anticoagulant, fibrinolytic and antiplatelet anticoagulant, fibrinolytic and antiplatelet
TRANSCRIPT
Anticoagulant, Fibrinolytic and Antiplatelet

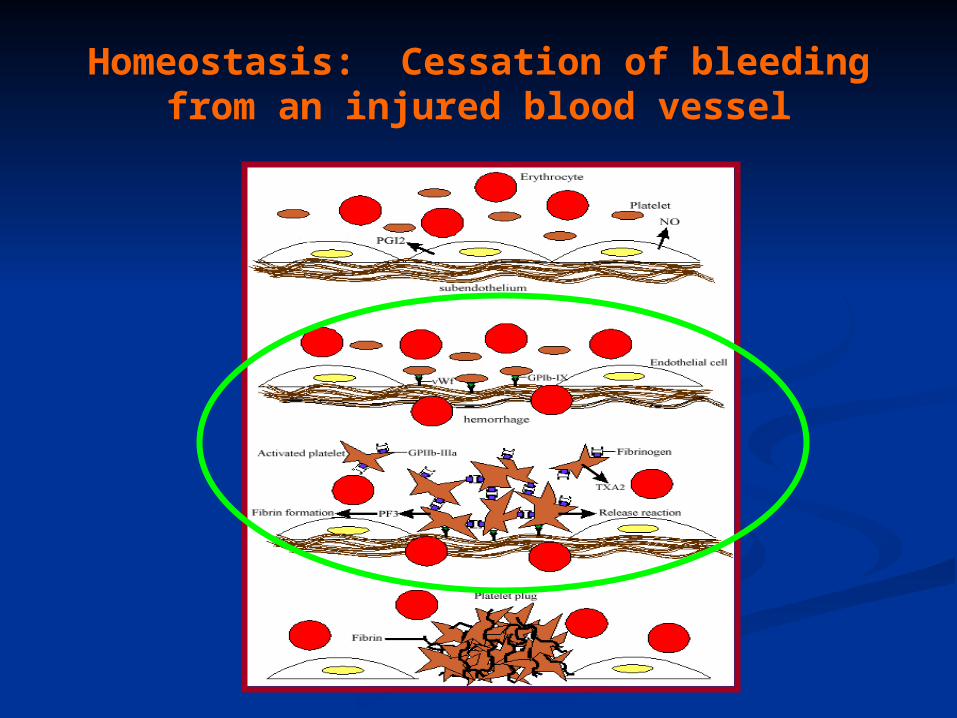
Homeostasis: Cessation of bleeding from an injured blood vessel
Primary Hemostasis
This stage occurs within seconds
1. Vasospasm: Vasoconstriction of the blood vessel by Prostacyclin (PI2), Thromboxane A2 (TXA2) and serotonin (5-HT). Slows down the bleeding.
2. Platelet Plug: Adherence of platelets to collagen of damaged endothelial cells. Platelet aggregation: Role of thrombin, adenosine diphosphate (ADP), PI2, TXA2, 5-HT and prostaglandins.
Secondary Hemostasis
This stage takes several minutes. Stabilizes the soft clot and maintains vasoconstriction.
3. Fibrin Clot: Conversion of prothrombin to thrombin. Thrombin stimulates the conversion of fibrinogen (Blood protein) to polymerized fibrin (mesh).
4. Dissolution of the clot by fibrinolysis: Plasminogen is converted to plasmin, the enzyme that dissolves the fibrin.
The hemostatic process is a protective mechanism to prevent blood loss from the circulatory system.
