advanced&metastatic breast cancer
TRANSCRIPT

BREAST CANCERLOCALLY ADVANCED AND METASTATIC DISEASE
Prepared by Mahran Alnahmi Supervisor Prof.Dr. Abbas Omar

INTRODUCTION
Breast cancer, the second-leading cause of cancer deaths in women, is the disease women fear most.
Breast cancer can also occur in men, but it's far less common.
Yet there's more reason for optimism than ever before.

Most common Cancer in women in developed countries. The lifetime risk (upto age 85)
1940 - 5% ---- ----one in 20.
2000- 12.6% -------- one in 8
Incidence worldwide incidence 1.2 million(WHO) Death – 2nd leading cause of cancer death. 40,000 in US per
year, worldwide much higher
STATISTICS

Hereditary (10% of pts have 1st deg relatives)Genetic mutations- BRCA 1, 2Radiation- esp. during childhood- mantle RT upto 20%
incidence by 50 y.Benign disease- proliferative, with atypiaPrevious h/o breast caDiet- obesity; dietary fat, anti-ox.- inconclusive. Hormonal factors- increased risk with excess exposure to
estrogens; Progesterone containing OCPs
ETIOLOGY

RISK FACTOR MODELS
Gail model: ( www.nci.nih.gov )Uses the following criteria:-current age-age at menarche-age at first child birth-no. of first degree relatives with breast ca-no. of previous benign biopsies-atypical hyperplasia in a prev. biopsy-race

PATHOLOGY
In-situ Carcinomas- DCIS, LCIS; Paget’s disease of nipple
Invasive Cas-Invasive Ductal Ca (80%)Invasive lobular Ca (10%)
Other invasive Cas- Medullary, papillary, tubular, cribriform, metaplastic, squamous, adenoid cystic, mucinous, secretory, undifferentiated.

“Intrinsic” breast cancer subtypes
Basal-like ER- PR- HER2- ck5/6+ and /or HER1+
Luminal A ER+ and/or PR+ HER2-
Luminal B ER+ and/or PR+ HER2+
HER2+ / ER – ER- PR- HER2+
“Unclassified” Negative for all five markers

SPREAD OF BREAST CANCER

Direct invasion- into chest muscles, wall, skin/nipple-areola.
Lymphatic- Locoregional - axilla, supraclavicular, infraclavicular and Internal mammary
Blood- Bones, lungs, liver, brain– Distant metastasis- stage IV
MODES OF SPREAD

Local- Lump, discharge, skin/nipple changes, axillary, arm swelling, ulcer ,Pain, tenderness- Inflammatory Ca
Distant- back ache, cough, breathlessness, headache, vomiting, anorexia, etc.
O/E – lump-hard, irregular , nipple retraction, peau de orange/puckering.
Nipple discharge, axillary nodes
CLINICAL SYMPTOMS-

History and physical Examination.Mammography.FNAC/biopsy of the lump/gland- histology and
receptor status studiesHer 2 /neu, prognostic indicator studiesEvaluation- CBC, RFT, LFT, ALP, S. Ca++, Cardiac
evaluation, Metastatic work up- CXR, USG A+P, Bone scan, ?
PET. CT thorax, brain- only if symptoms suggestive.
DIAGNOSIS

American Joint Committee on Cancer Staging System for Breast Cancer(p)T (Primary Tumor) Tis Carcinoma in situ (lobular or ductal) T1 Tumor ≤2 cm T1a Tumor ≥0.1 cm, ≤0.5 cm T1b Tumor >0.5 cm, ≤1 cm T1c Tumor >1 cm, ≤2 cm T2 Tumor >2 cm, ≤5 cm T3 Tumor >5 cm T4 Tumor any size with extension to the chest wall or skin T4a Tumor extending to the chest wall (excluding the pectoralis) T4b Tumor extending to the skin with ulceration, edema,nodules T4c Both T4a and T4b T4d Inflammatory carcinoma

N0 No regional node involvement, no special studies N0 (i-) No regional node involvement, negative IHC N0 (i+) Node(s) with isolated tumor cells spanning <0.2 mm
N0 (mol-) Negative node(s) histologically, negative PCR N0 (mol+) Negative node(s) histologically, positive PCR N1 Metastasis to 1-3 axillary nodes and/or int.
mammary positive by biopsy N1(mic) Micrometastasis (>0.2 mm, none >2.0 mm) N1a Metastasis to 1-3 axillary nodes N1b Metastasis in int. mammary by sentinel biopsy N1c Metastasis to 1-3 axillary nodes and int. mammary
by biopsy
(P)N (NODES)

N2 Metastasis to 4-9 axillary nodes or int. mammary clinically positive, without axillary metastasis
N2a Metastasis to 4-9 axillary nodes, at least 1 >2.0 mm N2b Int. mammary clinically apparent, negative axillary nodes N3 Metastasis to ≥10 axillary nodes or combination of axillary and int. mammary metastasis N3a ≥10 axillary nodes (>2.0 mm), or infraclavicular nodes N3b Positive int. mammary clinically with ≥1 axillary nodes or
>3 positive axillary nodes with int. mammary positive by biopsy N3c Metastasis to ipsilateral supraclavicular nodes

