age-related macular degeneration (amd) disruptions to the
TRANSCRIPT

MMED3937 Pathophysiology for Medical Science
74
Chronic Eye Conditions Age-related macular degeneration (AMD)
• A medical condition that usually affects older adults and results in central field of vision loss due to macular damage
• Two forms: dry and wet • It is a major cause of blindness and visual impairments in adults > 50 years • MD can make it difficult or impossible to read/recognise faces, although peripheral vision remains
relatively intact, allowing other ADLs • Begins with characteristic yellow deposits (drusen) in the macula, between the RPE and the
underlying choroid • Most people with these early changes (age-related maculopathy) have good vision • People with drusen can go on to develop advanced AMD • The risk is considerably higher when the drusen are large and numerous, and is associated with
disruptions to the RPE • Recent studies suggest that large and soft drusen are related to hypercholesterolaemia and may
respond to cholesterol-lowering agents Drusen formation
• Drusen – yellowish extracellular waste products that accumulate within and beneath the RPE layer • The source of proteins and lipids in drusen is unclear, with potential contributions by both the RPE
and choroid • Several trace elements are present in drusen, with the most concentrated being zinc • The protein composition of drusen includes apolipoproteins and some complements • Zinc has been suggested to play a role in drusen formation by precipitating and inhibiting the
elements of the complement cascade, especially by complement factor H • The presence of molecules that regulate inflammation in drusen has led some investigators to
conclude that these deposits are a product of the immune system • The results indicate that cellular remnants and debris derived from degenerate RPE cells become
sequestered between the RPE basal lamina and Bruch’s membrane (located in the retina between the choroid and RPE layer, provides support to the retina and functions as the basement membrane of the RPE layer), constituting an inflammatory stimulus and a potential nucleation site of drusen formation
• The entrapped cellular debris then becomes the target of encapsulation by a variety of inflammatory mediators, some of which are contributed by the RPE, and perhaps other cell types (some are extravasated from the choroidal circulation)
MMED3937 Pathophysiology for Medical Science
75
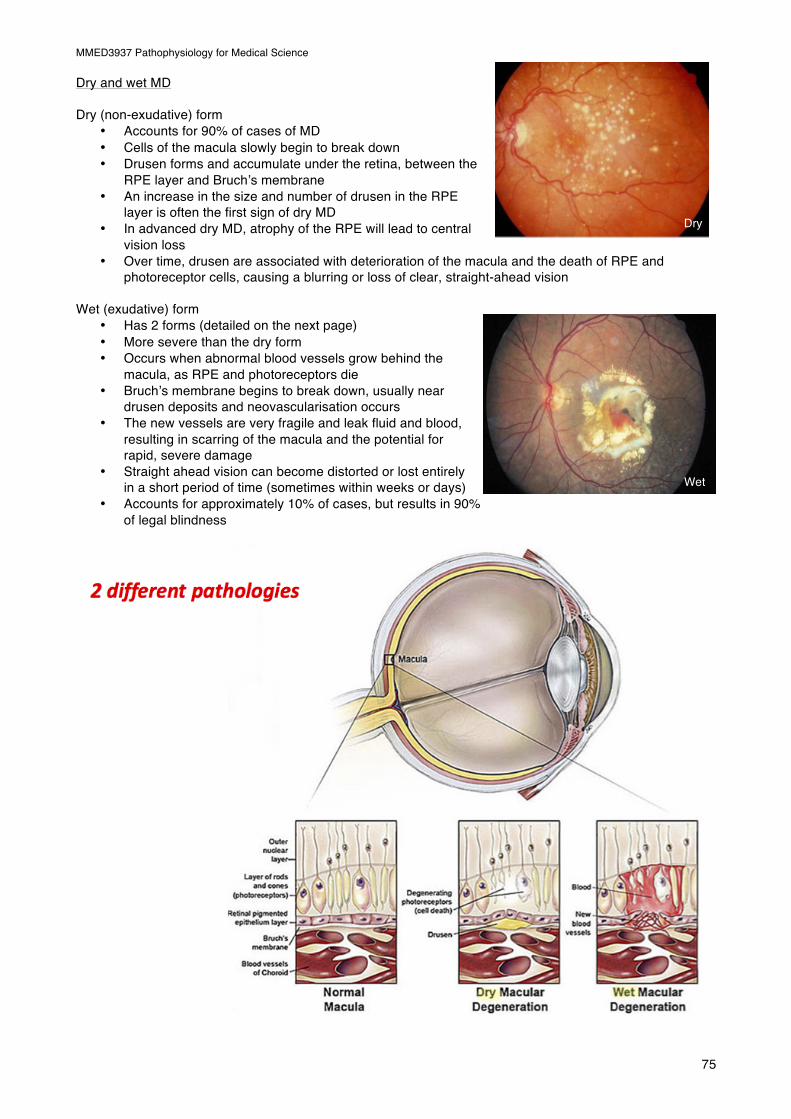
Dry and wet MD Dry (non-exudative) form
• Accounts for 90% of cases of MD • Cells of the macula slowly begin to break down • Drusen forms and accumulate under the retina, between the
RPE layer and Bruch’s membrane • An increase in the size and number of drusen in the RPE
layer is often the first sign of dry MD • In advanced dry MD, atrophy of the RPE will lead to central
vision loss • Over time, drusen are associated with deterioration of the macula and the death of RPE and
photoreceptor cells, causing a blurring or loss of clear, straight-ahead vision Wet (exudative) form
• Has 2 forms (detailed on the next page) • More severe than the dry form • Occurs when abnormal blood vessels grow behind the
macula, as RPE and photoreceptors die • Bruch’s membrane begins to break down, usually near
drusen deposits and neovascularisation occurs • The new vessels are very fragile and leak fluid and blood,
resulting in scarring of the macula and the potential for rapid, severe damage
• Straight ahead vision can become distorted or lost entirely in a short period of time (sometimes within weeks or days)
• Accounts for approximately 10% of cases, but results in 90% of legal blindness
Wet
Dry