Homeostasis: Cessation of bleeding from an injured blood vessel
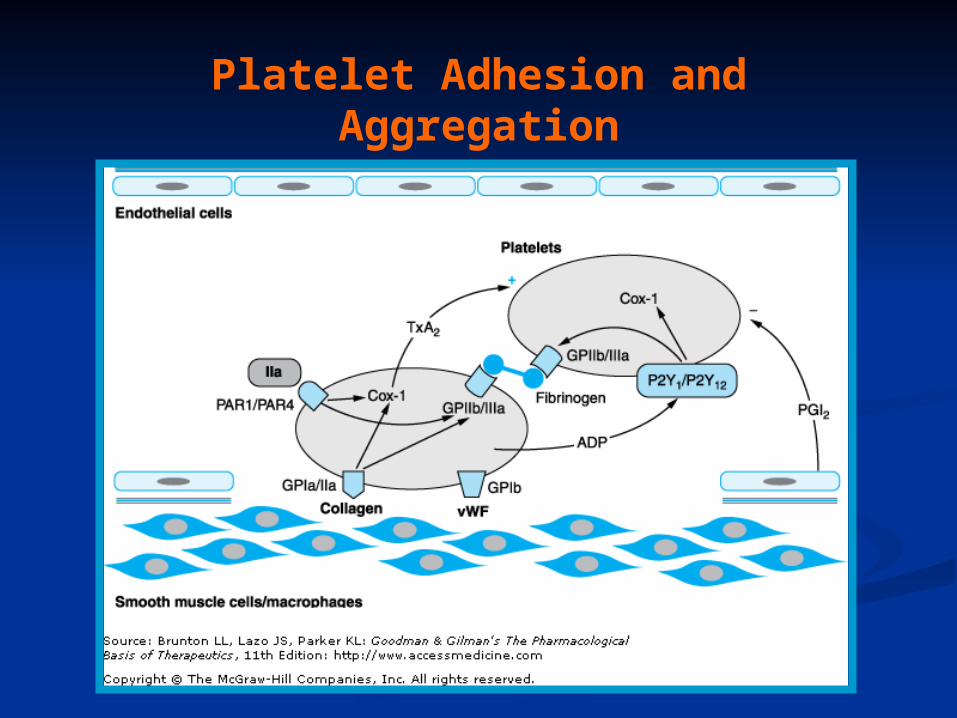
Platelet Adhesion and Aggregation

Blood Coagulation: One Type of Hemostatic Process
Intrinsic Pathway Activated when the blood comes in contact with
the subendothelial surface or negatively charged surface resulting from an injury to the blood vessel.
The Hageman factor (factor XII) binds to the subendothelial surface. It is then cleaved to XIIa. XIIa activates XI to form XIa. XIa activates IX to form IXa which then activates factor X to Xa.
Extrinsic Pathway Tissue factor (factor III) is located on the membrane
of most cells. Once activated, it converts VII to its active form, VIIa. A complex of VIIa+III+calcium+a phospholipid converts factor X to its active form, Xa.
Common Pathway Factor Xa is the convergence point for both the
intrinsic and extrinsic pathways. It initiates the common pathway.
Factor Xa converts prothrombin to active thrombin. Thrombin is required for the conversion of soluble