M (Metastasis)
M0 No distant metastasis M1 Distant metastasis

Tumor size less than 2 cm
STAGE 1
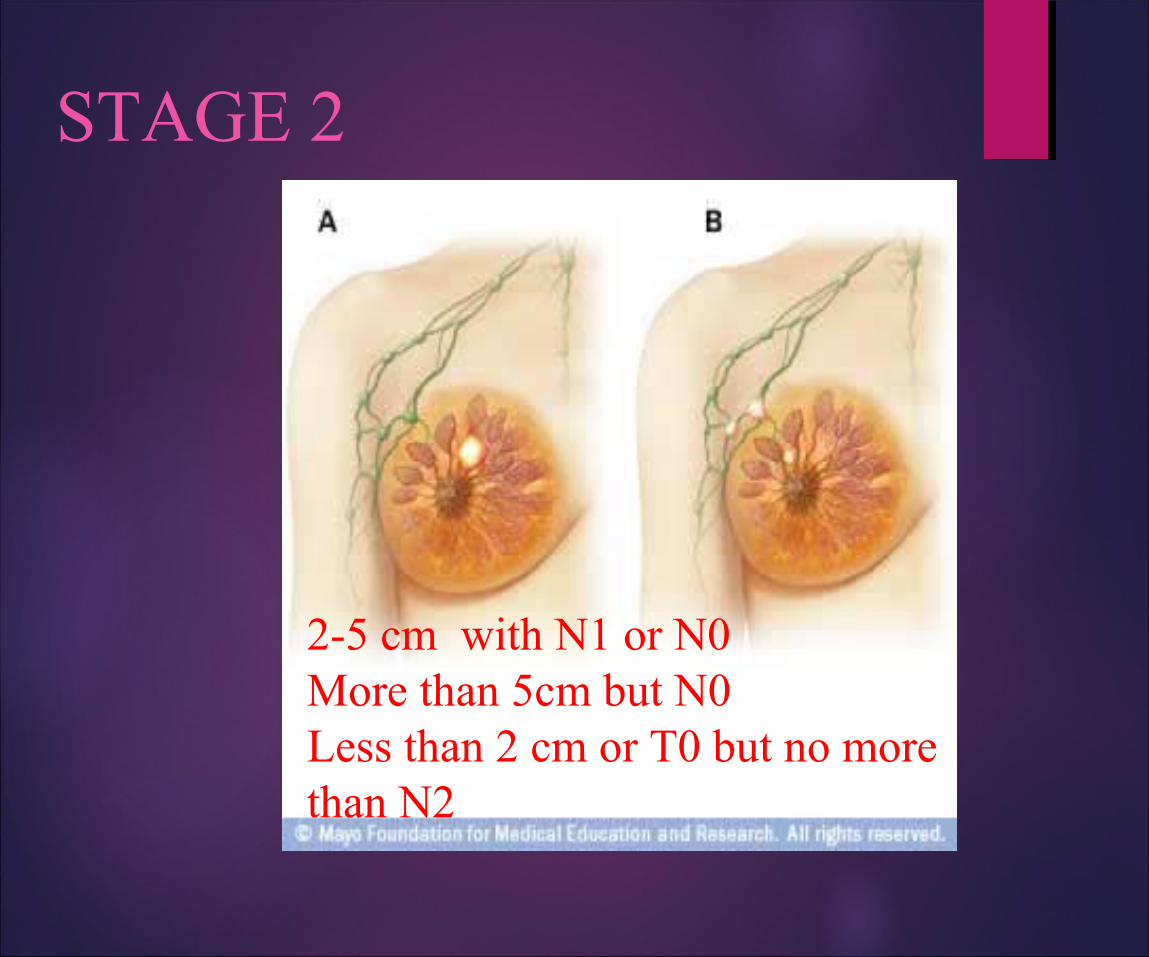
2-5 cm with N1 or N0More than 5cm but N0Less than 2 cm or T0 but no more than N2
STAGE 2

Larger than 5 cm with any NLess than 5 cm with nodal mattingLess than 5 cm with supraclavicular LN involvement
Stage 3

Inflammatory breast
STAGE 3

Metastatic breast cancer
STAGE 4

BREAST CANCER
Locally Advanced And Metastatic Disease

Locally Advanced and Metastatic Breast Cancer
Overview:Principles of neoadjuvant chemotherapy for locally
advanced and inflammatory breast cancerSystemic therapy of metastatic breast cancer
ChemotherapyHormonal agentsBiologic agentsBisphosphonates
Rationale for selection of treatment in metastatic diseasechemotherapy vs. hormonal agentsIdeal first line agents?
Locally Advanced Breast Cancer
Definition: breast cancer, without distant metastatic spread, which is unresectable due to
Satellite skin nodulesExtensive regional lymph node involvementFixation to skin or chest wall Inflammatory breast cancer


