adult medicine prn focus session—update on anticoagulant ... · 1:15 p.m. secondary stroke...
TRANSCRIPT

Annual Meeting
Adult Medicine PRN Focus Session—Update on Anticoagulant Use in Stroke Patients Activity No. 0217-0000-11-095-L01-P (Knowledge-Based Activity) Tuesday, October 18 1:15 p.m.–3:15 p.m. Convention Center: Rooms 317 & 318 Moderator: Nancy Yunker, Pharm.D., BCPS Assistant Professor of Pharmacy, Clinical Specialist, Internal Medicine, Virginia Commonwealth University, Richmond, Virginia Agenda 1:15 p.m. Secondary Stroke Prevention: What’s New? A Review of
Secondary Stroke Prevention Guidelines and the Evidence that Supports the Drug Therapy Susan C. Fagan, Pharm.D., FCCP, BCPS Jowdy Professor, Associate Head, Assistant Dean, University of Georgia College of Pharmacy, Augusta, Georgia
2:05 p.m. When Is a New Medication Better than the Tried and True? Use of Dabigatran in Atrial Fibrillation for Stroke Prevention Asha L. Tata, Pharm.D., BCPS Internal Medicine Clinical Specialist; Clinical Assistant Professor, University of Maryland School of Pharmacy, University of Maryland Medical Center Department of Pharmacy Services, Baltimore, Maryland
2:35 p.m. Quality Initiatives of Anticoagulation Safety: Attacking the Coagulation Cascade, Safely William E. Dager, Pharm.D., FCCP, BCPS Pharmacist Specialist, Department of Pharmaceutical Services, University of California Davis Medical Center, Sacramento, California
3:05 p.m. Panel Discussion William E. Dager, Pharm.D., FCCP, BCPS Susan C. Fagan, Pharm.D., FCCP, BCPS Asha L. Tata, Pharm.D., BCPS
Faculty Conflict of Interest Disclosures William E. Dager: no conflicts to disclose. Susan C. Fagan: serves as a consultant/member of advisory board for Pfizer, Inc, and Genentech, Inc. Asha L. Tata: no conflicts to disclose.
Update on Anticoagulant Use in Stroke Patients 1
Annual Meeting
Learning Objectives
1. Discuss the changes to the 2010 secondary prevention stroke guidelines. 2. Examine the literature supporting these changes. 3. Evaluate recommendations for stroke prevention in specific disease states/conditions. 4. Compare and contrast the pharmacology of dabigatran versus warfarin. 5. Summarize efficacy, safety, and pharmacoeconomic data for dabigatran. 6. Describe the role of therapy for dabigatran in the treatment of atrial fibrillation. 7. Improve medication management in secondary stroke prevention and in patient with atrial
fibrillation. 8. Describe the pharmacist’s role in enhancing anticoagulation safety in the hospital. 9. Provide dosing guidelines or protocols for the management of antithrombotic therapy.
Self-Assessment Questions Self-assessment questions are available online at www.accp.com/am
Update on Anticoagulant Use in Stroke Patients 2
Secondary Stroke Prevention: What’s New?
Susan C. Fagan, Pharm.D., FCCP
Jowdy Professor / Associate Head / Assistant Dean
University of Georgia
Conflicts of Interest
Dr. Fagan is a consultant for Pfizer, Inc and Genentech, Inc.Dr. Fagan receives research funding from NINDS and VA Merit Review
Objectives
Discuss changes in Acute Stroke Treatment and the 2010 Secondary Stroke Prevention Guidelines.
Examine the literature supporting these Examine the literature supporting these changes.
Make recommendations for stroke prevention in specific disease states/ conditions.
Stroke Facts
795,000 strokes per year in U.S.
Every 40 seconds, someone in the US has a stroke
87% ischemic
Blacks and Mexican Americans have higher stroke incidence than whites.
More women than men die of stroke each year
Heart Disease and Stroke Statistics – 2010 Update, American Heart Association
Self Assessment Question
What is the NEW treatment window for use of intravenous tPA in ischemic stroke?
a. < 3 hours
b < 6 hoursb. < 6 hours
c. < 4.5 hours
d. < 3.5 hours
The Story of tPA: Bench to Bedside in Record Time (7 years!)
1979: Purification of tPA from Bowes melanoma cell line 1981: Renal allograft patients treated with melanoma tPA 1982: Cloning of tPA and expression in mammalian line
(CHO) by Diane Pennica PhD at Genentech(CHO) by Diane Pennica, PhD, at Genentech 1983: Acute MI patients treated with melanoma tPA 1984: First patient treated with FDA-approved tPA (CHO) 1980s: Large clinical trials in acute MI patients 1987: FDA approval of tPA for acute MI 1996: FDA approval of tPA for acute ischemic stroke
tPA, tissue plasminogen activator; CHO, Chinese hamster ovary; MI, myocardial infarction.Collen D, Lijnen HR. Arterioscler Thromb Vasc Biol. 2009;29:1151-1155.
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 3

The One FDA-Approved Drug (1996): Tissue Plasminogen Activator (tPA)
3-hour window (FDA label)
Only 2% to 4% of patients with ischemic stroke receive it
Leads to recanalization in only about 50% of patients
Can the Time Window for tPAbe Extended Beyond 3 Hrs?
OR, odds ratio; CI, confidence interval.Bernstein R, Futterer S. Lancet. 2004;363:368-374.
ECASS III(3.0 to 4.5–hour window)
Inclusion Criteria• Acute ischemic stroke• Age: 18 to 80 years• 3.0 to 4.5 hours• Stroke symptoms present for 30 minutes
ECASS, European Cooperative Acute Stroke Study.Hacke W et al. N Engl J Med. 2008;359:1317-1329.