fibrinogen to insoluble fibrin protein. The fibrin meshwork is then stabilized by active factor XIIIa.
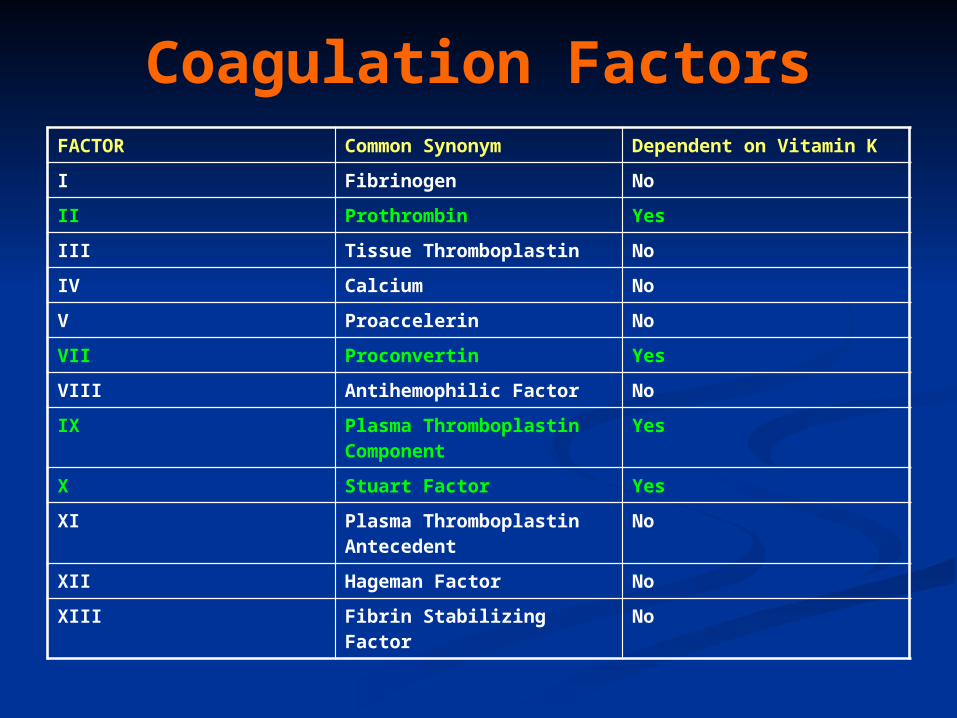
Coagulation FactorsFACTOR Common Synonym Dependent on Vitamin K
I Fibrinogen No
II Prothrombin Yes
III Tissue Thromboplastin No
IV Calcium No
V Proaccelerin No
VII Proconvertin Yes
VIII Antihemophilic Factor No
IX Plasma Thromboplastin Component
Yes
X Stuart Factor Yes
XI Plasma Thromboplastin Antecedent
No
XII Hageman Factor No
XIII Fibrin Stabilizing Factor No
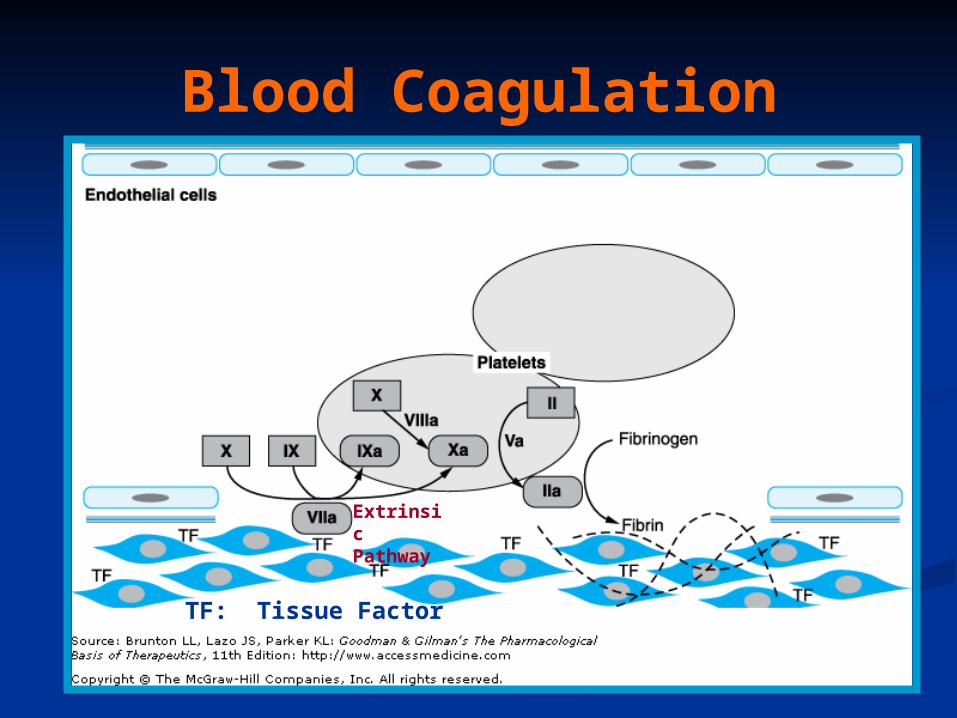
Blood Coagulation
Extrinsic Pathway
TF: Tissue Factor
Clotting Time Prothrombin Time; Prothrombin Ratio(PR) and Internationalized
Ratio(INR) Measures of the extrinsic/common pathway
PT reference range: 12-15 sec; measures factors II,V,VII,X and fibrinogen.; Used in conjunction with aPTT
PT: blood is combined with liquid citrate (chelates calcium; anticoagulant) in a testtube. There is a specific ratio of blood to citrate. The mixture is centrifuged and the plasma is collected. Thromboplastin (Tissue factor) is added to plasma and analyzed for clotting time.
