundation Trust (WSH) The table below summarises the activity and finance position at month 8. As noted with NNUH above contract monitoring is received one month in arrears therefore the month 9 finance position includes an estimate for December activity.
Full Yr
Plan
Plan to
Date
Actual to
Date
Variance
to Date
Var to Date
%
Full Yr
Plan
Plan to
Date
Actual to
Date
Variance
to Date
Var to Date
%
2,465 1,639 1,587 (52) -3.1% 2,898 1,926 1,865 (61) -3.2%
3,778 2,496 2,549 53 2.1% 4,942 3,265 3,271 6 0.2%
24,584 16,437 16,299 (138) -0.8% 2,793 1,868 1,912 44 2.4%
6,427 4,315 4,425 110 2.5% 741 498 504 6 1.3%
37,254 24,887 24,860 (27) -0.1% 11,375 7,557 7,552 (5) -0.1%
21,187 14,209 12,708 (1,501) -10.6% 1,227 823 837 14 1.8%
274 183 183 - 0.0%
322 214 214 0 0.2%
555 372 309 (63) -16.9%
0 0 9 9 0 0 4 4
58,442 39,096 37,577 (1,519) -3.9% 13,753 9,149 9,100 (49) -0.5%
CQUIN
Excluded Drugs
Totals
Outpatients
A&E
PbR sub-total
Cost & Volume
Block
Other Adjustments
Non-Elective Admissions
West Suffolk Hospital to M8
Activity Finance (£'000s)
Elective Admissions / Daycases
Other Acute Acute QIPP slipped further in month and is £802k behind the year to date plan however achievement remains in line with the revised delivery trajectory. From month 8 all counting and coding QIPP is reported against the respective provider. This was a change in presentation from previous months and is intended to enable a more accurate assessment of the QIPP impact on individual contracts. The revised delivery plan rises steeply during quarter 4 with further detail provided in the month 9 QIPP Report. Independent Providers continue to present a significant cost pressure. In month the position worsened by £80k increasing the year to date over spend up to £615k. The most notable over performance is elective activity with Spire (orthopaedics), Global Diagnostics (radiology) and Norfolk Surgical & Diagnostic Centres. This over performance is due largely to capacity issues within Acute providers. The EEAST contract continues to over perform against the A&E contract activity schedule (4.04%) which, together with divert costs, totals an overspend of £228k. The CCG also has in year pressures due to unplanned costs arising from the critical care risk share agreement (£123k) and Military & Justice charges (£176k). Community Health Services – underspend £338k The main variance within Community Health Services is a favourable £229k variance on the Integrated Community Equipment Store (ICES). Savings are expected to continue at this rate for the remainder of the year. At month 9 there is an adverse variance of £161k on NCH&C cost and volume activity which has largely resulted from the drive to reduce the backlog within the Orthopaedic Clinical Assessment and Treatment service. The backlog is now clear and providing referrals can be managed back to indicative activity levels by Primary Care, activity should return to budgeted levels for the remainder of the year. Less intensive packages have been agreed for four patients and this is largely responsible for the £165k favourable variance on Long Term Conditions. Neuro-rehabilitation packages within

this area are subject to a risk share agreement therefore the full year underspend will be adjusted dependent on activity of other CCG’s. Continuing Healthcare - overspend £752k Continuing Healthcare (CHC) is £752k overspent in total, with the largest area of overspend being £855k on Adult CHC, which includes QIPP over delivery of £94k. This overspend is due to higher than planned levels of growth in patient numbers which have now reached 8.3% for the year, compared to planned growth of 5%. Historic information suggests high growth in this service during the summer followed by a reduction in patient numbers through the winter. Month 9 saw a decrease in patient numbers for the first time this financial year, however these are still far in excess of those predicted. At month 9 Adult CHC includes £542k of QIPP delivery to date; which has helped to offset the higher than expected growth. In month 9, £126k of QIPP savings were achieved, bringing the year to date total to £582k. This is now ahead of plan and is expected to deliver a favourable variance for the whole year. The other overspend in this area is for £83k on the CHC Risk Pool in respect of retrospective claims before the CCG came into being. Month 9 contains the full year cost, which is higher than the plan value originally advised by NHS England. At month 9 Funded Nursing Care is £107k underspent due to a reduction in patient numbers compared to 2014/15. Despite positive QIPP delivery, CHC remains a major cost pressure in an area that is experiencing significant unplanned growth, this is being closely monitored and managed to reduce costs further wherever possible. Mental Health - underspend £413k Mental Health as a whole is £413k underspent, largely due to underspends of £157k on Learning Difficulties (LD) and £171k on Child & Adolescent Mental Health. These underspends are calculated using up to date package and provider information. Both are due to reduced patient numbers since 2014/15, offset in part by increased average cost per case. There is also an underspend of £85k on Other Mental Health, due largely to retrospective LD patients. Primary Care – overspend £603k The £603k overspend on Primary Care is largely due to under-delivery of prescribing QIPP. Work to reduce prescribing spend continues and is gathering pace; SNCCG is planning to achieve £795k of Prescribing QIPP in 2015/16 to help bring the CCG back in line with the budget. Local Enhanced Service costs are £283k overspent, largely due to £209k of Choose and Book costs which were not budgeted for while the Over 75s project is £307k underspent as some planned investments have not been made. Other – underspend £574k Within Other Costs there is a £574k underspend on contingency, see section 1e, and also a £60k underspend on Patient Transport and £158k overspend on CSU costs.

Finally there is a £16k adjustment to both budget and actuals with a nil variance, see section 1c. Running Costs (Corporate) – underspend £258k The running cost position is £258k underspent at M9 and are currently forecast to be £321k underspent at the year end. However of the £321k forecast underspend £340k is due to receipt of 2014/15 Quality premium income meaning we are currently forecasting a £19k overspend against the original running cost allocation of £5,055k. The budgets are under review to see what measures can be introduced to bring spending below the budget by the year end. 1c. Balancing Budget to Plan There is a £16k adjustment to both budget and actuals with a nil variance. NHS England have requested this adjustment because SNCCG have re-phased our budgets since our original plan was submitted, meaning our budget YTD deficit is different to our original planned YTD deficit. This adjustment re-phases our YTD budget to the original YTD plan while maintaining the variance of actual expenditure against our revised budget. The table below shows that if this adjustment was not made the YTD variance against our revised budget would remain at £1,067k but our reported variance against the year to date original plan phasing would be £1,083k.
M9 YTD
budget
M9 YTD
actual
M9 YTD
variance
Reported YTD deficit 4,803 5,870 1,067
Remove balancing of budget to plan 16 16 0
YTD deficit against budget 4,819 5,886 1,067
Remove re-phasing of budget -16
YTD deficit against original plan 4,803 5,886 1,083 Months 10 and 11 will also require re-phasing adjustments to match the YTD budget variance to the original plan variance, with the two variances becoming equal at £6,645k in M12. 1d. Forecast Outturn The forecast full year position for 2015/16 is a £6,645k deficit, which is in line with the financial plan submitted to NHS England in May 2015. There are however variances against the full year budget within individual cost areas. See the table in section 1a and appendix 1 for FOT variances from budget. 1e. Reserves SNCCG has set aside two reserves, the Commissioning Reserve and the Transformation Fund. The Commissioning Reserve is being drawn down in twelfths to support the year to date position and is expected to be used in full to achieve our planned forecast outturn. The Transformation Fund has been ring fenced to support initiatives relating to winter resilience. This fund is shown as fully committed in the year to date position, including the

£216k YTD cost of an unplanned £288k cost transfer from West Norfolk CCG arbitrated by NHS England; however the CCG will need to exert discretion over its application and any commitments will need to be carefully managed to enable the Fund to be used to mitigate the financial risks faced by the CCG – see section 1f. 1f. Risks Each month the CCG undertake a line by line best, most likely and worst case assessment of the financial position. The difference between the worst case and most likely costs are considered the full risk and these are then assessed against the probability of them happening to calculate the potential risk to the CCG. Presently we face a £911k potential risk. Against this however there are £911k of mitigations which also sit outside the forecast outturn, leaving a risk adjusted forecast outturn deficit of £6,645k, which is in line with the financial plan. 1g. Actions In addition to the original QIPP plan the CCG has identified a number of actions to support delivery of the financial plan, which the Governing Body needs to support or find alternatives of the same value to ensure delivery of the plan. These actions are being or will be taken:
• Renegotiating NSDC contract (estimated impact £52k) • Demand management of pathology test requests (estimated impact £70k) • Withholding payment from NNUH relating to Deaf Services overcharging and revising
Hearing Aid threshold with other Central Norfolk CCGs (estimated impact £21k) • Ceased purchase of intermediate care Spot beds (estimated impact £97k) • Renegotiating contracts with Community providers for provision of Intermediate Care
beds (estimated impact £68k) • Releasing Balance Sheet accruals no longer required (estimated impact £65k) • Application of efficiency to renegotiated contracts (estimated impact £40k)
2. QIPP SNCCG had £5,571k of QIPP schemes in the 2015/16 financial plan which needed to be delivered to meet our planned £6,645k deficit. The forecast outturn for those schemes has since been revised down due to slippage but they have been replaced by new schemes which are forecast to deliver the required planned savings and form part of the forecast outturn described in section 1d. Detail of each QIPP scheme with year to date and forecast outturn delivery is shown below. Total delivery is £3,173k year to date, which is £722k behind plan; the actions in section 1g need to be taken to recover this deficit.

M9 In-
Month
Plan
M9 In-
Month
Actual
M9 In-
Month
Variance
M9 YTD
Plan
M9 YTD
Actual
M9 YTD
VariancePlan FOT Variance
1 Application of 2% QIPP efficiency to NCH&C -435 -36 -36 0 -326 -326 0 -435 -435 0
2 Application of 4% QIPP efficiency to CSU -96 -8 -8 0 -72 -72 0 -96 -96 0
3 Impact from transactional agreements on the CCG -400 -33 -35 -1 -300 -311 -11 -400 -415 -15
4 ICES VAT recovery -200 -16 -16 0 -152 -152 0 -200 -200 0
5 Coding and Counting challenges -1,550 -129 -40 89 -1,163 -360 802 -1,550 -1,340 210
6 Impact from > 75s -334 -30 0 30 -247 -237 10 -334 -355 -21
7 Revised clinical thesholds policies -225 -25 -3 22 -150 -153 -3 -225 -31 194
8 Prescribing incentive scheme -1,105 -137 -23 114 -692 -447 245 -1,105 -812 293
9 Biosimilar HCD -96 -10 -10 0 -65 -52 13 -96 -52 44
10 Reduction in CHC spend through tighter controls -650 -54 -126 -72 -488 -582 -94 -650 -995 -345
11 ICES Efficiency scheme -30 -2 -44 -42 -23 -252 -229 -30 -345 -315
12 Formulary review and implement agreed restrictions -350 -44 0 44 -218 0 218 -350 0 350
13 Continence services -100 0 0 0 0 0 0 -100 -50 50
-5,571 -525 -340 185 -3,895 -2,944 952 -5,571 -5,127 444
0 0 -129 -129 0 -229 -229 0 -539 -539
-5,571 -525 -469 56 -3,895 -3,173 722 -5,571 -5,666 -95
In Month Position £'000s YTD Position £'000s Full Year Position £'000s
Original Schemes
Additional Schemes
ID No South Norfolk CCG QIPP at Month 9Full Year
Plan £'000s
See the QIPP report for more detail of these schemes and their delivery. In addition to this the CCG anticipate withholding of fines from providers to pay for Private Provider over performance. This over performance and cost is being driven by increased activity in the Acutes, particularly non-elective activity at NNUH. Fines do not currently form part of our QIPP reporting. 3. Underlying Position The table below shows that South Norfolk’s underlying position is a £5.6m deficit, this is calculated by taking our forecast outturn £6.6m deficit and removing non-recurrent income and expenditure. This position means that when allocation changes, growth and other cost pressures are taken into account the likely QIPP programme required to bring the CCG back to the £1.2m surplus position required by NHS England in 2016/17 is c. £13.3m. Any improvement that can be made to the underlying position in 2015/16 will reduce the QIPP target in 2016/17.
£m
2015/16 Forecast Outturn -6.6
Less 2014/15 surplus brought forward -0.6
2015/16 In-year position -7.3
Remove non-recurrent allocation -2.0
Remove non-recurrent expenditure 3.6
2015-16 Underlying Deficit -5.6
4. Allocation Adjustments There were three allocation adjustments in month 9, the largest being a non-recurrent increase for the 2014-15 Quality Premium Award. The other adjustments were for in-year Mental Health Liaison Psychiatry and MoD Out of hours. For all allocation increases we expect to incur equal cost with a net nil difference to our underlying position.

Description
Revenue
Resource
£000
Funding Type
Annual Allocation at Month 8 263,301
MoD - Out of hours - NHS England 3 Non-Recurrent
Liaison Psychiatry - NHS England 46 Non-Recurrent
14-15 Quality Premium award - NHS England 340 Non-Recurrent
Annual Allocation at Month 9 263,690 5. Activity Activity information is provided in the Integrated Quality & Performance Report. 6. Balance Sheet Statement of Financial Position at 31st December 2015 Statement of Financial Position at 31st
December 2015 £'000s
Position at
31/03/15
Position at
30/09/15
Position at
30/10/15
Position at
30/11/15
Position as
at 31/12/15
Comments
ASSETS EMPLOYED
Current assets
Trade and Other Receivables 4,136 4,727 3,845 5,526 2,532
Trade recievables increased in month 8 due to BCF
prepayment of December invoice (£1.7m) but an in-month
reduction in prepayments and a review of aged debts carried
out in month to chase all older than 30days (£0.1m) prior to
draft accounts preparation have significantly reduced them
to within normal levels.
Cash and Cash Equivalents 1,320 1,960 378 142 82
Cash values increased in September as some supplier
invoices were held awaiting credit notes, but since October
have been back to managed levels.
Total current assets 5,457 6,687 4,223 5,668 2,614
Current liabilities
Trade and Other Payables (21,891) (23,581) (25,370) (24,753) (23,003)SNCCGs level of creditors is expected to remain within
£21m to £25m. Slight decrease in Nov as payments made.
Provisions for liabilities and charges 0 0 0 0
Total current liabilities (21,891) (23,581) (25,370) (24,753) (23,003)
Non current liabilities
Trade and Other Payables (736) (582) (582) (582) (582)Research & Development deferred income for various
ongoing projects over one year.
Total non current liabilities (736) (582) (582) (582) (582)
Net assets employed (17,171) (17,476) (21,729) (19,667) (20,972)
FINANCED BY TAXPAYERS EQUITY
General fund (17,171) (17,476) (21,729) (19,667) (20,972) Negative figure as liabilities exceed assets.
Total taxpayers equity (17,171) (17,476) (21,729) (19,667) (20,972) CCGs are required to manage their cash so balances are no more than 1.25% of the monthly drawdown amount and our cash balance has now returned to normal levels.

7. Better Payment Practice Code The table below shows SNCCG’s performance against the Better Payment Practice Code (BPPC) up to December 2015; the CCG’s requirement is to pay 95% of eligible invoices within 30 days. In April to December this year that target has partly been met, with 96.8% compliance for NHS invoices but only 94.0% for non-NHS invoices giving a total of 94.5%. Despite only being partly met this is an improvement on earlier in the financial year, September’s year to date total was 93.5%, and 94.3% were paid within 30 days in October and November. The target not being met for non-NHS invoices is due to inefficiencies in the validation and approval process of invoices and the system automatic escalation process. The CCG is reviewing the BPPC report regularly with a focus on Non-NHS invoices to ensure that this percentage is further improved and invoices with queries are dealt with in a timely manner. The CCG takes its Better Payment Practice Code seriously and aims to pay all providers within the 30 days.
Better Payment Practice Code - Measures of Compliance
Apr 15 -
Dec 15
Apr 15 -
Dec 15
Non-NHS Payables Number £000
Total Non-NHS trade invoices paid in the year 6,980 49,736
Total Non-NHS trade invoices paid within target 6,558 44,759
Percentage of Non-NHS trade invoices paid within target 94.0% 90.0%
Apr 15 -
Dec 15
Apr 15 -
Dec 15
NHS Payables Number £000
Total NHS trade invoices paid in the year 1,801 132,746
Total NHS trade invoices paid within target 1,744 132,274
Percentage of NHS trade invoices paid within target 96.8% 99.6%
Apr 15 -
Dec 15
Apr 15 -
Dec 15
TOTAL Payables Number £000
Total invoices paid in the year 8,781 182,482
Total invoices paid within target 8,302 177,032
Percentage of total trade invoices paid within target 94.5% 97.0%
David Gilburt, Interim Chief Finance Officer – NHS South Norfolk CCG, 26th January 2016

Appendix 1 SNCCG M9 In Month, YTD and Forecast Outturn Financial Positions
M9
budgetM9 actual
M9
variance
M9 YTD
budget
M9 YTD
actual
M9 YTD
variance
Full Year
budget
Full Year
forecast
Full Year
variance
INCOME -22,173 -22,173 0 -197,951 -197,951 0 -263,691 -263,691 0
ACUTE NNUHFT 7,735 7,655 -80 70,714 70,203 -510 94,756 93,064 -1,692
WSHFT 1,103 1,116 13 9,856 9,860 4 13,199 13,203 4
CUHFT 143 137 -7 1,281 1,243 -38 1,716 1,658 -58
JPHFT 87 69 -19 781 754 -27 1,046 1,005 -40
QEHFT 84 92 8 749 762 13 1,003 1,016 13
Papworth 56 41 -15 504 571 67 675 762 87
Other Acute Contracts 72 62 -10 640 617 -23 857 822 -35
Non Contract Activity 157 107 -49 1,399 1,270 -129 1,874 1,674 -200
Private Providers 486 565 79 4,337 4,952 615 5,808 6,602 795
High Cost Drugs - NNUHFT 546 603 57 4,834 4,663 -171 6,489 6,267 -222
High Cost Drugs - WSHFT 47 51 5 413 348 -65 555 464 -91
High Cost Drugs - Other 39 52 14 290 288 -3 385 384 -1
Ambulance 602 662 60 5,416 5,644 228 7,221 7,496 274
EPA Pathology 298 282 -16 2,665 2,538 -127 3,568 3,384 -184
Risk Share 0 1 1 0 123 123 0 147 147
Other Acute 10 34 24 92 272 180 123 358 235
Acute QIPP -130 0 130 -1,157 0 1,157 -1,550 0 1,550
ACUTE Total 11,335 11,529 194 102,814 104,109 1,294 137,724 138,306 582
COMMUNITY HEALTH SERVICES NCH&C 1,851 1,898 47 16,764 16,925 161 22,318 22,422 104
Intermediate Care 101 89 -12 1,024 1,008 -16 1,328 1,242 -86
Long Term Conditions 150 109 -41 1,349 1,185 -165 1,799 1,478 -321
LTC Risk Share -79 -81 -2 -712 -836 -123 -950 -1,075 -125
ICES 98 57 -41 881 652 -229 1,175 877 -298
Reablement 87 87 0 787 787 0 1,049 1,049 0
Other Community 180 150 -30 1,375 1,411 35 1,793 1,883 91
COMMUNITY HEALTH SERVICES Total 2,389 2,310 -79 21,469 21,132 -338 28,512 27,875 -637
CONTINUING CARE CHC Adults 1,479 1,556 77 13,266 13,595 329 17,608 18,014 406
CHC Children 39 38 -1 350 276 -75 466 384 -83
CHC Risk Pool 0 0 0 731 814 83 731 814 83
NELCSU CHC Assessment 52 50 -2 458 453 -5 609 604 -5
CHC QIPP -59 0 59 -526 0 526 -700 0 700
FUNDED NURSING CARE 146 160 14 1,294 1,187 -107 1,723 1,583 -139
CONTINUING CARE Total 1,657 1,804 147 15,573 16,325 752 20,437 21,398 961
MENTAL HEALTH NSFT 1,313 1,313 0 11,814 11,814 0 15,752 15,752 0
IAPT 175 175 0 1,578 1,578 0 2,105 2,105 0
Child & Adolescent Mental Health 48 33 -15 430 259 -171 574 339 -234
Learning Difficulties 160 153 -7 1,440 1,283 -157 1,920 1,651 -269
Other Mental Health 183 163 -21 1,357 1,273 -85 1,810 1,669 -141
MENTAL HEALTH Total 1,879 1,837 -43 16,621 16,208 -413 22,161 21,517 -644
PRIMARY CARE Prescribing PPA 3,187 3,042 -145 28,314 27,745 -569 37,537 36,762 -775
Prescribing PPA QIPP -139 0 139 -1,166 0 1,166 -1,555 0 1,555
Prescribing Recharges -86 -69 17 -647 -562 86 -858 -749 108
Prescribing Rebates -7 -13 -6 -54 -129 -75 -72 -173 -101
Central Drugs 10 6 -4 74 62 -11 98 83 -15
Oxygen 63 71 9 563 592 29 750 790 39
Dressings 33 38 5 248 275 28 328 374 46
Other Prescribing Costs & Income 127 124 -3 955 961 6 1,265 1,282 17
NELCSU Medicines Management 36 38 2 324 342 17 433 456 23
Out of Hours and 111 Services 205 201 -4 1,843 1,794 -49 2,458 2,396 -62
Local Enhanced Services 94 118 25 842 1,125 283 1,123 1,487 363
Over 75s (excluding main providers) 79 45 -34 712 406 -307 950 541 -409
PRIMARY CARE Total 3,600 3,601 1 32,008 32,612 603 42,456 43,248 791
OTHER Patient Transport 138 125 -13 1,245 1,185 -60 1,660 1,554 -105
Better Care Fund 683 683 0 6,149 6,149 0 8,199 8,199 0
Safeguarding 8 8 0 72 74 2 95 98 3
CSU Programme Costs 49 96 47 443 601 158 591 802 211
Other 95 206 111 857 972 116 1,142 1,354 212
Transformation Fund 100 -116 -216 899 683 -216 1,198 910 -288
Contingency Reserve 64 0 -64 574 0 -574 766 0 -766
Balance Budget to Plan 866 866 0 -16 -16 0 0 0 0
OTHER Total 2,003 1,869 -134 10,222 9,648 -574 13,651 12,917 -733
CORPORATE Running Costs 676 415 -261 4,046 3,788 -258 5,395 5,074 -321
CORPORATE Total 676 415 -261 4,046 3,788 -258 5,395 5,074 -321
Total Expenditure 23,540 23,364 -175 202,754 203,821 1,067 270,336 270,336 0
(SURPLUS)/DEFICIT 1,367 1,192 -175 4,803 5,870 1,067 6,645 6,645 0
Note - negative variance = underspend and positive variance = overspend
YTD Position £'000s Full Year Position £'000sIn Month Position £'000s