ECASS III ICH
ICH, intracranial hemorrhage; SITS-MOST, Safe Implementation of Thrombolysis in Stroke-Monitoring Study; NINDS, National Institute of Neurological Disorders.Hacke W et al. N Engl J Med. 2008;359:1317-1329.
Expansion of the Time Window for Treatment of Acute Ischemic Stroke With IV tPA
A Science Advisory From the American Heart Association/American Stroke Association
rtPA should be administered to eligible patients who can be treated in the time period of 3.0 to 4.5 hours after stroke (Class I Recommendation, Level of Evidence B) Exclude patients with previous stroke and diabetes, age > 80 years, oral
anticoagulation, NIHSS > 25
IV, intravenous; rtPA, recombinant tissue plasminogen activator; NIHSS, National Institutes of Health Stroke Scale.del Zoppo GJ et al. Stroke. 2009;40:2945-2948.
Still: Earlier the Better
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 4

Strategies to Increase Recanalization Rates
IV Pharmacological tPA (FDA-approved)1
Tenecteplase,2 desmoteplase3
Monoclonal antibodies to antiplasmin4 Monoclonal antibodies to antiplasmin4
Intra-Arterial (Invasive) Pharmacological5
Mechanical6
Merci (FDA device approval)
Penumbra (FDA device approval)1. Wolpert S et al. AJNR Am J Neuroradiol. 1993;14:3-13. 2. Hacke W et al. Stroke. 2005;36:66-73. 3. Haley E et al. Stroke. 2005;36:607-612. 4. Nagai N et al. Blood. 2001;97:3086-3092.5. IMS Study Investigators. Stroke. 2004;35:904-911. 6. Gupta R et al. AJNR Am J Neuroradiol. 2006;27:521-523.
Secondary Prevention of Ischemic Stroke and TIA
Risk of Recurrent Stroke
• People who have already suffered an ischemic stroke or TIA are at highest risk of a second stroke or death
• Approximately 17% of strokes are second strokes
• Second stroke risk is highest in the 7 daysfollowing the event
American Heart Association. Heart Disease and Stroke Statistics 2003 update.Sacco RL et al. Stroke. 1998; 29(10): 2118-24.
German Stroke Databank.
Recurrent Vascular Events
Patients who suffer ischemic strokes who have a recurrent vascular event in the first 3 years, 80% of time will have a stroke, 20% an MI
Patients who suffer an MI, who have a recurrent vascular event in the first 3 years, 80% of the time will have a recurrent MI, 20% of the time a stroke
Stroke published online October 21, 2010; Stroke 2011;42:00-00
Components of Secondary Prevention
Blood pressure control
Diabetes management
Lipid management
Smoking cessation
Alcohol moderation
Weight reduction / Physical activity
Carotid Artery Interventions
Antiplatelet agents / anticoagulants
Statins
Diuretics +/- ACE inhibitors
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 5
Self Assessment Question
Which comorbidity would lead to a recommendation (ASA guidelines) of warfarinfor secondary stroke prevention?
a Vertebral dissectiona. Vertebral dissection
b. Atrial fibrillation
c. Patent foramen ovale (PFO)
d. Diabetes
2010 Guidelines: New
BP: choice of agents based on co-morbidities
Diabetes: use existing id li (i t d f
Intracranial stenosis: ASA 50-325 mg daily with risk factor reduction
Atrial fib: noguidelines (instead of <7%)
Lipids: reduce LDL at least 50% or target <70
Metabolic syndrome: risk reduction
Atrial fib: no clopidogrel + ASA; bridging OK
Antiplatelet: no new recs; removal of preference statements
Furie et al. Stroke published online October 21, 2010; Stroke 2011;42:00-00
2010 Guidelines: New
Dissection and PFO: antiplatelet vs anticoag unknown
Fabry’s disease:
Anticoag after ICH: restart warfarin after 7-10 days in high risk patientsy
alpha galactosidase enzyme replacement
Furie et al. Stroke published online October 21, 2010; Stroke 2011;42:00-00
Stroke Prevention - NoncardioembolicASA 2010 Recommendations
For patients with noncardioembolic ischemic stroke or TIA, antiplatelet agents are recommended rather than oral anticoagulation to reduce the risk
f t t k d th di l tof recurrent stroke and other cardiovascular events (Class I, Evidence A).
Furie et al. Stroke published online October 21, 2010; Stroke 2011;42:00-00
IMPACT OF PROFESSIMPACT OF PROFESS
Sacco RL et al. N Engl J Med 2008;359:1238-1251
Sacco RL et al. N Engl J Med 2008;359:1238-1251
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 6

Sacco RL et al. N Engl J Med 2008;359:1238-1251
PROFESS Outcomes
Recurrent stroke rate Clopidogrel: 8.8% IS: 7.9%; Hem: 0.4%
Aggrenox: 9.0% IS: 7.7%; Hem: 0.8%
Composite outcomes: Composite outcomes: stroke, stroke/death, death
Clopidogrel: 13.1%
Aggrenox 13.1%
Sacco RL et al. N Engl J Med 2008;359:1238-1251
Atrial FibrillationASA 2010 Recommendations
For patients with ischemic stroke or TIA with persistent or paroxysmal (intermittent) AF, anticoagulation with a vitamin K antagonist (target INR 2.5, range 2.0 to 3.0) is recommended (Class , g ) (I, Evidence A).
For patients unable to take oral anticoagulants, aspirin alone is recommended (Class I Evidence A).