INR normal range: 0.8-1.2
Activated Partial Thromboplastin Time (aPTT) Measure of the intrinsic pathway
aPPT normal range: 25-37 seconds aPPT:blood is combined with liquid citrate (chelates calcium; anticoagulant)
in a testtube. There is a specific ratio of blood to citrate. The mixture is centrifuged and the plasma is collected. A phospholipid (silica, kaolin, etc) and calcium are added to the plasma sample and analyzed for clotting time.
Partial Thromboplastin: thromboplastin is not added to the plasma sample.
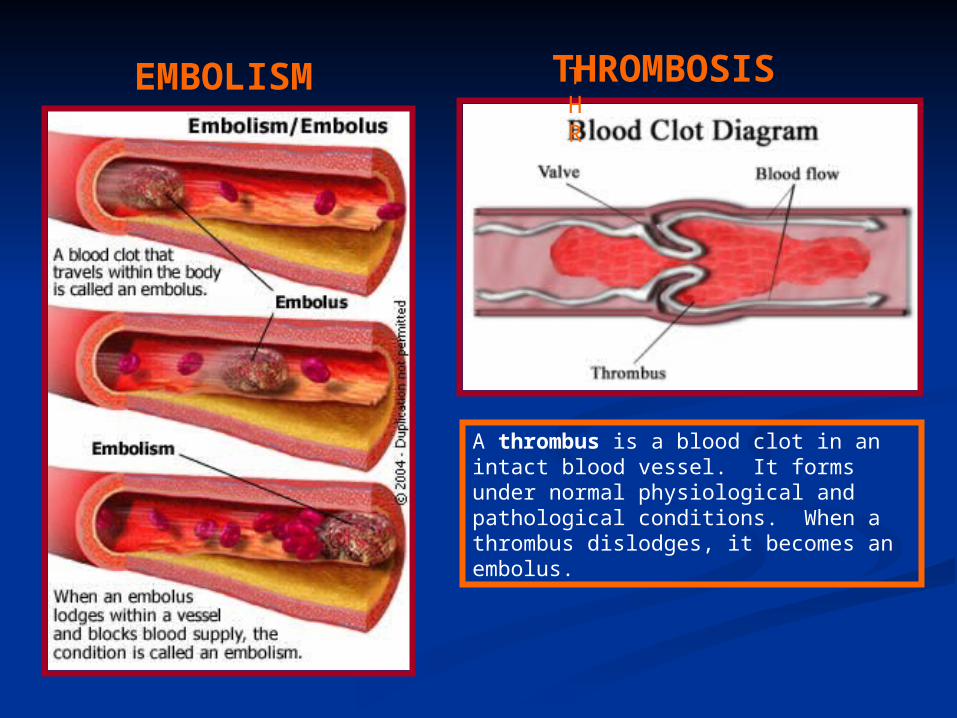
EMBOLISM THR
THROMBOSIS
A thrombus is a blood clot in an intact blood vessel. It forms under normal physiological and pathological conditions. When a thrombus dislodges, it becomes an embolus.