Locally Advanced Breast Cancer
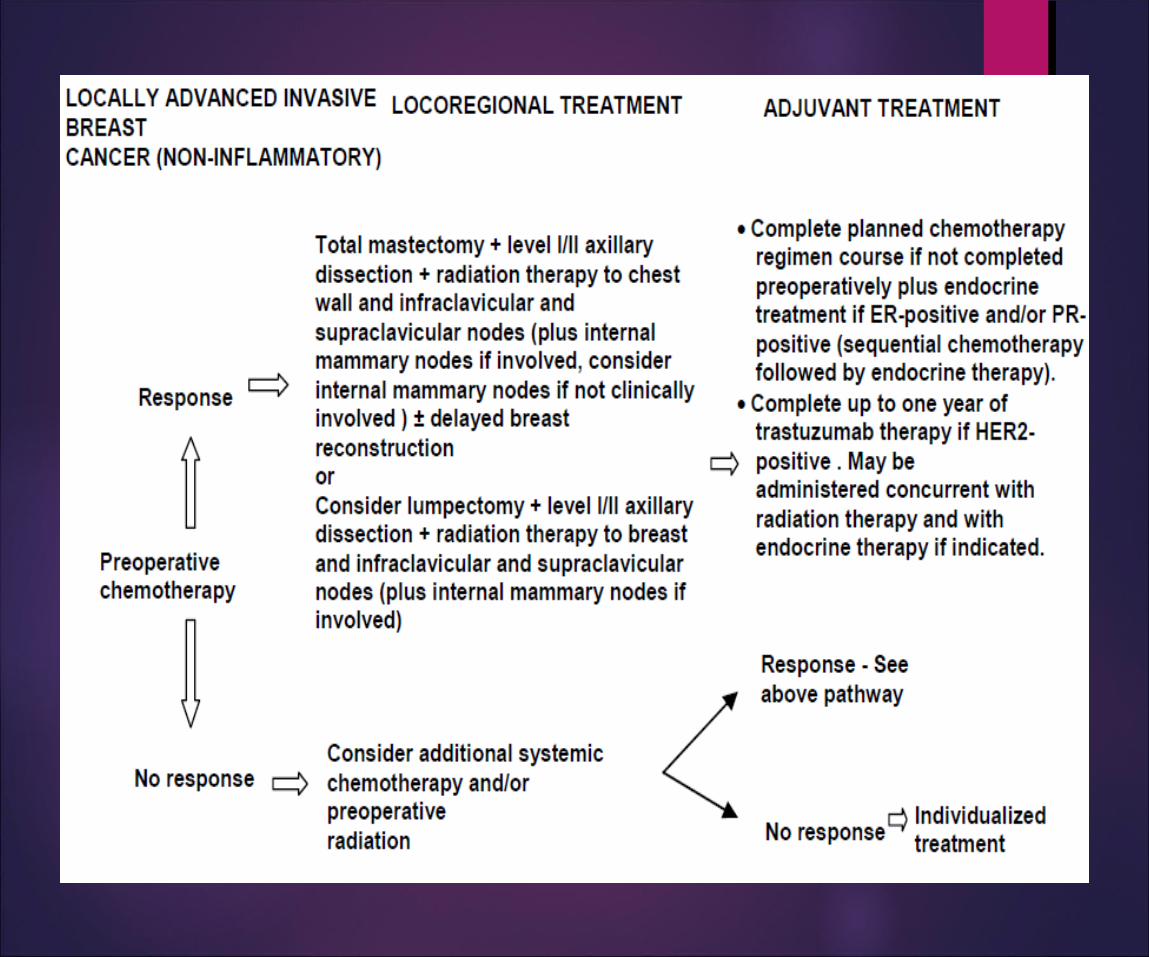
Combined modality treatment is the standard of care for locally advanced breast cancer.Neoadjuvant chemotherapy
Goals are to improve resectability of the tumour and to increase rates of breast conserving treatment and establish tumor sensitivity
Locoregional therapySurgery, or radiotherapy, or both.
Locally Advanced Breast Cancer
Response rates to neoadjuvant chemotherapy:
Major responders: 47-100%Clinical complete responders: 8-63%Pathologic complete responders: 3-30%
A major response to chemotherapy is associated with improved disease-free and overall survival.

Locally Advanced Breast Cancer
Survival is related to axillary lymph node status after neoadjuvant chemotherapy.
Positive nodes 5-year overall survival0 75%
1-4 40-50%
5-10 30%
>10 20%

Locally Advanced Breast Cancer
Survival is related to response of primary tumour to neoadjuvant chemotherapy.
Author Median follow-up, years
Survival, patients with complete response
Survival, patients with partial response
Method of response assessment
Eltahir, 1998
5 74% overall survival
36% overall survival
Clinical response
Kuerer, 1999
5 89% overall survival
64% overall survival
Pathologic response
Bonnadonna,1998
8 86% disease-free survival
56% disease-free survival
Clinical response

Locally Advanced Breast Cancer
Duration of neoadjuvant chemotherapy
Optimal duration of treatment is not known.Rule of thumb: “treat until maximal response.”May require from 2-8 treatments, depending on
rapidity of response.Patients should be assessed by multidisciplinary
team after every 2 cycles of chemotherapy to determine optimal timing of surgery.

DEFINITIONS FOR RESPONSE EVALUATION OF PRIMARY SYSTEMIC THERAPY
CLINICAL DEFINITION
Complete: no palpable mass detectable (cCR)
Partial: reduction of tumour area to < 50% (cPR)
IMAGING DEFINITION
No tumour visible by mammogram and/or ultrasound and/or MRI
PATHOLOGICAL DEFINITION
Only focal invasive tumour residuals in the removed breast tissue
Only in situ tumour residuals in the removed breast tissue (pCR inv)
No invasive or in situ tumour cells (pCR)
No malignant tumour cells in breast and lymph nodes (pCR breast and nodes).

Locally Advanced Breast Cancer
Ideal neoadjuvant chemotherapy regimen has not been identified.
Anthracycline based (epirubicin or adriamycin) chemotherapy is often used at start (AC, CAF, FEC).
Taxanes (taxol, taxotere) are also extremely effective and have been shown to increase the rate of pathologic complete responses.

Locally Advanced Breast Cancer
Impact of Taxanes in NeoadjuvantChemotherapy.TAX-301 trial
162 patients, randomly assigned to pre-operative CAVP X 8 cycles vs CAVP x 4 then Taxotere X4
5 year overall survival:CAVP X 8: 78%CAVP X 4 + Taxotere X 4: 97%

Role Of Docetaxel In Neo-adjuvant Therapy For Breast Cancer

Neoadjuvant Taxotere
The Aberdeen TrialNSABP B27GEPARDUO

4 cycles of Taxotere
4 cycles of CVAP
No Response
Response
Ra nd om
i se
All Patients
4 cycles of CVAP
First Phase
Tax301 StudyConducted by the Aberdeen Breast Group
Second phase
4 cycles of Taxotere
Final A
s sessment / S
u rgery

Aberdeen Tax 301Objective clinical response rates
1st phase: 4 cycles CVAP
Response % of patients
Complete 15
Partial 52
Stasis 33
Progression 1
ORR - 67%
N=162 patients; 4 cycles of CVAP given to all patients