1
Subject: Month 9 QIPP Delivery (2015/16) and Planning (16/17) Report
Presented by: Margaret Blackett, Interim Chief Officer
Prepared by:
Iain Taylor-Allen, Head of Performance and Business Intelligence
Submitted to: Governing Body
Date: 26th January 2016
Purpose of paper:
To inform the Governing Body of progress delivering SNCCGs 15/16 QIPP programme at month 9.
Executive Summary:
QIPP Delivery 2105/16 NHS South Norfolk CCG is reporting QIPP delivery of £3,173k to the end of Month 9 (December) against a budgeted plan of £3,895k, which is £723k behind plan. In Month 9 the CCG delivered £469k of savings, an increase on £410k delivered in Month 8. The year to date delivery at the end of Month 9 remains ahead of the revised phased delivery plan of £3,142k, with a favourable variance of £31k (Table 1 - page 3). However, it should be recognised that this has only been achieved as a result of an additional £229k (YTD) in year actions (Table 2 - page 4). Despite the progress made over the last few months the CCG is reporting a £444k risk to the delivery of the original £5,571k QIPP savings plan, with a reported forecast outturn of £5,127k, an improvement of £580k compared to month 8 (Table 2 - page 4).. The improved FOT is primarily due to a £640k contract variation submitted to the NNUHFT for under-delivery of Emergency Clinics. To mitigate the risk of under delivery of the 2015-16 QIPP programme, SNCCG has introduced a series of additional in year actions with a total reported value of £499k at month 9 (Table 2 - page 4). With the additional in year actions the reported 2015-16 QIPP FOT at month 9 is £5,626k, £55k better than plan. Whilst South Norfolk CCG is still reporting delivery of the planned financial position, it should be noted that the risk to delivery remains. Furthermore, many of the additional and increasingly challenging options for in year savings are already being implemented, reducing opportunities for further in year mitigation should this be required. At month 9 the reported position for SNCCGs three high QIPP programmes is as follows: Continuing Health Care - £126k delivered in month, £582k Month 9 YTD, with a forecast outturn of £995k, £345k above plan. See page 5 Prescribing - £23k delivered in month, £447k Month 9 YTD, with a forecast outturn of £812k, £293k below plan. See page 5
Agenda item: 6.2

2
Coding and Counting - £40k delivered in month, £360k Month 9 YTD, with a forecast outturn of £1,340k, £210k below plan. See page 6 QIPP Planning 2016/17 Progress to date is as follows:
• £14,121k total value of Opportunity • 37 projects in the ‘Gateway Process’ • 25 (68%) already achieved ‘approval to implement’, valued at £11,639k • 6 (16%) at Project Initiation Document stage, valued at £1,708k
Recommendation to Governing Body:
The Governing Body is asked to:
note and comment on progress to month 9 (December) with delivering SNCCGs challenging programme of savings, and the risks associated with the significant increase in required monthly savings to the end of the year to achieve the planned financial position;
Identify any additional in year opportunities for review and inclusion in the 15/16 QIPP Programme.
Key Risks
Clinical:
Programme budgets may need to be revised if funds are unavailable.
Finance and Performance:
Achieving the 15/16 QIPP target is critical to delivering the CCG’s financial position.
Impact Assessment (environmental and equalities):
N/A – Quality Impact Assessments completed and monitored for each QIPP scheme as part of the development process.
Reputation: Service redesign and/ or restriction may result in negative publicity for the CCG.
Reputational risk if the CCG fails to meet its 2015/16 financial targets.
Legal: N/A
Resource Required:
N/A
Reference document(s):
N/A
NHS Constitution:
N/A
Conflicts of Interest:
N/A
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)

3
1. QIPP Delivery – Month 8 Summary 1.1 The CCG has confirmed financial results up to and including Month 9. At Month 9 YTD
delivery stands at £3173k against a budgeted plan of £3,895k and a revised phased delivery plan of £3,142k. In month the CCG delivered £469k of savings, an increase from £410k delivered in Month 8.
1.2 The CCG is still striving to deliver the required £5,571k to achieve the financial position. However, the QIPP forecast outturn has been risk assessed at £5,127k in Month 9 (details in section 2 of this report) against the original plan of £5,571k.
1.3 The CCG recognises the need to identify and action additional contingency to provide
greater assurance of £5,571k delivery. Consequently, the CCG has identified and is taking action to implement an additional £499k of schemes to extend the current programme, £229k of which has already been delivered YTD
Table 1 – 2015/16 QIPP Savings Actuals vs. Budgeted and Phased Plans (Month 9)
£0.308
£0.616 £0.935
£1.373
£1.850
£2.326
£2.846
£3.370
£3.895
£4.453
£5.007
£5.571
£0.147£0.233
£0.435£0.607
£0.814
£1.447
£1.902
£2.486
£3.142
£3.884
£4.672
£5.572
£0.133 £0.239
£0.500
£0.780
£1.139
£1.621
£2.317£2.595
£3.173
£0.0
£1.0
£2.0
£3.0
£4.0
£5.0
£6.0
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
15/16 QIPP Savings Actual Vs. Budgeted & Revised Phased Delivery Plans - Month 9
Budgeted Delivery Plan (Monthly Cumulative) Revised Delivery Plan (Monthly Cumulative)
Actual Delivery (Monthly Cumulative)

4
Table 2 - South Norfolk M9 QIPP
Month 9
Plan Actuals Variance Plan Actuals Variance Plan FOT Variance
1 Application of 2% QIPP efficiency to NCH&C -36 -36 0 -326 -326 0 -435 -435 0
2 Application of 4% QIPP efficiency to CSU -8 -8 0 -72 -72 0 -96 -96 0
3 Impact from transactional agreements on the CCG -33 -35 -1 -300 -311 -11 -400 -415 -15
4 ICES VAT recovery -16 -16 0 -152 -152 0 -200 -200 0
5 Coding and Counting challenges -129 -40 89 -1,163 -360 802 -1,550 -1,340 210
6 Impact from > 75s -30 0 30 -247 -237 10 -334 -355 -21
7 Revised clinical thresholds policies -25 -3 22 -150 -153 -3 -225 -31 194
8 Prescribing incentive scheme -137 -23 114 -692 -447 245 -1,105 -812 293
9 Biosimilar HCD -10 -10 0 -65 -52 13 -96 -52 44
10 Reduction in CHC spend through tighter controls -54 -126 -72 -488 -582 -94 -650 -995 -345
11 ICES Efficiency scheme -2 -44 -42 -23 -252 -229 -30 -345 -315
12 Formulary review and implement agreed restrictions -44 0 44 -218 0 218 -350 0 350
13 Continence services 0 0 0 0 0 0 -100 -50 50
-525 -340 185 -3,895 -2,944 952 -5,571 -5,127 444
Plan Actuals Variance Plan Actuals Variance Plan FOT Variance
14 Spot & Block Beds 0 -75 -75 0 -109 -109 0 -220 -220
15 EPA 0 -54 -54 0 -100 -100 0 -140 -140
16 Hearing AID AQP: NNUH Norfolk Deaf Association Credit 0 0 0 0 0 0 0 -21 -21
17 Ophthalmology HCD 0 0 0 0 0 0 0 -1 -1
18 NSDC Tariff Negotiation 0 0 0 0 0 0 0 -52 -52
19 Control Acute Private Provider spend 0 0 0 0 0 0 0 0 0
20 Balance Sheet Review 0 0 0 0 0 0 0 -65 -65
21 Application of 2% QIPP efficiency to Serco Contract 0 0 0 0 -20 -20 0 -40 -40
0 -129 -129 0 -229 -229 0 -539 -499
-525 -469 56 -3,895 -3,173 723 -5,571 -5,666 -55
Full Year Position £'000s
ID No Original SchemesIn Month Position £'000s YTD Position £'000s Full Year Position £'000s
Total Original
Total Additional
Total QIPP
ID No Additional QIPP SchemesIn Month Position £'000s YTD Position £'000s

5
2. Major Programme Delivery
2.1 Continuing Health Care (CHC)
Delivery Team
GB Clinician – Graham Clarke
Director Accountable – Margaret Blackett
Management Lead - Ann Borrows
Clinical Lead – Alaina Barber
BI Lead – Sarah Bird
Finance Lead – Neil Blackburn
Support Co-ordinator – Sonia Bright
The CHC Programme continues to deliver ahead of the revised plan agreed in August, with £126k delivered in Month 9. The increased pace of delivery continues to support a revised forecast outturn of £995k, £345k above the original plan.
Complex Case Review Panel – Where packages of care have been brought to panel and reviewed, the value of the savings per week where the case has been deferred has been greater than anticipated.
Responsible Commissioner Review – A detailed review of patient packages of care has identified weekly costs greater than originally modelled and as a consequence has increased the level of available savings.
Broadcare Review – The review to determine whether patient packages are accurate, remain current and are suitable for patient need has achieved savings per patient in excess of expectations. The plan was based on a desktop review packages and removal of non-essential packages, however, the review also identified additional opportunity from duplicate or redundant packages.
Following a review of the impact of the VCFM contract in month 9, the CCG is no longer forecasting any additional in year savings from this workstream. To mitigate the forecast under delivery from VCFM, the CCG has focussed resource on completing a full review of Broadcare by the end of January and has a high level of confidence that additional savings will be actioned, maintaining the £995k FOT. 2.2 Prescribing
Delivery Team
GB Member/ Clinical Lead – Cathal Daly
Director Accountable – Margaret Blackett
Management Lead - Gill Bennett
BI Lead – Steve Powles
Finance Lead – Martin Browne
CSU Lead – John Reuben
The Prescribing scheme delivered £447k of savings from switches (Month 9 YTD) against a budgeted plan of £692k. Slippage in implementing the scheme reduced the available time to achieve the full year savings plan of £1,105k. As a consequence of delayed implementation, a £812k forecast outturn for the scheme has been reported at the end of month 9.

6
2.3 Acute
Delivery Team
GB Member/ Clinical Lead – Keeva Rogers
Director Accountable – Andrew Spring
Management Lead - Jim Barker
BI Lead – Seb Foster
Finance Lead – Andy Cook
CSU Lead – Frank Hume
Delivery of the Coding and Counting work programme continues to represent the greatest risk to the CCG out of the three major programme areas in 15/16. At Month 9 the CCG is reporting delivery of £360k YTD against a plan of £1,163. To ensure maximum benefit is achieved in challenging circumstances, South Norfolk CCG continues to pursue every opportunity to drive pace in delivery:
• Introduced new challenge process from November utilising all sources of challenges
• Continued pursuit of existing challenges as per NELIE and learning from other CCGs
(Essex, Cambridge, etc)
• Last week / next week work plan monitoring in place The issues impacting on delivery have been well documented, data access restrictions, under-delivery of external specialist support and pace of decision-making in the central system. However, despite the significant challenges SNCCG is reporting an improved revised forecast outturn of £1,340k at month 9 due to a high level of confidence in securing a contract variation for under delivery of Emergency Clinics at the NNUHFT. This is £210k under plan for this programme of work. 3. QIPP Planning 2016/17 3.1 As part of the three year financial recovery process SNCCG plans to deliver a QIPP
programme of circa £11,000k in 2016/7. This is a challenge to the organisation and requires considerable planning and resource.
Progress to date is as follows:
• £14,121k total value of Opportunity • 37 projects in the ‘Gateway Process’ • 25 (68%) already achieved ‘approval to implement’, valued at £11,639k • 6 (16%) at Project Initiation Document stage, valued at £1,708k
The current breakdown of schemes by Programme Area and Gateway stage are summarised in the table below:

7
SNCCG 2016/2017 QIPP Programme Plan
Programme Area No. of Schemes Value
Gateway 3 - Approval to
Implement
Value
(£m)Gateway 2 - PID
Value
(£m)
Gateway 1 - Plan on
a Page
Value
(£m)Gateway 0 - Idea
Value
(£m)
Acute 19 6.201 12 5.064 3 0.887 4 0.250 0 0.000
Acute Demand Management 2 1.145 0 0.000 1 0.621 1 0.524 0 0.000
Community Services 6 1.500 5 1.400 1 0.100 0 0.000 0 0.000
Continuing Healthcare 1 0.897 1 0.897 0 0.000 0 0.000 0 0.000
Mental Health 3 0.126 1 0.026 1 0.100 0 0.000 1 0.000
Children & Families 2 0.318 2 0.318 0 0.000 0 0.000 0 0.000
Primary Care 3 1.934 3 1.934 0 0.000 0 0.000 0 0.000
Better Care Fund 1 2.000 1 2.000 0 0.000 0 0.000 0 0.000
Totals 37 14.121 25 11.639 6 1.708 5 0.774 1 0.000
68% 16% 14% 3%
Gateway StatusSummary

Agenda Item: 6.5b
Meeting: SNCCG Governing Body Part 2
Date: 27 October 2015
South Norfolk Clinical Commissioning - Improvement Plan Report
Version Date: 12/01/2016
Version: v1.8
PWC Ref: Action Owner Priority Status RAG Status
Planned
Delivery Date Commentary on Delivery
1 (Pg.15)
Financial Reporting - The CFO should rapidly strengthen the financial
reporting to the Governing Body and sub committees, with reference to
good practice examples from other CCGS. Chief Finance Officer High Completed
We are constantly looking to identify further improvements that can be
made to reports and reporting arrangements
2 (Pg.15)
Communication - There should be clear and consistent communication of
the financial challenge externally to the CCG, including the presentation
of a finance report in the public section of every Governing Body meeting Chief Finance Officer High Completed
The communication of the financial challenge and current performance are
undertaken in the public element of the .board
3 (Pg.15)
Financial Planning - The CCG should develop a clear mid to long term
financial plan, linked to the CCGs overall strategic plan, which sets out
when and how the CCG will return to balance Chief Finance Officer High Completed
Initial plan submitted on 7th October 2015. Further iterations will be
required, assumptions may change and 2015/16 delivery will impact on
future plans
4 (Pg.15)
QIPP - The CCG should seek external support in the development and
implementation of the 2016/17 QIPP schemes. The CCG should use this
external review to formalise the process of identifying , developing and
implementing QIPP within the existing PMO structure to ensure that a
robust mechanism for the development of schemes is in place for future
years Chief Officer High Completed
5 (Pg.15)
Management Capacity - The CCG must undertake a complete, bottom up
review of management capacity based on its priorities and plans to
develop a recruitment plan that will meet its needs Chief Officer High Completed
6 (Pg.15)
Governing Body - The CCG must urgently commission comprehensive
organisational development support for the Governing Body. This should
include, as a minimum: The role and function of the Governing Body;
NHS finances; and Team building and development Chair High Completed
7 (Pg.15)
Turnaround - The CCG should clarify the roles and responsibilities of the
Turnaround Director. In the short term, this should be more traditional
hands on TD role which provides capacity to deliver turnaround whilst
steadying the organisation, allowing the accountable officer time to work
more strategically on the sustainability of the CCG and engagement Chief Officer High Completed
8 (Pg.15)
External Delivery Support - The CCG should urgently commission
external delivery support to facilitate the delivery of the QIPP scheme.
The PMO should be fully embedded and handed over to substantive staff Chief Officer High Completed The PMO is now staffed with substantive staff.
9 (Pg.15)
CCG Chair - The CCG chair should seek opportunities for external
support and mentoring from experienced CCG Chairs with NHS England
support Chair Medium Completed
10 (Pg.15)
Objectives - The CCG Chair should working with the Governing Body to
develop a clear set of objectives for the organisation and members of the
Governing Body. This should address the top priorities for the CCG over
the next eight weeks including development and delivery of QIPP,
financial reporting, relationship with the CSU and management capacity,
in order to demonstrate to the Governing Body and NHS England the
leadership capability in the organisation. The Chair should hold
Governing Body members tightly to account for the delivery of these
objectives, working with NHS England if necessary. Chair/ Chief Officer High Completed
11 (Pg.15)
Executive Portfolios - A full review of the executive portfolios and
responsibilities needs to be undertaken, to ensure appropriate focus and
balance across the team. In particular, only one member of the Executive
Team should adopt an oversight role, with other Executive Team
members responsible for individual areas, for example, finance, QIPP,
commissioning etc. Chief Officer High Completed
12 (Pg.15)
CSU - The CCG should work with other CCGs to determine an approach
to improving the value obtained from the CSU contract. This should
include clarification and quantification of current issues. The CCG should
work with the CSU to improve current relationships with support from NHS
England if required. Once the approach is agreed, a detailed action plan
with clear timelines and owners should be developed and executed. Chief Finance Officer Medium In Progress
Remedial
actions to be
agreed and in
place by 31 Dec
15
Draft detailed Action Plan completed 5/11/15. Meeting with CSU planned
for w/c 9/11/15 to finalise workplan. Fortnightly review meetings agreed.
Further meeting with CSU on 14th December where shortfalls in service
provided were identified. Remedial actions and timelines to remedy still to
be agreed
13 (Pg.15)
Commissioing - The CCG should work with Norwich and North Norfolk
CCGs to conduct a system-wide review of commissioning arrangements.
This review should clearly quantify and address any issues with current
CSU contracting arrangements and then potentially review more widely
the commissioning arrangements. Given the potential system-wide
impact, NHS England should be involved in the specification of any
review. Chief Officer High Completed
The arrangements will need to be embedded into the working practices of
the health community.
14 (Pg.15)
Commissioning - The central Norfolk commissioners consider a pooled
commissioning team to increase capacity and negotiating power with the
three main providers. This would also ensure that all three commissioners
are equally represented in contract negotiations. Chief Officer/ Chief Operating Officer High Completed
Paper agreed at Governing Body 28/07/15. Further work will be needed to
embed any arrangements into contracting and commissioning work
programmes.
15 (Pg.15)
Chief Financial Officer - The CCG should begin the recruitment process
for a permanent CFO, to allow an adequate period takes place between
the Interim CFO and the incoming substantive CFO to ensure continuity
and avoid a loss in momentum of the financial recovery plan. Chief Officer High In Progress Dec-15
CO appointment completed, process underway for the recruitment of
permanent CFO.
16 (Pg.15)
Clinical Engagement - A detailed engagement and communication plan
should be developed and subsequently delivered with a tailored approach
for each locality, but clearly linked to the CCG’s overall objectives and
FY15/16 plan. Chief Officer High Completed Oct-15 Paper to GB in October
17 (Pg.15)
Clinical Engagement - The CCG should consider reviewing the clinical
structure of the organisation including roles and responsibilities of
Governing Body members and Locality Leads. This review should also
consider the level of support and mentoring provided to clinical staff by
the Chair. Chair Medium Ongoing Jan-15
Discussions undertaken with GB members and Clinical Leads will be
converted into formal board paper in January
SNCCG Ref: Delivery of the Improvement Plan
Pg. 4 (Appendix A) Delivery of the 2015/16 Financial Plan Chief Operating Officer High In Progress Mar-16
Robust reporting, monitoring and governance structures in place, including
weekly PMO and FRSG meetings, Monthly Finance & Performance
Committee and Governing Body meetings now held monthly
Pg. 4 (Appendix A) Improvements in Financial management and reporting Chief Finance Officer High Ongoing Dec-15
We are continually working with the CSU to improve month end processes
and forecasting capability.But important changes introduced in terms of
Prescribing, CHC and risk assessment
Pg. 4 (Appendix A) QIPP Delivery Turnaround Director High Ongoing Mar-16
Robust reporting, monitoring and governance structures in place, including
weekly PMO and FRSG meetings, Monthly Finance & Performance
Committee and Governing Body meetings now held monthly
Pg. 4 (Appendix A) Development of the 2016/17 Plan Turnaround Director High In Progress Mar-16
16/17 Programme Plan in place with clear key milestones; aligned to local
and national contracting cycles (see detailed programme plan for
milestones)
Pg. 4 (Appendix A) Development of Medium Term Financial Plan Chief Finance Officer High Complete Mar-16Initial plan completed and submitted to NHSE 7th Oct 15. Further
iterations will be required.
Pg. 4 (Appendix A) Resetting of Strategic Direction Chief Officer High In Progress Mar-16 Work started, but will be directed by new AO
Pg. 4 (Appendix A) Implementing Transformational Change Turnaround Director High In Progress Mar-16
Care Homes Transformation project commenced. GP led Task & Finish
group set-up with first meeting on 06/11
Pg. 4 (Appendix A)
Ensuring that the CCG has the Capacity and Capability to deliver this
Agenda Chief Officer High Ongoing Mar-16
Adiitional staff appointed in 15/16. Seeking to appoint additional
commissioning staff. Next key stage review of running cost budget to
identify funding for new posts by December 2015
Pg. 4 (Appendix A) Implementing Collaborative Commissioning Arrangements Chief Officer High Completed Structures in place work on going to make them effective see below
Pg. 4 (Appendix A) Implementing Co-Commissioning arrangements for Primary Care Chief Operating Officer High In Progress Mar-16
Regional pro-forma signed-off by SNCCG CO December 2015 and sent to
NHSE for sign-off. Awaiting a response.
Pg. 4 (Appendix A)
Ensure the PMO is fit for purpose and delivers the relevant support to
QIPP delivery Chief Finance Officer High Completed
Additional capacity has been added to support delivery of QIPP. However,
the CCG will need to integrate the work into its working practices.
Pg. 4 (Appendix A) Engagement and improved locality Working Chief Officer High Completed
Actions taken:- Alignment of Directors and GB members to locality, set
agendas drawn up, individual practice visits and information being
reported on locality basis eg prescribing QIPP
Delivery of the 2015/16 Financial Plan
Pg. 5 (Appendix A) Management of the contracts and commissioning spend Chief Operating Officer High Ongoing
Mitigating actions to control forecast overspend in Acute Private Providers
taken.
Pg. 5 (Appendix A) Delivery of the Constitutional standards Chief Operating Officer High Ongoing Mar-17
Specific emphasis given to constitutional standards in contracting round,
all available contract levers being utilised
Pg. 5 (Appendix A)
QIPP Delivery:
- CHC Scheme
- Prescribing Scheme
- Coding & Counting Scheme
Turnaround Director:
- Director of Quality Assurance
- Director of Quality Assurance
- Chief Finance offficer High Ongoing Mar-16
Robust reporting, monitoring and governance structures in place, including
weekly PMO and FRSG meetings, Monthly Finance & Performance
Committee and Governing Body meetings now held monthly. Weekly
Project Delivery Group meeting embedded with PMO attendance and
detailed highlight reports