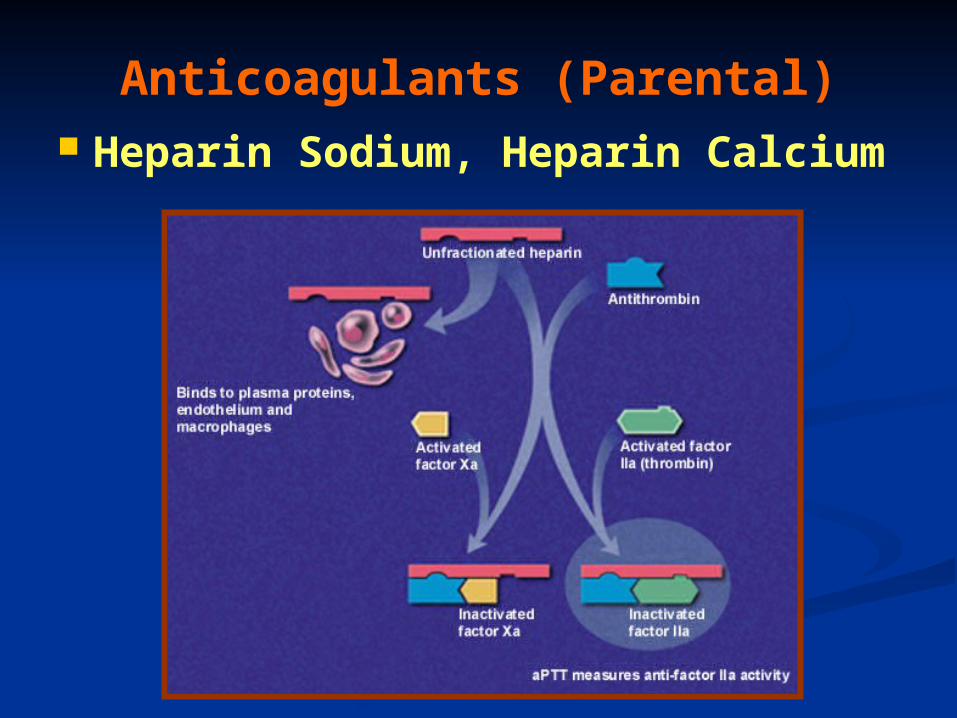
Anticoagulants (Parental) Heparin Sodium, Heparin
Calcium

Anticoagulants (Parental) Heparin Sodium, Heparin Calcium: Unfractionated: 5000-30,000 g/mol.
Naturally occurring mixture of sulfated muccopolysaccharides produced by mast cells and basophils.
Clinical Use: Prevention and treatment of embolism (i.e., post-op or following myocardial infarction), deep vein thrombosis, pulmonary embolism. Initial management of unstable angina or acute myocardial infarction.
MOA: Increases the activity of antithrombin III and inactivates thrombin. High doses will inhibit platelet aggregation.
Pharmacokinetics: Administration: Not absorbed from the gut; i.v. and s.c.. Immediate onset (30-60 mins); Hepatic elimination and excretion, some excreted unchanged in urine. Dosage is determined by the activated partial thromboplastin time (aPPT; 1.5-2 times is normal).
Side effects: Thrombocytopenia (early or delayed), hemorrhage.
Contraindications: existing bleeding condition or bleeding tendency.
Drug Interactions: Risk of bleeding is increased by salicylates
In case of overdose: protamine sulfate (positive charge binds heparin).
Anticoagulants (Parental) cont.
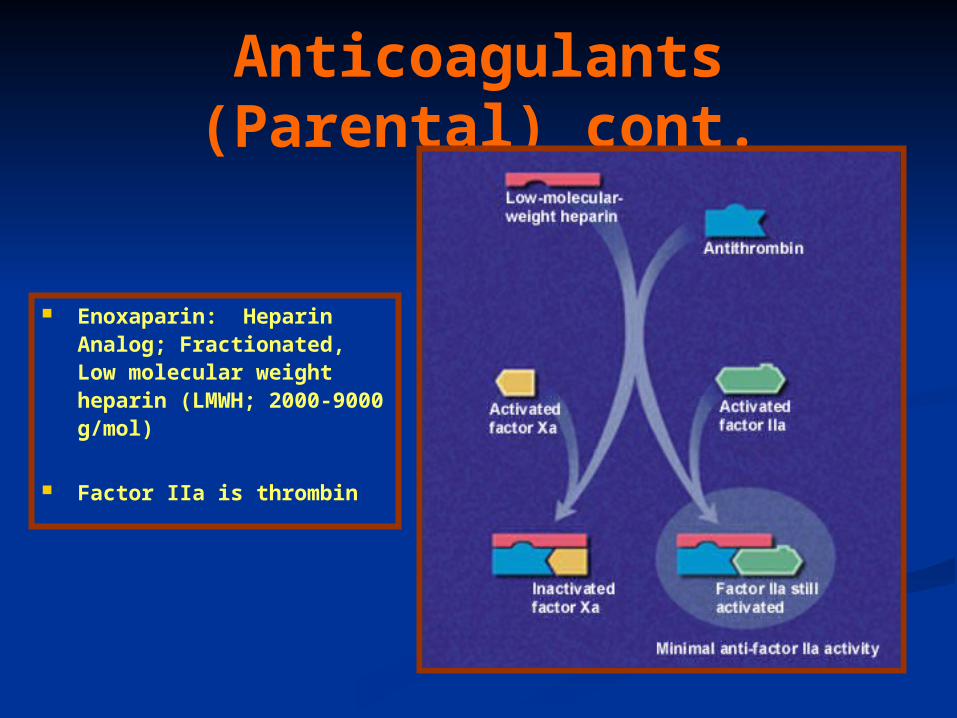