Aberdeen Tax301Objective clinical response rates2nd phase: responding patients
CVAP n=52
Taxotere n=52
Response % %
Complete 33 56
Additional partial 31 29
Maintained partial 29 6
Progression 4 0
ORR 64 85*
* p=0.03

Aberdeen Tax 301Objective clinical response rates
2nd phase: non-responding patients
Response % of patients
Complete 11
Partial 36
Stasis 31
Progression 9
ORR - 47%N=55 patients; additional 4 cycles of Taxotere given

Aberdeen Tax301 Aberdeen Tax301
Type of surgeryType of surgery undertaken
Breast conservation surgeryTaxotere 67%
CVAP 48%
Conservation Mastectomy0
20
40
60
80
100 Taxotere
CVAP
Type of surgery
% o
f pat
ient
s
(p<0.01)

Tax 301 Overall Survival
Time (months)
Median Follow - up: 60 months
Surv
ival
pro
babi
lity
1.0
0.9
0.8
0.720 40 60 80 100
Log rank p=0.04
TaxotereCVAP
97%
78%

Neoadjuvant Taxotere
The Aberdeen TrialNSABP B27
GEPAR-DUO

NSABP B-27
Operable Breast CancerOperable Breast Cancer
RandomizationRandomization
AC x 4 AC x 4 Tam X 5 YrsTam X 5 Yrs
AC x 4 AC x 4 Tam X 5 YrsTam X 5 Yrs
AC x 4 AC x 4 Tam X 5 YrsTam X 5 Yrs
SurgerySurgery Taxotere x 4Taxotere x 4 SurgerySurgery
SurgerySurgery Taxotere x 4Taxotere x 4
( 2411 pts )