Agenda Item: 6.5b
Meeting: SNCCG Governing Body Part 2
Date: 27 October 2015
Pg. 5 (Appendix A)
Appropriate identification of financial risk and ensuring appropriate
mitigations are put in place Chief Finance Officer High Ongoing Nov-15
Detailed update provided as part of November's scheduled reporting
In future this schedule will be updated whenever necessary
Pg. 5 (Appendix A) Ensuring that there is improvement in the quality of services at NSFT Director of Quality Assurance High In Progress Jun-16 Monitoring through CQSG
Pg. 5 (Appendix A) Complete the signing of the NSFT contract Chief Operating Officer High Completed
Pg. 5 (Appendix A)
Undertake a timely review of CQUINs and identify the correct value of
recompense Director of Quality Assurance Medium Ongoing Dec-15 Awaiting Director of Quality and Patient Safety to start
Delivery of the 2016/17 plan
Pg. 5 (Appendix A) Finalise the Commissioning intentions Chief Operating Officer High Completed
Pg. 5 (Appendix A) Identification and implement the de-commissioning list Chief Operating Officer High Completed Included in Commissioning Intentions & 16/19 Programme Plan
Pg. 5 (Appendix A) Development of Vanguard bid about Nursing Homes Chief Operating Officer High In Progress Jan-15
Regional reserve monies made available to Mid Norfolk for non-recurrent
support in 2015/16. Q4 2015 work commenced to propose 'solution' to
care home impact. Paper to GB outlining process for 2016/17
Pg. 5 (Appendix A) Review of existing contracts Chief Finance Officer High In Progress Dec-15 Review underway led by Deputy CFO
Pg. 5 (Appendix A) Develop a transformational approach to urgent care Turnaround Director High In Progress Mar-16Care Homes Transformation project commenced. GP led Task & Finish
group set-up with first meeting on 06/11
Pg. 5 (Appendix A) Renegotiate BCF Turnaround Director High Completed Completed and in 2016/17 QIPP Plan
Pg. 5 (Appendix A)
Undertake a review of variation in primary care and identify potential
savings and put together an action plan to deliver these savings Chief Finance Officer High In Progress Apr-16
Initial data has been collected. GP lead has been identified. Project Task
& Finish group to meet w/c 16/11/15 to review draft workplan and
timescales
Financial Reporting
Pg. 37 Budget Report writing training for Finance staff Deputy Chief Finance Officer High Outstanding Dec-15
JH escalated to CSU POD Director 04/11/15 for resolution - awaiting
response
Pg. 37 Financial management training for budget holders Deputy Chief Finance Officer In Progress Dec-15 Training being developed -
Pg. 37 Finance Training for Governing Body Members Interim Chief Officer Completed
Pg. 37 Improve Risk assessment and reporting Interim Chief Officer Completed
Pg. 37Greater alignment of Activity and finance reporting Head of Performance and Business
Intelligence Completed
Pg. 37 Greater focus on reasons for variance and corrective action Deputy Chief Finance Officer Completed But work ongoing
Pg. 37 Monthly reports to Governing Body and Leadership Team Deputy Chief Finance Officer Completed
Planning
Pg. 38 To appoint Turnaround Director to drive the process Interim Chief Officer Completed
Pg. 38 To set up a small group to produce and implement a decommissioning list Chief Operating Officer Completed
Pg. 38 To set up a process for delivering 16/17 plan Turnaround Director Completed
Pg. 38
To engage with locality groups and individual members, other
commissioners and providers on draft commissioning intentions Chief Operating Officer Completed
Pg. 38
To undertake a high level assessment of individual schemes that make up
the 2016/17 plan and identify which schemes to further develop Turnaround Director Completed
Pg. 38
Identify any potential cost pressures and update the medium term
financial plan for any known factors Deputy Chief Finance Officer Completed Mar-16 MTFP producerd but a numberr of reiterations expected
Pg. 38 High Level 16/17 plan produced Turnaround Director Completed GB Paper produced
Pg. 38
Produce 16/17 plan taking account of allocation changes, NHS England ‘s
Operational plan and based upon fully worked up QIPP schemes Turnaround Director In Progress Feb-16
16/17 Programme Plan in place with clear key milestones; aligned to local
and national contracting cycles (see detailed programme plan for
milestones, including reviewing impact of allocation changes)
Capacity & Capability
Pg. 44
A full review of Executive portfolios will be undertaken and responsibilities
to ensure appropriate focus and balance across the team Interim Chief Officer Completed
Pg. 44The CCG will begin the recruitment process for a permanent Chief Officer Chair Completed
Leadership and Governance
Pg. 46
The CCG Chair will work with the Governing Body to develop a clear set
of objectives for the organisation and members of the Governing Body.
This will address the top priorities for the CCG over the next eight weeks
including the development and delivery of QIPP financial reporting
relationship with the CSU and management capacity. The Chair will also
hold the governing body members to account for the delivery of these
objectives, working with NHS England if necessary. Chair Completed
Pg. 46
The training of Corporate Affairs Manager to achieve the ICAS Advanced
certificate in Health service Governance by the Acting Head of Corporate
Affairs Acting Head of Corporate Affairs In Progress Mar-16 Course commences September 2016
Commissioning Plan
Pg. 48 Paper for approval to Governing Body Interim Chief Officer/ Chair Completed
Pg. 48 Shadow joint executive to meet
Interim Chief Officer/ Chief Operating
Officer Completed
Pg. 48 Creation of 2 virtual teams in partnership with neighbouring CCGs
Interim Chief Officer/ Chief Operating
Officer In Progress Dec-15 work being lead by the CSU
Pg. 48 Joint executive to meet
Interim Chief Officer/ Chief Operating
Officer Completed
Co-commissioning in Primary Care
Pg. 49
Amendments to Constitution and Co-commissioning paper to SNCCG
Governing Body Acting Head of Corporate Affairs Completed
Pg. 49 Consultation with member practices commences Acting Head of Corporate Affairs/ Chair On going Mar-16
Part of task and finish group work plan and includes holding a
Development Day first quarter 2016
Pg. 49 Meeting arranged with NHSE to review draft proposals Chief Operating Officer Completed
Pg. 49
Visit to Cambridge and Peterborough CCG to view Joint Committee
arrangements Chief Operating Officer Completed
Pg. 49 Formal proposal submitted for consideration Chief Operating Officer Completed
Pg. 49
Amendments to Constitution formally discussed and agreed at Council of
Members Acting Head of Corporate Affairs/ Chair Completed
Pg. 49 If approved, CCG moves to mobilisation and full implementation
Chief Operating Officer/ Acting Head of
Corporate Affairs In Progress
November 2015
– March 2016
Submission pro-forma signed by CO and sent to NHSE for signing. NHSE
to submit proforma for consideration and sign-off.
Locality Working
Pg. 50
Full discussion regarding direction of Locality working to be discussed at
Council of Members Chair/ All Clinical Leads Ongoing Dec-15 For discussion at next CoM
Pg. 50
To develop proposals in line with agreed outcomes from Council of
Members, to include any Constitutional changes as required.
Chief Operating Officer/ Acting Head of
Corporate Affairs Ongoing Jan-15 For discussion at next CoM 27th January

Subject:
Audiology Eligibility Threshold for Treatment proposals
Presented by:
Dr Dustyn Saint/Jocelyn Pike
Prepared by:
SNCCG Commissioning Team SNCCG Communications and Engagement Team
Submitted to:
SNCCG Governing Body
Date: 26 January 2016
Purpose of paper:
For decision on implementation of proposed audiology eligibility thresholds for treatment
Executive Summary:
The CCG Governing Body agreed to a period of consultation in order to understand the spectrum of opinions before making a decision on whether to increase the eligibility threshold for the provision of hearing aids to adults who are assessed with slight or mild hearing loss. This paper outlines the consultation activity that took place, provides key themes from the responses received and provides information on 16/17 contract negotiations.
Recommendation to Governing Body:
The Governing Body is asked to:
1. Consider the consultation feedback received 2. Consider this in relation to 16/17 contract negotiations 3. Make a decision as to whether the Audiology eligibility threshold proposals should be
implemented.
Agenda item: 6.3

Key Risks
Clinical:
1. May create additional pressure on health services due to social isolation, wellbeing etc.
2. The World Health Organisation state that hearing loss is in the top 20 leading causes of burden of disease and by 2030 will be in the top 10 causes of burden of disease
Finance and Performance:
The CCG estimates that increasing the eligibility threshold for the provision of hearing aids to adults assessed with slight/mild hearing loss could deliver a minimum saving of £176,878 from AQP providers. Other savings could be achieved by widening the eligibility threshold proposals to Acute non-AQP Direct Access Hearing service providers. Greater efficiencies could be made by agreeing tariff reductions during 16/17 contract negotiations and agreeing a rebate on 15/16 activity.
Impact Assessment (environmental and equalities):
Equality Impact Assessment.
Audiology EIA, v3
06.01.16.doc
Reputation: If the Audiology threshold policy is implemented, SNCCG would be 1 of 2 CCGs in the country applying this measure. Three out of four CCGs in Staffordshire have decided not to implement hearing aid restrictions. North East Essex CCG has decided not to implement hearing aid restrictions.
Legal: There is a slight to moderate risk of legal challenge.
Resource Required:
Additional resource in the Acute Commissioning team is required in order to implement this policy
Reference document(s):
Hearing Loss
Guidance.zip
NHS Constitution:
2012 c. 7 PART 1 Further provision about clinical commissioning groups Section 26: 14Q Duty as to effectiveness, efficiency etc.
Each clinical commissioning group must exercise its functions effectively, efficiently and economically.
Conflicts of Interest:
None identified.
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
25.08.15 Leadership team 08.09.15 Governing Body

Feedback from the Audiology Restriction Consultation
19 January 2016 1. Introduction Since 2013, patients aged over 50 in Norfolk have benefited from direct access to adult hearing care services, delivered via Any Qualified Provider (AQP) NHS contracts with a range of local independent and NHS providers (Queen Elizabeth Hospital). Referrals are made directly from a patient’s GP enabling timely diagnosis and treatment. Additionally adults in Norfolk have benefited from Direct Access Hearing aid services available from other providers in the acute sector. Since the inception of the AQP process, there has been a steady increase in demand on hearing assessment and hearing aid services from these new providers, which has impacted on the financial situation faced by NHS South Norfolk CCG. Services from the acute sector which have been provided by Norfolk & Norwich University Hospital Foundation Trust (NNUHFT) and West Suffolk Hospital have been delivered via a block contract and despite close partnership working with these providers, exact finance and activity has not been possible to identify. A paper was presented to the SNCCG Leadership Team on 25 August 2015 and Governing Body on 8 September 2015 regarding the proposed eligibility thresholds to audiology services which detailed the potential savings for the AQP Independent Providers. It was agreed that a consultation would be carried out in order for the Governing Body to make an informed decision as to whether to proceed with the eligibility threshold proposals. The CCG launched this consultation, initially running from 9 November to 18 December, focussing on ‘Slight and Mild’ hearing loss for patients eligible for services commissioned under the AQP for adults 50 years and over. Following feedback from several interested parties, the CCG amended and refreshed it’s consultation on 11 December to widen the remit of the policy to all adults and extended the deadline for responses to 15 January 2016. This paper outlines the feedback from the consultation and provides the key themes from the feedback received. 2. Consultation The CCG consulted on its proposal to amend eligibility thresholds to access Direct Access Adult Hearing Services for adults aged 50 and over with hearing loss under 41dB. The policy would apply to patients with non-complex audiology conditions. Under the revised policy, the following exceptions for patients would apply:
Patients with hearing loss since childhood
Patients with a confirmed diagnosis of dementia
Patients with learning disability
Exceptionality for patients in employment with mild hearing loss who’s occupation
dictates a higher level of hearing capability i.e. patients who work in call centres
Patients with auditory processing disorder
Patients with severe multiple sensory disability
Patients with tinnitus
Sudden onset hearing loss
Multiple severe physical disabilities
Patients who are currently on an existing three year pathway, would only be affected if they were to be re-referred as a new patient. This policy does not include occupational hearing loss nor its related legal processes.

Any resulting changes to policy would also be reviewed on an annual basis. 3. Methodology The consultation focussing on ‘Slight and Mild’ hearing loss for patients aged over 50 years commenced Monday 9th November and was originally scheduled to conclude on Friday 18th December. The consultation was refreshed on 11 December to conclude on 15 January 2016 to widen the remit to all adults. Details of the proposed eligibility thresholds were made available on NHS South Norfolk CCG’s website (appendix 1) and the CCG invited comments on the following areas:
General feedback on the proposed changes to the CCG’s Commissioning policy
What impact a change in service may have on patients, and what the unintended consequences of this change may be
Comments and thoughts regarding the patients exceptions under the new policy
The priority of Adult Hearing Aid Services within the wider context of what the CCG commissions
Experiences of Adult Hearing Aid Services and the treatments and advice that was given to the patient
The document was emailed to a variety of stakeholders, including:
SNCCG Member practices
South Norfolk Patient Participation Groups
Healthwatch Norfolk
Norfolk County Council Health Overview and Scrutiny Committee (HOSC)
National Community Hearing Association
Norfolk Deaf Association
Age UK Norfolk
Equal Lives
South Norfolk Older People’s Forum
Action on Hearing Loss A briefing outlining the details of the consultation was provided to the Norfolk Health Overview and Scrutiny Committee (HOSC). HOSC confirmed that they would not be asking the CCG to present the proposals at its meeting on the 3rd December, but requested an internal briefing which was presented at the meeting. 4. Consultation 4.1 Stakeholder workshop A stakeholder workshop was held on 1 December 2015. Please see appendix 2 for feedback from this event. 4.2 Summary of Consultation feedback Please see appendix 3 for a full overview of the feedback received. The CCG is very grateful to those who provided feedback on this consultation. A large number of responses were received from respondents who shared their experiences of hearing aid services both positive and negative, giving the CCG a valuable insight into the impact hearing loss can have.

Many of the respondents acknowledged the financial challenge faced by the NHS, but felt that the CCG should reconsider the proposed eligibility threshold. Points raised included the following:
The negative impact on social isolation / mental health / cognitive decline of individuals who would no longer meet the criteria and the risk of an additional cost to the health economy
Hearing loss is relative to the individual, so defining a policy around a decibel level / hearing banding could be a hindrance
Concerns raised over fragmentation of services, particularly in relation to patients transitioning from child to adult hearing services.
How will the CCG address the needs of adults on benefits?
Stricter policies and monitoring is needed under the current AQP system
The AQP contracts have impacted on the hospital’s ability to manage caseloads, which has increased patient waiting times
If implemented, the restricted criteria would create a local clinical variation and does not adhere to NICE Guidelines
Possible negative impact on adults (18+) entering Further / Higher Education or employment
Hearing loss is a disability and requires appropriate support
Potentially low impact, as people with ‘Mild’ hearing loss may manage without hearing aids, or find using hearing aids an hindrance
Savings are small in comparison to the CCG’s total budget More detailed feedback is available on request and can also be accessed via the member’s area of SNCCG’s website. 5. Publicity Between 9th November 2015 and 15 January 2016 the CCG received two pieces of media coverage:
13th November – article on audiology consultation launch, editorial about ‘postcode lottery’ (EDP)
8th December – Letter: British Tinnitus Association criticises SNCCG’s proposed audiology policy (EDP)
5.1 Interested Groups Commissioners have met with several interested groups including the National Community Hearing Association, Action on Hearing Loss, British Academy of Audiology and National Children’s Deaf Society. These groups have expressed their view that not providing hearing aids to people with slight and mild hearing loss may impact the long term outcome and progressiveness of hearing loss in adults and young people.
6. 2016/17 Contract Negotiations AQP contracts are due to expire at the end of March 2016. South Norfolk, Norwich and North Norfolk Commissioners have arranged an AQP Hearing Aid service provider workshop to take place on 29th January in order to secure pathway efficiencies. For South Norfolk CCG this has the potential to realise an estimated £137,000 in efficiencies. One provider has also suggested that they may be willing to implement a rebate proposal that could see the CCG secure a further 10% rebate based on 15/16 activity levels, estimated at £21,000. If other AQP providers agree to follow this proposal, then this would bring the suggested rebate proposal to £54,000. Therefore the estimated efficiencies on 15/16 finance totals could be in the region of £191,000. If the decision is taken to agree the implementation of the proposed eligibility thresholds for Slight and Mild hearing loss, the savings from AQP Providers is estimated at £176,878.