Enoxaparin: Heparin Analog; Fractionated, Low molecular weight heparin (LMWH; 2000-9000 g/mol)
Factor IIa is thrombin
Anticoagulants (Parental)
Enoxaparin: Heparin Analog; Fractionated, Low molecular weight heparin (LMWH; 2000-9000 g/mol)
Clinical Use: Prevention and treatment of embolism (i.e., post-op or following myocardial infarction), deep vein thrombosis.
MOA: Inhibits factor Xa, very little effect on factor IIa; aPPT is not used to measure its anticoagulant activity. Binds less to plasma proteins.
Pharmacokinetics: Administration: i.v. and s.c. outpatient basis for DVT patients. Immediate onset (30-60 mins); Hepatic elimination and excretion, some excreted unchanged in urine.
Side effects: Thrombocytopenia (early or delayed), hemorrhage.
Contraindications: existing bleeding condition or bleeding tendency.
In case of overdose: protamine sulfate (positive charge binds heparin).
Anticoagulants (Oral) Coumarins: dicumarol and warfarin; warfarin is
structurally related to vitamin K.
Clinical Use: Treatment of embolism, deep vein thrombosis or atrial fibrillation, patients with prosthetic valves (at risk for thrombosis).
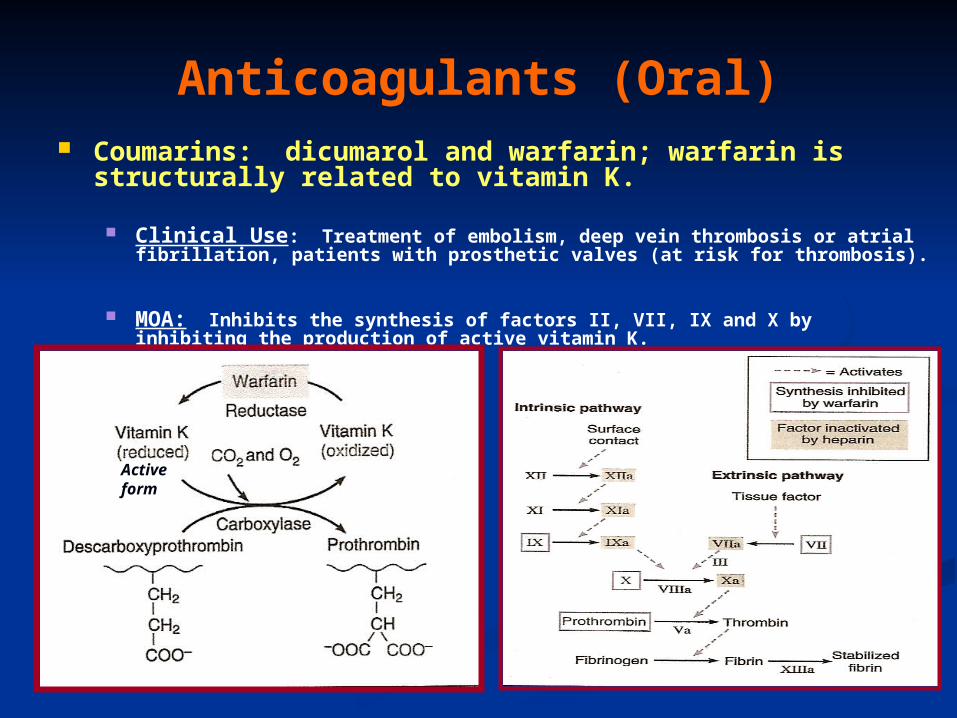
MOA: Inhibits the synthesis of factors II, VII, IX and X by inhibiting the production of active vitamin K.