Furie et al. Stroke published online October 21, 2010; Stroke 2011;42:00-00
Updated Atrial Fibrillation Guidelines - 2011 Dabigatran is an alternative to warfarin (Class
I, Level of Evidence B)
NOT for patients with prosthetic valves or hemodynamically significant valve diseasehemodynamically significant valve disease
NOT for patients with CrCl <15 mL/min
NOT for patients with advanced liver disease (altered clotting fxn)
Wann LS et al. Circulation 2011;123:1144-1150
Evidence
Original ArticleDabigatran versus Warfarin in Patients with Atrial Fibrillation
Stuart J. Connolly, M.D., Michael D. Ezekowitz, M.B., Ch.B., D.Phil., y, , , , , ,Salim Yusuf, F.R.C.P.C., D.Phil., John Eikelboom, M.D., Jonas Oldgren, M.D., Ph.D., Amit Parekh, M.D., Janice Pogue, M.Sc., Paul A. Reilly, Ph.D., Ellison Themeles, B.A., Jeanne Varrone, M.D., Susan Wang, Ph.D., Marco Alings, M.D., Ph.D., Denis Xavier, M.D., Jun Zhu, M.D., Rafael Diaz, M.D., Basil S. Lewis, M.D., Harald Darius, M.D., Hans-Christoph Diener, M.D., Ph.D., Campbell D. Joyner, M.D., Lars Wallentin, M.D., Ph.D., and the RE-LY Steering Committee and InvestigatorsN Engl J Med 2009; 361:1139-1151September 17, 2009
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 7
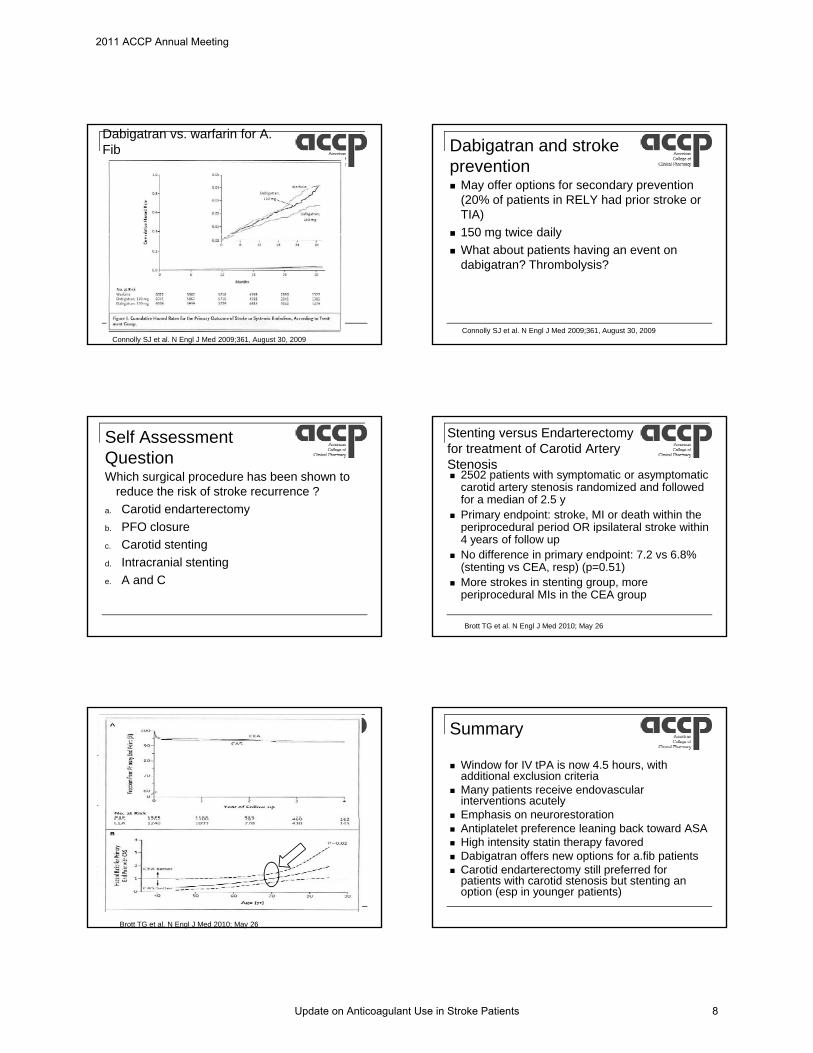
Dabigatran vs. warfarin for A. Fib
Connolly SJ et al. N Engl J Med 2009;361, August 30, 2009
Dabigatran and stroke prevention May offer options for secondary prevention
(20% of patients in RELY had prior stroke or TIA)
150 mg twice daily 150 mg twice daily
What about patients having an event on dabigatran? Thrombolysis?
Connolly SJ et al. N Engl J Med 2009;361, August 30, 2009
Self Assessment QuestionWhich surgical procedure has been shown to
reduce the risk of stroke recurrence ?
a. Carotid endarterectomy
b PFO closureb. PFO closure
c. Carotid stenting
d. Intracranial stenting
e. A and C
Stenting versus Endarterectomyfor treatment of Carotid Artery Stenosis 2502 patients with symptomatic or asymptomatic
carotid artery stenosis randomized and followed for a median of 2.5 y
Primary endpoint: stroke, MI or death within the periprocedural period OR ipsilateral stroke withinperiprocedural period OR ipsilateral stroke within 4 years of follow up
No difference in primary endpoint: 7.2 vs 6.8% (stenting vs CEA, resp) (p=0.51)
More strokes in stenting group, more periprocedural MIs in the CEA group
Brott TG et al. N Engl J Med 2010; May 26
Brott TG et al. N Engl J Med 2010; May 26
Summary
Window for IV tPA is now 4.5 hours, with additional exclusion criteria
Many patients receive endovascular interventions acutely
Emphasis on neurorestoration Emphasis on neurorestoration Antiplatelet preference leaning back toward ASA High intensity statin therapy favored Dabigatran offers new options for a.fib patients Carotid endarterectomy still preferred for
patients with carotid stenosis but stenting an option (esp in younger patients)
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 8

When is a new medication better than the tried and true? Use of dabigatran in atrial fibrillation for stroke prevention
Asha L. Tata, Pharm.D. BCPSInternal Medicine Clinical Pharmacy Specialist
University of Maryland Medical Center
Conflicts of Interest
No conflicts to disclose
Objectives
Compare and contrast the pharmacology of dabigatran versus warfarin
Summarize efficacy, safety, and Summarize efficacy, safety, and pharmacoeconomic data for dabigatran
Describe the place in therapy for dabigatran in the treatment of atrial fibrillation
Atrial Fibrillation (AF)
Affects more than 1% of general population with prevalence increasing with age
Independent risk factor for ischemic stroke Increased morbidity and mortality compared with non-AF Increased morbidity and mortality compared with non AF
related strokes
Economic burden Estimated indirect and direct costs $66 billion annually
Antiplatelet agents and vitamin K antagonists mainstay of anticoagulation therapy in AF
J Am Coll Cardiol 2010;56:2067-76.