It should be noted that the reduction in tariff and suggested rebate may not be forthcoming if the proposed restrictions are implemented. NHS SNCCG, will ensure that in 2016/17 all providers of Direct Access Hearing Aid services will be contracted on AQP terms. 7. Commissioning Framework for Hearing Services Currently several organisations including Action on Hearing Loss and the National Community Hearing Association are working with NHS England to develop the Commissioning Framework for Hearing Services. This framework will be published in April 2016 and will enable CCGs to follow good practice and reduce costs. It will also include model service specifications, and contracts etc. NHS South Norfolk CCG will ensure that flexible contractual provisions are made to enable the variation of in year contracts to apply all or parts of the forthcoming commissioning framework.
Appendix 1
Consultation on the Hearing Aids for People with Mild Adult-onset Hearing Loss
Commissioning Policy
Introduction
NHS South Norfolk Clinical Commissioning Group (CCG) is consulting with patients,
professionals, stakeholders and people living in South Norfolk on a new Commissioning
Policy regarding hearing aids for people with mild adult-onset hearing loss.
Context
Since 2013, adults aged over 50 in Norfolk
have benefited from direct access to adult
hearing care services, delivered via Any
Qualified Provider (AQP) NHS contracts
with a range of local independent and NHS
providers. Referrals are made directly from
a patient’s GP enabling timely diagnosis
and treatment.
Since the inception of the AQP, there has
been a steady increase in demand on
hearing assessment and hearing aid
services from these new providers, which
has impacted on the financial situation
faced by NHS South Norfolk CCG.
The CCG is proposing to revise its criteria towards adults who are eligible for hearing
aids, restricting the issue of hearing aids to patients with a hearing loss measured as
mild.
Why is this change proposed?
NHS South Norfolk CCG has given notice it will end the 2015-16 financial year with a £6.6
million deficit because of the financial challenges it faces. It aims to reduce costs in a
planned strategy that includes reviewing all areas of its expenditure, not just hearing aid
services. Other proposed savings so far are in prescribing costs, reducing expenditure in
What is ‘Any Qualified Provider’?
‘Any Qualified Provider’ (AQP) is a means of
commissioning certain NHS services in
England, with the intention of increasing the
choice that patients have in deciding when
and where they receive a treatment.
Clinical commissioning groups (CCGs)
determine the services to be commissioned
as AQP - providers must meet the
qualification criteria set for a particular service
and, once qualified, their service will appear
on Choose and Book for patients to select.
Change to the Consultation:
The CCG has decided to change and extend its audiology consultation, following
constructive feedback from members of the public received so far.
In response to feedback from a range of stakeholders, the CCG has made the
decision to consult on whether any proposed change in policy should apply to all
adults with mild hearing loss.

hospitals by examining more closely what the CCG is paying for and efficiencies in
community services.
A background on the range of health services that the CCG commissions can be found on
pages 8-13 of its Annual Report 2014-15.
If this proposal is adopted then the CCG would save an estimated minimum of £176,878
through restricting access to services via AQP providers (people aged 50 and over). Further
savings may be identified by applying this proposed policy across a wider age group.
Classification of Hearing Loss
The definition of adult-onset hearing loss is taken from the WHO document ‘Global Burden
of Hearing Loss’ where this is defined as ‘Cases of adult onset hearing loss due to ageing or
noise exposure. Excludes hearing loss due to congenital causes, infectious diseases, other
diseases or injury’.
Hearing loss is defined under the followings classifications:
Normal hearing (0-25 dB): At this level, hearing is within normal limits.
Mild hearing loss (26-40 dB): Mild hearing loss may cause inattention, difficulty
suppressing background noise, and increased listening efforts. Patients with this degree of
loss may not hear soft speech. Children may be fatigued after listening for long periods.
Moderate hearing loss (41-55 dB): Moderate hearing loss may affect language
development, syntax and articulation, interaction with peers, and self-esteem. Patients with
this degree of loss have trouble hearing some conversational speech.
Moderate – severe hearing loss (56-7- dB): Moderate-severe hearing loss may cause
difficulty with speech and decreased speech intelligibility. Patients with this degree of loss
do not hear most conversational-level speech.
Severe hearing loss (71-90 dB): Severe hearing loss may affect voice quality.
Profound hearing loss (>90 dB): With profound hearing loss (deafness), speech and
language deteriorate.
What is the CCG proposing?
The CCG is proposing to restrict access to Adult Hearing Services for patients with hearing
loss under 41dB.
The CCG's proposed policy will primarily impact on patients that have mild hearing loss as
part of their ageing (known as 'presbycusis'). In applying the policy, this will mainly affect
adult patients, although clinical advice will be sought for patients as they transition between
the children and adult audiology pathways. The CCG encourages feedback on how this
transition is managed as part of the consultation.
This policy would apply to patients with non-complex audiology conditions.
Under the revised policy, the following people with mild hearing loss will be eligible for
services:

Patients with hearing loss since childhood
Patients with a confirmed diagnosis of dementia
Patients with learning disability
Exceptionality for patients in employment with mild hearing loss who’s occupation
dictates a higher level of hearing capability i.e. patients who work in call centres
Patients with auditory processing disorder
Patients with severe multiple sensory disability
Patients with tinnitus
Sudden onset hearing loss
Multiple severe physical disabilities
People with moderate, severe or profound hearing loss will all continue to be eligible.
Patients who are currently on an existing three year pathway, would only be affected if they
were to be re-referred as a new patient.
This policy does not include occupational hearing loss nor its related legal processes.
The restricted policy would also be reviewed on an annual basis.
Impact
A number of providers have been commissioned via a standard NHS contract to provide
adult hearing aid services:
Scrivens
Specsavers
The Outside Clinic (Domiciliary)
Community Hearingcare Services
Queen Elizabeth Hospital Kings Lynn NHS Foundation Trust
Adult Hearing Aid services can also be accessed at the Norfolk & Norwich University
Hospital and the West Suffolk Hospital.
Applying this revised policy would produce potential savings of an estimated minimum of
£176,878 through restricting access to services via AQP providers (people aged over 50).
Further savings may be identified by applying this proposed policy across a wider age group.
How can I comment on this proposal?
NHS South Norfolk CCG is providing the opportunity to comment on the above proposal
regarding revising its commissioning policy for Adult Hearing Aids Services between Monday
9th November 2015 and Friday 15th January 2016.
The CCG would like to know the following:
General feedback on the proposed changes to the CCG’s Commissioning policy described above
What impact a change in service may have on patients, and what the unintended consequences of this change may be

Comments and thoughts regarding the patients exceptions under the new policy
The priority of Adult Hearing Aid Services within the wider context of what the CCG commissions
Your experiences of Adult Hearing Aid Services and the treatments and advice that was given to you
Comments on the above question can be answered via an online survey available here:
Feedback can also be sent to [email protected]
Or in writing to:
NHS South Norfolk Clinical Commissioning Group
Lakeside 400, Broadland Business Park
Old Chapel Way, Thorpe St Andrew NR7 0WG
What happens next?
South Norfolk CCG’s Governing Body will receive feedback and responses in time for its
meeting on January 26 2016, where it will make a decision on the proposal.
The outcomes of the decision will be communicated to everyone that responds, as well as all
affected professionals and stakeholders, after this date.

Appendix 2
South Norfolk Audiology Workshop – 1st December 2015
Workshop Notes
What would happen to current patients with ‘Mild’ hearing loss?
Patients already on the 3-year audiology services pathway would continue to receive
after care, replacements and support based on their needs
If the policy is introduced, new patients falling into the category of having ‘Mild’
hearing loss would not get NHS funded hearing services
How did the CCG reach ‘Mild’ hearing loss as the point with which to introduce restrictions?
Discussions were had around the clinical impact on people with ‘Mild’ hearing loss
and the effect this decision would have on their wellbeing
The CCG needs to focus on ensuring provision is available for urgent care and life
limiting illnesses and conditions
‘Mild’ defined as the range between 26-40 decibels
The CCG needs to consider the long term impact of its decision:
Increase in isolation in affected patients – from communities and families
Increase in related or other conditions for the individual
How will it affect people who live with ‘Mild’ hearing loss but don’t get check-ups?
The stigma of hearing loss – ‘non visual’ disability
Could create additional diagnoses of dementia
Older people / people with hearing loss – impact on driving ability?
Financial inequality of decision – some patients could afford hearing aids, others
couldn’t
Health and safety in the workplace of people with ‘Mild’ hearing loss without access
to hearing aids
Impact on people with dual sensory loss
Where does the scope of the CCG’s proposed policy change come from? How are they
working with current AQP providers?
Hearing services are being looked at alongside a range of other areas by the CCG
What work is being done regarding prevention? Could more resource focus on raising
awareness of hearing loss and early intervention? Patients who begin to use a hearing aid at
an earlier age are more likely to wear and use them long term.

Will this affect patients who need hearing aids in both ears or in a single ear? More definition
needed on ‘Mild’ hearing loss, as some patients cannot hear at certain frequencies. How will
the diagnosis / treatment of Auditory Processing Disorders be affected by the policy change?
More clinical / public education needed on hearing loss and associated services. Patients
are unaware they are on a ‘pathway’, and what that entails.
More analysis needed on the statistical impact on restricting services.
The CCG needs to focus on the whole of hearing aid services, rather than just AQP
provision – investigate inefficiencies in the whole system.
If the CCG’s policy is changed, more resource will be required to ‘police’ providers to
ensure patients are being treated in line with the policy
Focus on accessibility – not all independent providers can provide immediate support
Why focus on people over 50 as part of the proposed restricted policy?
The CCG will look at the impact on all people over the age of 18 years
People with ‘Mild’ hearing loss from childhood – what happens when they turn 18
years?
Discussing patient exceptions:
Patients on income support – how is this determined
Impact on adult social services
People looking for employment / volunteers / charity work – will they be exceptions?
Hearing loss as a CCG priority:
As important as all sensory needs
Impact on communication, which is a basic human function
Hearing loss research receives less funding than other conditions
Hearing loss will be one of the top 10 long term conditions by 2030
AQP system – inherently inefficient
How many people will this affect?
Is the CCG at risk of delaying bigger costs by restricting access to people with ‘Mild’ hearing
loss, as their condition will be worse and need further support once they have ‘Moderate’ to
‘Severe’ hearing loss.

Would more effective working relationships between commissioners, providers and the
voluntary sector not produce better results?
How will providers identify South Norfolk patients to ensure the changed policy is
implemented? Who would monitor this?

Appendix 3 - Feedback from the consultation 20/01/16 v3
The CCG has received feedback and comments from a wide range of stakeholders so far,
including members of the public, patients with hearing loss that have used services currently
available, support and advocacy organisations, and local Government and councillors.
Responses to online survey
From 9 November to 11 December 2015, the CCG launched and ran its consultation,
focusing on ‘Mild’ hearing loss patients eligible for services commissioned under AQP. This
would affect patients over 50 with ‘Mild’ hearing loss. The CCG amended and refreshed its
consultation on 11 December to widen the remit of the policy to all age groups, and
extended the deadline for responses to 15 January 2016.
The CCG has run an online survey to capture feedback on its proposed policy. For analysis,
this has been split into two sets of data – one set of feedback commenting on the proposed
policy change that would affect people over 50 years of age, and the other set focusing on
all patients with diagnosed ‘Mild’ hearing loss.
Data set one: 9 November to 11 December 2015
The CCG received 139 individual responses:
84 individual completed responses to its online survey
55 handwritten survey responses, supported by Action on Hearing
Responses are broken down into the following sources (multiple choices applicable):
Patient with hearing condition and / or with a hearing aid 80
Cochlear implantee 1
Carer or family member of a patient with a hearing condition 17
Audiologist 35
Health professional providing hearing aid services 8
Health professional not providing hearing aid services 4
GP and / or Primary Care team 0
Hearing support or advocacy organisation 6
Member of the Public 28
Other 5
Responders were also asked if they lived or work in South Norfolk or Breckland:
Yes – South Norfolk 49

Yes – Breckland 22
No – I do not work or live in either area 45
Did not answer 23
Data set two: 11 December to 15 January 2016
The CCG received 31 responses via its online survey.
Responses are broken down into the following sources (multiple choices applicable):
Patient with hearing condition and / or with a hearing aid 10
Cochlear implantee 0
Carer or family member of a patient with a hearing condition 8
Audiologist 8
Health professional providing hearing aid services 1
Health professional not providing hearing aid services 0
GP and / or Primary Care team 0
Hearing support or advocacy organisation 4
Member of the Public 8
Other 3
Responders were also asked if they lived or work in South Norfolk or Breckland:
Yes – South Norfolk 10
Yes – Breckland 6
No – I do not work or live in either area 15
Feedback on proposal
Impact of the Proposal
Feedback in support of the proposal:
Thresholds are needed for the modern NHS to cope with demand

Potentially low impact, as people with mild hearing loss may manage without hearing
aids, or find using hearing aids a hindrance
Patients with mild hearing loss would pay for their own hearing aids if diagnosed with
mild hearing loss
Stricter policies and monitoring needed under current AQP system
AQP contract has impacted on hospital’s ability to manage caseloads, which has
increased patient waiting times
Provide financial support for hearing aid purchase and maintenance if required
Maybe raising the threshold for people with a new diagnosis would be more
appropriate, but not for existing users
Could the proposal suggest a patient contribution to hearing aids, repairs or
batteries?
Current provision of hearing aids needs assessment – concerns regarding quality
and consistency of care across hearing aid providers
Feedback objecting to the proposal:
Increase the stigma of hearing loss
Not supporting mild hearing loss can lead to further / more rapid deterioration of
hearing, or require patients to live with their condition as it gets rapidly worse
Significant amount of national research into the benefits of people with ‘Mild’ hearing
loss receiving hearing aids
Hearing loss is relative to the individual, so defining a policy around a decibel level /
hearing banding could be a hindrance
Impact on social isolation / mental health / cognitive decline of the individuals
affected
Potentially undermine quality audiology services within the pathway, as routine
hearing aid services financially support paediatric Audiology, vestibular, complex
hearing and tinnitus services.
More investment would be needed in voluntary / charity support services for people
affected
Purchasing / maintaining hearing aids outside of the NHS is too expensive for many
aged over 50 years
Health and safety concerns – people without hearing aids driving or working in
potentially dangerous jobs?
Possible negative impact on 18 year olds entering Further / Higher Education or
employment
Short term saving, long term socio-economic loss
Impact on social life / employment / volunteering
The wider impact on health and social care – e.g. Mental Health, Speech and
Language
Too difficult to implement and police new policy proposal without eliminating any
proposed savings
Hearing loss is a disability and requires the appropriate support
Patient Exceptions
General feedback
Each patient needs to be assessed on a case-by-case basis

The proposed exception criteria is acceptable without changes required
The listed patient exceptions are fair, but further information is required in each case
Difficult to implement, with possible inconsistent application across the area by
clinicians
Would require more resource to ‘police’ the application of the proposed policy
Additional patient exceptions to consider:
People with tinnitus
People on low incomes
Retired people
School age young people / 18-year-olds entering FE / HE / employment
Carers
Healthcare workers
Anyone with another sensory impairment
Ex-armed forces / military
People with mental health problems
Patients with vestibular / balance problems
Status of Hearing Aid Services with CCG’s priorities
General Feedback
Hearing services low on the CCG’s priorities, but should be of high priority because
of the impact on patient’s health and wellbeing
Patients should be asked to make a contribution to hearing aids – e.g. payment for
batteries
The proposed policy will create additional pressure on front line services
Greater awareness of hearing conditions needed
The CCG needs to focus on the behaviour of AQP providers in selling hearing aids
Hearing is fundamental to people’s wellbeing and social inclusion
One in six people have hearing loss; this will increase over the next 20 years
Hearing aids are of little use to people with tinnitus, so many patients with that
condition do not use their hearing aids
"The World Health Organisation predicts that by 2030 adult onset hearing loss will be
a long-term condition ranking in the top ten disease burdens in the UK, on a par or
perhaps exceeding those of diabetes and cataracts.”
The NHS should improve the quality of hearing aids provided so that less repairs /
replacements are needed
Proposed policy would offer relatively small saving in comparison to the CCG’s deficit
Experience of Hearing Services locally
Positive experiences
NNUH has quality services, the best range of equipment and well trained staff
QEH services are very good
Addenbrooke’s provide a comprehensive service
Various independent providers – a good service
Negative experiences
AQP has resulted in a loss of staff from acute audiology departments
Independent providers offer a better service that hospitals
How are patients made aware of the choice of providers? How much information do
they have on the audiology pathway?
Do independent providers have specialist knowledge that is available at acute
providers?
Correspondence / Feedback from providers, charities and the voluntary sector
The CCG has been in written correspondence with a number of stakeholders, providing
insight from the provider, voluntary and charity sectors. The CCG has also received written
correspondence from its Member Practices in response to the consultation. These reports
will be submitted to the CCG’s Governing Body in full.
The list of responders within this category are listed as follows:
Action on Hearing Loss
The National Community Hearing Association
Norfolk and Norwich University Hospital NHS Foundation Trust
British Academy of Audiology
The National Deaf Children’s Society
Cambridgeshire Hearing Help CIO
Norfolk Deaf Association
Norfolk and Norwich Children’s Hearing Services Working Group
James Paget University Hospitals Children`s Hearing Services Working Group
British Society of Audiology
Sense
British Tinnitus Association
Independent audiology providers

Subject:
Delivering the forward view – NHS Planning Guidance 2016/17-2020/21
Presented by:
Jocelyn Pike
Prepared by:
Jocelyn Pike
Submitted to:
Governing Body – Part I
Date: 19th January 2015
Purpose of paper:
To summarise the :
Key points from the 2016/17 Planning Guidance;
The timelines for completion.
Recommendation to Governing Body:
1. The GB is asked to note the enclosed content and timelines.
Agenda item: 7.1

Key Risks
Clinical:
Implementing the requirements of the 16/17 Planning Guidance is key to ensuring services are safe and sustainable for patients.
Finance and Performance:
Implementing the requirements of the 16/17 Planning Guidance is key to delivering value for money and ensuring performance is in line with NHS constitutional standards.
Impact Assessment (environmental and equalities):
NA
Reputation: The reputation of the CCG is measured, in part, by its ability to translate national policy into local delivery.
Legal: NA
Resource Required:
It is proposed a dedicated resource be identified across the central system Norfolk, to lead on the development of the Sustainability and Transformation Plan. This is being proposed in Part II GB.
Reference document(s):
Documents referred to in report
NHS Constitution:
Implementing the requirements of the 16/17 Planning Guidance is key to ensuring performance is in line with NHS constitutional standards.
Conflicts of Interest:
None identified at this stage. However in developing the required plans a conflict may emerge with primary care and the elected GB leads. This will be identified and addressed whence it arises.
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
SNCCG Governing Body meeting 26th January 2016.