Active form
Anticoagulants (Oral)
Coumarins: dicumarol and warfarin; warfarin is structurally related to vitamin K.
Pharmacokinetics: Route of administration: p.o.; 100% absorbed; 99% bound to plasma proteins; slow onset of activity; Hepatic elimination and excreted in the urine. Dicumarol is incompletely absorbed from the gut.
Side effects: Hemorrhage.
Contraindications: Patients with Hemophilia.
Drug Interactions: Drugs that inhibit CytoP450 Enzymes will increase levels, ie cimetidine, Macrolide antibiotics, antifungal agents. Drugs that induce CytoP450 enzymes will decrease levels, ie rifampin and Barbituates.
In case of overdose: Vitamin K (phytonadione)
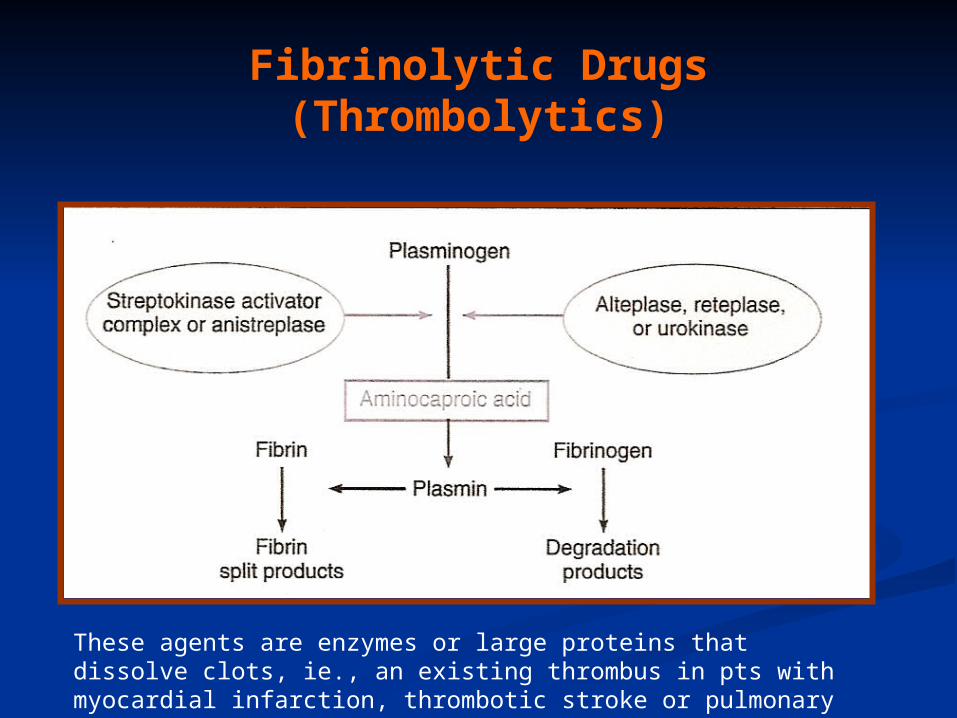
Fibrinolytic Drugs (Thrombolytics)
These agents are enzymes or large proteins that dissolve clots, ie., an existing thrombus in pts with myocardial infarction, thrombotic stroke or pulmonary embolism.

Fibrinolytic Drugs: (Thrombolytics)
Tissue Plasminogen Activator (t-PA); alteplase and reteplase MOA: It is a serine protease which activates plasminogen (bound to
fibrin) and increases plasmin levels. Clot specific and must bind to fibrin.