Risk Assessment: Stroke
CHADS2
Risk Factor Score
CHF 1
HTN 1
DM 1
CHA2DS2-VAScRisk Factor Score
CHF 1
HTN 1
Age ≥ 75 2DM 1
Age > 75 1
Stroke/TIA 2
Maximum score 6
Age ≥ 75 2
DM 1
Stroke, TIA, or thromboembolism
2
Vascular disease 1
Age 65-74 years 1
Sex category 1
Maximum score 9
0 – No antithrombotic therapy1 – Oral anticoagulation or antiplatelet therapy≥2 – Oral anticoagulation
Stroke 2010;41:2705-13.Curr Cardiol Rep 2011;13:9-17.
Risk Assessment: Bleeding
HAS-BLEDRisk Factor Score
HTN 1
Abnormal renal and liver function (1 point each)
1 or 2
Stroke 1Stroke 1
Bleeding tendency 1
Labile INRs (if on warfarin) 1
Elderly (age > 65 years) 1
Drugs or alcohol (1 point each) 1 or 2
Maximum score 9≥4 – High risk2-3 – Moderate risk0-1 – Low risk
Curr Cardiol Rep 2011;13:9-17.
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 9

Vitamin K Antagonists for AF
Superior to placebo and antiplatelet agents in patients at moderate-high risk of stroke
Underutilized, especially in elderly patientsp y y p Fear of bleeding
Fall risk
Patient with CHADS2 score of 3 would have to fall ~295 times in a year to outweigh warfarin benefit
Birmingham Atrial Fibrillation Treatment of the Aged Study (BAFTA) indicates that elderly patients benefit from anticoagulation therapy
Stroke 2010;41:2705-13.Curr Cardiol Rep 2011;13:9-17.
New Anticoagulants
VTE prophylaxis post orthopedic surgery
VTE treatment
Atrialfibrillation
Arterial disease
Other potential indications
Dabigatran: Ideal Anticoagulant?
Ideal Anticoagulant Warfarin Dabigatran
Oral administration + +
Fixed dosing - +
Predictable PK - +
Rapid onset/offset of action - +
N d f d i t tiNo drug or food interactions - +
No routine monitoring - +
Low risk of hemorrhage - +/-
Use in severe liver disease
- ?
Use in severe renal disease
+ ?
Available antidote + -
Inexpensive + -
Circulation 2011;123:1436-50.
Dabigatran (Pradaxa®)
Approved by FDA October 2010 for non-valvular AF
Mechanism of action
Prodrug
P t t titi ibl di t i hibit f th Potent, competitive, reversible direct inhibitor of the active site of thrombin
Formulation
Capsule containing tartaric acid pellets
Dispense in original manufacturer’s bottle and use within 30 days
Pradaxa® Product Information.Circulation 2011;123:1436-50.Am J Health-Syst Pharm 2011;68:1506-19.Ann Pharmacother 2011;45:603-14.
Dabigatran (Pradaxa®)Pharmacokinetics
Absorption Time to peak 0.5-2 hours
Time to steady state ~ 3 days
Bioavailability 3-7%
Distribution 35% protein bound
Vd 50-70L
M t b li Bioavailability 3-7% Ingestion of pellets can
increase by 75%
High-fat meal delays time to Cmax by 2 hours
Metabolism Not mediated by CYP450
P-gp substrate
Elimination 80% renal
T1/2 12-17 hoursPradaxa® Product Information.Circulation 2011;123:1436-50.Am J Health-Syst Pharm 2011;68:1506-19.Ann Pharmacother 2011;45:603-14.
Dabigatran (Pradaxa®)
Dosing CrCl > 30 mL/min – 150 mg orally twice daily
CrCl 15-30 mL/min – 75 mg orally twice daily
CrCl < 15 mL/min or dialysis – no recommendations
D i t ti Drug interactions Avoid with P-gp substrate inducers
No dose adjustments required for P-gp inhibitors
Proton pump inhibitor interaction not clinically significant
Adverse reactions Dyspepsia
Gastrointestinal bleeding
Pradaxa® Product Information.Circulation 2011;123:1436-50.Am J Health-Syst Pharm 2011;68:1506-19.Ann Pharmacother 2011;45:603-14.