40%
45%
100100
8080
6060
4040
2020
00
%%
p < 0.001p < 0.001
ACACN=1502N=1502
AC Taxotere AC Taxotere N=687N=687
65%
26%
NSABP B-27 Clinical ResponseNSABP B-27 Clinical Response
cCRcCRcPRcPRcNRcNR
14% 9%
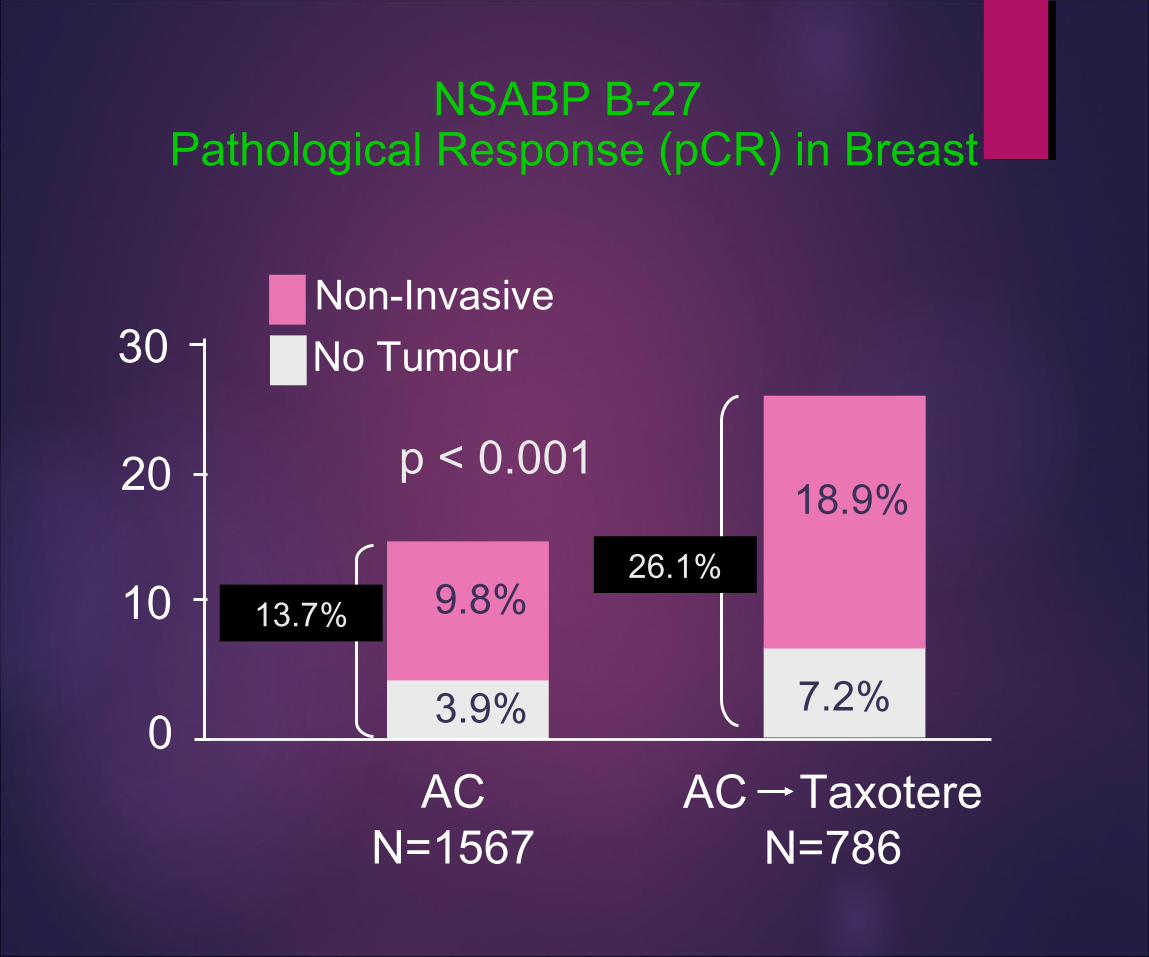
NSABP B-27 Pathological Response (pCR) in Breast
p < 0.001
AC TaxotereN=786
ACN=1567
3.9%
9.8%
7.2%
18.9%20
10
0
30 No TumourNon-Invasive
26.1%13.7%
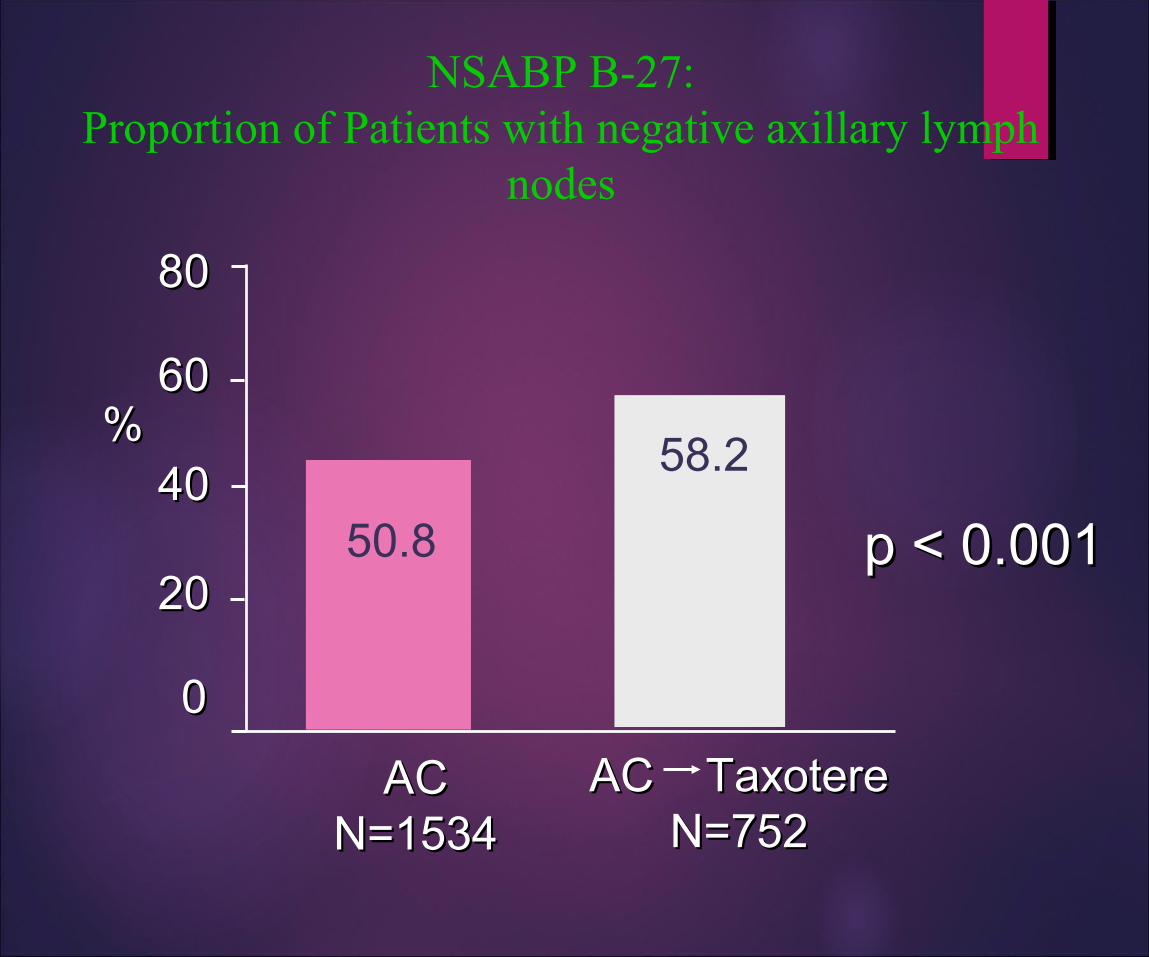
NSABP B-27:Proportion of Patients with negative axillary lymph
nodes
58.2
p < 0.001p < 0.001
ACACN=1534N=1534
AC TaxotereAC TaxotereN=752N=752
8080
6060
4040
2020
00
%%
50.8

NSABP B-27: Breast Conservation: Breast Conservation
p = 0.7061 63
8080
6060
4040
2020
00
%%
ACAC(N=1492)(N=1492)
AC TaxotereAC TaxotereN=718N=718

LOCALLY ADVANCED BREAST CANCER
Role of Herceptin (trastuzumab):Initial reports are encouraging, but use of herceptin cannot be
recommended outside of a clinical trial.
Role of High-dose chemotherapy with stem cell support:No improvement in DFS or OS, with significant increase in
toxicity and worsening of quality of life, therefore not recommended.

LOCALLY ADVANCED BREAST CANCER
Hormonal Management Acceptable in Estrogen Receptor and/or
Progesterone Receptor positive cancers.Best used in patients where chemotherapy is
relatively contraindicatedElderly
Poor performance status
Comorbid illness
Patient reluctance to accept chemotherapy

LOCALLY ADVANCED BREAST CANCER
Hormonal Management, continued:Rate of pathologic complete response is greatly
diminished.Rate of breast-conserving treatment is greatly
diminished.Response to treatment is much slower, e.g. 3-9
months.