Delivering the Forward View: NHS Planning Guidance 2016/17-2020/21
NHSE 22/12/15
Planning Process within Local Health Systems
The NHS are asked to spend the next six months delivering core access, quality and financial standards while planning properly for the next 5 years.
System leadership is needed to produce a Sustainability and Transformation Plan (STP) which involves:
Local leaders coming together as a team
Developing a shared vision with the local community which involves local government
Programming a coherent set of activities to make it happen
Execution against plan
Learning and adapting
Where collaborative and capable leadership can’t be found NHSE and NHS improvement will help secure remedies.
All NHS organisations are required to produce two separate but interconnected plans;
1. A local health and care system ‘Sustainability and Transformation Plan’ (STP) which will cover the period October 2016 to March 2021
STP footprints to be submitted on 29th January 2016
Full STP submission by end of June 2016 and will be formally assessed in July 2016
STPs must cover all areas of CCG and NHSE commissioned activity inc specialist and primary care, prevention, social care (reflecting agreed health and wellbeing strategies).
STPs will be the single application and approval process for access to transformational funding from 17/18 onwards (for initiatives such as new care models, PC access and infrastructure, technology roll out and to drive clinical priorities).
The most compelling and credible STPs will secure funding from April 2017 onwards so the quality of STPs is critical to determining how quickly local areas are able to access the national sustainability and transformation fund which is worth £2.1bn in 2016/17
STPs should be structured around the list of national challenges set out in Annex 1 of the guidance (these are a guide and the most important task is to create a clear and overall vision for your area)
STPs will be an umbrella plan, covering a number of strategic delivery plans which may cover different geographic footprints (eg for emergency are, a local focus on enhanced primary care and major trauma centres covering wider areas)
New models of care to feature prominently in STP, NHS interested in piloting secondary MH providers managing care budgets and reinvention of the acute medical model in small DGHs
There will be further guidance on STPs which will set out the timetable and early phasing of national products and engagement activities.
2. An Operational Plan for 2016/17 (OP) - This will need to reflect the emerging Sustainability and Transformation Plan
1st submission on 8th February 2016
Final submission on 11th April 2016
OPs to be agreed by NHSE by April 2016 and include commissioner and provider plans, based on contracts signed by March 2016.
Detailed requirements for OPs will be set out in the technical guidance, issued January 2016

OPs should be regarded as year 1 of the 5 year STP (and demonstrate significant progress on transformation)
All plans need to demonstrate;
How they intent to reconcile finance and activity
Planned contributions to efficiency savings
Plans to deliver the key must dos
How quality and safety will be maintained and improved
How risks will be jointly identified and mitigated
How Ops link to and support STPs
Trust plans need to focus on;
Cost reduction not income growth
Consistency between financial plans and workforce plans
Effective use of e-rostering
Tightly controlled procurement
Access to future transformation funding
£2.1bn in 2016/17 of which £1.8bn will replace DoH Funding and be distributed on a Trust by Trust basis by the NHS Improvement and agreed with NHSE.
STPs are the single application and approval process for being accepted onto transformation programmes and funding which will be available from April 2017.
Only the most compelling and credible STPs will secure funding.
Plans need to be good quality, ambitious, clear and powerful vision and coherence and demonstrate track record of progress.
Funding directed to initiatives such as the spread of new care models through and beyond vanguards, primary care access and infrastructure, technological roll-out and to drive clinical priorities.
Allocations, Finance and Tariff
For 16/17, CCG allocations will rise by an average of 3.4% and there is a commitment that no CCG will be more than 5% below its target funding level. Overall, primary medical spend will rise by 4% to 5% each year and specialised services will rise by 7% in 16/17, with a growth of at least 4.5% in subsequent years
NHSE has set firm three year allocations for CCGs followed by two indicative years.
To provide CCGs with a total place-based understanding of commissioning spend, NHSE will also publish allocations for primary care and specialised commissioned services.
Local health systems will need to develop a financial sustainability plan as part of the STP
NHSE is developing a single purchasing and supply chain arrangement for specialist commissioning high cost tariff excluded devices from April 2016 (NHSE will launch a consultation on the standard contract in January)

Commissioners will be required to deliver a reserve of 1%, plus an additional 0.5% contingency. Commissioners are required to spend 1% of their allocation non recurrently and this should be uncommitted at the start of the year and CCGs should plan to drawdown all cumulative surpluses in excess of 1% over the next 3 years.
On the tariff;
Include a 2% efficiency deflator and 3.1% inflation uplift
Remain on HRG4 for 16/17 with no change to specialist top ups
The specialised risk share will be suspended for 16/17
Returning the NHS provider sector to balance
During 2016/17 the NHS Trust and Foundation Trust Sector will, in aggregate, be required to return to financial balance.
£1.8b of income from sustainability and Transformation Fund will be calculated and distributed to Trusts by the NHS Improvement and agreed with NHSE
Greater alignment between commissioner and provider finances will be developed
Providers eligible for sustainability and transformation funding in 2016/16 will not face ‘double jeopardy’ scenario of incurring penalties and losing access to funding. A single penalty will be imposed.
Sustainability Funds will be released to Trusts Quarterly and on the delivery of achieving recovery milestones, deficit reduction, access standards and progress on transformation. Where trusts default on the conditions access to the fund will be denied and sanctions applied.
Forensic examination of deficit reduction of providers. Trusts to focus on cost reduction not income growth.
Greater consistency between trusts financial and workforce plans will be required in 2016/17 including evidence of e-rostering of nurses, midwives, HCAs and clinicians.
More focus on procurement - Providers expected to report and share data on their top 100 most common non-pay items and be required to only pay the best price available.
Capital investments proposed will be consistent with their clinical strategy, limited levels of finance available and the repayment of existing and new borrowing related to capital investment need to be funded from within the trusts own capital resource.
National ‘must dos’ for 2016/17
The Nine ‘must dos’ for 2016/17 for every local system are:
1) Develop a high quality and agreed STP
2) Return the system to aggregate financial balance
3) Develop and implement plans to address the sustainability and quality of primary care
4) Get back on track for access standards for A&E and ambulance waits
5) Improve and maintain the 18 weeks RTT standard

6) Deliver 62 day cancer wait standard (and progress 1 year survival rates)
7) Achieve and maintain the 2 new MH access standards and continue to meet dementia diagnosis standard)
8) Deliver action plans to transform care for people with learning disabilities
9) Develop and implement affordable plans to make improvements in quality
By March 2017, 25% of the local population will have access to acute hospital services that comply with four priority clinical standards on every day of the week. All areas will need to set out their ambitions for a 7 day service as part of their STP.
By March 2017, 20 percent of the population will have enhanced access to primary care.
There are three distinct challenges under the banner of seven day services:
Reducing excess deaths by increasing the level of consultant and diagnostic services available in hospitals at weekends. (must be offering 4 of the 10 standards in 2016/17, 5 of 10 in 2018 and complete coverage by 2020) Improving access ot out of hours care by achieving better integration and redesign of 111, minor injuries units, urgent care centres and GP Out of hours services. Improving Access to primary care at weekends and evenings where patients need it.
CCGs and councils will need to agree a joint plan to deliver Better Care Fund (BCF) in 2016/17, building on the 15/16 plans.
Commissioners must continue to increase investment in MH each year (to at least match their overall expenditure increase)
There will be a new CCG assessment framework to measure progress (‘Ofsted’ style), to be consulted on in January 2016.
Page 1 of 8
Subject:
Commissioning and performance update
Presented by:
Jocelyn Pike, Chief Operating Officer
Submitted to:
SNCCG Governing Body
Date:
26th January 2016
Purpose of paper:
To inform the Governing Body on: 1. Performance across the range of health services commissioned; and 2. Key commissioning decisions for information and discussion.
Recommendation to Governing Body:
The Governing Body is asked to note the enclosed update.
Key Risks
Clinical:
Contained within the report or specifically identified in the separate quality report.
Finance and Performance:
Performance risks identified within the report, no specific financial risks reported.
Impact Assessment (environmental and equalities):
N/A
Reputation: The CCG is required to deliver its Constitutional standards.
Legal: None
Resource Required:
N/A
Reference document(s):
Referenced in the report.
Agenda Item 7.2

Page 2 of 8
Performance Month 8 See enclosed Performance Tracker Month 8 – Excel sheet
NHS Constitution
Action
Norfolk and Norwich University Hospital Foundation Trust
A&E Summary of Contract performance notice 13.01.16
RAP submitted to the CCGs and Monitor on 28th April 2015 predicting compliance with the Operating Standard would be achieved by week ending 4th October 2015.
The Co-ordinating Commissioner considered that the Provider was in breach of the RAP as the validated performance as at 4th October 2015 was 90.7% against the 95% Operating Standard and therefore the agreed milestone for recovery was not achieved.
As the breach was not remedied within 5 Operational days from its occurrence, the Co-ordinating Commissioner issued an Exception Report on 15th October 2015 and under General Condition 9.21 of the 2015/2016 NHS Standard Contract, the Co-ordinating Commissioner instructed Commissioners party to the Contract to withhold 2% of the Actual Monthly Value for September and to continue to withhold 2% for each month the Provider’s breach continued.
On the 12th November 2015 the Co-ordinating Commissioner issued another Exception Report as performance had still not been rectified for the month of October and the Co-ordinating Commissioner instructed Commissioners party to the Contract to withhold a further 2% of the Actual Monthly Value in accordance with General Condition 9.21 for the month of October.
Within the Exception Report the Co-ordinating Commissioner advised the Trust that as the breach had not been rectified with 20 Operational Days of the Exception Report issued on 4th October 2015 Commissioners were able to permanently retain the 2% of Actual Monthly Value for September. However, as the Trust had confirmed that a revised plan would be submitted to its Board on 27th November, at this stage Commissioners were minded not to permanently retain monies but still reserved the right to do so pending review of the revised plan.
The Trust’s failure to remedy the breach of the Remedial Action Plan continued in November but as Commissioners and the Trust were actively working to agree a revised Remedial Action Plan to be reviewed during the Central Norfolk Local Escalation meeting with NHS England and Monitor on 2nd December 2015, the Co-ordinating Commissioner chose not to exercise the right to issue another Exception Report at that stage and continued to withhold 2% of the Actual Monthly Value for September 2015 and October 2015.
As an outcome of the Central Norfolk Local Escalation meeting a revised Remedial Action Plan was agreed effective from 1st December 2015 which committed the Trust to achieve performance of 90% for December 2015, 91% for January 2016, 93% by March 2016 and achieving and sustaining performance of 95% for April 2016 onwards.
The Trust failed to meet the agreed trajectory of 90% for December 2015 and as such the Co-ordinating Commissioner considers that the

Page 3 of 8
NHS Constitution
Action
Provider is in breach of the revised Remedial Action Plan as the milestone for recovery was not achieved.
As the breach has not been remedied within 5 Operational days from its occurrence, the Exception Report is being issued such that, under General Condition 9.21 of the 2015/2016 NHS Standard Contract, the Co-ordinating Commissioner is instructing Commissioners party to the Contract to withhold 2% of the Actual Monthly Value. In lieu of the Actual Monthly Value being available for December, 2% of the planned contract value will be withheld from the next monthly payment.
Due to the Trust’s failure to achieve the milestones within the agreed A&E Remedial Action Plan the Co-ordinating Commissioner will now exercise its right under GC9.22 to instruct all Commissioners party to the Contract to permanently retain 2% of the Actual Monthly Value for September 2015 and October 2015. If, 20 Operational Days after issue of the Exception Report under GC9.20, the Provider remains in breach of the Remedial Action Plan, the Co-ordinating Commissioner may notify the Provider that any further sums withheld under GC9.19 or GC9.21.1 are also to be retained permanently.
Ambulance handover
Update from SPRG 13.01.16: Healthwatch audit and review of arrival to handover issues has been completed, the report will be published to CCG’s wk 18.01.16. Verbal update was that the pathway is a 19 step process. It would appear that this is sound apart from step 18 in which exclusions from data submissions have been applied leading to the large discrepancy between EEAST and NNUHFT reported data sets. The SNCCG contract mandate specifically addresses this issue for 2016.17.
Ambulance Further work continues on the RAP, NHSE requested that commissioners reinvest the contract fines for 2015/16 back with EEAST to buy more PAS to increase red performance towards national average in the coming months. The continued work on the RAP is due to be reviewed at a subsequent meeting following AO Board on 5th Feb (EEAST have been told to ensure that they can assure commissioners of meeting and maintaining 70%+ Red performance on R2. It is also assumed that R1,R19 and Red Tail Breaches will also improve as a result of increasing PAS capacity. If RAP cannot be agreed on 5/2/16 this will need further escalation. NHSE and TDA will be conducting a review of EEAST Reference Costs as agreed at the escalation meeting and this will be ready for Locality AO Consideration in early Feb.
RTT No contract performance notices have been issued to the Trust since 12.11.15. Update from meeting between NNCCG, NNUHFT, Monitor and NHSE 02.12.15: there needs to be a substantial and sustainable investment in the Trust’s elective capacity in order to reduce long term reliance on a range of ad hoc but longstanding arrangements involving high levels of overtime, locum staffing and other temporary measures. The Trust’s recovery plan looks to a major recruitment drive of around 100 WTE, including 17 WTE Consultants. The Trust has an action plan in place to reduce the backlog of patients and move towards compliance against the incomplete standard. This includes:
Operation of a new temporary “Vanguard” Theatre
Increasing the utilisation and efficiency of the current Day procedure Unit
Maximising the opportunity to outsource work to other providers
Commissioning a comprehensive Validation exercise by external consultants

Page 4 of 8
NHS Constitution
Action
The original recovery trajectory against the Incomplete Standard at aggregate level stretched to August 2016. For this reason Commissioners rejected the RAP and agreed with the Trust to continue to explore further options to foreshorten recovery. These include:
Further work with the national PMO to source alternative capacity which is accessible for Norfolk patients. Some capacity has been identified at the Fitzwilliam Hospital,
Colchester with whom we need to confirm the exact detail of specialty availability. We are working closely with Kelvyn Price of the national PMO on this.
The Trust are exploring a contract with Medinet to bring more capacity onsite to the NNUH
The Trust will, subject to successful recruitment by Vanguard, bring the Vanguard Theatre into use at weekends
At the Escalation meeting, the issue of a second Vanguard theatre was raised. The Trust have explored this and will not be pursuing this as the lead time for mobilisation and the need to recruit Surgeons would not be effective in bringing forward the recovery date. However, the Trust will deploy a mobile Catheter Lab onsite so as to increase capacity for interventional radiology within the overall interventional-suite footprint.
The Trust is working with NCHC to access additional day theatre capacity at the Norwich Community Hospital site.
Whilst the exact benefit and timescale of all of these initiatives will be known by 29 January 2016, it is expected that the impact will improve delivery of the Incomplete Standard at aggregate level stretched by one month i.e. July 2016. The Trust is further committed to refreshing the recovery trajectory at the end of January and will update both NHSE and Monitor on progress.
NB It is has been reported (07.01.16) that there is an SNCCG Pt who has breached 52 weeks in vascular surgery with a reason of ‘Diagnostic Delay (in reporting results)’. The PT has a TCI of 15.01.16.
Cancer Extracted from contract performance notice issued 29.12.15
The Trust submitted RAP for Cancer 62 days in October 2015 which was accepted by the Commissioner. The Provider has failed to achieve against the trajectory of 77% for November 2015. The Provider achieved 72.2%. The Commissioner has also noted that the Trust anticipates their performance for December being below the trajectory of 85%. As the breach has not been remedied within 5 Operational days from its occurrence, an Exception Report was issued, 29.12.15, stating that under General Condition 9.21 and in lieu of the Actual Monthly Value being available for November, 2% of the planned contract value will be withheld from the next monthly payment. The Commissioners will continue to withhold 2% for each month the Provider’s breach continues or the required improvement has not been achieved and maintained, subject to a maximum monthly withholding of 10% of the Actual Monthly Value.
Diagnostics No new contractual information, however RAP delivery is being monitored via SPRG.
Cancellations NNUHFT remain outliers Nationally for this measure, however formal contract queries have not been raised in recognition of the impact that the Cancer and RTT RAPs have on this standard. The standard continues to be monitored via SPRG.

Page 5 of 8
NHS Constitution
Action
West Suffolk Hospital Foundation Trust
Ambulance Ambulance Handover delays of over 30 minutes
A RAP is in place for this. A meeting was held on 30 November to decide outstanding areas of agreement (data validation, Geofield, clock start definition). At the contract / SLA meeting which took place on 25 November, commissioners advised that the clock starts at the door of the hospital and that other Trusts had agreed a reasonable time addition. This will be discussed further at the next Contract / SLA meeting scheduled for 27 January.
Ambulance Handover delays of over 60 minutes
As above.
RTT Completed Pathways Admitted Patients
Overall achievement fell to 84%, 7 Specialties were below 90% this month: General Surgery (152/180 pts), Urology (106/128 pts), T&O(210/255), ENT(92/117 pts), Ophthalmology(203/229 pts), Oral (83/139 pts) and Gynaecology (143/172 pts)
Completed Pathways Non-Admitted Patients
7 specialties were below 95% - Gen Surgery (462/487 pts), Urology (129/136), Plastic Surgery (54/60 pts), Cardio (126/135 pts), Dermatology (357/377 pts), Geriatric(33/35 Pts) and Gynaecology (310/329 pts). Overall performance was above target at 96.5%.
Incomplete Pathways (waiting list)
Overall Performance on the Incomplete pathway is 96.5% and all specialties performed above the 92% target.
The Trust advises that the incompletes should remain resilient throughout winter however there are some concerns noted regarding impact of strike action. The Coordinating Commissioner has advised that plans are in place to highlight to the CCG early if there are any issues.
Mental Health Action
Inpatients DTOCs
There are still significant Lorenzo data issues relating to the reporting of DTOCs. NSFT are reporting around 5% on their Board report and this is also considered to be an estimate. Although NSFT are performing below target the level of DTOCs are causing considerable constraint on patient flow and contributing to patients continuing to be placed Out Of Trust. A separate situation report has been submitted to NHSE and will be presented to the new MH SRG at the end of Jan 16. District Councils have agreed to attend this forum in future to address the need for strategic dialogue with Housing.

Page 6 of 8
Mental Health Action
Out of Trust placements
Out Of Trust placements continue to be variable with volumes affected by capacity constraints. The closure of beds in Lowestoft, with a delay on upgraded facilities in Gt Yarmouth and Waveney continues to exert pressure on the Central Norfolk system. In addition DTOCs including patients with no fixed abode are constraining flow. As stated above a sitrep has been produced for NHSE and will be escalated to the new MH SRG at the end of Jan 16. As at 18/1/16 there were 5 out of trust placements all Older People.
CRHT admissions to adult acute
67.4% (95% standard) for Month 8. Data issues have been ruled out and this appears to be a quality performance issue to be escalated with NSFT. PISG meeting w/c 25/2 will determine contractual sanction
% long term patients in receipt of annual health check
72.7% (100% standard) for Month 8. Work continues to resolve issues relating to the Lorenzo system and the capturing and extraction of this information
Contacts CAMHS 8 wk RTT
75% (80% standard) for Month 8. Continued data errors due to incorrect category used when inputting information into Lorenzo
2 face to face contacts with valid assessment and care plan
90.9% (99% standard) for Month 8. The reliability of this data is still questionable due to user interface issues with the accurate capture of this data
AAT 72 hr standard
92% (99% standard) for Month 8. Manual reporting is still required as continued inconsistencies with Lorenzo produced data
AAT 28 day standard
Continued progression of CQN. Revised RAP for continued failure to deliver received 23/12/15 and being evaluated by the CCG.
Community Action
CNT Patients Advanced Care Planning: Data validation has corrected this figure to 91.7%, now meeting target. Died in Preferred Place of Care Quarterly audit; target not due until December.

Page 7 of 8
Community Action
Intermediate Care Beds
Average LOS Units in SNCCG area are currently operating within this target; the target is pan-Norfolk and has been subject to a CPN, which was closed as the relevant commissioners accepted the justification given by the provider as a result of the joint investigation around increased acuity of patients cared for in the units.
LAC Ofsted report published Oct 15 rated services for LAC as Inadequate, citing LAC health assessments as of particular concern There are a series of short term and long term plans to address the concerns raised by Ofsted A remodelling of the service is being undertaken with the provider, NCC Designated Doctor and CSU. Much of this work is dependent on NCC’s business process re-engineering exercise, the date of which has been delayed to January 2016 due to staff sickness. Contractual discussions between CCGs and NCH&C about the service specification, KPIs and funding for 15/16. CQN to be issued if short term actions do not address some of the concerns.
An increase in the capacity of core targeted and specialist CAMHS to manage the mental health needs of children and young people on
the edge of care and those who are looked after or adopted was included in the Transformation plan.
Pledge 2 Services Breaching 18 Week: 1 service, DASH outpatients. Contract Query Notice has been served; trajectory provided to CCG with
return to compliance of 18 weeks of 20th March 2016; lost capacity attributable to long-term sickness and change of role for two of the
consultants, which is being addressed by provider as part of the contract notice; the service is being reviewed for 2016/17.
111/OOH Action
111 Performance was difficult over Christmas (especially on the days following the bank holidays)
2 contract performance notices have been issued to IC24- 1 for OOH and 1 for 111
CPN meeting on 12.01.16 and remedial action plan is being prepared by IC24 and will come to commissioners within contract timescales
Lot of interest and concern from NHSE East of England. Meeting took place yesterday between Norwich CCG, IC24, and NHSE. Their
concerns focused on the number of areas of performance that need addressing and that IC24 are an experienced provide. Assurance
needed for NHSE that things in hand to recover performance by end of Feb and assurance that service can be delivered at Easter
OOH

Page 8 of 8
Commissioning update – for items not covered elsewhere on the agenda Vasectomies SNCCG currently commission non-complex Vasectomy services from Breckland Vasectomy Service, Norfolk Surgical Diagnostic Centre (NSDC) and Oak Street Vasectomy Services. The total spend for 14/15 for these providers was £54,985 and the full year estimated figure for 15/16 is £64,170. The local tariff for non-complex vasectomies is currently set at £250 per procedure with the national tariff for 16/17 expected to be in the region of £631 per procedure. Our acute providers provide complex vasectomy procedures at national tariff. A decision needs to be taken as to whether or not to put Vasectomies through the clinical thresholds policy. Other CCGs have taken the decision not to routinely fund vasectomies and the CCG is currently reviewing its position. Depending on the outcome of the decision to routinely fund, a further decision needs to be taken as to whether to offer contracts to the independent providers listed to commence 1st April 2016. Central MIND BME The current funding for the Central MIND BME service is due to end March 2016. The service was commissioned by Norfolk PCT originally to:
Support BME communities through effective Networks
Better support early intervention and access to primary and secondary care services; and
Facilitate primary and secondary care providers in provision of services to BME communities. A review of all third sector contracts funded by SNCCG suggests a lack of clarity around the impact the service has. Whilst the provider has been reporting on the service they have not been able to demonstrate achievement against the outcomes as listed, or that the service is providing value for money. Finally it is also evident that the service overlaps with existing delivery by the new Primary Care Mental Health Service link workers in the community. Given the outcome of the review as stated, the CCG has taken the decision it will no longer fund the service post March 2016.

Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15
NNUHFT 95% 90.1% 93.7% 90.3% 90.0% 90.5% 88.4% 87.0% 81.0% 81.0% 87.0%
WSHFT 95% 92.9% 95.6% 96.2% 95.7% 94.3% 96.3% 96.5% 96.5% 96.3%
NNUHFT 0 0 0 0 0 0 0 0 0 0
WSHFT 0 0 0 0 0 0 0 0 0 0
NNUHFT 0 63 157 154 192 155 186 196 196 186
WSHFT 0 57 99 115 147 160 127 145 145 127
NNUHFT 0 1 22 40 65 15 39 42 42 39
WSHFT 0 0 6 2 0 9 9 12 12 9
Cat A (Red 1) incidents response ≤ 8 minutes % EEAST 75% 79.9% 80.7% 75.5% 74.7% 73.5% 70.9% 73.5% 73.5% 70.9%
Cat A (Red 2) incidents response ≤ 8 minutes % EEAST 75% 71.5% 69.6% 66.1% 62.5% 61.8% 58.7% 60.2% 60.2% 58.7%
Cat A19 incidents response ≤ 19 minutes % EEAST 95% 95.5% 94.8% 92.6% 90.8% 90.6% 88.9% 90.0% 90.0% 88.9%
NNUHFT 90% 75.9% 75.9% 76.0% 75.7% 77.0% 75.2% 72.2% 72.2% 75.2%
WSHFT 90% 84.1% 89.9% 90.0% 89.0% 88.4% 87.7% 83.8% 83.8% 87.7%
NNUHFT 92% 89.4% 89.5% 89.1% 88.9% 88.2% 87.2% 86.6% 86.6% 87.2%
WSHFT 92% 96.1% 96.8% 97.1% 96.6% 97.1% 96.9% 96.7% 96.7% 96.9%
NNUHFT 95% 94.0% 95.0% 94.0% 93.3% 92.5% 90.9% 90.1% 90.1% 90.9%
WSHFT 95% 96.3% 96.0% 96.4% 96.4% 95.8% 55.9% 96.5% 96.5% 55.9%
NNUHFT 0 1 0 0 0 2 0 1 1 0
WSHFT 0 0 0 0 0 0 0 0 0 0
NNUHFT 0 0 0 0 1 0 0 1 1 0
WSHFT 0 0 0 0 0 0 0 0 0 0
NNUHFT 0 0 1 0 1 0 0 0 0 0
WSHFT 0 0 4 2 0 0 1 2 2 1
NNUHFT 96% 97.2% 98.1% 96.9% 96.8% 95.4% 97.4% 97.8% 97.8% 97.4%
WSHFT 96% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
NNUHFT 98% 100.0% 98.3% 99.1% 100.0% 99.1% 98.2% 99.1% 99.1% 98.2%
WSHFT 98% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
NNUHFT 94% 97.6% 98.3% 100.0% 98.0% 97.5% 95.8% 95.4% 95.4% 95.8%
WSHFT 94% 100.0% 100.0% 100.0% 100.0%
NNUHFT 94% 91.4% 87.3% 88.8% 83.7% 93.0% 94.0% 93.5% 93.5% 94.0%
WSHFT 94% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
NNUHFT 63.0% 65.0% 80.0% 28.6% 38.9% 27.3% 64.0% 64.0% 27.3%
WSHFT 100.0% 0.0% 0.0% 0.0% 0.0% 84.0% 71.4% 71.4% 84.0%
NNUHFT 90% 88.9% 100.0% 92.9% 84.4% 100.0% 86.3% 100.0% 100.0% 86.3%
WSHFT 90% 0.0% 0.0% 0.0% 0.0% 100.0% 96.9% 100.0% 100.0% 96.9%
NNUHFT 85% 77.2% 75.9% 75.9% 73.3% 81.9% 75.9% 77.9% 77.9% 75.9%
WSHFT 85% 87.9% 85.5% 96.4% 87.5% 88.1% 89.1% 89.1% 89.1% 89.1%
NNUHFT 93% 97.1% 99.1% 97.9% 99.6% 99.6% 99.0% 97.0% 97.0% 99.0%
WSHFT 93% 100.0% 99.0% 98.2% 99.2% 100.0% 96.9% 94.9% 94.9% 96.9%
NNUHFT 93% 88.0% 94.6% 98.8% 98.2% 96.3% 94.4% 98.3% 98.3% 94.4%
WSHFT 93% 95.4% 99.0% 99.6% 99.0% 98.4% 98.0% 98.1% 98.1% 98.0%
NNUHFT 1% 2.1% 2.0% 2.4% 3.2% 3.7% 4.5% 5.8% 5.8% 4.5%
WSHFT 1% 12.4% 13.1% 11.6% 4.9% 1.8% 0.1% 1.4% 1.4% 0.1%
NNUHFT 0 75 90
WSHFT 0 8 2
NNUHFT 0 0 0 0 0 0 0 0 0 0
WSHFT 0 0 0 0 0 0 0 0 0 0
NNUHFT 0 0 0 0 0 0 0 0 0 0
WSHFT 0 0 0 0 0 0 2 0 0 2
Mental Health CPA patients followed-up ≤ 7 days % SNCCG 95% 86.0% 82.0% 83.0% 79.0% 75.0% 78.0% 94.0% 87.0% 87.0% 94.0%
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15
NNUHFT 5 5 1 6 6 2 5 5 5 5
WSHFT 5 2 2 1 4 0 0 3 3 0
NNUHFT 0 0 0 0 0 0 0 0 0 0
WSHFT 0 0 0 0 0 0 0 0 0 0
NNUHFT 5 4 3 7 3 7 10 2 4 4 4
WSHFT 0 #N/A #N/A 0 0
NNUHFT 0 0 0 1 0 0 0 1 0 0 0
WSHFT 0 #N/A #N/A 0 0
NNUHFT #DIV/0! 2 0 2 1 3 0 3 0 0
WSHFT #DIV/0! 1 2 3 2 1 0 0 0 0
SIs Serious Incidents (SIs) reported in the period NNUHFT 9 10 7 15 9 15 17 11 12 12 11
Never Events Never Events reported in the period NNUHFT 0 0 0 0 1 0 0 0 1 1 0
Stroke patients ≥ 90% of time on stroke unit % NNUHFT 80% 79.1% 69.9% 75.9% 75.5% 86.3% 87.1% 87.1% 86.3%
Patients suspected TIA assessed/treated ≤ 24 % NNUHFT60% 100.0% 100.0% 100.0% 100.0% 100.0% 93.3% 93.3% 100.0%
Complete treatment moving to recovery % SNCCG 50% 47.9% 56.9% 48.0% 51.4% 55.3% 41.0% 56.0% 48.0% 48.0% 56.0%
Number who receive psychological therapies SNCCG 1% 1.0% 1.0% 1.0%
Dementia Diagnosis Rate SNCCG 67% 54.5% 55.0% 55.2% 55.8% 0.0% 0.0%
NNUHFT 73 89 78 93 94.79 89.62 89.62 94.79
WSHFT 78 92 92 94 93 91.14 91.14 93
NNUHFT 91 95 78 96 96 96.49 96.49 96
WSHFT 92 98 92 99 100 99.11 99.11 100
Mental Health
Friends and Family
Inpatients friends and family test score
A&E friends and family test score
Most Recent
Period
Pressure Ulcers
Grade 3 pressure ulcers reported
Grade 4 pressure ulcers reported
Complaints Complaints reported in period
Performance vs. Target
Stroke
Previous
PeriodMovement
Previous
Period
Month
Movement
Most Recent
Period
Infection
Clostridium difficile infections
MRSA bacteremias
Quality & Other
MeasuresPerformance Measure
Performance vs. Target
Urgent operations cancelled for a second time
CCG /
Provider
Current
Target
CCG /
Provider
Current
Target
NHS Constitution
Rights & PledgesPerformance Measure
Ambulance Handover
Ambulance handover delays of over 30 minutes
Ambulance handover delays of over 1 hour
A&E
A&E attendances ≤ 4 hours %
A&E 12 hours waits
Ambulance
RTT
Referral to treatment (admitted adj.) ≤ 18w %
Referral to treatment (incomplete) ≤ 18w %
Referral to treatment (non-admitted) ≤ 18w %
Admitted pathways (unadjusted) > 52 weeks
Incomplete pathways > 52 weeks
Non-admitted pathways > 52 weeks
Cancer
Diagnostics Diagnostic tests > 6 weeks %
MSA Mixed sex accommodation breaches
Cancer treatment consultant upgrade ≤ 62 days %
Cancer treatment screening service ≤ 62 days %
Cancer treatment urgent GP referral ≤ 62 days %
GP breast cancer referrals ≤ 2 weeks %
GP cancer referrals ≤ 2 weeks %
Cancer first treatment ≤ 31 days %
Cancer sub. treatment DRUGS ≤ 31 days %
Cancer sub. treatment RADIO. ≤ 31 days %
Cancer sub. treatment SURGERY ≤ 31 days %
Cancellations
Cancelled operations treated ≤ 28 days %

5 31 32 33 34 35 36 37 38 32
% of patients whose transfer of care was delayed 7.5% 4.8% 1.0% 0.0% 0.0% 1.0% 1.0% 1.1% 1.0%
Out of Area Placements 22 16 12 10 12 12 4 10
Acute Inpatient - Average length of stay 42.3 53.1 31.5 34.3 58.7 88.7 22.1 27.1
Average delay in days beyond 'fit for discharge' date 56.9 30.0 0.0 0.0 17.0 25.0 22.8 30.0
% of admissions to adult acute wards gate-kept by CRHT teams 95% 88.0% 44.0% 40.0% 51.9% 57.9% 44.2% 55.6% 67.4%
% of long-term (over 12 months) inpatients that have received
an annual health check100% 100.0% 100.0% 62.5% 60.0% 45.5% 41.7% 30.0% 72.7%
CPA patients followed-up ≤ 7 days % 95% 84.8% 78.8% 74.7% 83.3% 78.6% 78.4% 91.8% 87.1%
% of CAMHS patients being seen within 8 weeks of referral
received date (completed pathways)80% 83.5% 73.0% 83.3% 66.0% 62.9% 44.6% 67.2% 75.0%
% of Patients having at least two face to face attended contacts
with a valid MHCT assessment and a care cluster99% 98.5% 94.7% 92.9% 91.5% 90.4% 90.9% 91.9% 90.9%
% of contacts that have been entered within 72 hours of the
activity taking place99% 94.6% 96.0% 93.0% 92.0%
Access to CN&T - Category A 95% 99.4% 98.7% 97.5% 97.3% 98.3% 97.0% 98.7% 97.5%
Access to CN&T - Category B 85% 96.2% 96.3% 96.6% 96.7% 96.4% 96.4% 99.4% 97.0%
Access to CN&T - Category C 90% 98.0% 99.4% 97.8% 98.4% 98.6%
Fall Screening (High Risk) 100% 99.4% 100.0% 99.8% 99.8% 99.8% 100.0% 99.7% 99.8%
Patients Advanced Care Planning 75% 65.3% 55.7% 84.5% 78.1% 78.7% 84.0% 65.6%
Died in Preferred Place of Care 90%
IDD recorded 90% 95.8% 96.6% 98.6% 96.1% 95.5% 94.2% 95.7% 93.5%
Discharged by IDD 80%
Home Discharge Destination 65%
Readmissions - Intermediate Care 15% 12.6% 14.8% 14.1% 12.0% 12.1% 14.4% 12.1% 10.9%
Readmissions - Acute 15% 20.5% 16.4% 15.0% 19.1% 13.7% 17.4% 23.5% 14.5%
Average LOS 18 20.6 20.6 20.5 19.5 18.9 18.8 18.8 19.3
Delayed Transfers of Care 6%
NCH&C Responsible Delayed Transfers of Care 1% 0.9% 0.6% 0.3% 0.2% 0.4% 0.2% 0.4% 0.1%
Percentage of all patients having first seen appointment in
month where referral is less than 2 weeks prior - Norfolk95% 4.5% 10.3% 17.0% 39.3% 18.7% 49.7% 97.3% 95.0%
Percentage of all patients having first seen appointment in
month where referral is less than 2 weeks prior - SNCCG95% 7.4% 9.8% 19.0% 48.1% 23.0% 48.7% 97.3% 94.8%
Percentage of diagnostic reports received in month where
diagnostic request is less than 3 weeks prior - Norfolk90% 76.0% 93.1% 92.8% 96.3% 96.2% 92.4% 90.9% 93.2%
Percentage of diagnostic reports received in month where
diagnostic request is less than 3 weeks prior - SNCCG90% 68.9% 95.1% 94.6% 94.0% 96.8% 88.6% 92.9% 92.5%
Percentage of first treatment contacts recorded in month where
referral is less than 7 weeks prior - Norfolk90% 62.9% 79.9% 87.3% 89.4% 91.5% 93.5% 94.0% 96.5%
Percentage of first treatment contacts recorded in month where
referral is less than 7 weeks prior - SNCCG90% 65.4% 87.5% 87.5% 89.5% 91.2% 96.0% 95.7% 96.3%
% of Health Care Plans Completed with 4 Weeks - Norfolk 30.8% 35.7% 40.0% 65.0% 70.6% 73.9% 66.7% 60.0%
% of review assessments completed within 4 weeks - Norfolk 88.0% 74.5% 83.0% 85.0% 75.9% 51.2%68.7% 60.7%
Patients Waiting Over 18 weeks: Seen 5% 1.0% 0.2% 2.5% 3.4% 3.6% 3.6% 2.0% 1.5%
Patients Waiting Over 18 weeks: Not Seen 5% 1.6% 1.9% 4.1% 5.6% 4.4% 4.8% 2.5% 1.4%
Services Breaching 18 Week 0 1 2 2 5 3 3 3 1
111 disposal recommend attend A&E % 6.8% 7.3% 8.3% 8.7% 8.6% 7.3% 7.2% 7.0%
111 disposal ambulance dispatches % 10.3% 11.0% 11.6% 11.6% 11.1% 12.2% 12.2% 13.2%
111 triggered ambulances transporting patient % 59.4% 59.4% 63.6% 59.0% 59.2%
111 Warm Transfer to Clinician % 72% 69.8% 71.5% 76.7% 79.9% 73.2% 51.5% 57.8% 52.3%
Patients emergency seen ≤ 1 hour % 95% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
Patients emergency home visit seen ≤ 1 hour % 95% 100.0% 100.0% 100.0% 60.0% 100.0% 100.0% 100.0%
Patients urgent seen ≤ 2 hour % 95% 99.4% 99.4% 99.4% 99.3% 97.5% 76.6% 76.4% 70.1%
Patients urgent home visit seen ≤ 2 hour % 95% 96.9% 97.4% 97.3% 93.0% 93.9% 54.7% 65.3% 63.1%
Urgent calls returned by a clinician ≤ 20 minutes % 95% 96.4% 94.0% 93.0% 95.2% 91.6%
Urgent calls returned by a clinician ≤ 60 minutes % 95% 96.2% 91.1% 92.3% 96.3% 92.8%
Speak to GP within 1 hour 95% 77.4% 62.8% 70.3%
Speak to GP within 2 hours 95% 83.8% 70.6% 79.2%
OrgCode
Sum of OutturnNumeric
Row Labels 201504 201505 201506
111 disposal recommend attend A&E 6.770419777 7.313212 8.30145
111 disposal ambulance dispatches 10.28532105 10.96982 11.6155
111 triggered ambulances transporting patient 59.39269171 59.40356 63.5958
111 warm transfer to clinician 69.80749747 71.53063 76.7007
Patients emergency seen ≤ 1 hour 100 100 100
Patients emergency home visit seen ≤ 1 hour % 100 100 100
Patients clinically assessed as urgent seen ≤ 2 hour % 99.35483871 99.4186 99.3779
Patients urgent home visit seen ≤ 2 hour % 96.92307692 97.4359 97.2789
Urgent calls returned by a clinician ≤ 20 minutes 96.40151515 93.95425 92.9545
Urgent calls returned by a clinician ≤ 60 minutes 96.22389307 91.13757 92.2867
Grand Total 735.1592539 731.1635 742.112
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15
74.3% 77.5%
IC24
No longer collected
No longer collected
No longer collected
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15
Pledge 2
NCH&C
NCH&C
NCH&C
PerformancePerformance Measure Org Plan
Communtiy Nursing
& Therapy
Intermediate Care
BedsNCH&C
Orthopaedic
TriageNCH&C
LAC NCH&CNo
target
Trend
(12 months)
Trend
(12 months)
NSFT Performance Performance Measure Org Plan
111/OOH
PerformancePerformance Measure Org Plan
Contacts
Inpatients NSFT
Trend
(12 months)
OOH IC24
No longer collected
No longer collected
No longer collected
No data available due to NSFT system upgrade
and data quality issues
111 IC24
NSFT
EEAST

Subject:
MAZARS Independent review of deaths of people with a Learning Disability or Mental Health problem in contact with Southern Health NHS Foundation Trust April 2011 to March 015
Presented by:
Alison Leather
Prepared by:
Lisa Read NELCSU/Alison Leather
Submitted to:
Governing Body
Date: 13th January 2016
Purpose of paper:
To provide a summary of the MAZARS Independent review of deaths of people with a Learning Disability or Mental Health problem in contact with Southern Health NHS Foundation Trust April 2011 to March 015 including recommendations for Primary Care and CCG’s.
Executive Summary:
The broad findings of the report were:
There had not been effective focus or leadership from the Board relating to the investigation and analysis of data relating to the deaths of its service users.
Insufficient time and attention had been spent on understanding deaths, using the information available to the Trust. Poor analysis and limited reporting had been a consequence while an opportunity of learning from deaths as distinct from other incidents had been missed.
Management information, investigation and quality assurance had been given insufficient attention and there was no evidence of the Board or its directors enforcing improvement, despite warning signs throughout the last four years.
Board reporting on deaths and mortality was minimal. The Board had not been provided with sufficient reliable information to enable it to secure an accurate picture of the performance of SI reporting relating to deaths.
There had been inconsistent use of indicators at Board level with regular changes of measures of deaths over the period resulting in a lack of long term trend analysis and limited challenge.
Suicide numbers are reported on a rolling basis but unexpected deaths are only reported when they are considered to be SI reportable.
Non-Executive Directors had requested more information and assurance relating to investigations over the period and had been assured as to the quality of investigations. Despite this, investigations were not always undertaken when they should be and many are not robust.
The quality of investigations was poor and did not improve to any significant extent over the period despite reassurance to the Board.
Agenda item: 7.3

The Board had not improved the timeliness of SI reporting.
Information in annual reports and the quality account was misleading in the presentation of unexpected deaths amongst service users by only reporting unexpected deaths when they are SIRIs.
Background Following the death of Connor Sparrowhawk in 2013 a number of reviews took place into the practice at Southern Health NHS Foundation Trust in whose care he died. Southern Health NHS Foundation NHS Trust came into being in April 2011, formed when the specialist (largely mental health and learning disability-focused) Hampshire Partnership NHS Foundation Trust took over NHS primary care services across Hampshire. A further acquisition, of a specialist learning disability trust covering Oxfordshire, Wiltshire and Buckinghamshire (the former Ridgeway Trust) took place in November 2012. The current CEO of Southern Health NHS Foundation Trust, Katrina Percy, started as Chief Executive (designate) for the Hampshire Partnership Trust in May 2007, and remains Chief Executive of Southern Health NHS Foundation Trust. The Mazars report covers a four-year time period, from April 2011 to March. It is a review of all deaths of people in receipt of care from Mental Health and Learning Disability services in the Trust between April 2011 and March 2015. It is not a clinical case review of each service user and does not seek to identify clinically unavoidable deaths. It does seek to establish the extent of unexpected deaths in Mental Health and Learning Disability services provided by the Trust and to identify any themes, patterns or issues that may need further investigation based on a scope provided by NHS England. Scope of the Review The scope was to help secure:
A shared view across all the key players of risks within Southern Health NHS Foundation Trust services, of improvement action required, and plans to deliver change.
Advice to the Clinical Commissioning Groups (CCGs) about Learning Disability
Commissioning, data management and analysis, and adverse events indicators. Key points
No systematic oversight and management of the reporting of deaths
Quality of the investigation reports poor.
30% of all deaths (those reported as expected and unexpected) in Adult Mental Health services were investigated as a CIR ( Critical Incident Report) or SI
(serious incident reported on national Strategic Executive Information System database), less than 1% of deaths in Learning Disability services were investigated as a CIR or SI and 0.3% of all deaths of Older People in Mental Health services were investigated as a SI.
Trust policy not followed in respect of investigation of deaths
The Trust could not demonstrate a comprehensive, systematic approach to learning from deaths as evidenced by action plans, board review and follow up, high quality thematic reviews and resultant service change.
The quality of the SI reporting processes and standard of investigation was inadequate no effective action was taken to improve investigations during the review period.
On average it took nearly 10 months from the opening of an SI to closure
Involvement of families and carers in the investigation process had been minimal
Initial assessments and Investigations did not include other agencies where it would have been appropriate.