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 10
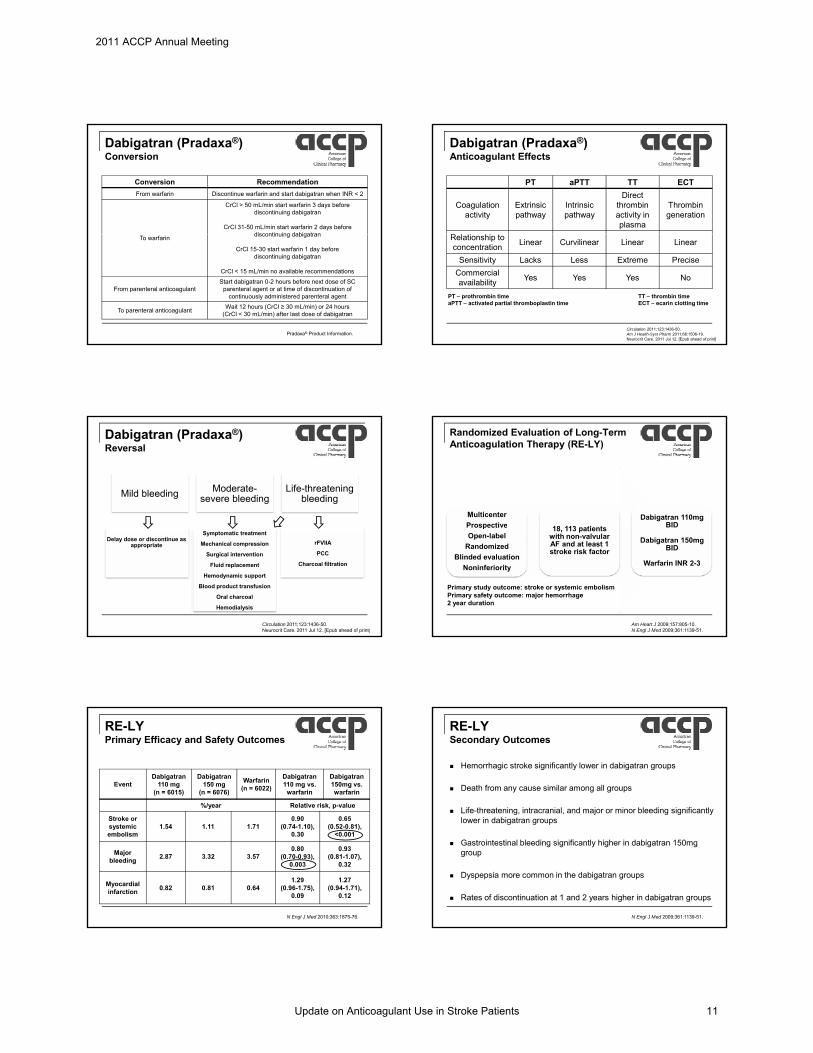
Dabigatran (Pradaxa®)Conversion
Conversion Recommendation
From warfarin Discontinue warfarin and start dabigatran when INR < 2
CrCl > 50 mL/min start warfarin 3 days before discontinuing dabigatran
CrCl 31-50 mL/min start warfarin 2 days before discontinuing dabigatran
To warfarindiscontinuing dabigatran
CrCl 15-30 start warfarin 1 day before discontinuing dabigatran
CrCl < 15 mL/min no available recommendations
From parenteral anticoagulantStart dabigatran 0-2 hours before next dose of SC
parenteral agent or at time of discontinuation of continuously administered parenteral agent
To parenteral anticoagulantWait 12 hours (CrCl ≥ 30 mL/min) or 24 hours
(CrCl < 30 mL/min) after last dose of dabigatran
Pradaxa® Product Information.
Dabigatran (Pradaxa®)Anticoagulant Effects
PT aPTT TT ECT
Coagulationactivity
Extrinsic pathway
Intrinsicpathway
Direct thrombin activity in plasma
Thrombin generation
R l ti hi tRelationship to concentration
Linear Curvilinear Linear Linear
Sensitivity Lacks Less Extreme Precise
Commercialavailability
Yes Yes Yes No
Circulation 2011;123:1436-50.Am J Health-Syst Pharm 2011;68:1506-19.Neurocrit Care. 2011 Jul 12. [Epub ahead of print]
PT – prothrombin timeaPTT – activated partial thromboplastin time
TT – thrombin timeECT – ecarin clotting time
Dabigatran (Pradaxa®)Reversal
Mild bleeding Moderate-severe bleeding
Life-threatening bleeding
Delay dose or discontinue as appropriate
Symptomatic treatment
Mechanical compression
Surgical intervention
Fluid replacement
Hemodynamic support
Blood product transfusion
Oral charcoal
Hemodialysis
rFVIIA
PCC
Charcoal filtration
Circulation 2011;123:1436-50.Neurocrit Care. 2011 Jul 12. [Epub ahead of print]
Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY)
Multicenter
Prospective 18 113 ti t
Dabigatran 110mg BIDProspective
Open-label
Randomized
Blinded evaluation
Noninferiority
18, 113 patients with non-valvular AF and at least 1 stroke risk factor
BID
Dabigatran 150mg BID
Warfarin INR 2-3
Primary study outcome: stroke or systemic embolismPrimary safety outcome: major hemorrhage2 year duration
Am Heart J 2009;157:805-10.N Engl J Med 2009;361:1139-51.
RE-LYPrimary Efficacy and Safety Outcomes
EventDabigatran
110 mg(n = 6015)
Dabigatran 150 mg
(n = 6076)
Warfarin (n = 6022)
Dabigatran 110 mg vs.
warfarin
Dabigatran 150mg vs. warfarin
%/year Relative risk, p-value
Stroke or 0 90 0 65Stroke or systemic embolism
1.54 1.11 1.710.90
(0.74-1.10), 0.30
0.65 (0.52-0.81),
<0.001
Major bleeding
2.87 3.32 3.570.80
(0.70-0.93),0.003
0.93 (0.81-1.07),
0.32
Myocardial infarction
0.82 0.81 0.641.29
(0.96-1.75), 0.09
1.27 (0.94-1.71),
0.12
N Engl J Med 2010;363:1875-76.
RE-LYSecondary Outcomes
Hemorrhagic stroke significantly lower in dabigatran groups
Death from any cause similar among all groups
Life-threatening, intracranial, and major or minor bleeding significantly l i d bi tlower in dabigatran groups
Gastrointestinal bleeding significantly higher in dabigatran 150mg group
Dyspepsia more common in the dabigatran groups
Rates of discontinuation at 1 and 2 years higher in dabigatran groups
N Engl J Med 2009;361:1139-51.