MMED3937 Pathophysiology for Medical Science
76
2 types of wet MD
I. Vision loss caused by abnormal blood vessel growth • Choroidal neovascularisation occurs when new abnormal new blood vessels grow from the
choroid, under and into the macular portion of the retina • These abnormal vessels leak fluid or blood between the choroid and macula • The fluid interferes with the retina’s function and causes blurring of central vision • In addition, what you see when looking straight ahead becomes wavy or crooked, and blank
spots block out your field of vision
II. Vision loss caused by fluid build-up between the choroid and RPE layer • This condition is also called RPE detachment • It occurs when fluid leaks from the choroid and collects between the choroid and the RPE layer • Abnormal choroidal blood vessel growth is not usually seen when the RPE is detached • Instead, fluid beneath the RPE causes what looks like a blister or bump under the macula

MMED3937 Pathophysiology for Medical Science
77
Risk factors for AMD Age
• Approximately 10% of patients 66 to 74 years old will have findings suggestive of AMD • This prevalence increases to 30% in patients 75 to 85 years of age
Family Hx
• The lifetime risk of developing late-stage MD is 50% for people with a positive family Hx, versus 12% for people with no positive family Hx of AMD – a four-fold risk
Genetics
• The genes for the complement system proteins factor H (CFH), CFB and C3 have been determined to be strongly associated with a person’s risk in developing AMD
HTN
• Administering anti-HTN drugs have been recently found to be associated with a lower risk of developing MD
Cardiovascular status
• High cholesterol, obesity and high fat intake is associated with an increased risk of MD Oxidative stress
• It has been proposed that age-related accumulation of low-molecular weight, phototoxic, pro-oxidant melanin oligomers within lysosomes in the RPE may be partly responsible for decreasing the digestive rate of photoreceptor outer segment (POS) by the RPE
• A decrease in the digestive rate of POS has been shown to be associated with lipofuscin formation – a classic sign of MD
Race • MD is more likely to be found in Caucasians than in people of African descent Smoking • Smoking increases the risk of MD by 2 to 3 times that of a non-smoker, and may be the most important
modifiable risk factor in its prevention
Risk factors
for AMDAge
Family Hx
Genetics
HTN Cardiovascular status
Oxidative stress
Race
Smoking

MMED3937 Pathophysiology for Medical Science
78
Signs and symptoms of MD • Drusen • Pigmentary alterations • Exudative changes: haemorrhages in the eye,
hard exudates, subretinal/sub-RPE/intra-retinal fluid
• Atrophy • Visual acuity drastically decreasing • Preferential hyperacuity perimetry changes • Atrophy: incipient and geographic • Slow recovery of visual function after exposure to
bright light
• Blurred vision: those with dry MD may be asymptomatic or notice a gradual loss of central vision, whereas those with wet MD often notice a rapid onset of vision loss
• Distorted vision: in the form of metamorphosia, in which a grid of straight lines appears wavy and parts of the grid may appear blank
• Trouble discerning colour: specifically dark ones from dark ones, and light ones from light ones
• Loss in contrast sensitivity
Management of AMD Dry AMD
• No medical/surgical intervention available • However, vitamin supplements with high doses of the antioxidants lutein and zeaxanthin have been
suggested by the National Eye Institute and others to slow the progression of dry MD and, may also improve visual acuity in some patients
Wet AMD
• Until recently, no effective treatments were known • New drugs, called anti-angiogenics or anti-VEGF (vascular endothelial growth factor) agents can
cause regression of the abnormal blood vessels and improvement of vision when injected directly into the vitreous humour of the eye
• The injections have to be repeated on a monthly or bi-monthly basis Cataracts
• Clouding of the lens in the eye that affects vision • Most are related to aging; very common in older people • By age 80, more than half of all Americans either have a cataract or had cataract surgery • Although most cataracts are related to aging, there are other types of cataracts:
− Secondary cataracts: can form after surgery for other eye problems, such as glaucoma. Cataracts can also develop in people who have other health problems, such as diabetes, and is linked to steroid use.
− Traumatic cataract: develop after eye injury, sometimes years later − Congenital cataract: some babies are born with cataracts or develop them in childhood. These
cataracts may be so small that they do not affect vision − Radiation cataract: develop after exposure to some types of radiation
Lens structure and function The lens has 3 main parts:
I. Lens capsule − Outermost layer of the lens − A smooth, transparent basement membrane that completely surrounds the lens − Capsule is elastic and is composed of collagen − Synthesised by the lens epithelium and its main components are Type IV collagen and sulphated
glycosaminoglycans (GAGs) − The capsule is very elastic, which causes the lens to assume a more globular shape when not
under tension of the zonular fibres