The Trust did not use the comprehensive information available to it to effectively understand the mortality and issues relating to its clients.
Commissioners have a role in demanding improved information about the death of clients and using it to seek improvement Summary of the Findings The broad findings of the report were:
There had not been effective focus or leadership from the Board relating to the investigation and analysis of data relating to the deaths of its service users.
Insufficient time and attention had been spent on understanding deaths, using the information available to the Trust. Poor analysis and limited reporting had been a consequence while an opportunity of learning from deaths as distinct from other incidents had been missed.
Management information, investigation and quality assurance had been given insufficient attention and there was no evidence of the Board or its directors enforcing improvement, despite warning signs throughout the last four years.
Board reporting on deaths and mortality was minimal. The Board had not been provided with sufficient reliable information to enable it to secure an accurate picture of the performance of SI reporting relating to deaths.
There had been inconsistent use of indicators at Board level with regular changes of measures of deaths over the period resulting in a lack of long term trend analysis and limited challenge.
Suicide numbers are reported on a rolling basis but unexpected deaths are only reported when they are considered to be SI reportable.
Non-Executive Directors had requested more information and assurance relating to investigations over the period and had been assured as to the quality of investigations. Despite this, investigations were not always undertaken when they should be and many are not robust.
The quality of investigations was poor and did not improve to any significant extent over the period despite reassurance to the Board.
The Board had not improved the timeliness of SI reporting.
Information in annual reports and the quality account was misleading in the presentation of unexpected deaths amongst service users by only reporting unexpected deaths when they are SIRIs.
Recommendations The Mazars report makes 23 recommendations for Southern Health NHS Foundation Trust, nine for commissioners, and seven for national bodies. These can be found on pages 37-44 of the report. There were several entries relating to the role of Primary care in the involvement of systems and processes to provide transparency and assurance to commissioners to learn from unexpected deaths, inform service improvement and commissioning intentions. Commissioners are seen to be essential in creating an environment in which multi-agency working to review pathways can take place in a client group that very often require multi-agency involvement but where there is a lack of multi-agency learning.

The recommendations to the commissioners are as follows: 1. The CCGs should take action to ensure:
Incidents are reported to the Strategic Executive Information System (StEIS) within 2 working days as required
That reports are provided to closure panels within 60 days as required
That the quality of IMAs, Critical Incident Reviews and Serious Incident investigations improves radically
That Serious Incident investigations are completed within an agreed timeframe
That the data provided to them relating to deaths is accurate. 2. All Commissioners of services from the Trust should ensure that all unexpected deaths
of people with a Learning Disability, inpatients on Older Peoples Mental Health wards and in cases of suicides of people in the period between referral and treatment are properly considered before a decision is taken not to report as a Serious Incident or report under CQC Regulation 16.
3. The CCGs, with CQC, should ensure that the Trust reports and investigates all deaths
in detention to ensure that full learning is derived from this group of deaths. 4. The CCGs, with NHS England, should review whether GPs should be involved in initial
management assessments of people with a Learning Disability and the extent to which GPs are sufficiently informed to talk with the Coroner if needed.
5. Commissioners should provide support to the mortality reviews in the Trust including
agreeing appropriate independent representation and if possible co-ordinate between them to identify a GP member.
6. All commissioners should monitor and co-ordinate between them, the progress of the
Trust in its improved use of mortality data and contract negotiations should reflect the changes required from this review.
7. The CCGs should discuss the implications of this review with acute care providers in the
area and agree a protocol for ensuring joint investigation between NHS providers, in particular, for people with a Learning Disability.
8. The CCGs with local authorities should develop a detailed needs assessment of people
with a Mental Health or Learning Disability in their area. 9. Commissioners should use the intelligence provided in this review to secure access to
data on Mental Health and Learning Disability services to:
Develop investigation protocols that look across pathways more systematically including in primary care
Inform service developments
Ensure that general ‘community physical care services’ need to be accessible to all groups of patients

Responses to the report
Recommended action
Request that providers supply commissioners with a response and self-assessment against the findings and recommendations of the report.
Consideration of additional elements to be included in the Quality Information Schedule.
Recommendation to Governing Body:
The Governing Body is asked to note the recommendations and content of the report.
Key Risks
Clinical:
Safeguarding
Finance and Performance:
N/A
Impact Assessment (environmental and equalities):
Reputation: N/A
Legal: Advice sought, regulatory impact
Resource Required:
N/A
Reference document(s):
See above
NHS Constitution:
Highlights an awareness of NHS Constitution
Conflicts of Interest:
N/A
GOVERNANCE
Commissioner Response to report
Commissioningresp
onsetomazarsreport.pdf
Joint response from NHS Improvement, NHS England and the Care Quality Commission
181217_ALB_statem
ent_on_Mazars_v8_FINAL.pdf
Statement delivered by Jeremy Hunt for the Department of Health
http://www.parliament.uk/business/publications/written-questions-
answers-statements/written-statement/Commons/2015-12-
17/HCWS421/
Process/Committee approval with date(s) (as appropriate)
Governing Body

Subject:
Governing Body Assurance Framework
Presented by:
Amanda Brown, Acting Head of Corporate Affairs
Prepared by:
Amanda Brown
Submitted to:
Governing Body
Date: 26 January 2016
Purpose of paper:
To discuss and approve the Governing Body Assurance Framework (GBAF).
Executive Summary:
The Governing Body Assurance Framework (GBAF) is attached. This is presented to each Governing Body meeting; its purpose is to set out the high risk areas that could potentially impact on the Clinical Commissioning Group and its ability to meet key objectives. Any actions taken to mitigate risks, outstanding actions and proposals to address identified risks are included in order to bring the risk to a level that is acceptable and manageable. Following discussions at the Senior Manager’s Meeting (SMT) and meetings with team risk owners, since the last Governing Body meeting on 22 December 2015 the GBAF has seen the following changes: Changes to the GBAF: In addition to updates to the action plan and progress section for each risk the following changes have been made:
A new risk concerning IC24 has been added to the GBAF with a rating of 4x4=16
Recommendation to Governing Body:
The Governing Body is asked to note and comment on the contents of the Governing Body Assurance Framework and the actions taken to mitigate risks.
Agenda item: 7.4

Key Risks
Clinical:
Quality and safety risks included on registers
Finance and Performance:
Finance and Performance Risks included on registers
Impact Assessment (environmental and equalities):
None
Reputation: Failure to address risks could have an adverse impact on CCG reputation.
Legal: Failure to identify and address risks could have a significant legal impact on the CCG
Resource Required:
N/A
Reference document(s): Internal Audit Report, Governance, Risk Management and Assurance Framework
NHS Constitution:
Conflicts of Interest: Conflicts of Interests declaration completed by all Governing Body members, staff and membership. Conflicts of Interests also declared at the start of each meeting.
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
Senior Managers meeting and Audit Committee for review and Governing Body for approval.

Corporate Affairs-Assurance Framework-GBAF 1
Updated: 26 January 2016 Governing Body Assurance Framework
NHS South Norfolk CCG aims to deliver the highest quality integrated healthcare which is appropriate, effective, efficient and sustainable in order to improve the health and well-being of the whole and diverse population of South Norfolk. The Assurance Framework forms the key document for the CCG in ensuring all principal risks to the CCG’s objectives are contro lled, that there is sufficient assurance as to the effectiveness of these controls, supporting the CCG’s system of internal control. The Assurance Framework supports the CCG to mitigate risks to as low a level as practicable. Risks that are controlled to an agreed target are then moved to a sub folder, with regular review to ensure controls do not alter and risks therefore do not increase. The Assurance Framework informed the Governing Body and Audit Committee agendas. The CCG’s Integrated Risk Management Strategy and Framework detail how the Assurance Framework is populated and maintained.
1.Governance Ensure that the CCG acts in accordance within its Constitution and statutory framework under the Health & Social Act 2012.
4. Reputation Ensure the CCG maintains a good public reputation and engages with all stakeholders
2. Finance Deliver the CCG’s financial plan for 2014/15 and ensure that any risks are mitigated
5. Organisational Development Develop the organisation both at staff and governing body level
3. Quality & Safety
Ensure that the services commissioned by the CCG are of good quality and safe.
6. Operating Plan Ensure that the organisation delivers the Operating Plan
Corporate Objective
Risk Description Unmitigated risk rating (LxC)
Controls in place to mitigate risk
Assurances on controls both internal and external (Evidence that risk is being effectively managed)
Mitigated Risk Rating (LxC)
Risk movement since last report?
Date of last change
Action Plan and progress report
Target Risk Rating (LxC)
Risk Owner
Meeting: Governing Body. Date: 26 January 2016

Corporate Affairs-Assurance Framework-GBAF 2
2. Finance
Deliver the CCG’s financial plan for 2015/16 and ensure that any risks are mitigated
Fin1 (inc Fin 2, Fin 3 & Fin 4) Risk of not achieving planned deficit £6.5m – in 2015/16 as agreed with NHS England
5x5=25 R
Monthly Reporting of Finance; QIPP; Contingency (0.3% of allocation) + other uncommitted reserves and slippage
Internal: GB Reports and Minutes, Audit Committee reports and Internal Audit work plan. Financial Recovery Board External: CCG assurance process
3x5=15 R
Same Added:
April 2015
Updated 28.08.15 Updated 15.10.15 Updated 11.11.15
FRP developed and being implemented with support from Deloitte LLP. FRP Board set up for weekly review. Turnaround Director appointed and developing contract challenge and data validation process (Ma 15) FR month 6 delivery plan reported to NHSE, actions in place to enable CCG to deliver planned deficit by yearend (Oct 15) FR month 7 delivery plan reported to NHSE, actions in place to deliver planned deficit by year-end and to mitigate risk additional QIPP scheme and detailed work plans (Nov 15) Completion date: June 2016
2x1=1 G
DG

Corporate Affairs-Assurance Framework-GBAF 3
3. Quality & Safety
Ensure that the services commissioned by the CCG are of good quality and safe.
Q&S14 To ensure that NSFT commissioned services are of a high quality and safe standard via CQC Outcome; inadequate
4x4 =16
R
Provider has an improvement plan, monitored by CQC, Monitor and SNCCG via CQRM
CQC, CQRM and Stakeholder meeting Assurances reported to Governing Body.
4 x 4 =
16 R
Same
Added 17 June 2015
Update Oct 2015 Update 23.12.15
23.12.15 – Progress is still being made and CQC/Monitor feels the pace of delivery against the Quality Improvement Plan has improved (last acknowledged at SAM on 16.12.15). Trust held a CQC mock inspection w/c 30.11.15. Initial feedback indicates improvement but more work is still required. The mock inspection identified Lorenzo as a significant concern. Outcome report due end of January 2016 and will be reviewed at CQRM. Completion Date Provisional date for next inspection June 2016
3x2 = 6
Y
Quality

Corporate Affairs-Assurance Framework-GBAF 4
2. Finance Deliver the CCG’s financial plan for 2015/16 and ensure that any risks are mitigated
Fin 22 Risk of financial QIPP challenge in 2015/16
5x5=25 R
Medium Term Financial Forecast submitted 7th April showing £4.7m QIPP requirement and £8.3m deficit (Feb 15) Turnaround Director appointed (Jan 15) Month 6 FRP Delivery presentation shows actions worth £2.5m to enable delivery of £6.4m deficit plan. (Oct 15) QIPP schemes anticipated to deliver in full at year end of £5.7m per plan (Oct 15)
Internal: GB Reports and Minutes, Audit Committee reports and Internal Audit work plan. CSU performance meeting reports FRP Board External: CCG
5x5=25 R
Same
Added 10.02.15 Updated 28.08.15 Updated 15.10.15
Transactional QIPP schemes to be developed for 1516 with support from Deloitte (Feb 15) FRP Board scrutiny (Mar 15) Month 2 QIPP monitoring included within finance report (Jun 15) QIPP Schemes now starting to deliver savings (Aug 15) Turnaround director and QIPP processes in place to be reviewed regularly to keep focus and see progress (Aug 15) QIPP schemes delivered £1.6m of £5.7m plan at month 6. Actions in place for FOT to deliver in full (Oct 15) NHS England fully aware of position at month 6 and supportive CCG will meet target (Oct 15) Completion Date
June 2016
1x1=1 G
DG

Corporate Affairs-Assurance Framework-GBAF 5
3. Quality & Safety & 6. Operating Plan Ensure that the organisation delivers the Operating Plan
CO1 (inc CO1a) Risk of not meeting operational standards – underperformance specifically 18 week RTT Standard in T&O, ENT, Gynea, Ophthalmology and Dermatology
5x4 = 20 R
SPRG process. HSCIC re process for C&B slots
Internal: GB External: CCG assurance process
5X4 = 20 R
Same Added April 2014 Updated Oct 2015 Updated Jan 2016
16.10.15: Trust submitted RTT recovery trajectory 14.08.15, this was rejected by commissioners with a stipulation to resubmit a full RAP on 02.10.15. RAP has not been received at the time of update, JB has escalated to CSU, CSU escalating to NNCCG for resolution. 27.10.15 Co-coordinating commissioner issues RTT Contract Performance Notice rejecting NNUHFT plan to achieve 92% Incomplete Pathway standard and progress to application of GC9.4 02.12.15 Meeting between NNCCG, NNUHFT, Monitor and NHSE, outcome was to reject revised RAP due to August 2016 proposed trajectory. Review of renegotiated date to occur 29.01.16 Completion date: TBC
2x3 = 6
Y
JP

Corporate Affairs-Assurance Framework-GBAF 6
3. Quality & Safety & 6. Operating Plan Ensure that the organisation delivers the Operating Plan
CO1 (inc CO1a) Risk of not meeting operational standards – underperformance specifically A&E
5x4 = 20 R
SPRG process
Internal: GB External: CCG assurance process
5X4 = 20 R
Same Added April 2014 Updated Oct 2015 Updated Jan 2016
15.10.15 co-ordinating commissioner issues exception report to NNUHFT for failure to achieve recovery deadline of 04.10.15 agreed in formal action plan. Under General Condition 9.21 of the 2015/2016 NHS Standard Contract, the Co-ordinating Commissioner has instructed Commissioners party to the Contract to withhold 2% of the Actual Monthly Value in accordance with General Condition 9.21. In lieu of the Actual Monthly Value being available for September, 2% of the planned contract value will be withheld from the next monthly payment. 13.01.16 contract performance notice issued confirming 2% contract value to be retained for Sept, Oct, 2015 if trajectory not achieved by 02.02.16 Completion date: April 2016
2x3 = 6
Y
JP

Corporate Affairs-Assurance Framework-GBAF 7
6. Operating Plan Ensure that the organisation delivers the Operating Plan
CO4 & Q&S2 Risk of EEAST not meeting Ambulance response times within SNCCG (Red 1&2 A8, Red 2 A18, Green 1-4 standards) Lack of assurance of service quality and patient safety
5x4=20 R
EEAST locality meetings to discuss operational delivery, and application of contractual sanctions to failing measures. Monthly and quarterly CQRM meetings in place
Internal: GB External: HOSC Acute Commissioning Network CPG
4x4 = 16 R
Same
Added 2.09.14 Incorporated both CO4 and Q&S2 into 1 risk Updated Nov 2015 Updated Jan 2016
06.11.15 Remedial Action Plan (RAP) reviewed by Accountable Officer (AO) group and rejected; discussions continue with EEAST, TDA and Monitor to produce acceptable RAP, but no date. 20.01.16 Andrew Pike (NHS E) instructed reinvestment £2m contract fines for 2015/16. RAP review 05.02.16, but remains un-agreed Completion date: April 2016
4x3 = 12 A
JP

Corporate Affairs-Assurance Framework-GBAF 8
6. Operating Plan Ensure that the organisation delivers the Operating Plan
CO5 (Inc CO5a) Risk of not completing Looked After Children (LAC) assessments within statutory guidance.
4x4 = 16 R
Application of contractual levers Review completed by CSU Child Health Team. Actions contained within NCH&C 14/15 SDIP CCGs have committed £83k additional funding for 15/16
Internal: GB External: CCG assurance process Child Health and Maternity Commissioning Network Commissioning Team report
4x4 = 16 R
Same Added June 2014 Updated Jan 2016
12.01.16 Ofsted report published Oct 15 rated services for LAC as Inadequate, citing LAC health assessments as of particular concern There are a series of short term and long term plans to address the concerns raised by Ofsted A remodelling of the service is being undertaken with the provider, NCC Designated Doctor and CSU. Much of this work is dependent on NCC’s business process re-engineering exercise, the date of which has been delayed to January 2016 due to staff sickness. Contractual discussions between CCGs and NCH&C about the service specification, KPIs and funding for 15/16. CQN to be issued if short term actions do not address some of the concerns.
An increase in the
capacity of core
targeted and specialist
CAMHS to manage
4x3= 12 A
JP

Corporate Affairs-Assurance Framework-GBAF 9
the mental health
needs of children and
young people on the
edge of care and those
who are looked after or
adopted was included
in the Transformation
plan.
Completion Date: March 2016

Corporate Affairs-Assurance Framework-GBAF 10
6. Operating Plan Ensure that the organisation delivers the Operating Plan
CO 22 Cancer – 31 day and 62 day target continued underperformance – NNUH
5x4 (20)
R
Paper going to SNCCG Business Seminar. NNUH have produced a remedial action plan but the timescales for achievement are too long.
SNCCG Gov Body. NNUH C&P Meeting and CQRM
5x4 (20)
R
Same
Added 5.02.15
Update
2015
Updated Jan
2016
23.10.15 Co-ordinating Commissioner accepts NNUHFT remedial action plan to recover 62 day operating standard by 31.12.15 RAP for Cancer 62 days in October 2015 was accepted by the Commissioner, but Trust failed trajectory in Nov. 29.12.15 exception report issued identifying 2% contract value withhold Completion date April 2016
2x4 (8)
A
JP
3. Quality & Safety Ensure that the services commissioned by the CCG are of good quality and safe.
IC24 contract commenced on 01.09.15. The service is facing recruitment challenges particularly medical cover
4 x 4 = 16 Monthly CQRM QPSAC
Ongoing recruitment Ongoing training
4 x 4 = 16
Added 19 January 2016
23.12.15 Concerns continue to be raised at CQRM, weekly improvement plan meetings in place.
AL
Risk Matrix - taken from CCG Risk Scoring and Identification Guidance and Process: RISK MATRIX
Likelihood
Consequence 1 – Rare 2 - Unlikely 3 – Possible 4 – Likely 5 – Almost Certain
1 – Negligible 1 2 3 4 5
2 – Minor 2 4 6 8 10
3 – Moderate 3 6 9 12 15
4 – Major 4 8 12 16 20
5 - Catastrophic 5 10 15 20 25

Subject:
Communications and Engagement Update
Presented by:
Oliver Cruickshank – Communication and Engagement Manager
Submitted to:
Governing Body
Date: 26 January 2016
Purpose of paper:
For information
Executive Summary:
Summary
Launched and maintained the CCG’s consultation on its policy regarding Adult Hearing Aid services for people with Mild hearing loss (9th November 2015 – 15th January 2016); helped to facilitate workshop with stakeholders on 1st December 2015
Continued communication support to Practices and patients regarding the CCG’s prescribing initiatives
Coordinated work with North Norfolk and Norwich CCGs and local providers in response to the Central System Resiliency Group’s communication needs in the run up to Winter 2015/16.
Supported and coordinated a ‘Health Transport’ event alongside colleagues at Norwich CCG, bringing together statutory, independent and voluntary transport providers, commissioners and patient representatives
Continued workshops between South Norfolk Council, Breckland District Council and the CCG
Supporting the ABCD Project’s Winter Wellbeing Festival on January 30th 2016, and evaluation of project – see Appendix A
Press
Campaign across Archant publications: Mental Health Watch – encouraging readers and stakeholders to support ongoing focus on mental health provision locally
Across November / December / January: focus on pressures at local acute providers
17/11/15 – CAMHS: Funding agreed for investment in children and adolescent mental health services across Norfolk
19/11/15 – Focus on perinatal services available in Norfolk
24/11/15 – West Norfolk CCG ends gluten free product prescribing
25/11/15 – Impact of Government comprehensive spending review
25/11/15 – SNCCG ceases funding for IVF following Governing Body meeting
28/11/15 – Fines for local acute providers. Editorial – providers must work closely with CCGs
Agenda item: 8.1

30/11/15 – Patients in Thetford with learning disabilities travel long distances for care
01/12/15 – Junior Doctor’s strike avoided
08/12/15 – Letter: British Tinnitus Association criticises SNCCG’s proposed audiology policy
09/12/15 – Focus on SNCCG’s change in approach to Prior Approval. Editorial: SNCCG and variation in care
12/12/15; 17/12/15; 23/12/15 – SNCCG in negotiation with All Hallows over beds
15/12/15 – Mental Health in schools, focusing on Neatherd, Dereham – mentions SNCCG’s ‘ABCD’ Project
19/12/15 – Focus on SNCCG’s ‘ABCD’ Project
23/12/15 – Walk-in Centre to support demand over busy Christmas period Patient and Service Users
Continued attendance at NSFT’s monthly City & South Service User and Carers Forum
Designing next PPG event for March / April 2016
GPs, Practice Managers, Surgery Staff
Communicating updates from the CCG regarding ongoing commissioning and QIPP activity
Helping to encourage Practices to submit project proposals for the CCG’s 16/17 QIPP plans
External Stakeholders
Attended Healthwatch Norfolk workshop focusing on Migrant communities accessing healthcare in Norfolk
Attended the Older People’s Strategic Partnership away day in Dereham
Key Risks
Clinical:
N/A
Finance and Performance:
QIPP – public feedback regarding the CCG’s QIPP activity could impact on future decisions (and financial performance)
Impact Assessment (environmental and equalities):
N/A
Reputation: Commissioning decisions - may cause significant scrutiny of the CCG from local and national media and focus groups
Legal: None
Resource Required:
Reference document(s):
‘Appendix A – ABCD Project Update’
NHS Constitution:
N/A
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
N/A