Multidisciplinary Cancer Breast Management

Multidisciplinary Cancer Breast Management

Multidisciplinary Cancer Breast Management

Multidisciplinary Cancer Breast Management
Trials of Neoadjuvant Trastuzumab:Summary of Efficacy
•Preoperative clinical responses observed
– Overall response rate, 70% to 90%– Clinical complete response, 15% to 30%– Pathologic complete response, approximately 18%
•Responses higher for patients with 3+ expression of HER2

The relative efficacy of neoadjuvant endocrine therapy versus chemotherapy in postmenopausal
women with ER positive breast cancer
Methods: 121 postmenopausal women with ER(+) and/or PgR(+) breast cancer T2N1–2, T3N0–1, T4N0M0 assigned to NAT with either CT Dox 60 mg/m2 + Pac 200 mg/m2, every 3 weeks, 4 cycles, n=62 patients (pts), or HT with aromatase inhibitors, anastrazole 1 mg, n = 30 pts, 3 months).
In CT arm the most frequent grade III/IV toxicity was alopecia ( 79.3 % ), neutropenia ( 43.1 %), cardiotoxicity (6.8 %), diarrhea (1.7%). HT was well tolerated. The most commonly adverse events were hot flushes (23.3%), vaginal discharge (6.6%), musculosskeletal disorders (1.7%).
Note this does not give the pathologic CR rate.

Multidisciplinary Cancer Breast Management

Multidisciplinary Cancer Breast Management

Multidisciplinary Cancer Breast Management

Letrozole Is More Effective Neoadjuvant Endocrine Therapy Than Tamoxifen for ErbB-1– and/orErbB-2–Positive, Estrogen Receptor–Positive Primary Breast Cancer: Evidence From a Phase III

LOCALLY ADVANCED BREAST CANCER
Summary:Standard of care is multimodality treatment.
Chemotherapy: should contain anthracyclines and/or taxanes and should begin before surgery.
Locoregional therapy: should be performed when a maximal tumour response has been obtained.
Post-operative chemotherapy: should be performed if less than 8 cycles were given pre-operatively, until a total of 8 cycles of chemotherapy have been given.
Hormonal management: is a slower option, and is restricted to ER and/or PR positive tumours.

METASTATIC BREAST CANCER
Goals of treatment of metastatic breast cancer:Cure: not a realistic goal
Few patients have complete responses, and disease free intervals are short.
Prolongation of survival:5-10% of patients will survive 5 years or more.
2-5% of patients are long-term survivors (>10 years).
Improvement of Quality of Life:Most patients experience fewer disease symptoms, with
manageable treatment side effects.

METASTATIC BREAST CANCER
Numerous treatment options exist:
Chemotherapy: anthracyclines, taxanes, vinorelbine, capecitabine
Hormonal therapies: tamoxifen (Nolvadex), anastrozole (Arimidex), letrozole (Femara), exemestane (Aromasin), megestrol acetate (Megace)
Biologic agents: trastuzumab (herceptin)
Bisphosphonates: pamidronate, zolendronate

METASTATIC BREAST CANCER
Different options can be combined.
Herceptin and chemotherapy.
Hormonal agents and bisphosphonates.
Herceptin, chemotherapy and bisphosphonates.

METASTATIC BREAST CANCER
How is initial therapy selected?
Patient factors: age, comorbid conditions, willingness to accept side effects.
Tumour factors: ER, PR, her-2/neu status.Course of illness: extent and location of metastases,
disease-free interval, pace of spread of metastases.Treatment factors: adjuvant chemotherapy, adjuvant
hormonal agents, adjuvant radiotherapy.

METASTATIC BREAST CANCER
The use of hormonal agents is favoured if:
Tumour is ER and/or PR positive.Disease-free interval is long.Few sites of metastases.Metastases do not involve visceral organs. Pace of disease progression is slow.Patient has responded to previous hormonal agents.

METASTATIC BREAST CANCER
Use of hormonal agents, continued
Hormonal agents require 8-12 weeks to determine their efficacy, thus they are not recommended for patients with extensive visceral metastases.
Initial response to hormonal agents is 50-60% in ER/PR positive patients.

METASTATIC BREAST CANCER
The use of chemotherapy is favoured if:Tumour is negative for ER and PR.Disease-free interval is short.Extensive metastases are present, especially visceral
disease (liver, lung).Disease is progressing rapidly.Patient has not responded to previous hormonal
agents.
Initial response to chemotherapy is 50-75%.No clear advantage of combination regimens over
use of sequential single agents.

METASTATIC BREAST CANCER
Hormonal agents:Tamoxifen:
Mixed estrogen receptor agonist-antagonist.Can be used in premenopausal and postmenopausal
women.Response rates are 50-60%.Duration of response may be years.Toxicities: hot flashes, increased risks of DVT/
pulmonary embolism, endometrial cancerMay be associated with tumour reluctance in up to
13% of patients.

METASTATIC BREAST CANCER
Hormonal agents, continued:Aromatase inhibitors:
Anastrozole (Arimidex), non-steroidal
Letrozole (Femara), non-steroidal
Exemestane (Aromasin), steroidal
Method of action: block conversion of adrenal androgens to estrogen in adipose tissue and in the breast.
Use is restricted to postmenopausal women.
Side effects: hot flashes, myalgias/arthralgias, increased risk of osteoporosis, altered lipid profiles.

METASTATIC BREAST CANCER
Hormonal agents, continued:
Aromatase inhibitors: Anastrozole and Letrozole:
are non-steroidal aromatase inhibitors.
are both superior to Megace in tamoxifen refractory patients.
Have similar efficacy to tamoxifen, with fewer side effects.

METASTATIC BREAST CANCER
Hormonal agents, continued:
Aromatase inhibitors:Exemestane:
is a steroidal aromatase inhibitor.
is superior to Megace, and at least as effective as Tamoxifen.
can be effective in patients who have failed non-steroidal aromatase inhibitors.

METASTATIC BREAST CANCER
Hormonal agents, continued:Megace (megestrol acetate)
Is a progestinBefore aromatase inhibitors, was considered
second-line therapy, after tamoxifen.May still have activity in some patients who have
failed tamoxifen and/or aromatase inhibitors.Side effects: increased appetite, weight gain,
increased risk of DVT/pulmonary embolism.