MMED3937 Pathophysiology for Medical Science
79
II. Lens epithelium − Located in the anterior portion of the lens between the lens capsule and the lens fibres − Composed of simple cuboidal epithelium − The cells regulate most of the homeostatic functions of the lens − Ions, nutrients and liquid enter the lens from the aqueous humour − Na+/K+ ATPase pumps ions our of the lens to maintain appropriate lens osmolality and volume − Cells of the lens epithelium also serve as progenitors for new lens fibres
III. Lens fibres
− Form the bulk of the lens − Are long, thin, transparent cells, firmly packed with diameters typically between 4 -7 micrometres
and lengths up to 12 mm long − Stretch lengthwise from the posterior to the anterior poles − When cut horizontally, are arranged in concentric layers, like the layers of an onion − If cut along the equator, it appears as a honeycomb − Mature lens fibres have no organelles or nuclei – to maintain transparency of lens
Crystallins and transparency
• Crystallins – water soluble proteins that compose over 90% of the protein within the lens • 3 main crystallin types are found in the human eye – alpha, beta and gamma crystallins • Crystallins tend to form soluble, high molecular weight aggregates that pack tightly in lens fibres,
thus increasing the index of refraction of the lens while maintaining its transparency • Beta and gamma crystallins are found primarily in the lens, while subunits of alpha-crystallins have
been isolated from other parts of the eye and body • Alpha crystallin proteins belong to a larger superfamily of molecular chaperone proteins • The chaperone function of alpha crystallins may also help maintain the lens proteins, which must last
a human his/her lifetime • Another important factor in maintaining the transparency of the lens is the absence of light-scattering
organelles within the mature lens fibres • Lens fibres also have a very extensive cytoskeleton that maintains the precise shape and packing of
the lens fibres; disruptions/mutations in certain cytoskeletal elements can lead to the loss of transparency
Cataract histology • The hallmark of cortical cataract is
globular degeneration • The process starts with alterations
in cellular morphology with swelling and aggregation of proteins
• The lens cell membrane eventually break down, releasing globules (1)
• Morgagnian globules consist of eosinophillic collection of proteins (aggregates of crystallins) of various sizes that have lost cell membranes
• Silts that appear as a result of cortical cataracts (2) usually contain eosinophillic material
• This distinguishes cataracts from artifactual separation of fibres during sectioning
• As slits coalesce to form large clefts, the cataract manifests spoke-like or wedge shaped opacities

MMED3937 Pathophysiology for Medical Science
80
Posterior pole (subcapsular) cataract • Normally, the posterior capsule of the lens is
devoid of epithelium • The presence of nucleated lens epithelial
cells (3) anterior to the posterior capsule (4) is the key histologic criterion for posterior subcapsular cataract
• Posterior subcapsular cataract begins with presumed proliferation and posterior migration of epithelial cells from the lens bow
• These cells, known as bladder or Wedl cells may enlarge five or six fold. However, they do not always appear swollen in sections
• Treatment: surgical removal of the cataract generally restores vision
• In children medicated with steroids, posterior subcapsular cataract may be abated when the steroids are stopped
Risk factors for cataracts
• Age: the risk of cataract increases with age • Long term exposure to UV light • Secondary effects of diseases such as diabetes and HTN • Trauma • Genetic factors • Exposure to ionising radiation
Mechanisms of vision impairment in age-related cataracts 2 main mechanisms:
I. Protein aggregation reduce the sharpness of the image reaching the retina • When lens proteins aggregate, it clouds the lens and reduces the light that reaches the retina • This clouding may become severe enough to cause blurred vision • Most age-related cataracts develop from protein aggregation • When a cataract is small, the cloudiness affects only a small part of the lens, the patient may not
notice any changes in vision • Cataracts tend to ‘grow’ slowly, so vision gets worse gradually
II. Lens discolouration
• The clear lens slowly adopts a yellowish/brownish colour, gradually adding a brownish tint to vision
• Over time, increased tinting may make it more difficult to read and perform other routine activities
• This gradual change in the amount of tinting does not affect the sharpness of the image transmitted to the retina
Common symptoms of a cataract
• Cloudy or blurred vision • Colours seem faded • Brownish/yellowish tint in vision • Glare – headlights, lamps or sunlight may appear too bright, a halo may appear around lights • Poor night vision • Double vision or multiple images in one eye (may clear as the cataracts gets larger) • Frequent prescription changes in glasses or contact lens