2 anti-plasmin
Fibrinolytic Drugs: (Thrombolytics)
Urokinase; enzyme obtained from urine MOA: Directly activates plasminogen; isolated from human
kidney, therefore less chance of evoking an allergic reaction.
Streptokinase: protein obtained from streptocci; anistreplase (a preformed complex of streptokinase and plasminogen)
MOA: Combines with plasminogen to form an active complex that converts plasminogen to plasmin to dissolve the fibrin.

Thrombolytics
Pharmacokinetics: Parental administration, i,.v.
Side effects: hemorrhage, hypersensitivity reactions and reperfusion arrythmias.
Contraindications: Bleeding disorders; recent surgery; severe hypertension.
Drug Interactions: Increases risk of bleeding with dicumarol, warfarn, heparin, aspirin, ticlopidine, abciximab.
In case of overdose: Aminocaproic acid inhibits fibrinolysis by competitively blocking plasminogen activation.

Antiplatelet Agents
GP: glycoproteinvWF: von Willebrand’s factor
Antiplatelet Agents Aspirin
Clinical Use: Prevention of atherosclerosis, thrombosis, transient ischemic attacks; unstable angina.
MOA: Irreversible cyclooxygenase inhibitor and inhibits the formation of thromboxane A2.
Pharmacokinetics: Oral administration
Side effects: Bleeding; gastrointestinal irritation, hypersensitivity reactions and thrombocypenia.
Contraindications: Bleeding disorders, hypersensitivity and Reye’s syndrome.
Drug Interactions: Increased hypoglycemic effects of sulfonylureas, inhibits uricosuric effect of probenecid.
In case of overdose: Forced Alkaline Diuresis

Antiplatelet Agents
Dipyridamole Clinical Use: Prosthetic valves; may be used as an adjunct with
aspirin therapy.
MOA: Lowers platelet calcium and increases the formation of cAMP (weak antiplatelet drug) , coronary vasodilator.
Pharmacokinetics: Oral administration
Side effects: GI distress, headache, dizziness and rash.
Contraindications: Hypersensitivity to this drug
Drug Interactions: Increases risk of bradycardia with Beta adrenergic receptor antagonists.

Antiplatelet Agents
Clopidogrel (Plavix®) Clinical Use: Prevention of atherosclerosis, thrombosis,
transient ischemic attacks; unstable angina.
MOA: Inhibits the binding of ADP to its receptor which is involved in the activation of platelet glycoprotein receptors binding to fibrinogen.
Pharmacokinetics: Oral administration; eliminated in urine and feces.
Side effects: Bleeding, neutropenia and thrombocytopenia.
Antiplatelet Agents Ticlopidine (Ticlid ®)
Clinical Use: Patients intolerant to aspirin; prevents thrombotic stroke.
MOA: Inhibits ADP-induced expression of platelet glycoprotein receptors and reduces fibrinogen binding and platelet aggregation. Effects on platelet function are irreversible.
Pharmacokinetics: Oral administration; eliminated in the urine and feces
Side effects: Bleeding; mild to moderate neutropenia, increased cholesterol and triglyeride levels.
Contraindications: Bleeding disorders, severe liver disease
Drug Interactions: Inhibits cytoP450 drug metabolizing enzymes.
Antiplatelet Agents
Abciximab Clinical Use: Percutaneous transluminal coronary
angioplasty as adjunct with aspirin and heparin.
MOA: Binds to platelet glycoprotein IIb/IIIa receptors and prevents binding to fibrinogen.
Pharmacokinetics: Parental administration, i.v.
Side effects: Bleeding, thrombocytopenia, hypotension and bradycardia.
Contraindications: Aneurysm, bleeding, recent surgery, stroke
Drug Interactions: Unknown
Hemostatic Agents
Aminocaprioic acid, Tranexamic acid, Antihemophilic factor, Antiinhibitor coagulants, Factor IX complex and Desmopressin
Clinical Use: Decrease bleeding which may be due to hereditary deficiencies, surgery, or thrombolytic overdose.