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 11

RE-LYConclusions
Rates of stroke and systemic embolism with both doses of dabigatran noninferior compared to warfarin
Dabigatran 110mg dose noninferior to warfarin with lower rates of major hemorrhagelower rates of major hemorrhage
Dabigatran 150mg dose superior to warfarin with similar rates of major hemorrhage but higher rates of gastrointestinal bleeding
N Engl J Med 2009;361:1139-51.
RE-LY Sub-analyses
Sub-group Findings
Previous TIA or strokePrimary efficacy and safety outcomes consistent with RE-LY in patients with
previous TIA or stroke
Previous vitamin K antagonistVitamin K antagonistnaïve vs. experienced
Previous vitamin K antagonist exposure does not influence benefits of dabigatran compared with warfarin
Cardioversion
Frequencies of stroke and major bleeding within 30 days of
cardioversion on dabigatran comparable to those on warfarin
Lancet Neurol 2010;9:1157-63.Circulation 2010;122:2246-53.Circulation 2011;123:141-136.
RE-LY Sub-analyses
Sub-group Findings
Time in therapeutic range (TTR)
For all vascular events, non-hemorrhagic events, and mortality
advantages of dabigatran greater at sites with poor INR control illustrating
local standards affect treatment choice
Bleeding risk in older vs. younger Patients
Both dabigatran doses have lower risks of intracranial and extracranial
bleeding in patients <75 years;In those ≥75 years, intracranial
bleeding risk is lower but extracranial bleeding similar with dabigatran
110mg and higher with dabigatran 150mg
Lancet 2010;376:975-83.Circulation 2011;123:2363-72.
Pharmacoeconomic Data
Outcome WarfarinDabigatran
110mgDabigatran
150mg
Quality-adjustedlife-years (QALYs)
10.28 10.70 10.84
Direct Costs (2008 U.S. dollars)
$143,193 $164,576 $168,398( )
Incremental cost-effectiveness
Ratios (ICERs) compared with
warfarin
NA $51,229 $45,372
Cost-effective alternative to warfarin if dabigatran 150 mg BID treatment daily cost < $13.70
Ann Intern Med 2011;154:1-11.
Pharmacoeconomic Data
Hypothetical cohort of 70- year old patients with AF using cost-effectiveness threshold of $50,000/QALY
Estimated dabigatran cost $9/day with average risk of major hemorrhage ~3%/year
CHADS2 score 0 – aspirin cost-effective
CHADS2 score 1-2 – warfarin cost-effective unless risk of hemorrhage high or INR TTR < 57.1%
CHADS2 score ≥ 3 - dabigatran 150mg BID cost-effective unless INR TTR >72.6%
Circulation 2011;123:2562-2570.
Current Challenges
Administration in hospitalized patients
Acute kidney injury
Non-adherent patients
Cost
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 12

Unresolved Issues
Long term efficacy Attainment of therapeutic
INRs in real life compared to clinical trials
Long term safety
Underweight/obese patients
Severe renal and hepatic impairment
Drug interactions Long term safety Rebound thrombosis
Myocardial infarction
Hepatotoxicity
Reversal
Drug interactions
Role of 75mg and 110mg doses
Use in other indications
Comparison to oral Factor Xa inhibitors
Circulation 2011;123:1436-50.Am J Health-Syst Pharm 2011;68:1506-9.Ann Pharmacother 2011;45:603-14.
Patient Case
82 yo AAF with PMH significant for HTN, AF, and severe dementia. Patient’s laboratory values are all WNL. Patient had been stable on warfarin for the past 10 years but over the past month has been refusing bloodwork. Your physician colleagues ask you your opinion in p y g y y pmanaging her anticoagulation. What is your recommendation?
A) Switch to aspirin 81mg daily
B) Switch to aspirin 81mg daily + clopidogrel 75 mg daily
C) Switch to dabigatran 150 mg twice daily
D) Discontinue anticoagulation given patient’s age and dementia
Place in Therapy
ACCF/AHA/HRS 2011 focused update recommendation Dabigatran is useful as an alternative to warfarin for the
prevention of stroke and systemic thromboembolism in patients with paroxysmal to permanent AF and risk factors for stroke or systemic embolization who do not have a prosthetic heart valve or hemodynamically significant valve disease, severe renal failure (C Cl 15 L/ i ) d d li di (i i d b li(CrCl <15 mL/min), or advanced liver disease (impaired baseline clotting function). (Level of Evidence: B)
Alternative to warfarin in moderate-high risk patients with: Difficulty achieving therapeutic INRs
Inability obtaining regular INR monitoring
Low risk for gastrointestinal bleeding
Low risk for cardiovascular events
Circulation 2011;123:1144-50.
Conclusions
Anticoagulation is the mainstay of treatment in AF with risk assessment for stroke and bleeding essential in individualizing therapy
Warfarin should continue to be used as the first line anticoagulant in most patients
Dabigatran offers an alternative in a small niche of patients who are poor candidates for warfarin
When is a new medication better than the tried and true? Use of dabigatran in atrial fibrillation for stroke prevention
Asha L. Tata, PharmD BCPSInternal Medicine Clinical Pharmacy Specialist
University of Maryland Medical Center
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 13

Quality initiatives of anticoagulant safety: attacking the coagulation cascade,
SAFELY
William Dager, Pharm.D., BCPS (AQ Cardiology) g , , ( Q gy)FCCP, FCSHP, FCCM, FASHP
Pharmacist Specialist, UC Davis Medical Center
Clinical Professor of Pharmacy, UC San Francisco School of Pharmacy
Clinical Professor of Medicine, UC Davis School of Medicine
Affiliate Faculty, ACLS American Heart Association
Objectives
Improve medication management in secondary stroke prevention and in patient with atrial fibrillation
Describe the pharmacist’s role in enhancing anticoagulation safety in the hospital
Provide dosing guidelines or protocols for the management of antithrombotic therapy
Thrombosis Management and Prevention: Why is Anticoagulation therapy oversight important?