1
Subject:
Transforming Care
Presented by:
Alison Leather
Prepared by:
Alison Leather/Clive Rennie
Submitted to:
Governing Body
Date: 12th January 2015
Purpose of paper:
To brief Governing Body on Transforming Care (January & October 2015) and to discuss and agree local solution for delivery of Transforming Care.
Executive Summary:
Transforming Care aims to deliver significant improvements in the care of children, young people and adults with Learning Difficulties. The most immediate focus being to ensure, where clinically appropriate, that people who are placed in in-patient care, move to less restrictive environments and community settings with support. Commissioners are required to ensure:
People who do not need to be in hospital are discharged
The right community services are available to support people in their own home (Intensive Support Teams)
Only those people who require admission to hospital are admitted
By March 2019 we are spending less on inpatient services and more on services in the community.
Locally Norfolk CCG’s commission 12 in-patient Assessment and Treatment beds from Hertfordshire Partnership Foundation Trust. The contract for these beds was extended in 2014 for two years and hence terminates on March 31st 2016. The contract covers West Norfolk CCG, Norwich CCG, North Norfolk CCG, South Norfolk CCG and Great Yarmouth and Waveney CCG (for patients in the Great Yarmouth area not Waveney). West Norfolk CCG are the only CCG to currently commission a community based Intensive Support Team. It has been effective in delivering an assumed reduction of the number of patients and occupied bed days used by WNCCG. This papers offers two models by way of next steps in enabling Norfolk CCG’s including West Norfolk and Great Yarmouth and Waveney to deliver the recommendations made in Transforming Care. The Governing body is asked to note the strategic direction outlined in Transforming Care and discuss and make a recommendation against the two operational models proposed.
Agenda item: 8.2

2
1. Context Winterbourne View, reported by Panorama in (2012), resulted in adult safeguarding issues and criminal actions against individuals who committed assaults on patients. Following on from Winterbourne View (2012) NHS England in partnership with Social Care committed to improving the health and outcomes of people with learning disabilities and autism, and transforming services to improve the quality of care throughout peoples’ lives. Transforming Care (January 2015) subsequently has established a clear programme of work with other national partners to improve services for people with learning disabilities and/or autism, who display behaviour that challenges, including those with a mental health condition. It is a system-wide change that will enable more people to live in the community, with the right support, and close to home. 2. National Guidance
Transforming Care (January 2015) has now evolved into the National Learning Disability Transformation Plan. Each CCG needs to submit a plan of action to NHSE by April 2016. Six pilot areas have been in operation for over a year and there is a clarity of national direction beginning to emerge.
The key points that have been forthcoming from the National Learning Disability Transformation Plan are:
NHS England have stated that c£45m of national funds will be available to support the transition over the next three years with match-funding being provided by CCGs. Confirmation of how the funds will be devolved is yet to be confirmed.
Forty nine Transforming Care Partnerships (TCPs) will be established bringing together health and care commissioners, providers, charities and people with learning disabilities and/or autism. These have to be in place locally by December 2015.
Transformation Plans: the TCP’s will then be responsible for developing local transformation plans. These need to be complete and submitted to NHS England by April 2016 in order to secure funds to support transition.
A new financial framework will be established with shared budgets across the NHS and local councils. NHS funding will move with them to community services, for as long as they need it.
A revised Service Model based on nine principles that defines what good services look like and based on the early learning from the six (Fast-Track) areas will be rolled out nationally. This includes a requirement to reduce current CCG inpatient capacity by a minimum of 45% and SCG inpatient capacity by a minimum of 25% with an overall of 35-50% of inpatient capacity being closed nationally with alternative care provided in the community.
By April 2016, every CCG will be expected to have a ‘local offer’ for how to expand the use of personal health budgets; this must include people with a learning disability.
Care and Treatment Reviews (CTRs) – to prevent unnecessary in-patient admissions and lengthy hospital stays will be put in place. Local review teams should include people with ‘lived experience’ of learning disabilities/ autism’ and aim to ensure there is a care plan in place to meet the individual’s needs. CTR’s will be undertaken either before a person goes into hospital where there is a known planned admission (Community CTR) or a as ‘blue light’ when the situation is urgent. If the later occurs a CTR has to be undertaken within 10 days of admission. This will require Accountable

3
officer sign-off. Discharge dates are to be set at the time of a CTR and a patient and/or care has the right to request a CTR where there are concerns about safety and wellbeing and /or there is no clear discharge plan and date.
CTR guidance identifies clear roles and responsibilities for CCG’s including:-
o Ensuring engagement of CCG commissioners o Ensuring any immediate actions resulting from reviews are followed up o Working in partnership with Local Authorities to deliver discharge/transfer plans o Tracking delivery of discharge/transfer plans recommended by CTR o Develop positive working relationships with inpatient and community providers to
ensure effective delivery. o Proving assurance to CCG Board o Providing assurance to Regional/Area Team
Each CCG will be expected to develop a local CTR Policy. This will include the following:
o Local population based data, including how many CTRs are anticipated for the
locality o Local risk criteria used to define the ‘At Risk of Admission’ population. o Governance arrangements locally
NHS England are putting in place local performance frameworks to monitor the implementation of Transforming Care. Assurance will be sought through weekly tracker reporting on progress at patient level as of January 2016. Accountable Officer sign-off will be required in some areas.
Although there are key points indicated it is important to consider that some vital issues have not been clearly defined as yet which could lead to unquantified risk for the CCG’s, examples of these are:
There appears to have been an assumption that the number of patients at the Specialised Commissioning level is set or constant, this is not correct. There is turnover of patients at this level, with step down taking place already for a number of patients. The level coming into that high level provision is currently random. This is a significant financial risk to CCG’s.
A common route into this level of provision is via Court direction and hence the Ministry of Justice. Offenders/ patients at this level are usually placed in very costly placements, based on the extent of their needs.
Guidance on pooling of resources between Health and Social Care has not been produced
Movement of funding with the patient has not been clarified. Sir Simon Stevens committed to a dowry for patients who have been in a specialised commissioning placement for more than five years, the detail of this commitment is unclear.
3. Local Context
Norfolk CCG’s commission 12 in-patient Assessment and Treatment beds (Astley Court) from Hertfordshire Partnership Foundation Trust. The contract for these beds was extended in 2014 for two years and terminates on March 31st 2016. The contract covers West Norfolk CCG, Norwich CCG, North Norfolk CCG, South Norfolk CCG and Great Yarmouth and Waveney CCG (for patients in the Great Yarmouth area not Waveney).
The average bed use for last two years is 8.4 beds across five CCG’s.
West Norfolk CCG are the only CCG to currently commission a community based Intensive Support Team for Learning Disabilities. This has to date realised an assumed

4
reduction of the number of patients and occupied bed days used by WNCCG. This is in keeping with the national picture. As a result West Norfolk have not confirmed their intention to re-commission any bed days at Astley Court after April 2016.
Great Yarmouth and Waveney CCG have confirmed their commissioning intentions to increase the span of the commissioned service to cover the Waveney area for both in-patient bed provision and an enhanced Community Intensive Support function. A new financial arrangement between the CCG’s is needed to ensure that a parity of arrangement is maintained.
The current contract financially appears to have been allocated on a per capita basis (Appendix A outlines current contract and financial split by CCG), which does not align with service usage.
The current inpatient view and costs are summarised at Appendix B.
Patient Safety and Quality Leads have confirmed that Hertfordshire Partnership Foundation Trust (HPFT) are considered to be the most capable provider of Learning Disability Services. As such it was agreed that HPFT should be assured that the contract would continue after 2016 dependent on the CCG’s agreeing a new service model.
Procurement colleagues have confirmed that the contract can be awarded to the existing provider and that any risk of external challenge can be mitigated against.
Summary table of CCG current spend on Learning Disability placements and anticipated CCG step down costs of patients in Specialised Commissioning placements
December 2015
CCG CCG Cost per annum
NHSE Costs per annum
Total CCG & NHSE costs per annum
Estimated stepdown from NHSE cost into eg Locked Hospital
Number of patients
NNCCG Total 820,664 542,000 1,362,664 286,000 7
SNCCG Total 843,960 796,000 1,639,960 715,000 10
NCCG Total 470,288 1,384,000 1,854,288 1,144,000 10
GY&W CCG 153,000 1,084,000 1,237,000 858,000 7
WNCCG Total 455,000 300,000 755,000 286,000 5
Grand Total 2,742,912 4,106,000 6,848,912 3,289,000 39
4. Next steps Norfolk CCG’s now need to confirm the preferred service model to be re-commissioned with HPFT. On-going engagement and consultation on the development of this service model has determined the following preferences:
North Norfolk CCG: commission a 6 block bed + partial LD IST model.
South Norfolk CCG: 8 beds plus partial LD IST
Norwich CCG: block purchase and suggested a business case for an LD IST is developed.
GY&W CCG: block booking covering Waveney area with ability to spot purchase if required and a partial LD IST.
West Norfolk CCG: opportunity to spot purchase beds from HPFT under the new arrangement.

5
As a result two service models have been proposed for consideration:
Option one: o Commission 1.5 Assessment and Treatment beds per CCG (North Norfolk
CCG; South Norfolk CCG; Norwich CCG & Great Yarmouth and Waveney CCG) per annum as part of a block contract totalling six beds.
o Ability to spot purchase additional beds as required at a previously agreed competitive rate
o Establishment of a ‘light’ LD Intensive Support Team that is able to support a reduced length of stay in an inpatient setting, enable some patients to remain in their own home and to undertake Clinical Treatment Reviews.
Option Two: o Commission a mixture of Assessment and Treatment beds and medium term
inpatient beds. The bed cohort would be used flexibly based on need as part of a block contract totalling 12 beds.
o Establish an ‘enhanced’ Intensive Support team with fully functioning multi-disciplinary team that is able to gate keep all inpatient beds; support a reduced length of stay in an inpatient setting, enable a wider range of patients to remain in their own home including Learning Disability patients who require Continuing Health Care; facilitate step down from Specialised Commissioning and to undertake Clinical Treatment Reviews.
5. Cost Benefit Analysis
Option one: x6 Assessment and Treatment beds; ability to spot purchase up to six more;
IST ‘light’
Option two: x 12 flexible use inpatient beds plus enhanced IST including MDT
Cost Benefit Cost Benefit The six bed model remains
within the current pricing envelope.
The 12 bed model plus the enhanced IST exceeds the current pricing envelope however these costs will be off- set by NHS England transformation funding.
This model will have the ability to gate keep all inpatient beds including those commissioned and provided by other providers e.g. Cawston Park.
Delivers national requirement to reduce inpatient bed capacity locally by an expected 20-25% based on local and national evidence.
Delivers national requirement to reduce local inpatient bed capacity by an expected 20-25% based on local and national evidence.
This option fulfils the national requirement to deliver an Intensive Support Team
This option fulfils the national requirement to deliver an Intensive Support Team
Limited ability if any to undertake NHS CHC assessments for patients with Learning Disabilities and reduce spend on cost on NHS funded care.
Spot beds will be available at £455 per day for beds 7 and 8, and £100 per day for beds 9-12 for CCGs participating in the block arrangement. This is a competitive rate and cheaper than currently expected by other providers. This cost would be over and above the additional cost envelope.
The financial hypothesis assumes this model would impact on current CCG spend on independent in-patient placements, to review LD CHC placement and potentially clinically challenge inappropriate packages of care, and to reduce the potential cost pressure of Specialised Commissioning step down placements by movement of the patient to the lowest intervention level as soon as possible. This will future proof both the Transforming Care

6
agenda and NHS CHC for people with LD.
The commissioning of medium term beds within a block contract would lessen the need for the usage of more expensive Independent hospital placements.
Ability to reduce length of stay and facilitate earlier discharge into the patient’s own home.
Ability to reduce length of stay and facilitate earlier discharge into the patient’s own home.
Ability to deliver CTR’s Ability to deliver CTR’s and NHS CHC Assessments
HPFT have been identified as the Most Capable Provider reducing the likelihood of challenge by the wider market.
This model is viewed as being potentially contestable by the wider market making the risk of challenge by wider local market place more likely.
The issue of apportionment of the costs remains, and the Working Group dealing with this would recommend consideration be given to a model, perhaps either a usage based model or a model based on all participating CCGs contributing equally to the block.
The issue of apportionment/ activity remains the recommended solution is that CCG’s would be allocated a bed day quota based on financial input into the block. It is recommended that this is retrospectively quarterly adjusted based on actual usage.
The ability to transfer/step down patients into their own homes or less restrictive environments is dependent on increasing capacity in District Councils/NCC housing & residential market
The ability to transfer/step down patients into their own homes or less restrictive environments is dependent on increasing capacity in District Councils/NCC housing & residential market.
6. Financial Modelling See Appendix B and C. 7. Recommendation to Governing Body:
The Governing Body are asked to consider the options for future service delivery of local Inpatient and Community based services for people with Learning Difficulties and make a recommendation to be taken forward to the JCC on behalf of South Norfolk CCG.

7
Appendix A
CURRENT CONTRACT PAYMENTS
Current annual contract values split by CCG are as follows:
Authority Annual Payment
NHS GY&W CCG (1 bed only –
to be increased to 2) £259,977
NHS North Norfolk CCG £411,072
NHS Norwich CCG £436,056
NHS South Norfolk CCG £483,580
NHS West Norfolk CCG £429,027
Total £2,019,711

8
Appendix B
LD inpatient review
December 2015
Area CCG Responsible Commissioner Provider
CCG Cost per
annum
NHSE Costs per
annum
Total CCG &
NHSE costs per
annum
Estimated
stepdown from
NHSE cost into
eg Locked
Hospital
Number of
patients
Central & East North Norfolk CCG NHSE Partnership in care 150,000 150,000 143,000 1
Other 392,000 392,000 143,000 2
NHSE Total 542,000 542,000 286,000 3
NNCCG Cawston Park 820,664 820,664 4
NNCCG Total 820,664 820,664 4
North Norfolk CCG Total 820,664 542,000 1,362,664 286,000 7
South Norfolk CCG NHSE Partnership in care 450,000 450,000 429,000 3
Other 346,000 346,000 286,000 2
NHSE Total 796,000 796,000 715,000 5
SNCCG Cawston Park 843,960 843,960 5
SNCCG Total 843,960 843,960 5
South Norfolk CCG Total 843,960 796,000 1,639,960 715,000 10
Norwich CCG NCCG Cawston Park 470,288 470,288 2
NCCG Total 470,288 470,288 2
NHSE Partnership in care 646,000 646,000 572,000 4
Other 738,000 738,000 572,000 4
NHSE Total 1,384,000 1,384,000 1,144,000 8
Norwich CCG Total 470,288 1,384,000 1,854,288 1,144,000 10
Great Yarmouth & Waveney CCG GY&WCCG Other 153,000 153,000 1
GY&WCCG Total 153,000 153,000 1
NHSE Partnership in care 150,000 150,000 143,000 1
Other 934,000 934,000 715,000 5
NHSE Total 1,084,000 1,084,000 858,000 6
Great Yarmouth & Waveney CCG Total 153,000 1,084,000 1,237,000 858,000 7
Central & East Total 2,287,912 3,806,000 6,093,912 3,003,000 34
West West Norfolk CCG NHSE Other 300,000 300,000 286,000 2
NHSE Total 300,000 300,000 286,000 2
WNCCG Cawston Park 283,920 283,920 2
Other 171,080 171,080 1
WNCCG Total 455,000 455,000 3
West Norfolk CCG Total 455,000 300,000 755,000 286,000 5
West Total 455,000 300,000 755,000 286,000 5
Grand Total 2,742,912 4,106,000 6,848,912 3,289,000 39

9
Key Risks
Clinical:
Patients are not able to access care in the most appropriate setting according to their individual needs.
Poor patient outcomes
Finance and Performance:
Increasing cost pressure of expanding population of patients with Learning Disabilities in South Norfolk due to step down from SCG
SNCCG unable to deliver national requirement to reduce local inpatient bed capacity by 10%
SNCCG not able to ‘step-down’ x5 patients as identified by SCG
Impact Assessment (environmental and equalities):
South Norfolk is not compliant with Green Light Tool Kit leaving people with Learning Difficulties at risk of discrimination
Reputation:
Legal: Advice not sought regulatory impact unknown
Appendix D
Costs for Model B
£ million per annum
Cost for 12 beds £2,147,000.00
Cost for full IST £761,000.00
Total Costs £2,908,000.00
Appendix C
Summary Costs, apportionment of Model A costs
(assuming each CCG uses 547.5 bed days per annum)
6 bed block IST Total
South
Norfolk
CCG
North
Norfolk
CCG
Norwich
CCG
Great
Yarmouth
& Waveney
CCG
West
Norfolk
CCG
1,621,845 £398,083.00 £2,019,928.00 £504,982.00 £504,982.00 £504,982.00 £504,982.00
6 bed block £1,621,845.00 £324,369.00 £324,369.00 £324,369.00 £324,369.00 £324,369.00
IST £398,083.00 £99,520.75 £99,520.75 £99,520.75 £99,520.75
£2,019,928.00 £423,889.75 £423,889.75 £423,889.75 £423,889.75 £324,369.00
Spot beds
Annual cost
4 beds @ £455 per day £166,075.00
2 beds @ £100 per day £36,500.00
Outside block @ £595 per day £217,175.00

10
Resource Required:
As identified in paper
Reference document(s):
Winterborne View 2012
Transforming Care 2015
NHS Constitution:
Fulfils requirement of NHS Constitution
Conflicts of Interest:
None identified
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
SMT Governing Body JCC

Subject:
Corporate Affairs Report
Presented by:
Amanda Brown, Acting Head of Corporate Affairs
Prepared by:
Amanda Brown, Acting Head of Corporate Affairs
Submitted to:
Governing Body
Date: 26 January 2015
Purpose of paper:
For information and to update the Governing Body.
Executive Summary:
Governing Body Elections An election for Governing Body members has been launched with 26 January 2016 being the closing date for applications. Applicants that meet the selection criteria will be notified to the membership and a formal election process begun. The closing date for ballots is 12 February 2016 and following a period to allow for any appeal confirmation of the results will be made on 2 March. Annual Report Work is progressing on the annual report, the full draft report and accounts should be submitted by 9am on Friday 22 April 2016. The final full audited and approved Annual report and accounts should be submitted by of noon on Friday 27 May 2016 to NHS England. The CCG will be holding an Audit Committee on Tuesday 24 May 2016 followed by a Governing Body meeting in the afternoon for approval of the annual report and accounts. These are nationally set deadlines and the CCG is currently on course to adhere to these. Stakeholder Survey The annual stakeholder survey will be launched shortly. The survey is part of the CCG annual assessment and provides an opportunity for CCGs and their stakeholders to answer questions about their relationships and how they can be improved to ensure better outcomes for patients. Elected members are asked to raise awareness of this survey with member practices when on visits or during discussions to help improve response rates. Information Governance Toolkit The Action Plan for the IG Toolkit has been prepared. The CCG Internal Auditors have met with members of the Corporate Affairs team to review selected requirements. Feedback
Agenda item: 8.4
from this first informal meeting was that there were no concerns with the Toolkit. There is some work to do with respect to providing refreshed versions of documents and minutes from later meetings. It is requested that the Governing Body delegate approval of submission of the IGT to the March meeting of the Audit Committee. Business Continuity Plans The Corporate Affairs team have undertaken a refresh and review of the CCG’s Business Continuity Plan, and has made minor changes required to the document to update named personnel in the policy.
Recommendation to Governing Body:
The Governing Body is asked to note the contents of the report and approved the delegation of approval of submission of the IGT to the March meeting of the Audit Committee.

Key Risks
Clinical:
Not applicable
Finance and Performance:
Not applicable
Impact Assessment (environmental and equalities):
Not applicable
Reputation: If the CCG is not compliant with all guidance and regulations it will affect its reputation
Legal: It is important that the CCG is fully compliant will all guidance and regulations
Resource Required:
None
Reference document(s):
None
NHS Constitution:
There are not specific references to the NHS Constitution in this document
Conflicts of Interest:
None
GOVERNANCE
Process/Committee approval with date(s) (as appropriate)
Governing Body for noting and approval