Sequencing of Hormonal agents in metastatic breast cancer:Postmenopausal patients:
Anastrozole or Letrozole as first lineExemestane as second lineTamoxifen and Megace remain options for third line
OR for patients who do not tolerate aromatase inhibitors.
Premenopausal patients:Tamoxifen as first lineMegace OR aromatase inhibitor with ovarian
ablation as second line.
METASTATIC BREAST CANCER

Chemotherapy:Numerous agents have activity in metastatic
breast cancer:AnthracyclinesTaxanesFluoropyrimidinesVinca alkaloidsOther drugs: cyclophosphamide, methotrexate,
gemcitabine
METASTATIC BREAST CANCER

Anthracyclines doxorubicin (Adriamycin),epirubicin, mitoxantrone
liposomal-PEGylated doxorubicin (Doxil-Caelyx)
Are among the most active agents in breast cancer (response rate at least 50%)
METASTATIC BREAST CANCER

Taxanes Paclitaxel (Taxol) Docetaxel (Taxotere)
Nanoparticle albumin-bound paclitaxel (Abraxane)Are the single most active drugs in breast cancer
and the most active in adriamycin-refractory patients. (RR = 60%)
Common toxicities include peripheral neuropathy, myalgias, arthralgias and alopecia.
METASTATIC BREAST CANCER
Paclitaxel (taxol) can induce anaphylactoid reactions, requiring
premedication with steroids and antihistamines.Efficacy and toxicity profile can be improved by
weekly administration (as opposed to q3weeks).Docetaxel (taxotere)
Can induce responses in 25% of patients who are resistant to paclitaxel.
Cumulative toxicities include fluid retention, sclerosis of tear ducts, loss of fingernails/toenails.
METASTATIC BREAST CANCER

Nanoparticle albumin-bound paclitaxel (Abraxane)Novel formulation, does not require Cremophor.No risk of anaphylactoid reaction, thus no need for
steroids.Better tissue penetration.Less toxic and more effective than paclitaxel.Approved in the USA, not yet approved in Canada.
METASTATIC BREAST CANCER

Fluoropyrimidines:5-fluorouracil:
is commonly used in combinations, such as CMF, CAF, FEC.
Has activity as a single agent, esp. in prolonged infusions, but these regimens are not convenient.
Toxicities: mucositis (stomatitis, enteritis, colitis), hand-foot syndrome, some myelosuppression
METASTATIC BREAST CANCER

Fluoropyrimidines, cont’dCapecitabine (Xeloda)
Oral 5-FU derivative, given BID X14 days q21days.
Prodrug is activated to 5-FU in tumour cells, mimics a prolonged 5-FU infusion.
Has activity even in patients who are refractory to anthracyclines and taxanes!! (RR=25%)
Dose limiting toxicity is usually hand-foot syndrome.
NOT HEPATICALLY METABOLIZED, thus ideal agent in patients with severe liver dysfunction!
METASTATIC BREAST CANCER

Vinca alkaloids:Vinorelbine (Navelbine)
Semi-synthetic vinca alkaloid, related to VCR/VBLLess neurotoxicity, due to diminished binding to
axonal microtubules.Active even in heavily pretreated patients (response
rates = 25-50%).Excellent toxicity profile: no nausea, no alopecia,
no mucositisWell tolerated by elderly, frail patients
METASTATIC BREAST CANCER

Other drugs:CyclophosphamideMethotrexateGemcitabine
All have limited activity as single agents, but are useful in combinations with other active drugs
e.g. CMF, CAF, Gemcitabine-Taxol
METASTATIC BREAST CANCER

Biologic agentsHerceptin (trastuzumab)
Humanized mouse monoclonal antibody directed against the her-2/neu protein.
Has activity against breast cancers that strongly overexpress her-2/neu (score= 3+/3).
Has activity as a single agent, even in heavily pre-treated patients.
METASTATIC BREAST CANCER
Herceptin, cont’d
Can be safely administered with taxanes and vinorelbine, with increased response rates (compared to chemotherapy alone).
Cannot be given with adriamycin; response rates increase BUT rate of cardiomyopathy rises to 27%!!!
Patients on herceptin who have received anthracyclines in the past need monitoring for cardiac toxicity.
METASTATIC BREAST CANCER

Bisphosphonates:Pamidronate (Aredia)Zolendronate (Zometa)
Given monthly to patients with bone metastases.Leads to decreased risk of skeletal complications
(pain, fractures, need for radiotherapy)Few toxicities: fever and chills post-infusion,
muscle spasms (transient hypocalcemia)Rare cumulative toxicity: osteonecrosis of the
mandible (!)
METASTATIC BREAST CANCER
A rational approach to selecting therapy for patients with metastatic breast cancer:
For patients with bone metastases: monthly administration of Pamidronate or
Zolendronate (regardless of ER/PR/her-2 status)
For patients with ER and/or PR positive breast cancer, with low burden of metastases and slow pace of disease: start with hormonal agents.If patient was on a hormonal agent at time of relapse,
try to select a non cross-resistant agent.
METASTATIC BREAST CANCER

A rational approach to selecting therapy for patients with metastatic breast cancer:For patients with ER-negative/PR-negative disease
OR for patients with high tumour burden OR with rapid disease progression:
Start with chemotherapyIn anthracycline-naïve patients, use anthracyclines.In patients who had adjuvant anthracyclines, use
taxanes.
METASTATIC BREAST CANCER

A rational approach to selecting therapy for patients with metastatic breast cancer:For patients with ER-negative/PR-negative disease OR
for patients with high tumour burden OR with rapid
disease progression:2nd, 3rd, 4th lines of treatment depend on patient’s
previous side effects and current symptoms.
e.g. navelbine contraindicated in patient with abnormal liver function tests; capecitabine would be a safer choice.
METASTATIC BREAST CANCER