ADE / Safety Concerns• UFH/Warfarin/LMWH → High incidence of Medication errors
Growing Science/Options Multi-disciplinary Component Financial Impact Pay for Performance: SCIP guidelines The Joint Commission
• VTE and Stroke Measures• Safety Goal 3E
Expanding Management Considerations• CMS outpatient follow-up
Challenges Faced in providing safe anticoagulation
Unfunded mandates
Budgets are shrinking
Prioritizing resources to meet basic patient carePrioritizing resources to meet basic patient care services
Creating successful systems, and identifying/training healthcare professionals to provide optimal, safe anticoagulation management
Stroke Core Initiatives
STK-1 - # of patients with stroke who have VTE prophylaxis or documentation of reason for no prophylaxis
STK-3 - # of ischemic stroke patients with a fib/flutter discharged home on anticoagulation
Patient Safety Goals
NPSG.03.05.01 Reduce the likelihood of patient harm associated with the use of anticoagulant therapy.
Note: This requirement applies only to hospitals that provide anticoagulant therapy and/or long-term anticoagulation prophylaxis (i.e. Atrial Fibrillation) where the clinical expectation is that the patient’s laboratory values for coagulation will remain outside y gnormal values.
This requirement does not apply to routine short-term prophylactic anticoagulation against VTE if the clinical expectation is that the patient’s laboratory values for coagulation will remain within, or close to, normal values.
Pre-Publication Version © 2009 by the Joint Commission on Accreditation of Healthcare Organizationshttp://www.jointcommission.org/NR/rdonlyres/122D9A33-6540-4B73-9D7A-F8B26C32A8CA/0/HAP_2010NationalPatientSafetyGoals_PrePub_20090909.pdf
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 14

Anticoagulation Safety GoalsChanges for 2010 Deleted requirement for written description (policy) of the program
Changed requirement for a baseline INR to a baseline assessment of anticoagulation status
Changed requirement for dietary notification to use of “authoritative ”resources”
Clarified educational requirements
Changes for 2011 A written policy addresses baseline and ongoing laboratory tests that
are required for heparin and low molecular weight heparin therapies anticoagulants.
• Applies to Warfarin, UFH and LMWH only
Joint Commission Perspectives®, August 2010, Volume 30, Issue 8 Copyright 2010 Joint Commission on Accreditation of Healthcare Organizations
NPS.03.05.01 2. Use approved protocols for the initiation and maintenance of anticoagulant therapy.
Is it drug dosing specific, or systems approach?
- How are anticoagulant orders initiated and managed
Challenges with warfarin dosing protocolsA patient (CHADS2 = 5 and CKD IV) arrives with a small GI
Bleed, gets 10mg SQ vitamin K x 3 days. INR = 1.2 after doubling the home warfarin dose for 5 days.
A AF patient with a recent ischemic stroke and ICH requiring a heparin drip. Baseline INR of 1.8
A patient gets 5mg of warfarin and has a INR of 1.5 the next day (with aPTT > 150). 3mg of warfarin is given and the next day INR is 1.0. Amiodarone and Metronidazole are ordered.
Proposed Stroke CMS measures Future CMS measures - Collection begins in 2013 FY2015 Proposed additions from CMS
Stroke Measure set STK-1 VTE Prophylaxis
STK 2 A i h b i h f i h i k STK-2 Antithrombotic therapy for ischemic stroke STK-3 Anticoagulation therapy for A fib/flutter STK-4 Thrombolytic therapy for acute ischemic stroke STK-5 Antithrombotic therapy by the end of hospital
day 2 STK-6 Discharged on statin STK-8 Stroke education STK-10 Assessed for rehab
ACCP 2008 Guidelines for Stroke Prevention in AF
Risk category Prior ischemic stroke, TIA, or
systemic embolism, or history of mitral stenosis (valvularAF) or prosthetic
≥ 2 stroke risk
factors†
Only 1 stroke risk
factor†
Age ≤ 75 years and no other stroke risk
factors†
AF), or prosthetic heart valve*
Recommended therapy
Warfarin (INR 2-3)
Warfarin (INR 2-3)
Warfarin (INR 2-3) or daily ASA 75–325 mg
Daily ASA 75-325 mg
*INR target may be higher than 2-3 for patients with prosthetic heart valves†Stroke risk factors—age > 75 years, history of hypertension, diabetes mellitus, and moderately or severely impaired left ventricular systolic function and/or heart failure
Singer DE, et al. Chest 2008;133:546S-592S.
ACC/AHA/ESC 2006 Guidelines for the Management of Patients
with AF Risk category Any high-risk factor* or more
than 1 moderate-risk factor†
One moderate-risk factor†
No risk factors
R d d W f i W f i (INR D il ASARecommended therapy
Warfarin (INR 2-3)
Warfarin (INR 2-3) or daily
ASA 81–325 mg
Daily ASA 81–325 mg
*High-risk factors—previous stroke/TIA/embolism, mitral stenosis, prosthetic heart valve (INR target may be higher than 2-3)†Moderate-risk factors—age ≥ 75 years, hypertension, heart failure, left ventricular ejection fraction ≤ 35%, diabetes mellitusDabigatran: Alt to Warf. (Persistent/Paroxysmal AF) and CVA risk but no prosthetic heart valve or severe renal/hepatic Dz)
Fuster V, et al. Circulation 2006;114:e257-e354; Wann LS et al. Heart Rhythm 2011;8:e1-8.