A rational approach to selecting therapy for patients with metastatic breast cancer:For patients with her-2/neu 3+ disease:
Herceptin should be given with taxane or vinorelbine chemotherapy.
Herceptin can be given as a single agent even in heavily pre-treated patients.
Herceptin as a single agent can be given as “maintenance” therapy after “inducing” a major reduction in tumour burden with herceptin-chemo combination.
METASTATIC BREAST CANCER

Hormone receptorpositive
Triple-negative
HER2-Positive
*Note, these are just examples. Each patient is different and treatment is tailored accordingly.
Treatment

HER2+ disease: a paradigm for advances in
targeted therapy
Lapatinib
Oral dual tyrosine kinase inhibitor of HER2 and EGFR
FDA approved in combination with capecitabine for trastuzumab-resistant disease
May have CNS penetration
Well tolerated; common toxicities include rash and diarrhea

Pertuzumab with trastuzumab
HER2 receptor
Trastuzumab
Pertuzumab
Dimerisation domain of HER2
• Inhibitor of HER dimerization: binds HER2 and prevents formation of homo- or heterodimers• Suppresses activation of several intracellular signaling cascades driving cancer cell growth• Synergistic with trastuzumab• Approved for first-line treatment of metastatic Her2+ breast cancer in combination with trastuzumab
and taxane chemotherapy

CLEOPATRA: phase 3 study of pertuzumab in untreated metastatic disease
1:1 HER2-positive
MBC
Docetaxel + trastuzumab + placebo
Docetaxel + trastuzumab + pertuzumab
N=808
Pertuzumab prolongs time until progression by six months (from 12.5 to 18.5 months)

Trastuzumab Emtansine (T-DM1)
T-DM1 is an antibody drug-conjugate
Trastuzumab linked to a potent chemotherapy (DM1)
Average of 3.5 DM1 per antibody

T-DM1 selectively delivers DM1 to HER2+ cells
Receptor-T-DM1 complex is internalized into HER2-positive cancer cell
Potent antimicrotubule agent is released once inside the HER2-positivetumor cell
T-DM1 binds to the HER2 protein on cancer cells
HER2

EMILIA: randomized trial comparing T-DM1 to capecitabine and lapatinib in
previously treated patients
1:1 HER2+ MBC (N=980)
•Prior taxane and trastuzumab
PDT-DM1 3.6 mg/kg q3w IV
Capecitabine 1000 mg/m2 orally bid, days 1–14, q3w
+ Lapatinib
1250 mg/day orally qd
PD
T-DM1 prolongs time until progression by three months (from 6.4 to 9.6 months)
RESULTE

Th3RESA: randomized trial comparing T-DM1 to physician’s choice
Study treatment continues until disease
progression or unmanageable toxicity
HER2 positive
Metastatic breast cancer
Prior trastuzumab, lapatinib and chemotherapy
T-DM1 q3w
Treatment of physician’s choice
N = 7952:1 randomization
2
1
T-DM1 prolongs time until progression by three months (from 3.3 to 6.2 months)

T-DM1 is well-tolerated
Common side effects:Decreased platelet countElevated liver tests
Does not cause typical chemotherapy side effectsNo hair loss
Significant nausea or diarrhea are not common
Does not cause immune suppression or significant neuropathy

ER+ disease: improving on already very effective
treatments

Endocrine therapy for metastatic disease
PremenopausalTamoxifenOvarian
suppression/ablationOvarian suppression +
aromatase inhibitionMegace
PostmenopausalTamoxifenAromatase Inhibitor +/-
everolimusFulvestrantMegace

New drug approval: everolimus
Approved by the FDA in 2012 for patients with metastatic, hormone-receptor positive, HER2-negative breast cancer
*Median time from study entry until worsening of cancer
What’s next for everolimus?
Multiple studies underwayIn HER2+ cancersIn triple negative cancersStudying this drug in combination with other
therapies

Testing the addition of an HSP90 inhibitor to hormonal therapy

Other agents of interest in ER+ disease
Endoxifen CDK 4/6 inhibitorsPI3Kinase inhibitorsAnti-IGF-1R AbSRC/Abl tyrosine kinase inhibitorsCombination therapy with targeted agents that may
overcome endocrine resistance

Triple negative breast cancer:still searching for a target

There are many chemotherapies that are active against metastatic disease
Mitotic inhibitors
vinorelbine
paclitaxel
docetaxel
Antifolatesmethotrexate
Topoisomerase inhibitorsdoxorubicin

Platinums
Sledge reported 47% response rate in first line metastatic disease
Abandoned for many years because of concerns about toxicity—largely replaced by taxanes
Recent interest in patients with triple negative breast cancer
DNA crosslinking mechanism of action
New data from a series of neoadjuvant studies supports activity in TNBC

New chemotherapy: eribulin
Halichondria okadai•Metastatic breast cancer•At least 2 prior chemotherapies

PARP inhibitors
PARP1 is a protein that is important for repairing single-strand DNA breaks
PARP inhibitors prevent DNA repair, leading to cell death
Fast-dividing tumors and tumors containing BRCA mutations, which also impair DNA repair, may be most sensitive to PARP inhibitors
Ongoing trials are investigating the efficacy of PARP inhibitors in breast cancer, particularly triple negative breast cancer and BRCA-associated breast cancer

Inhibit binding to receptor (AR)
T
AR
T
Cell nucleus AR
Cell cytoplasm
Inhibit nuclear translocation of AR
Inhibit AR-mediated DNA binding
Targeting the androgen receptor intriple negative breast cancer

Other agents of interest in triple negative disease
PI3Kinase inhibitorsSRC/Abl tyrosine kinase inhibitorsHSP90 inhibitorsMore to come…