AHA 2010 Stroke Guidelines for the Management of Patients with AF
CVA plus AF High Risk (CHADS – 5-6)
Thrombus on ECHO
Recommended VKA LMWH Bridge VKAtherapy (INR 2-3)
gto VKA is reasonable
(INR 2-3)
Ref. Furie KL Circulation 2010
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 15

Centralizing Experience: Financial Impact
Need for Hospitalization LOS ADE Cost of care
• Over-reversalH h• Home therapy
• Drug acquisition• Excessive Assays
Billing for service: Internist for surgical patients
Implementing and Assessing Anticoagulation Therapy
Patient/Condition
Outcomes
ProphylaxisTreatment
Thrombosis BleedingADECosts
DosingInteractionsDual-Triple therapyE id l/S i l
Ordering
UFH
LMWH
DTI
Monitoring
Pump SettingsCompatibilityAdministration Schedule (q___ “hr”)
IV Admixture ProcessRelease to Pyxis
aPTT , INRHgb, PltTiming
Epidural/Spinal Baseline Labs
Administration
aPTT = activated partial thromboplastin time; Hgb = hemoglobin; INR = International Normalized Ratio; Plt = platelets.
Preparation
ASA
ANTI-PLATELET
Improving medication management in secondary stroke prevention
Risk of thrombosis
Risk assessment Score: CHADS, CHA2DS2VASc ECHO observationsECHO observations
• Not studied as a independent factor
Plan for Therapy• Cardioversion, Ablation, Rate, Rate/Rhythm or Rhythm
control
Gage B et al JAMA. 2001;285: 2864-2870Lip GY, et al. Chest 2010;137:263-272
Improving medication management in secondary stroke prevention
Risk for Bleeding
HASBLED Score HASBLED Score Use of a anticoagulant How falls is to high of a risk Are independent factors for falls considered?
Lip G Chest 2010; 138(5):1093–1100
AF: Considerations for Bridging Having a Stroke on my watch is a very bad thing!
• → Clinicians tend to thus “bridge” to warfarin
• Careful planning for invasive procedures
Thrombus typically develops in the cardiac chamber• Aspirin?
• LMWH: What dose?
• UFH: Do I need to bolus? aPTT target?
Is the patient in sinus rhythm?
What is the risk for bleeding?• Any critical issues?
Atrial Fibrillation: LMWH or UFH RCT’s
Stroke: 14 day recurrent stroke rate AF but no warfarin (CHEST 2008: Bridge for high risk patients)
HAEST Dalteparin ASA OR
100 u/kg BID 160mg/day
8.5% 7.5% 1.1 (0.6-2.2)
Saxena UFH 12,500 BID No UFH
2.3% 4.9% 0.5 (0.3-0.8)
HAEST: Lancet 2000; Saxena Stroke 2001
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 16

Warfarin Management Considerations in AF
Does the dose need to be aggressive?
Was the INR elevated secondary to a clinical situation?• Considerations with any requested reversal therapy• Considerations with any requested reversal therapy
Is bridging necessary?
Was medication reconciliation accurate to the most recent regimen?
What was given in the hospital?
Potential drug interactions
Quality of Warfarin Management Considerations in AF
Hard outcomes: • Stroke, Bleeding, Hospitalizations, Mortality
Defining good practice• Time in therapeutic range (TTR)
• Standard Deviation of transformed INR etc
Trial RE-LY Rocket AF ARISTOLTE
Drug Dabigatran Rivaroxaban Apixaban
TTR 64% 55% 62%
Lind M et al. Thromb Res 2011; Connolly SJ NEJM 2009;361:1139-51; Ahrens I et al. Thromb Haemost 2011; Granger CB NEJM 2011
Why should AC programs include reversal therapies
Bleeding concern is very high or present• During Procedures (Ablation etc)
The cost of the reversal agent and prolonged length of staylength of stay
Inadequate reversal:• Cost of delayed surgery or avoidable bleeding
• Incorrect use or exposure to short acting agents
Over reversal has risks for:• Prolonged anticoagulation free period
• Need for dual anticoagulants
ASA vs Warfarin to prevent AF related stroke
ASA provides little protection against stroke in AF and is markedly inferior to adjusted-dose (INR 2-3) warfarin therapy
ASA vs Placebo: Pooled analysis of trials
ASA RRR f 21%• ASA – RRR of 21%
• WARFARIN - RRR of 68%
ASA + WARFARIN:
• ↑ major bleeding risk of major bleeding
• No additional protection against ischemic stroke in AF– Possible exception: AF and prosthetic heart valve
replacement Singer DE, et al. Chest 2008;133:546S-592S
Non-Pharmacologic Management Approaches
Procedure Anticoagulation therapy considerations
Cardioversion-TEE
Warf (INR 2-3) x 1-2 months; Bridging
Cardiac Ablation Warfarin - INR 2-3 before, during and post procedureEnoxaparin 0.5 to 1mg/kg Bridge post procedureDabigatran: Avoid during procedure
Cox-Maze III Procedure
Watchman Device May still require anticoagulation
Tying off atrial appendage May still require anticoagulation
How is AC balanced with any reversal strategy
What happens with new anticoagulants
Is the dose correct for the indication?
Any unidentified or missed special populations?• Renal/Age adjustments
• Combined TherapiesCombined Therapies
• Compliance
Drug interactions
Non-Compliance
How do we “…reduce the risk of adverse events associated with the use of these agents.”
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 17
Role of Pharmacists in Optimizing Outcomes in AF
Gatekeepers of safe medication use
Medication management• Keep the big picture in mind
.
• Anticoagulation services
• Treat the Patient, not the INR
• Monitor: Antiarrhythmic therapy, Heart Failure, Medications creating fall or bleeding risk
Role of Pharmacists in Optimizing Outcomes in AF
Development of clinical pathways• Optimize patient outcomes
• Standardize where possible, but allow for individualized therapy
.
• Inpatient ↔ Transition ↔ Outpatient
Formulary management• Timely review of new therapies and appropriate
restrictions to ensure therapies are prescribed appropriately and for the right patient based on efficacy, safety, and cost
2011 ACCP Annual Meeting
Update on Anticoagulant Use in Stroke Patients 18